Embed Size (px)
Citation preview

10 American Society of Hematology
Erythropoietin: A Paradigm for theDevelopment of Practice Guidelines
J. Douglas Rizzo, Jerome Seidenfeld, Margaret Piper, Naomi Aronson,Alan Lichtin, and Timothy J. Littlewood
Medicare system. It is estimated that sales each year inthe US for oncology indications are about $2.5 billion,with approximately 200,000 patients treated yearly. Thispaper will review the principles of evidence-based medi-cine, which will be applied to the use of epoetin in sub-sequent papers.
The current applications of epoetin are many. Theinitial indication for use by the FDA was in end-stagerenal dialysis patients to decrease transfusion require-ments. The current FDA approved indications for its useare 1) the treatment of anemia associated with chronicrenal failure; 2) the treatment of anemia related to therapywith zidovudine in HIV infected patients; 3) the treat-ment of anemia in patients with non-myeloid malignan-cies where anemia is due to the effect of concomitantlyadministered chemotherapy; and 4) the treatment of ane-mic patients scheduled to undergo elective, non-cardiac,non-vascular surgery to reduce the need for allogeneicblood transfusions, and in patients at high risk for peri-
Erythropoietin (EPO) is an endogenous hormoneproduced in the kidney that regulates red blood cellproduction within the body. Since the cloning andfirst clinical introduction of recombinant erythro-poietin (epoetin) in the late 1980s indications andusage of epoetin have expanded significantly. It isestimated that as many as one third of patients withsubstantial anemia (hemoglobin less than 10.0 g/dL) resulting from chemotherapy for cancer aretreated with epoetin. Though use of epoetin mayavoid the inconvenience and infectious risk ofblood transfusions, it is expensive and its benefit insome clinical scenarios has been modest. Likemany new technologies, strong evidence suggest-ing situations where the benefit is high has laggedbehind its adoption by patients and practitioners.As well, epoetin is expensive and third party payersdo not always reimburse it. Research suggeststhere is considerable variation in epoetin usage inpractice.
To provide guidance to hematology/oncologyspecialists regarding use of epoetin, the AmericanSociety of Hematology (ASH) and the AmericanSociety of Clinical Oncology (ASCO) proposed thatthe Agency for Healthcare Research and Quality(AHRQ) fund an evidence review by one of theEvidence-based Practice Centers (EPC) that wouldbe used to develop evidence-based guidelines formembers of the society. This review highlightsprinciples of evidence-based medicine, distills andappraises the evidence in the published literaturethat supports the use of epoetin, and presentsevidence-based recommendations for use ofepoetin in situations where benefit is substantiatedby high-quality studies. As well, this review ad-dresses some of the difficulties of performingclinical research in this area, provocative researchfindings that will require further study, and sugges-tions regarding epoetin in those areas wherefurther strong evidence has yet to be developed.
I. EVIDENCE-BASED MEDICINE AND EVIDENCE-BASED
PRACTICE GUIDELINES
J. Douglas Rizzo, MD*
Erythropoietin is an endogenous hormone produced inthe kidney that regulates red blood cell production withinthe body. The human gene for erythropoietin was clonedin the early 1980s,1,2 and the recombinant form was de-veloped shortly thereafter. The recombinant alfa formof erythropoietin (epoetin) became available after ap-proval for marketing by the US Food and Drug Admin-istration (FDA) in 1989. Its use has expanded dramati-cally since then. Epoetin rapidly became the mainstayof treatment for anemia of endstage renal disease (ESRD)in the US, somewhat related to its reimbursement by the
*IBMTR/ABMTR, Medical College of Wisconsin, 8701Watertown Plank Road, Milwaukee WI 53226-4801

Hematology 2001 11
operative transfusions with significant, anticipated bloodloss. Its use has grown to include a broad range of appli-cations outside of the indicated clinical settings, includ-ing cancer-related or cancer treatment-related anemia(such as stem cell transplantation), anemia of chronicdisease and sickle cell anemia.
Though epoetin can be effective in reducing ane-mia, and in general is an extremely well tolerated drug,it is not without risks. The most common clinically rel-evant side effect is hypertension, especially in patientswith ESRD.3 Hypertensive encephalopathy, seizures, andthrombotic/vascular events are rare but have been de-scribed.3 Inappropriate erythropoietic stimulation in nor-mal persons (e.g. “doping in athletes”) may be life threat-ening.4,5 In order to maximize the benefit of epoetintherapy and potentially minimize the costs, significantresearch has been done regarding the usage of epoetin.It is our goal in this education session to summarize andappraise the evidence for the use of epoetin in patientswith malignancy, and in doing so provide evidence-basedguidelines for its use, as well as suggestions for researchin areas where strong evidence is currently lacking. Thegoal of this article is to review the value of an evidence-based approach to clinical decision-making and brieflydescribe an approach to critical appraisal of the medicalliterature. The articles that follow will apply the prin-ciples of evidence-based medicine (EBM) to usage ofepoetin in patients with malignant diseases.
What Is Evidence-Based Medicine?Although the term ‘evidence-based medicine’ has re-cently achieved prominence, it reflects principles in epi-demiology and medicine that are not novel. EBM is theconscientious, explicit, and judicious use of current bestevidence in making decisions about the care of individualpatients.6 It combines clinical judgement and experience,best available scientific evidence, and patient preferencesto improve medical decision-making. All componentsof this decision-making triad are important. Clinical ex-perience and judgement are critical to recognizing clini-cal problems, understanding diagnostic testing, estab-lishing accurate diagnoses, identifying treatment alter-natives, and appropriately applying research evidenceto individual patients’ circumstances. Contrary to thecriticism that EBM represents an effort to undermineclinical expertise, many proponents suggest it empha-sizes the importance of good clinical judgement. Thequality and relevance of research evidence to a particu-lar patient’s problems determines its influence on medi-cal decision making. Patient preferences are an impor-tant component of medical decision making. Manifesta-tions of disease, comorbid conditions and value systemsvary widely between individuals, and their preferencesregarding treatment must be included in shared decision-
making. These three components of evidence-based de-cision making are highly interactive. Greater understand-ing of research evidence and patients preferences mayenhance clinical experience and judgement. Realizationof strengths and weaknesses of research evidence islikely to affect physician considerations of patient val-ues. Because evidence-based decision making incorpo-rates clinical judgement, best evidence, and patient pref-erences, it acknowledges that no single “cookbook” ap-proach fits any given patient’s situation.
Why Is Evidence-Based Medicine Important?Many factors appear to be involved in the increasingadoption of the principles of EBM. The desire to pro-vide high quality care in an era of cost containment isone strong factor. Patients, physicians and payers are allinterested in high quality care. EBM makes efficacy oneof the most important determinants of quality.
The medical literature continues to expand, with in-creasing numbers of textbooks and medical journals inprint. Though increasing the number of research articlesmight appear beneficial, the greater number of articlesmay not advance medical knowledge significantly, andphysicians may find fewer of value to their practice. Infact, with more journals searching for articles to pub-lish, work that may routinely be declined because ofquality issues may eventually find outlets. Though elec-tronic databases such as Medline provide rapid accessto the literature and address some of the problems ofgreater numbers or research articles and journals, effec-tive use of these databases requires skill and practice.The literature appraisal skills of EBM arm the clinicianwith an ability to be more selective regarding researchthat may benefit patients, decreasing the often time-con-suming search for relevant research evidence.
A second and paradoxical barrier to acquiring rel-evant scientific information that may be addressed byEBM is the opinion of experts. Expert opinion has tradi-tionally been a popular source of medical knowledge.Though physicians frequently seek the opinion of ex-perts to resolve medical dilemmas, experts frequentlyprovide conflicting recommendations. Experts may bebiased in their interpretation of the available researchevidence, either because of the “micro-specialized” na-ture of their practice population or their own participa-tion in focused research in a particular field. The es-sence of their expertise may be because of the biasedniche they have created in a field. Experts may practicebased upon subjective judgement rather than rigorousanalysis of available scientific evidence. A greater un-derstanding of the principles of EBM empowers physi-cians to evaluate expert recommendations in the appro-priate context of the hierarchy of research evidence anddetermine their usefulness and applicability to particu-

12 American Society of Hematology
lar patient problems. In situations where the researchevidence is weak, expert recommendations may have arole in clinical decision-making even though they arefounded on experience and opinion.
Wide, unexplained geographic variation in practicepatterns, best demonstrated for surgical procedures,7-9 isanother problem in medicine that may be improved withgreater use of the principles of EBM. There are manyinstances where practice patterns show variability farbeyond what may be expected based on clinical, demo-graphic or regional variations in patient populations. Suchvariation is likely to represent some level of inappropri-ate care (over- or under-use, for instance). Variationwould be expected to decrease with greater implemen-tation of evidence-based clinical practice. There is sub-stantial variation in the use of erythropoietin, which maybe influenced by practice setting (fee-for-service versusacademic or HMO), country of residence, reimburse-ment denial, and patient demand (via direct to consumeradvertising efforts).10
As health care spending continues to rise in the US,appropriate resource utilization has become an impor-tant issue in the daily practice of medicine. Finite medi-cal resources are available to all patients in the healthcare system, and appropriate allocation of these resourcesis the responsibility of physicians and society. Thoughpatients are concerned primarily with their own healthand payers may wish to constrain health care expendi-tures, physicians and society must take a perspective thatmaximizes the allocation of health care resources forthe benefit of all patients. An evidence-based approachmay offer some solutions to this inherent conflict. Asphysicians and patients make greater use of strong evi-dence to select among intervention alternatives, they aremore likely to be choosing interventions that improvepatient outcomes. Evidence-driven interventions may nothave the lowest cost, but they are likely to have the great-est benefit or efficacy. With a greater emphasis onstrength of evidence pervading medical culture, it is likelythat health care payers (employers and insurers), policymakers and even patients will demand better evidenceto substantiate high-cost treatment alternatives, constrain-ing resource utilization that does not yield high qualityoutcomes. Though cost-benefit ratios of health care in-terventions may vary across health care systems andpayers, EBM offers the opportunity to evaluate efficacyindependent of health care system financing.
Practicing Evidence-Based MedicineThis section briefly discusses the fundamentals of evidence-based medicine. Readers who are interested in more com-prehensive reviews of the topic are directed to books bySackett11 and Geyman12 or the ongoing series “Users’Guides to the Medical Literature” published in JAMA.13-45
Sackett has proposed the following steps in practic-ing EBM:11
1.Formulate a focused clinical question that can beanswered.
2.Search for the relevant evidence from the literature.
3.Critically evaluate the evidence for its usefulnessand validity.
4. Implement the evidence into decision-making.
Framing the questionThough superficially this step may seem self-evident, itinvolves some experience and clinical judgement toframe questions that will answer the needs of patientsand be amenable to literature review. Questions of inter-est may be about clinical findings, differential diagnosisor accuracy of diagnostic testing, causality, prognosis,therapy, prevention, quality of life or other topics. Whendefining a question, the basic elements to consider in-clude the population, the intervention of interest, thecomparison (treatment alternative) of interest (if rel-evant), and the outcomes to be evaluated. It is importantto be as precise as possible in outlining the question toexpedite the literature search and improve the applica-bility of the results of the search. When more than onequestion arises, clinical experience will help define thequestion most essential to the patient’s care that can beanswered in the limited time available.
Searching for evidenceThe usual source of evidence is electronic databases,which are increasingly available to most clinicians. Elec-tronic databases offer advantages of speed, breadth ofsearch (number of searchable sources), ability to spe-cifically narrow the search criteria to suit the question,and the ability to review either the abstract or, in manycases, the entire article on-line.
Primary publications can be reviewed throughMedline. A second set of electronic databases gives theuser access to secondary publications of the relevantclinical literature. These databases include the CochraneDatabase of Systematic Reviews and the ACP JournalClub and make available evidence-based reviews of theliterature (systematic reviews of randomized trials) onspecific topics. The Agency for Healthcare Research andQuality (AHRQ, www.ahcpr.gov) maintains evidence-based reviews performed by Evidence-based PracticeCenters (EPCs) as well as guidelines that have been de-veloped from the evidence based reviews. Some authorssuggest45 that an initial search be performed on thesesecondary publication databases to efficiently gatherevidence, when available, that has already undergonerigorous methodological and relevance review.

