Embed Size (px)
Citation preview

EvaluatingBiologic Therapiesfor PsoriasisStrategies to ReduceCost and ImprovePatient Accessand Outcomes
EvaluatingBiologic Therapiesfor PsoriasisStrategies to ReduceCost and ImprovePatient Accessand Outcomes
Supported by an educational grant from AbbVie.Supported by an educational grant from AbbVie.
Faculty
William J. Cardarelli, PharmDDirector of Pharmacy Revenue and Supply
Atrius HealthHarvard Vanguard Medical Associates
Watertown, Massachusetts
Alan Menter, MDChair of Dermatology
Baylor University Medical CenterDallas, Texas
Disclosure
• Dr. Cardarelli, PharmD: None
• Dr. Menter, MD: Advisory Board—AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Janssen Biotech, Inc., LEO Pharma; Consultant—AbbVie, Allergan, Amgen, Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Vitae, Xenoport; Investigator—AbbVie, Allergan, Amgen, Anacor, BoehringerIngelheim, Celgene, Dermira, Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Merck & Co. Inc., Neothetics, Novartis, Pfizer, Regeneron, Symbio/Maruho, Xenoport; Speaker—AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma; Grant Support—AbbVie, Allergan, Amgen, Anacor, Boehringer Ingelheim, Celgene, Dermira, Janssen Biotech, Inc., LEO Pharma, Merck & Co. Inc., Neothetics, Novartis, Pfizer, Regeneron, Symbio/Maruho, Xenoport
Learning Objectives
• Quantify the clinical and economic consequences of suboptimal screening, delayed treatment, and patient nonadherence within the management of psoriasis and associated comorbidities
• Distinguish between the efficacy, safety, and pharmacoeconomic profiles of biologic therapies
• Translate consensus statements and recent clinical outcomes data of biologic therapies to informed formulary decisions
• Employ health plan strategies that assist providers in improving screening, monitoring, and patient adherence to treatment
Overview of Psoriasis
• Approximately 7.5 million people in the United States have psoriasis
• Psoriasis occurs in all age groups but is primarily seen in adults
• Psoriasis usually occurs on the scalp, knees, elbows, hands, and feet
• Approximately 80% of those affected with psoriasis have mild to moderate disease, whereas 20% have moderate to severe psoriasis affecting >5% of the body surface area
• The most common form of psoriasis, affecting approximately 80% to 90% of patients with psoriasis, is plaque psoriasis
– Characterized by patches of raised, reddish skin covered with silvery-white scale
• In 2013, the total direct cost of treatment associated with psoriasis was estimated to be between $51.7 and $63.2 billion
• The average age of mortality for patients with psoriasis is approximately 10 years less than the general population
American Academy of Dermatology. https://www.aad.org/media/stats/conditions/psoriasis. Accessed May 5, 2016. International Federation of Psoriasis Associations. Psoriasis is a serious disease deserving global attention.pdf. www.ifpa-pso.org. Accessed May 18, 2016.
Comorbidities Associatedwith Psoriasis
• The incidence of Crohn’s disease and ulcerative colitis, two types of inflammatory bowel disease, is 3.8 to 7.5 times greater in patients with psoriasis than in the general population
• Patients with psoriasis also have an increased incidence of lymphoma, heart disease, obesity, type 2 diabetes mellitus, and metabolic syndrome
• Depression and suicide, smoking, and alcohol consumption are also more common in patients with psoriasis
• The prevalence of depression in patients with psoriasis may be as high as 50%
• Studies have shown that patients with psoriasis experience physical and mental disability just like patients with other chronic illnesses such as cancer, arthritis, hypertension, heart disease, and diabetes mellitus
American Academy of Dermatology. https://www.aad.org/media/stats/conditions/psoriasis. Accessed May 5, 2016.
Barriers to Patient Care
• Stigma
• Persistent symptoms
• Medication side effects
• Insurance coverage
• Comorbidities
• Nonadherence
Eissing L, et al. J Eur Acad Dermatol Venereol. 2016;30(4):569-575.
Barriers to Healthcare System
• Poor flow of data between system and caregiver
• Delivery of system design
• Poor integration of behavioral health into primary care
• Reimbursement hurdles
Biologics
• Biologics include a range of products
– Vaccines
– Blood and blood components
– Gene therapy
– Recombinant therapeutic proteins
• Biologics are composed of sugars, proteins, or nucleic acids or complex combinations of these substances, or may be living entities such as cells and tissues
• Biologics are isolated from a variety of natural sources
– Human
– Animal
– Microorganisms
What are Biologics Questions and Answers. http://www.fda.gov/aboutfda/centersoffices/officeofmedicalproductsandtobacco/cber/ucm133077.htm. Accessed May 6, 2016.
Biologic Drug Classes
• Tumor necrosis factor-alpha (TNF-α) blockers
– Certolizumab pegol
– Etanercept
– Adalimumab
– Infliximab
– Golimumab
• IL-12/23
– Ustekinumab
• IL-17A
– Secukinumab
– Ixekizumab
IL = interleukin.National Psoriasis Foundation. https://www.psoriasis.org/about-psoriasis/treatments/biologics. Accessed May 14, 2016.
