Embed Size (px)
Citation preview

Cochrane Database of Systematic Reviews
Interventions for replacing missing teeth: different types ofdental implants (Review)
Esposito M, Ardebili Y, Worthington HV
Esposito M, Ardebili Y, Worthington HV.
Interventions for replacing missing teeth: different types of dental implants.
Cochrane Database of Systematic Reviews 2014, Issue 7. Art. No.: CD003815.
DOI: 10.1002/14651858.CD003815.pub4.
www.cochranelibrary.com
Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .6BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Figure 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Figure 8. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Figure 9. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Figure 10. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Figure 11. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Figure 12. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Figure 13. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Figure 14. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Figure 15. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Figure 16. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Figure 17. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Figure 18. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Figure 19. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Figure 20. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Figure 21. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Figure 22. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Figure 23. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Figure 24. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Figure 25. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Figure 26. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Figure 27. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Figure 28. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Figure 29. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Figure 30. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Figure 31. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Figure 32. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Figure 33. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Figure 34. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Figure 35. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Figure 36. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Figure 37. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Figure 38. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Figure 39. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Figure 40. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Figure 41. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Figure 42. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Figure 43. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
iInterventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 44. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Figure 45. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Figure 46. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Figure 47. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Figure 48. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Figure 49. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Figure 50. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Figure 51. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Figure 52. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Figure 53. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Figure 54. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37Figure 55. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Figure 56. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Figure 57. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
50ADDITIONAL SUMMARY OF FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . .52DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .54AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .54ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .62CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
103DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Analysis 1.1. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium screws, Outcome
1 Implant failure: 1 year. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104Analysis 1.2. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium screws, Outcome
2 Implant failure: 3 years. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104Analysis 1.3. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium screws, Outcome
3 Implant failure: 5 years. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105Analysis 1.4. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium screws, Outcome
4 Implant failure: 10 years. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106Analysis 2.1. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss, Outcome
1 Implant failure: 1 year. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106Analysis 2.2. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss, Outcome
2 Implant failure: 3 years. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107Analysis 2.3. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss, Outcome
3 Implant failure: 5 years. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107Analysis 2.4. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss, Outcome
4 Implant failure: 10 years. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108Analysis 3.1. Comparison 3 Turned versus roughened implants, Outcome 1 Early implant failure. . . . . . . . 109Analysis 3.2. Comparison 3 Turned versus roughened implants, Outcome 2 Peri-implantitis. . . . . . . . . . 110
110ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .118APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .120WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .120HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .121CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .121DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .121SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .122DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .122INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiInterventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Interventions for replacing missing teeth: different types ofdental implants
Marco Esposito1, Yasmin Ardebili2, Helen V Worthington1
1Cochrane Oral Health Group, School of Dentistry, The University of Manchester, Manchester, UK. 2Private practice, Melbourne,Australia
Contact address: Marco Esposito, Cochrane Oral Health Group, School of Dentistry, The University of Manchester, Coupland 3Building, Oxford Road, Manchester, M13 9PL, UK. [email protected].
Editorial group: Cochrane Oral Health Group.Publication status and date: New search for studies and content updated (no change to conclusions), published in Issue 7, 2014.Review content assessed as up-to-date: 17 January 2014.
Citation: Esposito M, Ardebili Y, Worthington HV. Interventions for replacing missing teeth: different types of dental implants.Cochrane Database of Systematic Reviews 2014, Issue 7. Art. No.: CD003815. DOI: 10.1002/14651858.CD003815.pub4.
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Dental implants are available in different materials, shapes and with different surface characteristics. In particular, numerous implantdesigns and surface modifications have been developed for improving clinical outcome. This is an update of a Cochrane review firstpublished in 2002, and previously updated in 2003, 2005 and 2007.
Objectives
Primary: to compare the clinical effects of different root-formed osseointegrated dental implant types for replacing missing teeth forthe following specific comparisons: implants with different surface preparations, but having similar shape and material; implants withdifferent shapes, but having similar surface preparation and material; implants made of different materials, but having similar surfacepreparation and shape; different implant types differing in surface preparation, shape, material or a combination of these.
Secondary: to compare turned and roughened dental implants for occurrence of early implant failure (before prosthetic loading) andoccurrence of peri-implantitis.
Search methods
We searched the following electronic databases: the Cochrane Oral Health Group’s Trials Register (to 17 January 2014), the CochraneCentral Register of Controlled Trials (CENTRAL) (The Cochrane Library 2013, Issue 12), MEDLINE via OVID (1946 to 17 January2014) and EMBASE via OVID (1980 to 17 January 2014). We placed no restrictions on the language or date of publication whensearching the electronic databases.
Selection criteria
We included any randomised controlled trial (RCT) comparing osseointegrated dental implants of different materials, shapes andsurface properties having a follow-up in function of at least one year. Outcome measures were success of the implants, radiographicperi-implant marginal bone levels changes and incidence of peri-implantitis.
1Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data collection and analysis
At least two review authors independently conducted screening, risk of bias assessment and data extraction of eligible trials in duplicate.We expressed results using fixed-effect models (if up to three studies were present in a meta-analysis) or random-effects models (whenthere were more than three studies) using mean differences (MD) for continuous outcomes and risk ratios (RR) for dichotomousoutcomes with 95% confidence intervals (CI). We reported the following endpoints: one, three, five and 10 years after functionalloading.
Main results
We identified 81 different RCTs. We included 27 of these RCTs, reporting results from 1512 participants and 3230 implants in thereview. We compared 38 different implant types with a follow-up ranging from one to 10 years. All implants were made of commerciallypure titanium or its alloys, and had different shapes and surface preparations. We judged two trials to be at low risk of bias, 10 to beat unclear risk of bias and 15 to be at high risk of bias. On a ’per participant’ rather than ’per implant’ basis, we found no significantdifferences between various implant types for implant failures. The only observed statistically significant difference for the primaryobjective regarded more peri-implant bone loss at Nobel Speedy Groovy implants when compared with NobelActive implants (MD-0.59 mm; 95% CI -0.74 to -0.44, different implant shapes). The only observed statistically significant difference for the secondaryobjective was that implants with turned (smoother) surfaces had a 20% reduction in risk to be affected by peri-implantitis than implantswith rough surfaces three years after loading (RR 0.80; 95% CI 0.67 to 0.96). There was a tendency for implants with turned surfacesto fail early more often than implants with roughened surfaces.
Authors’ conclusions
Based on the results of the included RCTs, we found no evidence showing that any particular type of dental implant had superior long-term success. There was limited evidence showing that implants with relatively smooth (turned) surfaces were less prone to lose bonedue to chronic infection (peri-implantitis) than implants with much rougher surfaces (titanium-plasma-sprayed). These findings werebased on several RCTs, often at high risk of bias, with few participants and relatively short follow-up periods.
P L A I N L A N G U A G E S U M M A R Y
Interventions for replacing missing teeth: different types of dental implants
Review question
To compare the effects of different dental implants. These are implanted into bone and vary primarily in their shape, material and typeof surface.
Background
Missing teeth can sometimes be replaced with dental implants into the jaw, as bone can grow around the implant. A crown, bridgeor denture can then be attached to the implant. Many implant modifications have been developed trying to improve the long-termsuccess rates of implants, and different types have been heavily marketed. More than 1300 types of dental implants are available, indifferent materials, shapes, sizes, lengths and with different surface characteristics or coatings.
Study characteristics
This review of existing studies was carried out by the Cochrane Oral Health Group and the evidence is current up to 17 January 2014.We searched scientific databases for randomised controlled trials (studies where people are randomly put into one of two or moretreatment groups) comparing different types of dental implants in people who were followed up for at least one year.
We found 27 trials based in a wide range of countries - six in Italy; five in New Zealand, five in Sweden, three in the Netherlands,two in Korea, one in Turkey, one in Germany, one in Switzerland and three multicentre European trials. Most took place at universitydental clinics or hospitals, four were run in private practice and, in the multicentre European trials, a few were also in private practice.
There were comparisons made of 38 implant types with different surface characteristics, shapes, degree of titanium (metal) purity andtitanium alloys (mixtures of metal). The main outcome of the trials was failure of the implant to work.
Key results
2Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The review found there was not enough evidence from trials to demonstrate superiority of any particular type of implant characteristicor implant system over another.
There was no evidence showing that any particular type of dental implant had greater long-term success. There was limited evidenceshowing that implants with relatively smooth surfaces were less prone to lose bone due to chronic infection (peri-implantitis) thanimplants with much rougher surfaces. However, the evidence suggests they may fail earlier than implants with roughened surfaces.
Quality of the evidence
Two trials were at low risk of bias, 10 were at unclear risk of bias and 15 were at high risk of bias.
Most of the trials were underpowered, which means that there were not enough participants in the studies to be able to draw firmconclusions. Caution should be exercised when generalising the results of the included trials to ordinary clinical conditions.
3Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

SU
MM
AR
YO
FF
IN
DI
NG
SF
OR
TH
EM
AI
NC
OM
PA
RI
SO
N[E
xpla
nat
ion
]
Implanttype
Acomparedwith
implanttype
Bforimplantfailureandbone
loss
Patientorpopulation:adultswithmissingteeth
Settings:dentalclinics
Intervention:implantA
Com
parison:implantB
Outcomes
Illustrativecomparativerisks*(95%
CI)
Relativeeffect
(95%
CI)
Noofparticipants
(studies)
Qualityoftheevidence
(GRADE)
Com
ments
Assum
edrisk
Corresponding
risk
ImplantA
ImplantB
Implantfailure
--
Seecomments
--
There
were
numerous
comparisonsbetweendif-
ferent
implants
that
var-
iedby
surfacepreparation,
shape,materialandtype,
only1ofthesevaryingfor
each
comparison.Mostof
thecomparisonsweresin-
glestudies.Therewereno
statisticallysignificantdif-
ferencesforimplantfailure
Bonelevelchange
--
Seecomments
--
There
were
numerous
comparisonsbetweendif-
ferent
implants
that
var-
iedby
surfacepreparation,
shape,materialandtype,
only
1of
thesevarying
foreachcomparison.M
ost
ofthecomparisonswere
single
study.
Therewas
4Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

only1statisticallysignif-
icantdifferenceforbone
levelchange
from
1sin-
glestudy,which
indicated
morebone
loss
forNobel
Activethan
NobelSpeedy
Groovy(MD0.59mm;95%
CI0.44to0.74)
*The
basisfortheassumed
risk(e.g.themediancontrolgroupriskacross
studies)isprovided
infootnotes.Thecorrespondingrisk(and
its95%confidence
interval)isbasedon
the
assumedriskinthecomparison
groupandtherelativeeffectoftheintervention(andits95%CI).
CI:confidenceinterval;M
D:meandifference.
GRADEWorkingGroupgradesofevidence
Highquality:Furtherresearchisveryunlikelytochangeourconfidenceintheestimateofeffect.
Moderatequality:Furtherresearchislikelytohaveanimportantimpactonourconfidenceintheestimateofeffectandmaychangetheestimate.
Lowquality:Furtherresearchisverylikelytohaveanimportantimpactonourconfidenceintheestimateofeffectandislikelytochangetheestimate.
Verylowquality:Weareveryuncertainabouttheestimate.
5Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

B A C K G R O U N D
Description of the condition
Missing teeth may result in a functional and aesthetic deficit andhave traditionally been replaced with dentures or bridges. Dentalimplants offer an alternative; they are inserted into the jawbonesand used to support dental prostheses. Dental implants rely onthe maintenance of a direct structural and functional connectionbetween living bone and the implant surface; this is termed os-seointegration and was first described by Brånemark (Brånemark1977). Osseointegration has undoubtedly been one of the mostsignificant scientific breakthroughs in dentistry over since the early1960s.
Description of the intervention
Osseointegrated dental implants are available in different materi-als, body shapes, diameters, lengths, platforms, surface propertiesand coatings. In particular, the area of implant surface modifi-cations and coatings has been subjected to aggressive marketingaimed at establishing the superiority of a given surface over theothers. In implant dentistry, the word ’machined’ has frequentlybeen used as a description of a turned, milled or polished sur-face. However, a machined surface can be anything produced bya machine and surfaces produced with electro discharge, polish,ground, honed and sand blasting are all examples of machinedsurfaces (Stout 1990). Numerous surface modifications includingturned, blasted, acid-etched, porous-sintered, oxidised, plasma-sprayed, laser modified, hydroxyapatite-coated surfaces, highly hy-drophilic or a combination of these procedures have been devel-oped and are currently used with the aim of enhancing clinicalperformance. In addition, different materials are used to manu-facture dental implants including: titanium with various degree ofpurity, titanium alloys (e.g. Ti6Al4V) and ceramics (e.g. zirconia).It has been estimated that dentists have to choose from more than1300 types of implants that vary in form, material, dimension,surface properties and interface geometry (Binon 2000).Originally, Brånemark implants had machined (turned) surfaces.Turned surfaces are those originally formed by the milling (ma-chining) procedure of the titanium bar and are considered to besmooth surfaces. It was believed that rougher surfaces could im-prove the osseointegration process by allowing more bone to bein contact with the implant surface determining also an increasedmechanical retention. Following this concept, many procedureswere developed to roughen implant surfaces; however, one po-tential drawback was empirically observed: a suspected increasedincidence of peri-implantitis when compared with implants withturned surfaces (Esposito 1997). Peri-implantitis can be defined as“a site specific, plaque-induced infection with progressive loss ofthe bone supporting a functioning implant” (Esposito 1999). This
chronic infection affects at least 16% of people rehabilitated withimplants having turned surfaces after nine to 14 years in functionin one retrospective evaluation (Roos-Jansåker 2006). Turned im-plant surfaces are those considered to be less susceptible to peri-im-plantitis, and there is the potential risk that implants with rough-ened surfaces could be at higher risk for peri-implantitis.
Why it is important to do this review
In addition, because of the aggressive marketing, it is unclearwhether there are implant surface modifications, implant shapesor particular materials that can actually improve clinical results. Ifthis is the case, then clinicians and patients could choose whichdental implant system to use, if not, it would still be useful toknow that many modifications do not substantially alter the clini-cal outcomes. It would be also very useful to understand to whichdegree the roughening of implant surfaces could be advantageousin the long term.
O B J E C T I V E S
Primary objectives
To compare the clinical effects of different root-formed osseoin-tegrated dental implant types for replacing missing teeth for thefollowing specific comparisons:
1. implants with different surface preparations, but havingsimilar shape and material;
2. implants with different shapes, but having similar surfacepreparation and material;
3. implants made of different materials, but having similarsurface preparation and shape;
4. different implant types differing in surface preparation orshape or material, or a combination of these.
Secondary objectives
To compare turned and roughened dental implants for occurrenceof early implant failure (before prosthetic loading) and occurrenceof peri-implantitis.
M E T H O D S
Criteria for considering studies for this review
6Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Types of studies
Any randomised controlled trial (RCT) of parallel group and split-mouth design comparing identical dental implants positioned inthe same way differing only for:
• surfaces;• shapes;• material.
Any RCT comparing different dental implant systems.We excluded quasi-randomised trials.
Types of participants
People who received osseointegrated root-formed dental implantsfollowed up for at least one year after functional loading.
Types of interventions
Different dental implants (shape, material and surface character-istics) for replacing missing teeth.
Types of outcome measures
Primary outcome
• Biological or mechanical implant failure defined as:
◦ biological failure: implant mobility and removal ofstable implants dictated by progressive marginal bone loss orinfection. Biological failures were divided in early (failure toestablish osseointegration) and late failures (failure to maintainthe established osseointegration). Failures that occurred beforeprosthesis delivery or, in the case of immediate or early-loadedimplants a few months after prosthesis insertion, were consideredearly failures. Implant mobility could be assessed manually orwith instruments such as Periotest or resonance frequency(Osstell), with the prosthesis removed with the exception ofsingle implants;
◦ mechanical failure: implant fracture and any othermechanical complication not allowing use of the implant.
Secondary outcomes
• Radiographic peri-implant marginal bone level changes onperiapical radiographs taken with a paralleling technique. Thebaseline radiographs had to have been taken at implantplacement.
• Occurrence of peri-implantitis defined as implants affectedby progressive peri-implant marginal bone loss with signs ofinfection (only for the secondary objective).
Search methods for identification of studies
For the identification of studies included or considered for thisreview, we developed detailed search strategies for each databasesearched. These were based on the search strategy developed forMEDLINE (OVID) but revised appropriately for each database.The search strategy used a combination of controlled vocabularyand free-text terms and was linked with the Cochrane Highly Sen-sitive Search Strategy (CHSSS) for identifying RCTs in MED-LINE: sensitivity maximising version (2008 revision) as referencedin Chapter 6.4.11.1 and detailed in box 6.4.c of the CochraneHandbook for Systematic Reviews of Interventions Version 5.1.0(Higgins 2011). Details of the MEDLINE search are provided inAppendix 1. We linked the EMBASE search to the Cochrane OralHealth Group’s filter for identifying clinical trials (Appendix 2).
Electronic searches
We searched the following electronic databases:• the Cochrane Oral Health Group’s Trials Register (to 17
January 2014) (Appendix 3);• the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2013, Issue 12) (Appendix4);
• MEDLINE via OVID (1946 to 17 January 2014)(Appendix 1);
• EMBASE via OVID (1980 to 17 January 2014) (Appendix2).
Language
We did not place any restrictions on language or date of publicationwhen searching the electronic databases.
Unpublished studies
We wrote to all the authors of the identified RCTs, we checkedthe bibliographies of all identified RCTs and relevant review ar-ticles, and we used personal contacts in an attempt to identifyunpublished or ongoing RCTs. In the first version of this review,we also wrote to more than 55 oral implant manufacturers andwe requested information on trials through an Internet discussiongroup ([email protected]); however, we discontin-ued this due to poor yield.
Handsearching
Details of the journals being handsearched by the Cochrane OralHealth Group’s ongoing programme are given on the website:www.ohg.cochrane.org.We identified the following journals as being potentially impor-tant to be handsearched for this review: British Journal of Oraland Maxillofacial Surgery, Clinical Implant Dentistry and RelatedResearch, Clinical Oral Implants Research, European Journal of Oral
7Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Implantology, Implant Dentistry, International Journal of Oral andMaxillofacial Implants, International Journal of Oral and Maxillo-facial Surgery, International Journal of Periodontics and RestorativeDentistry, International Journal of Prosthodontics, Journal of Clini-cal Periodontology, Journal of Dental Research, Journal of Oral Im-plantology, Journal of Oral and Maxillofacial Surgery, Journal of Pe-riodontology and Journal of Prosthetic Dentistry. Where these havenot already been searched as part of the Cochrane Journal Hand-searching Programme, one review author handsearched the jour-nals up to the month in which the last electronic search was un-dertaken.
Data collection and analysis
Study selection
At least two review authors independently scanned the titles andabstracts (when available) of all reports identified through the elec-tronic searches. For studies appearing to meet the inclusion cri-teria, or for which there were insufficient data in the title andabstract to make a clear decision, we obtained the full report. Atleast two review authors independently assessed the full reportsto establish whether they met the inclusion criteria or not. Weresolved disagreements by discussion. Where resolution was notpossible, we consulted a third review author. We assessed risk ofbias and extracted data of all studies meeting the inclusion crite-ria. We recorded studies rejected at this or subsequent stages inthe Characteristics of excluded studies table, and gave reasons forexclusion.
Data extraction and management
At least two review authors independently extracted data usingspecially designed data extraction forms. We had piloted the dataextraction forms on several papers and modified them as required
before use. We resolved any disagreements by discussion and con-sulted a third review author where necessary. We contacted authorsfor clarification or missing information.For each trial, we recorded the following data:
• year of publication, country of origin and source of studyfunding;
• details of the participants including demographiccharacteristics, source of recruitment and criteria for inclusion;
• details of the type of intervention;• details of the outcomes reported, including method of
assessment, and time intervals.
Assessment of risk of bias in included studies
Two review authors independently undertook the risk of bias as-sessment of the included trials in duplicate as part of the dataextraction process. In the case that the paper to be assessed hadone or more review authors in the authors list, only those reviewauthors not involved in the trial evaluated it.We used the recommended approach for assessing risk of bias instudies included in Cochrane reviews (Higgins 2011). It is a two-part tool, addressing the six specific domains (namely, sequencegeneration, allocation concealment, blinding of the outcome as-sessor, incomplete outcome data, selective outcome reporting andother bias). Each domain includes one specific entry in a ’Risk ofbias’ table. Within each entry, the first part of the tool involvesdescribing what was reported to have happened in the study. Thesecond part of the tool involves assigning a judgement relating tothe risk of bias for that entry. This is achieved by answering pre-specified questions about the adequacy of the study in relation tothe entry.
Summarising risk of bias for a study
After taking into account the additional information provided bythe authors of the trials, we grouped studies into the followingcategories. We assumed that the risk of bias was the same for alloutcomes and each study was assessed as follows.
Risk of bias Interpretation Within a study Across studies
Low risk of bias Plausible bias unlikely to seriouslyalter the results
Low risk of bias for all key domains Most information was from studiesat low risk of bias
Unclear risk of bias Plausible bias that raises somedoubt about the results
Unclear risk of bias for 1 or morekey domains
Most information was from studiesat low or unclear risk of bias
High risk of bias Plausible bias that seriously weak-ens confidence in the results
High risk of bias for 1 or more keydomains
The proportion of informationfrom studies at high risk of bias wassufficient to affect the interpreta-tion of results
8Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Measure of treatment effect
For dichotomous outcomes, we expressed the estimate of effect ofan intervention as risk ratios (RR) together with 95% confidenceintervals (CIs). For continuous outcomes, we used mean differ-ences (MD) and standard deviations to summarise the data foreach group and express it as MD and 95% CIs.
Unit of analysis issues
The statistical unit was the participant and not the implant unlessthe clustering of the implants within the participants had beentaken into account in the analysis.
Dealing with missing data
We contacted trial authors to retrieve missing data where nec-essary. If we could not reach agreement, we excluded data untilfurther clarification was available. We would have used methodsfor estimating missing standard deviations in Section 7.7.3 of theCochrane Handbook for Systematic Reviews of Interventions if re-quired (Higgins 2011).
Assessment of heterogeneity
We would have assessed the significance of any discrepancies inthe estimates of the treatment effects from the different trials bymeans of Cochran’s test for heterogeneity and heterogeneity wouldhave been considered significant if P value < 0.1. We would haveused the I2 statistic, which describes the percentage total variationacross studies that is due to heterogeneity rather than chance, toquantify heterogeneity with an I2 statistic over 50% being consid-ered substantial heterogeneity.
Assessment of reporting biases
If there had been sufficient numbers of trials (more than 10) inany meta-analysis, we would have assessed publication bias accord-ing to the recommendations on testing for funnel plot asymmetry(Egger 1997), as described in the Cochrane Handbook for System-atic Reviews of Interventions (Higgins 2011). If we had identifiedasymmetry, we would have examined possible causes.
Data synthesis
We only performed a meta-analysis if there were studies of similarcomparisons reporting the same outcome measures. We combinedRRs for dichotomous data, and MDs for continuous data, usingfixed-effect models. We used random-effects models when therewere more than three studies in a meta-analysis. We combineddata from split-mouth studies with data from parallel group trialsusing the method outlined by Elbourne (Elbourne 2002), using
the generic inverse variance method in Review Manager (RevMan2012). We used the techniques described by Follmann to estimatethe standard error of the difference for split-mouth studies, wherethe appropriate data were not presented and could not be obtained(Follmann 1992). We would have calculated numbers needed totreat for an additional beneficial outcome (NNTB) for peopleaffected by implant failures. We followed the recommendations ofthe Cochrane Handbook for Systematic Reviews of Interventions forRCTs with parallel design with zero-cell counts (Higgins 2011).We added the fixed value of 0.5 to all cells with zero-cell counts andcalculated RRs using Review Manager software (RevMan 2012). Ifthere were no events in both arms, we undertook no calculations,because in this situation the study does not provide any indicationof the direction or magnitude of the relative treatment effect. Wepresented data that could not be meta-analysed in an additionaltable.
Subgroup analysis and investigation of heterogeneity
We would have assessed clinical heterogeneity by examining thetypes of participants and interventions for all outcomes in eachstudy. We planned the following subgroup analyses only for trialsincluded to answer the primary hypothesis; however, we foundinsufficient studies in the meta-analysis to undertake this.
1. Whether implants were placed in mandibles or maxillae.2. Whether implants were placed in partially or fully
edentulous jaws.3. Different number of placed implants (for instance
overdentures supported by two versus overdentures supported byfour implants).
4. Whether the implants were immediately placed in toothextraction sockets or not.
5. Whether the implants were placed in anterior or posteriorareas of the jaw.
6. Whether the implants were placed in augmented (grafted orregenerated) bone or not.
7. Whether the implants were placed with a submerged ornon-submerged technique.
8. Whether the implants were loaded at different times:immediate loading (up to one week) and conventional loading(three months or more for mandibles and six months or more formaxillae).
9. Different prosthetic designs (for instance overdenturesversus screw-retained dentures or implant-supported bridgesversus bridges supported by both implants and teeth).10. Whether the trial was supported by implantmanufacturer(s) or not.
Sensitivity analyses
We planned to undertake sensitivity analyses to examine the effectof the risk of bias on the overall estimates of effect. In addition, weplanned to examine the effect of including unpublished literature
9Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