Hematology 2001 13
Evaluating the evidenceThe critical appraisal of the literature for validity andusefulness is essential to deciding whether the evidencefits the scenario and can give useful guidance to the cli-nician. It is at this step in the process that methodologi-cal rigor must be evaluated. The fundamentals of as-sessing methodological rigor come from the disciplinesof epidemiology and biostatistics, and thus may requiresome additional instruction for individuals without re-search expertise.
A comprehensive review of the principles of criti-cal appraisal is beyond the scope of this article. Appraisaltools have been developed by various research teamsand encompass a broad range of research categories thatusers are likely to encounter. Perhaps the most compre-hensive of these tools is the JAMA series “Users’ Guidesto the Medical Literature.”13-45 These tools are designedto assist the user to ask key questions about the validityof the evidence presented and its relevance to the clini-cal question.
Practitioners of EBM must understand the limita-tions and potential for bias in clinical research. Clinicalresearch studies are frequently limited by small samplesizes, differences in selection criteria and prognosticcharacteristics in the treatment and control groups, shortlength of follow-up, and researchers’ expectations of theintervention group. These are particularly evident inobservational studies, which are often not controlled (e.g.no comparison group). Clinical observations play a criti-cal role in medicine; they are often the genesis of re-search projects/findings that eventually lead to clinicaltrials. However, practitioners of EBM must recognizethat unsystematic clinical observation, physiologic ra-tionale and intuition are, by themselves, insufficientgrounds for clinical decision making.45 For this reason,a hierarchy of strength of research designs is importantto understand when evaluating research articles (Table1).46 A well-designed randomized trial offers the great-est opportunity to minimize bias from clinical observa-tions and, therefore, is generally considered the stron-gest study design. The Evidence-based Medicine Work-ing Group suggests that systematic reviews of random-ized trials are even stronger than single randomized tri-als.45 Among those skilled in EBM, skepticism surroundsinterventions documented to be effective in researchdesigns that are not randomized clinical trials. Unfortu-nately, randomized clinical trials are rare in the litera-ture. There is often a lengthy lag time between technicalinnovation and completion and reporting of quality clini-cal trials demonstrating efficacy. In some cases, random-ized trials are not feasible or ethical. In other cases, ob-servational studies where the treatment effect is largeand consistent may be sufficient. Therefore, the hierar-chy is not absolute, leaving room for the experienced
clinician to judge the value of the evidence for the clini-cal situation in question.
Implementing the evidenceThe strength and validity of the evidence is but one partof the decision to implement the evidence. Clinical ex-pertise and patient preferences should also play a fun-damental role at this stage. In the shared decision-mak-ing model, physicians gather, collate, and present thenecessary evidence in an understandable manner to pa-tients, who then apply their belief systems and prefer-ences to reach a satisfactory choice. For instance, in cir-cumstances where evidence in support of treatment canonly be drawn from limited observational studies, a cli-nician and patient may decide to undergo treatment basedon patient preferences and a common-sense mechanismof action of the intervention, acknowledging the limita-tions. On the other hand, the same pair may use evi-dence from limited observational studies demonstratingharm to decide to forgo a particular treatment. Under-standing the strength and validity of the evidence givesthe physician the opportunity to tailor the research find-ings to individual patients and more appropriately in-corporate patient values.
An additional advantage to understanding EBM is agreater understanding of where the evidence is weak.For clinicians, this provides an area to focus future evi-dence reviews to remain up-to-date. For researchers,areas of weakness in the current evidence may suggestfuture research topics that would be of high value.
Translating Evidence into PracticeRecognizing that epoetin is an expensive interventionwith increasing use and significant variation in its use,the American Society of Hematology (ASH) and theAmerican Society of Clinical Oncology (ASCO) soughtto develop an evidence-based guideline to provide clini-cians direction on the usage of epoetin for anemic pa-tients with hematologic malignancies or undergoing che-motherapy for cancer. ASH and ASCO submitted a pro-
Table 1. Hierarchy of evidence.
I. Evidence obtained from at least one properly randomized trial.
II. Evidence obtained from well-designed controlled trials withoutrandomization.
III. Evidence obtained from well-designed cohort or case-controlled analytic studies, preferably from more than onecenter or research group.
IV. Evidence obtained from multiple time series with or withoutintervention. Dramatic results in uncontrolled experiments(e.g., the results of the introduction of penicillin treatment inthe 1940’s) could also be regarded as this type of evidence.
V. Opinions of respected authorities based on clinical experi-ence, descriptive studies and case reports, or reports ofexpert committees.

14 American Society of Hematology
posal to the AHRQ to support a systematic review of theliterature by an Evidence-based Practice Center regard-ing epoetin. The proposal was funded, and the evidencereport became available in early 2001. A publicationsummarizing the evidence for epoetin for anemia of can-cer therapy is now complete.47 Evidence-based guide-lines are being developed from the evidence review, andshould be available at the time of the Education Sessionat the ASH Annual Meeting in Orlando. The role oferythropoietin is still being defined.
II. BUILDING THE CASE: WHAT EVIDENCE EXISTS FOR
USAGE OF EPOETIN AND HOW GOOD IS THE EVIDENCE?
Jerome Seidenfeld, PhD,* Margaret Piper, PhD, MPH,and Naomi Aronson, PhD
The AHRQ EPC Program and Its Approach toSystematic Reviews
Program overviewIn 1997, the Agency for Health Care Policy and Re-search, now known as the AHRQ, launched an initiativeto promote evidence-based practice in everyday carethrough establishment of 12 Evidence-based PracticeCenters (EPCs). The EPCs develop evidence reports andtechnology assessments on clinical topics that are com-mon, expensive, and/or are significant for the Medicareand Medicaid populations. Through this program, AHRQpartners with private and public organizations to improvethe quality, effectiveness, and appropriateness of clini-cal care by facilitating the translation of research evi-dence into clinical practice. In 1998, ASH and ASCOjointly nominated the topic “Use of Epoetin in Oncol-ogy” to AHRQ for an EPC systematic review and evi-dence report.
The EPCs develop evidence reports and technologyassessments based on rigorous, comprehensive synthe-ses and analyses of relevant scientific literature, empha-sizing explicit and detailed documentation of methods,rationale, and assumptions. These scientific synthesesmay include meta-analyses and cost analyses. Each EPCcollaborates with other medical and research organiza-
tions so that a broad range of experts is included in thedevelopment process. More detailed information on theEPC program, the topic nomination process, and the listof EPCs is available at http://www.ahrq.gov/clinic/epcix.htm.1 Summaries and completed reports (with bib-liographies and evidence tables) are available at the sameURL for viewing or downloading. Printed copies alsomay be obtained from the AHRQ Publications Clear-inghouse (1-800-358-9295).
Systematic review methodsProtocols for systematic review are prospectively de-signed to define study objectives; search strategy; pa-tient populations of interest; study selection criteria andmethods to determine study eligibility; outcomes of in-terest; data elements to be abstracted and abstractionmethods; and methods to assess study quality. Usually,two independent reviewers complete each step of theprotocol. Reviewers individually evaluate studies againstselection criteria, abstract data separately, and comparetheir results after each step. Disagreements are gener-ally resolved by consensus but may require resolutionby a third reviewer.
A technical advisory group provides ongoing guid-ance on all phases of each EPC review. Six technicaladvisors participated in the evidence report on use ofepoetin in oncology patients. ASCO and ASH each ap-pointed two of the six advisors, and the EPC staff of theBlue Cross and Blue Shield Association TechnologyEvaluation Center (TEC) recruited the remaining two.
EPC reviews begin with a comprehensive literaturesearch that attempts to identify all publications of rel-evant controlled trials. The search strategy for the re-view on epoetin is described briefly in the Summaryposted on the AHRQ web site1 and more completely inthe full evidence report.2 The MEDLINE, Cancerlit, andEmbase databases, last searched in December 1998,yielded 2,915 references. Supplementary searches (e.g.,Current Contents, bibliographies from manufacturers)through October 30, 1999 yielded 28 additional publishedreports for a total retrieval of 2,943 references.
Next, studies are selected for data abstraction usingcriteria specified in the protocol. The primary study se-lection criteria for the epoetin review required that stud-ies be designed as controlled trials comparing the out-comes of managing anemia with and without epoetin ina patient population relevant to one of four clinical set-tings. These were anemia due primarily to cancertherapy; anemia due primarily to malignancy; myelo-ablation and autologous stem cell rescue; or myeloabla-tion and allogeneic stem cell rescue. We defined the set-ting as anemia primarily due to cancer therapy if trialslimited enrollment to patients undergoing concurrent che-motherapy or radiation therapy with conventional non-
* Blue Cross and Blue Shield Association, TechnologyEvaluation Center, 225 N Michigan Ave, Chicago IL 60601
This work was developed under contract with the Agency forHealthcare Research and Quality, Rockville, MD (AHRQcontract number 290-97-0015). The authors of this article areresponsible for its contents, including any clinical or treatmentrecommendations. No statement in this article should beconstrued as an official position of the Agency for HealthcareResearch and Quality or of the U.S. Department of Health andHuman Services.

Hematology 2001 15
myeloablative doses while on study. We defined the set-ting as anemia primarily due to malignancy if some en-rolled patients did not receive concurrent chemotherapyor radiation therapy while on study.2 Trials were excludedif there were < 10 similarly treated evaluable patients ineach arm.
In the available trials, epoetin treatment (with trans-fusion used as necessary) was always compared to redblood cell (RBC) transfusion alone; no trials comparedepoetin to any other alternative. All randomized con-trolled trials relevant to any of the four clinical settingswere included. Studies that used nonrandomized con-current or historical controls were included if the review-ers could determine that similar patients were includedin the treatment and control groups. Nonrandomized tri-als were considered to be of lesser quality than random-ized controlled trials.
The systematic review addressed the following ques-tions separately for each clinical setting:A. What were the relative effects on outcomes of man-
aging anemia with epoetin compared to transfusionalone? In settings other than stem cell transplants,what were the relative effects of epoetin treatmentwhen different Hb thresholds were used to initiatetreatment?
B. In the included studies, did varying the characteris-tics of the administration of epoetin affect the out-comes of treatment? Were the characteristics ofepoetin administration likely to confound interpre-tation of the evidence on the relative effects ofepoetin treatment according to the alternative Hbthresholds for initiating treatment?
C. Were there populations or subgroups of patientsmore or less likely to benefit from epoetin treatment?Were there laboratory measurements that either pre-dicted or permitted early identification of patientswhose anemia responded to epoetin?
D. What were the incidence and severity of adverseeffects associated with the use of epoetin and howdid these compare with the adverse affects of trans-fusion?
Abstraction of data on adverse events was also lim-ited to controlled trials because our objective was to es-timate the frequency of occurrence in the oncology set-ting of the common adverse effects of epoetin. This pre-cluded analysis of uncontrolled series, because adverseevents related to disease progression and cancer therapycould not be distinguished from those related to epoetin.
To supplement the systematic review, we conducteda literature-based meta-analysis of the effect of epoetinon the odds of transfusion for patients with anemia or atrisk of anemia due primarily to cancer therapy. A ran-
dom effects model was used to calculate the combinedodds ratio of transfusion for the 12 randomized controlledtrials that reported numbers or percentages of patientstransfused with or without epoetin administered subcu-taneously for treatment-related anemia. The odds ratioexpresses the relative likelihood that epoetin-treatedpatients will be transfused compared to the likelihoodfor controls. Published data were insufficient for litera-ture-based meta-analysis of other outcomes or of oddsof transfusion in other clinical settings.
Sensitivity analysis compared results of higher qual-ity trials to those of lesser quality trials. A trial was clas-sified as higher quality when it was randomized anddouble-blinded and met our criteria concerning limitson the number of subjects excluded from the analysis ofresults. We required that < 10% of subjects within eachstudy arm were excluded from the analysis and that theratio of exclusions from each arm was less than 2:1; or,alternatively, that results were reported as an intentionto treat analysis.
External reviewAHRQ requires that EPC reports undergo extensive re-view by external experts and representatives of stake-holder organizations. Early in each project, these indi-viduals review and provide input for modifying the studyprotocol. Later, they review and comment on the initialdraft. However, each EPC has ultimate responsibility forthe final draft of its reports, subject to AHRQ review.
For the epoetin report,2 a preliminary analysis of theevidence base was reviewed by the Blue Cross and BlueShield Association Medical Advisory Panel (MAP),which includes nationally recognized experts in tech-nology assessment and hematology/oncology. Addition-ally, 20 external reviewers critiqued the study protocoland draft report, and revisions were made based on theircomments. Eight were invited by TEC based on theirexpertise in medical oncology, hematology, transfusionmedicine, quality of life, and systematic review meth-odology. One reviewer directs another AHRQ EPC andis a medical oncologist. Ten reviewers were appointedby professional organizations other than ASCO or ASHand by patient advocacy groups. These reviewers in-cluded clinical and research specialists involved in thetreatment of cancer and/or management of cancer-re-lated anemia and patient advocacy representatives. Oneexternal reviewer was from the technical staff of OrthoBiotech, Inc. Lists of the MAP members, external re-viewers and technical advisors are included in the ap-pendices of the full evidence report.2
16 American Society of Hematology
Evidence on Outcomes of Epoetin for AnemiaPrimarily Due to Cancer Therapy
Our evidence review is based on data abstraction andanalysis of 22 controlled trials with a total enrollment of1,927 patients.3-24 All trials compared the outcomes ofmanaging anemia in patients undergoing therapy for amalignancy using epoetin treatment or RBC transfusionalone. Eighteen trials with a total 1,698 enrolled patients(88%) were randomized,3-20 and 7 of these (853 patients;44%) were placebo-controlled and double-blind.3-9 Forall 22 trials, the number of patients reported as evaluableis 1,838, which is 95% of all enrolled patients. We clas-sified the 22 trials into 3 categories defined by the studypatients’ mean Hb at enrollment: Hb ≤ 10 g/dL;3-7,9,11,15,16,23
Hb > 10 but < 12 g/dL;8,10,12,17,21,22,24 and Hb ≥ 12 g/dL.13,14,18-20 No trial directly compared the outcomes ofinitiating epoetin treatment at different Hb thresholds.
Epoetin versus transfusion and relative effects atdifferent Hb thresholdsThe systematic review found adequate and consistentevidence that epoetin increased Hb levels and percent-age of patients demonstrating hematologic responsewhen compared with controls managed by transfusionalone. This was true for pediatric patients as well asadults. For all randomized studies that gave epoetin sub-
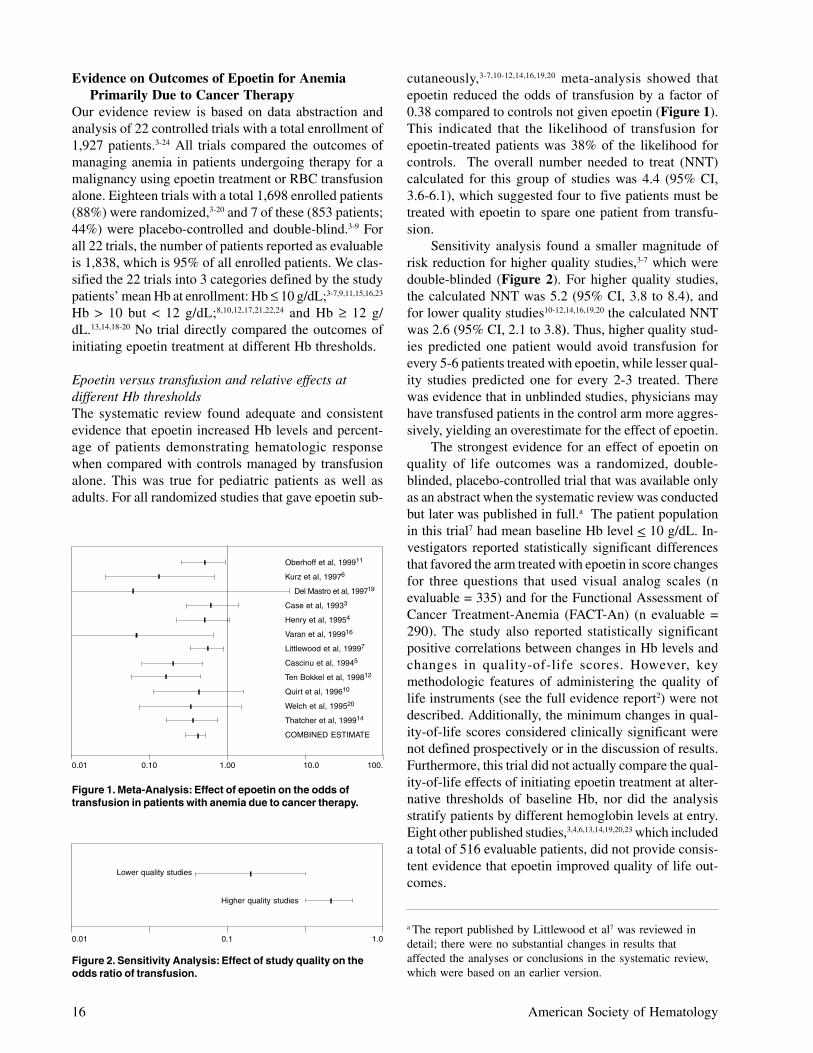
cutaneously,3-7,10-12,14,16,19,20 meta-analysis showed thatepoetin reduced the odds of transfusion by a factor of0.38 compared to controls not given epoetin (Figure 1).This indicated that the likelihood of transfusion forepoetin-treated patients was 38% of the likelihood forcontrols. The overall number needed to treat (NNT)calculated for this group of studies was 4.4 (95% CI,3.6-6.1), which suggested four to five patients must betreated with epoetin to spare one patient from transfu-sion.
Sensitivity analysis found a smaller magnitude ofrisk reduction for higher quality studies,3-7 which weredouble-blinded (Figure 2). For higher quality studies,the calculated NNT was 5.2 (95% CI, 3.8 to 8.4), andfor lower quality studies10-12,14,16,19,20 the calculated NNTwas 2.6 (95% CI, 2.1 to 3.8). Thus, higher quality stud-ies predicted one patient would avoid transfusion forevery 5-6 patients treated with epoetin, while lesser qual-ity studies predicted one for every 2-3 treated. Therewas evidence that in unblinded studies, physicians mayhave transfused patients in the control arm more aggres-sively, yielding an overestimate for the effect of epoetin.
The strongest evidence for an effect of epoetin onquality of life outcomes was a randomized, double-blinded, placebo-controlled trial that was available onlyas an abstract when the systematic review was conductedbut later was published in full.a The patient populationin this trial7 had mean baseline Hb level < 10 g/dL. In-vestigators reported statistically significant differencesthat favored the arm treated with epoetin in score changesfor three questions that used visual analog scales (nevaluable = 335) and for the Functional Assessment ofCancer Treatment-Anemia (FACT-An) (n evaluable =290). The study also reported statistically significantpositive correlations between changes in Hb levels andchanges in quality-of-life scores. However, keymethodologic features of administering the quality oflife instruments (see the full evidence report2) were notdescribed. Additionally, the minimum changes in qual-ity-of-life scores considered clinically significant werenot defined prospectively or in the discussion of results.Furthermore, this trial did not actually compare the qual-ity-of-life effects of initiating epoetin treatment at alter-native thresholds of baseline Hb, nor did the analysisstratify patients by different hemoglobin levels at entry.Eight other published studies,3,4,6,13,14,19,20,23 which includeda total of 516 evaluable patients, did not provide consis-tent evidence that epoetin improved quality of life out-comes.
a The report published by Littlewood et al7 was reviewed indetail; there were no substantial changes in results thataffected the analyses or conclusions in the systematic review,which were based on an earlier version.
Figure 2. Sensitivity Analysis: Effect of study quality on theodds ratio of transfusion.
0.01 0.1 1.0
Higher quality studies
Lower quality studies
Figure 1. Meta-Analysis: Effect of epoetin on the odds oftransfusion in patients with anemia due to cancer therapy.
0.01 0.10 1.00 10.0 100.
Oberhoff et al, 199911
Kurz et al, 19976
Del Mastro et al, 199719
Case et al, 19933
Henry et al, 19954
Varan et al, 199916
Littlewood et al, 19997
Cascinu et al, 19945
Ten Bokkel et al, 199812
Quirt et al, 199610
Welch et al, 199520
Thatcher et al, 199914
COMBINED ESTIMATE

