Embed Size (px)
Citation preview

333Chapter 36 Glanders
36
GlandersAnthony N.B. Kettle and Paul L. Nicoletti*
C H A P T E R
Glanders is one of the oldest recorded diseases of equids with zoonotic potential known since ancient times. Disease symp-toms were recorded by Hippocrates in 425 BC and was given the name “melis” by Aristotle in 350 BC.1,2 The common etiology of these diseases was first demonstrated by Viborg at the end of the eighteenth century.2 The etiologic agent, now known as Burkholderia mallei, was isolated in 1882 by Loeffler and Schütz from the liver and spleen of an infected horse.1,3 The mallein test for diagnosis of glanders was developed in 1890.4
By the second half of the nineteenth century, glanders was widespread in horses in North America, and a major epidemic of disease occurred in association with movement of horses during and after the Civil War.1,4,5 Burkholderia mallei was reportedly used as a biologic warfare agent in World Wars I and II and the Russian invasion of Afghanistan.6 Burkholderia mallei
is now regarded as a select agent (category B, U.S. Centers for Disease Control and Prevention) and all experimental work must be carried out in a Level 3 Biosafety facility.7,8 Disease caused by B. mallei must be reported to the World Organization for Animal Health (formerly the Office International des Epi-zooties [OIE]) in Paris.
Etiology
Burkholderia mallei (formerly Pseudomonas, Bacillus, Pfeifferella, Loefflerella, Malleomyces, Actinobacillus, Corynebacterium, and Mycobacterium) is a short, rod-shaped, gram-negative, aerobic, facultative intracellular, nonmotile, and non–spore-forming bac-terium. The organism survives outside the host for varying periods of time, depending on many factors. Virulence factors of B. mallei include capsular polysaccharide, lipopolysaccharide,
*The authors acknowledge and appreciate the original contributions of these authors, whose work has been incorporated into this chapter.
334 Section 3 Bacterial and Rickettsial Diseases
by subclinically infected horses. Poor sanitation, crowding, and immunosuppression from parasitism are considered risk factors. The incubation period varies from a few days to many months. The disease has been the target of eradication efforts for many decades because of its clinical effects in equids and its public health implications. The increasing number of outbreaks in recent years led to the classification of glanders as a reemerging disease.
Clinical Findings
Historically, glanders is described as either acute or chronic, but clinically it may be difficult to distinguish between the two forms. It is perhaps better to regard chronic glanders as a pro-gressive disease comprised of acute episodes occasionally inter-spersed with periods of latency. The host factors determining the course of the infection are unknown. Donkeys are most likely to die from acute disease within 7 to 10 days, whereas horses may either die rapidly or live for several years with chronic abscessation.
Acute glanders is characterized by bronchopneumonia and septicemia with a moderate to high fever, depression, and rapid weight loss. Frequently, highly infectious mucopurulent to hem-orrhagic nasal discharge forms crusts on the external nares. Submaxillary lymph nodes are frequently swollen, painless, and seldom rupture.
Chronic glanders is typically described as one of three forms: cutaneous (farcy), nasal, or pulmonary, although in practice there is much overlap between the three forms.