EvaluatingBiologic Therapiesfor PsoriasisStrategies to Reduce Cost and Improve Patient Access and Outcomes
EvaluatingBiologic Therapiesfor PsoriasisStrategies to Reduce Cost and Improve Patient Access and OutcomesAlan Menter, MDAlan Menter, MD
Apremilast
PDE4 = phosphodiesterase 4.Bjørgo E, et al. Handb Exp Pharmacol. 2011;204:345-363. Gottlieb AB, et al. Curr Med Res Opin.2008;24(5):1529-1538. Schafer PH, et al. Br J Pharmacol. 2010;159(4):842-855. Otezla [product information]. Summit, NJ: Celgene Corp; 2015.
Attenuation of T-cell activation
Broad anti-inflammatory effectson immune accessory cells
Possible direct effectson keratinocytes
Predicted mechanistic effects of (PDE4 inhibitor) in psoriasis

Week
Oral Apremilast (CC-10004) Phase 3 Study: ESTEEM 2 Study Design
• A randomized, double-blind, placebo-controlled, phase 3, efficacy, and safety study (NCT01232283)
• Patients had moderate to severe plaque psoriasis(PASI score ≥12, PGA ≥3, BSA ≥10%)
*Patients who achieved >PASI 50 response were re-randomized to apremilast or placebo.BID = twice daily; BSA = body surface area; PASI = Psoriasis Area and Severity Index; PGA = Physician Global Assessment.http://clinicaltrials.gov/show/NCT01232283. Paul C, et al. J Am Acad Dermatol. 2014;70(suppl 1):AB184(Abstract #P8412).
0 4 8 12 16 20 24 28 36 44 5232 40 48
Screening
Ran
do
miz
atio
n(2
:1)
Oral Placebo BID (n=138) Oral Apremilast 30 mg BID
Oral Apremilast 30 mg BID
Oral Placebo BID
Oral Apremilast 30 mg BID
Oral Apremilast 30 mg BID (n=275)
Loss of Response
Re-randomization* (1:1)
Oral Apremilast (CC-10004)Phase 3 Study: ESTEEM 2
Results
• At week 16, significantly more patients receiving APR30 achievedthe following:
– PASI 75: 28.8% 30 mg vs 5.8% placebo
– PASI 50: 55.5% 30 mg vs 19.7% placebo
– In patients receiving apremilast, diarrhea and nausea were predominantly mild in severity,had the highest incidence during the first week of dosing, and generally resolvedwithin 1 month
– SAEs (including serious infections, malignancies, and cardiovascular events) and laboratory value changes were consistent with prior apremilast studies; SAEs were lowacross treatment groups
Conclusion
• Apremilast significantly reduced the severity of moderate to severe psoriasis, including nail, scalp, and palmoplantar involvement, and was generally well tolerated with no new safety or laboratory findings
APR30 = apremilast 30 mg; SAE = serious adverse event.Rich P, et al. J Am Acad Dermatol. 2016;74:134-142.
Apremilast: Overall Safety Summary
• No new significant AEs were identified in these phase 2 trials
• AEs
– Increase in nausea, diarrhea, and headache: Up to 20% of patients
• Mostly mild and seen predominately in initial 3 to 4 weeks of treatment
– Weight loss (1-5 kg)
– Depression (occasional patient)
• No changes in laboratory parameters
• No cases of tuberculosis (new infection/reactivation) reported
• Approved for the treatment of psoriasis and psoriatic arthritis in 2014
AE = adverse event.Papp K, et al. Poster presented at the 72nd Annual Meeting of the AAD, Denver, CO, 2014 (Poster #8359); Paul C, et al. Poster presented at the 72nd Annual Meeting of the AAD, Denver, CO, 2014 (Poster #8412); Reich K, et al. Poster presented at the 72nd Annual Meeting of the AAD, Denver, CO, 2014 (Poster #8296). Apremilast (Otezla) National Drug Monograph. VA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives; January 2015.
Current FDA-Approved Biologic Therapies for Psoriasis
FDA = US Food and Drug Administration.
Type Agent Indication
TNF-α antagonists
EtanerceptPsoriatic arthritis,
Psoriasis
InfliximabPsoriatic arthritis,
Psoriasis
AdalimumabPsoriatic arthritis,
Psoriasis
IL-12/IL-23 antagonist UstekinumabPsoriatic arthritis,
Psoriasis
IL-17A antagonistIxekizumab Psoriasis
SecukinumabPsoriatic arthritis,
Psoriasis
Etanercept
• Only soluble TNF receptor antagonist
– Fully human protein
– Does not bind complement in vitro*(ie, not associated withcomplement-mediated cell lysis)
• Low immunogenicity
• Dosing schedule maintains stable serum concentrations
• Subcutaneous injection
*Clinical significance is unknown.TNF = tumor necrosis factor; IgG = immunoglobulin G.Enbrel [package insert]. Thousand Oaks, CA: Amgen; 2015.
Fc regionof humanIgG1
Extracellular domain of high-affinityhuman p75 TNF receptor
Etanercept in Psoriasis (Phase 3 US Study): PASI 75 Response
*P=.0006; †P<.0001 vs placebo.BIW = twice weekly; QW = once weekly.Leonardi C, et al. N Engl J Med. 2003;349:2014-2022.
