Embed Size (px)
Citation preview

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 1/14
Essentials of the Diagnosis of Heart Failure
Although heart failure is a common clinical syndrome, especially in the elderly, its diagnosis is oftenmissed. A detailed clinical history is crucial and should address not only current signs and symptoms of heart failure but also signs and symptoms that point to a specific cause of the syndrome, such as
coronary artery disease, hypertension or valvular heart disease. It is important to determine whether thepatient has had a previous cardiac event, in particular a myocardial infarction. The physical examinationshould include Valsalva's maneuver, a test that is highly specific and sensitive for the detection of leftventricular systolic and diastolic dysfunction in patients with heart failure. An electrocardiograph and achest radiograph should also be obtained. Two-dimensional echocardiography of the heart helpsdifferentiate systolic from diastolic dysfunction. Coronary angiography is indicated in patients with heartfailure and anginal chest pain and should be strongly considered in patients with an electrocardiogramsuggestive of ischemia or myocardial infarction. (Am Fam Physician 2000;61:1319-28.)
Heart failure affects an estimated 4.9 million Americans,1 or 1 percent of adults
50 to 60 years of age and 10 percent of adults in their 80s.2 Each year, about
400,000 new cases of heart failure are diagnosed in the United States.1
Thisclinical syndrome is the most frequent cause of hospitalizations in the elderly and
is responsible for 5 to 10 percent of all hospital admissions.1 Heart failure causes or contributesto approximately 250,000 deaths every year.3
The clinical syndrome of heart failure manifests when cellular respiration becomes impaired
because the heart cannot pump enough blood to support the metabolic demands of the body, or
when normal cellular respiration can only be maintained with an elevated left ventricular filling pressure.4
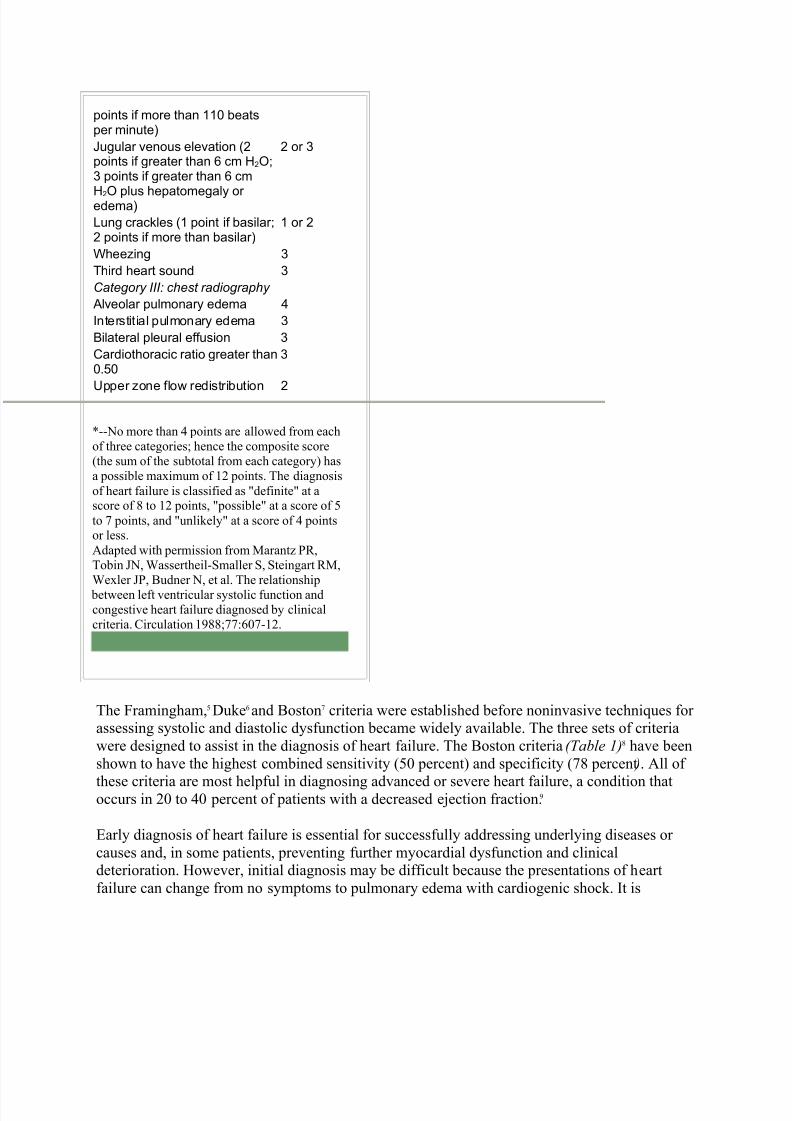
TABLE 1Boston Criteria for DiagnosingHeart Failure
Criterion Pointvalue*
Category I: history
Rest dyspnea 4
Orthopnea 4Paroxysmal nocturnal dyspnea 3
Dyspnea while walking on levelarea
2
Dyspnea while climbing 1
Category II: physical examination
Heart rate abnormality (1 point if 91 to 110 beats per minute; 2
1 or 2
8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 2/14
points if more than 110 beatsper minute)
Jugular venous elevation (2points if greater than 6 cm H2O;3 points if greater than 6 cm
H2O plus hepatomegaly or edema)
2 or 3
Lung crackles (1 point if basilar;2 points if more than basilar)
1 or 2
Wheezing 3
Third heart sound 3
Category III: chest radiography
Alveolar pulmonary edema 4
Interstitial pulmonary edema 3
Bilateral pleural effusion 3
Cardiothoracic ratio greater than0.50
3
Upper zone flow redistribution 2
*--No more than 4 points are allowed from each
of three categories; hence the composite score