Hematology 2001 17
The most robust evidence that epoetin reduced useof RBC transfusions for patients undergoing therapy formalignancy was from trials in groups with baseline Hb< 10 g/dL. 3-7,9,11,15,16,23 Transfusion outcomes did not ap-pear to be superior in trials where epoetin treatment wasinitiated in groups with mean Hb > 10 g/dL compared totrials where mean Hb was < 10 g/dL. Among trials onadults with baseline Hb < 10 g/dL, the range of differ-ences between epoetin and control arms for percentageof patients transfused was 9-45%.3-7,11,15 For baseline Hb> 10 but < 12 g/dL 8,10,12,17,21,22,24 the range was 7-47%; therange was 7-39% for baseline Hb ≥ 12 g/dL.13,14,18-20 How-ever, these ranges are wide and it is uncertain whetherthe three groups of studies compare patient populationsthat are similar except for baseline Hb.
The available evidence was inadequate to determinewhether outcomes of epoetin treatment were superiorwhen treatment was initiated in groups with mean Hb >10 g/dL, compared to groups where mean Hb is < 10 g/dL. Randomized controlled trials, double blinded andadequately powered, are needed to compare the out-comes of epoetin treatment initiated at various Hb thresh-olds. Inferences from indirect comparison of the resultsof the available trials cannot resolve this question.
While it is possible that adequately powered com-parative trials might demonstrate the superiority ofepoetin intervention at the higher Hb levels, our exami-nation of the evidence suggests two reasons why thatmay not prove to be true. First, patients with Hb at entrybelow the mean may have accounted for most of thetransfusions among epoetin-treated patients in trialswhere baseline Hb was < 10 g/dL. Thus the greatest yieldfor reducing the number of patients transfused in thispopulation might come from initiating epoetin beforethe Hb level falls substantially below 10, rather than byinitiating epoetin treatment at a level substantially above10 g/dL. Second, in all trials, patients who were unre-sponsive to epoetin may have accounted for a substan-tial proportion of patients transfused. Initiating epoetintreatment at a higher Hb level is unlikely to reduce trans-fusions for this subgroup.
Effects of different methods for administering epoetinThe meta-analysis examined whether the characteristicsof epoetin administration (dosing regimen, treatmentduration, and dose range) had an effect on the estimateof the summary odds ratio for transfusion. Only epoetindose appeared to have an independent effect on transfu-sion outcomes, but this was potentially confounded bystudy quality. However, the results of two randomizedcontrolled trials that directly compared lower and higherdoses of epoetin (450 vs. 900 units/kg/week) did notprovide convincing evidence that the higher dose wasmore effective in preventing transfusions.12,14
Effects of patient characteristics1.Age: Epoetin was effective in preventing transfu-
sion in pediatric patients.16,23 No studies reported out-comes stratified specifically for geriatric patients,but adults up to age 90 were included in sometrials.3,4,7
2.Malignant Disease: There was evidence that epoetinproduced hematologic responses and probably re-duced transfusions in patients with non-myeloidhematologic malignancies7,15 to a similar degree asin patients with tumors of solid organs or tissues.
3. Radiotherapy: Although epoetin increased Hb lev-els for patients managed with radiotherapy alone,mean Hb levels of control patients did not decreasefrom baseline values.13,17,22 The radiotherapy regi-mens utilized apparently did not contribute to or ex-acerbate pre-existing mild anemia.
4.Platinum Regimens: The evidence demonstratedbenefit from epoetin for patients receiving chemo-therapy regimens with or without either cisplatin orcarboplatin (see the full evidence report2 for cita-tions).
5.Predictors of Response: The 22 trials included inthis evidence base reported no significant predic-tors of response to epoetin therapy.2 In particular,neither baseline serum erythropoietin nor the ratioof observed to predicted serum erythropoietin lev-els (O/P ratio) predicted response in any analysis.
Adverse effectsLimited evidence on adverse events was available fromthe studies included in this review, but the frequenciesof those reported did not appear to differ markedly be-tween epoetin-treated patients and controls.2 The onlystatistically significant difference was a greater frequencyof fatigue reported by patients in the control arms.
Evidence on Outcomes of Epoetin for AnemiaDue Primarily to Malignant Disease
The literature search identified 6 controlled trials, allrandomized, with a total enrollment of 693 patients thatmet inclusion criteria for this systematic review.25-30 Threetrials were placebo-controlled and double-blind (n = 332;48%).25-27 Of the 693 patients enrolled, 648 (93.5%) werereported as evaluable. Patients in this evidence base haddiagnoses known to have a high occurrence of anemiaof malignancy (multiple myeloma, non-Hodgkin’s lym-phoma, chronic lymphocytic leukemia [CLL], andmyelodysplastic syndromes [MDS]). With the exceptionof one trial on patients with MDS,25 the preponder-ance of patients in these trials received concurrenttherapy for their malignancy.

18 American Society of Hematology
Epoetin versus transfusion andrelative effects at different Hb thresholdsThere was consistent evidence that epoetin increased Hblevels and percentage of patients demonstrating hema-tologic response in patients with anemia of malignancy.The evidence on transfusion outcomes was sparse, butsuggested a favorable effect of epoetin treatment. Theonly report on measurements of quality of life was anabstract that did not provide sufficient detail for inter-pretation of the results.27 All patients included in thesestudies had baseline hemoglobin < 10 g/dL. The evi-dence did not address alternative thresholds for initiat-ing epoetin treatment in patients with anemia of malig-nancy.
Effects of different methods for administering epoetinThe studies suggested that starting doses in the 200-450units/kg per week range were adequate to achieve he-matologic response. However, the only study of patientswith MDS used a much higher dose, 1050 units/kg perweek, yet obtained a smaller increase in response rate.25
The distinct mechanism of anemia in this clonal disor-der probably contributed to the reduced response rate.
Effects of patient characteristics1. Malignant disease: A statistically significant hema-
tologic response in the epoetin arm was reported forall hematologic malignancies included in this review.However, the limited evidence available suggestedthat hematologic response rates were lower for pa-tients with MDS.
2. Age: All studies were of adults; there were no stud-ies of pediatric patients or studies that separatelyreported on geriatric patients.
3. Prior Transfusion: Epoetin increased hematologicresponses or Hb levels for patients with either mul-tiple myeloma or non-Hodgkin’s lymphoma (NHL),irrespective of history of prior transfusion.28-30 Asingle study of MDS patients reported that epoetinincreased hematologic responses for patients with-out previous history of transfusion but not for thosepreviously transfused.25 However history of priortransfusion may be associated with other character-istics, such as duration and progression of disease,which may have affected erythropoiesis in MDSpatients.
4.Predictors of Response: This group of studies didnot provide sufficient evidence to draw conclusionson predictors of response. Only the serum concen-tration of endogenous erythropoietin at baseline25,30
and the ratio of observed to expected concentrationsof serum erythropoietin28,30 were reported as signifi-cant predictors of response in at least two trials.
Adverse effectsThere was a statistically significant increase in hyper-tension (10% versus 1%, p = 0.011) and a non-signifi-cant increase in thromboembolic events (3% versus zero,p = 0.55) among those treated with epoetin. The reportedfrequency of other adverse events did not appear to dif-fer between epoetin-treated patients and controls.
Evidence on Outcomes of Epoetin for Anemia Due toMyeloablation and Allogeneic Stem Cell Rescue
Evidence concerning the use of epoetin after high dosechemotherapy and allogeneic stem cell transplantation(alloSCT) was derived from 7 controlled studies31-37 (to-tal enrollment, 493) of patients with malignancies rep-resentative of those undergoing alloSCT in clinical prac-tice. Of the 7 controlled trials, all but 2 were random-ized (total enrollment in randomized studies, 400);31-35
non-randomized trials compared epoetin-treated patientsto historical controls.36,37 The largest study enrolled andevaluated 215 patients;31 all other studies enrolled fewerthan 100 patients.
These studies compared the outcomes of controlsmanaged with RBC transfusion initiated at a pre-definedthreshold to the outcomes of epoetin treatment supple-mented with RBC transfusion when necessary. One studyexclusively enrolled pediatric patients.37 Enrolled patientshad a variety of hematologic tumors. All studies usedbone marrow as the stem-cell source, and all studiesadministered epoetin intravenously.
Epoetin versus transfusionEpoetin consistently resulted in a statistically significantdecrease in the time to RBC engraftment, as indicatedby achievement of a pre-determined Hb level indepen-dent of transfusion support.31-37 The range of reductionreported was 1-2 weeks. Reticulocyte measures, whichtend to predict RBC engraftment, also suggested morerapid engraftment with epoetin administration.31, 33-37
Outcomes for day of last transfusion were related to andcorrelated with RBC engraftment by Hb level results,with statistically significant results that favored theepoetin-treated study arm.31,32,36 Epoetin administrationis unlikely to spare anyone from transfusion as recipi-ents of alloSCT are uniformly anemic following the pro-cedure and response to erythropoietin, whether endog-enous or exogenous, is not immediate. The evidencesuggested that epoetin treatment may have decreased thenumber of RBC units transfused.32,34,35,37 Limited evi-dence suggested that epoetin treatment had no signifi-cant effect on length of hospital stay.32,33 This is not sur-prising given the number of complications from alloSCTthat are unrelated to anemia.