on the review’s findings. However, we found too few trials in themeta-analyses to undertake these analyses to investigate to whatextent the risk of bias might have influenced the results. We willdo this in future updates as soon as a sufficient number of trialshaving different risk of bias are available.
Presentation of main results
We produced ’Summary of findings’ tables for the main outcomesof this review using GRADEpro software. We assessed the qualityof the body of evidence by considering the overall risk of bias of theincluded studies, the directness of the evidence, the inconsistencyof the results, the precision of the estimates, the risk of publicationbias and the magnitude of the effect. We categorised the qualityof the body of evidence for each of the primary outcomes as high,moderate, low or very low.
R E S U L T S
Description of studies
Results of the search
The search for this review was part of a wider search for all eligibletrials for the series of Cochrane reviews on dental implants. Thissearch is conducted every six months and has so far included about8600 records.
Included studies
See Characteristics of included studies table.We identified 27 trials to be included in the review (Batenburg1998; Astrand 1999; Moberg 2001; Tawse-Smith 2001; Astrand2002; Gatti 2002; Heydenrijk 2002; Tawse-Smith 2002; Payne2003; Payne 2004; Wennström 2004; Fröberg 2006; Lang 2007;Lee 2007; Schincaglia 2007; Crespi 2009; Kielbassa 2009; Prosper2009; Song 2009; Akoglu 2011; Alsabeeha 2011; den Hartog
2011; Heberer 2011; Al-Nawas 2012; Esposito 2012; Esposito2013a; Pozzi 2014).
Characteristics of trial setting and investigators
• Of the 27 included trials, six were conducted in Italy (Gatti2002; Schincaglia 2007; Crespi 2009; Prosper 2009; Esposito2012; Pozzi 2014), five in New Zealand (Tawse-Smith 2001;Tawse-Smith 2002; Payne 2003; Payne 2004; Alsabeeha 2011),five in Sweden (Astrand 1999; Moberg 2001; Astrand 2002;Wennström 2004; Fröberg 2006), three in the Netherlands(Batenburg 1998; Heydenrijk 2002; den Hartog 2011), two inKorea (Lee 2007; Song 2009), one in Turkey (Akoglu 2011), onein Germany (Heberer 2011), and one in Switzerland (Esposito2013a). Three were multicentre European trials (Lang 2007;Kielbassa 2009; Al-Nawas 2012),
• Sixteen trials had a parallel group study design and 11 had asplit-mouth design (Astrand 2002; Wennström 2004; Fröberg2006; Lee 2007; Schincaglia 2007; Prosper 2009; Song 2009;Heberer 2011; Al-Nawas 2012; Esposito 2013a; Pozzi 2014).
• Sixteen trials received support from industry (Batenburg1998; Astrand 1999; Tawse-Smith 2001; Astrand 2002;Tawse-Smith 2002; Payne 2003; Payne 2004; Wennström 2004;Lang 2007; Schincaglia 2007; Kielbassa 2009; den Hartog 2011;Heberer 2011; Al-Nawas 2012; Esposito 2012; Esposito 2013a).
• All trials were conducted at university dental clinics orhospitals with eight exceptions: four trials were conducted inprivate practices (Gatti 2002; Fröberg 2006; Esposito 2012;Esposito 2013a) and four multicentre trials in which a fewcentres were private practices (Lang 2007; Prosper 2009;Al-Nawas 2012; Pozzi 2014). All studies included adults only.
Characteristics of interventions
Thirty-eight implant types with different surface characteristics,shapes, degree of titanium purity and titanium alloys were com-pared.
1. Ankylos Plus® grit-blasted and high temperature etchedsurface, titanium grade 2 cylindrical screws with internal conicalconnection (Dentsply-Friadent, Mannheim, Germany) (Crespi2009) (Figure 1; Figure 2).
10Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Ankylos Plus® grit-blasted and high-temperature etched surface, titanium grade 2 cylindricalscrews with internal conical connection (Dentsply-Friadent, Mannheim, Germany).
Figure 2. Radiographic image: Ankylos Plus® grit-blasted and high-temperature etched surface, titanium
grade 2 cylindrical screws with internal conical connection (Dentsply-Friadent, Mannheim, Germany).
1. Astra® turned titanium grade 3 cylindrical screws withinternal connection (Astra Tech AB, Mölndal, Sweden)(Wennström 2004) as in Figure 3 but with turned surface(Figure 4).
11Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 3. Astra® TiO2-blast titanium grade 3 cylindrical screws with internal connection (Astra Tech AB,Mölndal, Sweden).
Figure 4. Radiographic image: Astra® TiO2-blast titanium grade 3 cylindrical screws with internal
connection (Astra Tech AB, Mölndal, Sweden).
1. Astra® TiO2-blast titanium grade 3 cylindrical screws withinternal connection (Astra Tech AB) (Astrand 1999; Wennström2004; Lee 2007; Akoglu 2011) (Figure 3; Figure 4).
2. Astra® TiO2-blast titanium grade 3 tapered screws withinternal connection (Astra Tech AB) (Lee 2007) (Figure 5;Figure 6).
12Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 5. Astra® TiO2-blast titanium grade 3 tapered screws with internal connection (Astra Tech AB).
Figure 6. Radiographic image: Astra® TiO2-blast titanium grade 3 tapered screws with internal connection
(Astra Tech AB).
1. Brånemark® Standard turned titanium grade 1 cylindricalscrews with external hexagon (Nobel Biocare AB, Göteborg,Sweden) (Batenburg 1998; Moberg 2001) (Figure 7; Figure 8).
Figure 7. Brånemark® Standard turned titanium grade 1 cylindrical screws with external hexagon (Nobel
Biocare AB, Göteborg, Sweden).
13Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 8. Radiographic image: Brånemark® Standard turned titanium grade 1 cylindrical screws withexternal hexagon (Nobel Biocare AB, Göteborg, Sweden).
1. Brånemark® Mark II turned titanium grade 1 cylindricalscrews with external hexagon (Nobel Biocare AB) (Astrand 1999;Astrand 2002; Gatti 2002) (Figure 9; Figure 10).
Figure 9. Brånemark® Mark II type turned titanium grade 1 cylindrical screws with external hexagon
(Nobel Biocare AB, Göteborg, Sweden).
14Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 10. Radiographic image: Brånemark® Mark II type turned titanium grade 1 cylindrical screws withexternal hexagon (Nobel Biocare AB).
1. Brånemark® conical transmucosal turned titanium grade 1cylindrical screws with external hexagon (Nobel Biocare AB)(Gatti 2002) (Figure 11).
Figure 11. Brånemark® conical transmucosal turned titanium grade 1 cylindrical screws with externalhexagon (Nobel Biocare AB, Göteborg, Sweden).
1. Brånemark® Mark III turned titanium grade 4 cylindricalscrews with external hexagon (Nobel Biocare AB) (Fröberg2006) (Figure 12; Figure 13).
15Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 12. Brånemark® Mark III type turned titanium grade 4 cylindrical screws with external hexagon(Nobel Biocare AB, Göteborg, Sweden).
Figure 13. Radiographic image: Brånemark® Mark III type turned titanium grade 4 cylindrical screws with
external hexagon (Nobel Biocare AB, Göteborg, Sweden).
1. Brånemark® Mark III TiUnite oxidised titanium grade 4cylindrical screws with external hexagon (Nobel Biocare AB)(Fröberg 2006) (Figure 14; Figure 15).
16Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 14. Brånemark® Mark III TiUnite oxidised titanium grade 4 cylindrical screws with external hexagon(Nobel Biocare AB, Göteborg, Sweden).
Figure 15. Radiographic image: Brånemark® Mark III TiUnite oxidised titanium grade 4 cylindrical screws
with external hexagon (Nobel Biocare AB, Göteborg, Sweden).
1. Brånemark® Mark IV turned titanium grade 4 screws withexternal hexagon (Nobel Biocare AB) (Schincaglia 2007) (Figure16; Figure 17).
17Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 16. Brånemark® Mark IV type turned titanium grade 4 screws with external hexagon (NobelBiocare AB, Göteborg, Sweden).
Figure 17. Radiographic image: Brånemark® Mark IV type turned titanium grade 4 screws with external
hexagon (Nobel Biocare AB, Göteborg, Sweden).
1. Brånemark® Mark IV TiUnite oxidised titanium grade 4cylindrical screws with external hexagon (Nobel Biocare AB)(Payne 2004;Schincaglia 2007) (Figure 18; Figure 19).
18Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 18. Brånemark® Mark IV TiUnite oxidised titanium grade 4 cylindrical screws with external hexagon(Nobel Biocare AB, Göteborg, Sweden).
Figure 19. Radiographic image: Brånemark® Mark IV TiUnite oxidised titanium grade 4 cylindrical screws
with external hexagon (Nobel Biocare AB, Göteborg, Sweden).
1. NobelActive® TiUnite oxidised titanium grade 4 taperedscrews with internal connection (Nobel Biocare AB) (Kielbassa2009; Pozzi 2014) (Figure 20; Figure 21).
19Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 20. NobelActive® TiUnite oxidised titanium grade 4 tapered screws with internal connection (NobelBiocare AB, Göteborg, Sweden).
Figure 21. Radiographic image: NobelActive® TiUnite oxidised titanium grade 4 tapered screws with
internal connection (Nobel Biocare AB, Göteborg, Sweden).
1. NobelActive® TiUnite oxidised titanium grade 4 taperedscrews with external hexagon (Nobel Biocare AB) (Kielbassa2009) (Figure 22).
20Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 22. NobelActive® TiUnite oxidised titanium grade 4 tapered screws with external hexagon (NobelBiocare AB, Göteborg, Sweden).
1. NobelReplace® Tapered Groovy TiUnite oxidised titaniumgrade 4 tapered screws with internal connection (Nobel BiocareAB) (Kielbassa 2009; den Hartog 2011) (Figure 23; Figure 24).
Figure 23. NobelReplace® Tapered Groovy TiUnite oxidised titanium grade 4 tapered screws with internal
connection (Nobel Biocare AB, Göteborg, Sweden).
21Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Figure 24. Radiographic image: NobelReplace® Tapered Groovy TiUnite oxidised titanium grade 4 taperedscrews with internal connection (Nobel Biocare AB, Göteborg, Sweden).
1. Replace® Select Tapered TiUnite oxidised titanium grade 4tapered screws with internal connection (Nobel Biocare AB)(den Hartog 2011) (Figure 25; Figure 26).
Figure 25. Replace® Select Tapered TiUnite oxidised titanium grade 4 tapered screws with internalconnection (Nobel Biocare AB, Göteborg, Sweden).
22Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 26. Radiographic image: Replace® Select Tapered TiUnite oxidised titanium grade 4 tapered screwswith internal connection (Nobel Biocare AB, Göteborg, Sweden).
1. Nobel Speedy Groovy TiUnite oxidised titanium grade 4tapered screws with external connection (Nobel Biocare AB)(Pozzi 2014) (Figure 27; Figure 28).
Figure 27. Nobel Speedy Groovy TiUnite oxidised titanium grade 4 tapered screws with external
connection (Nobel Biocare AB, Göteborg, Sweden).
23Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 28. Radiographic image: Nobel Speedy Groovy TiUnite oxidised titanium grade 4 tapered screwswith external connection (Nobel Biocare AB, Göteborg, Sweden).
1. Implantium® sand-blasted, large grit, acid-etched (SLA)titanium grade 4 cylindrical screws with microthreads 0.5 mmbelow the top of the implant and internal connection (Dentium,Seoul, Korea) (Song 2009) (Figure 29).
Figure 29. Implantium® sand-blasted, large grit, acid-etched (SLA) titanium grade 4 cylindrical screws with
microthreads 0.5 mm below the top of the implant and internal connection (Dentium, Seoul, Korea).
1. Implantium® SLA titanium grade 4 cylindrical screws withmicrothreads to top of the implant and internal connection(Dentium) (Song 2009) (Figure 30).
24Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 30. Implantium® SLA titanium grade 4 cylindrical screws with microthreads to top of the implantand internal connection (Dentium, Seoul, Korea).
1. IMZ® TPS (titanium plasma-sprayed) titanium grade 2cylindrical screws with internal interlocking connection(Friedrichsfeld AG, Mannheim, Germany) (Batenburg 1998;Heydenrijk 2002) (Figure 31; Figure 32).
Figure 31. IMZ® TPS (titanium plasma-sprayed) titanium grade 2 cylinders with internal interlocking
connection (Friedrichsfeld AG, Mannheim, Germany).
25Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 32. Radiographic image: IMZ® TPS (titanium plasma-sprayed) titanium grade 2 cylinders withinternal interlocking connection (Friedrichsfeld AG, Mannheim, Germany).
1. ITI® TPS titanium grade 4 cylindrical screws with internalconnection (Institut Straumann AG, Waldenburg, Switzerland)(Astrand 2002; Heydenrijk 2002; Payne 2003) (Figure 33;Figure 34).
Figure 33. ITI® TPS titanium grade 4 cylindrical screws with internal connection (Institut Straumann AG,
Waldenburg, Switzerland).
26Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 34. Radiographic image: ITI® TPS titanium grade 4 cylindrical screws with internal connection(Institut Straumann AG, Waldenburg, Switzerland).
1. ITI® TPS titanium grade 4 cylindrical hollow screws withinternal connection (Institut Straumann AG) (Batenburg 1998;Moberg 2001) (Figure 35).
Figure 35. Radiographic image: ITI® TPS titanium grade 4 cylindrical hollow screws with internal
connection (Institut Straumann AG, Waldenburg, Switzerland).
1. ITI® SLA titanium grade 4 cylindrical solid screws withinternal connection with a 2.8-mm turned neck (InstitutStraumann AG) (Lang 2007; Akoglu 2011; Heberer 2011)(Figure 36; Figure 37).
27Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 36. ITI® SLA/ SLActive titanium grade 4 cylindrical screws with internal connection with a 2.8 mmturned neck (Institut Straumann AG, Waldenburg, Switzerland).
Figure 37. Radiographic image: ITI® SLA/ SLActive titanium grade 4 cylindrical screws with internal
connection with a 2.8 mm turned neck (Institut Straumann AG, Waldenburg, Switzerland).
1. ITI® SLA solid titanium grade 4 tapered screws withinternal connection (Institut Straumann AG) (Lang 2007)(Figure 38; Figure 39).
28Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 38. ITI® SLA/ SLActive/ Roxolid solid titanium grade 4 tapered screws with internal connection(Institut Straumann AG, Waldenburg, Switzerland).
Figure 39. Radiographic image: ITI® SLA/ SLActive/ Roxolid solid titanium grade 4 tapered screws with
internal connection (Institut Straumann AG, Waldenburg, Switzerland).
1. ITI® SLActive solid titanium grade 4 cylindrical screwswith internal connection (Institut Straumann AG) (Heberer2011) (Figure 36; Figure 37).
2. ITI® SLActive solid titanium grade 4 tapered screws withinternal connection (Institut Straumann AG) (Al-Nawas 2012)(Figure 38; Figure 39).
3. ITI® Roxolid™ SLActive solid titanium grade 4 taperedscrews with internal connection (Institut Straumann AG)(Al-Nawas 2012) (Figure 38; Figure 39).
4. MegaGen EZ Plus titanium grade 4 tapered screw withinternal connection (MegaGen Implant, Gyeongbuk, SouthKorea) (Esposito 2012) (Figure 40).
29Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 40. MegaGen EZ Plus titanium grade 4 tapered screw with internal connection (MegaGen Implant,Gyeongbuk, South Korea).
1. MegaGen EZ Plus Xpeed titanium grade 4 tapered screwwith internal connection (MegaGen Implant) (Esposito 2012)(Figure 41).
Figure 41. MegaGen EZ Plus Xpeed titanium grade 4 tapered screw with internal connection (MegaGen
Implant, Gyeongbuk, South Korea).
1. Neoss sand-blasted, acid-etched titanium grade 4cylindrical screws with internal connection (Neoss Ltd,Harrogate, UK) (Alsabeeha 2011) (Figure 42; Figure 43).
30Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 42. Neoss sand-blasted, acid-etched titanium grade 4 cylindrical screws with internal connection(Neoss Ltd, Harrogate, UK).
Figure 43. Radiographic image: Neoss sand-blasted, acid-etched titanium grade 4 cylindrical screws withinternal connection (Neoss Ltd, Harrogate, UK).
1. Seven TPS titanium grade 4 screws with external hexagon(Sweden & Martina, Padua, Italy) (Crespi 2009) (Figure 44).
31Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 44. Seven TPS titanium grade 4 screws with external hexagon (Sweden & Martina, Padua, Italy).
1. Southern® sand-blasted titanium grade 4 cylindrical screwswith external hexagon (Southern Implants, Irene, South Africa)(Tawse-Smith 2001; Tawse-Smith 2002; Payne 2003; Payne2004; Alsabeeha 2011) (Figure 45).
Figure 45. Southern® sand-blasted titanium grade 4 cylindrical screws with external connection (Southern
Implants, Irene, South Africa).
1. Southern® sand-blasted titanium grade 4 8-mm widetapered screws with external hexagon (Southern Implants)(Alsabeeha 2011) (Figure 46).
32Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 46. Southern® sand-blasted titanium grade 4 8mm wide tapered screws with external connection(Southern Implants, Irene, South Africa).
1. SPI® Element implant sand-blasted acid-etched titaniumgrade 4 cylindrical screw with internal connection (ThommenMedical, Waldeburg, Switzerland) (Esposito 2013a) (Figure 47;Figure 48).
Figure 47. SPI® Element implant sand-blasted acid-etched titanium grade 4 cylindrical screw with internal
connection (Thommen Medical, Waldeburg, Switzerland).
33Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 48. Radiographic image: SPI® Element implant sand-blasted acid-etched titanium grade 4 cylindricalscrew with internal connection (Thommen Medical, Waldeburg, Switzerland).
1. SPI® Element implant sand-blasted acid-etched titaniumgrade 4 cylindrical screw with internal connection (ThommenMedical) treated with a monolayer of permanently bound multi-phosphonic acid molecules (Nano Bridging Molecules, Gland,Switzerland) (Esposito 2013a) (Figure 49; Figure 50).
Figure 49. SPI® Element implant SurfLink treated titanium grade 4 cylindrical screw with internal
connection (Thommen Medical, Waldeburg, Switzerland).
34Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 50. Radiographic image: SPI® Element implant SurfLink treated titanium grade 4 cylindrical screwwith internal connection (Thommen Medical, Waldeburg, Switzerland).
1. Steri-Oss® HL series, 3.8-mm diameter acid-etchedtitanium grade 5 cylindrical screws with external hexagon (Steri-Oss, Yorba Linda, CA, USA) (Tawse-Smith 2001; Tawse-Smith2002) (Figure 51; Figure 52).
Figure 51. Steri-Oss® HL series, 3.8 mm in diameter acid-etched titanium grade 5 cylindrical screws with
external connection (Steri-Oss, Yorba Linda, CA, USA).
35Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 52. Radiographic image: Steri-Oss® HL series, 3.8 mm in diameter acid-etched titanium grade 5cylindrical screws with external connection (Steri-Oss, Yorba Linda, CA, USA).
1. SwissPlus® sand-blasted acid-etched titanium grade 4cylindrical screw with internal connection (Zimmer Dental Inc.Calsbad, USA) (Akoglu 2011) (Figure 53).
Figure 53. SwissPlus® sand-blasted acid-etched titanium grade 4 cylindrical screw with internal connection
(Zimmer Dental Inc. Calsbad, USA).
1. WINSIX® implant sand-blasted acid-etched titaniumgrade 4 cylindrical screw with internal connection (Winsix Ltd,London, UK) (Prosper 2009) (Figure 54).
36Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 54. WINSIX® implant sand-blasted acid-etched titanium grade 4 tapered screw with internalconnection (Winsix Ltd, London, UK).
37Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

1. WINSIX® implant sand-blasted acid-etched titaniumgrade 4 tapered screw with internal connection (Winsix Ltd)(Prosper 2009) (Figure 55).
Figure 55. WINSIX® implant sand-blasted acid-etched titanium grade 4 cylindrical screw with internal
connection (Winsix Ltd, London, UK).
Participant inclusion criteria
We included people with the following edentulism types.• Edentulous jaws (Astrand 1999; Heberer 2011).• Edentulous mandibles (Batenburg 1998; Moberg 2001;
Tawse-Smith 2001; Gatti 2002; Heydenrijk 2002; Tawse-Smith2002; Payne 2003; Fröberg 2006; Akoglu 2011; Alsabeeha 2011;Al-Nawas 2012).
• Edentulous maxillae (Payne 2004). In this trial, maxillaewere treated either with a ridge expansion osteotomy or acombined ridge split and osteotomy procedure, depending onthe ridge bucco-palatal width and the degree of ridge resorption.Autogenous bone grafts were used to fill intraosseous grooves ofthe ridge split-cases.
• Fully or partially edentulous maxillae (Esposito 2012).• Partially edentulous jaws (Wennström 2004; Lee 2007;
Crespi 2009; Kielbassa 2009; Prosper 2009; Song 2009; Heberer2011; Esposito 2013a). In one trial, implants were placed infresh extraction sockets without any bone augmentationprocedure (Crespi 2009).
• Partially edentulous maxillae (Astrand 2002).• Partially edentulous posterior mandibles (Schincaglia 2007;
Pozzi 2014).• Single implants in both jaws (Lang 2007), or in the anterior
maxilla (den Hartog 2011). In one trial, implants were placed infresh extraction sockets that could be augmented with anorganicbovine bone and bioresorbable barriers (Lang 2007).
38Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Loading time
• Immediate loading (Gatti 2002; Fröberg 2006; Schincaglia2007; Crespi 2009; Kielbassa 2009).
• Early loading (Tawse-Smith 2002; Payne 2003; Payne2004; den Hartog 2011). More specifically: two weeks (Payne2003); six weeks (Tawse-Smith 2002; Alsabeeha 2011); six to 10weeks in the mandible and nine to 14 weeks in the maxilla(Heberer 2011; Esposito 2012); eight weeks (Akoglu 2011;Al-Nawas 2012); and 12 weeks after placement (Payne 2004;den Hartog 2011).
• Conventional loading (at least three months in themandible and six months in the maxilla) (Batenburg 1998;Astrand 1999; Moberg 2001; Tawse-Smith 2001; Heydenrijk2002; Wennström 2004; Fröberg 2006; Lee 2007; Prosper 2009;Song 2009; Esposito 2013a; Pozzi 2014).
Prosthetic design
• Screw-retained cross-arch fixed prostheses on four to siximplants (Astrand 1999; Moberg 2001; Fröberg 2006; Heberer2011).
• Bar-retained overdentures supported by two implants(Batenburg 1998; Heydenrijk 2002), or four implants (Gatti2002), or on unspecified number of implants (Heberer 2011).
• Overdentures retained by one ball or locator attachment(Alsabeeha 2011), two locator attachments (Al-Nawas 2012),two ball attachments (Tawse-Smith 2001; Tawse-Smith 2002;Payne 2003; Akoglu 2011), or three ball attachments (Payne2004).
• Single crows and fixed prostheses supported up to siximplants (Esposito 2012).
• Screw-retained partial prostheses on two to four implants(Astrand 2002; Wennström 2004; Lee 2007; Schincaglia 2007;Song 2009; Heberer 2011; Esposito 2012).
• Crowns cemented on single implants (Lang 2007; Crespi2009; Kielbassa 2009; Prosper 2009; den Hartog 2011; Esposito2013a; Pozzi 2014).
Characteristics of outcome measures
The primary outcome (biological and mechanical failures) wasrecorded in all trials with one exception (Wennström 2004), forwhich the author did no reply whether they removed or not thescrew-retained partial fixed prostheses to evaluate implant stability.Occurrence of peri-implantitis was mentioned in only four tri-als comparing implants with turned surfaced with implants withroughened surfaces (Astrand 1999; Moberg 2001; Astrand 2002;Schincaglia 2007). Another trial reported the number of peo-ple who had lost implants for peri-implantitis at 10 years, butnot on the occurrence of peri-implantitis and when it occurred(Batenburg 1998). No reply to our request of clarification wasprovided.
The secondary outcomes (bone level measurements) were recordedin all trials. However, in four trials, peri-implant bone level mea-surements were fully or partially performed on panoramic ra-diographs (Moberg 2001; Gatti 2002; Heberer 2011; Al-Nawas2012), in 10 trials, baseline radiographs were taken at implantloading (Batenburg 1998; Tawse-Smith 2001; Astrand 2002;Tawse-Smith 2002; Payne 2004; Wennström 2004; Lee 2007;Song 2009; Akoglu 2011; Alsabeeha 2011), and in one trial, theywere not presented as mean values but as frequencies (Prosper2009). Such bone level measurements were considered to be in-accurate either for the quality of the radiographs or for not usingthe proper baseline and were not included in the present analy-ses. In one trial, the measurements of 78 implant surfaces out of178 were missing, therefore the radiographic data were not used(Fröberg 2006). In two trials, bone level assessment was calculatedon a site basis (only for three year data Kielbassa 2009) and theauthors were not able to supply the required data (participant ba-sis) (Heydenrijk 2002; Kielbassa 2009). The five-year data of an-other trial were not used since the authors published separate datafor maxillae and mandibles (Astrand 1999), while we requestedcombined data, which were not supplied. The three-year data ofa split-mouth study could not be used since we did not have thestandard deviation of the difference (Astrand 2002). Bone levelchanges data were not yet available for one ongoing study (Lang2007).
Duration of follow-up after implant loading
• One year (Payne 2004; Lang 2007; Kielbassa 2009; Song2009; Alsabeeha 2011; Heberer 2011; Al-Nawas 2012; Esposito2012; Esposito 2013a; Pozzi 2014).
• Fifteen months (den Hartog 2011).• Eighteen months (Fröberg 2006; Prosper 2009).• Two years (Gatti 2002; Crespi 2009).• Three years (Moberg 2001; Astrand 2002; Lee 2007;
Schincaglia 2007).• Five years (Astrand 1999; Heydenrijk 2002; Wennström
2004; Akoglu 2011).• Ten years (Batenburg 1998; Tawse-Smith 2001;
Tawse-Smith 2002; Payne 2003).
Sample size
Only seven studies undertook a priori sample size calculations(Astrand 1999; Astrand 2002; Schincaglia 2007; Kielbassa 2009;Song 2009; den Hartog 2011; Pozzi 2014). The sample size wascalculated to detect a true difference of 0.3 mm in Astrand 2002,0.4 mm in Astrand 1999, and 0.5 mm in den Hartog 2011; Pozzi2014 in marginal bone levels thought to be of clinical significance.Another study calculated the sample size considering the implantas statistical unit but this was not correct (Schincaglia 2007). Itwas unclear how the sample size was calculated in two studies(Kielbassa 2009; Song 2009).
39Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

One multicentre study did not report any sample size calculation,but we believe the sample to be sufficiently large (208 participants)to detect a statistically significant difference, if any (Lang 2007).
Inclusion/exclusion criteria
For more details, see the Characteristics of included studies table.
Main inclusion criteria
• People with edentulous mandibles of 8 to 15 mm of boneheight (Payne 2003).
• People with edentulous mandibles of 13 to 15 mm of boneheight (Tawse-Smith 2001; Tawse-Smith 2002).
• People with edentulous mandibles of 15 to 25 mm of boneheight not requiring augmentation procedures (Akoglu 2011).
• People with edentulous mandibles allowing placement ofimplants at least 9 mm long (Gatti 2002), with sufficient bonewidth to allow placement of 3.3-mm implants not requiringaugmentation procedures (Al-Nawas 2012).
• People with edentulous mandibles (Moberg 2001; Fröberg2006; Alsabeeha 2011).
• People with severely resorbed edentulous mandibles(Batenburg 1998; Heydenrijk 2002).
• People with edentulous maxillae (Payne 2004).• People with edentulous jaws not needing augmentation
procedures (Astrand 1999).• People with fully or partially edentulous jaws not needing
augmentation procedures (Kielbassa 2009; Esposito 2012),following removal of a malignant tumour and radiotherapy(Heberer 2011).
• People with partially edentulous maxillae not needingaugmentation procedures (Astrand 2002).
• People with partially edentulous jaws not needingaugmentation procedures (Wennström 2004; Prosper 2009),requiring two (Esposito 2013a) adjacently placed implants (Lee2007; Song 2009). Wennström 2004 included only participantswith a history of periodontitis.
• People with partially edentulous mandibles not needingaugmentation procedures requiring at least two implants (Pozzi2014).
• People with bilateral partially edentulous posteriormandibles requiring at least two implants each (Schincaglia2007).
• People requiring one or two immediate post-extractivemaxillary implants in the aesthetic zone (premolar to premolar)(Crespi 2009).
• People requiring immediate post-extractive maxillary singleimplants in the aesthetic zone (premolar to premolar) betweentwo adjacent teeth (Lang 2007).
• People requiring maxillary single implants in the aestheticzone (first premolar to first premolar) between two adjacent teethin healed sites (den Hartog 2011).
Main exclusion criteria
• Radiotherapy in the head and neck region (Batenburg1998; Tawse-Smith 2001; Astrand 2002; Gatti 2002;Heydenrijk 2002; Tawse-Smith 2002; Payne 2003; Wennström2004; Kielbassa 2009; Akoglu 2011; Alsabeeha 2011; denHartog 2011; Al-Nawas 2012; Esposito 2012; Esposito 2013a).
• Severe intermaxillary skeletal discrepancy (Gatti 2002).• Severe clenching and bruxism (Astrand 2002; Gatti 2002;
Crespi 2009; Kielbassa 2009; Prosper 2009; Al-Nawas 2012).• Any history of bruxism (Tawse-Smith 2001; Tawse-Smith
2002; Payne 2003; Payne 2004).• Drug or alcohol abuse or both (Moberg 2001; Astrand
2002; Gatti 2002; Crespi 2009; Kielbassa 2009; Prosper 2009;Akoglu 2011; Al-Nawas 2012; Esposito 2012).
• Uncontrolled diabetes (Gatti 2002; Wennström 2004;Fröberg 2006; Kielbassa 2009; Al-Nawas 2012; Esposito 2013a;Pozzi 2014).
• Any evidence of previous and current smoking(Tawse-Smith 2001; Tawse-Smith 2002; Payne 2003; Payne2004; Prosper 2009; den Hartog 2011; Heberer 2011).
• Smoking more than 10 cigarettes per day (Gatti 2002; Lang2007; Crespi 2009; Al-Nawas 2012; Pozzi 2014).
• Smoking more than 20 cigarettes per day (Astrand 2002).• Current steroid treatment (Astrand 2002; Gatti 2002).• Current chemotherapy treatment (Astrand 2002; Gatti
2002).• Very soft bone (Tawse-Smith 2001; Tawse-Smith 2002;
Payne 2003; Alsabeeha 2011).• Grafted or regenerated bone (Payne 2004; Schincaglia
2007; Kielbassa 2009; Akoglu 2011; Al-Nawas 2012; Esposito2012).
• Extremely resorbed maxillae (Payne 2004).• Sites with interproximal or buccal bone defects (Crespi
2009).• Extraction sites less than three months (Schincaglia 2007;
Esposito 2012).• Insertion torque less than 35 Ncm (Pozzi 2014), or less
than 20 Ncm and implant stability quotient less than 60(Schincaglia 2007).
• Different opposing occlusion bilaterally (Schincaglia 2007).• Untreated periodontitis (Wennström 2004; Prosper 2009;
Al-Nawas 2012; Esposito 2012; Esposito 2013a; Pozzi 2014).• Periodontal bone loss greater than 20% at the adjacent
teeth (Lang 2007).• Full-mouth plaque and bleeding scores greater than 25% at
baseline (Lang 2007).• Teeth to be replaced affected by periodontal disease (Lang
2007).• Presence of clinically active periodontal disease as expressed
by probing pocket depths of 4 mm or greater and bleeding onprobing (index score >1) (den Hartog 2011).
• Presence of symptomatic periapical radiolucencies, acute
40Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