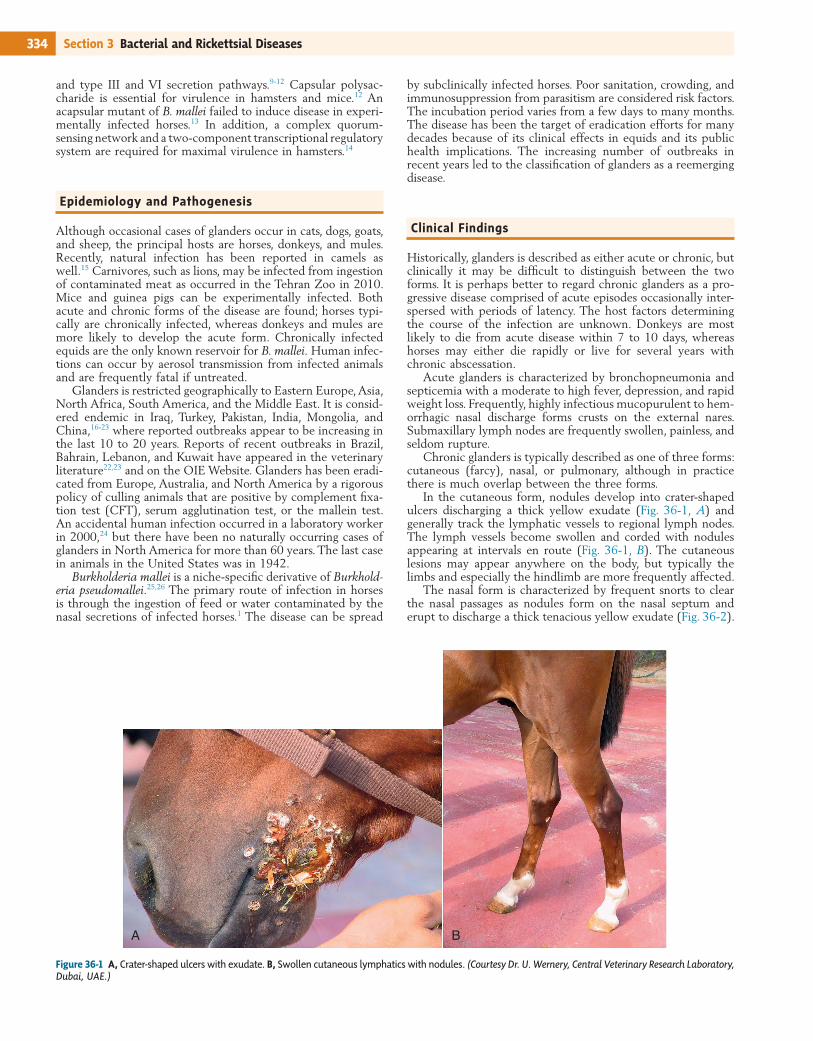
In the cutaneous form, nodules develop into crater-shaped ulcers discharging a thick yellow exudate (Fig. 36-1, A) and generally track the lymphatic vessels to regional lymph nodes. The lymph vessels become swollen and corded with nodules appearing at intervals en route (Fig. 36-1, B). The cutaneous lesions may appear anywhere on the body, but typically the limbs and especially the hindlimb are more frequently affected.
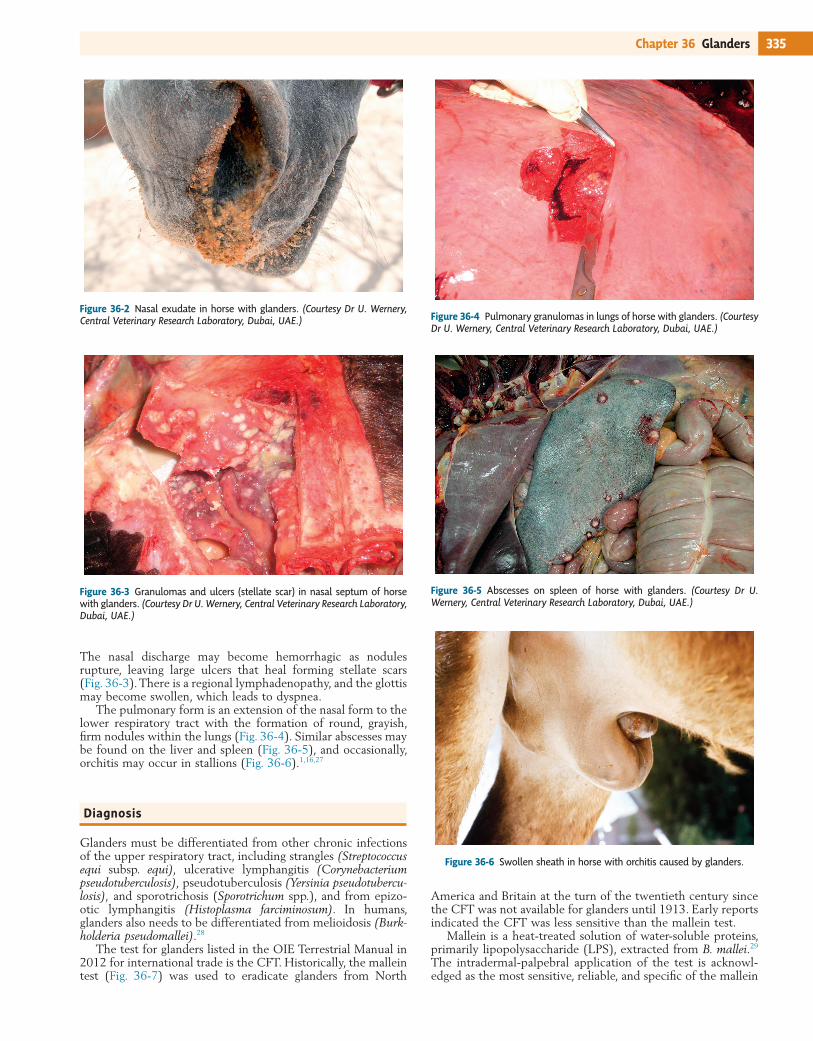
The nasal form is characterized by frequent snorts to clear the nasal passages as nodules form on the nasal septum and erupt to discharge a thick tenacious yellow exudate (Fig. 36-2).
