Embed Size (px)
DESCRIPTION
Equine Laryngeal Disorders: Left Laryngeal Hemiplegia & Epiglottic Entrapment
Citation preview

LARYNGEAL DYSFUNCTION:
Dane Tatarniuk, DVMDec. 12, 2012
1. Left Laryngeal Hemiplegia
2. Epiglottic Entrapment

ANATOMY & FUNCTION

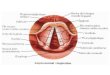
Equine Larynx
Anatomy Paired arytenoids Epiglottis Thyroid Cricoid

Equine Larynx
Intrinsic muscles Move laryngeal
cartilages in relation to each other
Cricoarytenoideus dorsalis – abduction of arytenoids & tensing of vocal folds
Thyroarytenoideus, arytenoideus transversus, cricoarytenoideus lateralis – adduction of arytenoids

Equine Larynx
Arytenoid Function Situated on either side of cricoid Composed of hyaline cartilage Cricoarytenoid joint – diarthrodial
Facilitates adduction & abduction movement 3 processes
Corniculate, cuneate & muscular process Arytenoids adduct (close) during swallowing reflex Arytenoids abduct (rima glottidis dilates) fully at high-
intensity exercise to maximize airflow Abduction of arytenoid counter-acts increasing negative
inspiratory pressure (which acts to adduct arytenoids) Decreased airflow hypoxemia hypercarbia metabolic
acidosis musculoskeletal fatigue poor performance

Equine Larynx
Epiglottis Anatomy & Function Triangular structure with apex
pointing rostral Attached to thyroid via
thyroepiglottic ligament Composed of elastic cartilage Normally situated above soft palate
Soft palate against epiglottic base Scallop appearance laterally Vascular pattern dorsally Flips caudally to cover rima glottis
during swallowing

CASE #1

Case #1- Signalment
7 years old Gelding Canadian Warmblood Discipline: Eventing

Case #1 - History
Tiring with exercise 6 month history
Noise Less of a concern
Evaluation by rDVM Standing endoscopy Laryngeal paralysis Referred to UMEC

Case #1 – Diagnostics
Normal vital parameters
Resting endoscopy, standing, un-sedated
Left laryngeal hemiplegia Grade 4
Recurrent laryngeal neuropathy
No other concurrent upper airway abnormalities noted

Left Laryngeal Paralysis
Neurogenic atrophy of intrinsic laryngeal musculature (94% of cases)
Loss of abductor and adductor arytenoid function Cricoarytenoideus dorsalis muscle
Progressive loss of function (not immediate) Other causes:
Perivascular damage from IV injection, guttural pouch mycosis, neck trauma, abscessation of head/neck, neck neoplasms, organophosphate toxicity, plant poisoning, hepatic encephalopathy, lead toxicity, CNS disease

Laryngeal Paralysis Grades
Grade 1 Arytenoid movements synchronous & symmetrical Full adduction attained
Grade 2 Arytenoid movements are asynchronous or
asymmetrical at times Full adduction attained
Grade 3 Arytenoid movements are asynchronous or
asymmetrical Full adduction can not be attained
Grade 4 Complete immobility of arytenoid cartilage

Case #1 - Therapy
Recommendation: Prosthetic Laryngoplasty
“Tie Back” Prosthesis between arytenoid and cricoid Create abduction Provide adequate airflow but not allow aspiration
+/- ventriculectomy via laryngotomy Eliminate noise, further stabilize airway Can be used as sole procedure in draft horses
+/- ventriculocordectomy via standing laser endoscopy 2 cm crescent wedge of tissue removed from leading
edge of vocal fold

Case #1 - Therapy
Pre-operative medication Potassium penicillin, 22,000iu/kg, IV Gentamicin, 6.6mg/kg, IV Phenylbutazone, 4.4mg/kg, IV Tetanus toxoid, IM
General anesthesia Small endotracheal tube Left lateral recumbancy Neck extended IV catheter low in left jugular vein or on right side 5L fluid bag under proximal neck
Help extend throatlatch upwards

Case #1 - Therapy
Surgery ~10cm cranial-caudal incision, cranial extent
starting at left ramus of mandible Ventral and parallel to lingual-facial vein Blunt dissect lingual-facial vein from
omohyoideus muscle Avoid pertinent nerves and vasculature
Dissect between sternocephalicus and cricothyroideus muscles
Follow plane of dissection under lingual-facial vein until expose larynx & associated laryngeal musculature

Case #1 - Therapy
Palpate caudal aspect of cricoid cartilage & muscular process of left arytenoid cartilage
Assistant retracts upwards Suture
#5 Ethibond (Polyester) Alternatives: Stainless steel wire,
nylon, polyethylene Pass suture through cricoid cartilage
(x 2) Walk needle off caudal aspect of
cricoid Stay axial to dorsal sagittal ridge ‘Notch’ of cricoid cartilage Auer &
Stick

