Embed Size (px)
Citation preview

CLIN. RESEARCH & REG. AFFAIRS, 10(3), 187-202 (1993)
EQUIVALENCE AND IDENTITY CONCEPTS IN MANUFACTURING AND STABILITY TESTING.
J.T. Carstensen School of Pharmacy
University of Wisconsin, Madison, WI 53706
INTRODUCTION
The quality, safety and efficacy of a product on the market is tied into its stability
and manufacture, both as regards physical and chemical parameters. This paper will call attention to some of the shortcomings and some of the approximations that are made in manufacturing and in stability testing, and also call attention to the fact that there is a substantial difference between the words "equivalence" and "identity". The article to follow consists of (documented) instances of the authors's experiences, as outside observer, of FDA/Industry interactions. They do not, in any way, claim to be the view of either Industry or the FDA.
CLASSIFICATION OF IDENTITY
In order to talk about manufacturing and stability of a drug product, there are two fundamental aspects (and several subdivisions):
0 0 The storage condition.
The drug product including the package
In a Utopian sense, it would seem simple to state that:
0 0 tested in the clinic, 0 approved by the FDA, 0 0
a product is made by a certain procedure,
manufactured on large scale, and tested for drug decomposition and other attributes as a function of time.
187
Copyright @ 1993 by Marcel Dekker, Inc.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

188 CARSTENSEN
The last point would, then, be the function which involves the concept of stability monitoring. In the Utopian situation we then have the set of (unrealistic) conditions that
1. It is possible to, at any time, produce an exact large-scale replicate of the product which was produced at the clinical test time
It is possible to store this at isothermal, iso-RH conditions until it is used by the patient.
2 .
There are obvious flaws in each of these arguments. The first concept will be examined first.
REPRODUCIBILITY
A simple-minded view of the FDAAndustry interactions is best presented in a historical sense: Why did the FDA come into strong being in the first place? The answer is the ethylene glycol solvent used in a pediatric preparation in the late thirties. The product killed a number of children. The answer, hence, is that someone did something which was professionally incorrect.
In fact if all products were produced with the concept of product quality first and foremost in mind, and if professionals (pharmacists, engineers, chemists, management) strived to ensure that what a company had PROVEN clinically at year zero, was really what they would give to the patient or customer in year X, then there would really be no need for a FDA.
The flip side of such an idealistic coin is that, of course, there would be an FDA anyway, because there are people who would, politically, not want to see the FDA disappear, and the argument would be that the statement above would never be true.
The above considerations beg for one of the following approaches, presented in question form:
1. How can one, realistically, attain a situation which is close to the Utopian situation?
However, another approach would be:
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABILITY TESTING 189
2 . How much can a company get away with?a
A thud premise would be, and t h s is often close to reality:
3 . It is difficult to figure out what the FDA wants, so the company might run the operation as it thinks it can economically best do it, and still be professional about it.
It is the author's opinion that it is mostly the third situation which prevails in Industry, both ethical and generic, although there may always be some aspect of point 2 above present. In the following it will be assumed that it is statement 3 above whch is correct
The first erroneous part of this statement is to say:
The FDA.
There are people and groups in the FDA that are at odds with one another, and if a company complies with one group, then another may still not agree. So a company may obtain the approval on an NDA or an ANDA and find that the compliance branch disapproves.
The approval process simply says to the company: If what you say is correct then you may market the product. The pre-NDA or ANDA inspection (or any other FDA audit) addressess: Is what you say correct? It is like getting approval on a bank loan, but then having it rejected upon inspection of the house you want to buy.
483 CITATIONS
Violations of CGMP's are often referred to as 483 citations or simply 483's. It is difficult to have an inspection without an inspector finding something wrong. A company has thirty days to correct 483's, and on the re-inspection a set of new and
a This is a somewhat cynical statement, but it is not free from having basis in fact in certain cases that have passed through the courts of the U.S.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