Hematology 2001 19
Effects of different methods for administering epoetinTransfusion outcomes appeared to be associated withthe duration of follow-up for reporting and statisticalcomparison; shorter follow-up was more often associ-ated with a significant beneficial effect,34,35,37 whereaslonger follow-up may have been complicated by trans-fusions for graft-versus-host disease and resulted in non-significant differences in outcomes for the epoetin-treated arms.31,33 For both RBC engraftment and RBCtransfusion outcomes, results obtained with epoetin doseextremes (525 or 3500 U/Kg/week)35,37 did not appearto differ from those obtained with the moderate doses(700-1050 U/kg/week) used in the majority of studies.
Effects of patient characteristicsAge: Although only one small study37 (non-randomized,historical controls) specifically examined the use ofepoetin in a pediatric population, results were consis-tent with those obtained in all other studies, which en-rolled primarily adult populations. Additionally, signifi-cant results were obtained in this study using a dose perkg per week that was half or less the doses used in stud-ies of adult patients.
Adverse effectsThere did not appear to be significant adverse eventsassociated with epoetin treatment in patients receivingallogeneic stem-cell transplants; however, reporting wassparse. The available evidence showed no depression ofplatelet engraftment with epoetin treatment.
Evidence on Outcomes of Epoetin for Anemia Due toMyeloablation and Autologous Stem Cell Rescue
The literature search and review for studies of epoetinuse after autologous transplantation identified 6 con-trolled trials (total enrollment, 321).31,37-41 Three of the 6trials were randomized (total enrollment, 169);31,38,39 non-randomized trials compared epoetin-treated patients tohistorical controls.37,40,41 Studies ranged in size from 2038
to 11431 enrolled patients. All of the studies used bonemarrow as the exclusive source of stem cells except forone39 in which patients with Hodgkin’s lymphoma weregiven pooled bone marrow and peripheral blood stemcells. Nevertheless, it appears that results from these stud-ies can be generalized to patients transplanted with pe-ripheral blood stem cells, the current standard of care.
Epoetin versus transfusionThe evidence did not support a beneficial effect ofepoetin administration on RBC engraftment, RBC trans-fusion, or length of hospital stay outcomes. It is particu-larly noteworthy that 2 studies31,37 that used the same epoetinprotocol for both allogeneic and autologous stem cell trans-plant patients reported several outcomes significantly im-
proved for allogeneic stem cell transplant patients, but notfor autologous stem cell transplant patients.
Effects of different methods for administering epoetinSince the available evidence did not show a clear benefitfor epoetin treatment, there was no evidence to favor aparticular dose, dosing regimen, or treatment duration.Although it is possible that treatment duration was too shortin all included studies to significantly improve outcomes,reticulocyte measures, an early indicator of RBC engraft-ment, did not indicate a probable response.31,37,39
Effects of patient characteristicsEpoetin did not show a beneficial effect for the entirepopulation of patients treated in these studies. Resultsamong the subpopulations were consistent with overallresults, and no subpopulation that derived benefit fromepoetin treatment could be identified. The lack of re-sponse to epoetin in patients given bone marrow stemcells suggests that patients given peripheral blood stemcells also would be unlikely to respond. Preparations ofperipheral blood stem cells mobilized with growth fac-tors contain progenitor cells from the erythroid (andother) lineages. These progenitors are farther along thematuration pathway to functional end-stage cells, andmay be less dependent on erythropoietin, than areunstimulated stem cells harvested from the bone mar-row. The time to recovery of red cell counts and correc-tion of anemia thus seems less likely to be shortened byepoetin therapy after infusion of peripheral blood stemcells than after infusion of bone marrow stem cells.
Adverse effectsThere did not appear to be significant adverse eventsassociated with epoetin treatment in patients receivingautologous stem-cell transplants; however, reporting wassparse. The available evidence showed no depression ofplatelet engraftment with epoetin treatment.
III. AMERICAN SOCIETY OF HEMATOLOGY/AMERICAN SOCIETY OF CLINICAL ONCOLOGY
GUIDELINES ON THE USE OF ERYTHROPOIETIN
Alan Lichtin, MD*
At the time of the writing, the joint American Society ofHematology/American Society of Clinical Oncology(ASH/ASCO) erythropoietin (EPO) guidelines are not yetcompleted. Thus, the following discussion of the guide-lines is preliminary. Once it is published, this review shouldbe discarded in favor of the actual manuscript.
* Dept. of Hematology/Oncology, Cleveland Clinic Founda-tion, 9500 Euclid Avenue, Cleveland OH 44195-0002

20 American Society of Hematology
Subjects to Be Addressed by the GuidelinesThe previous chapters in this section discuss the valueof evidence-based medicine, and an evidence-based re-view of the medical literature regarding erythropoietinusage in cancer and cancer chemotherapy.
The Blue Cross and Blue Shield TEC evidence re-view has been accepted for publication and is internetaccessible.1,2 Using the evidence-based review performedby the TEC center, ASCO and ASH have undertakendevelopment of an evidence-based guideline to provideguidance to clinicians making decisions between treat-ment alternatives for patients with anemia. Our guide-lines will focus on the following clinical questionsthought to be important to clinicians and patients.
1. Is the use of EPO appropriate and is it recommendedto reduce the need for red blood cell transfusionsfor patients with chemotherapy-associated anemiaand a declining hemoglobin to a level of 10 g/dL?
2.For patients with declining hemoglobin concentra-tions but for hemoglobin between 10-12 g/dL, is itappropriate to use EPO? Are there clinical situa-tions, such as underlying cardiac or pulmonary com-promise, for which use of erythropoietin in the 10-12 g/dl range may be appropriate?
3.Is a dose of erythropoietin appropriate at 150 U/kgthrice weekly for a minimum of 4 weeks with con-sideration for dose escalation to 300 U/kg for anadditional 4-8 weeks?
4.At what point should non-responding erythropoietintreated patients have their erythropoietin discontin-ued?
5.Is the use of erythropoietin associated with an im-provement in the health related quality of life (QOL)for patients with clinically significant anemia (withbaseline hemoglobin > 10 g/dL)?
6.Does erythropoietin therapy help patients withMDS?
7.What is the role of erythropoietin in myeloma, non-Hodgkin’s lymphoma or chronic lymphocytic leu-kemia patients?
8.What is the role of iron in supporting the use of eryth-ropoietin?
The Blue Cross and Blue Shield TEC performed an ex-haustive literature review and determined criteria for“high quality studies.” Articles selected as “high qual-ity” were generally randomized controlled trials (RCT)with large numbers, with adequate power to result instatistically significant differences between randomizedgroups. Non-randomized, observational, and uncon-trolled studies were generally excluded from analysis.The ASH/ASCO guideline will primarily use these “high
quality studies” in its analysis of the literature, thoughevidence from non-randomized studies will also be con-sidered, when appropriate.
Strength of Current EvidenceWe expect the guidelines will help physicians distill theevidence for the use of erythropoietin and make informeddecisions regarding treatment alternatives for anemia.Erythropoietin is generally convenient and low risk,though it is expensive. Transfusions are also expensive,have infectious and infusion-related risks, and are timeconsuming. In an era of financial constraints, a societalgoal is to maximize health benefits from health care ex-penditures. Weighing the risks and benefits of both eryth-ropoietin and transfusion is a part of the daily life of apracticing hematologist-oncologist, and it is our hopethat the guideline will help inform the clinician aboutthe evidence supporting either of these treatment alter-natives.
Hemoglobin levels at entry into trials, duration oftherapy, and populations being treated vary from studyto study. Overall, however, there appears to be sufficientevidence supporting a rise in hemoglobin level and de-crease in red cell transfusion requirements in erythro-poietin-treated patients, especially solid tumor chemo-therapy patients who are receiving platinum-basedtherapy (guideline items 1 and 2). The size of this effectis modest. The meta-analysis presented in the TEC pa-per states that about five patients need to be treated witherythropoietin to save one patient from needing a trans-fusion.
Many studies have used doses of EPO of 150 U/kgTIW. Gabrilove’s widely quoted abstract3 and subsequentpublication4 recommend dosing 40,000 units once perweek based upon hemoglobin improvement in a largesingle-arm study. The convenience of this approach forpatients has led to wide clinical practice. Unfortunately,there is no randomized controlled trial comparing dos-ing with 40,000 units once per week with weight-baseddosing (guideline item 3). Many physicians currently use40,000 units once per week and, if there is no responseafter 4 to 6 weeks, will raise the dose. Though this is com-mon practice, there is not strong evidence in the litera-ture supporting a dose-effect relationship for EPO responsein patients on chemotherapy, or who have anemia second-ary to underlying malignancy (guideline item 4).
There are multiple non-randomized studies, and onerandomized clinical trial to support an improvement inQOL for patients treated with EPO. However, QOL isdifficult to assess (see discussion below) and it is likelythe guidelines will focus on this as one area where sub-stantial further research is needed to establish conclu-sively that overall QOL is improved with usage of EPO(guideline item 5).

Hematology 2001 21
Likewise, the benefit of erythropoietin to treat ane-mia for patients with MDS, myeloma, non-Hodgkin lym-phoma and CLL is an area where research opportunitiesexist (guideline items 6 and 7).
Areas of Weakness in Current EvidenceThere are shortcomings common to many of the studiesevaluating erythropoietin, including some of the RCTs.These include methodologic concerns, appropriate con-sideration of adjunctive therapy for anemia, and diffi-culties inherent in assessing quality of life.
Methodologic concerns in some erythropoietin stud-ies may reduce the strength and validity of their conclu-sions. For example, in the Littlewood Study,5 there is anabandonment of the intention to treat analysis for someoutcomes, including quality of life (QOL). Nearly 23%of patients were not evaluable for QOL outcomes be-cause of incomplete data or language barriers. If thesepatients were not similar to those evaluated for QOL,the improvement in QOL among patients treated withEPO demonstrated in this RCT may be confounded byother factors (effectively nullifying the goal of ran-domization) and may therefore be less valid.
Nutritional deficiency is one of the most commoncauses of anemia and is common in patients with malig-nancies. There is non-uniformity in these studies as tohow carefully iron status is monitored and how aggres-sively iron deficiency is treated. Tolerance of oral ironmay be poor in a population already suffering from thegastrointestinal side effects of chemotherapy. No studyhas documented compliance with iron therapy or dem-onstrated whether iron-deficient patients on EPO, treatedwith iron, responded to the iron before EPO was initi-ated. Intuitively, one must optimize all non-erythropoi-etin related erythron stimulants (i.e., iron, Vitamin B12and folic acid) in order for EPO to work. No matter whatdose of EPO is given, if a patient has absent iron stores,one would expect a blunted response to EPO. Ferritinalone is a poor barometer of iron status. Patients withmalignancy receiving chemotherapy will have an el-evated ferritin level, because it is an acute phase reac-tant. Iron saturation alone is also a poor barometer, sincethe anemia of malignancy may represent the “anemia ofchronic disease” with misleadingly low percentage satu-ration. In one randomized study, iron deficiency wasnoted, but patients were not given iron supplementation.6
The authors relied on EPO alone to stimulate erythro-poiesis, even when iron deficiency was identified.6 Re-sponse to EPO may have been underestimated in thesepatients.
Evaluation of the effect of EPO on quality of lifepresents special difficulties. QOL is a subjective judge-ment of an individual’s existence and is generally con-sidered to encompass physical, functional, social, emo-
tional, and economic aspects (often referred to as do-mains). Work capacity, sleep habits, depression, familyrelationships, etc. affect a patient’s perception of QOL.QOL is important, and one goal of any therapy is to helppatients to feel better. However, raising hemoglobin doesnot always equate with increased strength or QOL.
Because QOL is subjective, special instruments arenecessary for its measurement. The QOL instrumentspresently used in the EPO literature are linear analogscales (LASA) or the Functional Assessment of CancerTherapy–Anemia (FACT-An) scoring system. One de-bate in assessing QOL is whether to use a “general” in-strument that has been widely used in various diseases,or to use an instrument “specific” to the disease processbeing evaluated. While the former gives the opportunityto compare changes in quality of life across diseases (liketreatment for renal failure with treatment for lung can-cer), it may not be as sensitive as the latter for changesexpected with some diseases. Many investigators handlethis by including both general and specific instrumentsin their study. Whichever type of instrument is used, it isessential that changes in quality of life be benchmarkedto correlate significant clinical changes with significantchanges in QOL. This is to be certain we understandwhich changes, as measured by any QOL instrument,represent clinically meaningful changes. For example,many would agree that raising hemoglobin from 5 to 14g/dL is likely to make a person stronger, feel better, andincrease QOL. A legitimate question is whether a rise inhemoglobin from 9.8 to 10.7, or even to 11.3 g/dL, trans-lates into meaningfully improved global QOL, versusan improvement in fatigue as one component of overallQOL. The science of correlating rise in hemoglobin witha rise in QOL is still developing.
EPO studies have not blinded the patient and/or in-vestigators to the changes in hemoglobin level. Patientsin a trial measuring EPO’s effect on hemoglobin whoknow their hemoglobin is rising may translate that physi-ologic success into higher scores on a LASA or a FACT-An scoring system, whether or not they have experiencedsymptomatic improvement. The only way to control forthis would be to blind both the investigator and the pa-tient to hemoglobin changes, yet this might be impracti-cal. Patients’ response to chemotherapy may affect theirQOL, regardless of response to EPO. As well, depres-sion, neuropathy, inattention, and lack of exercise mayalso affect patients’ assessment of QOL.7-11
Opportunities for Further ResearchThe problems with the EPO literature as mentioned abovemay be addressed by future studies. Can studies be de-signed to help physicians predict who will respond toerythropoietin? There are data suggesting that there is acorrelation between baseline serum erythropoietin level