(the sum of the subtotal from each category) has
a possible maximum of 12 points. The diagnosis
of heart failure is classified as "definite" at ascore of 8 to 12 points, "possible" at a score of 5
to 7 points, and "unlikely" at a score of 4 pointsor less.
Adapted with permission from Marantz PR,
Tobin JN, Wassertheil-Smaller S, Steingart RM,
Wexler JP, Budner N, et al. The relationship
between left ventricular systolic function and
congestive heart failure diagnosed by clinical
criteria. Circulation 1988;77:607-12.
The Framingham,5 Duke6 and Boston7 criteria were established before noninvasive techniques for assessing systolic and diastolic dysfunction became widely available. The three sets of criteria
were designed to assist in the diagnosis of heart failure. The Boston criteria (Table 1)8 have been
shown to have the highest combined sensitivity (50 percent) and specificity (78 percent ). All of
these criteria are most helpful in diagnosing advanced or severe heart failure, a condition thatoccurs in 20 to 40 percent of patients with a decreased ejection fraction.9
Early diagnosis of heart failure is essential for successfully addressing underlying diseases or
causes and, in some patients, preventing further myocardial dysfunction and clinicaldeterioration. However, initial diagnosis may be difficult because the presentations of heart
failure can change from no symptoms to pulmonary edema with cardiogenic shock. It is

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 3/14
estimated that heart failure is correctly diagnosed initially in only 50 percent of affected
patients.10,11 A systematic approach can improve overall accuracy in diagnosing this condition.
History
The first step in diagnosing heart failure is to obtain a complete clinical history. The patientshould be questioned about dyspnea, cough, nocturia, generalized fatigue and other signs andsymptoms of heart failure.
Dyspnea, a cardinal symptom of a failing heart, often progresses from dyspnea on exertion to
orthopnea, paroxysmal nocturnal dyspnea and dyspnea on rest. Cough, usually nocturnal and
nonproductive, may accompany dyspnea and often occurs in similar settings (i.e., on exertion or when the patient is supine).
Nocturia, also a frequent sign of heart failure, occurs secondary to increased renal perfusion
when the patient is supine.12 Generalized fatigue (caused by the low perfusion state) and
peripheral edema with inability to wear usual footwear are frequent complaints.
As heart failure progresses, gastrointestinal symptoms (e.g., abdominal bloating, anorexia and
fullness in the right upper quadrant) are occasionally seen. With severe, longstanding heart
failure, cardiac cachexia (emaciation resulting from heart disease) may develop secondary to protein-losing enteropathy and increased levels of certain cytokines, such as tumor necrosis
factor. Cardiac cachexia may mimic the cachexia seen in patients with disseminated malignant
disease.