190 CARSTENSEN
different 483's may be issued, so the situation can be difficult. In the worst scenario, the company could be shut down. Officers of the corporation would be asked to appear before the court on short notice and argue why the FDA should not order the plant closed.
But reason, in general, prevails in the FDA, even though different points of view may be espoused by different fractions within the agency. So how does a company deal with such a situation?
Again, let us return to the original premise: That in the Utopian version, one wants to guarantee the public, that what is sold to them is "identical" to what was tested in the clinic. Possible modes of action are listed in the following.
PREREQUISITES
One idealistic view here would be, taking solid dosage forms as an example:
An innovator comes up with a new drug substance and drug product, tests it for toxicity, safety, dose level, clinical effects, stability and bioavailability. This is an expensive affair, but if the firm gets permission to market, the rewards are great for up to 17 years (patent life).
Let us look at the process by which the product is made, it can either be:
(a) (b) a wet granulated product.
a dry-blended product which is encapsulated or directly compressed or
In the process of making the product for clinical trials, there is usually not much material available (synthesis), and the first batches will be smaller (and in dose- ranging, they will not necessarily be the correct strength).
So there are scale-up trials, and larger and larger equipment is used. In today's climate the FDA requires some assurance, in a clinical sense, that the larger batch is equivalent to the smaller batch. So there are bioequivalence guidelines.
But bioequivalence is not bioequality?!
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABILITY TESTING 191
Suppose, for the time being, that a process and product are approved. In the ideal situation, the product procuded by all subsequent batches would be exactly the same (a premise which is not correct).
In an operational sense, i.e. when the product is in production, the repeatability of a process is a function of (a) the product, (b) the equipment and (c) the personnel.
The product should be robust. In other words it is not enough to be able to make simply a prototype of the product in the development stage. The constancy of the product under manufacturing variations and perturbations should be assured. An example of this would be that if a hydrate is used in the formula, it may start losing water under certain FU-I condhons and it might gain water under other conditions.
The personnel should be well trained. By this it is not simply meant that they are shown what valves to turn at a given time, but they should have an appreciation of what the law is, as regards quality. Also they should understand the reasons for the various ingredients and steps in the process.
The working climate should be one of neither leisure nor work overload. Contented employees are a good cornerstone for good quality. Not everything can be supervised, so one relies, to a certain extent on the intelligence and attitude of the worker.
One danger is that on-line operators have a tendency to become self-styled efficiency experts and they try to take shortcuts. Such practices must be constantly policed.
The personnel should be well supervised. The supervisor should spend a fair amount of time on the floor, and it should be he, not the operator, who has the say when decisions have to be made.
THE LIMITS OF WRITTEN INSTRUCTIONS
Written instructions are often used to make procedures reproducible. However,
nothing can be written so that two different people will do exactly the same thing
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

192 CARSTENSEN
simply by reading such instructions. That is why training is important. Even then things may change, since, a bit like folklore, small changes creep in, and the mode of manufacture ten years after introduction might be different, even if the instructions were the same.
An example of this is a product made in the US in the 60's and 70's. It was
transferred to Puerto Rico, and after two years of bad experience there, the company transferred it back to the States. By then Stateside personnel could not make it well either (they had "forgotten" how to). The problems were eventually ironed out, but it shows that however good instructions may be, they are never all encompassing and perfect.
ASSURING II REPRODUCIBILITY
Even if the written word can never quite suffice, there must, nevertheless, be written methods, and the more complete they are, and the better they are enforced, the better the reproducibility of the product.
There are two aspects to this:
1. Quality Assurance: This is the quality-conscious, procedure-driven mode of manufacturing the product.
Quality Control. This is the spot-checking, after the fact, that the product meets certain specifications.
2.
Both are necessary in the quest for reproducibility, imperfect as they may be. How good they are depends on the breadth and width of the specifications, standard operating procedures and specific instructions, the training and attitude of the personnel and the soundness with which scheduling and general operation is carried out.
Quality Control is, as mentioned, spot-checking the quality of the product. Meeting specifications does not assure that a product is satisfactory. Statistical concepts such as a-errors and gerrors and operational characteristics curves deal with the
deviations that can be expected, and introduce such terms as Manufacturers Cost and Consumer Risk.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABILITY TESTING 193
So reproducibility is not "assured" by means of testing (Quality Control). Quality
Control does not supplant the necessity for process control. An example is the official Sterility Test where Operational Characteristics Charts will, alarmingly, show that there are high probabilities of passing batches that are not satisfactory (i.e. contain an unacceptable percentage of non-sterile ampoules).
So even if the release assay of a product is within specifications the product might still be less than acceptable quality. This means that one must always define what it means that a product is satisfactory. This is the basis for the statistical evaluation (e.g. OCC's) and sample size determination.
How well a process runs should always be monitored by the use of Quality Control Charts (Deming, Shewhart's)
PROCESS CHANGES
The Utopian situation discussed earlier of a product made at time X being physically identical to the batch made at the time of clinical testing is never achieved. As mentioned there are scaling-up steps in product development. So the best that can be done is to:
1.
2.
Assign meaningful manufacturing procedures that are always followed.
Set meaningful specifications, i.e. specifications of pertinent parameters, and hopefully ALL the pertinent parameters. (This, in itself, is also Utopian, because it is difficult, at the inception of a product, to visualize all the parameters that may be of importance).
Even when a company has the best intentions of always malung the product "the same way" there will be situations where changes are necessary.
If a process change is made it may be either major or minor. This article will not attempt differentiation between what constitutes a minor and what constitutes a major change. This is a legal issue, and if a company is ever entangled in it, it should obtain an outside legal opinion, and make sure to notify the FDA of it immediately. Simply to assume that it is minor, and that reporting it can wait until the yearly report is unwise.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