abscesses or chronic sinus tracts at the implant site (Lang 2007;Crespi 2009; den Hartog 2011; Esposito 2012; Esposito 2013a).
• Lack of primary implant stability (Lang 2007).• Less than 2 mm of keratinised mucosa (Lang 2007; Akoglu
2011).• Signs or symptoms of temporomandibular disorders
(Prosper 2009).• Poor general health (Heberer 2011).• People who could not be restored with a retrievable
prosthesis to allow for individual implant stability assessment(Esposito 2012).
• Treatment with intravenous bisphosphonates (Esposito2012; Esposito 2013a; Pozzi 2014).
Excluded studies
We excluded 53 trials due to problems with the data presented(Friberg 1992; Gher 1994; Geertman 1996; Boerrigter 1997;
Jones 1997; Kemppainen 1997; Truhlar 1997; Karlsson 1998;Reingewirtz 2000; Van Steenberghe 2000; Khang 2001; Roccuzzo2001; Geurs 2002; Karabuda 2002; Mau 2002; Tomatis 2002;Åstrand 2003; Friberg 2003; Joly 2003; Mau 2003; Rocci 2003;Testori 2003; da Cunha 2004; Shin 2006; Du Preez 2007; Goené2007; Oates 2007; Orsini 2007; Stavropoulos 2007; Nickenig2009; Piao 2009; Schätzle 2009; Cehreli 2010; Kim 2010;Liddelow 2010; Park 2010; Sanz 2010; Shibli 2010; Tan 2010;Zetterqvist 2010; Mackie 2011; Tallarico 2011; Tymstra 2011;Abtahi 2012; Canullo 2012; Kang 2012; Liaje 2012; Peñarrocha-Diago 2012; Van Assche 2012; Esposito 2013b; Gultekin 2013;Kadkhodazadeh 2013; Thoma 2014). See Characteristics ofexcluded studies table.
Risk of bias in included studies
The agreed risk of bias of the included trials after having incorpo-rated the information provided by the authors is summarised inFigure 56 and Figure 57.
Figure 56. Risk of bias graph: review authors’ judgements about each risk of bias domain presented as
percentages across all included studies.
41Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 57. Risk of bias summary: review authors’ judgements about each risk of bias domain for eachincluded study.
42Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sequence generation
Fifteen (56%) trials described an adequate method of sequencegeneration and we assessed them as being at low risk of biasfor this domain (Batenburg 1998; Astrand 2002; Payne 2003;Payne 2004; Fröberg 2006; Lang 2007; Lee 2007; Kielbassa 2009;Prosper 2009; Alsabeeha 2011; den Hartog 2011; Al-Nawas 2012;Esposito 2012; Esposito 2013a; Pozzi 2014). It was unclear fromthe trial report and communication with authors whether sequencegeneration for 11 studies (41%) had an adequate method andwe assessed these studies as being at unclear risk of bias for thisdomain (Astrand 1999; Moberg 2001; Tawse-Smith 2001; Gatti2002; Heydenrijk 2002; Tawse-Smith 2002; Schincaglia 2007;Crespi 2009; Song 2009; Akoglu 2011; Heberer 2011). One study(3%) used a method of randomisation that induced an unbalancednumber of implants of the two types (Wennström 2004).
Allocation concealment
Allocation concealment was reported as having being done ade-quately in eight (30%) of the included studies (Wennström 2004;Lang 2007; Akoglu 2011; Alsabeeha 2011; den Hartog 2011;Esposito 2012; Esposito 2013a; Pozzi 2014). It was unclear fromthe trial report and communication with authors whether al-location for 16 (59%) studies had been adequately concealed,and we assessed these studies as being at unclear risk of bias forthis domain (Batenburg 1998; Moberg 2001; Tawse-Smith 2001;Astrand 2002; Gatti 2002; Heydenrijk 2002; Tawse-Smith 2002;Payne 2003; Payne 2004; Fröberg 2006; Lee 2007; Crespi 2009;Prosper 2009; Song 2009; Heberer 2011; Al-Nawas 2012). Noallocation concealment procedures were implemented in three(11%) trials (Astrand 1999; Schincaglia 2007; Kielbassa 2009),and we assessed these trials as being at high risk of bias for thisdomain.
Blinding of outcome assessors
For four trials (15%), outcome assessors were blinded (Lang 2007;Heberer 2011; Esposito 2012; Esposito 2013a), whereas for 15trials (55%) (Batenburg 1998; Moberg 2001; Tawse-Smith 2001;Astrand 2002; Heydenrijk 2002; Tawse-Smith 2002; Payne 2003;Payne 2004; Wennström 2004; Fröberg 2006; Schincaglia 2007;Crespi 2009; Akoglu 2011; den Hartog 2011; Pozzi 2014), it wasunclear whether outcome assessors were blinded and we consideredthese studies at unclear risk of detection bias. In eight trials (30%)(Astrand 1999; Gatti 2002; Lee 2007; Kielbassa 2009; Prosper2009; Song 2009; Alsabeeha 2011; Al-Nawas 2012), outcomeassessors were not blinded and we considered these studies at highrisk of detection bias.
Incomplete outcome data
There were low numbers of drop-outs in all but four trials(Tawse-Smith 2002; Payne 2003; Fröberg 2006; Kielbassa 2009),which were assessed as at high risk of bias. All outcome datawere reported in 21 trials (78%) (Batenburg 1998; Moberg 2001;Tawse-Smith 2001; Astrand 2002; Gatti 2002; Tawse-Smith 2002;Payne 2003; Payne 2004; Lang 2007; Schincaglia 2007; Lee 2007;Crespi 2009; Kielbassa 2009; Prosper 2009; Song 2009; Akoglu2011; den Hartog 2011; Heberer 2011; Esposito 2012; Esposito2013a; Pozzi 2014). In two trials, the radiographic data of one par-ticipant were missing (Alsabeeha 2011; Astrand 1999), and in twotrials, radiographs were missing for two participants (Heydenrijk2002; Al-Nawas 2012), but we assessed these as at low risk ofbias. In another trial, not all the radiographic data were presented,which confirmed the high risk of bias assessment for this study forthis domain (Fröberg 2006). In one trial, it was unclear whetherprostheses were removed to assess implant mobility and, for thisreason, the study could be used only to answer the first part ofthe secondary objective, and we assessed the incomplete outcomedata as at unclear risk of bias (Wennström 2004). Therefore, weassessed four trials as at high risk of bias, one at unclear risk of biasand the remaining 22 (81%) at low risk of bias for this domain.
Selective reporting
We assessed all but four of the trials (85%) included in this reviewas being at low risk of selective reporting bias because they allreported most of the main outcomes of this review (Moberg 2001;Wennström 2004; Lang 2007; Prosper 2009). In one trial, not allevaluated outcomes were presented (Lang 2007), in one trial, datawere not given for participants in which implants failed (Prosper2009), and one trial comparing Astra implants with a turned versusa TiO2-blasted surface did not disclose how many implants ofeach type were placed and presented the various outcomes dataof the two different surfaces combined, rendering the comparisonuseless (Wennström 2004). Therefore, we assessed these trials asbeing at high risk of bias for this domain. We judged one trialat unclear risk of bias because at the three-year examination, twoITI implants were treated for peri-implantitis but their fate wasreported (Moberg 2001).
Other potential sources of bias
In 21 of the trials (78%), we identified no other potential source ofbias (Batenburg 1998; Moberg 2001; Tawse-Smith 2001; Payne2003; Payne 2004; Wennström 2004; Fröberg 2006; Lang 2007;Lee 2007; Schincaglia 2007; Crespi 2009; Kielbassa 2009; Prosper2009; Song 2009; Alsabeeha 2011; den Hartog 2011; Heberer2011; Al-Nawas 2012; Esposito 2012; Esposito 2013a; Pozzi
43Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2014). We scored two trials (7%) at high risk of bias: the plannedpublication at five years was cancelled by the authors and theauthors justified this as the sponsored implants were no longercommercially available (Astrand 2002). However, this publicationwould have contained crucial information on the occurrence oroutcome of peri-implantitis. In one trial, most of the failed Steri-Oss implants were placed by a surgeon who placed only Steri-Oss implants and who was judged, afterwards, to have insufficientclinical experience; therefore, the effect of the different implantsystems is confounded by the different degree of surgical experi-ence of different operators (Tawse-Smith 2002). We scored fourtrials (15%) at unclear risk of bias, because in one trial, eight par-ticipants treated with Brånemark implants were scored as havingtype IV bone quality (very soft bone) according to the Lekholmand Zarb classification (Lekholm 1985) versus one participant inthe Astra group (Astrand 1999). For two trials, the amount of in-formation presented was insufficient to judge on the comparabil-ity of controls and test groups at entry (Heydenrijk 2002; Akoglu2011), and in one trial, we judged the sample size of five partici-pants per group to be insufficient (Gatti 2002).
Overall risk of bias
The final ’Risk of bias’ assessment, after incorporating the addi-tional information kindly provided by the authors of the trials issummarised in Figure 56 and Figure 57. For each trial, we assessedwhether it was at low, unclear or high risk of bias. We judged twotrials (7%) to be at low risk (Esposito 2012; Esposito 2013a), 10trials (37%) to be at unclear risk of bias and 15 trials (56%) to beat high risk of bias.
Effects of interventions
See: Summary of findings for the main comparison Implanttype A compared with implant type B for implant failure and boneloss; Summary of findings 2 Turned implants compared withroughened implants for early implant failure and peri-implantitis
Primary objectives
We presented implant failures and marginal bone level changes atone, three, five and 10 years in the following subgroups. Data forsingle studies are presented in additional tables (Table 1; Table 2;Table 3; Table 4; Table 5).
1. Trials comparing implants with different surface
preparations, but having similar shape and material (six
trials)
We included six trials in the following comparisons (Wennström2004; Fröberg 2006; Schincaglia 2007; Heberer 2011; Esposito2012; Esposito 2013a).
Astra cylindrical implants: turned versus TiO2-blastedsurface (Tiobalst)
One trial with a split-mouth design compared one Astra cylin-drical implant with a turned surface versus one to three implantswith a TiO2-blasted surface (Figure 3; Figure 4) supporting screw-retained fixed prostheses in partially edentulous participants forfive years (Wennström 2004). Fifty-one participants were includedand four participants dropped out after the first year post-loading.The number of the two implants types was imbalanced since moreTiO2 implants were placed, but the numbers of each implant typeswere not disclosed. It is unknown whether implant stability wasassessed with the prostheses removed. One turned implant failedearly and another three implants with an unknown surface typefractured. The data of this study could only be used for the firstpart of the secondary objective.
Brånemark Mark III implants: turned versus oxidised surface(TiUnite)
One trial with a split-mouth design compared three BrånemarkMark III implants with turned surfaces (Figure 12) versus threeBrånemark Mark III with TiUnite oxidised surfaces (Figure 14)supporting screw-retained metal-ceramic cross-arch prostheses forone year (Fröberg 2006). The implants were immediately loaded.Fifteen participants were included. There were no baseline differ-ences for position, implant stability quotient or implant lengthbetween the two groups. There were no withdrawals or failures.
Brånemark Mark IV implants: turned versus oxidised surface(TiUnite)
One trial with a split-mouth design compared two or threeBrånemark Mark IV implants with turned surfaces (Figure 16)versus two Brånemark Mark IV with a TiUnite oxidised surfaces(Figure 18) supporting screw-retained metal-ceramic prosthesesfor three years (Schincaglia 2007). The implants were immediatelyloaded. Ten participants were included. There were no baselinedifferences for position, insertion torque values or implant lengthbetween the two groups with the exception that two out of 10 pros-theses supported by the turned implants included three implants.There were no withdrawals. One implant with a turned surfacefailed three months after placement. Another turned implant dis-played rotational mobility one month after placement, but was re-tightened and put out of occlusion. Two months later the implantwas stable and was used to support the definitive restoration. Therewas no statistically significant difference for failures and marginalbone level changes (Table 1) of the different surfaces.
ITI regular neck: SLA standard versus SLActive surface
One trial with a split-mouth design compared ITI SLA standard(regular neck) (Figure 36; Figure 37) versus ITI SLActive surfaces
44Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Figure 36; Figure 37) supporting bar retained overdentures andfixed prostheses for one year in irradiated participants (Heberer2011). The implants were early loaded. Twenty participants wereincluded. There were no baseline differences for implant positionbetween the two groups. There was one withdrawal due to a re-current tumour. There were two early failures in the SLA standardgroup in two participants prior to loading. There was no statis-tically significant difference for failures of the different surfaces(Table 1).
MegaGen EZ Plus implants with blasted surface: standardversus calcium-incorporated (Xpeed) surface
One trial with a parallel group design compared MegaGen EZ Plusimplants with blasted surfaces; standard (Figure 40) versus cal-cium-incorporated (Xpeed) (Figure 41) supporting fixed prosthe-ses for one year (Esposito 2012). The implants were early loaded.Sixty participants were included. There were no baseline differ-ences for sex, age, length of the implant used or bone qualitybetween the two groups. There were no withdrawals or failures.There was no statistically significant difference for marginal bonelevel changes of the different surfaces (Table 1).
SPI Element implants with sand-blasted acid-etched surface:standard versus SurfLink-modified surface
One trial with a split-mouth design compared one SPI Elementimplant with sand-blasted acid-etched surface (Figure 47; Figure48) versus one identical implant with a SurfLink-modified surface(Figure 49; Figure 50) supporting single cement-retained metal-ceramic crowns for one year (Esposito 2013a). The implants wereconventionally loaded. Twenty-three participants were included.There were no baseline differences for position, insertion torquevalues or implant length between the two groups. There was onewithdrawal and no failures. There was no statistically significantdifference for marginal bone level changes of the different surfaces(Table 1).
2. Trials comparing implants with different shapes, but
having similar surface preparation and material (seven trials)
We included seven trials in the following comparisons (Gatti 2002;Lang 2007; Lee 2007; Kielbassa 2009; Prosper 2009; Song 2009;Pozzi 2014).
Astra cylindrical versus Astra conical implants
One trial with a split-mouth design compared one Astra TiO2-blast titanium cylindrical screw without microthreads on the coro-nal portion (Figure 3) versus one Astra TiO2-blast titanium ta-pered screw with microthreads on the coronal portion (Figure 5),placed adjacent to each other for three years (Lee 2007). Thirty-four participants (22 maxillae and 12 mandibles) were originally
included. There were no baseline differences for implant length,bone quality and quantity between the two groups. There were nowithdrawals or failures.
Brånemark Mark II type versus Brånemark conicaltransmucosal implants
One trial with a parallel group design compared four BrånemarkMark II type screws (Figure 9) versus four Brånemark conicaltransmucosal screws (Figure 11) supporting mandibular overden-tures for two years (Gatti 2002). The implants were immediatelyloaded. Five participants were included in each group. There wereno baseline differences for sex, age and length of the implant usedbetween the two groups. There were no withdrawals or failures.
Implantium microthreads at the top versus Implantiummicrothreads 0.5 mm below the top
One trial with a split-mouth design compared one Implantiumscrew-shaped threaded implant with microthreads at the coronalportion of the implant (Figure 29) versus one Implantium screw-shaped implant with microthreads 0.5 mm below the coronal por-tion of the implant (Figure 30) for one year (Song 2009). The im-plants were placed adjacent to each other and were conventionallyloaded. Twenty participants were originally included. There wereno baseline differences for length of the implant used between thetwo groups. There were no withdrawals or failures.
ITI cylindrical versus ITI tapered implants
One trial with a parallel group design compared single immediatepost-extractive ITI SLA implants of cylindrical (Figure 36) versustapered (Figure 38) design for one year (Lang 2007). One hundredand four participants were included in each group. There were nobaseline differences for age, sex, smokers, full mouth plaque andbleeding scores, and implant location, between the two groups.There were no withdrawals or failures.
NobelActive external connection versus NobelActive internalconnection implants
One trial with a parallel group design compared NobelActive ta-pered implants with external connection (Figure 22) versus No-belActive transmucosal tapered implants with internal connection(Figure 20) for three years (Kielbassa 2009). Sixty-four participantswere included in the internal connection group and 53 participantswere included in the external connection group. There were nobaseline differences for age, sex, smokers, full mouth plaque, bleed-ing scores and implant location between the two groups. Nine par-ticipants dropped out from the external connection group versus18 participants from the internal connection group. Three partici-pants lost one implant with external connection versus five partic-ipants who lost five implants with internal connection. There was
45Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

no statistically significant difference for failures or for marginalbone level changes between the implant shapes after one year offunction (Table 2).
NobelActive external connection versus NobelReplaceimplants
One trial with a parallel group design compared NobelActive ta-pered implants, variable-thread design and external connection(Figure 22) versus NobelReplace standard tapered implants (Figure23) for three years (Kielbassa 2009). Fifty-three participants wereincluded in the external connection group and 60 participants wereincluded in the NobelReplace group. There were no baseline dif-ferences for age, sex, smokers, full mouth plaque, bleeding scoresand implant location between the two groups. Nine participantsdropped out in the NobelActive external connection group versus18 participants in the NobelReplace group. There were three im-plant failures in three participants from the NobelActive externalconnection group and six failures in five participants from the No-belReplace group, including two implants that fractured at inser-tion. There was no statistically significant difference for failures orfor marginal bone level changes between the implant shapes afterone year of function (Table 2).
NobelActive internal connection versus NobelReplaceimplants
One trial with a parallel group design compared NobelActive ta-pered implants, variable-thread design and internal connection(Figure 22) versus NobelReplace standard tapered implants (Figure23) implants for three years (Kielbassa 2009). Sixty-four partici-pants were included in the NobelActive internal connection groupand 60 participants were included NobelReplace group. Therewere no baseline differences for age, sex, smokers, full mouthplaque, bleeding scores and implant location between the twogroups. Eighteen participants dropped out in the NobelActive in-ternal connection group versus 18 participants in the NobelRe-place group. There were five failures in five participants from theNobelActive internal connection group and six failures in five par-ticipants from the NobelReplace group, including two implantsthat fractured at insertion. There was no statistically significantdifference for failures or for marginal bone level changes betweenthe implant shapes after one year of function (Table 2).
NobelActive internal connection versus Nobel Speedy Groovyexternal connection implants
One trial with a split-mouth design compared one NobelActivetapered implant with internal connection (Figure 20; Figure 21)versus one Nobel Speedy Groovy tapered screw with external con-nection (Figure 27) inserted into healed sites and conventionallyloaded for one year (Pozzi 2014). Thirty-four participants wereincluded. The implants were loaded after four months. There
were no baseline differences for implant location between the twogroups. There were no withdrawals or failures. Significantly moremarginal bone loss occurred at Nobel Speedy Groovy implants (-0.59 mm; 95% confidence interval (CI) -0.74 to -0.44; P value <0.001) (Table 2).
WINSIX cylindrical versus WINSIX tapered implants
One trial with a split-mouth design compared WINSIX cylin-drical screws (Figure 31) versus WINSIX tapered screws (Figure32) inserted into healed sites and conventionally loaded for twoyears (Prosper 2009). Sixty-eight participants were included. Eachparticipant received three tapered implants and three cylindricalimplants. Of these implants, one was placed submerged, one non-submerged and one was platform switched. There were no baselinedifferences for implant location between the two groups. At oneyear, there were two withdrawals and four WINSIX cylindricalimplants failed versus two WINSIX tapered implants. There wasno statistically significant difference for failures (Table 2).
3. Trials comparing implants with different materials, but
having similar surface preparation and shape (one trial)
One trial was included in the following comparison (Al-Nawas2012).
ITA SLActive implants: titanium grade 4 versus titanium-13zirconium (Roxolid)
One trial with a split-mouth design compared one ITI SLAc-tive (titanium grade 4) implant (Figure 38; Figure 39) versus oneITI SLActive Roxolid (titanium-13zirconium) implant (Figure38; Figure 39) supporting overdentures on two locators for oneyear (Al-Nawas 2012). The implants were early loaded after six toeight weeks. Ninety-two participants were included. There wereno baseline differences for position, implant stability quotient andimplant length between the two groups. There were four with-drawals. One Roxolid implant failed versus two implant failures intwo participants in the SLActive group. There was no statisticallysignificant difference for failures between the implant materialsafter one year of function (Table 3).
4. Trials comparing implants with different surface
preparation or shape or material, or a combination (13
trials)
Thirteen trials were included in the following comparisons(Batenburg 1998; Astrand 1999; Moberg 2001; Tawse-Smith2001; Astrand 2002; Heydenrijk 2002; Tawse-Smith 2002; Payne2003; Payne 2004; Crespi 2009; Akoglu 2011; Alsabeeha 2011;den Hartog 2011).
46Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Ankylos Plus (Dentsply) versus Seven (Sweden & Martina)implants
One trial with a parallel group design compared Seven (Figure44) versus Ankylos Plus implants (Figure 1) for two years (Crespi2009). Implants were placed flapless into post-extractive sites andwere immediately loaded. There were 24 in the Seven group and21 participants in the Ankylos group. There were no baseline dif-ferences for age, sex, smokers, full mouth plaque and bleedingscores, and implant location between the two groups. There wereno failures or withdrawals. There were no statistically significantdifferences for marginal bone loss (Table 4).
Astra TiO2-blast cylindrical versus turned Brånemark MarkII implants
One trial with a parallel group design compared submerged Astra(Figure 3) versus submerged Brånemark screws (Figure 9) in to-tally edentulous participants for five years (Astrand 1999). Thirty-three fully edentulous participants (17 maxillae and 16 mandibles)were originally included in each group. There were no baselinedifferences for sex, bone quantity and length of the implant usedbetween the two groups. However, eight participants treated withBrånemark implants were scored as having type IV bone quality(very soft bone) according to the Lekholm and Zarb classification(Lekholm 1985) versus one participant in the Astra group. Therewere two withdrawals after the third year due to death from theAstra group. Ten Brånemark implants failed in five participants(one participant lost five implants and the prosthesis) versus threeAstra implant failures in two participants (two failures in the sameparticipant were due to implant fracture: one between one-yearand three-year follow-ups and the other thereafter). Two additionalAstra implants in the same participant were successfully treatedfor peri-implantitis (suppuration combined with advanced boneloss). There were no statistically significant differences for failureor marginal bone level changes between the implant systems afterfive years of function (Table 4).
Astra TiO2-blast versus ITI SLA titanium implants
One trial with a parallel group design compared two submergedAstra (Figure 3) versus two non-submerged ITI implants (Figure36) placed in the intraforaminal region supporting overdenturesin edentulous mandibles for five years (Akoglu 2011). Twelve par-ticipants were included in each group. It is unclear whether impor-tant baseline differences existed between the two groups. The im-plants were early loaded eight weeks after placement. There wereno drop-outs or failures.
Astra TiO2-blast versus SwissPlus (Zimmer) cylindricalimplants
One trial with a parallel group design compared two submergedAstra (Figure 3) versus two non-submerged SwissPlus implants
(Figure 53) placed in the intraforaminal region supporting over-dentures in the edentulous mandible for five years (Akoglu 2011).Twelve participants were included in each group. It is unclearwhether important baseline differences existed between the twogroups. The implants were early loaded eight weeks after place-ment. There were no drop-outs or failures.
Brånemark versus IMZ (Friedrichsfeld) implants
One trial with a parallel group design compared two submergedBrånemark (Figure 7) versus two IMZ submerged implants (Figure31) supporting overdentures in edentulous mandibles for 10 years(Batenburg 1998). Thirty participants were included in eachgroup. There were no baseline differences for sex, mean edentu-lous period, mandibular bone quantity and height between thetwo groups. Three participants in the Brånemark group could notattend the five-year examination due to sickness. One participantin the IMZ group died between the 5-year and 10-year follow-up.One Brånemark and four IMZ implants failed. One Brånemarkand one IMZ implant failed at abutment connection, while theother three IMZ implants failed for peri-implantitis between yearsseven and 10. There was no statistically significant difference forfailures after 10 years of function (Table 4).
Brånemark Mark II versus ITI TPS hollow screw implants
Two trials compared submerged Brånemark Mark II versus non-submerged ITI TPS implants (Batenburg 1998; Moberg 2001).One trial with a parallel group design compared two BrånemarkMark II screws implants (Figure 7) versus two ITI TPS hollowscrews implants (Figure 35) supporting mandibular overdenturesfor 10 years (Batenburg 1998). Thirty participants were includedin each group. There were no baseline differences for sex, meanedentulous period, mandibular bone quantity and height betweenthe two groups. Two participants of the ITI group died, one priorto the one-year examination and the other prior to the three-yearexamination. Three participants in the Brånemark group and onein the ITI group could not attend the five-year examination dueto sickness. One Brånemark implant failed prior to the abutmentconnection operation. There was no statistically significant dif-ference for failures between the implant systems after 10 years offunction (Analysis 1.4).One trial with a parallel group design compared Brånemark MarkII screws (Figure 7) versus ITI TPS hollow screws (Figure 35)supporting mandibular fixed prostheses for three years (Moberg2001). Twenty participants were included in each group. Therewere no baseline differences for participant sex, age and location ofimplants between two groups. Three participants died prior to thethree-year examination (one in the Brånemark group and two inthe ITI group). Two Brånemark implants failed (one early failureand one for peri-implantitis between years one and two). OneITI implant failed for peri-implantitis at two years. However, two
47Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

additional ITI implants were affected by peri-implantitis at thethree-year examination and were under treatment. Their outcomewas unknown at the time of reporting. There was no statisticallysignificant difference for failures between the implant systems afterthree years of function (Analysis 1.2).We performed a meta-analysis of the two above studies (Batenburg1998; Moberg 2001). There was no statistically significant differ-ence for failures between the implant systems after three years offunction (Analysis 1.2).
Brånemark Mark II versus ITI TPS solid screw implants
One split-mouth trial compared Brånemark Mark II screws (Figure9) versus ITI TPS solid screws (Figure 33) supporting maxillarypartial screw-retained prostheses for three years (Astrand 2002).Twenty-eight participants were included. There were no baselinedifferences for implant length, bone quality and quantity betweenthe two groups. Two participants died before the three-year follow-up. Two Brånemark implants failed (early failures) in the sameparticipant and two ITI implants failed for peri-implantitis in twodifferent participants: one implant failed at one year and the otherafter three years. An additional five ITI implants showed clinicalsigns of peri-implantitis and the fate of two of these ITI implantswas considered questionable. There was no statistically significantdifference for failures after three years of function between implantsystems (Table 4).
Brånemark Mark IV TiUnite versus Southern (SouthernImplants) regular implants
One trial with a parallel group design compared non-submergednarrow diameter implants with roughened surfaces (Brånemark Mark IV TiUnite (Figure 18) versus Southern screws (Figure 45) forthe treatment of totally edentulous maxillae using three unsplintedimplants supporting an overdenture for one year (Payne 2004).Maxillae were treated with either a ridge expansion osteotomy ora combined ridge split and osteotomy procedure, depending onthe ridge bucco-palatal width. Autogenous bone grafts were usedto fill intraosseous defects of the ridge split-cases. The implantswere early loaded 12 weeks after placement. Twenty participantswere included in each group. It is unclear whether important base-line differences existed between the two groups. Two participantsdropped out: one from the Brånemark group (only one implant ofthree could be placed) and one from the Southern group (death).Fifteen implants failed in 11 participants (five Brånemark and 10Southern implants). There was no statistically significant differ-ence for failure between the implant systems after one year of func-tion (Table 4).
IMZ titanium TPS versus ITI TPS hollow implants
One trial with a parallel group design compared two submergedIMZ TPS cylinders (Figure 31) versus two non-submerged ITI
TPS hollow screws (Figure 35) supporting overdentures in edentu-lous mandibles for 10 years (Batenburg 1998). Thirty participantswere included in each group. There were no baseline differencesfor sex, mean edentulous period, mandibular bone quantity andheight between the two groups. Two participants from the ITIgroup died, one prior to the one-year examination and the otherprior to the three-year examination. At the five-year examination,one additional participant of the ITI group was ill and could notattend the examination and one participant in the IMZ groupdied between the 5-year and 10-year follow-up. One IMZ implantfailed prior to the abutment connection operation while anotherthree IMZ implants failed for peri-implantitis between years sevenand 10. There was no statistically significant difference for failuresafter 10 years of function (Table 4).
IMZ titanium TPS versus ITI TPS solid implants
One trial with a parallel group design compared two non-sub-merged IMZ TPS cylinders (Figure 33) versus two non-submergedITI TPS solid screws (Figure 31) supporting overdentures in eden-tulous mandibles for five years (Heydenrijk 2002). Twenty partic-ipants were included in each group. It was unclear whether therewere any baseline differences for the two groups. Two participantsdropped out from ITI group (one died before the three-year fol-low-up and the other become ill after the three-year follow-up),and one from the IMZ group (moved abroad after the three-yearfollow-up). One IMZ implant failed (late failure). There was nostatistically significant difference for failures between the implantsystems after five years of function (Table 4).
ITI SLA versus Southern implants
One trial with a parallel group design compared two unsplintednon-submerged ITI SLA screws (Figure 33) versus two unsplintednon-submerged Southern screws (Figure 45) in totally edentulousmandibles supporting overdentures for 10 years (Payne 2003). Im-plants were early loaded two weeks after placement. Twelve par-ticipants were included in each group. There were no baseline dif-ferences for age, number of years edentulous, number of previousdentures, bone quality and quantity between the two groups. Oneparticipant dropped out from the ITI group and two participantsdied. From the Southern group, one participant dropped out andtwo died at the 10-year point. No implants failed and there was nostatistically significant difference for marginal bone level changes10 year after loading (Table 4).
ITI SLA titanium implants versus SwissPlus (Zimmer)cylindrical implants
One trial with a parallel group design compared two non-sub-merged ITI (Figure 36) versus two non-submerged SwissPlus im-plants (Figure 53) placed in the intraforaminal region supportingoverdentures in the edentulous mandible for five years (Akoglu
48Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2011). Twelve participants were included in each group. It is un-clear whether important baseline differences existed between thetwo groups. The implants were early loaded eight weeks after place-ment. There were no drop-outs or failures.
NobelReplace Select Tapered versus NobelReplace Groovyimplants
One trial with a parallel group design compared single NobelRe-place Select tapered (Figure 25) versus single NobelReplace Groovyimplants (Figure 23) for one year (den Hartog 2011). We ex-cluded a third group of 31 participants treated with NobelPerfectGroovy because implants were placed more supracrestally, makingthe comparison unreliable. Thirty-one participants were includedin each group. There were no baseline differences for age, implantlocation and whether or not a pre-implant augmentation proce-dure was required between the two groups. One NobelReplaceSelect implant failed five months after placement (Table 4). Therewas no statistically significant difference for marginal bone levelchanges (Table 4).
Southern regular versus Steri-Oss implants
Two trials with a parallel group design compared non-submergedSouthern (Figure 45) versus non-submerged Steri-Oss screws(Figure 51) for the treatment of totally edentulous mandibles usingtwo unsplinted implants supporting an overdenture (Tawse-Smith2001; Tawse-Smith 2002). The design of the two trials was identi-cal with the exception that in one trial the implants were conven-tionally loaded at 12 weeks (Tawse-Smith 2001), whereas in theother the implants were early loaded at six weeks (Tawse-Smith2002). In both trials, Steri-Oss implants were described as hav-ing a turned surface, but after having analysed the surface of oneimplant, kindly provided by the authors, it was realised that theimplant surface was chemically treated.One trial with a parallel group design included 12 participantsin each of the two groups followed up to 10 years (conventionalloading at 12 weeks) (Tawse-Smith 2001). There were no baselinedifferences in bone quality and quantity between the two groups.There were four drop-outs over a 10-year period: three in the Steri-Oss group (two drop-outs and one death) and one in the Southerngroup (death). There was one early implant failure in the Steri-Ossgroup. There was no statistically significant difference for failuresbetween the implant systems after 10 years of function (Analysis2.1; Analysis 2.2; Analysis 2.3; Analysis 2.4).The other trial with a parallel group design included 12 partici-pants in each group followed up to 10 years (early loading at sixweeks) (Tawse-Smith 2002). There were no baseline differencesin bone quality and quantity between the two groups. There weretwo drop-outs over a 10-year period in the Steri-Oss group andthree participants died in the Southern group. Five participants inthe Steri-Oss group had seven early failures. No implant was lost
in the Southern group. Most of the failed implants were placedby one surgeon who only placed some Steri-Oss implants. Therewas no statistically significant difference for failures between theimplant systems after 10 years of function (Analysis 2.1; Analysis2.2; Analysis 2.3; Analysis 2.4).We performed meta-analyses of the two above studies (Tawse-Smith 2001; Tawse-Smith 2002). There were no statistically sig-nificant differences for implant failures (Analysis 2.1; Analysis 2.2;Analysis 2.3; Analysis 2.4); however, the CI indicated Southernimplants failed from 10% more up to 98% less than Steri-Ossimplants at each follow-up to 10 years after function (P value =0.06; risk ratio (RR) 0.14; 95% CI 0.02 to 1.10 at 10 years).
Southern regular versus turned Neoss implants
One trial with a parallel group design (Alsabeeha 2011) compareda single non-submerged Southern regular (Figure 45) versus Neossimplants (Figure 42) placed in the midline for the treatment oftotally edentulous mandibles supporting an overdenture for oneyear. Twelve participants were included in each group. No baselinedifferences for age, number of years being edentulous, numberof previous dentures, bone quality and quantity between the twogroups. One participant dropped out from the Southern group.One implant failed in the Southern group. There was no statisti-cally significant difference for implant failures (Table 4).
Southern wide versus turned Neoss implants
One trial with a parallel group design compared non-submergedSouthern wide (Figure 46) versus Neoss implants (Figure 42) forthe treatment of totally edentulous mandibles using a single im-plant placed in the midline supporting an overdenture for oneyear (Alsabeeha 2011). Twelve participants were included in eachgroup. There were no baseline differences for age, number of yearsbeing edentulous, number of previous dentures, bone quality andbone quantity between the two groups. There were no drop-outsor failures.
Southern regular versus Southern wide
One trial with a parallel group design compared non-submergedSouthern regular (Figure 45) versus Southern wide implants(Figure 46) for the treatment of totally edentulous mandibles usinga single implant placed in the midline supporting an overdenturefor one year (Alsabeeha 2011). Twelve participants were includedin each group. There were no baseline differences for age, num-ber of years being edentulous, number of previous dentures, bonequality and bone quantity between the two groups. One partici-pant dropped out from the Southern regular group. One implantfailed in the Southern regular group. There was no statisticallysignificant difference for implant failures (Table 4).
49Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Secondary objectives
Turned versus roughened surfaces
Early implant failure
Seven studies provided data for early implant failure (Batenburg1998; Astrand 1999; Moberg 2001; Astrand 2002; Wennström2004; Fröberg 2006; Schincaglia 2007). All these trials, with oneexception in which there were no failures (Fröberg 2006), showedat least one early failure of implants with a turned surface ver-sus no or few failures for implants with roughened surfaces. Themeta-analysis comparing early implant failures between variousimplants with turned and roughened surfaces demonstrated noheterogeneity (RR 2.79; 95% CI 0.87 to 8.90; P value = 0.08)(Analysis 3.1). The CI for this relative failure rate went from theroughened surfaces failure rate being only 10% worse than theturned surfaces to being up to nine times better.
Peri-implantitis
At three years (four trials)
One meta-analysis comparing the occurrence of peri-implantitisbetween various implants with turned and roughened surfacesat three years included four trials (Analysis 3.2) (Astrand 1999;
Moberg 2001; Astrand 2002; Schincaglia 2007). Considering theparticipant as the unit for the analysis, there was evidence that moreimplants with rough surfaces were affected by peri-implantitis (RR0.80; 95% CI 0.67 to 0.96; P value = 0.01). Implants with turnedsurfaces had a 20% reduction in risk of being affected by peri-implantitis. For the other trial, no data were presented and theauthors did not reply to our request for information (Batenburg1998).
At five years (one trial)
Only one trial was available comparing the occurrence of peri-implantitis between various implants with turned and roughenedsurfaces at five years (Astrand 1999). There was no statistically sig-nificant difference for the occurrence of peri-implantitis betweenthe implants with turned and roughened surfaces (Table 5). Foranother trial, no data were presented and the author did not replyto our request for information (Batenburg 1998).
At 10 years (one trial)
One trial with a parallel group design reported the number ofparticipants who had lost implants because of peri-implantitis be-tween implants with turned and roughened surfaces at 10 years(Batenburg 1998). There was no statistically significant differencefor implant lost for peri-implantitis between the implants withturned and roughened surfaces (Table 5).
50Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

