-
How to Ultrasound the Equine Larynx
Katherine S. Garrett, DVM
Authors address: Rood and Riddle Equine Hospital, PO Box 12070,
Lexington, Kentucky 40580-2070; e-mail: [email protected].
2010 AAEP.
1. Introduction
Abnormalities of the upper airway (UA) are fre-quently
implicated as a cause of poor performance,exercise intolerance, or
abnormal respiratory noise inthe equine.13 Common abnormalities
involving thefunction of the arytenoid cartilages include
recurrentlaryngeal neuropathy, arytenoid chondritis, and laryn-geal
dysplasia. Dorsal displacement of the soft palate(DDSP) and
pharyngeal collapse affect the pharyngealregion. Congenital
abnormalities and dynamic lar-ynx collapse associated with poll
flexion can affectmultiple regions of the larynx and pharynx.
Resting UA endoscopy is widely available and isoften the first
diagnostic tool used in evaluation ofUA abnormalities. In many
cases, resting endos-copy is sufficient for diagnosis. However,
dynamicevaluation, either using a treadmill or a portableover
ground videoendoscopy system, is considered toprovide a more
accurate diagnosis than resting en-doscopy.46 Unfortunately,
dynamic UA examina-tion requires specialized equipment that may not
beavailable locally, may be cost prohibitive for someclients, and
may not be appropriate for some horses.Additionally, some UA
abnormalities cannot be fullyassessed using UA endoscopy.
Laryngeal ultrasonography, first described byChalmers et al. in
2006,7 is a relatively new additionto the diagnostic repertoire for
UA disorders. Ithas proven to be useful clinically in the diagnosis
of
many conditions of the UA, especially disorders re-sulting in
abnormal arytenoid movement includingrecurrent laryngeal
neuropathy, arytenoid chondri-tis, and laryngeal dysplasia, a
congenital malforma-tion of the larynx.710 Laryngeal
ultrasonographycan be especially helpful in cases where a
dynamicexamination cannot be performed.
An appreciation of the pathologic changes that occurin diseases
of the UA is helpful in understanding theultrasonographic changes
that accompany each dis-ease. Recurrent laryngeal neuropathy
results in de-nervation atrophy and subsequent loss of function
ofthe intrinsic laryngeal muscles innervated by the re-current
laryngeal nerve, including the cricoarytenoi-deus dorsalis (CADM),
cricoarytenoideus lateralis(CALM), transversus arytenoideus,
vocalis, and ven-tricularis muscles.11,12 Clinically, this
condition man-ifests itself as decreased or absent arytenoid
abductionand affects the left arytenoid more commonly than theright
arytenoid.4 Denervated muscle has a charac-teristic
ultrasonographic appearance; the muscle be-comes hyperechoic to
normal muscle and has a morehomogeneous appearance with a loss of
the normalstriated pattern.1315 These changes have been ob-served
ultrasonographically in the CALM and CADMof horses with treadmill
UA endoscopy-confirmed re-current laryngeal neuropathy.8,10
The precise etiology of arytenoid chondritis re-mains unclear
but likely results from local trauma
AAEP PROCEEDINGS Vol. 56 2010 249
IMAGING
NOTES
-
to and subsequent bacterial infection of the aryte-noid
cartilage.16 Some horses may have granulo-mas only on the axial
surface of the arytenoidcartilage, whereas the pathology may
progress toinvolve the entire arytenoid cartilage in otherhorses.