22 American Society of Hematology
and response to EPO. Unfortunately, it is not the stron-gest of correlations, but generally, the higher serum eryth-ropoietin level, the less likely for the patients to respond.Outliers exist, so it is impossible to be definitive whenrecommending the erythropoietin level as a predictor ofresponse. Unfortunately, in many of the previous che-motherapy studies, pre-treatment erythropoietin levelswere not drawn on all patients. Another problem withsome studies, especially in myeloma, lymphoma, andCLL, is the lumping together of patients with the samediagnosis but who may have very different prognoses orhistologic sub-types. Lymphoma is a clear examplewhere necessity for treatment, steroid responsiveness,and perhaps response to erythropoietin, differs based onhistologic sub-type, but none of the current studies sepa-rate indolent disease from intermediate or high-gradelymphoma. Future research may differentiate the role ofdisease subtype, stage and prior therapy on the respon-siveness of a patient to EPO.
Amgen is evaluating a new form of erythropoietincalled “Novel erythropoiesis stimulating protein(NESP).” This is glycosylated in such a way that it canbe dosed once per week (as many clinicians are alreadydosing EPO) or even once every two weeks. Data havebeen presented in abstract form12 that suggest a responseprofile similar to EPO. It is too early to speculate onwhat role NESP will occupy in the treatment of anemiccancer patients.
Hopefully, the ASH/ASCO evidence-based reviewwill help patients and physicians know how to optimizeuse of this drug. It will also point out how future studiescan contribute answers to some of the questions for whichthere is not strong evidence in the current literature.
IV. THE EFFICACY OF RECOMBINANT ERYTHROPOIETIN
IN CANCER-RELATED ANEMIA:WHERE DO WE GO FROM HERE?
Timothy J. Littlewood, MD*
Incidence and Symptoms of AnemiaAnemia is very common in patients with hematologicalmalignancy or solid tumors. It can be attributed to theanemia of chronic disease, to tumor infiltration of thebone marrow and to the myelosuppressive effects of thechemotherapy.1 For example, in patients with myelomaapproximately 50% will have a hemoglobin of < 10.5g/dL at presentation and most of the remainder will de-velop anemia during their initial chemotherapy.2,3 Suc-
cessful control of the myeloma will usually improve thehemoglobin level, but anemia will recur with diseaseprogression. For patients with lymphoma, anemia (he-moglobin < 12.0 g/dL) is present in approximately 40%at diagnosis, and this figure increases towards 70% after3-4 cycles of chemotherapy.4
Common symptoms of anemia include fatigue,breathlessness, swollen feet, chest pain and loss of men-tal acuity. Fatigue is very common in patients with he-matological malignancy and may be caused by physi-ological factors (such as anemia) or psychological fac-tors. Approximately 75% of patients with cancer expe-rience fatigue during their treatment, which is often notfully appreciated by their physicians, and approximatelyone half reported that the fatigue had an important nega-tive impact on their daily activities.7
Erythropoietin production is impaired in patientswith malignant disease. Miller et al5 demonstrated therelative decrease in erythropoietin production, which oc-curs in patients with malignant disease, by contrastingserum erythropoietin levels in patients with iron defi-ciency anemia with the levels in patients with a varietyof cancers. Miller showed that for any hemoglobin con-centration, serum erythropoietin levels were lower inpatients with cancer than for patients with iron deficiency.Although the patients studied had solid tumors, the samerelative erythropoietin deficiency has been demonstratedin approximately 75% of patients with hematologicalmalignancies such as CLL, lymphoma and myeloma.6
Treatment of AnemiaThe possible treatments for the anemia are to do noth-ing, to transfuse with red cells or to treat with recombi-nant human erythropoietin (rHuEpo). The majority ofanemic cancer patients do not get treated,8 probably be-cause symptoms of fatigue and lethargy are attributed tothe underlying malignancy and/or treatment.
Blood transfusion is the most commonly used treat-ment for anemia in patients receiving chemotherapy. Thehemoglobin level at which a transfusion will be suggestedvaries considerably.8 Some doctors recommend transfu-sion when the hemoglobin falls below 10.0 g/dL; othersbelieve that transfusion should be withheld until the he-moglobin is less than 8.0g/dL. Blood transfusion iscostly, inconvenient for the patient, usually must be givenin a hospital environment and is, of course, not com-pletely safe. However, for the majority of patients it isan effective way to safely increase the hemoglobin con-centration and make them feel better. The beneficial ef-fects usually last for 2-4 weeks, at which point anotherblood transfusion may be needed if the underlying causeof anemia has not been reversed.
RHuEpo is an alternative treatment option for ane-mic patients with hematological malignancy. Substan-
* Hematology Department, John Radcliffe Hospital, OxfordOX39DU, United Kingdom
Dr. Littlewood is on the speaker’s bureau for three companies.

Hematology 2001 23
tial data detail its use in patients with lymphoproliferativedisorders, in myelodysplasia and following bone mar-row transplantation. RHuEpo is not commonly used inpatients with acute leukemia, probably because serumerythropoietin levels tend to be high and because theintensive myelotoxic chemotherapy regimens mitigateagainst a treatment response.
RHuEpo in Anemic Patients with Malignant DiseaseIn 1990 Ludwig et al9 published a report on rHuEpo treat-ment of 13 anemic patients with advanced myeloma. Thetreatment dose of rHuEpo was 150 U/kg body weightby subcutaneous injection three times per week. Themedian baseline hemoglobin was 10.2 g/dL, and 11(85%) of the patients responded to treatment with a he-moglobin rise of > 2.0g/dL. The time to response rangedfrom 3-20 weeks with a median of 5 weeks. As a resultof this important initial study, several randomized trialswere conducted to establish the effectiveness of rHuEpoin anemic patients with CLL, non-Hodgkin’s lymphomaand myeloma.
A summary of the results from 4 trials is shown inTable 2.9-12 Response was defined as an increase in he-moglobin of > 2.0g/dL above baseline independently ofblood transfusion. This was achieved in 58-85% of pa-tients in the treatment arms and in 7-24% in the placeboarms. These differences were statistically significant. Theproportion of patients requiring transfusion decreasedby approximately 50% in the treatment compared to theplacebo arms. Two of these studies randomized patientsto different doses of rHuEpo and were able to demon-strate that a starting dose of, or equivalent to, 150 U/kgsubcutaneously 3 times per week produced a superiorresponse to a lower starting dose. Doubling the dose to300 U/kg 3 times per week in non-responders after 4weeks produces a response in a further quarter of pa-tients. All of the studies confirmed that rHuEpo is safewith a side effect profile similar to that found in the pla-cebo treated arms.
In a study by Rose et al13 221 anemic patients withCLL were randomized to treatment with rHuEpo or pla-cebo. The baseline hematocrits were 27.5% on the treat-ment group compared to 27.7% in the placebo group.The mean hematocrit increased by 5.7% in the rHuEpogroup compared to 1.5% in the placebo group (p <0.0001), and 50% of the rHuEpo group had a hemat-ocrit increase of > 6 points above baseline compared to15% of the placebo group (p < 0.0001). rHuEpo-treatedpatients who achieved a hematocrit above 38% had asignificant improvement in many domains of quality oflife compared to the patients treated with placebo.
These important findings have been supported bythree very large, single-arm, community-based studiesin the United States.14-16 The observational study by
Gabrilove16 was notable for showing that a once weeklydosing schedule of rHuEpo was equivalent to a 3 timesper week regimen.
In an attempt to confirm these findings a large,multicenter, placebo controlled, double blind, random-ized trial was instigated.17 Three hundred seventy-fivepatients with solid or nonmyeloid hematological malig-nancies and hemoglobin levels ≤ 10.5 g/dL or > 10.5 g/dL but ≤ 12.0 g/dL following a decrease in hemoglobin≥ 1.5 g/dL per cycle or month since starting chemo-therapy were randomized 2:1 to 150-300 IU/kg epoetinalfa (251 patients) or placebo (124 patients) t.i.w. sub-cutaneously for at least 12-24 weeks or 3-6 chemotherapycycles plus 4 weeks after chemotherapy. The primaryefficacy endpoint was proportion of patients transfused;secondary endpoints included hemoglobin level andQOL measurements. The protocol was amended beforestudy end to collect survival data up to 12 months afterthe last patient completed study.
Epoetin alfa, compared with placebo, significantlydecreased transfusion requirements (p = .0057) and in-creased hemoglobin (p < .001); also, epoetin alfa pro-vided significantly (p < .01) greater improvement of allprimary cancer- and anemia-specific QOL domains includ-ing energy level, ability to do daily activities, and fatigue.Although the study was not powered for survival as anendpoint, Kaplan-Meier estimates showed a trend in over-all survival favouring epoetin alfa (p = .13, log rank test).Side effects were comparable between groups.
The conclusions drawn from this, and other studiesdescribed above, are that rHuEpo is indicated for thetreatment of anemic patients with non-myeloid hemato-logical malignancies and solid tumors and will, in addi-tion to reducing transfusion need, result in an importantimprovement in QOL.
MyelodysplasiaAnemia is the most common hematological abnormal-ity in patients with MDS. Treatment of MDS withrHuEpo has been investigated in a number of relativelysmall studies.18,19 A meta-analysis of 17 trials20 includ-ing 205 patients was published in 1995. In the majorityof these studies, patients were eligible for treatment with
Table 2. Clinical studies of recombinant human erythropoietin(rHuEpo) in patients with myeloma and lymphoma.
No. Treatment ControlAuthor Year Patients Response % Response %
Ludwig (*) 1990 13 85
Cazzola 1995 146 61 7
Osterborg 1996 121 60 24
Dammaco (*) 2001 145 58 9
* indicates studies where only patients with myeloma wereinvestigated

24 American Society of Hematology
rHuEpo if they had a hemoglobin of < 10.5g/dL or weretransfusion dependent. Response was generally definedas abolition of the need for transfusion or a rise in he-moglobin of > 1.5g/dL in non-transfusion dependentpatients. The overall response rate in the 17 trials was16% (33/205 patients) using quite a range of rHuEpodoses given either subcutaneously and intravenously. Themedian time to response was 8 weeks, and some of theresponses, with continued rHuEpo administration, weredurable. The patients most likely to respond were thosewho did not have sideroblastic anemia, those who werenot transfusion dependent and those whose serum eryth-ropoietin level was less than 200 U/L.
Three groups have investigated the impact of com-bination treatment with rHuEpo and G-CSF on the ane-mia of patients with MDS.21-23 When a complete response(CR) was defined as achieving a hemoglobin of > 11.5g/dl and partial response (PR) a rise in hemoglobin of >1.5 g/dL or a 100% reduction of transfusion need, a re-sponse rate of 36% (CR 21.4%; PR 14.4%) was seenwhen the results of the Scandinavian and US studies werepooled.24 In the German study,21 a good erythroid re-sponse (GER) was defined as a complete loss of trans-fusion need or as an increase of > 2.0 g/dL in hemoglo-bin, and a partial erythroid response (PER) as a reduc-tion in transfusion need of > 50% or an increase in he-moglobin of 1-2 g/dL. After 12 weeks of treatment theresponse rate was 61% (GER 43%; PER 18%) and after36 weeks the response rate was 80% (GER 56%; PER24%). If the Scandinavian response criteria were appliedto this study the overall response rate would have been50% at 12 weeks and 56% at 36 weeks. Responses havebeen durable with continued treatment in most patients,23
and the treatment has been well tolerated. No increasein risk of transformation to acute myeloid leukemia wasnoted, but a non-significant fall in platelet counts wasseen in some patients.24 There was no significant differ-ence in erythroid response rates for patients with refrac-tory anemia, refractory anemia with ringed sideroblastsor refractory anemia with excess blasts in these studies.A predictive model for response in patients with MDShas been proposed by Hellström-Lindberg.24 This modelwas based on a retrospective analysis from the combinedresults of the Scandinavian and US groups. Using multi-variate analysis the serum erythropoietin level and redcell transfusion need were used to create a scoring sys-tem that allowed patients with a high, intermediate, orlow chance of response to be identified. This model hasrecently been confirmed and simplified in a prospectivestudy.25
Patients with a transfusion need of < 2 units permonth and a serum erythropoietin concentration of <500 U/l had a 74% response rate to combined erythro-poietin/G-CSF compared to a response rate of 23% and
7% for those patients with a > 2 units per month transfu-sion need or serum erythropoietin concentration > 500U/l or both of these risk factors, respectively.
With these data available where should we go fromhere with treatment of an individual patient in the clinicand in terms of future clinical studies?
Blood Transfusion NeedTreatment with rHuEpo will reduce transfusion need byapproximately 50%, excluding transfusions requiredduring the first month of treatment before the rHuEpohas had the opportunity to work. This will be importantfor patients who are enthusiastic about avoiding bloodtransfusions on safety grounds and also where there areconcerns about the adequacy of the blood supply. Somepatients who are red cell transfusion dependent (perhapsin a palliative care setting) can benefit enormously fromrHuEpo with a significant reduction or abolition of trans-fusion need.
Are further studies in this field likely to be of value?The mean hemoglobin has been < 10.0 g/dl for patientsentered into most of the randomized trials of rHuEpo todate and approximately one fifth to one third of enteredpatients have already required transfusion at enrollment.Whether treating patients at a higher hemoglobin con-centration (say > 12.0 g/dL) would influence hemoglo-bin response or the need for transfusion is unknown andcould usefully be addressed by future studies.
Quality of LifeQOL in patients treated with rHuEpo was reported toimprove by several investigators. Demetri15 showed thatthe improvement in QOL as a function of a rise in he-moglobin level occurred independently of tumor re-sponse. An analysis of the Glaspy and Demetri data byCleeland26 demonstrated a statistically significant, non-linear relationship between hemoglobin level and QOL.RHuEpo related increases in hemoglobin were associ-ated with quality of life improvements for the hemoglo-bin range of 8.0-14.0 g/dL. The largest QOL improve-ment for each 1 g/dl increment in hemoglobin occurredwhen the hemoglobin increased from 11.0-12.0 g/dL,and little benefit was noted when the hemoglobin in-creased between 7.0-8.0 g/dL. This is somewhat counter-intuitive and a confirmatory prospective study would beenormously helpful, albeit logistically difficult.
Is it possible then to tell fatigued, anemic patientswith cancer that treatment with rHuEpo is guaranteed tomake them feel better? The short answer is no. Whatyou can say is that those patients who have a hemoglo-bin response to treatment with rHuEpo tend to have animprovement in their quality of life and some patientswill benefit enormously. Given that there are so manyfactors that influence a patient’s perception of QOL (and