Confusion and altered mental status may occur because of decreased cerebral perfusion or cardiac cirrhosis. In heart failure, cirrhosis develops secondary to chronic passive congestion of
the liver.
The patient should be asked about previous chest pain or myocardial infarction because coronary
artery disease is responsible for up to 75 percent of cases of heart failure with decreased leftventricular function.13 A history of myocardial infarction has a better combination of sensitivity,
specificity and positive and negative predictive value for heart failure compared with other
symptoms or aspects of the medical history.14
In patients with severe,longstanding heart failure, cardiac
cachexia may mimic the cachexiathat occurs in patients withdisseminated malignant disease.

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 4/14
It is important to identify a history of hypertension, in that high blood pressure is the second
most frequent cause of heart failure. Information about other possible causes of heart failure
should also be sought (Table 2).
Once heart failure is suspected, the functional class of the patient should be determined. The
New York Heart Association (NYHA) functional classification of congestive heart failure is presented in Table 3.15
TABLE 2Causes of Heart Failure
Most common causesCoronary artery diseaseHypertensionValvular heart disease (especially aortic and mitral disease)
Other causesInfections: viruses (including human immunodeficiency virus), bacteria, parasitesPericardial diseasesDrugs (e.g., doxorubicin [Adriamycin], cyclophosphamide [Cytoxan], cocaine)AlcoholConnective tissue diseaseInfiltrative disease (e.g., amyloidosis, sarcoidosis, hemochromatosis, malignancy)TachycardiaObstructive cardiomyopathyNeuromuscular disease (e.g., muscular or myotonic dystrophy, Friedreich's ataxia)Metabolic disorders (e.g., glycogen storage disease type 2 [Pompe's disease] and type 5 [McArdle'sdisease])Nutritional disorders (e.g., beriberi, kwashiorkor)Pheochromocytoma
RadiationEndomyocardial fibrosisEosinophilic endomyocardial diseaseHigh-output heart failure (e.g., intracardiac shunt, atrioventricular fistula, beriberi, pregnancy, Paget'sdisease, hyperthyroidism, anemia)Peripartum cardiomyopathyDilated idiopathic cardiomyopathy
Physical Examination
A complete physical examination is the second
component in the diagnosis of heart failure. The patient'sgeneral appearance should be assessed for evidence of
resting dyspnea, cyanosis and cachexia.
Blood Pressure and Heart Rate
The patient's blood pressure and heart rate should be recorded. High, normal or low blood pressure may be present. The prognosis is worse for patients who present with a systolic blood
pressure of less than 90 to 100 mm Hg when not receiving medication (angiotensin-converting
Coronary artery disease and
hypertension are the leadingcauses of heart failure.
8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 5/14
enzyme [ACE] inhibitors, beta blockers or duretics).16 Tachycardia may be a sign of heart failure,
especially in the decompensated state. The heart rate increases as one of the compensatory ways
of maintaining adequate cardiac output. A decrease in the resting heart rate with medical therapycan be used as a surrogate marker for treatment efficacy. A weak, thready pulse and pulsus
alternans are associated with decreased left ventricular function. The patient should also be
monitored for evidence of periodic breathing (Cheyne-Stokes respiration).
TABLE 3New York Heart Association Functional Classification of Congestive HeartFailure
The rightsholder did not grant rights to reproduce this item in electronic media. For the missing item, see the original print version of this publication.