In more severe cases, the arytenoid be-comes thickened with
irregular margins and hasimpaired movement, which may be
appreciated en-doscopically.17 The presence of arytenoid
cartilagethickening, irregular margination, and
abnormalechogenicity typical of this disease has been imagedusing
ultrasonography.7
A congenital defect known as laryngeal dysplasia(also known as
fourth branchial arch defect or4-BAD) may cause abnormal arytenoid
movement ofeither the left or right arytenoid cartilage.18,19
Horses with this condition may also have constantor intermittent
rostral displacement of the palato-pharyngeal arch during UA
endoscopy or dorsal dis-placement of the soft palate.9,20 Horses
withlaryngeal dysplasia have characteristic anatomicabnormalities,
including lack of a cricothyroid artic-ulation and extension of the
thyroid lamina dorsalto the muscular process of the arytenoid
cartilage,and they may have pharyngeal muscle abnormali-ties as
well.1921 The ultrasonographic appearanceof these anatomic features
has been described.9
The pathophysiology of DDSP has not been fullyelucidated but may
involve an inability to maintaina rostral position of the larynx.22
Interestingly, achange in the position of the basihyoid bone after
sur-gical treatment (laryngeal tie-forward) is associatedwith an
increased likelihood of racing post-operative-ly.23 This finding
prompted initial investigation into
an ultrasonographic marker for DDSP, which hasshown that horses
with DDSP had a smaller averagedistance between the skin and
basihyoid bone thanhorses without DDSP.24 However, the difference
inthis measurement between horses with and withoutDDSP was less
than 2 mm, limiting its use in clinicalsituations.
The etiology of other UA disorders, including pha-ryngeal
collapse, billowing of the soft palate, epiglot-tic retroversion,
laryngeal collapse associated withflexed head position, and axial
deviation of thearyepiglottic folds, remains unclear.16,25 No
char-acteristic ultrasonographic findings of these disor-ders have
been described.
The purpose of this paper is to provide the prac-titioner with
instruction on how to perform a laryn-geal ultrasonographic
examination and incorporatethis tool it into his or her evaluation
of the UA.
2. Materials and Methods
Horses are prepared for the examination by sedationwith xylazine
hydrochloride (0.4 mg/kg, IV). Mosthorses do not need to have the
laryngeal regionclipped before examination, but if the coat is
coarseor thick, clipping will improve image quality. Thehead is
held in an extended position by a handleror stand to move the
laryngeal region caudally inrelation to the mandible. A linear or
curvilineartransducer can be used for the examination. A fre-quency
of 810 mHz typically provides adequatepenetration while preserving
resolution.
Examination of the lateral portion of the larynxcan be performed
in the dorsal and transverseplanes. In the dorsal plane, an initial
image of the
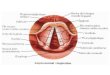
Fig. 1. Dorsal plane ultrasound image of the lateral aspect of a
normal larynx (A). Transducer position is shown in B. Note
theposition of the cricoarytenoideus lateralis muscle (small
arrowheads) between the thyroid cartilage (small arrows) and the
arytenoidcartilage (large arrowhead). The cricoid cartilage (large
arrow) is caudal to the thyroid cartilage. Rostral is to the left
of the image andcaudal is to the right of the image.
250 2010 Vol. 56 AAEP PROCEEDINGS
IMAGING
-
superficially positioned thyroid cartilage, the cricoidcartilage
caudal to the thyroid cartilage, and thearytenoid cartilage deep to
the thyroid cartilage canbe obtained (Fig. 1). The CALM is imaged
betweenthe thyroid and arytenoid cartilages, and the
crico-thyroideus muscle is imaged between the thyroidand cricoid
cartilages. By moving the transducerslightly dorsally, one can
image the cricothyroid ar-ticulation, which is formed by the caudal
cornu ofthe thyroid cartilage and the articular process ofthe
cricoid cartilage (Fig. 2). Mineralization of thecaudal cornu of
the thyroid cartilage is common, butthis does not seem to be
clinically significant. Fromthe cricothyroid articulation, the
transducer is moveddorsally and angled slightly ventrally. In this
loca-tion, one can image the cricoarytenoid articulationbetween the
muscular process of the arytenoid car-tilage and the dorsal cricoid
cartilage. The lateralportion of the CADM may be evaluated as
well(Fig. 3).
The lateral aspect of the larynx is also evaluatedin the
transverse plane. The initial image obtainedis the superficially
positioned thyroid lamina withthe arytenoid cartilage deep to the
thyroid laminaand the CALM and vocalis muscle between the thy-roid
and cricoid cartilages (Fig. 4). In some horses,the vocalis muscle
is imaged distinctly from theCALM, but in others, the distinction
between thetwo muscles cannot be defined. If the transducer ismoved
caudally, the caudal cornu of the thyroid
cartilage, the cricothyroid articulation, and the cri-coid
cartilage are imaged.