0
80
Pe
rce
nta
ge
of
Pa
tie
nts
(%
)
12 Weeks
20
60
40
10
50
70
30
Placebo/Etanercept 25 mg BIW
Etanercept 25 mg QW
Etanercept 25 mg BIW
Etanercept 50 mg BIW
N=652
4
0
80
24 Weeks
20
60
40
10
50
70
30
33
*14
†
34
†
49
25
44
59
Infliximab
Indications
• Rheumatoid arthritis, Crohn’s disease, psoriatic arthritis, ulcerativecolitis, ankylosing spondylitis
Contraindications
• Serious infection
• Thrombocytopenia
• Malignancies
Administration
• Intravenous infusions 5 mg/kg atweeks 0, 2, and 6 weeks, thenevery 8 weeks
Remicade [package insert]. Horsham, PA: Janssen Biotech, Inc; 2015.
HumanFc Region
MouseFabRegion
MouseHeavy Chain
HingeRegion
S-SS-S
NH2
NH2 NH2
NH2
HumanHeavy Chain
COOH COOH
TNF-BindingRegion
TNF-BindingRegion
Infliximab in Psoriasis: Maintenance of Response through Week 50
Key points of two EXPRESS studies
• PASI score at week 10 was 75% but at week 50 was 60%
• Thus, approximately 25% of patients will lose PASI 75 response over 1 year of therapy
• Persistence of a PASI 75 response is associated with the maintenance of detectable serum levels of infliximab between infusions
– 5% of patients had significantly abnormal liver function test results(5X baseline)
EMEA = European Medicines Agency; MTX = methotrexate.Reich K, et al. Dermatology. 2010;221(2):172-178. Menter A, et al. J Am Acad Dermatol. 2007;56:31.e1-e15.
Question: Why were dermatologists not allowed (EMEA and FDA)to use concomitant MTX during these two pivotal studies?
Always allowed in rheumatology studies!
Review of Infliximab Treatment for Psoriasis in Patients Receiving Therapy for at Least 1 Year
Study
• 120 patients with psoriasis were treated with infliximab at Baylor, Dallas, between 2002 and 2008
Results
• Mean follow-up: 2.2 years
• >90% clear at week 12
• Concomitant MTX required by 52% of patients
• >1 standard dose of 5 mg/kg required by 87% of patients every 8 weeks to maintain clearance
• 16% of patients discontinued infliximab post 1 year of treatment, primarily due to loss of response
Kamili QU, et al. J Drugs Dermatol. 2011 May;10(5):539-544.
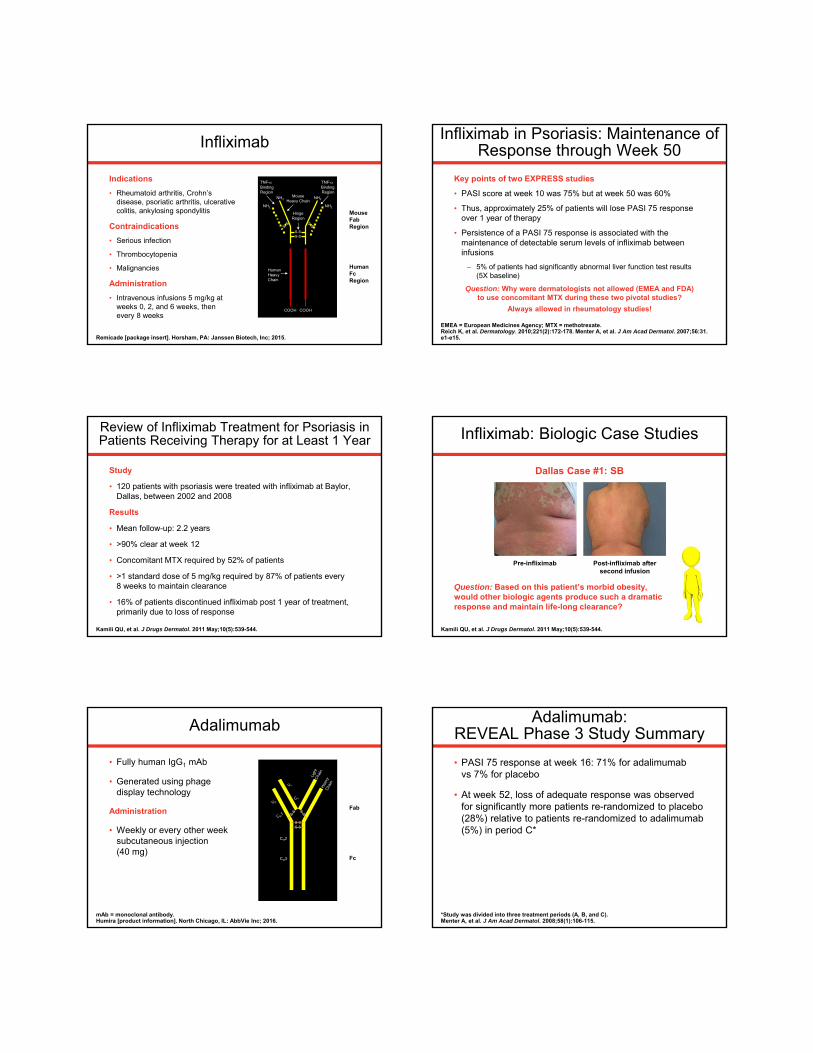
Infliximab: Biologic Case Studies
Question: Based on this patient’s morbid obesity, would other biologic agents produce such a dramatic response and maintain life-long clearance?
Kamili QU, et al. J Drugs Dermatol. 2011 May;10(5):539-544.