Case #1 - Therapy
Intra-operative endoscopic exam Ensure suture does not penetrate laryngeal
mucosa Tunnel leading edges of suture
Under cricopharyngeus muscle Pass suture in caudal-medial to cranial-lateral
direction through muscular process (x2) Engage spine, not tip, of muscular process
Tie cranial suture strand to caudal strand (x2) Assess abduction of left arytenoid with
endoscope Curvature of corniculate cartilage comes into
contact with pharyngeal wall Close musculature & skin routinely
Stent bandage
Auer & Stick

Case #1 – Post Op Care
Post operative medication Potassium penicillin, 22,000iu/kg, IV, QID, 3
days Gentamicin, 6.6mg/kg, IV, SID, 3 days Phenylbutazone, 2.2mg/kg, PO, BID, 5 days Trimethoprim sulfa, 15mg/kg, PO, BID, 5 days
Fed on the ground Exercise
4 weeks of stall rest then 2 weeks of small paddock
Return to exercise at 6 to 8 weeks post-op

Case #1 – Recheck Endoscopy
24 hour recheck endoscopy Maintained abducted
position Estimate 60 to 70% of
rima glottidis area attained
4 week follow up Horse doing well

Prognosis
Success depends on use of horse and measurement of success
Between 50% to 70% of horses have improved performance following laryngoplasty surgery
Success better in horses not intended to race
Decreased noise production not a measure of improved airway function

Complications
Complications decrease prognosis Dysphagia Bilateral nasal discharge
Feed, water, saliva Aspiration pneumonia Chronic coughing Incisional infection Prosthesis failure Chondritis

CASE #2

Case #2 - Signalment
11 years old Gelding Quarter Horse Discipline: Mounted
shooting

Case #2 - History
History of intermittent coughing Severe coughing fit while at show Difficulty eating No performance issues Attended by rDVM

Case #2 – rDVM Diagnostics
Oral exam: normal Head radiographs: normal Endoscopy:
Epiglottic entrapment Severe thickening and necrotic ulceration of
aryepiglottic tissue Intermittent dorsal displacement of soft
palate Small ulcer present on the left rim of soft
palate

Case #2 – rDVM Endoscopy

Case #2 – rDVM Therapy
Procaine Penicillin 22,000iu/kg IM BID Flunixin Meglumine 1.1mg/kg PO SID
Recheck Endoscopy by rDVM: At 7 days - continued entrapment with
intermittent soft palate displacement; improvement of the ulcer
At 14 days - continued healing of ulcers, intermittent soft palate displacement, periodic ventral pharyngeal collapse

Case #2 – Referral Presentation After 14 days medical therapy,
Improvement in ulcer Epiglottic entrapment persists
Case referred for further management
Initial endoscopy: Confirm epiglottic entrapment with mild ulceration Ulceration less compared to previous exam
images Ventral aryepiglottic tissue normal with no
ulceration No adhesions present between epiglottis and
aryepiglottic tissue

Case #2 - Initial Endoscopy

Epiglottic Entrapment
Loose aryepiglottic folds & subepiglottic mucosa displace dorsally above the epiglottis
Exercise intolerance main complaint usually Less commonly coughing, nasal exudate
Prevalence 0.9% in Thoroughbreds Can be induced by
Epiglottic hypoplasia Aryepiglottic fold inflammation / swelling
Chronic cases Thickened, fibrous tissue 45% have ulceration present

Case #2 - Assessment
Recommendation: Surgery Entrapment unlikely to resolve without
intervention Techniques:
Standing vs. general anesthesia Laser axial transection Sharp axial transection
Determined to post-pone surgical management Additional 7 days
Allow ulcer to heal further prior to surgery Decrease risk of adhesion, granuloma
formation

Case #2 – Interim
Medical therapy Procaine Penicillin, 22,000iu/kg, IM, BID, 7
days Flunixin Meglumine, 0.55mg/kg, PO, BID, 3
days Throat Spray, 10cc, PO, SID, 7 days
Glycerin 9cc Dimethyl sulfoxide 1cc

Surgical Techniques
Sharp axial division of aryepiglottic tissue Curved bistoury knife passed nasally and
applied under endoscopic guidance Scalpel transection through laryngotomy or
pharyngotomy Axial division allows membrane to retract
and heal in normal sub-epiglottic position Tissue sparing, minimize scar tissue
If thickened or ulcerated Can consider taking out triangular wedge
segments of aryepiglottic tissue instead of axial division

Surgical Techniques
Laser axial division of aryepiglottic tissue Contact vs. non-contact Tip of laser applied to caudal aspect of
tissue (on midline) and moved rostrally 10 to 12 watts Continue dissection until elastic property of
aryepiglottic tissue causes entrapping membrane to retract below epiglottis
Care to not cause collateral damage to epiglottis, soft palate or pharynx

Case #2 – Surgery
Surgical management 7 days following initial UMEC exam 21 days following initial rDVM exam
Pre-operative medication Detomidine, 0.02mg/kg, IV, given to effect Intranasal lidocaine, 100cc Procaine Penicillin, 22,000iu/kg, IM Gentamicin, 6mg/kg, IV Phenylbutazone, 4.4mg/kg, IV

Case #2 - Surgery
Standing axial excision of aryepiglottic tissue using diode contact laser