AD
DI
TI
ON
AL
SU
MM
AR
YO
FF
IN
DI
NG
S[E
xpla
nat
ion
]
Turned
implantscomparedwith
roughenedimplantsforearlyimplantfailureandperi-implantitis
Patientorpopulation:adultswithmissingteeth
Settings:dentalclinics
Intervention:turnedimplants
Com
parison:roughenedimplants
Outcomes
Illustrativecomparativerisks*(95%
CI)
Relativeeffect
(95%
CI)
Noofparticipants
(studies)
Qualityoftheevidence
(GRADE)
Com
ments
Assum
edrisk
Corresponding
risk
Roughened
implants
Turned
implants
Earlyimplantfailure
50per1000
140per1000
(44to445)
RR2.79
(0.87to8.90)
285
(6)
⊕⊕
⃝⃝
low
1,2
-
Peri-implantitis
50per1000
40per1000
(34to48)
RR0.80
(0.67to0.96)
144
(4)
⊕⊕
⃝⃝
low
2,3
-
*The
basisfortheassumed
risk(e.g.themediancontrolgroupriskacross
studies)isprovided
infootnotes.Thecorrespondingrisk(and
its95%confidence
interval)isbasedon
the
assumedriskinthecomparison
groupandtherelativeeffectoftheintervention(andits95%CI).
CI:confidenceinterval;RR:riskratio.
GRADEWorkingGroupgradesofevidence
Highquality:Furtherresearchisveryunlikelytochangeourconfidenceintheestimateofeffect.
Moderatequality:Furtherresearchislikelytohaveanimportantimpactonourconfidenceintheestimateofeffectandmaychangetheestimate.
Lowquality:Furtherresearchisverylikelytohaveanimportantimpactonourconfidenceintheestimateofeffectandislikelytochangetheestimate.
Verylowquality:Weareveryuncertainabouttheestimate.
1Downgradedas4studiesathighriskofbiasand2unclear.
2Downgradedforimprecision(lowsamplesize/eventrates).
3Downgradedas3studiesathighriskofbiasand1unclear.
51Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D I S C U S S I O N
Summary of main results
In order to evaluate the possible effects of different implant char-acteristics, a trial should be designed in a way that only the charac-teristic of interest (i.e. surface roughness or implant shape or im-plant material) is different and all the other parameters are iden-tical. Trials evaluated the following comparisons.
Different implant surfaces
Six trials evaluated the potential effect of different implant surfaces,with only two trials comparing the same surfaces. There was noevidence to suggest that one implant surface had a lower failurerate or led to lower marginal bone changes than another.
Different implant shapes
Seven trials evaluated the potential effect of 13 different implantshapes, with no trials comparing the same shapes. After one year,no significant differences for implant failures between the testeddifferent implant designs were observed. The only statistical sig-nificant difference observed regarded one trial comparing peri-im-plant marginal bone loss at Nobel Speedy Groovy implants withNobelActive implants, which showed that Nobel Speedy Groovyimplants lost 0.59 mm more bone than NobelActive implants oneyear after loading (Pozzi 2014),
Different implant materials
Only one trial compared implants made of two different materials:titanium grade 4 versus a titanium-13zirconium alloy (Roxolid),but there was no difference in failure rate or bone loss (Al-Nawas2012).
Different implant systems
Thirteen trials compared different implant systems with a com-bination of different surface characteristics, shapes, dimensions,purity of titanium, surgical protocols (submerged versus non-sub-merged etc.). There was no evidence to suggest that one implantsystem led to fewer implant failures or less bone loss than anotherimplant system.
Early failures between implants with turned and
roughened surfaces
Seven trials compared early implant failures between implants withturned and roughened surfaces. Although not statistically signifi-cant, the limits of the confidence interval from the meta-analysiswent from the turned surfaces being 10% worse than the rough-ened surfaces to being nine times better.
Occurrence of peri-implantitis between implants with
turned and roughened surfaces
Four trials presented data on the occurrence of peri-implantitisbetween implants with turned and roughened surfaces at threeyears after loading, one at five years, and one trial provided theinformation of how many implants failed for peri-implantitis upto 10 years after loading. At three years, the meta-analysis showedthat implants with turned surfaces had a 20% reduction in risk ofbeing affected by peri-implantitis; however, the five-year and 10-year data did not show any evidence of a difference.
Overall completeness and applicability ofevidence
There was insufficient evidence to draw any useful conclusions, asmost of the trials were underpowered. The generalisation of theresults of the included trials to ordinary clinical conditions shouldbe considered with caution. In general, treatments were adminis-tered by experienced clinicians and the follow-up regimens werestrict. It is unlikely that dentists with non-comparable experiencecould match similar positive results. The observation that the in-clusion of a less trained surgeon might have influenced the resultof one trial support this suggestion (Tawse-Smith 2002).
Quality of the evidence
The most striking aspect is that only 27 out of 81 identified ran-domised controlled trials (RCTs) could be included in the presentreview. This was due to several problems, the most common be-ing: studies were not RCTs or were quasi-random trials, data werepresented in a way we could not use or insufficient data were pre-sented, too short follow-up (less than one year after loading), lackof proper assessment of the primary outcome measure (stabilityof individual implants), study discontinuation or evaluating im-plants for other application (orthodontics). In addition, peri-im-plant bone level change data of many included trials could notbe used because they were not recorded from the proper baseline(implant placement) but at later stages (loading) when a substan-tial portion of bone loss already occurred or because they werepresented at implant level and not participant level. In a previousinvestigation, it was found that the design, analysis and reportingof RCTs on oral implants was generally poor (Esposito 2001a),which may explain why so many trials had to be excluded fromthe present review.The quality assessment of the included trials is summarised inFigure 56 and Figure 57. Figure 56 represents a summary of theoverall judgement of the risk of bias, which tries to quantify thepotential risk of bias of the included trials, whereas Figure 57describes our judgement about each of the six risk of bias domainsfor each included study. We assessed only two trials as being at
52Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

low risk of bias (Esposito 2012; Esposito 2013a), assessed 15 as athigh risk of bias.The source of study funding, in particular when trials were spon-sored by implant manufacturers, is a potential source of bias. Fif-teen (58%) out of 27 included trials reported that they were com-mercially funded. It is possible that there could be bias in thisarea. However, these studies would probably not have taken placeunless there was commercial funding and is difficult to evaluatethis aspect objectively. Ideally, independent studies should be con-ducted. We did not classify trials sponsored by manufacturers asunclear risk of bias when they compared their own different im-plant types, even though there might be a tendency of overesti-mating the outcome of the new implants type.The primary outcome measure in this review was the success of theimplants, both from a biological (successful osseointegration andlack of infection) and a biomechanical (no fracture or deformationrendering the implant useless) point of view. In order to ascertainin a reliable way if an implant is clinically osseointegrated, itsstability ought to be evaluated with the prosthesis removed (withthe exception of single implants) otherwise implant failures canbe underestimated (Gröndahl 1997). Here the decision was toexclude those trials in which individual implant stability was nottested after removing the prostheses.The assessment of radiographic bone level changes around im-plants is a secondary or surrogate or predictive outcome measurethat is commonly used. A predictive outcome can be defined as ameasure of the disease process. Predictive outcome measures can-not be recommended as primary parameters to evaluate effective-ness of dental implants; however, they may be useful diagnostictools for the early detection of potential problems, allowing earlytreatment to preserve healthy conditions (Esposito 2001b). Pri-mary or true outcomes such as implant failures are often rare anddistant events, whereas, surrogate endpoints are in general sensi-tive predictors for the true outcomes. The problem of using meanmarginal bone level assessments is that a severe marginal bone lossaffecting few implants is diluted by the averaging process. In ad-dition, once an implant has failed, its values are removed from thecalculations, suddenly improving the bone level measurements.These limitations of the mean marginal bone level measurementsmay delay an early detection of a statistically significant difference.One possible way to overcome this problem is to dichotomise thebone level measurements, establishing an arbitrary threshold levelof severe bone loss (for instance 5 mm), and to count how manyparticipants had at least one implant affected by such severe boneloss. Implants that failed because of progressive bone loss shouldremain in the bone change calculations, even though it is rarelyperformed in practice.In this review update, we decided to include only those radio-graphic assessments that presented radiographs taken at implantplacement as baseline data in order to evaluate more appropriatelythe bone level changes at different implant types, since most ofthe bone resorption occurs just after implant placement/loading.
We excluded one trial (Tymstra 2011), and only partially includedanother (den Hartog 2011), because similar implants with differ-ent shapes were systematically placed at different levels with re-spect to the bone crest. In addition, bone levels measurements weretaken using different reference points when the same referencepoint could have been used. While authors followed the manu-facturer guidelines for placing the implants, the different implantpositions are likely to effect marginal bone level changes. The aimof this review was to evaluate the possible effect of different im-plant characteristics. To achieve this it is imperative that, wheneverpossible, implants are placed in a similar position to exclude allother possible confounding factors. The excluded trials reportedstatistically more bone loss one year after loading at NobelPer-fect Groovy implants of 0.8 mm (den Hartog 2011) and 1.8 mm(Tymstra 2011).Investigators should design studies carefully deciding on either aparallel group or a split-mouth design on outset, not combiningthe two different study designs in the same study. Split-mouthstudies should ideally have equal numbers of implants in eachgroup placed per participant. The analysis of these studies shouldbe a ’paired’ analysis, taking the pairing of the implants withinparticipants into account. Another commonly encountered prob-lem is that both split-mouth and parallel group studies are anal-ysed at the level of the implant, not taking the clustering of theimplants within a participant into account. Finally, the data of thetwo different groups should be reported separately and compared,and the data should not be combined in a single group. The de-sign and analysis of these studies is frequently complex and it isrecommended that statisticians are involved in the initial planningstages and protocol writing for these studies.None of the trial authors characterised the implant surfaces them-selves. This is understandable since they relied on the informa-tion provided by the manufacturers or published in other studies.However, after having analysed the surface of some implants, werealised that the surface description of the Steri-Oss implants re-ported in two trials did not correspond to what we actually found(Tawse-Smith 2001; Tawse-Smith 2002). In fact, the surface wasacid-etched and not turned as described in the articles. Such a find-ing was indeed unexpected. In experimental research, it is recom-mended that authors characterise in detail the surface propertiesof their implants. We feel that the same recommendation couldbe given for clinical trials where the implant characteristics couldbe described in detail and possibly independently verified.
Potential biases in the review process
One of the review authors was an author on two included andone excluded trial. We ensured that other review authors indepen-dently undertook the risk of bias for these trials.
53Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Agreements and disagreements with otherstudies or reviews
We identified no other systematic reviews with similar objectivesand methodology.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Based on the results of the included randomised controlled trials(RCTs), there was no evidence showing that any particular type ofdental implant has superior long-term success over another type ofimplant. There was limited evidence showing that implants withrelatively smooth (turned) surfaces are less prone to lose bone dueto chronic infection (peri-implantitis) than implants with muchrougher surfaces (titanium-plasma-sprayed). These findings werebased on several RCTs, often at high risk of bias, with few partic-ipants and relatively short follow-up periods.
Implications for research
More well-designed, long-term RCTs are required to understandif there is any design, surface modification or material able to im-prove the effectiveness of oral implants significantly. It is recom-mended that such trials include:
• test and control implants placed in the same way whenpossible;
• a sufficient number of participants to disclose a truedifference, if any;
• a proper group allocation concealment;
• independent outcome assessors when blinding is notpossible to minimise detection bias;
• a sufficient duration (five years or more).
Such trials should be reported according to the Consolidated Stan-dards of Reporting Trials (CONSORT) guidelines (www.consort-statement.org). Ideally, these trials should investigate only one as-pect, such as the role of various degrees of surface roughness orthe role of calcium-phosphate coatings, or some specific implantdesign or materials thus minimising the numerous confoundingfactors such as different implant shapes or clinical procedures.
A C K N O W L E D G E M E N T S
We want to thank:
• Paul Coulthard, Maria Gabriella Grusovin, AsbjornJokstad, Lawrence Murray-Curtis and Peter Thomsen for thecontribution they gave to earlier versions of this review;
• Anne Littlewood (Cochrane Oral Health Group) for herassistance with literature searching;
• Luisa Fernandez Mauleffinch and Phil Riley (CochraneOral Health Group) for their help with the preparation of thisreview;
• Bilal Al-Nawas, Per Åstrand, Kurt Bütow, RobertoCalandriello, Luigi Canullo, Murat Cehreli, Laurens denHartog, Bertil Friberg, Klaus Gotfredsen, Susanne Heberer,Marjorie Jeffcoat, Cuneyt Karabuba, Pentti Kemppainen, AndrejM. Kielbassa, Niklaus Lang, Edwin McGlumphy, AntonioFernando Martorelli de Lima, Henny Meijer, Ik-Sang Moon,Yasemin Kulak Ozkan, Alan Payne, Gerry Raghoebar, MarioRoccuzzo, Gian Pietro Schincaglia, Andreas Stavropoulos,Andrew Tawse-Smith and Nele Van Assche for providing us withinformation on their trials;
• Ian Brook, Jan Clarkson, Laurens den Hartog, BertilFriberg, Sue Furness, Anne-Marie Glenny, Jayne Harrison, LeeHooper, Andrej M. Kielbassa, Klaus Lang, Ian Needleman, AlanPayne, Gerry Raghoebar, Gian Pietro Schincaglia, William Shaw,Michele Nieri and Andreas Stavropoulos for reviewing variousversions of this review.
54Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Akoglu 2011 {published data only}
Akoglu B, Ucankale M, Ozkan Y, Kulak-Ozkan Y. Five-year treatment outcomes with three brands of implantsupporting mandibular overdentures. International Journalof Oral and Maxillofacial Implants 2011;26(1):188–94.
Al-Nawas 2012 {published data only}Al-Nawas B, Bragger U, Meijer HJA, Naert I, Persson R,Perucchi A, et al. A double-blind randomized controlledtrial (RCT) of Titanium-13Zircomium versus TitaniumGrade IV small-diameter bone level implants in edentulousmandible - results from a 1-year observation period. Clinical
Implant Dentistry and Related Research 2012;14(6):896–904.
Alsabeeha 2011 {published data only}
Alsabeeha NH, Payne AG, De Silva RK, Murray ThomsonW. Mandibular single-implant overdentures: preliminaryresults of a randomised control trial on early loadingwith different implant diameters and attachment systems.Clinical Oral Implants Research 2011;22(3):330–7.
Astrand 1999 {published and unpublished data}
Engquist B, Åstrand P, Dahlgren S, Engquist E, FeldmannH, Gröndahl K. Astra Tech and Brånemark system implants- a prospective comparative study. Clinical Oral ImplantsResearch 2000;11(4):385 (Abs No 3).Engquist B, Åstrand P, Dahlgren S, Engquist E, FeldmannH, Gröndahl K. Marginal bone reaction to oral implants: aprospective comparative study of Astra Tech and BrånemarkSystem implants. Clinical Oral Implants Research 2002;13(1):30–7.∗ Åstrand P, Engquist B, Dahlgren S, Engquist E, FeldmannH, Gröndahl K. Astra Tech and Brånemark Systemimplants: a prospective 5-year comparative study. Resultsafter one year. Clinical Implant Dentistry and RelatedResearch 1999;1(1):17–26.Åstrand P, Engquist B, Dahlgren S, Gröndahl K, Engquist E,Feldmann H. Astra Tech and Brånemark system implants:a 5-year prospective study of marginal bone reactions.Clinical Oral Implants Research 2004;15(4):413–20.
Astrand 2002 {published and unpublished data}∗ Åstrand P, Engquist B, Anzen B, Bergendal T, Hallman M,Karlsson U, et al. Nonsubmerged and submerged implantsin the treatment of partially edentulous maxilla. Clinical
Implant Dentistry and Related Research 2002;4(3):115–27.Åstrand P, Engquist B, Anzén B, Bergendal T, HallmanM, Karlsson U, et al. A three-year follow-up report of acomparative study of ITI dental implants and Brånemarksystem implants in the treatment of the partially edentulousmaxilla. Clinical Implant Dentistry and Related Research
2004;6(3):130–41.
Batenburg 1998 {published and unpublished data}∗ Batenburg RH, Meijer HJ, Raghoebar GM, Van OortRP, Boering G. Mandibular overdentures supported bytwo Brånemark, IMZ or ITI implants. A prospective
comparative preliminary study: one-year results. ClinicalOral Implants Research 1998;9(6):374–83.Meijer HJ, Batenburg RH, Raghoebar GM, Vissink A.Mandibular overdentures supported by two Brånemark,IMZ or ITI implants: a 5-year prospective study. Journal ofClinical Periodontology 2004;31(7):522–6.Meijer HJ, Raghoebar GM, Batenburg RH, Vissink A.Mandibular overdentures supported by two Branemark,IMZ or ITI implants: a ten-year prospective randomizedstudy. Journal of Clinical Periodontology 2009;36(9):799–806.
Crespi 2009 {published data only}
Crespi R, Capparé P, Gherlone E. Radiographic evaluationof marginal bone levels around platform-switched andnon-platform-switched implants used in an immediateloading protocol. International Journal of Oral Maxillofacial
Implants 2009;24(5):920–6.
den Hartog 2011 {published and unpublished data}
den Hartog L, Meijer HJA, Stegenga B, Tymstra N, VissinkA, Raghoebar GM. Single implants with different neckdesigns in the aesthetic zone: a randomized clinical trial.Clinical Oral Implants Research 2011;22(11):1289–97.
Esposito 2012 {published and unpublished data}Esposito M, Grusovin MG, Pellegrino G, Soardi E, Felice P.Safety and effectiveness of maxillary early loaded titaniumimplants with a novel nanostructured calcium-incorporatedsurface (Xpeed): 1-year results from a pilot multicenterrandomised controlled trial. European Journal of Oral
Implantology 2012;5(3):241–9.
Esposito 2013a {published and unpublished data}
Esposito M, Dojcinovic I, Germon L, Levy N, CurnoR, Buchini S, et al. Safety and efficacy of a biomimeticmonolayer of permanently bound multi-phosphonic acidmolecules on dental implants: 1 year post-loading resultsfrom a pilot quadruple-blinded randomised controlled trial.European Journal of Oral Implantology 2013;6(3):227–36.
Fröberg 2006 {published data only}
Fröberg KK, Lindh C, Ericsson I. Immediate loadingof Brånemark System Implants: a comparison betweenTiUnite and turned implants placed in the anteriormandible. Clinical Implant Dentistry and Related Research
2006;8(4):187–97.
Gatti 2002 {published and unpublished data}
Gatti C, Chiapasco M. Immediate loading of Brånemarkimplants: a 24-month follow-up of a comparativeprospective pilot study between mandibular overdenturessupported by conical transmucosal and standard MK IIimplants. Clinical Implant Dentistry and Related Research2002;4(4):190–9.
Heberer 2011 {published and unpublished data}
Heberer S, Kilic S, Hossamo J, Raguse JD, Nelson K.Rehabilitation of irradiated patients with modified andconventional sandblasted acid-etched implants: preliminary
55Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

results of a split-mouth study. Clinical Oral Implants research
2011;22(5):546–51.
Heydenrijk 2002 {published data only}Heijdenrijk K, Raghoebar GM, Meijer HJ, Stegenga B, vander Reijden WA. Feasibility and influence of the microgapof two implants placed in a non-submerged procedure: afive-year follow-up clinical trial. Journal of Periodontology2006;77(6):1051–60.Heydenrijk K, Raghoebar GM, Meijer HJ, Stegenga B.Clinical and radiologic evaluation of 2-stage IMZ implantsplaced in a single-stage procedure: 2-year results of aprospective comparative study. International Journal of Oral
and Maxillofacial Implants 2003;18(3):424–32.∗ Heydenrijk K, Raghoebar GM, Meijer HJ, van derReijden WA, van Winkelhoff AJ, Stegenga B. Two-stageIMZ implants and ITI implants inserted in a single-stageprocedure. Clinical Oral Implants Research 2002;13(4):371–80.Meijer HJ, Heijdenrijk K, Raghoebar GM. Mucosal andradiographic aspects during the healing period of implantsplaced in a one-stage procedure. International Journal ofProsthodontics 2003;16(4):397–402.
Kielbassa 2009 {published and unpublished data}Arnhart C, Kielbassa AM, Martinez-de-Fuentes R,Goldstein M, Jackowski J, Lorenzoni M, et al. Comparisonof variable-thread tapered implant designs to a standardtapered implant design after immediate loading. A 3-yearmulticentre randomised controlled trial. European Journal
of Oral Implantology 2012;5(2):1–14.∗ Kielbassa AM, Martinez-de Fuentes R, Goldstein M,Arnhart C, Barlattani A, Jackowski J, et al. Randomizedcontrolled trial comparing a variable-thread novel taperedand a standard tapered implant: interim one-year results.Journal of Prosthetic Dentistry 2009;101(5):293–305.
Lang 2007 {published and unpublished data}
Lang N, Tonetti MS, Suvan JE, Bernard JP, BotticelliD, Fourmousis I, et al. Immediate implant placementwith transmucosal healing in areas of aesthetic priority. Amulticentre randomized-controlled clinical trial I. Surgicaloutcomes. Clinical Oral Implants Research 2007;18(2):188–96.
Lee 2007 {published data only}
Lee DW, Choi YS, Park KH, Kim CS, Moon IS. Effect ofmicrothread on the maintenance of marginal bone level: a3-year prospective study. Clinical Oral Implants Research2007;18(4):465–70.
Moberg 2001 {published data only}
Moberg LE, Köndell PÅ, Sagulin GB, Bolin A, HeimdahlA, Gynther GW. Brånemark System and ITI DentalImplant System for treatment of mandibular edentulism. Acomparative randomized study: 3-year follow-up. Clinical
Oral Implants Research 2001;12(5):450–61.
Payne 2003 {published and unpublished data}
Ma S, Tawse-Smith A, Thomson WM, Payne AG. Marginalbone loss with mandibular two-implant overdentures usingdifferent loading protocols and attachment systems: 10-year
outcomes. International Journal of Prosthodontics 2010;23(4):321–32.∗ Payne AG, Twase-Smith A, Thomson WM, Kumara R.Early functional loading of unsplinted roughened surfaceimplants with mandibular overdentures 2 weeks aftersurgery. Clinical Implant Dentistry and Related Research2003;5(3):143–53.
Payne 2004 {published data only}
Payne AGT, Tawse-Smith A, Thomson WM, DuncanWD, Kumara R. One-stage surgery and early loading ofthree implants for maxillary overdentures: a 1-year report.Clinical Implant Dentistry and Related Research 2004;6(2):1–14.
Pozzi 2014 {published data only}Pozzi A, Agliardi E, Tallarico M, Barlattani A. Clinicaland radiological outcomes of two implants with differentprosthetic interfaces and neck configurations: randomized,controlled, split-mouth clinical trial. Clinical ImplantDentistry and Related Research 2014;16(1):96–106.
Prosper 2009 {published data only}Prosper L, Radaelli S, Pasi M, Zarone F, Radaelli G,Gherlone E. A randomized prospective multicenter trialevaluating the platform-switching technique for theprevention of postrestorative crestal bone loss. InternationalJournal of Oral Maxillofacial Implants 2009;24(2):299–308.
Schincaglia 2007 {published data only}
Fung K, Marzola R, Scotti R, Tadinada A, SchincagliaGP. A 36-month randomized controlled split-mouth trialcomparing immediately loaded titanium oxide-anodizedand machined implants supporting fixed partial dentures inthe posterior mandible. International Journal of Oral andMaxillofacial Implants 2011;26(3):631–8.∗ Schincaglia GP, Marzola R, Scapoli C, Scotti R. Immediateloading of dental implants supporting fixed partial denturesin the posterior mandible: a randomized controlled split-mouth study. Machined versus titanium oxide implantsurface. International Journal of Oral and MaxillofacialImplants 2007;22(1):35–46.
Song 2009 {published data only}
Song DW, Lee DW, Kim CK, Park KH, Moon IS.Comparative analysis of peri-implant marginal bone lossbased on microthread location: a 1-year prospective studyafter loading. Journal of Periodontology 2009;80(12):1937–44.
Tawse-Smith 2001 {published and unpublished data}Ma S, Tawse-Smith A, Thomson WM, Payne AG. Marginalbone loss with mandibular two-implant overdentures usingdifferent loading protocols and attachment systems: 10-yearoutcomes. International Journal of Prosthodontics 2010;23(4):321–32.∗ Tawse-Smith A, Perio C, Payne AG, Kumara R,Thomson WM. One-stage operative procedure using twodifferent implant systems: a prospective study on implantoverdentures in the edentulous mandible. Clinical Implant
Dentistry and Related Research 2001;3(4):185–93.
56Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tawse-Smith 2002 {published data only}
Ma S, Tawse-Smith A, Thomson WM, Payne AG. Marginalbone loss with mandibular two-implant overdentures usingdifferent loading protocols and attachment systems: 10-yearoutcomes. International Journal of Prosthodontics 2010;23(4):321–32.∗ Tawse-Smith A, Payne AG, Kumara R, ThomsonWM. Early loading on unsplinted implants supportingmandibular overdentures using a one-stage operativeprocedure with two different implant systems: a 2-yearreport. Clinical Implant Dentistry and Related Research
2002;4(1):33–42.
Wennström 2004 {published and unpublished data}Wennström J, Ekestubbe A, Gröndahl K, Karlsson S,Lindhe J. Oral rehabilitation with implant-supported fixedpartial dentures in periodontitis-susceptible subjects. A 5-year prospective study. Journal of Clinical Periodontology2004;31(9):713–24.
References to studies excluded from this review
Abtahi 2012 {published data only}
Abtahi J, Tengvall P, Aspenberg P. A bisphosphonate-coatingimproves the fixation of metal implants in human bone.A randomized trial of dental implants. Bone 2012;50(5):1148–51.
Åstrand 2003 {published data only}Åstrand P, Billström C, Feldmann H, Fischer K, HenricssonV, Johansson B, et al. Tapered implants in jaws with softbone quality: a clinical and radiographic 1-year study ofthe Brånemark System Mark IV fixture. Clinical ImplantDentistry and Related Research 2003;5(4):213–8.
Boerrigter 1997 {published and unpublished data}∗ Boerrigter EM, van Oort RP, Raghoebar GM, Stegenga B,Schoen PJ, Boering G. A controlled clinical trial of implant-retained mandibular overdentures: clinical aspects. Journalof Oral Rehabilitation 1997;24(3):182–90.Meijer HJ, Raghoebar GM, Van’t Hof MA. Comparison ofimplant-retained mandibular overdentures and conventionalcomplete dentures: a 10-year prospective study of clinicalaspects and patient satisfaction. International Journal of Oral
and Maxillofacial Implants 2003;18(6):879–85.Meijer HJ, Raghoebar GM, Van’t Hof MA, Visser A. Acontrolled clinical trial of implant-retained mandibularoverdentures: 10 years’ results of clinical aspects andaftercare of IMZ implants and Branemark implants.Clinical Oral Implants Research 2004;15(4):421–7.Meijer HJ, Raghoebar GM, Van’t Hof MA, Visser A,Geertman ME, Van Oort RP. A controlled clinical trialof implant-retained mandibular overdentures; five-years’results of clinical aspects and aftercare of IMZ implants andBrånemark implants. Clinical Oral Implants Research 2000;11(5):441–7.
Canullo 2012 {published and unpublished data}
Canullo L, Iannello G, Penarrocha M, Garcia B. Impact ofimplant diameter on bone level changes around platformswitched implants: preliminary results of 18 months follow-
up a prospective randomized match-paired controlled trial.Clinical Oral Implants Research 2012;23:1142–6.
Cehreli 2010 {published data only}Cehreli MC, Uysal S, Akca K. Marginal bone level changesand prosthetic maintenance of mandibular overdenturessupported by 2 implants: a 5-year randomized clinical trial.Clinical Implant Dentistry and Related Research 2010;12:114–21.
da Cunha 2004 {published data only}
da Cunha HD, Francischone CE, Filho HN, de OliveiraRC. A comparison between cutting torque and resonancefrequency in the assessment of primary stability and finaltorque capacity of standard and TiUnite single-toothimplants under immediate loading. International Journal ofOral and Maxillofacial Implants 2004;19(4):578–85.
Du Preez 2007 {published data only}Bütow KW, Du Preez LA, Benninghoff W. Comparisonof three different implant system in the same patient: apreliminary report. Journal of Dental Research 2002;81(Special Issue B, Divisional Abstracts):B-372 (Abs No 27).∗ Du Preez LA, Bütow KW, Benninghoff W. A comparisonof three different implant systems in the same patient.International Dentistry (South African Edition) 2007;8:20–6.
Esposito 2013b {published and unpublished data}
Esposito M, Blasone R, Favaretto G, Stacchi C, Calvo M,Marin C, et al. A comparison of two dental implant systemsin partially edentulous patients: 4-month post-loadingresults from a pragmatic multicentre randomised controlledtrial. European Journal of Oral Implantology 2013;6(2):169–79.
Friberg 1992 {published and unpublished data}
Friberg B, Grondahl K, Lekholm U. A new self-tappingBranemark implant: clinical and radiographic evaluation.International Journal of Oral and Maxillofacial Implants1992;7(1):80–5.
Friberg 2003 {published data only}
Friberg B, Jisander S, Widmark G, Lundgren A, Ivanoff CJ,Sennerby L, et al. One-year prospective three-center studycomparing the outcome of a ’soft bone implant’ (prototypeMk IV) and the standard Branemark implant. Clinical
Implant Dentistry and Related Research 2003;5(2):71–7.
Geertman 1996 {published and unpublished data}∗ Geertman ME, Boerrigter EM, Van Waas MA, van OortRP. Clinical aspects of a multicenter clinical trial of implant-retained mandibular overdentures in patients with severelyresorbed mandibles. Journal of Prosthetic Dentistry 1996;75(2):194–204.Geertman ME, Boerrigter EM, van Waas MA, van Oort RP,van’t Hof MA, Kwakman JM, et al. Comparison of dentalimplant systems for mandibular overdentures [in Dutch].Nederlands Tijdschrift voor Tandheelkunde 1998;105(12):447–50.Meijer HJ, Geertman ME, Raghoebar GM, Kwakman JM.Implant-retained mandibular overdentures: 6-year results ofa multicenter clinical trial on 3 different implant systems.
57Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Journal of Oral and Maxillofacial Surgery 2001;59(11):1260–8.Meijer HJA, Geertman ME, Raghoebar GM. Implant-retained mandibular overdentures: a multicenter study ondifferent implant systems. Clinical Oral Implants Research
2000;11(4):394 (Abs No 39).
Geurs 2002 {published data only}∗ Geurs NC, Jeffcoat RL, McGlumphy EA, Reddy MS,Jeffcoat MK. Influence of implant geometry and surfacecharacteristics on progressive osseointegration. InternationalJournal of Oral and Maxillofacial Implants 2002;17(6):811–5.Jeffcoat MK, McGlumphy EA, Reddy MS, Geurs NC,Proskin HM. A comparison of hydroxyapatite (HA) -coatedthreaded, HA-coated cylindrical, and titanium treadedendosseous dental implants. International Journal of Oraland Maxillofacial Implants 2003;18(3):406–10.Jeffcoat MK, McGlumphy EA, Reddy MS, Geurs NC,Proskin HM. Success of hydroxyapatite vs titaniumimplants: 5 years results. Journal of Dental Research 2002;81(Special Issue A):A-38 (Abs No 0074).Jeffcoat RI, McGlumphy EA, Geurs NC, Reddy MS,Jeffcoat MK. Influence of hydroxyapatite implant coatingon Periotest mobility over time. Journal of Dental Research2000;79(Special Issue):603 (Abs No 3671).McGlumphy EA, Peterson LJ, Larsen PE, Eaton JJ. Softtissue measurements changes for three randomly placedimplant types. Journal of Dental Research 2000;79(SpecialIssue):466 (Abs No 2585).Wang I-C, Reddy MS, McGlumphy EA, Jeffcoat MK.Surface coating and endosseous dental implant success(two-year follow-up). Journal of Dental Research 2000;79(Special Issue):467 (Abs No 2585).
Gher 1994 {published data only}
Gher ME, Quintero G, Assad D, Monaco E, RichardsonAC. Bone grafting and guided bone regeneration forimmediate dental implants in humans. Journal ofPeriodontology 1994;65(9):881–91.
Goené 2007 {published data only}Goené RJ, Testori T, Trisi P. Influence of a nanometer-scale surface enhancement on de novo bone formation ontitanium implants: a histomorphometric study in humanmaxillae. International Journal of Periodontics and RestorativeDentistry 2007;27:211–9.
Gultekin 2013 {published and unpublished data}Gultekin BA, Gultekin P, Leblebicioglu B, BasegmezC, Yalcin S. Clinical evaluation of marginal bone lossand stability in two types of submerged dental implants.International Journal of Oral and Maxillofacial Implants2013;28:815–23.
Joly 2003 {published data only}∗ Joly JC, de Lima AF, da Silva RC. Clinical andradiographic evaluation of soft and hard tissue changes
around implants: a pilot study. Journal of Periodontology
2003;74(8):1097–103.Joly JC, de Lima AF, da Silva RC. Clinical and radiographicevaluation of soft- and hard-tissue changes around implants.Journal of Dental Research 2003;82(Special Issue):B-214(Abs No 1621).
Jones 1997 {published data only}
Jones JD, Lupori J, Van Sickels JE, Gardner W. A 5-yearcomparison of hydroxyapatite-coated titanium plasma-sprayed and titanium plasma-sprayed cylinder dentalimplants. Oral Surgery, Oral Medicine, Oral Pathology, Oral
Radiology and Endodontics 1999;87(6):649–52.∗ Jones JD, Saigusa M, Van Sickels JE, Tiner BD, GardnerWA. Clinical evaluation of hydroxyapatite-coated titaniumplasma-sprayed and titanium plasma-sprayed cylinderdental implants: a preliminary report. Oral Surgery, OralMedicine, Oral Pathology, Oral Radiology and Endodontics
1997;84(2):137–41.
Kadkhodazadeh 2013 {published and unpublished data}
Kadkhodazadeh M, Heidari B, Abdi Z, Mollaverdi F, AmidR. Radiographic evaluation of marginal bone levels arounddental implants with different designs after 1 year. ActaOdontologica Scandinavica 2013;71:92–5.
Kang 2012 {published and unpublished data}Kang YI, Lee DW, Park KH, Moon IK. Effect of thread sizeon the implant neck area: preliminary results at 1 year offunction. Clinical Oral Implants Research 2012;23:1147–51.
Karabuda 2002 {published data only}Karabuda C, Tosun T, Ermis E, Ozdemir T. Comparison of2 retentive systems for implant-supported overdentures: softtissue management and evaluation of patient satisfaction.Journal of Periodontology 2002;73(9):1067–70.
Karlsson 1998 {published and unpublished data}
Gotfredsen K, Karlsson U. A prospective 5-year studyof fixed partial prostheses supported by implantswith machined and TiO2-blasted surface. Journal ofProsthodontics 2001;10(1):2–7.∗ Karlsson U, Gotfredsen K, Olsson C. A 2-year report onmaxillary and mandibular fixed partial dentures supportedby Astra Tech dental implants. A comparison of 2 implantswith different surface textures. Clinical Oral Implants
Research 1998;9(4):235–42.
Kemppainen 1997 {published and unpublished data}Kemppainen P, Eskola S, Ylipaavalniemi P. A comparativeprospective clinical study of two single-tooth implants: apreliminary report of 102 implants. Journal of Prosthetic
Dentistry 1997;77(4):382–7.
Khang 2001 {published data only}
Khang W, Feldman S, Hawley CE, Gunsolley J. A multi-center study comparing dual acid-etched and machined-surfaced implants in various bone qualities. Journal ofPeriodontology 2001;72(10):1384–90.
Kim 2010 {published data only}Kim JJ, Lee DW, Kim CK, Park KH, Moon IS. Effectof conical configuration of fixture on the maintenance
58Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