Dallas Case #1: SB
Pre-infliximab Post-infliximab after second infusion
Adalimumab
• Fully human IgG1 mAb
• Generated using phage display technology
Administration
• Weekly or every other week subcutaneous injection(40 mg)
mAb = monoclonal antibody.Humira [product information]. North Chicago, IL: AbbVie Inc; 2016.
Fc
Fab
S-SS-S
CH2
CH3
Adalimumab:REVEAL Phase 3 Study Summary
• PASI 75 response at week 16: 71% for adalimumabvs 7% for placebo
• At week 52, loss of adequate response was observed for significantly more patients re-randomized to placebo (28%) relative to patients re-randomized to adalimumab (5%) in period C*
*Study was divided into three treatment periods (A, B, and C).Menter A, et al. J Am Acad Dermatol. 2008;58(1):106-115.

Adalimumab: Results from an Open-Label Extension Study for Patients from REVEAL
Results
• 75% / 90% / 100% improvement in PASI score response rates (last observation carried forward) was sustained in 83% / 59% / 33% of patients after100 weeks and 76% / 50% / 31% after 160 weeks of continuous therapy, respectively
• Some patients with less than PASI 75 responses in REVEAL also achieved long-term PASI 75 responses
Gordon K, et al. J Am Acad Dermatol. 2012 Feb; 66(2):241-251.
Adalimumab: Efficacy of Switching between TNF-α Inhibitors in Psoriasis
• Italian Psocare Registry study of 5423 patients receiving TNF-αtherapy (September 2005-September 2010)
• Study looked to assess the variables that predicted the efficacy of TNF-α switching
• 105 patients who switched to a second TNF-α inhibitor were assessed
• 75% improvement in PASI 75 score was reached by 29% after16 weeks and by 45.6% after 24 weeks
• Patients who switched because of secondary loss of efficacy(loss of initial PASI 75 response) or AEs/intolerance were more likely to reach PASI 75 than those who switched as a result of primary inefficacy (PASI 75 never achieved)
Piaserico S, et al. J Am Acad Derm. 2014;70(2):257-262.e3.
Ustekinumab: Key Actions of IL-12and IL-23 in Psoriasis
Torti DC, et al. J Am Acad Dermatol. 2007;57:1059-1068. Fantuzzi F, et al. Expert Opin Ther Targets. 2008;12(9):1085-1096.
Ustekinumab is not known to bind to any other cytokines
SkinPlaques
keratinocyte
hyperproliferation
TH1 cell
differentiation
TNF-
IFN-
keratinocyte
hyperproliferation
TH17 cell
differentiation
IL-17
IL-22
TNF-
SkinPlaques
Increasedinflammation
pro-inflammatory
factors
IL-12
p40p35
IL-23
p40p19
Ustekinumab
Ustekinumab:Phase 3 PASI Response over 28 Weeks
P<.001 vs placebo for all comparisons.ITT = intention to treat; NRI = nonresponder imputation. Leonardi CL, et al. Lancet. 2008;371(9625):1665-1674.
PHOENIX 1: Week 28ITT-NRI
0
100
Pe
rce
nta
ge
of
Pa
tie
nts
(%
)
PASI 90PASI 50
20
60
80
40
PASI 75
90
10
50
70
30
PHOENIX 2: Week 28ITT-NRI
0
100
PASI 90
20
60
80
40
PASI 50 PASI 75
90
10
50
70
30
Ustekinumab 45 mg (n=250)
Ustekinumab 90 mg (n=243)
9196
71
79
4956
93 95
70
79
45
54
Ustekinumab 45 mg (n=397)
Ustekinumab 90 mg (n=400)
Results of Ustekinumab Treatment after 1 Injection
Baseline Week 12
Review of Ustekinumab Treatment for Psoriasis inPatients Maintained on Therapy for at Least 1 Year
Study
• Medical records of 119 patients with psoriasis treated with ustekinumab at referral clinic in Dallas between 2009 and 2013 were reviewed for response rates, side effects, and concomitant therapies
Results
• Median follow-up: 31 months
• 47% (56) of patients obtained near-complete clearance (ie, response of >90% of initial body surface area involvement) upon final follow-up visit or when ustekinumab treatment was discontinued
• 50% (59) of patients received concomitant systemic treatments, primarily MTX
• 42% (50) of patients required either an increase in the dose of ustekinumab to90 mg and/or administration more frequently than every 12 weeks to achieve and maintain psoriasis clearance
• 19% (23) of patients discontinued treatment, primarily for suboptimal response or loss of response
Wilder EG, et al. J Drugs Dermatol. 2014;13(8):905-910.

The IL-17 Family Includes6 Cytokines (IL17A – IL-17F)
Gu C, et al. Cytokine. 2013 Nov;64(2):477-485.