The ventral portion of the larynx can be examinedin transverse
and median planes. In a transverseplane, the tracheal rings can
serve as a referencepoint. From the tracheal rings, as the
transducer ismoved rostrally, the ventral aspect of the
cricoidcartilage is identified (Fig. 5), followed by the thy-roid
cartilage. Deep to the thyroid cartilage, thevocal folds may be
imaged, and their movements canbe observed (Fig. 6). The
mineralized rostral as-pect of the ventral thyroid cartilage is
encounterednext. Between the thyroid cartilage and the basi-hyoid
bone, the thyrohyoid bones may be imagedlaterally. The basihyoid
bone appears as a horizon-tal line (Fig. 7), and if the transducer
is angledrostrally from this position, the ceratohyoid bonesare
imaged. By moving the transducer rostrally,the lingual process of
the basihyoid bone is imaged.The depth of the basihyoid bone can be
measured atthe junction between the lingual process and body ofthe
basihyoid bone. In the median plane, the rela-tionship between the
lingual process and the miner-alized rostral aspect of the thyroid
cartilage can beevaluated. The ventral aspect of the cricoid
andtracheal rings can also be imaged.
Fig. 2. Dorsal plane ultrasound image of the lateral aspect of
anormal larynx. This image is slightly dorsal and caudal to
Figure1. The cricothyroid articulation (small arrowhead) is formed
bythe caudal cornu of the thyroid cartilage (small arrows) and
thearticular process of the cricoid cartilage (large arrow). The
mus-cular process of the arytenoid cartilage is also imaged
(largearrowhead). Rostral is to the left of the image and caudal is
to theright of the image.
Fig. 3. Dorsal plane ultrasound image of the dorsolateral
aspectof a normal larynx. This image is dorsal to Figure 1. The
crico-arytenoid articulation (small arrowhead) is formed by the
mus-cular process of the arytenoid (large arrowhead) and
thedorsolateral cricoid cartilage (large arrow). The lateral
portion ofthe cricoarytenoideus dorsalis muscle is imaged (small
arrows).Rostral is to the left of the image and caudal is to the
right of theimage.
AAEP PROCEEDINGS Vol. 56 2010 251
IMAGING
-
In general, the overall symmetry of the laryngealcartilages and
associated musculature should beevaluated. The cartilages should be
smoothly mar-ginated with homogeneous echogenicity,
althoughmineralization of the thyroid and arytenoid carti-lages is
fairly common (Fig. 8), especially in olderhorses. The muscles
normally have heterogeneousechogenicity and have a striated pattern
in a longi-tudinal view.
Comparison of the relative echogenicity of the leftand right
CALM and CADM enables the practitio-ner to assess whether one
structure has the hyper-echogenicity characteristic of denervation
atrophy
of recurrent laryngeal neuropathy. Ultrasoundmachine settings
should be kept constant betweenleft and right sides of the larynx,
and images shouldbe evaluated in dorsal and transverse planes.
Sideby side comparison is often useful (Fig. 9). Itshould be borne
in mind that many factors will con-tribute to the ultrasonographic
appearance of themuscles, and therefore, comparison within a horse
ispreferable to comparison between horses.
The contour of the arytenoid cartilages should beassessed
critically. The arytenoid cartilages shouldhave a trumpet bell
shape with smooth margins.Horses with chondritis have irregularity
of the axialand abaxial margins with thickening of the cartilageand
abnormal echogenicity within the arytenoid car-tilage (Fig. 10).
Horses may have only a granulomaor chondroma on the axial surface
of the arytenoidcartilage without diffuse arytenoid chondritis.
Ul-trasonographically, this manifests as focal irregular-ity of the
axial margin, smooth abaxial margin, andnormal arytenoid cartilage
width.
The anatomic abnormalities characteristic oflaryngeal dysplasia
can also be observed. The ex-tension of the thyroid cartilage
dorsal to the muscu-lar process of the arytenoid cartilage can best
beimaged in the transverse plane (Fig. 11), whereasthe lack of a
cricothyroid articulation is best imagedin the dorsal plane (Fig.