Figure 36-1 A, Crater-shaped ulcers with exudate. B, Swollen cutaneous lymphatics with nodules. (Courtesy Dr. U. Wernery, Central Veterinary Research Laboratory, Dubai, UAE.)
A B
and type III and VI secretion pathways.9-12 Capsular polysac-charide is essential for virulence in hamsters and mice.12 An acapsular mutant of B. mallei failed to induce disease in experi-mentally infected horses.13 In addition, a complex quorum-sensing network and a two-component transcriptional regulatory system are required for maximal virulence in hamsters.14
Epidemiology and Pathogenesis
Although occasional cases of glanders occur in cats, dogs, goats, and sheep, the principal hosts are horses, donkeys, and mules. Recently, natural infection has been reported in camels as well.15 Carnivores, such as lions, may be infected from ingestion of contaminated meat as occurred in the Tehran Zoo in 2010. Mice and guinea pigs can be experimentally infected. Both acute and chronic forms of the disease are found; horses typi-cally are chronically infected, whereas donkeys and mules are more likely to develop the acute form. Chronically infected equids are the only known reservoir for B. mallei. Human infec-tions can occur by aerosol transmission from infected animals and are frequently fatal if untreated.
Glanders is restricted geographically to Eastern Europe, Asia, North Africa, South America, and the Middle East. It is consid-ered endemic in Iraq, Turkey, Pakistan, India, Mongolia, and China,16-23 where reported outbreaks appear to be increasing in the last 10 to 20 years. Reports of recent outbreaks in Brazil, Bahrain, Lebanon, and Kuwait have appeared in the veterinary literature22,23 and on the OIE Website. Glanders has been eradi-cated from Europe, Australia, and North America by a rigorous policy of culling animals that are positive by complement fixa-tion test (CFT), serum agglutination test, or the mallein test. An accidental human infection occurred in a laboratory worker in 2000,24 but there have been no naturally occurring cases of glanders in North America for more than 60 years. The last case in animals in the United States was in 1942.
Burkholderia mallei is a niche-specific derivative of Burkhold-eria pseudomallei.25,26 The primary route of infection in horses is through the ingestion of feed or water contaminated by the nasal secretions of infected horses.1 The disease can be spread
335Chapter 36 Glanders
Figure 36-2 Nasal exudate in horse with glanders. (Courtesy Dr U. Wernery, Central Veterinary Research Laboratory, Dubai, UAE.)