Family Member Main Function Receptor
IL-17A • Neutrophil recruitment• Extracellular pathogen defense• Bone metabolism• Regulation of intestinal inflammation• Endothelial cell migration and angiogenesis• Keratinocyte proliferation
IL-17RAIL-17RC
IL-17F
IL-17A/F heterodimer
IL-25 (IL-17E)
• Promotes TH2 responses• Modulates allergic responses and asthma• Provides protective immunity to extracellular
pathogens (eg, parasitic infections)
IL-17RAIL-17RB
IL-17B
Under investigation
IL-17RB
IL-17C IL-17RE
IL-17D Unknown
• Humanized IgG4 mAb against IL-17A
– Contains Ser to Pro mutation in the hinge region to prevent the formation of half antibodies
• Neutralizes IL-17A homodimers and IL-17A/F heterodimers
– Half-life: 10.5 days
• Positive proof-of-concept
– Psoriasis
– Rheumatoid arthritis
Ixekizumab
Leonardi C, et al. N Engl J Med. 2012;366(13):1190-1199. Genovese MC, et al. Arthritis Rheum. 2010;62(4):929-939.
Th17 cell
dectin-1dectin-2
Dendriticcell
TLR2
Staphylococcus speciesStreptococcus species Candida species
IL-23
IL-22(and IL-17A)
Keratinocyte proliferation
IL-17A(and IL-22)
TNF-
Keratinocytes
Proinflammatorycytokine production(eg, TNF-)
Antimicrobialpeptide production
Neutrophil accumulationIL-17A
IL-17 receptor
IL-17 receptor
TNF-
Ixekizumab Selectively Blocks IL-17A
Anti-Interleukin-17Monoclonal Antibody Ixekizumab
in Chronic Plaque Psoriasis
Leonardi C, et al. N Engl J Med. Mar 2012;366(13):1190-1199.
• Back-to-back publication with brodalumab
Ixekizumab: Anti-IL-17 mAbin Chronic Plaque Psoriasis
Study
• Phase 2, double-blind, placebo-controlled trial
• 142 patients with moderate to severe plaque psoriasis
• Subcutaneous injections of 10, 25, 75, or 150 mg ixekizumab or placebo at weeks 0, 2, 4, 8, 12, and 16
Results
• PASI 75 at week 12: 82% vs 7.7% at the 150-mg dose
• PASI 90 at week 12: 71% vs 0% for the 150-mg dose
• AEs occurred in 63% of patients in both groups
• No SAEs or MACEs were observed
MACE = major adverse cardiovascular event.Leonardi C, et al. N Engl J Med. Mar 2012;366(13):1190-1199.
10
0
20
30
40
50
60
70
80
90
100
20181614121086420
Ixekizumab: PASI 100 Responseover Time to Week 20
*P<.05 compared to placebo.Leonardi C, et al. N Engl J Med. Mar 2012;366(13):1190-1199.
Pe
rce
nta
ge
of
Pa
tie
nts
(%
)
Weeks
Ixekizumab 10 mg
Ixekizumab 25 mg
Ixekizumab 75 mg
Ixekizumab 150 mg
Placebo
***
**
*
* **
**

Ixekizumab: Key Findings
• Ixekizumab had a rapid onset of action as evidenced bythe following:
– Impressive PASI scores in the two highest-dose groupscompared to placebo at week 1
– Higher percentage of patients in the highest-dose group with PASI 75 or sPGA score of 0 or 1 at week 2
• Approximately 40% of patients in the two highest-dose groups (PASI 100 and sPGA 0) had clear skin at 12 weeks
• There were no SAEs
• TEAEs were similar across groups with no dose-related trend in any individual TEAE
sPGA = Static Physician’s Global Assessment; TEAE = treatment-emergent adverse event.Leonardi C, et al. N Engl J Med. Mar 2012;366(13):1190-1199.
IL-23
IL-17A
Secukinumab: An mAb That Selectively Targets IL-17A
Yamauchi PS, et al. J Drugs Dermatol. 2015;14(3):244-253. Nestle FO, et al. N Engl J Med. 2009;361(5):496-509. Mease PJ. Curr Opin Rheumatol. 2015;27(2):127-133. Lønnberg AS, et al. Clin Cosmet Investig Dermatol. 2014;7:251-259. Cosentyx [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
IL-23receptor
TNF-
IL-12
IL-22
TH17
IL-17Areceptor
IL-23
Secukinumab: An mAb That Selectively Targets IL-17A
Cosentyx [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2015.
.
IL-23receptor
TNF-
IL-12
IL-22
TH17
IL-17Areceptor
IL-17A
Secukinumab
The clinical significance of the secukinumab mechanism of action is unknown
Secukinumab in Plaque Psoriasis —Results of Two Phase 3 Trials
Langley RG, et al. N Engl J Med. 2014;371(4):326-338.
Secukinumab Induction and Maintenance Regimen: Finding Study
Study
• Phase 2, randomized, double-blind, placebo-controlled
• 404 patients with moderate to severe psoriasis
• 150-mg induction subcutaneous injections
Results
• PASI 75 and PASI 90 at weeks 20 and 28 for fixed interval vs start of relapse
– Fixed interval: 85% PASI 75 and 58% PASI 90
– Start of relapse: 67% PASI 75 and 21% PASI 90
Safety
• Nil increase in infection rates vs placebo
Rich P, et al. Br J Dermatol. 2013 Feb;168(2):402-411.
Not Using a Biologic in a Patient with Moderate to Severe Psoriasis May Cause…
• Deformed joints
• Decreased quality of life
• Heart attacks
• Strokes
• Early death
Menter A, et al. J Am Acad Dermatol. 2008;58(5):826-850.