12). In these horses, therelationship between the thyroid
cartilage, cricoary-tenoideus lateralis muscle, and arytenoid
cartilageis abnormal; the CALM is often positioned caudal tothe
thyroid cartilage in the gap between the thyroidcartilage and
cricoid cartilage.
Fig. 5. Transverse plane ultrasound image of the ventral
aspectof the cricoid cartilage (arrows) of a normal larynx. Left is
to theleft of the image and right is to the right of the image.
Fig. 4. Transverse plane ultrasound image of the lateral aspect
of a normal larynx (A). Transducer position is shown in B. Note
theposition of the cricoarytenoideus lateralis muscle (CAL) between
the thyroid cartilage (arrows) and the arytenoid cartilage
(arrow-heads). The arytenoid cartilage has a trumpet bell shape and
the cricoarytenoideus lateralis muscle has a striated appearance
withheterogeneous echogenicity. Dorsal is to the left of the image
and ventral is to the right of the image.
252 2010 Vol. 56 AAEP PROCEEDINGS
IMAGING
-
Medical records of Rood and Riddle Equine Hos-pital were
examined to identify horses that had un-dergone UA endoscopy
(resting and/or dynamic) aswell as laryngeal ultrasonography.
Results of UAendoscopy and laryngeal ultrasonography as well asthe
final diagnosis were recorded.
3. Results
Between 2008 and 2009, 330 horses that presentedto Rood and
Riddle Equine Hospital for evaluationof the UA underwent laryngeal
ultrasonography.A variety of breeds and uses were represented
inthis group. All horses underwent resting UA en-doscopy, and a
subset (148 horses) underwent tread-mill UA endoscopy as well.
One hundred thirty-one horses were diagnosedwith left recurrent
laryngeal neuropathy based onresults of resting and/or treadmill UA
endoscopy or
previous prosthetic laryngoplasty. One hundredtwenty of these
horses (92%) had hyperechogenicityof the left CALM and/or CADM
characteristic ofmuscle denervation. The remaining 11 horses
hadnormal echogenicity of the left CALM and CADM; 4of these 11
horses were also diagnosed with DDSPduring dynamic UA examination.
In the opinion ofthe attending clinician, DDSP was felt to be
theprimary cause of poor performance. Three of theeleven horses did
not undergo dynamic examination,and diagnosis was made during
resting UA endos-copy only.
Fig. 6. Transverse plane ultrasound image (A) of the ventral
aspect of the thyroid cartilage (arrows) of a normal larynx at the
levelof the vocal folds (arrowheads). Transducer position is shown
in B. The movement of the vocal folds can be observed during
respiration.Left is to the left of the image and right is to the
right of the image.
Fig. 7. Transverse plane ultrasound image of the basihyoid
bone(arrowheads) and the ceratohyoid bones (arrows) of a
normallarynx, obtained with the transducer positioned ventrally.
Left isto the left of the image and right is to the right of the
image.
Fig. 8. Transverse plane ultrasound image of the lateral
aspectof a normal larynx. Note the mineralization of the
muscularprocess of the arytenoid cartilage (arrow). Dorsal is to
the left ofthe image and ventral is to the right of the image.
AAEP PROCEEDINGS Vol. 56 2010 253
IMAGING
-
Conversely, there were 127 horses with hyper-echogenicity of the
CALM and/or CADM. One hun-dred twenty-two (96%) of these horses
werediagnosed with recurrent laryngeal neuropathy us-ing resting
and/or dynamic UA endoscopy. The re-maining five horses were
diagnosed with DDSP(three horses), axial deviation of the
aryepiglotticfolds (one horse), and axial deviation of the
vocalcords and aryepiglottic folds (one horse) during dy-namic UA
endoscopy.
Twenty-nine horses were diagnosed with arytenoidchondritis using
resting UA endoscopy. In three ofthese cases, arytenoid chondritis
was initially diag-nosed during UA endoscopy, but ultrasonographic
ex-amination showed a normal arytenoid contour. Oneof these three
horses was subsequently diagnosed withDDSP during a dynamic
treadmill examination. An-
other horse had hyperechogenicity of the CALM andwas diagnosed
with recurrent laryngeal neuropathyduring dynamic treadmill
examination. The thirdhorse did not undergo dynamic examination but
wasdiagnosed with DDSP based on results of resting UAendoscopy.