194 CARSTENSEN
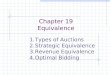
4.3 -
4.2 - n E E
4.1- m 2! Y '- 4.0- f
3.9 -
y = 4.4494 + -0.50197*LOG(x) R"2 = 0.994
0 10 Hardness
20
Fig. 1. Typical thicknesdhardness relation in a tablet below the critical pressure.
EQUIVALENCE AND IDENTITY
In a scientific sense, a change would be justified if it produces exactly the same product as before the change was made. We shall see shortly that this is not 100% possible. So the next question becomes: are the resultant changes sufficiently small so that the products before and after are "equivalent"?
Suppose a tablet product were manufactured and only tested for hardness (Fig. 1). If a process change were made and it was found that the hardness did not change one might say that the product met all specifications it met before, so it is "the same". But turning this a bit around, someone might ask: "Was it necessary to change the tableting pressure to achieve that?", and if the answer is yes, then the products are no longer the same. Even if the answer were No, they might still not be "the same", because only one parameter had been tested in that case.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABILITY TESTING 195
The disintegration might change. The dissolution profile might change. And suppose they didn't? When testing is carried out one will never produce exactly the same number twice in a row, so the numbers will not be the same, so even if identity were possible, the question becomes whether the differences are "significant"? One can assess this statistically and if the differences caused by the change are "insignificant", then the product produced by the altered process is "equivalent" to that of the old process. As judged by the parameters tested! ! But, to repeat, it is never possible to completely describe a product by a finite number of parameters.
Since it is not possible to prove "identity" one compromises and uses the concept of "equivalence". This is another word for "failing to show that things are different". This is associated with a certain confidence limit, e.g. the new process might produce product which was actually 90% as effective as that produced by the old process. Various FDA guidelines provide some requirements on the "power of the test", i.e. one is 95% certain that the parameter of the test is at least 90% of the value of the item with whch it is being compared.
Let us say that a product is produced, and in a four year span four process changes are made. In the extreme, the following might be the case: the first time the "efficiency" could be 90% of what it was in the approval batch, in the second it could be 90% of 90% i.e. 81% as "effective" and the fourth time it could be 0.81 x 0.81 = 65% as "effective" as it was originally. Grantedly, this is the worst case scenario, but is shows the problem that exists with process changes and the concept of equivalence.
So the wise way is never to have process changes. But in real life, that is not possible. So for this, and other reasons, it is necessary to couple the concept with "physical equivalence".
To reiterate: procedural changes are necessary from time to time, and there may be many good reasons for this. The equipment may have given out, and replacement of the same equipment is not longer possible. As mentioned the definition and dividing lines between minor and major are difficult to define. In general a minor change is one which tightens the tolerances of a product without a change in
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