Biosimilars Are Projected to Moderate Drug Expenditures and Expand Patient Access to Biologics
• Continuing growth in US prescription drugs
– Top drugs for first 9 months of 2014 based on expenditures
• In clinics: infliximab, pegfilgrastim, epoetin alfa
• In hospitals: infliximab, rituximab, pegfilgrastim
– 7% to 9% projected increases in total drug expenditures for 2015 across all settings
• Biosimilars are predicted to lead to a $44.2 billion reduction (range, $13-$66 billion) in direct spendingon biologic drugs from 2014-2024
Schumock GT, et al. Am J Health Syst Pharm. 2015;72(9):717-736. Mulcahy AW, et al. http://www.rand.org/content/dam/rand/pubs/perspectives/PE100/PE127/RAND_PE127.pdf. Accessed June 2015.
Definitions
• According to the FDA, biosimilar or biosimilarity means:
• That the biological product is highly similar to the reference product notwithstanding minor differences in clinically inactive components
— AND —
• There are no clinically meaningful differencesbetween the biological product and the reference product in terms of the safety, purity, and potency of the product
FDA. http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm290967.htm. Accessed June 2015.
Biosimilars Are Approved According to Specific, Highly Stringent Regulations
• Quality standards for biosimilars are the same as for original biologics
• In highly regulated countries, biosimilars are evaluated according to rigorous guidelines and must have the following:
– Highly comparable structural and functional attributes
– No clinically relevant differences
• Products that do not meet these high standards are not approved and not put into circulation
• Biosimilars have been in use in Europe since 2006 with safety profiles comparable to their respective reference product
Strober BE, et al. J Am Acad Dermatol. 2012 Feb;66(2):317-322.
The Many Faces of Psoriasisand Psoriatic Arthritis
Dactylitis Arthritis mutilans Enthesitis
Evolution of Psoriasis Immunopathogenesis and Therapeutic Approaches over the Past 3 Decades
• A disease of keratinocyte dysfunction (pre-1980s)
– Therapeutic approach: MTX, UVB, PUVA, retinoids
• An immunologic disease (1980s)
– Therapeutic approach: Cyclosporine
• An IL-12/Th1-mediated disease (1990-2004)
– Therapeutic approach: Anti-CD2, anti-CD11a, TNF-α blockers
• An IL-23/Th17-mediated disease (2005-present)
– Multiple therapeutic approaches: IL-12/IL-23, IL-23, IL-17, IL-17R blockers
UVB = ultraviolet light B; PUVA = psoralen + ultraviolet light A; TNF = tumor necrosis factor.Blauvelt A. Expert Rev Dermatol. 2007;2(1):69-78. Di Cesare A, et al. J Invest Dermatol. 2009;129(6):1339-1350. Martin DA, et al. J Invest Dermatol. 2013;133(1):17-26.
New Biologics:General Impressions
• PASI 90 is the new PASI 75!
• New biologics are more targeted to the skin immune system than to the systemic immune system, which makes efficacy very high and safety profiles very good
• It is too early to say whether biologics willimprove systemic inflammation and decrease cardiovascular risks
Langley, RG, et al. N Engl J Med. 2014 Jul 24;371(4):326-338.

IL-23 Drugs in Development
Tildrakizumab: A Humanized IgG1κ mAb that Targets the Unique p19 Subunit of IL-23
Clinical trials
• Results from a randomized, double-blind, phase 2b clinical trial showed that tildrakizumab was effective in treating moderate to severe plaque psoriasis
• At week 16, the proportion of subjects achieving PASI 75 was significantly higherat all doses when compared to placebo (4.4%)
– 33.3% on 5 mg
– 64.4% on 25 mg
– 66.3% on 100 mg
– 74.4% on 200 mg
• The final drug dose was given on week 40, and the participants were followeduntil week 72
• Tildrakizumab demonstrated a low rate of relapse after cessation of therapy,with only 3.6% of the participants who achieved PASI 75 at week 52 on anydose of tildrakizumab relapsing before week 72
• Phase 3 studies are in progress
Tildrakizumab (MK-3222) [product information]. Whitehouse Station, NJ: Merck & Co; 2016. Campa M, et al. Dermatol Ther (Heidelb). 2016 Mar;6(1):1-12.
Tildrakizumab: An Anti-IL-23 mAbthat Improves Psoriasis (Phase 2)
Note: Tildrakizumab is not currently FDA approved for psoriasis.Presented at the 71st American Academy of Dermatology Annual Meeting. Miami, FL; 2013.
10PA
SI
75
Re
sp
on
se
Ra
te (
%)
0
20
30
40
50
60
70
80
161286420
Weeks
Placebo100 mg
200 mg
5 mg
25 mg
BI-655066
• BI-655066 is a high-affinity mAb targeting the p19 subunit of IL-23 and is currently in development for moderate to severe psoriasis and Crohn’s disease
Clinical trials
• A phase 1, proof-of-concept study of BI-655066 demonstrated a similar frequency of side effects with varying doses of BI-655066 compared to placebo
• The most common side effects were mild to moderate upper respiratory infections, mild nasopharyngitis, and mild to moderate headache
• After a single intravenous or subcutaneous dose, PASI 75 was achieved in 87% of subjects, PASI 90 in 58% of subjects, and PASI 100 in 16% of subjects
• Additional trials are ongoing
BI-655066 [product information]. Ingelheim, Germany: Boehringer Ingelheim; 2015. Krueger JG, et al. J Allergy Clin Immunol. 2015;136:116-124.e7.