Hematology 2001 25
that there is no fully accepted definition for the term), itis not surprising that correcting one parameter (hemo-globin) will not make all the patients feel wonderful allof the time. Further, large randomized trials of rHuEpo,powered to detect a priori meaningful differences inQOL, at different entry levels of hemoglobin would alsobe very useful in determining the point at which treat-ment with rHuEpo would provide optimal improvementor maintenance of QOL.
There has been a suspicion for some time that theimprovement in a patient’s QOL precedes any increasein hemoglobin and may not be just a placebo effect. Pro-ponents of this idea will be fascinated to read that eryth-ropoietin has neuroprotective effects in a mouse model.27
Perhaps some QOL effect from rHuEpo is centrallymediated?
Does Treatment with rHuEpo Improve Survival?Anemia at presentation has an adverse impact on prog-nosis for patients with hematological malignancies suchas lymphoma, myeloma and CLL and similar findingshave been reported for patients with some solid tumors.More advanced disease is likely to be associated with alower hemoglobin, but this may not be the only expla-nation for the poor outcome noted in anemic patients.Several non-randomized studies of chemo- and radio-therapy in patients with solid tumors have suggested thatcorrecting anemia during the course of treatment im-proves prognosis compared to similar patients with ane-mia left untreated.28-30
A recent randomized, placebo controlled, double-blind clinical trial of erythropoietin was reported in whichthe rHuEpo treated patients had a median survival of 17months compared to a median survival of 11 months inthe placebo treated patients.17 A subgroup analysis ac-cording to whether the patients had a hematologicalmalignancy (173 patients) or a solid tumor (202 patients)showed that the survival advantage for the rHuEpotreated group held true irrespective of the underlyingtumor type. The investigators concluded that althoughthe study was neither designed nor powered for survivalas an endpoint, the results suggest a survival benefit witherythropoietin. Further trials are underway to determineif a survival benefit is apparent, since other uncontrolledvariables may have influenced survival such as tumorstage, intensity of chemotherapy, extent of bone mar-row involvement, and disease progression.
If treatment with rHuEpo truly increases survival inanemic patients with cancer this would be very excitingand the mechanism producing the effect would be ea-gerly sought. Data from patients with solid tumors sug-gest that many tumors are hypoxic31 and that anemiacontributes to that hypoxia.32 Hypoxic tissues are lessradiosensitive than normoxic ones,33 and many cytotoxic
drugs may be less effective in hypoxic compared tonormoxic conditions.34 Studies show that regardless oftreatment, patients with hypoxic tumors are likely to haveless local disease control and less chance of cure com-pared to patients with better oxygenated tumors of thesame size and stage.35,36 Three explanations for the ad-verse impact of tumor hypoxia on survival have beenpostulated.37 First, hypoxia may induce changes withinthe tumor cells of the expression of oxygen-dependentproteins such as vascular endothelial growth factor(VEGF), which stimulates angiogenesis and increasesthe potential for tumor growth and metastases. Secondly,ionizing radiation results in the formation of free radi-cals within cells. In the presence of oxygen, the free radi-cals are fixed and interact with DNA and cell membranesto cause cell death. When cells are hypoxic, free radi-cals are not fixed and cell death may not occur.38 Thirdly,hypoxia may produce a growth advantage for tumor cellsthat are resistant to apoptosis, with a decrease in thepotential for cure or control. In addition, hypoxic tumorsmay overexpress the tumor suppressor gene p53, a cellphenotype with a higher malignant potential. Anemiamay also impair survival by influencing the patient’soverall well-being which may, in turn, impact the deliv-ery of appropriate doses of chemo and or radiotherapy.
A new insight into the mechanisms by which rHuEpotreatment might prolong survival was described thisyear.39 In a mouse myeloma model, the investigatorsshowed that treatment with rHuEpo produced completetumor responses in 51% of mice compared with 5.4%complete responses in control mice. Further detailedlaboratory studies suggested that rHuEpo triggered atumor specific immune response mediated predominantlyby CD8+ T cells. How rHuEpo caused this effect is notunderstood.
Data from patients with HIV infection also show anadverse impact of anemia on survival and also suggestthat treatment with rHuEpo can prolong survival com-pared to patients receiving no treatment or blood trans-fusion.40 Whether rHuEpo stimulates a T cell responsein these patients is not known.
What Can Be Recommended?From the available data there is excellent evidence torecommend the use of erythropoietin in anemic patientswith lymphoproliferative disorders who are receivingchemotherapy, with the aim of maintaining the hemo-globin at > 12.0 g/dL.10,26
Similarly, most research has been conducted in pa-tients with malignancies who are receiving concurrentchemo or radiotherapy. However, anemic patients withmalignant disease who are not being actively treated mayalso benefit from treatment with erythropoietin.41
The possibility that treatment with erythropoietin

26 American Society of Hematology
might enhance survival is intriguing, but it would be pre-mature to advise treatment with rHuEpo on this basis.Future studies, both in the laboratory and the clinic, arevital.
In MDS there are no placebo controlled, random-ized trials. Nevertheless, the data indicate that treatingpatients with the combination of erythropoietin and G-CSF is effective in the majority of patients whose baselinered cell transfusion need is < 2 U/month and who have aserum erythropoietin concentration of < 500 U/l. Patientsmeeting neither or just one of these criteria respond muchless well. A trial of treatment in such patients, who havecomplications from blood transfusion (such as the de-velopment of multiple red cell antibodies), making theprovision of blood difficult, is a reasonable approach.There are few data on QOL benefits in MDS patientstreated with erythropoietin/G-CSF and no studies to de-termine whether such treatment might have any impacton life expectancy. The lack of such data makes recom-mendations about the use of rHuEpo in patients withMDS uncertain. Further research is needed.
Many physicians were trained that anemia is not im-portant in patients with malignant disease until it be-came very severe. This thinking results in patients expe-riencing substantial morbidity and possible impairmentin survival. Effective treatment is available for many pa-tients using rHuEpo, but uncertainties about its real worthand its high cost still precludes its use in many healthcare systems.
REFERENCES
I. Evidence-Based Medicine and Evidence-BasedPractice Guidelines
1. Lin F-K, Suggs S, Lin C-H, et al. Cloning and expression of thehuman erythropoietin gene. Proc Natl Acad Sci USA.1985;82:7580-7584.
2. Jacobs K, Shoemaker C, Rudersdorf R, et al. Isolation andcharacterization of genomic and cDNA clones of humanerythropoietin. Nature. 1985;313; 806-810.
3. Amgen, Inc. Epogen (epoetin alfa) prescribing information. In:Physicians’ Desk Reference. 54th ed. Montvale: MedicalEconomics Press; 2000.
4. Adamson JW, Vapnek D. Recombinant erythropoietin to improveathletic performance. N Engl J Med. 1991;324:698-699.
5. Catlin DH, Hatton CK. Use and abuse of anabolic and otherdrugs. Adv Intern Med. 1991;36:399-424.
6. Sackett DL, Rosenberg WM, Gray JA, et al. Evidence basedmedicine: what it is and what it isn’t. BMJ. 1996;312:71-72.
7. The Dartmouth atlas of health care. Chicago: AmericanHospital Publishing, 1998.
8. O’Connor GT, Quinton HB, Traven ND, et al. Geographicvariation in the treatment of acute myocardial infarction: theCooperative Cardiovascular Project. JAMA. 1999;281:627-633.
9. Birkmeyer JD, Sharp SM, Finlayson SR, Fisher ES, WennbergJE. Variation profiles of common surgical procedures. Surgery.1998;124(5):917-923.
10. Adams JR, Elting LS, Lyons D, Demetri GD, Lembersky BC,Bennett CL. Evaluation of EPO use and direct-to-consumer
marketing effects: Results from a survey of American andInternational Hematologists and Oncologists. Proc Am Soc ClinOncol. 2001;20:249a.
11. Sackett DL, Richardson WS, Rosenberg W, Haynes RB.Evidence-based medicine: How to practice and teach EBM.New York: Chuchill Livingstone, 1997.
12. Geyman JP, Deyo RA, Ramsey SD, Evidence-based clinicalpractice: Concepts and approaches. Boston: ButterworthHeineman, 2000.
13. Guyatt GH, Rennie D. Users’ guides to the medical literature.JAMA. 1993;270(17):2096-2097.
14. Oxman AD, Sackett DL, Guyatt GH, The Evidence-BasedMedicine Working Group. Users’ guides to the medicalliterature. I. How to get started. JAMA. 1993; 270:2093-2095.
15. Guyatt GH, Sackett DL, Cook DJ, Evidence-Based MedicineWorking Group. Users’ guides to the medical literature. II. Howto use an article about therapy or prevention. A. Are the resultsof the study valid? JAMA. 1993;270(21):2598-2601.
16. Guyatt GH, Sackett DL, Cook DJ, Evidence-Based MedicineWorking Group. Users’ guides to the medical literature. II. Howto use an article about therapy or prevention. B. What were theresults and will they help me in caring for my patients? JAMA.1994;271(1):59-63.
17. Jaeschke R, Guyatt G, Sackett DL, Evidence-Based MedicineWorking Group. Users’ guides to the medical literature. III.How to use an article about a diagnostic test. A. Are the resultsof the study valid? JAMA. 1994;271(5):389-391.
18. Jaeschke R, Guyatt GH, Sackett DL, The Evidence-BasedMedicine Working Group. Users’ guides to the medicalliterature. III. How to use an article about a diagnostic test. B.What are the results and will they help me in caring for mypatients? JAMA. 1994;271(9):703-707.
19. Levine M, Walter S, Lee H, Haines T, Holbrook A, Moyer V,Evidence-Based Medicine Working Group. Users’ guides to themedical literature. IV. How to use an article about harm. JAMA.1994;271(20):1615-1619.
20. Laupacis A, Wells G, Richardson WS, Tugwell P, Evidence-Based Medicine Working Group. Users’ guides to the medicalliterature. V. How to use an article about prognosis. JAMA.1994;272(3):234-237.
21. Oxman AD, Cook DJ, Guyatt GH, Evidence-Based MedicineWorking Group. Users’ guides to the medical literature. VI.How to use an overview. JAMA. 1994;272(17):1367-1371.
22. Richardson WS, Detsky AS, Evidence-Based MedicineWorking Group. Users’ guides to the medical literature. VII.How to use a clinical decision analysis. A. Are the results of thestudy valid? JAMA. 1995;273(16):1292-1295.
23. Richardson WS, Detsky AS, Evidence Based Medicine WorkingGroup. Users’ guides to the medical literature. VII. How to use aclinical decision analysis. B. What are the results and will theyhelp me in caring for my patients? JAMA. 1995;273:1610-1613.
24. Hayward RS, Wilson MC, Tunis SR, Bass EB, Guyatt G,Evidence-Based Medicine Working Group. Users’ guides to themedical literature. VIII. How to use clinical practice guidelines.A. Are the recommendations valid? JAMA. 1995;274:570-574.
25. Wilson MC, Hayward RS, Tunis SR, Bass EB, Guyatt G,Evidence-Based Medicine Working Group. Users’ guides to theMedical Literature. VIII. How to use clinical practice guide-lines. B. What are the recommendations and will they help youin caring for your patients? JAMA. 1995;274(20):1630-1632.
26. Guyatt GH, Sackett DL, Sinclair JC, Hayward R, Cook DJ,Cook RJ, Evidence-Based Medicine Working Group. Users’guides to the medical literature. IX. A method for gradinghealth care recommendations. JAMA.1995;274(22):1800-1804.
27. Naylor CD, Guyatt GH, The Evidence-Based MedicineWorking Group. Users’ guides to the medical literature. X. Howto use an article reporting variations in the outcomes of health