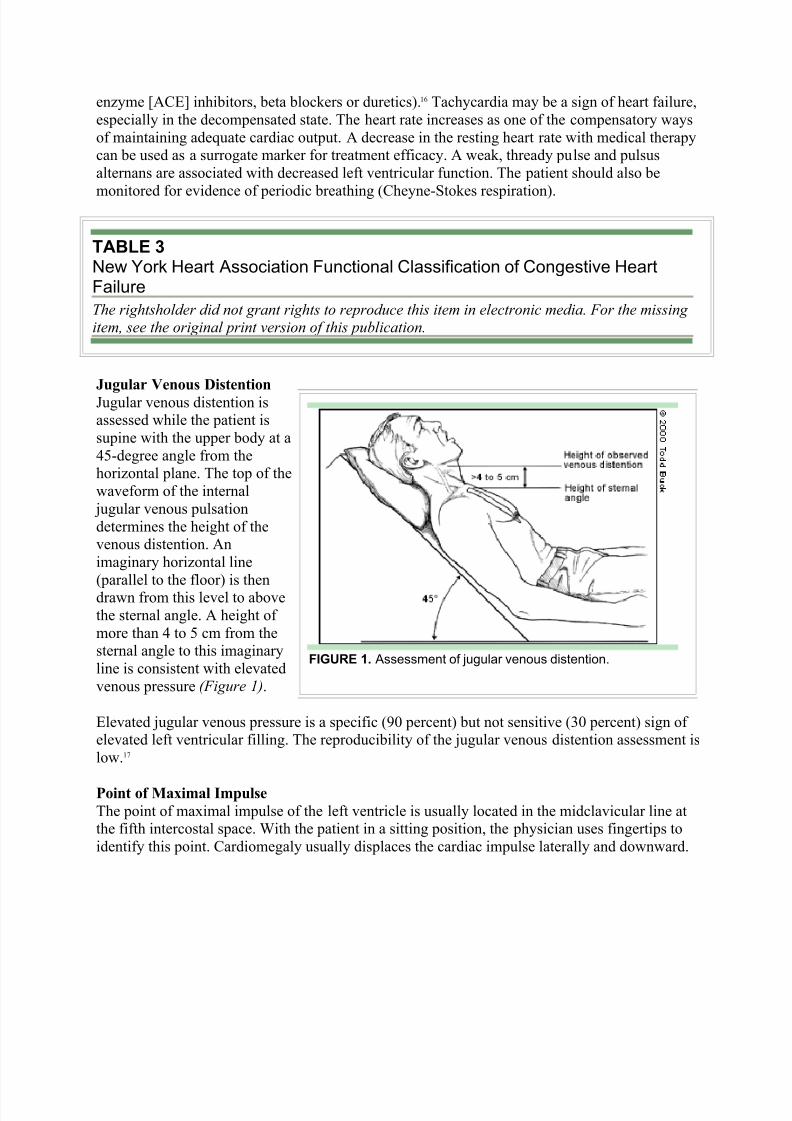
Jugular Venous Distention
Jugular venous distention isassessed while the patient is
supine with the upper body at a
45-degree angle from thehorizontal plane. The top of the
waveform of the internal
jugular venous pulsation
determines the height of thevenous distention. An
imaginary horizontal line
(parallel to the floor) is thendrawn from this level to above
the sternal angle. A height of
more than 4 to 5 cm from thesternal angle to this imaginary
line is consistent with elevated
venous pressure (Figure 1).
Elevated jugular venous pressure is a specific (90 percent) but not sensitive (30 percent) sign of elevated left ventricular filling. The reproducibility of the jugular venous distention assessment is
low.17
Point of Maximal Impulse
The point of maximal impulse of the left ventricle is usually located in the midclavicular line atthe fifth intercostal space. With the patient in a sitting position, the physician uses fingertips to
identify this point. Cardiomegaly usually displaces the cardiac impulse laterally and downward.
FIGURE 1. Assessment of jugular venous distention.

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 6/14
At times, the point of maximal impulse may be difficult to locate and therefore loses sensitivity
(66 percent). Yet the location of this point remains a specific indicator (96 percent) for
evaluating the size of the heart.14
Third and Fourth Heart Sounds
A double apical impulse can represent an auscultated third heart sound (S3). Just as with thedisplaced point of maximal impulse, a third heart sound is not sensitive (24 percent) for heart
failure, but it is highly specific (99 percent).14 Patients with heart failure and left ventricular hypertrophy can also have a fourth heart sound (S4). The physician should be alert for murmurs,
which can provide information about the cause of heart disease and also aid in the selection of
therapy.
Pulmonary Examination
Physical examination of the lungs may reveal rales and pleural effusions. Despite the presence of
pulmonary congestion, rales can be absent because of increased lymphatic drainage and
compensatory changes in the perivascular structures that have occurred over time. Wheezing
may be the sole manifestation of pulmonary congestion. Frequently, asthma is erroneouslydiagnosed in patients who actually have heart failure.