of marginal bone level: preliminary results at 1 year offunction. Clinical Oral Implants Research 2010;21:439–44.
Liaje 2012 {published and unpublished data}Liaje A, Ozkan YK, Ozkan Y, Vanlioglu B. Stability andmarginal bone loss with three types of early loaded implantsduring the first year after loading. International Journal of
Oral and Maxillofacial Implants 2012;27:162–72.
Liddelow 2010 {published data only}
Liddelow G, Henry P. The immediately loaded singleimplant-retained mandibular overdenture: a 36-monthprospective study. International Journal of Prosthodontics2010;23:13–21.
Mackie 2011 {published data only}Mackie A, Lyons K, Thompson WM, Payne AG.Mandibular two-implant overdentures: prosthodonticmaintenance using different loading protocols andattachment systems. International Journal of Prosthodontics2011;24(5):405–16.
Mau 2002 {published data only}∗ Mau J, Behneke A, Behneke N, Fritzemeier CU, Gomez-Roman G, d’Hoedt B, et al. Randomized multicentercomparison of two coatings of intramobile cylinder implantsin 313 partially edentulous mandibles followed up for 5years. Clinical Oral Implants Research 2002;13(5):477–87.Young M, Mau J, Spiekermann H, SPPI Group. Coatingand prognostic factors for implant integration deficiency.Clinical Oral Implants Research 2002;13(4):xviii.
Mau 2003 {published data only}∗ Mau J, Behneke A, Behneke N, Fritzmeier CU, Gomez-Roman G, d’Hoedt B, et al. Randomized multicentercomparison of 2 IMZ and 4 TPS screw implants supportingbar-retained overdentures in 425 edentulous mandibles.International Journal of Oral and Maxillofacial Implants
2003;18(6):835–47.Mau J, Spiekermann H, Yong M, SPPI Study Group.Randomised comparison of 2-IMZ cylinder and 4-TPSscrew implants supporting bar-retained overdentures in340 edentulous mandibles. Clinical Oral Implants Research2000;11(4):394.
Nickenig 2009 {published and unpublished data}
Nickenig A, Wichmann M, Schlegel KA, Nkenke E, EitnerS. Radiographic evaluation of marginal bone levels adjacentto parallel-screw cylinder machined-neck implants andrough-surfaced microthreaded implants using digitizedpanoramic radiographs. Clinical Oral Implants Research2009;20:550–4.
Oates 2007 {published data only}Oates TW, Valderrama P, Bischof M, Nedir R, JonesA, Simpson J, et al. Enhanced implant stability with achemically modified SLA surface: a randomized pilot study.International Journal of Oral and Maxillofacial Implants2007;22:755–60.
Orsini 2007 {published data only}
Orsini G, Piattelli M, Scarano A, Petrone G, KenealyJ, Piattelli A, et al. Randomized, controlled histologicand histomorphometric evaluation of implants with
nanometer-scale calcium phosphate added to the dual acid-etched surface in the human posterior maxilla. Journal ofPeriodontology 2007;78:209–18.
Park 2010 {published data only}
Park JC, Ha SR, Kim SM, Kim MJ, Lee JB, Lee JH. Arandomized clinical 1-year trial comparing two types ofnon-submerged dental implants. Clinical Oral ImplantsResearch 2010;21:228–36.
Peñarrocha-Diago 2012 {published and unpublished data}Peñarrocha-Diago MA, Flichy-Fernández AJ, Alonso-González R, Peñarrocha-Oltra D, Balaguer-Martínez J,Peñarrocha-Diago M. Influence of implant neck design andimplant-abutment connection type on peri-implant health.Radiological study. Clinical Oral Implants Research 2012Aug 28 [Epub ahead of print].
Piao 2009 {published data only}
Lee SY, Piao CM, Koak JY, Kim SK, Ku Y, Rhyu IC. A 3-year prospective radiographic evaluation of marginal bonelevel around different implant systems. Journal of OralRehabilitation 2010;37:538–44.∗ Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH,et al. Marginal bone loss around three different implantsystems: radiographic evaluation after 1 year. Journal ofOral Rehabilitation 2009;36:748–54.
Reingewirtz 2000 {published data only}Reingewirtz Y, Cuisinier F, Senfer B, Tenenbaum H. Tissueresponse in type IV bone of two biocoated implant types.International Dental Journal 2000;50 Suppl(6):341.
Rocci 2003 {published data only}∗ Rocci A, Martignoni M, Gottlow J. Immediate loading ofBranemark System TiUnite and machined-surface implantsin the posterior mandible: a randomized open-endedclinical trial. Clinical Implant Dentistry and Related Research
2003;5 Suppl(1):57–63.Rocci A, Rocci M, Rocci C, Scoccia A, Gargari M,Martignoni M, et al. Immediate loading of BranemarkSystem TiUnite and machined-surface implants in theposterior mandible. Part II: a randomized open-ended 9-year follow-up clinical trial. International Journal of Oral
and Maxillofacial Implants 2013;28(3):891–5.
Roccuzzo 2001 {published and unpublished data}
Roccuzzo M, Aglietta M, Bunino M, Bonino L. Earlyloading of sandblasted and acid-etched implants: arandomized-controlled double-blind split-mouth study.Five-year results. Clinical Oral Implants Research 2008;19:148–52.∗ Roccuzzo M, Bunino M, Prioglio F, Bianchi SD. Earlyloading of sandblasted and acid-etched (SLA) implants: aprospective split-mouth comparative study. Clinical Oral
Implants Research 2001;12(6):572–8.
Sanz 2010 {published data only}
Sanz M, Cecchinato D, Ferrus J, Pjetursson EB, Lang NP,Lindhe J. A prospective, randomized-controlled clinical trialto evaluate bone preservation using implants with differentgeometry placed into extraction sockets in the maxilla.Clinical Oral Implants Research 2010;21:13–21.
59Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schätzle 2009 {published data only}
Schätzle M, Mannchen R, Balbach U, Hämmerle CH,Toutenburg H, Jung RE. Stability change of chemicallymodified sandblasted/acid-etched titanium palatal implants.A randomized-controlled clinical trial. Clinical Oral
Implants Research 2009;20:489–95.
Shibli 2010 {published data only}Shibli JA, Grassi S, Piattelli A, Pecora GE, Ferrari DS,Onuma T, et al. Histomorphometric evaluation ofbioceramic molecular impregnated and dual acid-etchedimplant surfaces in the human posterior maxilla. ClinicalImplant Dentistry and Related Research 2010;12:281–8.
Shin 2006 {published data only}
Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographicevaluation of marginal bone level around implants withdifferent neck designs after 1 year. International Journal ofOral and Maxillofacial Implants 2006;21(5):789–94.
Stavropoulos 2007 {published and unpublished data}
Stavropoulos A, Karring T, Kostopoulos L. Fully vs. partiallyrough implants in maxillary sinus floor augmentation: arandomized-controlled clinical trial. Clinical Oral ImplantsResearch 2007;18(1):95–102.
Tallarico 2011 {published data only}
Tallarico M, Vaccarella A, Marzi GC. Clinical andradiological outcomes of 1-versus 2-stage implantplacement: 1-year results of a randomised clinical trial.European Journal of Oral Implantology 2011;4(1):13–20.
Tan 2010 {published data only}
Tan WC, Lang NK, Schmidlin K, Zwahlen M, PjeturssonBE. The effect of different implant neck configurationson soft and hard tissue healing: a randomized-controlledclinical trial. Clinical Oral Implants Research 2010;22:14–9.
Testori 2003 {published data only}
Testori T, Bianchi F, Del Fabbro M, Szmukler-Moncler S,Francetti L, Weinstein RL. Immediate non-occlusal loadingvs. early loading in partially edentulous patients. PracticalProcedures and Aesthetic Dentistry 2003;15(10):787–94.
Thoma 2014 {published and unpublished data}
Thoma DS, Sanz Martin I, Benic GI, Roos M, HämmerleCHF. Prospective randomized controlled clinical studycomparing two dental implant systems: demographic andradiographic results at one year of loading. Clinical Oral
Implants Research 2014;25(2):142–9.
Tomatis 2002 {unpublished data only}Tomatis M, Calandriello R, Rangert B. Immediate loadingof Branemark implants with two different surfaces. ClinicalOral Implants Research 2002;13(4):xxx.
Truhlar 1997 {published data only}
Manz MC. Factors associated with radiographic verticalbone loss around implants placed in a clinical study. Annals
of Periodontology 2000;5(1):137–51.Manz MC. Radiographic assessment of peri-implant verticalbone loss: DICRG interim report No. 9. Journal of Oraland Maxillofacial Surgery 1997;55(12 Suppl 5):62–71.Morris HF, Manz MC, Tarolli JH. Success of multiple
endosseous dental implant designs to second-stage surgeryacross study sites. Journal of Oral and Maxillofacial Surgery1997;55(12 Suppl 5):76–82.Morris HF, Ochi S. Hydroxyapatite-coated implants: a casefor their use. Journal of Oral and Maxillofacial Surgery 1998;56(11):1303–11.Morris HF, Ochi S. Influence of research center on overallsurvival outcomes at each phase of treatment. Annals ofPeriodontology 2000;5(1):129–36.Morris HF, Ochi S. Influence of two different approachesto reporting implant survival outcomes for five differentprosthodontic applications. Annals of Periodontology 2000;5:90–100.Morris HF, Ochi S. Survival and stability (PTVs) of siximplant designs from placement to 36 months. Annals of
Periodontology 2000;1:15–21.Morris HF, Ochi S, Winkler S. Implant survival in patientswith type 2 diabetes: placement to 36 months. Annals ofPeriodontology 2000;5(1):157–65.Morris HF, Winkler S, Ochi S. A 48-month multicentricclinical investigation: implant design and survival. Journal
of Oral Implantoloy 2001;27(4):180–6.∗ Truhlar RS, Farish SE, Scheitler LE, Morris HF, Ochi S.Bone quality and implant design-related outcomes throughstage II surgical uncovering of Spectra-System root formimplants. Journal of Oral and Maxillofacial Surgery 1997;55(12 Suppl 5):46–54.Truhlar RS, Morris HF, Ochi S. Implant surface coating andbone quality-related survival outcomes through 36 monthspost-placement of root-form endosseous dental implants.Annals of Periodontology 2000;5(1):109–18.Truhlar RS, Morris HF, Ochi S. Stability of the bone-implant complex. Results of longitudinal testing to 60months with the Periotest device on endosseous dentalimplants. Annals of Periodontology 2000;5(1):42–55.
Tymstra 2011 {published data only}Tymstra N, Raghoebar GM, Vissink A, Den Hartog L,Stellingsma K, Meijer HJ. Treatment outcome of twoadjacent implant crowns with different implant platformdesigns in the aesthetic zone: a 1-year randomized clinicaltrial. Journal of Clinical Periodontology 2011;38:74–85.
Van Assche 2012 {published and unpublished data}Nicu EA, Van Assche N, Coucke W. Teughels W, QuirynenM. RCT comparing implants with turned and anodicallyoxidised surfaces: a pilot study, a 3-year follow up. Journal
of Clinical Periodontology 2012;39:1183–90.Quirynen M, Van Assche N. RCT comparing minimallywith moderately rough implants. Part 2: microbialobservations. Clinical Oral Implants Research 2012;23:625–34.∗ Van Assche N, Coucke W, Teughels W, Naert I, CardososMV, Quirynen M. RCT comparing minimally withmoderately rough implants. Part 1: clinical observations.Clinical Oral Implants Research 2012;23:617–24.
Van Steenberghe 2000 {published data only}Joacobs R, Pittayapat P, Van Steenbrghe D, De MarsG, Gijbels F, Van Der Donck A, et al. A split-mouth
60Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

comparative study up to 16 years of two screw-shapedtitanium implant systems. Journal of Clinical Periodontology2010;37:1119–27.Van Assche N, Pittayapat P, Jacobs R, Pauwels M, TeughelsW, Quirynen M. Microbiological outcome of two screw-shaped titanium implant systems, placed following a splitmouth randomised protocol at the 12th year of follow upafter loading. European Journal of Oral Implantology 2011;4(2):103–16.∗ van Steenberghe D, De Mars G, Quirynen M, JacobsR, Naert I. A prospective split-mouth comparative studyof two screw-shaped self-tapping pure titanium implantsystems. Clinical Oral Implants Research 2000;11(3):202–9.
Zetterqvist 2010 {published data only}
Zetterqvist L, Feldman S, Rotter B, Vincenzi G, WennströmJL, Chierico A, et al. A prospective, multicenter,randomized-controlled 5-year study of hybrid and fullyetched implants for the incidence of peri-implantitis.Journal of Periodontology 2010;81:493–501.
References to studies awaiting assessment
Cecchinato 2013 {published data only}
Cecchinato D, Lops D, Salvi GE, Sanz M. A prospective,randomized, controlled study using OsseoSpeedT M
implants placed in maxillary fresh extraction socket: softtissues response. Clinical Oral Implants Research 2013;00:1–8. [DOI: 10.1111/clr.12295]
Dellavia 2013 {published data only}Dellavia C, Canullo L, Allievi C, Lang NP, PellegriniG. Soft tissue surrounding switched platform implants:an immunohistochemical evaluation. Clinical Oral
Implants Research 2013;24(1):63–70. [DOI: 10.1111/j.1600-0501.2011.02301.x]
De Wilde 2013 {published data only}De Wilde EA, Jimbo R, Wennerberg A, Naito Y, Coucke P,Bryington MS, et al. The soft tissue immunologic responseto hydroxyapatite-coated transmucosal implant surfaces: astudy in humans. Clinical Implant Dentistry and RelatedResearch in press.
Enkling 2012 {published data only}
Enkling N, Albrecht D, Gallo N, Dürstler M, Bayer S,Stark H, et al. Equivalent bone-level-alterations at implantswith platform-switching and implants with matching-platforms.. Proceedings of the 90th General Session &Exhibition of the IADR; 2012 June 20-23, 2012; IguaçuFalls, Brazil. Alexandria, VA: International Association forDental Research, 2012:Oral session presentation no. 40.
Ho 2013 {published data only}
Ho DSW, Yeung SCH, Zee KY, Curtis B, Hell P, TumuluriV. Clinical and radiographic evaluation of NobelActiveT M
dental implants. Clinical Oral Implants Research 2013;24(3):297–304.
Osman 2013 {published data only}
Osman RB, Swain MV, Atieh M, Ma S, Duncan W.Ceramic implants (Y-TZP): are they a viable alternative
to titanium implants for the support of overdentures? Arandomized clinical trial. Clinical Oral Implants Researchin press.
Pang 2014 {published data only}Pang KM, Lee JW, Lee JY, Lee JB, Kim SM, Kim MJ,et al. Clinical outcomes of magnesium-incorporatedoxidised implants: a randomised double-blind clinical trial.Clinical Oral Implants Research 2014;25(5):616–21. [DOI:10.1111/clr.12091]
Romanos 2013 {published data only}Romanos GE, Malmstrom H, Feng C, Ercoli C, CatonJ. Immediately loaded platform-switched implants in theanterior mandible with fixed prostheses: a randomized,split-mouth, masked prospective trial. Clinical ImplantDentistry and Related Research 2013 Mar 28 [Epub aheadof print]. [DOI: 10.1111/cid.12065]
Sanz 2013 {published data only}
Sanz M, Cecchinato D, Ferrus J, Salvi GE, Ramseier CA,Lang NP, et al. 3-year clinical trial comparing immediateimplants with different geometry. Proceedings of the 91stGeneral Session & Exhibition of the IADR; 2013 Mar20-23; Seattle, WA, USA. Alexandria, VA: InternationalAssociation for Dental Research, 2013:195.
Sanz 2014 {published data only}Sanz M, Cecchinato D, Ferrus J, Salvi GE, Ramseier C,Lang NP, et al. Implants placed in fresh extraction socketsin the maxilla: clinical and radiographic outcomes from a 3-year follow-up examination. Clinical Oral Implants Research2014;25(3):321–7. [DOI: 10.1111/clr.12140]
Siddiqi 2013 {published data only}
Siddiqi A, Kieser JA, De Silva RK, Thomson WM, DuncanWJ. Soft and hard tissue response to zirconia versus titaniumone-piece implants placed in alveolar and palatal sites:a randomized control trial. Clinical Implant Dentistryand Related Research 2013 Sep 23 [Epub ahead of print].[DOI: 10.1111/cid.12159]
Wang 2014 {published data only}
Wang Y-C, Kan JYK, Rungcharassaeng K, Roe P, LozadaJL. Marginal bone response of implants with platformswitching and non-platform switching abutments inposterior healed sites: a 1-year prospective study. ClinicalOral Implants Research 2014 Jan 3 [Epub ahead of print].[DOI: 10.1111/clr.12312]
Additional references
Binon 2000Binon PP. Implants and components: entering the newmillennium. International Journal of Oral and Maxillofacial
Implants 2000;15(1):76–94.
Brånemark 1977Brånemark PI, Hansson BO, Adell R, Breine U, LindstromJ, Hallen O, et al. Osseointegrated implants in thetreatment of the edentulous jaw. Experience from a 10-yearperiod. Scandinavian Journal of Plastic and ReconstructiveSurgery. Supplementum 1977;16:1–132.
61Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Cawood 1988Cawood JI, Howell RA. A classification of the edentulousjaw. International Journal of Oral and Maxillofacial Surgery
1988;17(4):232–6.
Egger 1997Egger M, Smith GD, Schneider M, Minder C. Bias inmeta-analysis detected by a simple, graphical test. BMJ
1997;315:629–34.
Elbourne 2002Elbourne DR, Altman DG, Higgins JPT, Curtin F,Worthington HV, Vail A. Meta-analyses involving cross-over trials: methodological issues. International Journal of
Epidemiology 2002;31(1):140–9.
Esposito 1997Esposito M, Hirsch, J-M, Lekholm U, Thomsen P. Failurepatterns of four osseointegrated oral implant systems.Journal of Materials Science: Materials in Medicine 1997;8:843–7.
Esposito 1999Esposito M, Hirsch J-M, Lekholm U, Thomsen P.Differential diagnosis and treatment strategies for biologiccomplications and failing oral implants. A review of theliterature. International Journal of Oral and MaxillofacialImplants 1999;14:473–90.
Esposito 2001aEsposito M, Coulthard P, Worthington HV, Jokstad A.Quality assessment of randomized controlled trials of oralimplants. International Journal of Oral and MaxillofacialImplants 2001;16(6):783–92.
Esposito 2001bEsposito M, Worthington HV, Coulthard P. In search oftruth: the role of systematic reviews and meta-analysesfor assessing the effectiveness of rehabilitation with oralimplants. Clinical Implant Dentistry and Related Research
2001;3(2):62–78.
Follmann 1992Follmann D, Elliott P, Suh I, Cutler J. Variance imputationfor overviews of clinical trials with continuous response.Journal of Clinical Epidemiology 1992;45(7):769–73.
Gröndahl 1997Gröndahl K, Lekholm U. The predictive value ofradiographic diagnosis of implant instability. InternationalJournal of Oral and Maxillofacial Implants 1997;12:59–64.
Higgins 2011Higgins JPT, Green S. Cochrane Handbook for SystematicReviews of Interventions Version 5.1.0 [updated March2011]. The Cochrane Collaboration, 2011. Available fromwww.cochrane-handbook.org.
Lekholm 1985Lekholm U, Zarb GA. Patient selection and preparation. In:Branemark PI, Zarb GA, Albrektsson T editor(s). Tissue-Integrated Prostheses. Chicago: Quintessence Publishing Co,Inc., 1985:199–209.
RevMan 2012 [Computer program]The Nordic Cochrane Centre, The Cochrane Collaboration.Review Manager (RevMan). Version 5.2. Copenhagen:The Nordic Cochrane Centre, The Cochrane Collaboration,2012.
Roos-Jansåker 2006Roos-Jansåker AM, Lindahl C, Renvert H, Renvert S.Nine- to fourteen-year follow-up of implant treatment.Part II: presence of peri-implant lesions. Journal of ClinicalPeriodontology 2006;33:290–5.
Stout 1990Stout KJ, Davies EJ, Sullivan PJ. Atlas of Machined Surfaces.London: Chapman and Hall, 1990.
References to other published versions of this review
Esposito 2003Esposito M, Worthington HV, Thomsen P, Coulthard P.Interventions for replacing missing teeth: different types ofdental implants. Cochrane Database of Systematic Reviews
2003, Issue 3. [DOI: 10.1002/14651858.CD003815]
Esposito 2005aEsposito M, Coulthard P, Thomsen P, WorthingtonHV. Interventions for replacing missing teeth: differenttypes of dental implants. Cochrane Database of
Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD003815.pub2]
Esposito 2007Esposito M, Murray-Curtis L, Grusovin MG, CoulthardP, Worthington HV. Interventions for replacing missingteeth: different types of dental implants. Cochrane Databaseof Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD003815.pub3]
∗ Indicates the major publication for the study
62Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Akoglu 2011
Methods 5-year follow-up, randomised parallel group study.
Participants Adults with mandibular edentulism treated with 2 mandibular implants in the in-traforaminal region to support an overdentureTreated in the Department of Oral Surgery and the Department of Prosthetic Dentistry,University of Marmara, Turkey36 enrolled and results given for 36.Exclusion criteria: drug or alcohol abuse, health condition precluding surgery, logisticor physical reasons that could affect followup, psychiatric problems, and a history ofradiotherapy to the head and neck, neoplasia, or bone augmentation to the implant site
Interventions Group 1: Astra® TiO2-blast titanium grade 3 cylindrical screws with internal connection(Astra Tech AB, Mölndal, Sweden).Group 2: ITI® SLA titanium grade 4 cylindrical solid screws with internal connectionwith a 2.8-mm turned neck (Institut Straumann AG, Waldenburg, Switzerland)Group 3: Zimmer SwissPlus sand-blasted acid-etched titanium grade 4 cylindrical screwwith internal connection (Zimmer Dental) supporting overdentures on 2 implants con-nected with ball attachments
Outcomes Implant stability, complications, marginal bone level changes on standardised periapicalradiographs, plaque index, sulcus bleeding index, peri-implant probing depth, peri-implant marginal bone loss, participant satisfaction
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Study reported: “The patients were ran-domly divided into three groups....”Authors did not address this point in theirreply.
Allocation concealment (selection bias) Low risk No information provided in the originalarticle.Authors replied: “Allocation concealmentwas centralised by a central office unawareof subject characteristics; and sequentiallynumbered, sealed, opaque envelopes wereused to inform the surgeon of which im-plant to place at the time of implant place-ment.”
63Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Akoglu 2011 (Continued)
Blinding (performance bias and detectionbias)All outcomes
Unclear risk No information provided in the originalarticle.Authors replied: “Outcome assessors wereblind. Two prosthodontists who were notinvolved in the treatment of the patientsperformed the clinical and radiographicevaluations.”Comment: outcome assessors could not beblinded.
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented and no with-drawals.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Unclear risk Insufficient information to evaluate thecomparability of groups at entry
Al-Nawas 2012
Methods 1-year follow-up, randomised split-mouth study.
Participants Adults with mandibular edentulism, requiring 2 mandibular implants in the intraforam-inal region support an overdentureTreated in multicentre clinics in Germany, Italy, Belgium, the Netherlands and Switzer-land92 enrolled and results given for 89.Exclusion criteria: any medical conditions contraindicating implant surgery, a history ofradiotherapy of the head and neck region, bone grafted jaws
Interventions Group 1: ITI® Roxolid tapered screws with internal connection (Institut StraumannAG, Waldenburg, Switzerland)Group 2: ITI® SLActive titanium grade 4 tapered solid screws with internal connec-tion (Institut Straumann AG, Waldenburg, Switzerland) supporting overdentures on 2implants connected with locator attachments
Outcomes Marginal bone level changes on panoramic radiographs, implant stability, implant mo-bility, plaque index, sulcus bleeding index, complications
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk The study did not mention how ramdomallocation was generatedAuthors replied: “The random sequence
64Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Al-Nawas 2012 (Continued)
was generated by a computer program.”
Allocation concealment (selection bias) Unclear risk Study reported: “Except for the material,both devices were identical and the ster-ile glass-tube containers were marked Aor B. Blinding keys were kept centrally atthe sponsor. The first implant was ran-domly allocated to either the right or theleft intraforaminal region of the edentu-lous mandible, the other one placed in thecontralateral side. Randomization was per-formed using sealed envelopes which wereopened after bone exposure during surgery.”
Blinding (performance bias and detectionbias)All outcomes
High risk Study reported: “Clinical examinationswere performed after 6 months, but thestudy was unblinded only after 12 monthspost-surgery.”Authors replied: “The outcome assessorswere not specified or restricted, as out-come was recorded before unblinding ... The outcome assessors were not furtherspecified for the secondary clinical parame-ters. The primary criterion was ”radiologicbone loss“. This one was blindly assessedby a centre which was not involved into re-cruitment.”Comment: outcome assessors for clinicaloutcomes were not blinded at the treatmentcentres with the exceptions of radiographicevaluation, which we did not use
Incomplete outcome data (attrition bias)All outcomes
Low risk Not all outcome data presented, 4 with-drawals out of 92 participants; 1 failure inthe ITI Roxolid and 2 failures in the SLAc-tive group
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
65Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Alsabeeha 2011
Methods 1-year follow-up, randomised parallel group study.
Participants Adults with mandibular and maxillary edentulism, requiring a single mandibular implantin the midline to support an overdentureTreated in the School of Dentistry, New Zealand.36 enrolled and results given for 35.Exclusion criteria: any medical conditions contraindicating implant surgery, a history ofradiotherapy of the head and neck region, bone grafted jaws and bone quality type IV(very soft bone)
Interventions Group 1: Southern® sand-blasted titanium grade 4, 8-mm wide tapered screws withexternal connection (Southern Implants, Irene, South Africa)Group 2: Southern® sand-blasted titanium grade 4 cylindrical screws with externalconnectionGroup 3: Neoss sand-blasted acid-etched titanium grade 4 cylindrical screws with internalconnection (Neoss Ltd, Harrogate, UK) single implants
Outcomes Marginal bone level changes on standardised periapical radiographs, implant stability(resonance frequency analysis), implant and prosthodontic success, complications
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “...the randomisation andallocation of the 36 participants into threedifferent interventions of 12 participantseach was commenced. A simple randomi-sation protocol using 36 sequentially num-bered opaque sealed envelopes was followed..... to ensure maximum concealment. Adental assistant not involved in the studyperformed the randomisation and alloca-tion procedures.”Authors replied: “A simple randomisationprocedure was performed using 36 sequen-tially numbered opaque sealed envelopes.In brief, three separate sets of envelopes(12 envelopes each, with each envelopecontaining a card denoting one of the3 planned interventions) ......... The en-velopes were shuffled repeatedly and thor-oughly and then marked sequentially from1 to 36. This protocol was performed bya dental nurse not involved in the clinicaltrial and not exposed to the different inter-ventions intended.”
66Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Alsabeeha 2011 (Continued)
Allocation concealment (selection bias) Low risk Study reported: “A dental assistant not in-volved in the study performed the ran-domisation and allocation procedures.”Authors replied: “To ensure maximum con-cealment, a tin foil was wrapped aroundeach card carrying the specific interventionwithin each envelope. The envelopes werelocked up under the care of the same den-tal nurse carrying the randomisation pro-cedure and were opened sequentially at theday of surgery.”
Blinding (performance bias and detectionbias)All outcomes
High risk Study reported: “Blinding of outcome as-sessors to the interventions was not possi-ble.”Authors replied: “The prosthodontist wasthe outcome assessor.”Comment: ideally, an independent out-come assessor should have performed theassessment
Incomplete outcome data (attrition bias)All outcomes
Low risk Radiographic data of 1 participant miss-ing, otherwise fully reported. 1 failure and1 drop-out in the Southern regular group
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
Astrand 1999
Methods 5-year follow-up randomised, parallel group study.
Participants Edentulous adults treated in the University Hospital of Linkoping, Sweden68 enrolled (34 in each group) and results given for 66.Exclusion criteria: 2 participants were excluded at the implant installation since theydid not meet the inclusion criteria (insufficient bone volume with need of bone graft orguided tissue regeneration)
Interventions Group 1: Astra® (Astra Tech AB, Mölndal, Sweden) TiO2-blasted submerged titaniumscrews.Group 2: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark II type submergedturned titanium screws supporting fixed prostheses
Outcomes Pain from implant region, implant stability tested with superstructure removed, prosthe-ses survival, marginal bone level changes on standardised intraoral radiographs, plaqueaccumulation, bleeding on probing, operation time, mechanical complications, peri-im-plant infections with bone loss (peri-implantitis), presence or absence of attached peri-
67Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Astrand 1999 (Continued)
implant mucosa1-, 3- and 5-year data used.
Notes 8 participants in the Brånemark group were scored at implant insertion as having type IVbone quality (very soft bone) according to the Lekholm and Zarb classification (Lekholm1985) versus 1 participant in the ITI group.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Study reported: “Two randomisationschedules were generated one for implantinstallation in the mandible and one for themaxilla. The patients were randomised inblocks with an equal probability of receiv-ing Astra Tech or Brånemark implants.”Authors replied: “Randomisation was car-ried out with equal possibilities for bothtypes of implant. Randomisation scheduleswere sent to the clinics participating in thestudy.”
Allocation concealment (selection bias) High risk Unclear from the study.Authors replied: “Randomisation schedulewere sent to the clinician participating inthe study, and they included the patientconsecutively after this schedule. Specialmeasures to conceal the schedules untiltreatment were not made.”
Blinding (performance bias and detectionbias)All outcomes
High risk An independent assessor made the radio-graphic evaluations.Other outcome assessors not blinded.
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data provided by authors onrequest, 2 out of 68 participants withdrew.All failed and fractured implants accountedfor, but missing baseline radiograph for 1mandible in Astra group. Marginal bonelevel data, mean and standard deviation ona participant basis provided on request foreach study group. 2 withdrawals in the As-tra group after year 3 due to participantdeath
Selective reporting (reporting bias) Low risk No selective reporting identified.
68Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Astrand 1999 (Continued)
Other bias Unclear risk 8 participants in the Brånemark group werescored at implant insertion as having typeIV bone quality (very soft bone) accordingto the Lekholm and Zarb classification (Lekholm 1985) versus 1 participant in theITI group.
Astrand 2002
Methods 3-year follow-up randomised, split-mouth study.
Participants Adults aged 20-75 years with partially edentulous maxillae.Treated in 5 different dental clinics in Sweden. 28 enrolled and results given for 26Exclusion criteria: known leukocyte dysfunction, uncontrolled endocrine disorders, psy-chotic disorders, heavy smoking habits (> 20 cigarettes/day), alcohol or drug abuse,current steroid or chemotherapy treatments, local irradiation therapy, insufficient bonevolume with need of bone graft or guided tissue regeneration, heavy bruxism, currentperiodontitis, < 6 months healing after tooth extraction
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark II type submergedturned titanium screwsGroup 2: ITI® (Institut Straumann AG, Waldenburg, Switzerland) non-submergedsolid titanium plasma-sprayed screws supporting maxillary fixed partial prostheses
Outcomes Pain from implant region, prostheses survival, marginal bone level changes on standard-ised intraoral radiographs, plaque accumulation, bleeding on probing, mechanical com-plications, hyperplasia of the peri-implant mucosa, peri-implant infections with boneloss (peri-implantitis)1-year data used.
Notes Implant stability not recorded. Data on implant failures may be underestimated andwere therefore not included in the statistical calculations
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “A randomisation list wasgenerated.......The study was performed inthe maxilla as a split-mouth study; theBrånemark implants were used on one side,and the ITI implants were used on the con-tralateral side of the residual dentition ac-cording to a randomisation procedure. Atthis procedure, a blocking size of four wasused, giving an equal probability of the pa-tient’s receiving ITI or Brånemark implants
69Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Astrand 2002 (Continued)
in the right or left side of the jaw.”Authors replied: “The randomisation wascarried out with equal possibility forBrånemark and ITI implants.”
Allocation concealment (selection bias) Unclear risk Unclear from the study.Authors replied: “... no special measureswere taken to conceal the randomisationschedules until treatment.”
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study reported: “The [radiographic] mea-surements were taken by two of the inves-tigators working independently. In cases ofa difference of > 0.5 mm the radiographswere re-examined by both investigators andconsensus was sought.”It was not possible to blind outcome asses-sors.
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data provided on request fromauthors, 2 participants died before the 3-year follow-up
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias High risk The planned publication at 5-year was can-celled by the authors and the authors jus-tified this as the sponsored implants notto be commercially available any longer. Inour mind, this publication would have con-tained crucial information on the occur-rence/outcome of peri-implantitis
Batenburg 1998
Methods 10-year follow-up randomised, parallel group study.
Participants Edentulous adults for at least 2 years with severely resorbed mandibles (class V-VI ac-cording to the classification of Cawood 1988).Treated in the University Hospital of Groningen, the Netherlands90 enrolled (30 in each group) and results at 10 years given for 83Excluded: people subjected to radiotherapy in the head and neck region or pre-prostheticsurgery or previous oral implantology were excluded
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) submerged turned tita-nium screwsGroup 2: ITI® (Institut Straumann AG, Waldenburg, Switzerland) non-submergedhollow titanium plasma-sprayed screws
70Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Batenburg 1998 (Continued)
Group 3: IMZ® (Friedrichsfeld AG, Mannheim, Germany) submerged titaniumplasma-sprayed cylinders supporting overdentures on 2 implants connected with a bar
Outcomes Periotest and tapping the implant with superstructures removed, sensibility of lip andchin, marginal bone level changes on standardised intraoral radiographs, plaque accu-mulation, calculus, bleeding on probing, mucosa score, probing pocket depth, mucosarecession, width of attached peri-implant mucosa1-, 3- 5- and 10-year data used.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “Allocation to one of thetreatment options was carried out by meansof 90 envelopes, which contained a notewith the implant system.”Authors replied: “patients were allocated bylot, i.e. by randomly picking one of the en-velopes.”
Allocation concealment (selection bias) Unclear risk No information provided in the originalarticle.Authors’ reply did not clarify the proce-dure.
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study reported: “Bias was prevented by thefact that there was no sequence in mea-suring the radiographs and measurementswere not performed per patient. In this way,there was no recollection by the observer asto bone loss in earlier years.”Comment: outcome assessors could not beblinded; however, it is unclear who mea-sured the various outcomes whether an in-dependent assessor or 1 of the operators.Authors could only have mixed the se-quence of baseline and 1-year radiographs,not the other since reported the results overthe years
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented. At the 1-yearexamination, 1 participant in the ITI groupdied. At the 5-year examination, 3 partic-ipants of the Brånemark group and 1 ofthe ITI group were unable to attend due tosickness. In addition, 1 participant in the
71Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Batenburg 1998 (Continued)
ITI group died. At the 10-year examina-tion, 3 participants of the Brånemark groupand 1 of the ITI group were unable to at-tend due to sickness. In addition, 1 partici-pant in the IMZ group died. Low attritionover 10 years: 7/90 participants
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
Crespi 2009
Methods 1-year follow-up, randomised parallel group study.
Participants Adults requiring an immediate post-extractive implants in the maxillae or mandibleTreated in the Department of Dentistry, San Raffaele Hospital, Milan, Italy45 enrolled and results given for 45.Exclusion criteria: chronic systemic disease, presence of dehiscence or fenestration of theresidual bony walls, coagulation disorders, presence of signs of acute infection aroundalveolar bone at the surgical site, smokers > 10 cigarettes/day, alcohol or drug abuse, orbruxism
Interventions Group 1: Ankylos Plus® grit-blasted and high temperature etched surface, titanium grade2 cylindrical screws with internal conical connection (Dentsply-Friadent, Mannheim,Germany)Group 2: 7 TPS titanium grade 4 screws with external hexagon (Sweden & Martina,Padua, Italy), immediate post-extractive and immediately loaded implants supportingsingle cemented crowns
Outcomes Marginal bone level changes on standardised periapical radiographs, plaque scores, bleed-ing index, pain, occlusion, prosthesis mobility, implant stability
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk No description in the article.Authors replied: “randomisation was doneon patient assignment (by chance) to thegroup 1 or 2.”No further information was provided.
Allocation concealment (selection bias) Unclear risk No description in the article.Authors did not reply to our question.
72Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Crespi 2009 (Continued)
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study clarified: “A blinded radiologist mea-sured the changes in marginal bone heightover time.”Authors replied: “The dental hygienistwho measured the clinical parameters wasblinded; implant stability was measured bythe prosthodontist.”Comment: as the implant shapes were dif-ferent, the radiographic outcome assessorcould not be blinded
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
den Hartog 2011
Methods 18-month follow-up, randomised parallel group study.
Participants Adults requiring a single implant in the aesthetic zone (first to first maxillary premolar)between 2 adjacent teethTreated in a University Medical Center, Groningen, the Netherlands93 enrolled and results given for 93.Exclusion criteria: American Society of Anesthesiologists score ≥ III, presence of clinicallyactive periodontal disease as expressed by probing depths ≥ 4 mm and bleeding onprobing, presence of peri-apical lesions, sites with < 6 mm mesio-distal width, smokersand a history of radiotherapy of the head and neck region
Interventions Group 1: NobelReplace® Tapered Groovy TiUnite oxidised titanium grade 4 taperedscrews with external connection (Nobel Biocare AB)Group 2: NobelReplace® Select Tapered TiUnite oxidised titanium grade 4 taperedscrews with external connectionGroup 3: NobelPerfect® Groovy TiUnite oxidised titanium grade 4 tapered screws withexternal connection single implants
Outcomes Marginal bone level changes on standardised periapical radiographs, implant survival,papilla index, plaque scores, bleeding index, probing pocket depths, photographic as-sessments
Notes The part of the trial comparing NobelPerfect Groovy with the other 2 implants wasnot used in the present review since NobelPerfect Groovy implants were systematicallypositioned at a higher position with respect to the adjacent bone. The article reportedstatistically significant more bone loss (0.8 mm) at NobelPerfect Groovy implants
Risk of bias
73Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