Hematology 2001 27
services. JAMA. 1996;275(7):554-558.28. Naylor CD, Guyatt GH, Evidence-Based Medicine Working
Group. Users’ guides to the medical literature. XI. How to usean article about a clinical utilization review. JAMA.1996;275(18):1435-1439.
29. Guyatt GH, Naylor CD, Juniper E, Heyland DK, Jaeschke R,Cook DJ, Evidence-Based Medicine Working Group. Users’guides to the medical literature. XII. How to use articles abouthealth-related quality of life. JAMA. 1997;277(15):1232-1237.
30. Drummond MF, Richardson WS, O’Brien BJ, Levine M,Heyland D, Evidence-Based Medicine Working Group. Users’guides to the medical literature. XIII. How to use an article oneconomic analysis of clinical practice. A. Are the results of thestudy valid? JAMA. 1997;277(19):1552-1557.
31. O’Brien BJ, Heyland D, Richardson WS, Levine M, DrummondMF, Evidence-Based Medicine Working Group. Users’ guidesto the medical literature. XIII. How to use an article oneconomic analysis of clinical practice. B. What are the resultsand will they help me in caring for my patients? JAMA. 1997;277(22):1802-1806.
32. Dans AL, Dans LF, Guyatt GH, Richardson S, Evidence-BasedMedicine Working Group. Users’ guides to the medicalliterature: XIV. How to decide on the applicability of clinicaltrial results to your patient. JAMA. 1998;279(7):545-549.
33. Richardson WS, Wilson MC, Guyatt GH, Cook DJ, NishikawaJ, Evidence-Based Medicine Working Group. Users’ guides tothe medical literature: XV. How to use an article about diseaseprobability for differential diagnosis. JAMA.1999;281(13):1214-1219.
34. Guyatt GH, Sinclair J, Cook DJ, Glasziou P, Evidence-BasedMedicine Working Group and the Cochrane ApplicabilityMethods Working Group. Users’ guides to the medicalliterature: XVI. How to use a treatment recommendation.JAMA. 1999;281(19):1836-1843.
35. Barratt A, Irwig L, Glasziou P, et al, Evidence-Based MedicineWorking Group. Users’ guides to the medical literature: XVII.How to use guidelines and recommendations about screening.JAMA. 1999;281(21):2029-2034.
36. Randolph AG, Haynes RB, Wyatt JC, Cook DJ, Guyatt GH.Users’ Guides to the Medical Literature: XVIII. How to use anarticle evaluating the clinical impact of a computer-basedclinical decision support system. JAMA.1999;282(1):67-74.
37. Bucher HC, Guyatt GH, Cook DJ, Holbrook A, McAlister FA,Evidence-Based Medicine Working Group. Users’ guides to themedical literature: XIX. Applying clinical trial results. A. Howto use an article measuring the effect of an intervention onsurrogate end points. JAMA.1999;282(8):771-778.
38. McAlister FA, Laupacis A, Wells GA, Sackett DL. Users’ Guidesto the Medical Literature: XIX. Applying clinical trial results. B.Guidelines for determining whether a drug is exerting (morethan) a class effect. JAMA.1999;282(14):1371-1377.
39. McAlister FA, Straus SE, Guyatt GH, Haynes RB, Evidence-Based Medicine Working Group. Users’ guides to the medicalliterature: XX. Integrating research evidence with the care ofthe individual patient. JAMA. 2000;283(21):2829-2836.
40. Hunt DL, Jaeschke R, McKibbon KA. Evidence-BasedMedicine Working Group. Users’ guides to the medicalliterature: XXI. Using electronic health information resourcesin evidence-based practice. JAMA. 2000;283(14):1875-1879.
41. McGinn TG, Guyatt GH, Wyer PC, Naylor CD, Stiell IG,Richardson WS, Evidence-Based Medicine Working Group.Users’ guides to the medical literature: XXII: how to usearticles about clinical decision rules. JAMA. 2000;284(1):79-84.
42. Giacomini MK, Cook DJ, Evidence-Based Medicine WorkingGroup. Users’ guides to the medical literature: XXIII.Qualitative research in health care. A. Are the results of thestudy valid? JAMA. 2000;284(3):357-362.
43. Giacomini MK, Cook DJ, Evidence-Based Medicine WorkingGroup. Users’ guides to the medical literature: XXIII.Qualitative research in health care. B. What are the results andhow do they help me care for my patients? JAMA.2000;284(4):478-482.
44. Richardson WS, Wilson MC, Williams JW Jr, Moyer VA, NaylorCD, Evidence-Based Medicine Working Group. Users’ guides tothe medical literature: XXIV. How to use an article on the clinicalmanifestations of disease. JAMA. 2000;284(7):869-875.
45. Guyatt GH, Haynes RB, Jaeschke RZ, et al, Evidence-BasedMedicine Working Group. Users’ Guides to the MedicalLiterature: XXV. Evidence-based medicine: principles forapplying the Users’ Guides to patient care. JAMA.2000;284(10):1290-1296.
46. U.S. Preventive Services Task Force. Guide to ClinicalPreventive Services (2nd ed). Baltimore: Williams & Wilkins,1996.
47. Seidenfeld J, Piper M, Flamm C, et al. Epoetin treatment foranemia of cancer therapy: a systematic review and meta-analysis of controlled clinical trials. J Natl Cancer Inst.2001;93:1204-1214.
II. Building the Case: What Evidence Exists forUsage of Epoietin and How Good Is the Evidence?
1. http://www.ahrq.gov/clinic/epcix.htm, accessed on June 1, 2001.2. Aronson N, Seidenfeld J, Piper MA, Flamm C, Hasselblad V.
Use of Erythropoietin in Oncology. Evidence Report/Technol-ogy Assessment No. 30. (Prepared by the Blue Cross and BlueShield Association Evidence-based Practice Center underContract No. 290-97-0015.) AHRQ Publication No. 01-E009.Rockville, MD: Agency for Healthcare Research and Quality.
3. Case DC Jr, Bukowski RM , Carey RW, Fishkin EH, Henry DH,Jacobson RJ, et al. Recombinant human erythropoietin therapyfor anemic cancer patients on combination chemotherapy. JNatl Cancer Inst. 1993;85(10):801-6.
4. Henry DH, Brooks BJ Jr, Case DC Jr, et al. Recombinant humanerythropoietin therapy for anemic cancer patients receivingcisplatin chemotherapy. Cancer J Sci Am. 1995;1(4):252-260.
5. Cascinu S, Fedeli A, Del Ferro E, Fedeli SL, Catalano G.Recombinant human erythropoietin treatment in cisplatin-associated anemia: a randomized, double-blind trial withplacebo. J Clin Oncol. 1994;12(5):1058-62.
6. Kurz C, Marth C, Windbichler G, et al. Erythropoietin treatmentunder polychemotherapy in patients with gynecologicmalignancies: a prospective, randomized, double-blind placebo-controlled multicenter study. Gynecol Oncol. 1997;65(3):461-6.
7. Littlewood TJ, Bajetta E, Nortier JWR, Vercammen E, RapoportB for the Epoetin Alfa Study Group. Effects of epoetin alfa onhematologic parameters and quality of life in cancer patientsreceiving nonplatinum chemotherapy: results of a randomized,double-blind, placebo-controlled trial. J Clin Oncol.2001;19:2865-2874.
8. Wurnig C, Windhager R, Schwameis E, et al. Prevention ofchemotherapy-induced anemia by the use of erythropoietin inpatients with primary malignant bone tumors (a double-blind,randomized, phase III study). Transfusion. 1996;36(2):155-9.
9. Porter JC, Leahey A, Polise K, Bunin G, Manno CS. Recombi-nant human erythropoietin reduces the need for erythrocyte andplatelet transfusions in pediatric patients with sarcoma: arandomized, double-blind, placebo-controlled trial. J Pediatr.1996;129(5):656-60.
10. Quirt I, Coutere F, Pichette R, et al. The role of recombinanthuman erythropoietin (EPO) in reducing red blood celltransfusions and maintaining quality of life (QOL) in patientswith lymphoma and solid tumors receiving cytotoxic chemo-therapy: results of a randomized, double-blind, placebo-

28 American Society of Hematology
controlled clinical trial. Blood. 1996;88(10 Suppl. 1):347a.(abstract # A1378).
11. Oberhoff C, Neri B, Amadori D, et al. Recombinant humanerythropoietin in the treatment of chemotherapy-inducedanemia and prevention of transfusion requirement associatedwith solid tumors: a randomized, controlled study. Ann Oncol.1998;9(3):255-60.
12. ten Bokkel Huinink WW, de Swart CAM, van Toorn DW, et al.Controlled multicentre study of the influence of subcutaneousrecombinant human erythropoietin on anaemia and transfusiondependency in patients with ovarian carcinoma treated withplatinum-based chemotherapy. Med Oncol. 1998;15(3):174-82.
13. Sweeney PJ, Nicolae D, Ignacio L, et al. Effect of subcutaneousrecombinant human erythropoietin in cancer patients receivingradiotherapy: final report of a randomized, open-labelled, phaseII trial. Br J Cancer. 1998;77(11):1996-2002.
14. Thatcher N, De Campos ES, Bell DR, et al. Epoetin alphaprevents anaemia and reduces transfusion requirements inpatients undergoing primarily platinum-based chemotherapy forsmall cell lung cancer. Br J Cancer. 1999;80(3-4):396-402
15. Silvestris F, Romito A, Fanelli P, Vacca A, Dammacco F. Long-term therapy with recombinant human erythropoietin (rHu-EPO) in progressing multiple myeloma. Ann Hematol.1995;70(6):313-8.
16. Varan A, Buyukpamukcu M, Kutluk T, Akyuz C. Recombinanthuman erythropoietin treatment for chemotherapy-relatedanemia in children. Pediatrics 1999;103(2):E161-4.
17. Henke M, Guttenberger R, Barke A, Pajonk F, Potter R,Frommhold H. Erythropoietin for patients undergoingradiotherapy: a pilot study. Radiother Oncol 1999;50(2):185-90.
18. Gamucci T, Thorel MF, Frasca AM, Giannarell D, Calabresi F.Erythropoietin for the prevention of anaemia in neoplasticpatients treated with cisplatin. Eur J Cancer 1993;29A (Suppl2):S13-4.
19. Del Mastro L, Venturini M, Lionetto R, et al. Randomizedphase III trial evaluating the role of erythropoietin in theprevention of chemotherapy-induced anemia. J Clin Oncol.1997;15(7):2715-21.
20. Welch RS, James RD, Wilkinson PM, Belli F, Cowan RA.Recombinant human erythropoietin and platinum-basedchemotherapy in advanced ovarian cancer. Cancer J Sci Am.1995;1(4):261-66.
21. Markman M, Reichman B, Hakes T, Rubin S, Jones W, LewisJL Jr., et al. The use of recombinant human erythropoietin toprevent carboplatin-induced anemia. Gynecol Oncol.1993;49(2):172-6.
22. Lavey RS, Dempsey WH. Erythropoietin increases hemoglobinin cancer patients during radiation therapy. Int J Radiat OncolBiol Phys. 1993;27(5):1147-52.
23. Leon P, Jimenez M, Barona P, Sierrasesúmaga L. Recombinanthuman erythropoietin for the treatment of anemia in childrenwith solid malignant tumors. Med Pediatr Oncol.1998;30(2)110-16.
24. Dusenbery KE, McGuire WA, Holt PJ, et al. Erythropoietinincreases hemoglobin during radiation therapy for cervicalcancer. Int J Radiat Oncol Biol Phys. 1994; 29:1079-84.
25. Italian Cooperative Study Group for rHuEpo inMyelodysplastic Syndromes. A randomized double-blindplacebo-controlled study with subcutaneous recombinanthuman erythropoietin in patients with low-risk myelodysplasticsyndromes. Br J Haematol. 1998;103(4):1070-4.
26. Garton JP, Gertz MA, Witzig TE, et al. Epoetin alfa for thetreatment of the anemia of multiple myeloma. A prospective,randomized, placebo-controlled, double-blind trial. Arch InternMed. 1995;155(19):2069-74.
27. Rose E, Rai K, Revicki D, Brown R, Reblando J and the EPO inAnemia of CLL Study Group. Clinical and health statusassessments in anemic chronic lymphocytic leukemia (CLL)patients treated with epoetin alfa (EPO) [abstract]. Blood.1994;84:526a.
28. Osterborg A, Boogaerts MA, Cimino R, et al. Recombinanthuman erythropoietin in transfusion-dependent anemic patientswith multiple myeloma and non-Hodgkin’s lymphoma—arandomized multicenter study. The European Study Group ofErythropoietin (Epoetin Beta) Treatment in Multiple Myelomaand Non-Hodgkin’s Lymphoma. Blood. 1996;87(7):2675-2682.
29. Dammacco F, Silvestris F, Castoldi GL, et al. The effectivenessand tolerability of epoetin alfa in patients with multiplemyeloma refractory to chemotherapy. Int J Clin Lab Res.1998;28:127-134.
30. Cazzola M, Messinger D, Battistel V, et al. Recombinant humanerythropoietin in the anemia associated with multiple myelomaor non-Hodgkin’s lymphoma: dose finding and identification ofpredictors of response. Blood. 1995;86:4446-4453.
31. Link H, Boogaerts MA, Fauser AA, et al. A controlled trial ofrecombinant human erythropoietin after bone marrowtransplantation. Blood. 1994;84:3327-3335.
32. Klaesson S, Ringden O, Ljungman P, Lonnqvist B, Wennberg L.Reduced blood transfusions requirements after allogeneic bonemarrow transplantation: results of a randomised, double-blindstudy with high-dose erythropoietin. Bone Marrow Transplant.1994;13:397-402.
33. Biggs JC, Atkinson KA, Booker V, et al. Prospectiverandomised double-blind trial of the in vivo use of recombinanthuman erythropoietin in bone marrow transplantation fromHLA-identical sibling donors. The Australian Bone MarrowTransplant Study Group. Bone Marrow Transplant.1995;15:129-134.
34. Steegmann JL, Lopez J, Otero MJ, et al. Erythropoietintreatment in allogeneic BMT accelerates erythroid reconstitu-tion: results of a prospective controlled randomized trial. BoneMarrow Transplant. 1992;10:541-546.
35. Vannucchi AM, Bosi A, Linari S, et al. High doses of recombi-nant human erythropoietin fail to accelerate platelet reconstitu-tion in allogeneic bone marrow transplantation. Results of apilot study. Haematologica. 1997;82:53-56.
36. Link H, Brune T, Hubner G, et al. Effect of recombinant humanerythropoietin after allogenic bone marrow transplantation. AnnHematol. 1993;67:169-173.
37. Locatelli F, Zecca M, Pedrazzoli P, et al. Use of recombinanthuman erythropoietin after bone marrow transplantation inpediatric patients with acute leukemia: effect on erythroidrepopulation in autologous versus allogeneic transplants. BoneMarrow Transplant. 1994;13:403-410.
38. Vannucchi AM, Bosi A, Ieri A, et al. Combination therapy withG-CSF and erythropoietin after autologous bone marrowtransplantation for lymphoid malignancies: a randomized trial.Bone Marrow Transplant. 1996;17:527-531.
39. Chao NJ, Schriber JR, Long GD, et al. A randomized study oferythropoietin and granulocyte colony-stimulating factor (G-CSF) versus placebo and G-CSF for patients with Hodgkin’sand non-Hodgkin’s lymphoma undergoing autologous bonemarrow transplantation. Blood. 1994;83:2823-8.
40. Ayash LJ, Elias A, Hunt M, et al. Recombinant humanerythropoietin for the treatment of the anaemia associated withautologous bone marrow transplantation. Br J Haematol.1994;87:153-161.
41. Pene R, Appelbaum FR, Fisher L, et al. Use of granulocyte-macrophage colony-stimulating factor and erythropoietin incombination after autologous marrow transplantation. BoneMarrow Transplant. 1993;11:219-222