Guselkumab (CNTO 1959)
• Guselkumab (CNTO 1959) is a fully human IgG1λ monoclonal IL-23 antagonist targeting the unique p19 subunit of IL-23
Clinical trials
• In a phase 2, randomized, double-blind, placebo-controlled, dose-ranging, active-comparator study, patients randomized to guselkumab were significantly more likely to achieve a PGA score of 0 (clear) or 1(almost clear) at 16 weeks when compared to placebo: 34% in the 5-mg dose group, 61% in the 15-mg dose group, 79% in the 50-mg dose group,86% in the 100-mg dose group, 83% in the 200-mg dose group, and7% in the placebo group
• At 16 weeks, a score of 0 or 1 on the PGA was seen in 58% of patients randomized to adalimumab, which was significantly lower than the 50-mg, 100-mg, and 200-mg doses of guselkumab
Guselkumab (CNTO 1959) [product information]. Beerse, Belgium: Janssen Research and Development. Gordon KB, et al. N Engl J Med. 2015;373:136-144.
IL-23 and IL-17 as Treatment Targets in Psoriasis
Conclusions
• Both IL-23 and IL-17 are promising targets in the treatment of moderate to severe plaque psoriasis
• Biologic drugs targeting these cytokines and their receptors have proved to be effective and safe in clinical trials and have offered greater efficacy than pre-existing biologics
– Evidenced by large proportions of patients achieving not only PASI 75 but also PASI 90 and PASI 100
• It is important to be vigilant in following the safety profile of these drugs both in clinical trials and in post-marketing registries to ensure their long-term safety
Campa M, et al. Dermatol Ther (Heidelb). 2016 Mar;6(1):1-12.

Biopharmaceuticals and Biosimilarsin Psoriasis: What the Dermatologist
Needs to Know
Strober BE, et al. J Am Acad Dermatol. 2012 Feb;66(2):317-322.
EvaluatingBiologic Therapiesfor PsoriasisStrategies to Reduce Cost and Improve Patient Access and Outcomes
EvaluatingBiologic Therapiesfor PsoriasisStrategies to Reduce Cost and Improve Patient Access and OutcomesWilliam Cardarelli, PharmDWilliam Cardarelli, PharmD
Opportunities for P&T Committee
• Increase committee’s knowledge of psoriasis therapies
– Both current and emerging therapies
• Develop evidence-based guidelines for earlier treatment intervention
– Work closely with thought leaders to adapt recommendations as bestpractices change
– Understand the value of early diagnosis and treatment
• Explore opportunities for innovative strategies that maintain access while reducing costs
– Maximize adherence to lower overall costs and improve outcomes
– Consider formulary designs that reduce patient out-of-pocket spending
– Is this a place for the Medical Home?
P&T = Pharmacy and Therapeutics.American Society of Health-System Pharmacists. ASHP guidelines on the pharmacy and therapeutics committee and the formulary system. Am J Health-Syst Pharm. 2008; 65:1272-83.
American Academy of Dermatology Clinical Decision Tree
*Patients with nondeforming psoriatic arthritis without any radiographic changes, loss of range of motion, or interference with tasks of daily living should not automatically be treated with TNF inhibitors. It would be reasonable to treat these patients with nonsteroidal anti-inflammatory agent or to consult rheumatologist for therapeutic options. †Patients with limited skin disease should not automatically be treated with systemic treatment if they do not improve, because treatment with systemic therapy may carry more risk than the disease itself.PUVA = psoralen plus ultraviolet (UV)-A.American Academy of Dermatology. Accessed May 10, 2016 @https://www.aad.org/mobile-psoriasis/#clinical-decision-tree. Menter A, et al. J Am Acad Dermatol. 2008;58(5):826-850.
Anti-TNF +/- MTX*
UVB / PUVATopicals/
Targeted phototherapy
YES
Systemic Biologic
Psoriasis +/- Psoriatic Arthritis
NO
Lack of Effect†
Limited Disease Extensive Disease
Coverage Issues
• What are the trends?
• Guideline revisions?
• Earlier, more aggressive therapy?
• Oral drugs are covered under pharmacy benefit, but access to drugs covered under medical benefit subject to P&T review
• Supportive medications: Coverage determined by route of administration
• Medicare Part B vs Part D determination further blurs the boundaries of coverage

Comparison of Annual Treatment Costs of Selected Agents
*Dosing regimens for adalimumab and ustekinumab are based on FDA recommendations. Dosing regimen for etanercept is based on the PRESTA trial. †Average wholesale price was determined from the Red Book Drug Topics, 2014. USD = United States dollar.Cheng J, et al. Drugs in Context. 2014;3:212266. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295913/pdf/212266.pdf. Accessed May 28, 2016.
TreatmentRecommended Dosage
Schedule*
AverageWholesale Price†
(2014 USD)
Initial Then Maintenance
(USD)Maintenance
(USD)
EtanerceptInitial: 50 mg twice weekly
for 3 months, then50 mg once weekly
15.47/mg 46,395 37,311
Adalimumab
Initial 80-mg single dose,then 40 mg every otherweek starting 1 week
after initial dose
46.92/mg 39,041 36,038
Ustekinumab
Initial: Assuming≤100 kg: 45 mg at 0 and
4 weeks, then every12 weeks thereafter
196.63/mg 53,909 44,924
Actual Total Cost
• Whether a product is being bought or sold, price is only a part of the actual total cost
• Costs of quality, including paying for outcomes, and costs of the transaction, including resources, effort, time, payment terms, and renegotiations, must be considered when assessing or comparing actual total costsof propositions, products, or services
© Christopher Barrat & Alan Chapman 2004. www.businessballs.com. Accessed May 19, 2016.