den Hartog 2011 (Continued)
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “A specifically designedlocked computer software program wasused to randomly assign patients to oneof three study groups ...... Randomizationby minimization (Altman 1991) was usedto balance possible prognostic variables be-tween the three groups.”
Allocation concealment (selection bias) Low risk Study reported: “The allocation result waskept in a locked computer file that was notaccessible for the examiner and the practi-tioners. The surgeon that inserted the im-plants was informed about the allocationon the day of the surgery.”Authors further responded to clarification:“The surgeon was informed about the al-location before initial site preparation byreading indeed a list to know what implantshould be installed. This list was updated bythe person that entered each study partici-pant into the computer program. This wasa locked computer program that was notaccessible for the examiner and the prac-titioners and the randomisation occurredafter details regarding age, whether or notan augmentation procedure was indicatedand the location of the implant site wereentered in the program.”
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study reported: “All data were retrieved byone blinded examiner according to a spec-ified protocol.”Comments: the assessment of the periapicalradiographs could not be blinded due todifferent implant designs
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals. 1 implant failure in the NobelRe-place Select group
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
74Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Esposito 2012
Methods 1-year follow-up, randomised parallel group study.
Participants Adults with fully or partial edentulism, requiring 1-6 maxillary implantsTreated in 2 different centres in Italy.60 enrolled and results given for 60.Exclusion criteria: any medical conditions contraindicating implant surgery, a history ofradiotherapy of the head and neck region, bone grafted jaws and people that could notbe restored with a retrievable prosthesis to allow for implant stability assessment
Interventions Group 1: MegaGen EZ Plus titanium grade 4 tapered screws with sand-blasted surfacewith internal connection (MegaGen Implant, Gyeongbuk, South Korea) standard formGroup 2: MegaGen EZ Plus titanium grade 4 tapered screws with sand-blasted surfacewith internal connection (MegaGen Implant, Gyeongbuk, South Korea) modified form(calcium-incorporated surface: Xpeed) supporting early loaded screw-retained fixed pros-thesis
Outcomes Prosthesis and implant success, implant stability assessed using a manual wrench with atorque of 20 Ncm, complications, marginal bone level changes on standardised periapicalradiographs
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study clarified: “A computer-generated re-stricted random list was created by one ofthe authors who was not involved in patientrecruitment or treatment, and had access tothe random list stored in a password-pro-tected portable computer.”
Allocation concealment (selection bias) Low risk Study clarified: “The randomised codesdesignated as ’implant 1’ and ’implant 2’were enclosed in sequentially numbered,identical, opaque, sealed envelopes. En-velopes were opened sequentially only af-ter the implant sites were prepared, there-fore treatment allocation was concealed tothe investigators in charge of enrolling andtreating the patients.”
Blinding (performance bias and detectionbias)All outcomes
Low risk Study clarified: “Two independent andfully blinded dentists not aware of pa-tient allocation evaluated stability with theprostheses removed. Another independentand fully blinded dentist evaluated peri-im-plant marginal bone level changes.”
75Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Esposito 2012 (Continued)
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals or failures.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
Esposito 2013a
Methods 1-year follow-up randomised, split-mouth study.
Participants Adults with partial edentulism, requiring 2 maxillary or mandibular implantsTreated in a private practice in Switzerland.23 enrolled and results given for 22.Exclusion criteria: general contradictions to implant surgery, a history of radiotherapyof the head and neck region, uncontrolled diabetes, untreated periodontitis, pregnant,requiring augmentation procedure at implant placement, treated with intravenous bis-phosphonates and requiring immediate implants
Interventions Group 1: SPI® Element implant sand-blasted acid-etched titanium grade 4 cylindri-cal screw with internal connection (SPI® Element, Thommen Medical, Waldeburg,Switzerland) original formGroup 2: SPI® Element implant sand-blasted acid-etched titanium grade 4 cylindri-cal screw with internal connection (SPI® Element, Thommen Medical, Waldeburg,Switzerland) modified surface (SurfLink®, Nano Bridging Molecules, Gland, Switzer-land) supporting conventionally loaded cemented single implants. The SurfLink con-sisted of a monolayer of permanently bound multi-phosphonic acid molecules
Outcomes Crown/implant failures, complications, peri-implant marginal bone level changes, mar-ginal bleeding
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study clarified: “A computer generated re-stricted random list was created for assign-ment of implant type.”
Allocation concealment (selection bias) Low risk Study clarified: “The study centre received,at the beginning of the study, a series ofnumbered, identical, opaque, sealed en-velopes containing the implantation siteand implant type distribution for each pa-tient. This letter was opened before the
76Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Esposito 2013a (Continued)
surgery and after obtaining signed in-formed consent from the patient. There-fore, treatment allocation was concealed tothe investigator in charge of enrolling andtreating the patients.”
Blinding (performance bias and detectionbias)All outcomes
Low risk Study clarified: “A quadruple-blind design(patients, operator, out- come-assessor andstatistician) was adopted. Random codeswere broken only after the complete statisti-cal analyses were made. Since the SurfLink-treated implants were not distinguishableby the naked eye from the untreated con-trol, the blinding procedure was success-ful. Two trained researchers evaluated theradiographs ...... not involved in the Sur-fLink implant preparation or patient treat-ment, performed all radiographic assess-ments without knowing group allocation.Each assessment was double-checked by anexperienced dentist (Dr Marco Esposito)trained in bone level assessments and finalvalues were accepted only if both assessorsagreed on the individual measurement.”
Incomplete outcome data (attrition bias)All outcomes
Low risk 1 baseline radiograph unreadable, other-wise no withdrawals.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
Fröberg 2006
Methods 18-month follow-up randomised, split-mouth study.
Participants Adults with edentulous mandibles.Treated in a private dental practice in Nässjö, Sweden.15 enrolled and results given for 15.Exclusion criteria: systemic diseases resulting in increased risk of infection and impairedhealing, serious cardiac diseases, deficient homeostasis and blood dyscrasias, anticoagu-lant medication, psychological diseases, uncontrolled acute infections
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark III TiUnite oxi-disedGroup 2: Mark III turned immediately loaded titanium screws supporting screw-retainedcross-arch fixed prostheses
77Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fröberg 2006 (Continued)
Outcomes Implant stability (resonance frequency analysis), marginal bone level changes on stan-dardised intraoral radiographs, marginal bleeding index
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “The ”toss of a coin proce-dure“ was used to select the half of the jawwhere the three turned implants had to beplaced. An identical surgical procedure wasthen performed in the corresponding con-tralateral area of the mandible where thethree TiUnite implants were placed.”
Allocation concealment (selection bias) Unclear risk No description in the article.No answer to our request of clarification.
Blinding (performance bias and detectionbias)All outcomes
Unclear risk No description in the article.No answer to our request of clarification.
Incomplete outcome data (attrition bias)All outcomes
High risk Not all radiographic data presented, butotherwise no withdrawals
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
Gatti 2002
Methods 2-year follow-up randomised, parallel group study.
Participants Edentulous adults for at least 3 months with mandibles having a residual bone height inthe intraforaminal area adequate to harbour 4 implants at least 9 mm long. Treated in aprivate dental practice in Milan, Italy10 enrolled (5 in each group) and results given for 10.Exclusion criteria: severe intermaxillary skeletal discrepancy, strong gagging reflex, severeclenching or bruxism, previous implant surgery in the inter-foraminal area, drug oralcohol abuse, moderate or heavy smoking (> 10 cigarettes/day), radiotherapy in the headand neck region or treatment with antiblastic chemotherapeutics, chronic liver and renaldisease, uncontrolled diabetes, haemophilia or other bleeding disorders or treatmentwith cumarin, metabolic bone disorders, immunocompromised conditions includinghuman immunodeficiency virus, current steroid treatment, current pregnancy, generalcontraindications for surgical procedures, physical or psychiatric handicaps that couldinterfere with good oral hygiene, presence of mucosal disease such as lichen planus
78Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Gatti 2002 (Continued)
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark II type non-sub-merged turned titanium screwsGroup 2: Brånemark® conical transmucosal screws used without abutments supportingoverdentures on 4 implants connected with a bar and immediately loaded
Outcomes Implant stability, marginal bone level changes on intraoral radiographs taken with aparalleling technique and on intraoral panoramic radiographs, plaque accumulation,gingival index, probing pocket depth1- and 3-year data used.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk No information provided in the article.Authors replied: “Randomisation done bylot by another person other than the sur-geon.”
Allocation concealment (selection bias) Unclear risk No information provided in the article.No answer to our request of clarification.
Blinding (performance bias and detectionbias)All outcomes
High risk No information provided in the article.Authors replied: “No blinding was done.”
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Unclear risk Nothing to report with exception of thevery low sample size (only 5 participantsper group)
Heberer 2011
Methods 14-month follow-up randomised, split-mouth study.
Participants Adults with ≥ 1 missing teeth following malignant tumour removal and radio-chemo-therapy up to 72 Gy before implant placement. Radiotherapy was delivered infractions of 2 Gy given daily for 5 days each week over 6 weeks. Implants were insertedat least 6 months after radiotherapyTreated in the Charite University Medicine in Berlin, Germany20 enrolled and results given for 20.Exclusion criteria: poor general health and smokers.
79Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Heberer 2011 (Continued)
Interventions Group 1: 50 ITI (Institut Straumann AG, Waldenburg, Switzerland) non-submergedsolid titanium screws with SLA surfaceGroup 2: 52 ITI SLActive surface non-submerged solid titanium modified surface char-acterised by a hydroxylated TiO2 film, early loaded at 6 weeks in mandibles and at 10weeks in maxillas with 16 bar-supported overdentures and 4 fixed prostheses
Outcomes Implant stability, marginal bone level changes on intraoral panoramic radiographs, plaqueaccumulation, bleeding index, probing pocket depth
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Study reported: “Test and control site wererandomly assigned according to a split-mouth design.”Author replied: “Following a randomisa-tion list the implant were placed.”
Allocation concealment (selection bias) Unclear risk Not described in the article.The authors did not reply to this question.
Blinding (performance bias and detectionbias)All outcomes
Low risk Not described in the article.Author replied: “The radiological and clini-cal data assessment was performed blinded.The examiner had no knowledge of whatimplant (SLA or SLActive) was used.”
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented. There were 2failures before loading. There was 1 with-drawal at 1 year due to cancer recurrenceand the mandible with 5 implants (2 SLAand 3 SLActive) had to be resected
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other biases identified.
80Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Heydenrijk 2002
Methods 5-year follow-up randomised, parallel group study.
Participants Edentulous adults for at least 2 years with severely resorbed mandibles (class V-VI ac-cording to the classification of Cawood 1988).Treated in the University Hospital of Groningen, the Netherlands40 enrolled (20 in each group) and results given for 37.Exclusion criteria: people subjected to radiotherapy in the head and neck region or pre-prosthetic surgery or previous oral implantology
Interventions Group 1: IMZ® (Friedrichsfeld AG, Mannheim, Germany) non-submerged titaniumplasma-sprayed cylindersGroup 2: ITI® (Institut Straumann AG, Waldenburg, Switzerland) non-submergedsolid titanium plasma-sprayed screws supporting overdentures on 2 implants connectedwith a bar
Outcomes Periotest, marginal bone level changes on standardised intraoral radiographs, plaque ac-cumulation, bleeding index, calculus, mucosa score, probing pocket depth, microbio-logical sampling
Notes Outcome assessors could not be blinded. 3 withdrawals: 2 from the ITI group for death(year 3) and illness (year 4) and 1 from the IMZ group for moving (year 4)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Study reported: “The randomization pro-cess was as follow: a series of 60 inte-gers were randomized and subsequently as-signed to the consecutive patients. The first20 randomized integers were assigned toIMZ 1-stage, the second 20 integers toIMZ 2-stage, and the remaining integersto ITI. A note with the assigned treatmentmodality was put in an envelope for eachpatient. In this way, the consecutive pa-tients received a randomly assigned treat-ment modality.”No answer to our request of clarification.
Allocation concealment (selection bias) Unclear risk No information provided in the article.No answer to our request of clarification.
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study reported: “Measurements were doneby the same observer throughout the eval-uation period after calibration.”No answer to our request of clarification.
81Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Heydenrijk 2002 (Continued)
Incomplete outcome data (attrition bias)All outcomes
Low risk 3 out of 40 withdrawals: 2 from the ITIgroup for death (year 3) and illness (year 4)and 1 from the IMZ group for moving (year4). All outcome data presented apart from2 radiographs missing for 2 participants, 1from each group
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Unclear risk Insufficient information to evaluate thecomparability of groups at entry
Kielbassa 2009
Methods 3-year follow-up randomised, multicentre, parallel group study
Participants Adults with ≥ 1 missing teeth in a healed site (for at least 6 months after extraction) ofthe maxilla or mandible, with a residual bone height adequate to harbour implants witha diameter of at least 3.5 mm and length of at least 10 mm longTreated in 12 different University Hospitals in Berlin, Seville, Jerusalem, Vienna, Rome,Witten, Freiburg, Graz, Milan, Bern, Liege and Madrid177 enrolled (NobelActive Internal 64 included, NobelActive External 53, NobelReplace60 included) results given for 127 participants at 3 yearsExclusion criteria: health problems that would preclude surgical procedures, drug oralcohol abuse, any pathological condition, severe bruxism, psychiatric disease, inabilityof the person to provide informed consent, the need for bone augmentation to obtain anideal position of the implant(s), residence outside the city of the respective study centreor inability for follow-up
Interventions Group 1: NobelActive® TiUnite oxidised titanium grade 4 tapered screws with internalconnection (Nobel Biocare AB, Göteborg, Sweden)Group 2: NobelActive® TiUnite oxidised titanium grade 4 tapered screws with externalhexagonGroup 3: NobelReplace® Tapered Groovy TiUnite oxidised titanium grade 4 taperedscrews with internal connection, placed in healed sites with immediate provisional singlecrown restorations
Outcomes Crestal bone levels around implants, implant stability, soft tissue aesthetics, number ofadverse events at participant level, papilla score, plaque accumulation
Notes At 3-years, 45 participants were lost to follow-up: 18 in the tapered implant with variablethread group, 9 in the transmucosal tapered implant with variable-thread design group,and 18 in the standard tapered implant group
Risk of bias
Bias Authors’ judgement Support for judgement
82Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kielbassa 2009 (Continued)
Random sequence generation (selectionbias)
Low risk Study clarified: “Prior to surgery, patientswere randomised into 1 of the 3 treatmentgroups using sealed, numbered, opaque en-velopes prepared in advance by the spon-sor. The envelopes were prepared froma random-number table using a blockingmethod of 12 assignments per block.”
Allocation concealment (selection bias) High risk Study clarified: “The details of the ran-domisation procedure were unknown to allof the investigators. Thus, a complete sep-aration of the individuals involved in thegeneration and implementation of the as-signments was guaranteed.”Authors replied: “Different implants wereallocated to patients after inclusion, andright (usually several days) before surgery.Due to the fact that the different im-plant types needed different instrumentsand components (i.e. drills, drivers etc), itwas not practical to break the allocation sealafter flap elevation. Hence the seal was bro-ken as soon as possible (most times afterthe patient was included and had signed in-formed consent forms), and before the be-ginning of the surgical procedure.”
Blinding (performance bias and detectionbias)All outcomes
High risk Study clarified: “Due to the nature of thetreatment, neither the study personnel northe patients could be blinded to treatmentassignment.”Authors replied: “... apart from the radio-graphic assessment, the other parameterswere evaluated by the surgeon at each studycentre. With the follow-ups, another den-tist took care occasionally (in some casesthe surgeon was not available).”Comment: the outcome assessors couldhave been blinded to some of the outcomemeasures, otherwise independent assessorscould have been used
Incomplete outcome data (attrition bias)All outcomes
High risk At 3-years, 45 participants out of 177 werelost to follow-up. All outcome data pre-sented
Selective reporting (reporting bias) Low risk No selective reporting identified.
83Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kielbassa 2009 (Continued)
Other bias Low risk No other biases identified.
Lang 2007
Methods 1-year follow-up randomised, parallel group study.
Participants Adults > 21 years needing an immediate post-extractive implant in the aesthetic zone(premolar to premolar) between 2 adjacent teethTreated at 9 different centres possibly London, Rimini, Boston, Bern, Connecticut,Copenhagen, Geneva, Zurich and Athens208 enrolled (104 in each group) and results given for 208.Exclusion criteria: generic contraindication to oral surgery, smoking > 10 cigarettes/day, periodontal bone loss > 20% at the adjacent teeth, full-mouth plaque and bleedingscores > 25% at baseline, teeth to be replaced affected by periodontal disease, presenceof symptomatic periapical radiolucencies, acute abscesses or chronic sinus tracts at theimplant site, lack of primary implant stability, < 7 mm of mesio-distal space between theadjacent teeth, < 2 mm of keratinised mucosa
Interventions Group 1: ITI® (Institut Straumann AG, Waldenburg, Switzerland) submerged sand-blasted large-grit acid-etched (SLA) solid titanium screws: cylindricalGroup 2: ITI® (Institut Straumann AG, Waldenburg, Switzerland) submerged sand-blasted large-grit acid-etched (SLA) solid titanium screws: tapered shapeSites were augmented with granules of deproteinised bovine bone mineral (BioOss Spon-giosa) and resorbable barriers (BioGide) if there was a residual gap defect of at least 0.5mm between the bone and the implant, exposed SLA surface in a supracrestal location,and a buccal bony plate < 1 mm
Outcomes Implant stability (resonance frequency analysis), complications, marginal bone levelchanges on standardised intraoral radiographs, participant evaluation of the surgical pro-cedure, operator and assistant evaluation of the surgical procedure
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study clarified: “Patients were entered intothe study by a Central Registrar. After hav-ing been entered into the study, all subjectswere randomly assigned to one of the twotreatment regimens according to pre-de-fined randomisation tables and using a bal-anced random-permuted block approachstratifying for smoking status.”
84Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lang 2007 (Continued)
Allocation concealment (selection bias) Low risk Study clarified: “Assignment was concealedfrom the investigator until the time duringthe surgical procedure that required appli-cation of the cylindrical or the tapered im-plant by an opaque envelope.”
Blinding (performance bias and detectionbias)All outcomes
Low risk There was no information about blindingin the article.Authors replied: “Every centre had an as-sessor separate from the surgeon that per-formed the procedures. From the transmu-cosal part of the implant it was not possibleto tell which implant had been used exceptfor the radiographs. These, however, werenot accessible to the assessors.”
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals.
Selective reporting (reporting bias) High risk Not all evaluated outcomes were presented.
Other bias Low risk No other biases identified.
Lee 2007
Methods 3-year follow-up randomised, split-mouth study.
Participants Partially edentulous adults showing good oral health.Treated in the College of Dentistry, Yonsei University, Seoul, Korea17 enrolled and results given for 17.Exclusion criteria: no specific criteria mentioned.
Interventions Group 1: Astra® TiO2-blast titanium grade 3 cylindrical screws with internal connectionwithout the Microthread ™ (Astra Tech AB, Mölndal, Sweden)Group 2: Astra® TiO2-blast titanium grade 3 tapered screws with internal connectionwith the Microthread™, placed adjacent to each other restored as a 2-unit fixed prosthesis
Outcomes Marginal bone level changes on standardised intraoral radiograph, pain from the implantregions, implant stability, gingival inflammation, superstructure complications
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
85Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lee 2007 (Continued)
Random sequence generation (selectionbias)
Low risk Study :reported “At the same edentulousarea of each patient, one fixture of each im-plant type was installed in a randomised or-der.”Authors replied: “randomisation was doneby throwing coins.”
Allocation concealment (selection bias) Unclear risk There was no information about allocationconcealment in the articleThe authors replied that allocation conceal-ment was done during surgery
Blinding (performance bias and detectionbias)All outcomes
High risk There was no information about blindingin the article.Comment: we considered that the studywas not blinded.
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
Moberg 2001
Methods 3-year follow-up randomised, parallel group study.
Participants Adults with edentulous mandibles treated in the University Dental Clinic of the Karolin-ska Institute, Huddinge, Sweden40 enrolled (20 in each group) and results given for 36.Exclusion criteria: general or local contraindications (such as systemic medical condi-tions, drug abuse or local jaw pathology), or both
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark II type submergedturned titanium screwsGroup 2: ITI® (Institut Straumann AG, Waldenburg, Switzerland) non-submergedhollow titanium plasma-sprayed screws supporting fixed prostheses
Outcomes Periotest and tapping the implant with superstructures removed at 3 years, marginal bonelevel changes on intraoral and panoramic radiographs, plaque accumulation, marginalbleeding, probing pocket depths, tightness of screws, sensory changes, treatment time,participant satisfaction, mechanical and biological complications, peri-implant infectionswith bone loss1- and 3-year data used.
Notes
86Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Moberg 2001 (Continued)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk No information provided in the article.No answer to our request of clarification.
Allocation concealment (selection bias) Unclear risk No information provided in the article.No answer to our request of clarification.
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Not possible, but no information providedon who made the assessments (an inde-pendent outcome assessor could have beenused)No answer to our request of clarification.
Incomplete outcome data (attrition bias)All outcomes
Low risk 4 out of 40 withdrawals: 2 in theBrånemark group (1 died and 1 did notattend the radiographic examination) and2 died in the ITI group. All outcome datapresented
Selective reporting (reporting bias) Unclear risk At the 3-year examination, 2 ITI implantswere treated for peri-implantitis and theirfate was not reported
Other bias Low risk No other bias identified.
Payne 2003
Methods 10-year follow-up randomised, parallel group study.
Participants Adults aged 55-80 years with edentulous mandibles having 8-15 mm of residual anteriorbone heightTreated in the School of Dentistry, University of Otago, Dunedin, New Zealand24 enrolled (12 in each group) and results given for 18.Exclusion criteria: people with type IV bone quality (very soft bone) according to theLekholm and Zarb classification (Lekholm 1985) detected at implant insertion (none),previously bone-grafted or irradiated jaws, history of bruxism, any evidence of currentor previous smoking and any systemic diseases likely to compromise implant surgery
Interventions Group 1: ITI® (Institut Straumann AG, Waldenburg, Switzerland) non-submergedsand-blasted large-grit acid-etched (SLA) solid titanium screwsGroup 2: Southern® (Southern Implants Ltd, Irene, South Africa) non-submerged sand-blasted acid-etched titanium screws supporting overdentures on 2 implants early loadedat 2 weeks
87Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Payne 2003 (Continued)
Outcomes Resonance frequency analysis, marginal bone level changes on standardised intraoralradiographs, prostheses survival, plaque accumulation, modified gingival index, probingpocket depth, width of the keratinised mucosa, recession, prosthetic maintenance events1-, 3-, 5- and 10-year data used.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “A table of random num-bers was used with maximum concealmentto allocate...”
Allocation concealment (selection bias) Unclear risk Study reported: “A table of random num-bers was used with maximum concealmentto allocate....”Allocation concealment unclear from thestudy.
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Outcome assessors could not be blinded;however, independent outcome assessorscould have been used
Incomplete outcome data (attrition bias)All outcomes
High risk All outcome data presented. 6 withdrawalsout of 24 participants over 10 years: 3 inthe ITI group (2 died and 1 lack of interest)and 3 in the Southern group (2 died and 1dropped out)
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
Payne 2004
Methods 1-year follow-up randomised, parallel group study.
Participants Adults aged 55-80 years with edentulous maxillae opposing overdentures supported by2 implantsTreated in the School of Dentistry, University of Otago, Dunedin, New Zealand40 enrolled (20 in each group) and results given for 38.Exclusion criteria: maxillae with a shape type E (extremely resorbed) according to theLekholm and Zarb classification (Lekholm 1985) on radiographs, previously bone-grafted maxillae, history of bruxism, any evidence of current or previous smoking andany systemic disease likely to compromise implant surgery
88Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Payne 2004 (Continued)
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) TiUnite non-submergedoxidised titanium screws of 3.3 mm diameterGroup 2: Southern® (Southern Implants Ltd, Irene, South Africa) non-submerged sand-blasted acid-etched titanium screws 3.25 mm diameter supporting maxillary overden-tures on 3 unsplinted implants early loaded at 12 weeksMaxillae were treated with either a ridge expansion osteotomy or a combined ridge splitand osteotomy procedure, depending on the ridge bucco-palatal width and the degreeof ridge resorption. Autogenous bone grafts were used to fill intraosseous grooves of theridge split-cases
Outcomes Stability test, marginal bone level changes on standardised intraoral radiographs, reso-nance frequency values1-year data used.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “Using a table of randomnumbers the participants were randomly al-located (with maximum concealment).”
Allocation concealment (selection bias) Unclear risk Study reported: “Using a table of randomnumbers the participants were randomly al-located (with maximum concealment).”
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Outcome assessors could not be blinded;however, independent outcome assessorscould have been used
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented. 2 withdrawalsout of 40 participants: 1 in the Brånemarkgroup (1 of the study implants could notbe placed) and 1 in the Southern group(death)
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
89Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pozzi 2014
Methods 1-year follow-up randomised, split-mouth study.
Participants Adults with partially edentulous mandibles.Treated in a private dental practice in Rome, Italy.34 enrolled and results given for 34.Exclusion criteria: severe bleeding disorders, uncontrolled diabetes or cancer, psycholog-ical diseases, untreated periodontitis and people taking intravenous bisphosphonates
Interventions Group 1: NobelActive® TiUnite oxidised titanium grade 4 tapered screws with internalconnection (Nobel Biocare AB)Group 2: Nobel Speedy Groovy TiUnite oxidised titanium grade 4 tapered screws withexternal connection (Nobel Biocare AB) placed in healed sites loaded after 4 months ofhealing with single crowns
Outcomes Implant stability (resonance frequency analysis), marginal bone level changes on stan-dardised intraoral radiographs, surgical and prosthetic complications, bleeding on prob-ing and plaque scores
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study clarified: “A pregenerated randomsequence was created... Opaque envelopeswere sealed according to pregenerated list.”
Allocation concealment (selection bias) Low risk Study clarified: “An independent judgeprepared all envelopes. Each edentuloussite of each patient was randomly assignedto one of the two implant groups. Immedi-ately after flap elevation, an assistant indi-cated which implant had to be placed firstfollowing the indications contained in thesequentially numbered envelope.”
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study clarified: “An independent assessormade intraoral radiographs by means ofa custom radiographic holder and paralleltechnique.... An independent radiologist,not previously involved in this study, per-formed all the bone height measurements.”, “One blinded outcome assessor who wasotherwise not involved in the study per-formed all resonance frequency measure-ments.”Comment: the assessors of the reso-
90Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pozzi 2014 (Continued)
nance frequency measurements cannot beblinded
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals.
Selective reporting (reporting bias) Low risk Data on complications not reported in thearticle, but reported to us
Other bias Low risk No other bias identified.
Prosper 2009
Methods 2-year follow-up randomised, split-mouth study.
Participants Adults aged 25-70 years with 6 posterior missing teeth, at least 1 in each posteriorquadrantTreated in 12 dental centres in 5 major demographic areas of Italy68 enrolled and results given for 66.Exclusion criteria: previous dental implant surgery, temporomandibular disorders, anyevidence of current or previous smoking and any systemic disease likely to compromiseimplant surgery
Interventions Group 1: WINSIX® cylindrical screws (WINSIX Ltd, London, UK)Group 2: WINSIX® tapered screws inserted into healed sites and conventionally loadedsupporting single crowns for 2 yearsEach participant received 3 tapered implants and 3 cylindrical implants. Of these im-plants, 1 was placed submerged, 1 was non-submerged and 1 was platform switched
Outcomes Stability test using the implant stability quotient, marginal bone level changes on stan-dardised intraoral radiographs, sulcus bleeding index, plaque index, pain levels
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk Study reported: “Randomization was donewith sealed opaque envelopes containingdesignations based on within patient allo-cation lists randomly generated at the per-muted block size of 6 and stratified accord-ing to centre.”
Allocation concealment (selection bias) Unclear risk There was no clarification from the studyas to whether the surgeons knew which im-plant they would be placing before prepa-
91Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prosper 2009 (Continued)
ration of the surgical site
Blinding (performance bias and detectionbias)All outcomes
High risk Outcome assessors could not be blinded.Study reported for crestal bone levels: “Allmeasurements ...were made by the samecalibrated examiner, who was blinded tothe subjects.”Comment: the examiner would be awareof the shape of the implant from the ra-diographs. There is no information in thestudy as to who carried out the clinical ex-aminationsIndependent outcome assessors could havebeen used.
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, 2 withdrawalsout of 68 participants over first 12 months:4 cylindrical implants failed vs. 2 taperedimplants. There were 2 withdrawals in thefirst 12 months
Selective reporting (reporting bias) High risk Data not given for the participants in whichimplants failed
Other bias Low risk No other bias identified.
Schincaglia 2007
Methods 3-year follow-up randomised, split-mouth study.
Participants Adults with bilateral distal partial edentulous mandibles allowing the placement of atleast 2 x 8.5-mm long implantsTreated in the School of Dentistry, University of Bologna, Italy10 participants enrolled and results given for 10.Exclusion criteria: need of augmentation procedures, extraction sites healing < 4 months,different type of opposing bilateral occlusion, implants inserted with a torque < 20 Ncmor with an implant stability quotient < 60
Interventions Group 1: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark IV TiUnite oxi-disedGroup 2: Brånemark® (Nobel Biocare AB, Göteborg, Sweden) Mark IV turned, imme-diately loaded titanium screws supporting screw-retained partial fixed prostheses
Outcomes Resonance frequency analysis, marginal bone level changes on intraoral radiographs,pocket depths, sulcus bleeding index, plaque index, prostheses survival3-year data used.
Notes
92Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schincaglia 2007 (Continued)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Study reported: “Test and control sideswere randomly assigned according to a pre-determined randomisation table.”Authors replied: “A list with 10 positionswas created before patient’s recruitment.For each position the test side (where thetest implants should have been inserted)was chosen by flip coin. Then, the eligiblepatients were consecutively assigned to aposition of the list as they entered the study(first patient to position 1 ...).”
Allocation concealment (selection bias) High risk There was no clarification from the study.Authors replied: “Therefore the test and thecontrol sides were known at the time ofpatient enrolment and the surgeon was notblinded.”
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Study reported: “A blinded examiner mea-sured the bone on each radiograph.”No information provided for the other out-comes.
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals. The authors provided the meanradiographic bone loss change at a partici-pant level on request
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
Song 2009
Methods 1-year follow-up randomised, split-mouth study.
Participants Adults aged 37-78 years with partially edentulous sites.Most participants were in good health, and the 2 participants who had diabetes andhypertension were well controlled with medication. Treated in the College of Dentistry,Yonsei University, Seoul, Korea20 enrolled and results given for 20.Exclusion criteria: no specific criteria.
93Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Song 2009 (Continued)
Interventions Group 1: Implantium® sand-blasted, large grit, acid-etched (SLA) titanium cylindricalscrews with microthreads 0.5 mm below the top of the implant and internal connection(Dentium, Seoul, Korea)Group 2: Implantium® SLA titanium cylindrical screws with microthreads to top of theimplant and internal connection (Dentium)Implants were placed adjacent to each other restored as a 2-unit fixed prosthesis apartfrom 2 participants where the implants were splinted to fabricate 3- and 4-unit prostheses.Mandibular implants were loaded after 3 months and maxillary implants after 6 months
Outcomes Prosthesis and implant failure, complications, marginal bone level changes on standard-ised intraoral radiograph, pain, discomfort, modified plaque index and modified sulcusbleeding index1-year data used.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk The study did not state how randomisationwas done.Authors replied: “Randomisation was doneby throwing coins.”
Allocation concealment (selection bias) Unclear risk The study did not state if there was alloca-tion concealment.Authors replied: “it was concealed to sur-geons.”
Blinding (performance bias and detectionbias)All outcomes
High risk It was not possible to blind the outcomeassessors to the radiographic readings butindependent assessors could have been usedas well as blinded assessor could have beenused to test implant mobility
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented, no with-drawals.