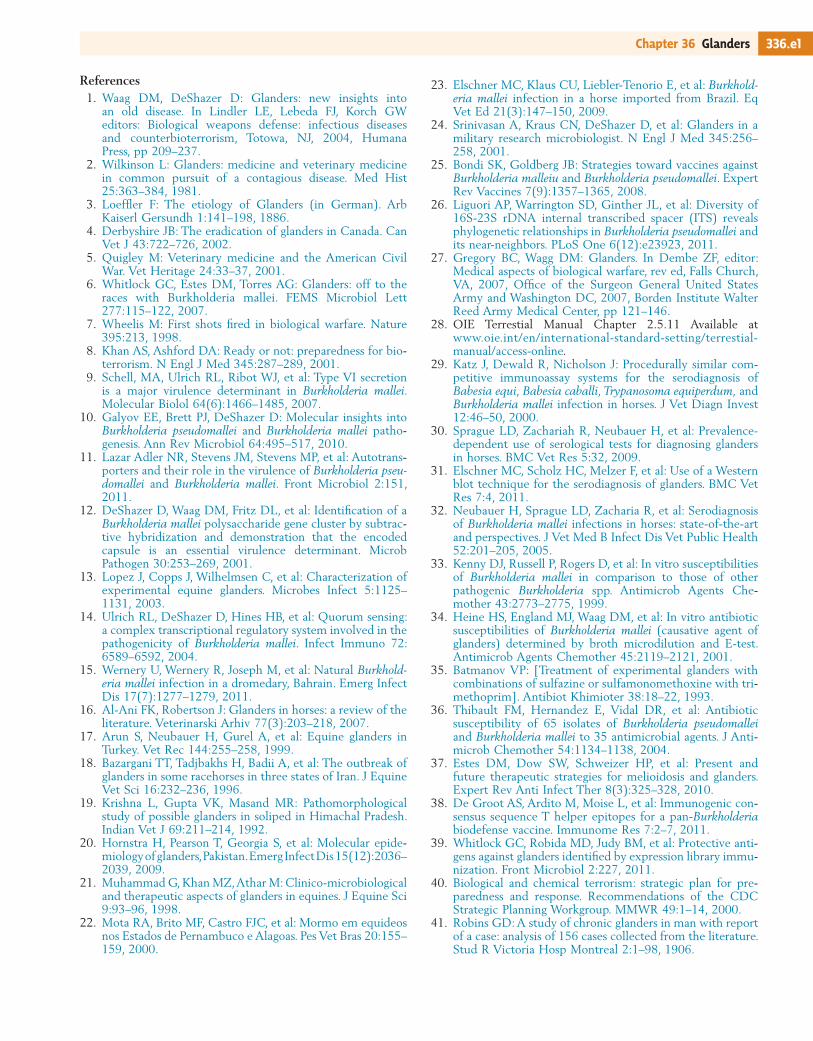
Figure 36-3 Granulomas and ulcers (stellate scar) in nasal septum of horse with glanders. (Courtesy Dr U. Wernery, Central Veterinary Research Laboratory, Dubai, UAE.)
The nasal discharge may become hemorrhagic as nodules rupture, leaving large ulcers that heal forming stellate scars (Fig. 36-3). There is a regional lymphadenopathy, and the glottis may become swollen, which leads to dyspnea.
The pulmonary form is an extension of the nasal form to the lower respiratory tract with the formation of round, grayish, firm nodules within the lungs (Fig. 36-4). Similar abscesses may be found on the liver and spleen (Fig. 36-5), and occasionally, orchitis may occur in stallions (Fig. 36-6).1,16,27
Diagnosis
Glanders must be differentiated from other chronic infections of the upper respiratory tract, including strangles (Streptococcus equi subsp. equi), ulcerative lymphangitis (Corynebacterium pseudotuberculosis), pseudotuberculosis (Yersinia pseudotubercu-losis), and sporotrichosis (Sporotrichum spp.), and from epizo-otic lymphangitis (Histoplasma farciminosum). In humans, glanders also needs to be differentiated from melioidosis (Burk-holderia pseudomallei).28
The test for glanders listed in the OIE Terrestrial Manual in 2012 for international trade is the CFT. Historically, the mallein test (Fig. 36-7) was used to eradicate glanders from North
Figure 36-4 Pulmonary granulomas in lungs of horse with glanders. (Courtesy Dr U. Wernery, Central Veterinary Research Laboratory, Dubai, UAE.)
Figure 36-5 Abscesses on spleen of horse with glanders. (Courtesy Dr U. Wernery, Central Veterinary Research Laboratory, Dubai, UAE.)
Figure 36-6 Swollen sheath in horse with orchitis caused by glanders.
America and Britain at the turn of the twentieth century since the CFT was not available for glanders until 1913. Early reports indicated the CFT was less sensitive than the mallein test.