Fig. 9. Comparison of echogenicity of the cricoarytenoideus
late-ralis (arrows) and cricoarytenoideus dorsalis (arrowheads)
mus-culature. Horses with recurrent laryngeal neuropathy
haveincreased echogenicity and more homogeneous echogenicity of
thecricoarytenoideus lateralis and cricoarytenoideus dorsalis
mus-cles. Dorsal plane ultrasound images of the
cricoarytenoideuslateralis muscle of a horse with recurrent
laryngeal neuropathy(A) and a normal horse (B). Transverse plane
ultrasound imagesof the cricoarytenoideus dorsalis muscle of a
horse with recurrentlaryngeal neuropathy (C) and a normal horse
(D). Dorsal planeultrasound images of the cricoarytenoideus
lateralis muscle of ahorse with recurrent laryngeal neuropathy (E)
and a normalhorse (F). In the dorsal plane images, rostral is to
the left andcaudal is to the right and in the transverse plane
images, dorsalis to the left of the image and ventral is to the
right of the image.
Fig. 10. Transverse plane ultrasound image of the lateral
aspectof the larynx of a horse with arytenoid chondritis. The
arytenoidcartilage (arrows) is severely thickened with irregular
marginsand increased echogenicity in its interior. Dorsal is to the
left ofthe image and ventral is to the right of the image.
Fig. 11. Transverse plane ultrasound image of the lateral
aspectof the larynx of a horse with laryngeal dysplasia. The
thyroidlamina (arrowhead) extends dorsal to the muscular process of
thearytenoid cartilage (arrow). Dorsal is to the left of the image
andventral is to the right of the image.
254 2010 Vol. 56 AAEP PROCEEDINGS
IMAGING
-
Five horses were diagnosed with arytenoid gran-ulomas or
chondromas during resting UA endos-copy. In all five horses,
ultrasonography revealedthe mass on the axial surface of the
arytenoid car-tilage, and there was no evidence of arytenoid
chon-dritis affecting the entire cartilage.
Seven horses were diagnosed with laryngeal dys-plasia. In all
cases, ultrasonography showed a lackof a cricothyroid articulation
and extension of thethyroid cartilage dorsal to the muscular
process ofthe arytenoid cartilage unilaterally or
bilaterally.Abnormalities seen during UA endoscopy of thesehorses
included abnormal left or right arytenoid car-tilage movement,
rostral displacement of the pala-topharyngeal arch, and dorsal
displacement of thesoft palate.
Other more unusual anatomic malformationshave been diagnosed in
individual cases. One foalwith abnormal UA noise and exercise
intolerancehad cyst-like structures in the thyroid, arytenoid,and
cricoid cartilages as well as the first trachealring. An adult
horse with dorsal displacement ofthe soft palate was found to have
a basihyoid bonemalformation. A Paint horse heterozygous (N/H)for
hyperkalemic periodic paralysis (HYPP) had hy-pertrophy of the left
vocalis muscle.
Seventy-five horses were diagnosed with DDSP.These horses did
not have any characteristic ultra-sonographic abnormalities.
All horses with normal UA endoscopic exami-nations had normal
ultrasonographic examinations.Additionally, horses with pharyngeal
collapse, bil-lowing of the soft palate, epiglottic
retroversion,laryngeal collapse associated with flexed head po-
sition, abnormal arytenoid movement secondaryto
thrombophlebitis, and axial deviation of thearyepiglottic folds had
normal ultrasonographicexaminations.
4. Discussion
Ultrasonography of the laryngeal region can be per-formed easily
in an ambulatory or hospital setting,is a non-invasive and safe
procedure, and requiresno specialized equipment beyond an
ultrasound ma-chine with a linear or curvilinear transducer.
Clip-ping of the hair is not required, and light sedation
isgenerally sufficient to ensure patient compliance;therefore,
client and patient acceptance of the pro-cedure has been
excellent.