Hematology 2001 29
III. ASH/ASCO Guidelines on the Use ofErythropoietin
1. See http://www.ahrq.gov/clinic/epcix.htm2. Seidenfeld J, Piper M, Flamm C, et al. Epoetin treatment for
anemia of cancer therapy: a systematic review and meta-analysis of controlled clinical trials. J Natl Cancer Inst. 2001. Inpress.
3. Gabrilove JL, Einhorn LH, Cleeland CS, Livingston RB, WinerE. Once weekly dosing of epoetin alfa increases hemoglobinand improves quality of life (QOL) in patients with hematologicmalignancies. Blood. 1999;94(suppl. 1):400a,
4. Gabrilove JL, Cleeland CS, Livingston RB, Sarokhan B, WinerE, Einhorn LH. Clinical evaluation of once weekly dosing ofEpoetin Alfa in chemotherapy patients. Improvements inhemoglobin and quality of life are similar to three-times-weekly dosing. J Clin Oncol. 2001;19(11):2875-2882.
5. Littlewood TJ, Bajetta E, Nortier JWR, Vercammen E, RapoportB. Effects of epoetin alfa on hematologic parameters andquality of life in cancer patients receiving nonplatinumchemotherapy: results of a randomized, double blind, placebocontrolled trial. J Clin Oncol. 2001;19(11):2865-2874.
6. Osterborg A, Boogaerts MA, Cimino R, et al. Recombinanthuman erythropoietin in transfusion dependent anemic patientswith multiple myeloma and non-Hodgkin’s lymphoma. Arandomized multicenter study. Blood. 1996;87(7):2675-2682.
7. Dimeo F, Fetscher S, Lange W, Mertelsmann R, Keul J. Effectsof aerobic exercise on the physical performance and incidenceof treatment related complications after high dose chemo-therapy. Blood. 1997;90(9):3390-3394.
8. Breitbart W, Rosenfeld B, Kain M, Funesti-Esch J. A random-ized double-blind, placebo controlled trial of psychostimulantsfor the treatment of fatigue in ambulatory patients with humanimmunodeficiency virus disease. Arch Int Med. 2001;161:411-420.
9. Cella D, Perman A, Passik S, Jacobsen P, Breitbart W. Progresstoward guidelines for the management of fatigue. NCCNproceedings. Oncology. 1998;12(11A):369-377.
10. Brezden C, Phillips DA, Abdolell M, Bunston T, Tannock I.Cognitive function in breast cancer patients receiving adjuvantchemotherapy. J Clin Oncol. 2000;18(14):2695-2701.
11. Courneya K, Friedenreich CM. Physical exercise and quality oflife following cancer diagnosis. A literature review. Ann BehavMed. 1999;21(2):171-179.
12. Glaspy J, Jadeja J, Justice G, et al. Randomized, active-controlled, phase I/II, dose-escalation study of NESP adminis-tered weekly and every two weeks in patients with solid tumors.Proc Am Soc Clin Oncol. 2001;20:387a.
IV. The Efficacy of Recombinant Erythropoietinin Cancer-Related Anemia: Where Do We Gofrom Here?
1. Spivak JL. Recombinant human erythropoietin and the anemiaof cancer. Blood. 1994;84: 997-1004.
2. San Miguel JF, Garcia-Sanz R, Gonzalez M, et al. A newstaging system for multiple myeloma based on the number of S-phase plasma cells. Blood. 1995;85(2):448-455.
3. Kyle RA. Multiple myeloma: Review of 869 cases. Mayo ClinProc. 1975;50(1):29-40.
4. Coiffier B. Anemia associated with non-platinum chemotherapy(CT) for Hodgkin’s lymphoma (HL) or non-Hodgkinslymphoma (NHL) [abstract]. ECCO 10 Programme 1999:35:S19, abstract 54.
5. Miller CB, Jones RJ, Piantadosi S, et al. Decreased erythropoi-etin response in patients with the anemia of cancer. N Engl JMed. 1990;322(24):1689-1692.
6. Cazzola M, Mercuriali F, Brugnara C. Use of recombinanterythropoietin outside the setting of uremia. Blood.1997;89:4248-4267.
7. Vogelzang NJ, Breitbart W, Cella D et al. Patient, caregiver andoncologist perceptions of cancer-related fatigue: results of atripart assessment survey. Semin Hematol. 1997;34(Suppl 2):4-12.
8. Barrett-Lee PJ, Bailey NP, O’Brien MER, Wager E. Large scaleUK audit of blood transfusion requirements and anaemia inpatients receiving cytotoxic chemotherapy. Br J Cancer.2000:82:93-97.
9. Ludwig H, Fritz E, KotzmannH, Hocker P, Gisslinger H, BarnasU. Erythropoietin treatment of anemia associated with multiplemyeloma. N Engl J Med. 1990;322:1693-1699.
10. Cazzola M, Messinger D, Battistel V et al. Recombinant humanerythropoietin in the anemia associated with multiple myelomaor non-Hodgkin’s lymphoma: dose finding and identification ofthe predictors of response. Blood. 1995;86:4446-4453.
11. Osterborg A, Boogaerts MA, Cimino R, et al. Recombinanthuman erythropoietin in transfusion-dependent anemic patientswith multiple myeloma and non-Hodgkin’s lymphoma—arandomised multicentre study. Blood. 1996;87:2675-2682.
12. Dammaco F, Castoldi G and Rodjer S. Efficacy of epoetin alfain the treatment of anaemia of multiple myeloma. Br J Haem.2001;113:172-179.
13. Rose E, Rai K, Revicki D, Brown R and Reblando J. Clinicaland health status assessments in anemic chronic lymphocyticleukemia (CLL) patients treated with epoetin alfa (epo).Blood.1994;84:526a.
14. Glaspy J, Bukowski R, Steinberg D, et al. Impact of therapywith epoetin alfa on clinical outcomes in patients withnonmyeloid malignancies during cancer chemotherapy incommunity oncology practice. J Clin Oncol. 1997;15(3):1218-1234.
15. Demetri GD, Kris M, Wade J, et al. Quality-of-life benefit inchemotherapy patients treated with epoetin alfa is independentof disease response or tumor type: Results from a prospectivecommunity oncology study. J Clin Oncol. 1998;16(10):3412-3425.
16. Gabrilove JL, Einhorn LH, Livingston RB, Winer E, CleelandCS. Once-weekly dosing of Epoetin alpha is similar to three-times-weekly dosing in increasing hemoglobin and quality oflife. J Clin Oncol. 2001;19(11):2875-2882.
17. Littlewood TJ, Bajetta E, Nortier JW, Vercammen E, RapoportB. Effects of epoetin alfa on hematologic parameters andquality of life in cancer patients receiving nonplatinumchemotherapy: results of a randomized, double-blind, placebo-controlled trial. J Clin Oncol. 2001;19(11):2865-2874.
18. Italian Cooperative Study Group for rHuEpo inMyelodysplastic Syndromes. A randomised double-blindplacebo controlled study with subcutaneous recombinanthuman erythropoietin in patients with low risk myelodysplasticsyndromes. Br J Haematol. 1998;103:1070-1074.
19. Stein RS, Abels RI, Krantz SB. Pharmacologic doses ofrecombinant human erythropoietin in the treatment ofmyelodysplastic syndromes. Blood. 1991;78:1658-1663.
20. Hellstrom-Lindberg E. Efficacy of erythropoietin in themyelodysplastic syndromes: a meta-analysis of 205 patientsfrom 17 studies. Br J Haematol. 1995;89:67-71.
21. Negrin RS, Stein R, Vardiman J, et al. Treatment of the anemiaof myelodysplastic syndromes using recombinant humangranulocyte colony stimulating factor in combination witherythropoietin. Blood. 1993;82:737-743.
22. Hellstrom-Lindberg E, Ahlgren T, Beguin E, et al. Treatment ofanemia in myelodysplastic syndromes with granulocyte colonystimulating factor plus erythropoietin: results from a random-ized phase II study and long term follow up of 71 patients.

30 American Society of Hematology
Blood. 1998;92:68-75.23. Mantovani L, Lentini G, Hentschel B, et al. Treatment of
anaemia in myelodysplastic syndromes with prolongedadministration of recombinant human granulocyte colony-stimulating factor and erythropoietin. Br J Haematol.2000;109:367-375.
24. Hellstrom-Lindberg E, Negrin R, Stein R et al. Erythroidresponse to treatment with G-CSF plus erythropoietin for theanaemia of patients with myelodysplastic syndromes: proposalsfor a predictive model. Br J Haematol. 1997;99:344-351.
25. Hellstrom-Lindberg E, Ahlgren T, Dahl I et al. A final decisionmodel for treating the anemia of myelodysplastic syndromes(MDS) with Epo and G-CSF. Blood. 2000;96:2347a.
26. Cleeland CS, Demetri GD, Glaspy J, Cella DF, Portenoy RK.Identifying haemoglobin level for optimal quality of life:results of an incremental analysis. Proc Am Soc Clin Oncol.1999; 18; 2215a.
27. Brines ML, Ghezzi P, Keenan S et al. Erythropoietin crosses theblood-brain barrier to protect against experimental brain injury.PNAS. 2000;97:10526-10531.
28. Grogan M, Thomas GM, Melamed I, et al. The importance ofhemoglobin levels during radiotherapy for carcinoma of thecervix. Cancer. 1999;86:1528-1536.
29. Antonadou D, Cardamekis E, Sarris V, Tzigounia N. Effect ofthe administration of recombinant human erythropoietin inpatients with pelvic malignancies during radiotherapy.Radiother Oncol 1998;48:S122.
30. Glaser C, Millesi W, Gossweiner S, et al. r-HuErythropoietinsupply increases efficacy of neoadjuvant radiochemotherapy inpatients with oral squamous cell carcinoma. Proc Am Soc ClinOncol. 1998;17:397a .
31. Molls M, Stadler P, Becker A, Feldmann HJ, Dunst J. Relevanceof oxygen in radiation oncology. Mechanisms of action,correlation to low hemoglobin levels. Strahlenther Onkol.1998;174(Suppl IV):13-16.
32. Kelleher DK, Matthiensen U, Thews O, Vaupel P. Blood flow,oxygenation and bioenergetic status of tumors after erythropoi-etin treatment in normal and anemic rats. Cancer Res.1996;56:4728-4734.
33. Hall EJ: The oxygen effect and reoxygenation. In Hall EJ, ed.Radiobiology for the Radiologist, 4th ed. Philadelphia:Lippincott; 1994:133-152.
34. Teicher BA, Holden SA, Al-Achi A, Herman TS. Classificationof antineoplastic treatments by their differential toxicity towardputative oxygenated and hypoxic tumor subpopulations in vivoin the FSaIIC murine fibrosarcoma. Cancer Res. 1990;50:3339-3344.
35. Höckel M, Schlenger K, Arral B, Mitze M, Schäffer U, VaupelP. Association between tumour hypoxia and malignantprogression in advanced cancer of the uterine cervix. CancerRes. 1996;56:4509-4515.
36. Brizel DM, Sibley GS, Prosnitz LR, Scher RL, Dewhirst MW.Tumor hypoxia adversely affects the prognosis of carcinoma ofthe head and neck. Int J Radiat Oncol Biol Phys. 1997;38:285-289.
37. Höckel M, Schlenger K, Hockel S, Vaupel P. Associationbetween tumor hypoxia and malignant progression: the clinicalevidence in cancer of the uterine cervix. In Vaupel P, KelleherDK, eds. Tumor Hypoxia. Stuttgart: WissenschaftlicheVerlagsgesellschaft mbh; 1999:65-74.
38. Hall EJ. The oxygen effect and reoxygenation. In Hall EJ, ed.Radiobiology for the Radiologist, 4th ed. Philadelphia;Lippincott: 1994:133-152.
39. Mittelman M, Neumann D, Peled A, Kanter P, Haran-Ghera N.Erythropoietin induces tumor regression and antitumor immuneresponses in murine myeloma models. Proc Natl Acad Sci USA.2001;98:5181-5186.
40. Moore RD. Human immunodeficiency virus infection, anemiaand survival. Clin Infect Dis. 1999;29:44-49.
41. Abels RI. Use of recombinant human erythropoietin in thetreatment of anemia in patients who have cancer. Semin Oncol.1992;19(Suppl 8):29-35.





