Case #2 - Surgery
Standing axial excision of aryepiglottic tissue using diode contact laser

Case #2 - Surgery
Rostral edge of epiglottis appears hypoplastic Blunted prominence
Residual thickening of aryepiglottic tissue present on left edge of epiglottis Contract with time Require transection at
future date

Case #2 – Post Op Care
Phenylbutazone, 2.2mg/kg, PO, BID, 5 days Procaine Penicillin, 22,000iu/kg, IM, BID, 3
days Throat Spray, 10cc, PO, SID, 7 days
Glycerin 7.7cc Dimethyl sulfoxide 0.8cc Dexamethasone 1.5cc
Recheck endoscopy 24 hours later Confirmed epiglottis free
Discharged 24 hours after surgery

Case #2 – Recheck
Recheck endoscopy 6 days post-surgery Swelling decreased
considerably Some residual
inflammation present

Prognosis
Reported re-entrapment rate is 5 to 15% with curved bistoury
Reported re-entrapment rate is 4% with laser axial division
Between 10 to 15% of cases develop DDSP following un-entrapment
Complications reduce prognosis: Thermal trauma to epiglottis, soft palate Lacerations to epiglottis, soft palate Cicatrix

REVIEW

Review: Laser
Types: Neo-dymium : yttrium aluminum garnet (Nd:YAG) Gallium aluminum arsinate diode
Quartz or silica fiber-optics to conduct laser energy Human safety - wear protective eyewear
Specific to wavelength of laser – avoid ocular injury Smoke plume
Xylene, toluene – can be toxic If considerable amount produced consider smoke evacuator
Laser energy converted to thermal energy when contacting tissue Incise, coagulate, vaporize Wavelength used influences amount absorbed, scattered,
reflected, transmitted

Review: Laser
Precision incision Smaller fiber (400–600μm) Small contact area, high power density Direct contact with tissue 10 to 15 watts power
Non-specific tissue ablation Larger fiber (800–1000μm) Less specific, do not require direct contact Up to 50 watts power Can coagulate tissue 5mm deep Capable with Nd:YAG, not capable with diode

Review: Recent Literature
Dart, 2009. “Effect of Prosthesis Number and Position on Rima Glottidis Area in Equine Laryngeal Specimens.” Placed dorsal suture and lateral suture
dorsally in the cricoid & through the rostral and proximal muscular process
1.5 cm lateral to the 1st suture & more caudal and distal in the muscular process
When tied independently, no difference in rima glottis area 8.51cm2 & 8.46cm2
When both sutures were tied together, mean area was greater than when either suture was tied alone 9.31cm2

Review: Recent Literature
Rakesh, 2008. “Implications of different degrees of arytenoid cartilage abduction on equine upper airway characteristics”. Used computational fluid dynamics modeling to
measure the effects of different degrees of abduction Tested abduction at 100%, 88% & 75% cross
sectional area of rima glottis 88% cross sectional area optimal
less reduction in airflow less collapsing pressure less stress on the repair

Review: Recent Literature
Aitken, 2011. “Epiglottic abnormalities in mature non-racehorses: 23 cases.” 8+ years, non race-horses Primary complaint
70% chronic cough 13% nasal discharge Racehorses – exercise intolerance
57% epiglottic entrapment All chronic: thick, ulcerated, and blunted epiglottis
74% resolution of symptoms with appropriate management 24% prolonged medical management (therapy >2 weeks) due to
post-surgical epiglottic inflammation 9% developed DDSP post-epiglottic surgery

Review: Recent Literature
Lacourt, 2011. “Treatment of Epiglottic Entrapment by Trans-nasal Axial Division in Standing Sedated Horses Using a Shielded Hook Bistoury.” Reviewed 33 cases using conventional bistoury technique
2 – laceration of soft palate 2 – laceration of epiglottis
Shield hook in 8 standardbreds Minimize damage to soft palate, epiglottis
Mean surgical time = 83 seconds 6 resolution with one incision 2 resolution with two incisions
Inexpensive Faster Authors opinion: technically easier

References
Aitken, 2011. “Epiglottic abnormalities in mature non-racehorses: 23 cases.” JAVMA 238: 12, 1634 – 1638.
Dart, 2009. “Effect of Prosthesis Number and Position on Rima Glottidis Area in Equine Laryngeal Specimens.” Vet Surg 38: 452 – 456.
Lacourt, 2011. “Treatment of Epiglottic Entrapment by Trans-nasal Axial Division in Standing Sedated Horses Using a Shielded Hook Bistoury.” Vet Surg 40: 299 – 304.
Fulton I: Larynx, in Auer JA, Stick JA (eds): Equine Surgery (ed 4). Philadelphia, PA, WB Saunders, 2006, pp 592 – 623.
Palmer SE. “The use of lasers for treatment of upper respiratory tract disorders” Vet Clin Equine (2003) 19: p245 – 263.
Rakesh, 2008. “Implications of different degrees of arytenoid cartilage abduction on equine upper airway characteristics”. EVJ 40 (7), 629 – 635.