196 CARSTENSEN
equipment. But this is not an official definition. In such cases, one should define the product, by all possible means and show that it is "the same".
The concern is, of course, that nothing be on the market which is not safe, not of quality and not efficacious. This would appear to be the reason that there is a tendency on the FDA's part to ask for all the tests they can possibly think of. It is author's feeling that often the FDA asks for so many tests that a company becomes counteractive, not proactive, and therefore will do as little as is required to meet the "demands". That is one reason that the FDA, themselves, really do not like Guidelines. But once issued, they become a way of life, and one starts thinking, that if something is done according to Guidelines, then it is satisfactory. The Guidelines then tend to take the aspect of being the law, and people feel that if they follow them, then that is all that is expected.
It should be pointed out that Guidelines cannot be followed only partially. One example is expiration where, originally, certain generic companies simply formulated their products to pass the official Accelerated Test (three months 40°C, 75% RH), and then assumed they had met their responsibilities. This, of course, is not true. If they are met, then the FDA will grant (in many cases) a 2 year expiration period. But the follow-up at real time is still necessary. In the follow-up it is necessary to be 95% sure that average of the product (batch) is above the lower label claim at expiration date. Also the company is responsible for individual units being above 85% Label Claim if one considers this the limit of content uniformity (with one "outlier" being allowed above 75% Label Claim).
SCHEDULING, PLANT CAPACITY AND PRODUCT QUALITY
A problem which leads to uncertainty of quality on the part of the manufacturer is the number of products that are made at a given site. The more products a company has on one site, the more clean-up and set-up time and the greater the chances of cross-contamination. Not only does that add to cost and uncertainty of quality, but it is also inefficient.
In setting price of products, such costs as man-power, actual power, floor space cost (depreciation) are costed out. Clean-up and set-up are also computed in, but
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABILITY TESTING 197
the manufacturing cost is rarely compared with what it would have been if, for instance, only one or two products were made on a site. And the probability of rejected batches is rarely accounted for in the product cost? Here the aspects of product overcrowding come in.
Correcting a 483 is not easy. Let us take an example: Suppose there is a substantial batch-to-batch difference in a wet-granulated tablet product. The granulation step is not time and temperature specific and the company might suspect this to be the cause of the poor reproducibility and suggest standardization of the manner in which water is added. It should be noted that the binder solution may be
the root cause, but what is the prime effect of the conditions under which it is added to the powder mass? A seasoned pharmaceuticist might gauge a measurable endpoint to be a given particle size distribution and suggest that the paste temperature always be 50°C at the time of addition. A priori, it is not know whether this will correct the problem, so one could, for instance, make two batches, showing by manipulation that the change would make the desired tightening of specifications. Not until then would the step be incorporated, and the FDA would probably approve the tightening of the SOP. Notice the word tightening rather than change. That temperature of granulation paste is, indeed, important is exemplified in Figure 2.
Arriving at such conclusions and demonstrating them takes time, equipment time in particular. If a company is cited on only one product, then there should be ample time in 30 days to amve at a solution. But if the company is cited on ten products, then it cannot go through the investigation for all ten in a "reasonable" length of time (which is often 30 days). Furthermore, when the FDA returns, there may be more 483's issued.
What, then, caused the problem?
(1) The company did not spend the time on characterizing its product in the first place and
It would not be in an impossible situation if it were only a problem of a single product But if (a) the company is malung too many products for the physical facility or (b) the effort it has made to characterize the product and process are insufficient to rationally assess the effect of changes, then the situation becomes difficult.
(2)
The outcome is often that
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

198 CARSTENSEN
50
40
30
20
10
0
A 95Oc
0 1000 2000 3000 Diameter pm
2. Particle size distribution of lactose-starch granulations where the starch paste has been added at different tempeiatures. liquid added at 90°C, triangles at 95°C
Circles:
Some products can be put on hold. If for instance some of the 483's deal with products for which a company seeks an ANDA or an NDA the company could simply fix up the product as per suggestions in good time, and then reapply.
If, for instance, ten 483's were issued for products on the market a company could sort out the ones which could be fixed up with minor effort and correct them. Suppose there were now four products left where major experimentation would be necessary to meet the requests of the FDA, the company has a third option.
Tackle the products according to economic importance. If only two could be investigated in a "reasonable length of time" then the two which were most important financially would be investigated and a product recall instituted on the other two.
It is noted that the effect of the inspection has been to reduce the number of products made in the facility. Harsh medicine, but it may allow the company to
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABXLXTY TESTING 199
stay in business, and that would be the important point. The other two products could be revised in time, and reapplied for.
CONSCIENTIOUS PRODUCT DEFINITION, VALIDATION
Let it first be repeated, that products can not physically, be made in an identical, reproducible fashion at all for several reasons.
Raw materials always have high and low specification limits. Let us assume, for instance, that there are four raw materials in a product, and each of these is tested for 3 attributes. There is a high and a low limit on each of these, so if a company had to test something as simple as the "effect of the excipients" then, if it could, it would have to carry out experiments at high and low specification limit for each, whch calculates out to 4 x 3 x 2 = 24 large scale experiments.
But even if it were desired to do so, it would still not be possible to carry out these experiments, because one would have to ask the raw material supplier to supply different lots in large amounts, each at the extremes of the specification limits, a request he would and could not accommodate. So at the specification level of excipients alone, a company will have a problem.
But even that is not correct, because alternate suppliers are necessary and this
constitutes one more complicating factor. The answer to the problem is the next best thing: To keep on testing and assuring, in the long run, that the product is satisfactory as specified when it is made with raw materials in a given specification range.
PHYSICAL CHARACTERISTICS MONITORING
Most companies do not do extensive physical testing of their products. What would be desirable is given below.
When the product is in the development stage, all (in so far as that is possible) the significant physical parameters and all the process parameters that could be of importance should be pinpointed and monitored. A partial list of these would be, for a granulation, for instance:
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