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
94Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tawse-Smith 2001
Methods 10-year follow-up randomised, parallel group study.
Participants Edentulous mandibles having 13-15 mm of residual anterior bone heightTreated in the School of Dentistry, University of Otago, Dunedin, New Zealand24 enrolled (12 in each group) and results given for 20.Exclusion criteria: people with type IV bone quality (very soft bone) according to theLekholm and Zarb classification (Lekholm 1985) detected at implant insertion (none),previously bone-grafted or irradiated jaws, history of bruxism, any evidence of currentor previous smoking and any systemic disease likely to compromise implant surgery
Interventions Group 1: Steri-Oss® (Steri-Oss, Yorba Linda, California, USA) non-submerged acid-etched titanium screws HL series, 3.8 mm in diameterGroup 2: Southern® (Southern Implants Ltd, Irene, South Africa) non-submerged sand-blasted acid-etched titanium screws supporting mandibular overdentures on 2 implantsconventionally loaded at 12 weeks
Outcomes Prosthesis and implant failures, complications, marginal bone level changes on standard-ised intraoral radiographs, plaque accumulation, modified sulcus bleeding index, prob-ing pocket depth, width of the keratinised mucosa1-, 3-, 5- and 10-year data used.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Not reported in the study.Authors replied: “Patients were first al-located on a one-by-one basis to eachof our implant systems (total was actu-ally 4 systems: Sterioss, Southern, ITI andBrånemark). Thereafter using a table ofrandom numbers we went down each listand allocated the patient to a loading group(either 12 weeks, 6 weeks and for forth-coming publications 2 weeks).”
Allocation concealment (selection bias) Unclear risk Unclear from the study and authors’ replydid not clarify the matter
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Not reported in the study.Authors replied: “Outcome assessors weredefinitively blinded with respect to theloading schedule, however the loadingschedule was not under investigation andwe judged that it was not possible to blindfor the outcome measures of interest in thepresent review.”
95Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tawse-Smith 2001 (Continued)
Comment: it remains unclear whether anindependent outcome assessor was used
Incomplete outcome data (attrition bias)All outcomes
Low risk All outcome data presented. 4 drop-outsoccurred over a 10-year period: 3 in theSteri-Oss group (2 drop-outs and 1 death)and 1 in the Southern group (death)
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias Low risk No other bias identified.
Tawse-Smith 2002
Methods 10-year follow-up randomised, parallel group study.
Participants Edentulous mandibles having 13-15 mm of residual anterior bone heightTreated in the School of Dentistry, University of Otago, Dunedin, New Zealand24 enrolled (12 in each group) and results given for 19.Exclusion criteria: people with type IV bone quality (very soft bone) according to theLekholm and Zarb classification (Lekholm 1985) detected at implant insertion (none),previously bone-grafted or irradiated jaws, history of bruxism, any evidence of currentor previous smoking, any systemic disease likely to compromise implant surgery
Interventions Group 1: Steri-Oss® (Steri-Oss, Yorba Linda, California, USA) non-submerged acid-etched titanium screws HL series, 3.8 mm in diameterGroup 2: Southern® (Southern Implants Ltd, Irene, South Africa) non-submerged sand-blasted acid-etched titanium screws supporting mandibular overdentures on 2 implantsearly loaded at 6 weeks
Outcomes Periotest, marginal bone level changes on standardised intraoral radiographs, prosthesessurvival, plaque accumulation, modified sulcus bleeding index, probing pocket depth,width of the keratinised mucosa1-, 3-, 5- and 10-year data used.
Notes Most of the failed implants were placed by a surgeon who placed only Steri-Oss implants
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk Not reported in the study.Authors replied: “Patients were first allo-cated on a one-by-one basis to each ofour implant systems (total was actually4 systems: Steri-Oss, Southern, ITI andBrånemark). Thereafter using a table ofrandom numbers we went down each list
96Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tawse-Smith 2002 (Continued)
and allocated the patient to a loading group(either 12 weeks, 6 weeks and for forth-coming publications 2 weeks).”
Allocation concealment (selection bias) Unclear risk Unclear from the study and authors’ replydid not clarify the matter
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Not reported in the study.Authors replied: “outcome assessors weredefinitively blinded with respect to theloading schedule, however the loadingschedule was not under investigation andwe judged that it was not possible to blindfor the outcome measures of interest in thepresent review.”Comment: it remains unclear whether anindependent outcome assessor was used
Incomplete outcome data (attrition bias)All outcomes
High risk All outcome data presented, 2 drop-outsoccurred over a 10-year period in the Steri-Oss group and 3 participants died in theSouthern group, out of 12 participants ineach group
Selective reporting (reporting bias) Low risk No selective reporting identified.
Other bias High risk Most of the failed Steri-Oss implants wereplaced by a surgeon who placed only Steri-Oss implants and who was judged, after-wards, to have insufficient clinical experi-ence, therefore effect of the different im-plant systems is confounded by the differ-ent degree of surgical experience of differ-ent operators
Wennström 2004
Methods 5-year follow-up randomised split-mouth study.
Participants Partially edentulous adults with a previous history of periodontal diseaseTreated in the University of Goteborg, Sweden.51 enrolled and results given for 47.Exclusion criteria: people with inadequate self performed plaque control, insufficientbone volume at the recipient sites (i.e. need for ridge augmentation or sinus lift pro-cedures), uncontrolled diabetes, haemophilia, metabolic bone disorder, history of renalfailure, radiation treatment to the head or neck region, current chemotherapy, pregnancy
97Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wennström 2004 (Continued)
Interventions Group 1: Astra® (Astra Tech AB, Mölndal, Sweden) submerged titanium cylindricalscrews with TiO2-blasted surfaces.Group 2: Astra® (Astra Tech AB, Mölndal, Sweden) submerged titanium cylindricalscrews with turned surfaces supporting screw-retained partial fixed prostheses
Outcomes Prosthesis success, implant survival, peri-implant marginal bone level changes, prostheticcomplications, plaque score, bleeding sites, probing pocket depth, width of the kera-tinised mucosa
Notes Authors did not disclose how many implants with a turned or a TiO2-blasted surfacewere placed and reported the data of the various outcomes combined for both implanttypes, rendering the comparison of the 2 surfaces meaningless
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
High risk Study reported: “Each patient received aminimum of two implants, and by ran-domization every second implant that wasinstalled had been designed with a ma-chined surface and the remaining with aroughened Tioblast surface.”No reply to letter.Comment: this method of allocation deter-mines an imbalanced number of implantsof the 2 different types
Allocation concealment (selection bias) Low risk Study reported: “The randomization codefor the single patient was made available forthe operator first after he had completedpreparation of the recipient sites.”
Blinding (performance bias and detectionbias)All outcomes
Unclear risk Unclear from the study.No reply to letter.
Incomplete outcome data (attrition bias)All outcomes
Unclear risk 4 withdrawals after 2, 3 and 4 years, 3 due toparticipant death and 1 because the partic-ipant did not come back. Unclear whetherprostheses were removed to assess implantmobility and, for this reason, the studycould be used only to answer the first partof the secondary objectiveNo reply to letter.
Selective reporting (reporting bias) High risk Authors did not disclose how many im-plants with a turned or a TiO2-blasted sur-
98Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wennström 2004 (Continued)
face were placed and reported the data ofthe various outcomes combined for bothimplant types, rendering the comparison ofthe 2 surfaces meaningless. No reply to ourletter for requesting more details
Other bias Low risk No other biases identified.
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Abtahi 2012 Follow-up < 1 year post-loading.
Boerrigter 1997 The number of participants at entry in each group changed during the 10-year follow-up. Implant stabilitywas not assessed. The authors did not reply to our letter
Canullo 2012 The prostheses were permanently cemented on the implants.Authors replied: “the implant restorations were not removed to assess mobility after 1 year.”Individual implant stability could not be assessed.
Cehreli 2010 The author informed us that this was a retrospective study.
da Cunha 2004 Follow-up < 1 year post-loading.
Du Preez 2007 Quasi-randomised trial.
Esposito 2013b Follow-up < 1 year post-loading, but the trial is ongoing.
Friberg 1992 Study classified as not a randomised controlled trial after author’s reply
Friberg 2003 Quasi-randomised trial.
Geertman 1996 Data of 2 different randomised controlled trials were combined. Asked for separate data. No reply to letter
Geurs 2002 Unclear which implant type(s) failed and number of drop-outs. Author’s reply did not clarify the issue
Gher 1994 Problems with design and analysis. The unit of randomisation was both the participant and the implantand it was not possible to use the data without further information from authors. The authors did notreply to our letter
Goené 2007 Experimental mini-titanium implants placed in humans and removed for histology 4-8 weeks after un-loaded healing
99Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Gultekin 2013 Some prostheses were permanently cemented on the implants.Authors replied: “It was not possible to check implants separately after loading as to whether they weremobile or not because all restorations were cemented.”Individual implant stability could not be assessed.
Joly 2003 Follow-up < 1 year post-loading.
Jones 1997 Study judged not to be a randomised controlled trial. No reply to letter
Kadkhodazadeh 2013 Study judged not to be a randomised controlled trial due to unbalanced placements of different implanttypes. No reply to letter
Kang 2012 It was uncertain whether the adjacent implants were splinted or not, and whether the restorations wereremoved to assess stability. No reply to our letter
Karabuda 2002 Study classified as not a randomised controlled trial after author’s reply
Karlsson 1998 Not all participants were participating in a split-mouth study. Author’s reply did not clarify the issue
Kemppainen 1997 1 group of participants received 1 implant type whereas the other group received implants of the samebrand but with different shapes (ITI hollow cylinders or screws)
Khang 2001 Implant stability only assessed at delivery of final prosthesis on fixed prostheses and overdentures and notat later follow-up with removed prosthesis. Type of ’split-mouth’ study with unequal number of implantsrandomly allocated to each participant. Author had no time to re-analyse data
Kim 2010 Trial described as a randomised controlled trial; however, authors reported the following: “The mesiodistallocation of each implants were randomly determined. However, because of the difference in coronaldiameter of fixtures, mostly S were implanted mesial to C.”We interpret this as the trial being not truly randomised.
Liaje 2012 Implant stability was not assessed.The authors reported: “The prosthesis were cemented after the fabrication and the implant stability wasnot assessed at 1 year.”
Liddelow 2010 ’Risky’ trial comparing 2 different single implants immediately loaded with a mandibular overdenture.The study was discontinued due to excessive implant failures
Mackie 2011 Compilation of various randomised controlled trials evaluating different implant systems (Steri-Oss, South-ern, Straumann, Brånemark) and loading protocols of 2, 6 and 12 weeks. Some of these trials are alreadyincluded in the present review
Mau 2002 Unusually high drop-out rate often for questionable reasons (only data of 189 of the 313 participantsadmitted in the trial were presented). Early failures counted as drop-outs. Unclear success criteria. Unclearfollow-up periods. We were unable to extract any meaningful data. No reply to letter
100Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Mau 2003 Problem as number of implants was confounded with implant type: participants having an overdenturesupported by 2 IMZ cylinders were compared with participants with an overdenture supported by 4 ITITPS screws
Nickenig 2009 Quasi-randomised trial. Unclear randomisation procedure.
Oates 2007 Follow-up < 1 year post-loading.
Orsini 2007 Trial evaluating experimental implants placed in humans and retrieved 2 months after placement forhistological evaluation
Park 2010 Follow-up < 1 year post-loading.
Peñarrocha-Diago 2012 It was unclear from the study whether the prosthesis were removed to assess implant stabilityAuthors responded: “due to the absence of clinical symptoms or radiological signs that indicate problemsin those splinted implants, we saw unjustified the removal of the fixed prostheses of those splinted implantsby bar/bridges. So at 12 months of loading, mobility was not assessed in those splinted implants.”We did not consider this was acceptable since it has been demonstrated that implants can be mobile evenin absence of radiographic signs
Piao 2009 Implant stability not recorded, radiographic baseline used was set at loading and not at implant placement.No reply to letter
Reingewirtz 2000 Study classified as not a randomised controlled trial since only one Calcitek implant was compared with23 Microdent. Not written to authors
Rocci 2003 Not a randomised controlled trial but quasi-randomised trial with alternate assignment
Roccuzzo 2001 Problem as time of implant loading was confounded with implant type: ITI SLA implants healed for 6weeks, whereas ITI TPS implants healed for 12 weeks. Mobile implants not considered failures
Sanz 2010 Follow-up < 1 year post-loading. Unclear numbers of participants within each group
Schätzle 2009 Trial evaluating different palatal implants for orthodontic anchorage and not dental implant for supportingdental prostheses
Shibli 2010 Trial evaluating experimental implants placed in humans and retrieved 2 months after placement forhistological evaluation
Shin 2006 Number of enrolled participants unclear. No reply to letter.
Stavropoulos 2007 Implant stability could not be assessed because prostheses were permanently cemented
Tallarico 2011 There was a confounding factor of a 1-stage vs. 2-stage approach as the primary objective of the trial
Tan 2010 The stability of individual implants was not assessed with the removed prostheses
101Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Testori 2003 Problem as implant types: Osseotite and Osseotite NT were confounded with early and immediate loading
Thoma 2014 Some prostheses were permanently cemented on the implants.Authors replied: “Some implants were splinted (as being part of a fixed partial prostheses), single implantsnext to each other were not splinted. Splinted implant prostheses were not removed.”Individual implant stability could not be assessed.
Tomatis 2002 Study classified as not a randomised controlled trial after author’s reply
Truhlar 1997 Due to the extreme complexity of the study design, we were unable to extract any meaningful data. Noreply to letter
Tymstra 2011 Implants having identical surface and material with different shapes that were positioned in a differentway
Van Assche 2012 It was unclear from the study whether the prosthesis were removed to assess implant stabilityAuthors responded: “Only if radiographic signs indicated a possibility of implant mobility.”We did not consider this was acceptable since it has been demonstrated that implants can be mobile evenin absence of radiographic signs. There was also a difference in number of participants and the failures ofimplants between different reports
Van Steenberghe 2000 Split-mouth design. Outcome data of a certain number of implants were not reported
Zetterqvist 2010 Participants had sites randomly assigned to have implants with different surfaces. This generated a trialthat has not a parallel group or a split-mouth design and we are unable to use this type of data. Data onimplant failures were not presented either
Åstrand 2003 Parallel group study in which participants in the test group received Brånemark Mark IV implants in bonequality type 3 and 4 and Brånemark Mark II or standard implants in bone quality type 1 and 2. Participantsin the control group received Brånemark standard or Mark II implants in all bone quality types. In orderto use the data, we needed only data of implants placed in bone quality type 3 and 4. Written to the authorwho was unable to provide data in the appropriate form
102Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Different implant systems: Brånemark turned versus ITI TPS hollow titanium screws
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 Implant failure: 1 year 2 99 Risk Ratio (M-H, Fixed, 95% CI) 1.64 [0.22, 12.01]2 Implant failure: 3 years 2 96 Risk Ratio (M-H, Fixed, 95% CI) 2.38 [0.37, 15.38]3 Implant failure: 5 years 1 54 Risk Ratio (M-H, Fixed, 95% CI) 3.0 [0.13, 70.53]4 Implant failure: 10 years 1 54 Risk Ratio (M-H, Fixed, 95% CI) 3.0 [0.13, 70.53]
Comparison 2. Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 Implant failure: 1 year 2 48 Risk Ratio (M-H, Fixed, 95% CI) 0.14 [0.02, 1.08]2 Implant failure: 3 years 2 47 Risk Ratio (M-H, Fixed, 95% CI) 0.14 [0.02, 1.06]3 Implant failure: 5 years 2 46 Risk Ratio (M-H, Fixed, 95% CI) 0.14 [0.02, 1.08]4 Implant failure: 10 years 2 39 Risk Ratio (M-H, Fixed, 95% CI) 0.14 [0.02, 1.10]
Comparison 3. Turned versus roughened implants
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 Early implant failure 7 404 Risk Ratio (M-H, Random, 95% CI) 2.79 [0.87, 8.90]2 Peri-implantitis 4 Risk Ratio (Random, 95% CI) 0.80 [0.67, 0.96]
103Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.1. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium
screws, Outcome 1 Implant failure: 1 year.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 1 Different implant systems: Br nemark turned versus ITI TPS hollow titanium screws
Outcome: 1 Implant failure: 1 year
Study or subgroup Branemark ITI Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Batenburg 1998 1/30 0/29 33.7 % 2.90 [ 0.12, 68.50 ]
Moberg 2001 1/20 1/20 66.3 % 1.00 [ 0.07, 14.90 ]
Total (95% CI) 50 49 100.0 % 1.64 [ 0.22, 12.01 ]Total events: 2 (Branemark), 1 (ITI)
Heterogeneity: Chi2 = 0.25, df = 1 (P = 0.61); I2 =0.0%
Test for overall effect: Z = 0.49 (P = 0.63)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Branemark Favours ITI
Analysis 1.2. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium
screws, Outcome 2 Implant failure: 3 years.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 1 Different implant systems: Br nemark turned versus ITI TPS hollow titanium screws
Outcome: 2 Implant failure: 3 years
Study or subgroup Branemark ITI Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Batenburg 1998 1/30 0/29 34.3 % 2.90 [ 0.12, 68.50 ]
Moberg 2001 2/18 1/19 65.7 % 2.11 [ 0.21, 21.32 ]
Total (95% CI) 48 48 100.0 % 2.38 [ 0.37, 15.38 ]Total events: 3 (Branemark), 1 (ITI)
Heterogeneity: Chi2 = 0.03, df = 1 (P = 0.87); I2 =0.0%
Test for overall effect: Z = 0.91 (P = 0.36)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Branemark Favours ITI
104Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium
screws, Outcome 3 Implant failure: 5 years.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 1 Different implant systems: Br nemark turned versus ITI TPS hollow titanium screws
Outcome: 3 Implant failure: 5 years
Study or subgroup Branemark ITI Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Batenburg 1998 1/27 0/27 100.0 % 3.00 [ 0.13, 70.53 ]
Total (95% CI) 27 27 100.0 % 3.00 [ 0.13, 70.53 ]Total events: 1 (Branemark), 0 (ITI)
Heterogeneity: not applicable
Test for overall effect: Z = 0.68 (P = 0.50)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Branemark Favours ITI
105Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.4. Comparison 1 Different implant systems: Brånemark turned versus ITI TPS hollow titanium
screws, Outcome 4 Implant failure: 10 years.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 1 Different implant systems: Br nemark turned versus ITI TPS hollow titanium screws
Outcome: 4 Implant failure: 10 years
Study or subgroup Branemark ITI Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Batenburg 1998 1/27 0/27 100.0 % 3.00 [ 0.13, 70.53 ]
Total (95% CI) 27 27 100.0 % 3.00 [ 0.13, 70.53 ]Total events: 1 (Branemark), 0 (ITI)
Heterogeneity: not applicable
Test for overall effect: Z = 0.68 (P = 0.50)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Branemark Favours ITI
Analysis 2.1. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus
Steri-Oss, Outcome 1 Implant failure: 1 year.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss
Outcome: 1 Implant failure: 1 year
Study or subgroup Southern Steri-Oss Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tawse-Smith 2001 0/12 1/12 21.4 % 0.33 [ 0.01, 7.45 ]
Tawse-Smith 2002 0/12 5/12 78.6 % 0.09 [ 0.01, 1.48 ]
Total (95% CI) 24 24 100.0 % 0.14 [ 0.02, 1.08 ]Total events: 0 (Southern), 6 (Steri-Oss)
Heterogeneity: Chi2 = 0.39, df = 1 (P = 0.53); I2 =0.0%
Test for overall effect: Z = 1.88 (P = 0.059)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Southern Favours Steri-Oss
106Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus
Steri-Oss, Outcome 2 Implant failure: 3 years.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss
Outcome: 2 Implant failure: 3 years
Study or subgroup Southern Steri-Oss Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tawse-Smith 2001 0/12 1/11 22.1 % 0.31 [ 0.01, 6.85 ]
Tawse-Smith 2002 0/12 5/12 77.9 % 0.09 [ 0.01, 1.48 ]
Total (95% CI) 24 23 100.0 % 0.14 [ 0.02, 1.06 ]Total events: 0 (Southern), 6 (Steri-Oss)
Heterogeneity: Chi2 = 0.34, df = 1 (P = 0.56); I2 =0.0%
Test for overall effect: Z = 1.90 (P = 0.057)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Southern Favours Steri-Oss
Analysis 2.3. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus
Steri-Oss, Outcome 3 Implant failure: 5 years.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss
Outcome: 3 Implant failure: 5 years
Study or subgroup Southern Steri-Oss Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tawse-Smith 2001 0/11 1/11 21.4 % 0.33 [ 0.02, 7.39 ]
Tawse-Smith 2002 0/12 5/12 78.6 % 0.09 [ 0.01, 1.48 ]
Total (95% CI) 23 23 100.0 % 0.14 [ 0.02, 1.08 ]Total events: 0 (Southern), 6 (Steri-Oss)
Heterogeneity: Chi2 = 0.39, df = 1 (P = 0.53); I2 =0.0%
Test for overall effect: Z = 1.89 (P = 0.059)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Southern Faviurs Steri-Oss
107Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.4. Comparison 2 Different implant systems: Southern blasted/etched titanium screws versus
Steri-Oss, Outcome 4 Implant failure: 10 years.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 2 Different implant systems: Southern blasted/etched titanium screws versus Steri-Oss
Outcome: 4 Implant failure: 10 years
Study or subgroup Southern Steri-Oss Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tawse-Smith 2001 0/11 1/9 23.8 % 0.28 [ 0.01, 6.10 ]
Tawse-Smith 2002 0/9 5/10 76.2 % 0.10 [ 0.01, 1.59 ]
Total (95% CI) 20 19 100.0 % 0.14 [ 0.02, 1.10 ]Total events: 0 (Southern), 6 (Steri-Oss)
Heterogeneity: Chi2 = 0.24, df = 1 (P = 0.62); I2 =0.0%
Test for overall effect: Z = 1.87 (P = 0.061)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours Southern Favours Steri-Oss
108Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Turned versus roughened implants, Outcome 1 Early implant failure.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 3 Turned versus roughened implants
Outcome: 1 Early implant failure
Study or subgroup Turned Roughened Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Batenburg 1998 1/30 1/60 18.0 % 2.00 [ 0.13, 30.88 ]
Astrand 1999 3/33 1/33 27.5 % 3.00 [ 0.33, 27.38 ]
Moberg 2001 1/20 0/20 13.6 % 3.00 [ 0.13, 69.52 ]
Astrand 2002 1/28 0/28 13.5 % 3.00 [ 0.13, 70.64 ]
Wennstrom 2004 1/51 0/51 13.3 % 3.00 [ 0.13, 71.96 ]
Froberg 2006 0/15 0/15 Not estimable
Schincaglia 2007 1/10 0/10 14.1 % 3.00 [ 0.14, 65.90 ]
Total (95% CI) 187 217 100.0 % 2.79 [ 0.87, 8.90 ]Total events: 8 (Turned), 2 (Roughened)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.07, df = 5 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 1.73 (P = 0.083)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours turned Favours roughened
109Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Turned versus roughened implants, Outcome 2 Peri-implantitis.
Review: Interventions for replacing missing teeth: different types of dental implants
Comparison: 3 Turned versus roughened implants
Outcome: 2 Peri-implantitis
Study or subgroup log [Risk Ratio] Risk Ratio Weight Risk Ratio
(SE) IV,Random,95% CI IV,Random,95% CI
Astrand 1999 -1.61 (1.53) 0.3 % 0.20 [ 0.01, 4.01 ]
Moberg 2001 -1.14 (1.11) 0.6 % 0.32 [ 0.04, 2.82 ]
Astrand 2002 -0.21 (0.09) 98.6 % 0.81 [ 0.68, 0.97 ]
Schincaglia 2007 0 (1.34) 0.4 % 1.00 [ 0.07, 13.82 ]
Total (95% CI) 100.0 % 0.80 [ 0.67, 0.96 ]Heterogeneity: Tau2 = 0.0; Chi2 = 1.55, df = 3 (P = 0.67); I2 =0.0%
Test for overall effect: Z = 2.46 (P = 0.014)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours turned Favours roughened
A D D I T I O N A L T A B L E S
Table 1. Results from trials comparing different implant surfaces (five trials)
Comparison Outcome Data Effect estimate (95% CI)P value
Brånemark Mark III implants:turned versus oxidised surface(TiUnite)(Fröberg 2006)Split-mouth
Implant failure (1 year) No failures -
Brånemark Mark IV implants:turned versus oxidised surface(TiUnite)(Schincaglia 2007)Split-mouth
Failure Turned 0/10Oxidised 1/10
RR 0.33 (0.82 to 7.32)P value = 0.49
Bone level (1 year) Turned 1.06 ± 0.618 mmOxidised 0.92 ± 0.649 mm
MD 0.11 (-0.38 to 0.60)P value = 0.66
Bone level (3 years) - MD -0.15 (-0.56 to 0.26)P value = 0.48
110Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
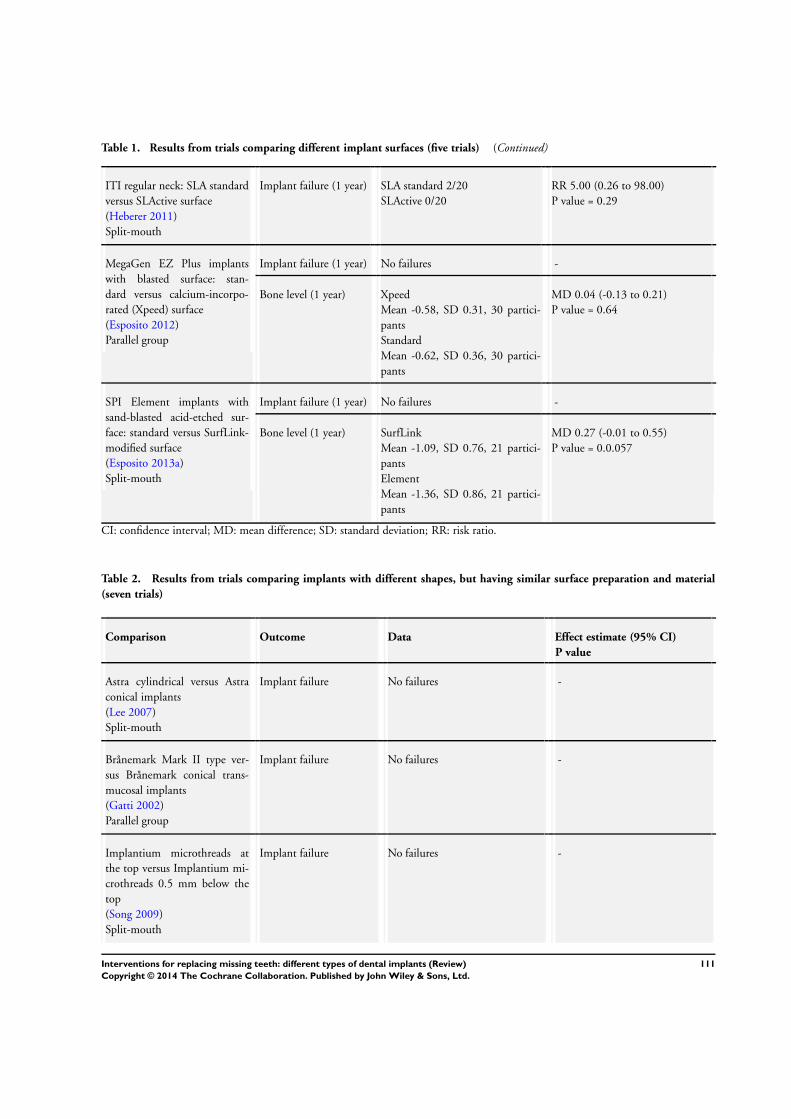
Table 1. Results from trials comparing different implant surfaces (five trials) (Continued)
ITI regular neck: SLA standardversus SLActive surface(Heberer 2011)Split-mouth
Implant failure (1 year) SLA standard 2/20SLActive 0/20
RR 5.00 (0.26 to 98.00)P value = 0.29
MegaGen EZ Plus implantswith blasted surface: stan-dard versus calcium-incorpo-rated (Xpeed) surface(Esposito 2012)Parallel group
Implant failure (1 year) No failures -
Bone level (1 year) XpeedMean -0.58, SD 0.31, 30 partici-pantsStandardMean -0.62, SD 0.36, 30 partici-pants
MD 0.04 (-0.13 to 0.21)P value = 0.64
SPI Element implants withsand-blasted acid-etched sur-face: standard versus SurfLink-modified surface(Esposito 2013a)Split-mouth
Implant failure (1 year) No failures -
Bone level (1 year) SurfLinkMean -1.09, SD 0.76, 21 partici-pantsElementMean -1.36, SD 0.86, 21 partici-pants
MD 0.27 (-0.01 to 0.55)P value = 0.0.057
CI: confidence interval; MD: mean difference; SD: standard deviation; RR: risk ratio.
Table 2. Results from trials comparing implants with different shapes, but having similar surface preparation and material(seven trials)
Comparison Outcome Data Effect estimate (95% CI)P value
Astra cylindrical versus Astraconical implants(Lee 2007)Split-mouth
Implant failure No failures -
Brånemark Mark II type ver-sus Brånemark conical trans-mucosal implants(Gatti 2002)Parallel group
Implant failure No failures -
Implantium microthreads atthe top versus Implantium mi-crothreads 0.5 mm below thetop(Song 2009)Split-mouth
Implant failure No failures -
111Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Results from trials comparing implants with different shapes, but having similar surface preparation and material(seven trials) (Continued)
ITI cylindrical versus ITI ta-pered implants(Lang 2007)Parallel group
Implant failure No failures -
NobelActive external connec-tion versus NobelActive inter-nal connection implants(Kielbassa 2009)Parallel group
Implant failure (1 year) Internal 4/63External 3/50
RR 1.06 (0.25 to 4.51)P value = 0.94
Implant failure (3 years) Internal 3/41External 5/45
RR 0.66 (0.17 to 2.58)P value = 0.55
Bone level (1 year) InternalMean 0.89, SD 1.36, 53 partici-pantsExternalMean 0.59, SD 0.98, 44 partici-pants
MD 0.30 (-0.17 to 0.77)P value = 0.21
NobelActive external connec-tion versus NobelReplace im-plants(Kielbassa 2009)Parallel group
Implant failure (1 year) External 3/50NobelReplace 5/56
RR 0.67 (0.17 to 2.67)P value = 0.57
Implant failure (3 years) External 3/41NobelReplace 3/41
RR 1.00 (0.21 to 4.67)P value = 1.00
Bone level (1 year) ExternalMean 0.59, SD 0.98, 44 partici-pantsNobelReplaceMean 0.59, SD 0.98, 44 partici-pants
MD 0.00 (-0.41 to 0.41)P value = 1.00
NobelActive internal connec-tion versus NobelReplace im-plants(Kielbassa 2009)Parallel group
Implant failure (1 year) Internal 3/50NobelReplace 5/56
RR 0.90 (0.25 to 3.15)P value = 0.86
Implant failure (3 years) Internal 3/41NobelReplace 3/41
RR 1.00 (0.21 to 4.67)P value = 1.00
Bone level (1 year) InternalMean 0.89, SD 1.36, 53 partici-pantsNobelReplaceMean 0.59, SD 0.98, 44 partici-pants
MD 0.30 (-0.17 to 0.77)P value = 0.21
NobelAc-tive internal connection versusNobel Speedy Groovy externalconnection implants(Pozzi 2014)
Bone level (1 year) NobelActiveMean 0.51, SD 0.34, 34 partici-pantsNobel Speedy Groovy
MD -0.59 (-0.74 to -0.44)P value < 0.001
112Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Results from trials comparing implants with different shapes, but having similar surface preparation and material(seven trials) (Continued)
Split-mouth Mean1.10, SD 0.52, 34 partici-pantsAnalysis assumes correlation of 0.5
WINSIX cylindrical versusWINSIX tapered implants(Prosper 2009)Split-mouth
Implant failure (1 year) Cylindrical 4/66Tapered 2/66
RR 2.00 (0.38 to 10.58)P value = 0.41
CI: confidence interval; MD: mean difference; RR: risk ratio; SD: standard deviation.
Table 3. Results from trials comparing implants with different materials, but having similar surface preparation and shape(one trial)
Comparison Outcome Data Effect estimate (95% CI)P value
ITA SLActive implants: tita-nium grade 4 versus titanium-13zirconium (Roxolid)(Al-Nawas 2012)Split-mouth
Implant failure (1 year) SLActive 2/89Roxolid 1/89
RR 2.00 (0.18 to21.66)P value = 0.57
CI: confidence interval; RR: risk ratio.
Table 4. Results from trials comparing implants with different surface preparation, shape, material or a combination (13 trials)
Comparison Outcome Data Effect estimate (95% CI)Pvalue
Ankylos Plus Dentsply versusSeven Sweden & Martina im-plants(Crespi 2009)Parallel group
Implant failure No failures -
Bone level (1 year) InternalMean 0.20, SD 0.58, 21 partic-ipantsReplaceMean 0.17, SD 0.54, 27 partic-ipants
MD 0.03 (-0.29 to 0.35)P value = 0.85
Astra TiO2-blast cylindricalversus turned Brånemark MarkII implants(Astrand 1999)Parallel group
Implant failure (1 year) Astra 1/33Brånemark 4/33
RR 0.25 (0.03 to 2.12)P value = 0.20
113Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 4. Results from trials comparing implants with different surface preparation, shape, material or a combination (13 trials)(Continued)
Implant failure (3 years) Astra 2/33Brånemark 5/33
RR 0.40 (0.08 to 1.92)P value = 0.25
Implant failure (5 years) Astra 2/31Brånemark 5/33
RR 0.43 (0.09 to 2.04)P value = 0.28
Bone level (1 year) AstraMean -0.26, SD 0.60, 32 par-ticipantsBrånemarkMean -0.17, SD 0.37, 33 par-ticipants
MD -0.09 (-0.33 to 0.15)P value = 0.47
Bone level (3 years) AstraMean -0.23, SD 0.88, 32 par-ticipantsBrånemarkMean -0.17, SD 0.44, 33 par-ticipants
MD -0.06 (-0.40 to 0.28)P value = 0.73
Bone level (5 years) AstraMean -0.23, SD 0.88, 31 par-ticipantsBrånemarkMean -0.17, SD 0.44, 33 par-ticipants
MD -0.06 (-0.40 to 0.28)P value = 0.73
Astra TiO2-blast versus ITISLA titanium implants(Akoglu 2011)Parallel group
Implant failure No failures -
Astra TiO2-blast versus Swiss-Plus (Zimmer) cylindrical im-plants(Akoglu 2011)Parallel group
Implant failure No failures -
Brånemark versus IMZ im-plants(Batenburg 1998)Parallel group
Implant failure (1 year) Brånemark 1/30IMZ 1/30
RR 1.00 (0.07 to 15.26)P value = 1.00
Implant failure (3 years) Brånemark 1/30IMZ 1/30
RR 1.00 (0.07 to 15.26)P value = 1.00
Implant failure (5 years) Brånemark 1/27IMZ 1/30
RR 1.11 (0.07 to 16.91)P value = 0.94
114Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 4. Results from trials comparing implants with different surface preparation, shape, material or a combination (13 trials)(Continued)
Implant failure (10 years) Brånemark 1/27IMZ 4/29
RR 0.27 (0.03 to 2.25)P value = 0.23
Brånemark MKII versus ITITPS hollow screw implants-(Batenburg 1998; Moberg2001)Parallel group
Implant failure (1 and 3 years) - Pooled RR at 3 years 2.38 (0.13to 70.53)P value = 0.50
Brånemark MKII versus ITITPS hollow screw implants-(Batenburg 1998)Parallel group
Implant failure (5 years) Brånemark 1/27ITI 0/27
RR 3.00 (0.37 to 15.38)P value = 0.36
Brånemark MKII versus ITITPS hollow screw implants-(Batenburg 1998)Parallel group
Implant failure (10 years) Brånemark 1/27ITI 0/27
RR 3.00 (0.37 to 15.38)P value = 0.36
Brånemark MKII versus ITITPS solid screw implants(Astrand 2002)Split-mouth
Implant failure (3 years) Brånemark 1/28ITI 2/28 (assume parallel foranalysis)
RR 0.05 (0.05 to 5.20)P value = 0.56
Brånemark MKIV TiUnite ver-sus Southern regular implants(Payne 2004)Parallel group
Implant failure (1 year) Brånemark 4/19Southern 7/19
RR 0.57 (0.20 to 1.63)P value = 0.30
IMZ titanium TPS versus ITITPS hollow implants(Batenburg 1998)Parallel group
Implant failure (1 year) IMZ 1/30ITI 0/29
RR 2.90 (0.12 to 68.50)P value = 0.51
Implant failure (3 years) IMZ 1/30ITI 0/29
RR 2.90 (0.12 to 68.50)P value = 0.51
Implant failure (5 years) IMZ 1/30ITI 0/27
RR 2.71 (0.12 to 63.84)P value = 0.54
Implant failure (10 years) IMZ 4/29ITI 0/27
RR 8.40 (0.47 to 149.04)P value = 0.15
115Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 4. Results from trials comparing implants with different surface preparation, shape, material or a combination (13 trials)(Continued)
IMZ titanium TPS versus ITITPS solid implants(Heydenrijk 2002)Parallel group
Implant failure (1 year) IMZ 1/20ITI 0/20
RR 3.00 (0.13 to 69.52)P value = 0.49
Implant failure (3 years) IMZ 1/20ITI 0/19
RR 3.00 (0.13 to 69.52)P value= 0.49
Implant failure (5 years) IMZ 1/19ITI 0/18
RR 2.85 (0.12 to 65.74)P value = 0.51
ITI SLA versus Southern im-plants(Payne 2003)Parallel group
Implant failure (10 years) No failures -
Bone change (1 year) ITI TPSMean 0.26, SD 0.23, 12 partic-ipantsSouthernMean 0.28, SD 0.15, 12 partic-ipants
MD -0.02 (-0.18 to 0.14)P value = 0.80
Bone change (3 years) ITI TPSMean 0.26, SD 0.23, 10 partic-ipantsSouthernMean 0.24, SD 0.18, 11 partic-ipants
MD 0.02 (-0.20 to 0.24)P value = 0.86
Bone change (5 years) ITI TPSMean 0.47, SD 0.46, 10 partic-ipantsSouthernMean 0.30, SD 0.36, 10 partic-ipants
MD 0.17 (-0.19 to 0.53)P value = 0.36
Bone change (10 years) ITI TPSMean 0.33, SD 0.55, 9 partici-pantsSouthernMean 0.41, SD 0.58, 9 partici-pants
MD -0.08 (-0.60 to 0.44)P value = 0.76
ITI SLA titanium implants ver-sus SwissPlus (Zimmer) cylin-drical implants(Akoglu 2011)Parallel group
Implant failure (5 years) No failures -
116Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 4. Results from trials comparing implants with different surface preparation, shape, material or a combination (13 trials)(Continued)
NobelReplace Select Taperedversus NobelReplace Groovyimplants(den Hartog 2011)Parallel group
Implant failure (1 year) NobelReplace Select 1/31NobelReplace Groovy 0/31
RR 3.00 (0.13 to 70.92)P value = 0.50
Bone level (1 year) AstraMean 1.19, SD 0.82, 31 partic-ipantsBrånemarkMean 0.9, SD 0.57, 31 partici-pants
MD 0.29 (-0.06 to 0.64)P value = 0.11
Southern regular versus Steri-Oss implants(Tawse-Smith 2001; Tawse-Smith 2002)Parallel group
Implant failure (1, 3, 5 and 10years)
- -
Southern regular versus turnedNeoss implants(Alsabeeha 2011)Parallel group
Implant failure (1 year) Southern Regular 1/11Neoss 0/12
RR 3.25 (0.15 to 72.36)P value = 0.46
Southern wide versus turnedNeoss implants(Alsabeeha 2011)Parallel group
Implant failure (1 year) No failures -
Southern regular versus South-ern wide(Alsabeeha 2011)Parallel group
Implant failure (1 year) Southern regular 1/11Southern wide 0/12
RR 3.25 (0.15 to 72.36)P value = 0.46
CI: confidence interval; MD: mean difference; SD: standard deviation; RR: risk ratio.
Table 5. Results from trials comparing turned and roughened surfaces
Comparison Outcome Data Effect estimate (95% CI)P value
Turned versus roughened sur-faces(Batenburg 1998; Astrand1999; Astrand 2002; Moberg
Implants affected by peri-im-plantitis (3 years)(Astrand 1999; Astrand 2002;Moberg 2001; Schincaglia
4 trials Pooled RR 0.80 (0.67 to 0.96)P value = 0.01
117Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 5. Results from trials comparing turned and roughened surfaces (Continued)
2001; Schincaglia 2007)3 parallel group and 2 split-mouth
2007)
Implants affected by peri-im-plantitis (5 years)(Astrand 1999)
Turned 0/33Roughened 1/31
RR 0.31 (0.01 to 7.42)P value = 0.47
Implants lost for peri-implanti-tis (10 years)(Batenburg 1998)
Turned 0/27Roughened 3/29
RR 0.15 (0.01 to 2.83)P value = 0.21
CI: confidence interval; RR: risk ratio.
A P P E N D I C E S
Appendix 1. MEDLINE (OVID) search strategy
1. exp Dental Implants/2. exp Dental Implantation/ or dental implantation3. exp Dental Prosthesis, Implant-Supported/4. ((osseointegrated adj implant$) and (dental or oral))5. dental implant$6. (implant$ adj5 dent$)7. (((overdenture$ or crown$ or bridge$ or prosthesis or restoration$) adj5 (Dental or oral)) and implant$)8. “implant supported dental prosthesis”9. (“blade implant$” and (dental or oral))10. ((endosseous adj5 implant$) and (dental or oral))11. ((dental or oral) adj5 implant$)12. OR/1-11The above subject search was linked to the Cochrane Highly Sensitive Search Strategy (CHSSS) for identifying randomised trials inMEDLINE: sensitivity maximising version (2008 revision) as referenced in Chapter 6.4.11.1 and detailed in box 6.4.c of the CochraneHandbook for Systematic Reviews of Interventions, Version 5.1.0 (Higgins 2011).1. randomized controlled trial.pt.2. controlled clinical trial.pt.3. randomized.ab.4. placebo.ab.5. drug therapy.fs.6. randomly.ab.7. trial.ab.8. groups.ab.9. or/1-810. exp animals/ not humans.sh.
118Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