Mallein is a heat-treated solution of water-soluble proteins, primarily lipopolysaccharide (LPS), extracted from B. mallei.29 The intradermal-palpebral application of the test is acknowl-edged as the most sensitive, reliable, and specific of the mallein

336 Section 3 Bacterial and Rickettsial Diseases
susceptibility patterns of 15 isolates of B. mallei to 35 antimi-crobial agents.36 The most effective drugs in vitro included imipenem, ceftazidime, ciprofloxacin, piperacillin, doxycycline, and aminoglycosides. There were no obvious differences in sus-ceptibility patterns among human, animal, and environmental isolates. Recently, experimental work has been done with granu-lysin and silver carbine compounds.37 The availability of several B. mallei genome sequences has greatly facilitated the develop-ment of new therapeutics; however, much work remains to be done to determine a suitable treatment regimen for horses. The difficulty with treatment in horses is in determining whether the infection has been eliminated.
Prevention
Glanders has been successfully eliminated from most countries through rigorous slaughter of animals with a positive mallein test. Quarantine of in-contact animals and pretesting of horses for movement are necessary components of disease control. A wide variety of national and international regulations exist, and glanders is a reportable disease for the OIE and many countries.
There is no vaccine for prevention of glanders in animals. Research efforts currently are focused on development of a vaccine for people in case the organism becomes an instrument of bioterrorism. A recent report highlights promising results for a vaccine using T-helper epitopes,38 and a series of protective antigens have been identified by genome analysis that may also be useful in the development of a vaccine.39
Public Health Considerations
Glanders is a rare but serious zoonotic disease. Most human cases are ultimately traced to direct contact with B. mallei through exposure to infected animals or laboratory exposure to the organism.24,27,41 The organism often enters via cutaneous exposure through the hands or arms. The incubation period is estimated to be a few days to several weeks but can be much longer. Local suppuration and regional lymphadenopathy with fever and lethargy are often the first symptoms.24 Dissemination of infection occurs 1 to 4 weeks after lymph node involvement becomes apparent. Systemic effects may include abscesses in the liver, spleen, lungs, pleura, subcutis, and muscles.24,27,40,41 Mortality in acutely affected people with untreated disease approaches 95% within 3 weeks. As previously mentioned, several antibiotics have reliable activity against B. mallei24,33-36 and are usually used in combination against B. mallei infections. In a recent report of glanders in a laboratory worker, treatment with imipenem and doxycycline for 2 weeks, followed by azithromycin and doxycycline for 6 months, was successful (in vitro susceptibility testing did not support the use of azithro-mycin).24,27 Glanders in human patients may be difficult to diagnose because of a lack of awareness and rarity of human disease.27
The complete reference list is available online at www. expertconsult.com.
tests for glanders. The immunologic basis for the test is primar-ily a stimulation of memory T cells. Anergy may result in a false-negative reaction. False-positive reactions may also occur. In negative horses, mallein may induce antibodies that are detectable for up to 19 weeks after injection.30
The CFT is currently the test used for international trade, but a number of nonspecific false-positive results occur.30 These false positives are thought to derive at least in part from the use of crude cell-antigen preparations and also from cross-reactions with other bacteria.
Recently, a Western immunoblot technique has been pro-posed (but has yet to be validated) for resolving the false posi-tives found in the CFT for use in areas with low glanders prevalence.31 Several other serologic tests and diagnostic tech-niques are now available for glanders diagnosis, including polymerase chain reaction (PCR), agglutination, indirect hem-agglutination, enzyme-linked immunosorbent assay (ELISA), counter immunoelectrophoresis, Rose-Bengal staining, and competitive ELISA (cELISA).32 Culture and immunohisto-chemical staining for bacterial antigen may be used. Although rarely used, guinea pigs are highly susceptible, and an acute purulent orchitis occurs in a few days after inoculation of mate-rial (Strauss test). A lack of sensitivity of this procedure and culture has been reported.17 Recent advances in our under-standing of B. mallei and the increasing availability of molecular diagnostic tools may soon result in a new generation of more sensitive and specific diagnostic tests for glanders in horses.32
Therapy
Euthanasia and slaughter of equids with glanders are strongly recommended and may be mandatory in some countries. Although there are relatively few studies of antimicrobial sus-ceptibility patterns of B. mallei, it appears that this organism is resistant to many antimicrobial drugs, including β-lactam antibiotics.33-36 A recent study examined the antimicrobial
Figure 36-7 Performing the intradermal mallein test. (Courtesy Dr U. Wernery, Central Veterinary Research Laboratory, Dubai, UAE.)