200 CARSTENSEN
Physical parameters:
- Granule particle size distribution before and after milling - Active content of sieve fractions - Hardness/F'ressure profile - Athy-Heckel parameter - Disintegration - Dissolution (multiple point) - Friability. - Moisture - Yield
Process hameters: - Relative Humidity and Room Temperature - Blending time - Temperature of granulation liquid. - Workload (torque) profile (header- endpoint)
Drying temperature and time. (Air inlet and exit temperatures in fluid bed drying. Moisture test in upper, middle and lower tray in tray drying).
- Hammer speed and knife direction (in the experimental stage, defining the size distribution under different conditions).
It would be a wise policy to retain samples of granulations of production material for later comparison, should there be a future shift in process parameters. In such cases it is often a problem of a batch failing, and the question arises: what was the reason for the failure? If a company had reference material (retention samples of in- process material), then it might be able to rationally assess possible causes. It is better to be able to say, "The problem was that the granulation contained too many fines", than not to be able to say anything at all. It is even better to be able to say, "The high content of fines was due to inadvertent over-drylng".
One might argue that if a company was run in an ideal manner, it would not be very competitive. But if all companies would have to do the same, then this argument would not hold.
THE REAL VERSUS THE UTOPIAN STORAGE CONDITIONS
Having now discussed the Utopian versus the Real situation as regards the manner in which drug products are produced, one becomes aware that product monitoring post-NDA is a statistical problem to an extent.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

MANUFACTURING AND STABILITY TESTING 20 1
It is economically unfeasible to stability-test each batch made, so a skip-lot sampling program is used. Most often the rule is to test one batch per year or two percent of the number of batches produced in one year.
The stability data are usually input into a computerized stability program, and data are either pooled, or if that is not justifiable, they are assessed batch per batch. But, once in production, the "equivalence" of batches should be such, that pooling should be possible.
How then are the batches tested? The answer is: isothermally.
Isothermal stability testing is as far from reality as one might imagine, but at present there are no other methods used, although some have been suggestedl. There is no real-life situation where the temperature will always be 25°C (or 30°C) and the relative humidity will always be 4O%RH. The numbers generated in isothermal storage are idealized. They can, to some degree, mimic what would happen to a batch on the average in the market place, but it by no means mimics the real life storage, and the expected performance of individual batches. It is, at best, a compromise with reality, prescribed in such a fashion that testing can be camed out
and reported. In the minds of many, however, the statement that the product is stable at room temperature seems to be a guarantee that any unit in the market place will always lie within limits of whatever attribute is being discussed. This is not the case.
So, once again, we are Utopian.
SUMMARY
The aspects of "identity" and "equivalence" have been discussed, as have certain aspects of "reproducibility". The opinion is forwarded that testing as many parameters routinely, both in process and after the fact, is advisable to explain occasional product failures.
The aspects of the environment for good manufacturing (personnel, machinery, capacity) have been discussed.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

202 CARSTENSEN
REFERENCES
1. Rhodes, C.T. and Carstensen, J.T.: "Rational Policies for Stability Testing", 1993, Clinical Research and Drug Regulatory Affairs, 1993, Submitted.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B K
iel o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.




























![DYNAMICAL ALTERNATING GROUPS, STABILITY, PROPERTY …kerr/topfullgroups13.pdf · DYNAMICAL ALTERNATING GROUPS 3 all ‘2-Betti numbers is an invariant of measure equivalence [19]](https://img.dokumen.tips/doc/110x75/5d2f078388c993893a8c49e6/dynamical-alternating-groups-stability-property-kerr-dynamical-alternating.jpg)