Liver Size and Hepatojugular Reflux
The key component of the abdominal examination is the evaluation of liver size. Hepatomegalymay occur because of right-sided heart failure and venous congestion.
The hepatojugular reflux can be a useful test in patients with right-sided heart failure. This test
should be performed while the patient is lying down with the upper body at a 45-degree angle
from the horizontal plane. The patient keeps the mouth open and breathes normally to preventValsalva's maneuver, which can give a false-positive test. Moderate pressure is then applied over
the middle of the abdomen for 30 to 60 seconds. Hepatojugular reflux occurs if the height of theneck veins increases by at least 3 cm and the increase is maintained throughout the compression period.18
Lower Extremity Edema
Lower extremity edema, a common sign of heart failure, is usually detected when the
extracellular volume exceeds 5 L. The edema may be accompanied by stasis dermatitis, an oftenchronic, usually eczematous condition characterized by edema, hyperpigmentation and,
commonly, ulceration.
Valsalva's Maneuver
Valsalva's maneuver is rarely used in the evaluation of patients with heart failure. Yet this test issimple to perform and carries one of the best combinations of specificity (91 percent) and
sensitivity (69 percent) for the detection of left ventricular systolic and diastolic dysfunction in
patients with heart failure.19,20
Valsalva's maneuver is performed with the blood pressure cuff inflated 15 mm Hg over the
systolic blood pressure. While the physician auscultates over the brachial artery, the patient is
asked to perform a forced expiratory effort against a closed airway (the Valsalva's maneuver).

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 7/14
8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 8/14
atypical presentations in this age group. Anorexia, generalized weakness and fatigue are often
the predominant symptoms of heart failure in geriatric patients. Mental disturbances and anxiety
are also common.
When older persons become symptomatic on exertion, they decrease their level of activity to the
point of becoming relatively asymptomatic. A cycle of symptoms on exertion and consequentdecrease in activity frequently continues as the disease progresses, until the patient finally
becomes symptomatic at rest (i.e., NYHA class IV).
The physical findings in older patients with heart failure may be difficult to interpret accurately.
Resting tachycardia is uncommon, and pulse contour abnormalities are difficult to assess
secondary to peripheral arteriosclerotic changes. At times, auscultatory findings on the lung
examination are atypical because of concomitant pulmonary disease.21
Laboratory Findings
Most patients with heart failure have normal electrolyte levels. However, extended use of kaliuretic diuretics can lead to hypokalemia, and the use of potassium-sparing diuretics and ACE
inhibitors may result in hyperkalemia. Blood urea nitrogen and creatinine levels may become
elevated, reflecting prerenal azotemia. Hyponatremia may be present in patients with advancedheart failure.
When the liver becomes congested, serum transaminase and bilirubin levels may become
elevated, and jaundice may be present. With chronic congestive hepatomegaly, cardiac cirrhosis
may occur and cause hypoalbuminemia, hypoglycemia and an increased prothrombin time.
The prognosis is worse in patients with hyponatremia or abnormalities secondary to congested
hepatomegaly.
Anemia may contribute to worsening heart failure. When severe, anemia may even cause heart
failure.
In all patients with newly diagnosed heart failure, thyroid function tests should be performed torule out hypothyroidism or hyperthyroidism.
It may soon be possible to routinely obtain serum measurements of two plasma enzymes secreted
by the overloaded heart. Plasma atrial natriuretic peptide is secreted in response to increased
intra-atrial pressure, and brain natriuretic peptide (BNP) is secreted by the failing ventricle.
Levels of these enzymes, but specifically BNP, are elevated in patients with dyspnea resultingfrom heart failure. In one study, elevated BNP levels had more than a 90 percent specificity and
sensitivity for heart failure.22

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 9/14
Diagnostic Tests
Patients with heart failure andatrial fibrillation, atrial tachycardia,ventricular tachycardia or leftbundle branch block have aworse prognosis than patientswith heart failure who do not have
these electrocardiographicfindings.
Electrocardiography
An electrocardiogram (ECG) should be obtained in all patients who present with heart failure.
No specific ECG feature is indicative of heart failure, but atrial and ventricular arrhythmias are
common findings. For example, atrial fibrillation is present in 25 percent of patients withcardiomyopathy, especially elderly patients with advanced heart failure.23 The prognosis is worse
for patients with atrial fibrillation, atrial or ventricular tachycardia, or left bundle branch
block.16,24
Low voltage on the ECG in association with conduction disturbances may suggest the presenceof amyloidosis.