11. 9 not 10
Appendix 2. EMBASE (OVID) search strategy
1. tooth implantation/2. ((implant-supported or implant$) adj support$).mp.3. ((osseointegrated adj implant$) and (dental or oral)).mp.4. ((dental implant$ or dental-implant or implant$) adj (dent$ or oral or tooth)).mp.5. (((overdenture$ or crown$ or bridge$ or prosthesis or prostheses or restoration$) adj5 (dental or oral)) and implant$).mp.6. “implant supported dental prosthesis”.mp.7. (“blade implant$” and (dental or oral or tooth or teeth)).mp.8. ((endosseous adj5 implant$) and (dental or oral or tooth or teeth)).mp.9. ((dental or oral or tooth or teeth) and implant$).mp.10. or/1-9The EMBASE subject search was run with the Cochrane Oral Health Group search strategy for identifying randomised controlledtrials in EMBASE:1. random$.ti,ab.2. factorial$.ti,ab.3. (crossover$ or cross over$ or cross-over$).ti,ab.4. placebo$.ti,ab.5. (doubl$ adj blind$).ti,ab.6. (singl$ adj blind$).ti,ab.7. assign$.ti,ab.8. allocat$.ti,ab.9. volunteer$.ti,ab.10. CROSSOVER PROCEDURE.sh.11. DOUBLE-BLIND PROCEDURE.sh.12. RANDOMIZED CONTROLLED TRIAL.sh.13. SINGLE BLIND PROCEDURE.sh.14. or/1-1315. (exp animal/ or animal.hw. or nonhuman/) not (exp human/ or human cell/ or (human or humans).ti.)16. 14 NOT 15
Appendix 3. The Cochrane Oral Health Group’s Trials Register search strategy
Updated searches were undertaken using the Cochrane Register of Studies and the search strategy below from January 2013:#1 (“dental implant*” or “oral implant*” or “implant support*” or “endosseous implant*” or “blade implant*”) AND (INREGISTER)#2 ((implant* and (oral or dental))) AND (INREGISTER)#3 (“subperiosteal implant*”) AND (INREGISTER)#4 (implant* AND overdenture*) AND (INREGISTER)#5 (((overdenture* OR crown* OR bridge* OR prosthesis OR prostheses OR restoration*) AND (“dental implant*” OR “Oral implant”OR (zygoma* AND implant*)))) AND (INREGISTER)#6 (#1 or #2 or #3 or #4 or #5) AND (INREGISTER)Previous searches of the Register were undertaken using the Procite software and the search strategy below:
(dental-implants OR “dental implant*” OR “oral implant*” OR dental-implantation OR dental-prosthesis-implant-supported OR“implant supported” OR “implant supported prosthesis” OR dental-implantation-endosseous-endodontic OR “endosseous implant*”OR blade-implantation OR “blade implant*” OR (implant* AND (oral OR dental)) or dental-implantation-subperiosteal OR “sub-periosteal implant” OR (implant* AND overdenture*) OR ((overdenture* OR crown* OR bridge* OR prosthesis OR prostheses ORrestoration*) AND (“dental implant*” OR “Oral implant” OR (zygoma* AND implant*))))
119Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Appendix 4. The Cochrane Central Register of Controlled Trials (CENTRAL) search strategy
#1 DENTAL IMPLANTS explode all trees (MeSH)#2 DENTAL IMPLANTATION explode all trees (MeSH)#3 DENTAL PROSTHESIS IMPLANT-SUPPORTED single term (MeSH)#4 ((osseointegrat* near implant*) and (dental* or oral*))#5 (dental next implant*)#6 (implant* near dent*)#7 dental-implant*#8 ((overdenture* near dental*) and implant*)#9 ((overdenture* near oral*) and implant*)#10 ((crown* near dental*) and implant*)#11 ((crown* near oral*) and implant*)#12 ((bridge* near dental*) and implant*)#13 ((bridge* near oral*) and implant*)#14 ((prosthesis near dental*) and implant*)#15 ((prosthesis near oral*) and implant*)#16 ((prostheses near dental*) and implant*)#17 ((prostheses near oral*) and implant*)#18 ((restoration* near dental*) and implant*)#19 ((restoration* near oral*) and implant*)#20 (implant next supported next dental next prosthesis)#21 (blade next implant*)#22 ((endosseous near implant*) and dental)#23 ((endosseous near implant*) and oral*)#24 ((dental* near implant*) or (oral* near implant*))#25 (#1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24)
W H A T ’ S N E W
Last assessed as up-to-date: 17 January 2014.
Date Event Description
21 August 2014 Amended Minor edits
H I S T O R Y
Protocol first published: Issue 3, 2002
Review first published: Issue 4, 2002
120Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Date Event Description
18 June 2014 New citation required but conclusions have not changed Review update including 11 new studies; 27 includedstudies in total. Methods have been updated and risk ofbias done on all included studies. Change of authors
4 March 2014 New search has been performed Searches updated to January 2014.
4 June 2008 Amended Converted to new review format.
10 August 2007 New citation required and conclusions have changed Substantive amendment. This update of the review in-cludes four new additional included and three new ex-cluded randomised controlled trials. The follow up ofone previously included study has been prolonged to 5years. The quality assessment section has been simpli-fied. Minor changes to the conclusions
C O N T R I B U T I O N S O F A U T H O R S
Conceiving, designing and coordinating the review (Marco Esposito (ME)).
Developing search strategy and undertaking searches (ME).
Screening search results and retrieved papers against inclusion criteria (ME, Yasmin Ardebili (YA)).
Appraising quality (ME, YA, Helen Worthington (HW)).
Extracting data from papers (ME, HW, YA).
Writing to authors for additional information (ME, HW, YA).
Data management for the review and entering data into Review Manager (HW, ME, YA).
Analysis and interpretation of data (ME, HW).
Writing the review (ME, YA).
Providing general advice on the review (HW).
D E C L A R A T I O N S O F I N T E R E S T
Marco Esposito is working as independent methodological consultant for various implant-related projects for some of the companieswhose implants were used both in included and excluded trials. In particular, he was one of the authors of two of the included and oneof the excluded trials; however, he was not involved in their quality assessment.
Yasmin Ardebili: no interests to declare.
Helen V Worthington: no interests to declare.
121Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S O U R C E S O F S U P P O R T
Internal sources
• School of Dentistry, The University of Manchester, UK.• MAHSC, UK.
The Cochrane Oral Health Group is supported by the Manchester Academic Health Sciences Centre (MAHSC) and the NIHRManchester Biomedical Research Centre.
External sources
• Cochrane Oral Health Group Global Alliance, UK.All reviews in the Cochrane Oral Health Group are supported by Global Alliance member organisations (British Association of OralSurgeons, UK; British Orthodontic Society, UK; British Society of Paediatric Dentistry, UK; British Society of Periodontology, UK;Canadian Dental Hygienists Association, Canada; Mayo Clinic, USA; National Center for Dental Hygiene Research & Practice,USA; New York University College of Dentistry, USA; and Royal College of Surgeons of Edinburgh, UK) providing funding for theeditorial process (http://ohg.cochrane.org/).
• National Institute for Health Research (NIHR), UK.CRG funding acknowledgement:The NIHR is the largest single funder of the Cochrane Oral Health Group.Disclaimer:The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR, NHS or theDepartment of Health.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
None.
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Dental Implantation, Endosseous; ∗Dental Implants; Dental Prosthesis Design; Dental Restoration Failure [statistics & numericaldata]; Jaw, Edentulous [∗rehabilitation]; Jaw, Edentulous, Partially [rehabilitation]; Randomized Controlled Trials as Topic
MeSH check words
Humans
122Interventions for replacing missing teeth: different types of dental implants (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.