336.e1Chapter 36 Glanders
References1. Waag DM, DeShazer D: Glanders: new insights into
an old disease. In Lindler LE, Lebeda FJ, Korch GW editors: Biological weapons defense: infectious diseases and counterbioterrorism, Totowa, NJ, 2004, Humana Press, pp 209–237.
2. Wilkinson L: Glanders: medicine and veterinary medicine in common pursuit of a contagious disease. Med Hist 25:363–384, 1981.
3. Loeffler F: The etiology of Glanders (in German). Arb Kaiserl Gersundh 1:141–198, 1886.
4. Derbyshire JB: The eradication of glanders in Canada. Can Vet J 43:722–726, 2002.
5. Quigley M: Veterinary medicine and the American Civil War. Vet Heritage 24:33–37, 2001.
6. Whitlock GC, Estes DM, Torres AG: Glanders: off to the races with Burkholderia mallei. FEMS Microbiol Lett 277:115–122, 2007.
7. Wheelis M: First shots fired in biological warfare. Nature 395:213, 1998.
8. Khan AS, Ashford DA: Ready or not: preparedness for bio-terrorism. N Engl J Med 345:287–289, 2001.
9. Schell, MA, Ulrich RL, Ribot WJ, et al: Type VI secretion is a major virulence determinant in Burkholderia mallei. Molecular Biolol 64(6):1466–1485, 2007.
10. Galyov EE, Brett PJ, DeShazer D: Molecular insights into Burkholderia pseudomallei and Burkholderia mallei patho-genesis. Ann Rev Microbiol 64:495–517, 2010.
11. Lazar Adler NR, Stevens JM, Stevens MP, et al: Autotrans-porters and their role in the virulence of Burkholderia pseu-domallei and Burkholderia mallei. Front Microbiol 2:151, 2011.
12. DeShazer D, Waag DM, Fritz DL, et al: Identification of a Burkholderia mallei polysaccharide gene cluster by subtrac-tive hybridization and demonstration that the encoded capsule is an essential virulence determinant. Microb Pathogen 30:253–269, 2001.
13. Lopez J, Copps J, Wilhelmsen C, et al: Characterization of experimental equine glanders. Microbes Infect 5:1125–1131, 2003.
14. Ulrich RL, DeShazer D, Hines HB, et al: Quorum sensing: a complex transcriptional regulatory system involved in the pathogenicity of Burkholderia mallei. Infect Immuno 72:6589–6592, 2004.
15. Wernery U, Wernery R, Joseph M, et al: Natural Burkhold-eria mallei infection in a dromedary, Bahrain. Emerg Infect Dis 17(7):1277–1279, 2011.
16. Al-Ani FK, Robertson J: Glanders in horses: a review of the literature. Veterinarski Arhiv 77(3):203–218, 2007.
17. Arun S, Neubauer H, Gurel A, et al: Equine glanders in Turkey. Vet Rec 144:255–258, 1999.
18. Bazargani TT, Tadjbakhs H, Badii A, et al: The outbreak of glanders in some racehorses in three states of Iran. J Equine Vet Sci 16:232–236, 1996.
19. Krishna L, Gupta VK, Masand MR: Pathomorphological study of possible glanders in soliped in Himachal Pradesh. Indian Vet J 69:211–214, 1992.
20. Hornstra H, Pearson T, Georgia S, et al: Molecular epide-miology of glanders, Pakistan. Emerg Infect Dis 15(12):2036–2039, 2009.
21. Muhammad G, Khan MZ, Athar M: Clinico-microbiological and therapeutic aspects of glanders in equines. J Equine Sci 9:93–96, 1998.