Chest Radiography
Chest radiographs can be helpful in the diagnosis of heart failure. Cardiomegaly is usually
manifested by the presence of an increased cardiothoracic ratio (greater than 0.50) on a posteroanterior view. However, patients with predominantly diastolic dysfunction may have
normal heart size, one of the distinguishing markers of diastolic versus systolic dysfunction.
Right ventricular enlargement is suggested by the loss of free space between the cardiac
silhouette and the sternum on a lateral view.
Signs of increased pulmonary venous pressure seen on chest radiographs may progress from
redistribution of blood flow from the bases of the lungs to the apices to linear densities reflecting
interstitial edema (Kerley's lines) to a hazy appearance concentrated mostly around the hila of themediastinum and presenting a butterfly pattern.

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 10/14
Chest radiographs are also helpful in detecting
pleural effusion secondary to heart failure.
Echocardiography
Transthoracic two-dimensional echocardiography
with Doppler flow studies is highly recommended for all patients with heart failure.25 This test helps in the
assessment of left ventricular size, mass and function.
The ejection fraction can be calculated by several
methods, including visual estimation, which has good
correlation with ejection fractions obtained by
angiography26 or radionuclide cineangiography.27
Regional wall motion and valvular integrity can also
be evaluated.
Transesophageal echocardiography offers higher quality images than transthoracic studies. However,
this technique is invasive and is best reserved for use
when the quality of the two-dimensional
echocardiogram is unacceptable.
Angiography
Radionuclide angiography is another noninvasive
method for assessing systolic and diastolic function.
This imaging technique is used when two-dimensional echocardiography is not diagnostic because adequate images could not be obtained or the findings do not agree with the clinical
picture. Radionuclide angiography provides a reliable and quantitative measurement of the leftventricular ejection fraction and the regional wall motion. However, ectopic activity and atrialfibrillation adversely affect the accuracy of its measurements.28
Left ventricular angiography can be used to assess the ejection fraction, the left ventricular
volume and the severity of valvular regurgitation or stenosis. In addition, detailed measurements
of ventricular filling pressures and indices of left ventricular diastolic relaxation rate can behelpful in confirming diastolic dysfunction.
Other Techniques
Magnetic resonance imaging (MRI)29 and ultrafast or cine computed tomography (CT)30 can
measure the ejection fraction and assess regional wall motion. However, assessment of cardiacfunction using these studies is only performed in a limited number of centers, and the superiority
of the studies to echocardiography and angiography has not been proved.
Sometimes coronary artery disease must be excluded as a causal factor in patients with heartfailure. Cardiac catheterization and coronary angiography should be strongly considered in all
patients with heart failure and angina who are candidates for interventional procedures. In
patients with known coronary artery disease and heart failure but no angina, coronary
FIGURE 3. Two-dimensionalechocardiogram showing a four-chambersview of the heart in a patient with systolicdysfunction. Note dilated LV. (LV = leftventricle; RV = right ventricle; RA = rightatrium; LA = left atrium)
FIGURE 4. Two-dimensionalechocardiogram showing a four-chambersview of the heart in a patient with diastolicdysfunction. Note the normal LV size withhypertrophy.

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 11/14
arteriography or noninvasive testing (i.e., a thallium stress test or stress echocardiogram),
followed by coronary arteriography in those patients with ischemia, should be considered. The
intensity of the search for ischemic heart disease in patients with heart disease depends on the patient's probability of having coronary artery disease.