Currently, ultrasonography of the larynx is anexcellent tool for
investigation of the reason for ab-normal arytenoid movement,
because the cause maybe difficult to determine with resting UA
endoscopyalone. Evidence of hyperechogenicity of the leftCALM and
CADM would support a diagnosis ofleft recurrent laryngeal
neuropathy as a cause ofpoor performance or abnormal UA noise. In
casesof arytenoid chondritis, ultrasonography permitsimaging of
nearly the entire arytenoid cartilage.This has allowed us to assess
the extent of disease inthe cartilage, diagnose any associated
abscesses orperilaryngeal inflammation, and monitor responseto
treatment. In some of the cases in this report,the ultrasonographic
findings did not support adiagnosis of arytenoid chondritis,
leading to addi-tional investigation and revision of the
diagnosis.Congenital abnormalities involving the
laryngealcartilages can be imaged directly instead of beinginferred
from UA endoscopic abnormalities.
Although previous work24 has shown a small(2 mm) difference in
the depth of the basihyoidbone between horses with and without
DDSP, nosignificant difference was identified between thesegroups
in our population. No abnormal ultraso-nographic findings were
observed for a group ofconditions of the UA (pharyngeal collapse,
billowingof the soft palate, epiglottic retroversion, and
axialdeviation of the aryepiglottic folds), but furtherwork may
reveal characteristic findings in thesediseases.
In our practice, ultrasonography of the larynx hasbeen
incorporated as a routine procedure for inves-tigation of UA
disorders, because it contributes to amore thorough evaluation of
the UA. Endoscopy isan excellent tool for assessment of laryngeal
func-tion and abnormalities visible at the luminal aspectof the
larynx, but ultrasonography allows more com-plete examination of
the laryngeal cartilages andassociated musculature, structures that
were pre-viously difficult to evaluate. Additionally,
ultra-sonography can be useful in evaluation of poorperformance or
abnormal UA noise in cases where adynamic UA examination is not
feasible (because ofavailability, financial or liability concerns,
concur-
Fig. 12. Dorsal plane ultrasound image of the lateral aspect
ofthe larynx of a horse with laryngeal dysplasia. The thyroid
car-tilage (arrow) and the cricoid cartilage (small arrowhead) do
notarticulate. The cricoarytenoideus lateralis muscle (large
arrow-heads) is positioned between the thryoid cartilage and
cricoidcartilage in the gap between the two cartilages. Rostral is
to theleft of the image and caudal is to the right of the
image.
AAEP PROCEEDINGS Vol. 56 2010 255
IMAGING
-
rent lameness, or other factors). Hopefully, futurework will
expand the uses of laryngeal ultrasonog-raphy for a variety of UA
conditions.
References1. Martin BB, Davidson EJ, Durando MM, et al. Clinical
ex-
ercise testing: overview of causes of poor performance.
In:Hinchcliff KW, Kaneps AJ, Geor RJ, et al., eds. Equine
sportsmedicine and surgery. Edinburgh: Saunders, 2004;3241.
2. Martin BB Jr., Reef VB, Parente EJ, et al. Causes ofpoor
performance of horses during training, racing, or showing:348 cases
(19921996). J Am Vet Med Assoc 2000;216:554558.
3. Morris EA, Seeherman HJ. Clinical evaluation of poor
per-formance in the racehorse: the results of 275
evaluations.Equine Vet J 1991;23:169174.
4. Anonymous. Workshop summary consensus statements onequine
recurrent laryngeal neuropathy, in Proceedings.Havemeyer Foundation
Workshop on Equine Recurrent La-ryngeal Neuropathy 2003;9397.
5. Desmaizieres LM, Serraud N, Plainfosse B, et al.
Dynamicrespiratory endoscopy without treadmill in 68
performanceStandardbred, Thoroughbred and saddle horses under
natu-ral training conditions. Equine Vet J 2009;41:347352.
6. Rakestraw PC, Hackett RP, Ducharme NG, et al.
Arytenoidcartilage movement in resting and exercising horses.
VetSurg 1991;20:122127.
7. Chalmers HJ, Cheetham J, Yeager AE, et al. Ultrasonographyof
the equine larynx. Vet Radiol Ultrasound 2006;47:476481.