PriceUnit cost
ValueThe right product
at the righttime and place
(quality andoutcome)
TransactionCost of resources,
effort, time, anddoing business
Comparative Effectiveness Research
• Direct comparison of existing healthcare interventions
• Assists patients and providers in making informed decisions to improve healthcare for individuals and the overall population
• Pragmatic trials: Clinical research trials
– Measure effectiveness: The benefit a treatment produces in routine clinical practice
– Different from regular clinical trials that measure efficacy: Whether the treatment works
• Two methods used by researchers to gather evidence
– Study the available evidence of each choice for different groups of patients from existingclinical trials, clinical studies, and other research
– Facilitate trials to find new evidence of effectiveness or comparative effectiveness of a test, treatment, procedure, or healthcare service
Agency for Healthcare Research and Quality. What Is Comparative Effectiveness Research. http://effectivehealthcare.ahrq.gov/index.cfm/what-is-comparative-effectiveness-research1/. Accessed November 20, 2012. Roland M, et al. BMJ. 1998;316:285.
MCO Initiatives toImprove Outcomes and Adherence
• Value-based benefit design
• Medication therapy management
• Formulary management
• Pay-for-performance
• Strengthen patient-provider relationships
• Patient empowerment
• Integrated communication channels
• Telephone counseling
• Medication reminders
MCO = managed care organization.Tutty S, et al. Eff Clin Pract. 2000;3(4):170-178. Hoffman L. Am J Manag Care. 2002;9:70-80.
Provider Strategies toIncrease Adherence
• Active patient participation
• Adequate communication
• Family support
• Positive reinforcement by provider
• Simplified drug regimen
Strategies to Improve Medication Adherence: Integrated Communication Channels
• Multi–provider-level communication with patients regarding the importance of medication adherence
– Physicians
– Pharmacists
– Nurses
– Case managers
• Provider responsibilities
– Communicate respect for the patient's perspective of his/her condition
– Provide rationale for any recommended treatment
– Negotiate a plan and anticipate and address problems
– Discuss adherence at every visit in a nonjudgmental way
– Establish a collaborative process of problem solving
Roter D. J Pharmacoepidemiol. 1995;3:37-48.

Biosimilar vs Interchangeable
Biosimilar
• Highly similar to the US-licensed reference biologicproduct notwithstanding minor differences in clinically inactive components
• No clinically meaningful differences from the reverence product in terms of safety, purity, and potency
FDA. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/default.htm. Accessed May 19, 2016.
Biosimilar vs Interchangeable (cont)
Interchangeable
• Biosimilar to the US-licensed reference product
• Expected to produce the same clinical result to the reference product in any given patient
• If a product is indicated for multiple administrations, then the product must be able to be alternated with the reference product without any loss of efficacy or change in risk of AEs
• Product may be substituted at the pharmacy level without the intervention of a healthcare provider
FDA. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/default.htm. Accessed May 19, 2016.
Outstanding Questions
• Is the pathway to biosimilars still a work in progress?
• Is the cost to conduct studies and to achieve interchangeability prohibitive?
• How comfortable will physicians be prescribing biosimilar agents?
• How will MCOs manage these agents?
FDA. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/default.htm. Accessed May 19, 2016.
Algorithm forFormulary Decision Making
Drug review—oral/writtenpresentation by clinical pharmacist
Experience/opinion—oral comments byinvited consultants and committee members
Does drug offer substantial improvement in therapy overexisting formulary drugs for like indications, or is it a
completely new therapy not previously covered by medications?
Add to formulary with guidelines forcost-effective and safe use if needed
Does drug offer at least equal clinical benefit toexisting formulary drugs for like indications?
Add to formulary with guidelines forcost-effective use if needed
Do not add toformulary
Do not add toformulary
Can any safety concernsbe managed?
Does financial impact of drugsupport formulary addition?
NO
YES
NO
NO
NOYES
YES
YES
The Future ofPharmacy Benefit Management
• The role of the pharmacy will become more prominent as healthcare reform unfolds
– The pharmacy will be forced out of its “silo” and into the care team
• Accountable care organization models will require more integration of medical and pharmacy data
– Physicians can no longer be agnostic to costs whether they occur in the medical arena or the pharmacy arena
• Aggressive management of the drug benefit and the pharmacy network will be critical to the ability of the MCOs to provide affordable access to drugs
– Narrow pharmacy networks
– Medication therapy management
– Trend management tools for specialty pharmacy drugs
Berger J, et al. Am J Pharm Benefits. 2014;6(3):124-128. http://www.ajpb.com/journals/ajpb/2014/ajpb_mayjune2014/drivers-of-change-in-pharmacy-benefit-management. Published online June 20, 2014. Accessed May 15, 2016.
Conclusion
• MCOs can contribute to cost-effective, improved care in patients with psoriasis
– Understand the current treatment options better
– Evaluate the value of newer agents
– Design benefit language to address the needs of those patients with all stages of this disease

Questions?





