If imaging techniques cannot confirm the cause of cardiac dysfunction, an endomyocardial biopsy may provide important information in patients receiving cardiotoxic drugs and in patients
suspected of having infectious (i.e., acute or chronic viral myocarditis), genetic or systemicdiseases with possible cardiac involvement.25 However, the diagnostic yield of this procedure is
typically less than 10 percent.31
TABLE 4Clues for Differentiating Between Systolic and Diastolic Dysfunction inPatients with Heart Failure
Clues from the evaluation Systolic dysfunction Diastolic dysfunction
History Hypertension XX XXX
Coronary artery disease* XXX X
Diabetes mellitus XXX XX
Valvular heart disease* XXX --Physical examination Third heard sound (S3) gallop* XXX X
Fourth heart sound (S4) gallop* X XXX
Rales XX XX
Jugular venous distention XX X
Edema XX X
Displaced point of maximal impulse* XX --Mitral regurgitation* XXX X
Chest radiograph Cardiomegaly* XXX X
Pulmonary congestion XXX XXX
Electrocardiogram Q wave XX X
Left ventricular hypertrophy* X XXX
Echocardiogram Decreased ejection fraction* XXX --Dilated left ventricle* XX --
Left ventricle hypertrophy* X XXX
X = suggestive; the number of Xs reflects the relative weight; -- = not suggestive.
*--Particularly helpful in distinguishing systolic from diastolic dysfunction in heart failure.
Adapted with permission from Young JB. Assessment of heart failure. In: Braunwald E. Atlas of heart disease. Vol
4. Philadelphia: Current Medicine, 1995:7.1-7.2.
Systolic vs. Diastolic Dysfunction

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 12/14
As many as 40 percent of patients with clinical heart failure have diastolic dysfunction with
normal systolic function.32 In addition, many patients with systolic dysfunction have elements of
diastolic dysfunction. With systolic dysfunction, the pumping ability of the ventricle is impaired.With diastolic dysfunction, ventricular filling is defective.
Ventricular diastolic function depends on the pressure-to-volume relationship in the leftventricle. Decreased compliance of the left ventricular wall leads to a higher pressure for a given
diastolic volume. The end result is impaired ventricular filling, inappropriately elevated left atrialand pulmonary venous pressure, and decreased ability to increase stoke volume. These
dysfunctions lead to the clinical syndrome of heart failure.
Findings suggestive of diastolic dysfunction on the two-dimensional echocardiogram are left
ventricular hypertrophy, a dilated left atrium, a normal or nearly normal ejection fraction andreversal of the normal pattern of flow velocity (measured by Doppler flow studies) across the
mitral valve (Figures 3 and 4).
Treatment of Diastolic or Systolic Dysfunction

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 13/14
*--Diuretics are best used to treat acute congestive heart failure and as adjunctive therapy for hypertension.†--Note that the likelihood of angioedema and renal insufficiency is increased with ACE inhibitors andangiotensin-receptor blockers. Watch for late-breaking results from clinical trials on the efficacy of angiotensin-receptor blockers alone and in combination with ACE inhibitors compared with ACE inhibitorsalone.‡--The addition of milrinone is preferred in patients already receiving a beta blocker.
FIGURE 5. Suggested algorithm for the treatment of diastolic or systolic dysfunction. (ACE = angiotensin-converting enzyme; NYHA = New York Heart Association; IV = intravenous.)
Differentiating between systolic and diastolic dysfunction is essential because their long-termtreatments are different33 (Table 434 and Figure 5). The treatments of choice in patients with
systolic dysfunction are ACE inhibitors, digoxin, diuretics and beta blockers. In patients with
diastolic dysfunction, the cornerstones of treatment depend on the underlying cause. Beta
blockers and calcium channel blockers are frequently used when diastolic dysfunction issecondary to ischemia or hypertension.
The history, physical examination, ECG and chest radiographs provide some clues that can behelpful in differentiating systolic and diastolic dysfunction. For example, predominantly systolicdysfunction is suggested by a history of myocardial infarction and younger patient age, a
displaced point of maximal impulse and an S3 gallop on the physical examination, the presence
of Q waves on the ECG and the finding of cardiomegaly on the chest radiograph. In contrast,
diastolic dysfunction is suggested by a history of hypertension and older patient age, a sustained point of maximal impulse and an S4 gallop on the physical examination, left ventricular

8/9/2019 Essentials of the Diagnosis of Heart Failure
http://slidepdf.com/reader/full/essentials-of-the-diagnosis-of-heart-failure 14/14
hypertrophy on the ECG and a normal-sized heart on the chest radiograph. 36 However, the
findings can overlap considerably, and echocardiography of the heart is usually necessary.





