8. Chalmers HJ, Cheetham J, Mohammed HO, et al. Ultra-sonography
as an aid in the diagnosis of recurrent laryngealneuropathy in
horses, in Proceedings. 16th American Col-lege of Veterinary
Surgeons Symposium 2006;34.
9. Garrett KS, Woodie JB, Embertson RM, et al. Diagnosisof
laryngeal dysplasia in five horses using magnetic resonanceimaging
and ultrasonography. Equine Vet J 2009;41:766771.
10. Garrett KS, Woodie JB, Embertson RM. Association oftreadmill
upper airway endoscopic evaluation of arytenoidmovement with
results of laryngeal ultrasonography andresting upper airway
endoscopic evaluation for diagnosis ofrecurrent laryngeal
neuropathy in Thoroughbred racehorses.Equine Vet J, submitted.
11. Duncan ID, Amundson J, Cuddon PA, et al.
Preferentialdenervation of the adductor muscles of the equine
larynx.I. Muscle pathology. Equine Vet J 1991;23:9498.
12. Duncan ID, Reifenrath P, Jackson KF, et al.
Preferentialdenervation of the adductor muscles of the equine
larynx.II. Nerve pathology. Equine Vet J 1991;23:99103.
13. Gunreben G, Bogdahn U. Real-time sonography of acuteand
chronic muscle denervation. Muscle Nerve 1991;14:654664.
14. Kullmer K, Sievers KW, Reimers CD, et al. Changes
ofsonographic, magnetic resonance tomographic, electromyo-graphic,
and histopathologic findings within a 2-month pe-riod of
examinations after experimental muscle denervation.Arch Orthop
Trauma Surg 1998;117:228234.
15. Walker FO. Neuromuscular ultrasound. Neurol Clin
2004;22:563590.
16. Holcombe SJ, Ducharme NG. Abnormalities of the upperairway.
In: Hinchcliff KW, Kaneps AJ, Geor RJ, et al.,eds. Equine sports
medicine and surgery. Endinburgh:Saunders, 2004;559598.
17. Haynes PF, Snider TG, McClure JR, et al. Chronic chondri-tis
of the equine arytenoid cartilage. J Am Vet Med
Assoc1980;177:11351142.
18. Kannegieter NJ, Goulden BE, Anderson LJ.
Right-sidedlaryngeal dysfunction in a horse. New Zeal Vet J
1986;34:6668.
19. Lane JG. Fourth branchial arch defects in
Thoroughbredhorses: a review of 60 cases, in Proceedings. 2nd
WorldEquine Airways Symposium 2001. Available at
http://www.ivis.org/proceedings/weas/2001/Lane.pdf. Accessed on
Janu-ary 21, 2010.
20. Goulden BE, Anderson LJ, Davies AS, et al. Rostral
dis-placement of the palatopharyngeal arch: a case report.Equine
Vet J 1976;8:9598.
21. Dixon PM, McGorum BC, Else RW. Cricopharyngeal-laryngeal
dysplasia in a horse with sudden clinical onsetidiopathic laryngeal
hemiparesis. New Zeal Vet J 1993;41:134 138.
22. Ducharme NG, Hackett RP, Woodie JB, et al.
Investigationsinto the role of the thyrohyoid muscles in the
pathogenesis ofdorsal displacement of the soft palate in horses.
Equine Vet J2003;35:258263.
23. Cheetham J, Pigott JH, Thorson LM, et al. Racing
perfor-mance following the laryngeal tie-forward procedure: a
case-controlled study. Equine Vet J 2008;40:501507.
24. Chalmers HJ, Yeager AE, Ducharme N.
Ultrasonographicassessment of laryngohyoid position as a predictor
of dorsaldisplacement of the soft palate in horses. Vet Radiol
Ultra-sound 2009;50:9196.
25. Strand E, Fjordbakk CT, Holcombe SJ, et al. Effect of
pollflexion and dynamic laryngeal collapse on tracheal pressurein
Norwegian Coldblooded Trotter racehorses. Equine Vet
J2009;41:5964.
256 2010 Vol. 56 AAEP PROCEEDINGS
IMAGING
Table of Contents