22. Mota RA, Brito MF, Castro FJC, et al: Mormo em equideos nos Estados de Pernambuco e Alagoas. Pes Vet Bras 20:155–159, 2000.
23. Elschner MC, Klaus CU, Liebler-Tenorio E, et al: Burkhold-eria mallei infection in a horse imported from Brazil. Eq Vet Ed 21(3):147–150, 2009.
24. Srinivasan A, Kraus CN, DeShazer D, et al: Glanders in a military research microbiologist. N Engl J Med 345:256–258, 2001.
25. Bondi SK, Goldberg JB: Strategies toward vaccines against Burkholderia malleiu and Burkholderia pseudomallei. Expert Rev Vaccines 7(9):1357–1365, 2008.
26. Liguori AP, Warrington SD, Ginther JL, et al: Diversity of 16S-23S rDNA internal transcribed spacer (ITS) reveals phylogenetic relationships in Burkholderia pseudomallei and its near-neighbors. PLoS One 6(12):e23923, 2011.
27. Gregory BC, Wagg DM: Glanders. In Dembe ZF, editor: Medical aspects of biological warfare, rev ed, Falls Church, VA, 2007, Office of the Surgeon General United States Army and Washington DC, 2007, Borden Institute Walter Reed Army Medical Center, pp 121–146.
28. OIE Terrestial Manual Chapter 2.5.11 Available at www.oie.int/en/international-standard-setting/terrestial-manual/access-online.
29. Katz J, Dewald R, Nicholson J: Procedurally similar com-petitive immunoassay systems for the serodiagnosis of Babesia equi, Babesia caballi, Trypanosoma equiperdum, and Burkholderia mallei infection in horses. J Vet Diagn Invest 12:46–50, 2000.
30. Sprague LD, Zachariah R, Neubauer H, et al: Prevalence-dependent use of serological tests for diagnosing glanders in horses. BMC Vet Res 5:32, 2009.
31. Elschner MC, Scholz HC, Melzer F, et al: Use of a Western blot technique for the serodiagnosis of glanders. BMC Vet Res 7:4, 2011.
32. Neubauer H, Sprague LD, Zacharia R, et al: Serodiagnosis of Burkholderia mallei infections in horses: state-of-the-art and perspectives. J Vet Med B Infect Dis Vet Public Health 52:201–205, 2005.
33. Kenny DJ, Russell P, Rogers D, et al: In vitro susceptibilities of Burkholderia mallei in comparison to those of other pathogenic Burkholderia spp. Antimicrob Agents Che-mother 43:2773–2775, 1999.
34. Heine HS, England MJ, Waag DM, et al: In vitro antibiotic susceptibilities of Burkholderia mallei (causative agent of glanders) determined by broth microdilution and E-test. Antimicrob Agents Chemother 45:2119–2121, 2001.
35. Batmanov VP: [Treatment of experimental glanders with combinations of sulfazine or sulfamonomethoxine with tri-methoprim]. Antibiot Khimioter 38:18–22, 1993.
36. Thibault FM, Hernandez E, Vidal DR, et al: Antibiotic susceptibility of 65 isolates of Burkholderia pseudomallei and Burkholderia mallei to 35 antimicrobial agents. J Anti-microb Chemother 54:1134–1138, 2004.
37. Estes DM, Dow SW, Schweizer HP, et al: Present and future therapeutic strategies for melioidosis and glanders. Expert Rev Anti Infect Ther 8(3):325–328, 2010.
38. De Groot AS, Ardito M, Moise L, et al: Immunogenic con-sensus sequence T helper epitopes for a pan-Burkholderia biodefense vaccine. Immunome Res 7:2–7, 2011.
39. Whitlock GC, Robida MD, Judy BM, et al: Protective anti-gens against glanders identified by expression library immu-nization. Front Microbiol 2:227, 2011.
40. Biological and chemical terrorism: strategic plan for pre-paredness and response. Recommendations of the CDC Strategic Planning Workgroup. MMWR 49:1–14, 2000.
41. Robins GD: A study of chronic glanders in man with report of a case: analysis of 156 cases collected from the literature. Stud R Victoria Hosp Montreal 2:1–98, 1906.





























