Embed Size (px)
Citation preview

3/30/2018
1
Epinephrine
Cardiovascular Emergencies Symposium 2018
Corey M. Slovis, M.D.Vanderbilt University Medical Center
Metro Nashville Fire DepartmentNashville International Airport
Nashville, TN
High Quality BLS
• Compress at 100-120/minute
• Compress 2 inches
• Allow full chest rise
• Minimize interruptions
• Do not hyperventilate (8-10/minute)
ACLS like BCLS continues to evolve
“High Quality” ACLS
• Intubate Oxygenate and Hyperventilate
• Epinephrine 1 mg Q 3 minutes
• Atropine 1 mg Q 3 minutes
• Calcium Chloride 1 mg Q 3 minutes
• Bicarbonate 2 amps IVP / 1 Q 5 min
• Intubate Oxygenate and Hyperventilate
• Atropine 1 mg Q 3 minutes
• Calcium Chloride 1 mg Q 3 minutes
• Bicarbonate 2 amps IVP / 1 Q 5 min
Circulation 2015:132 (suppl 2);5444-64
Standard dose epinephrine (1 mg Q 3-5 minutes) may be reasonable for patients
with cardiac arrest (class 11b)
Epinephrine Use
3/30/2018
2
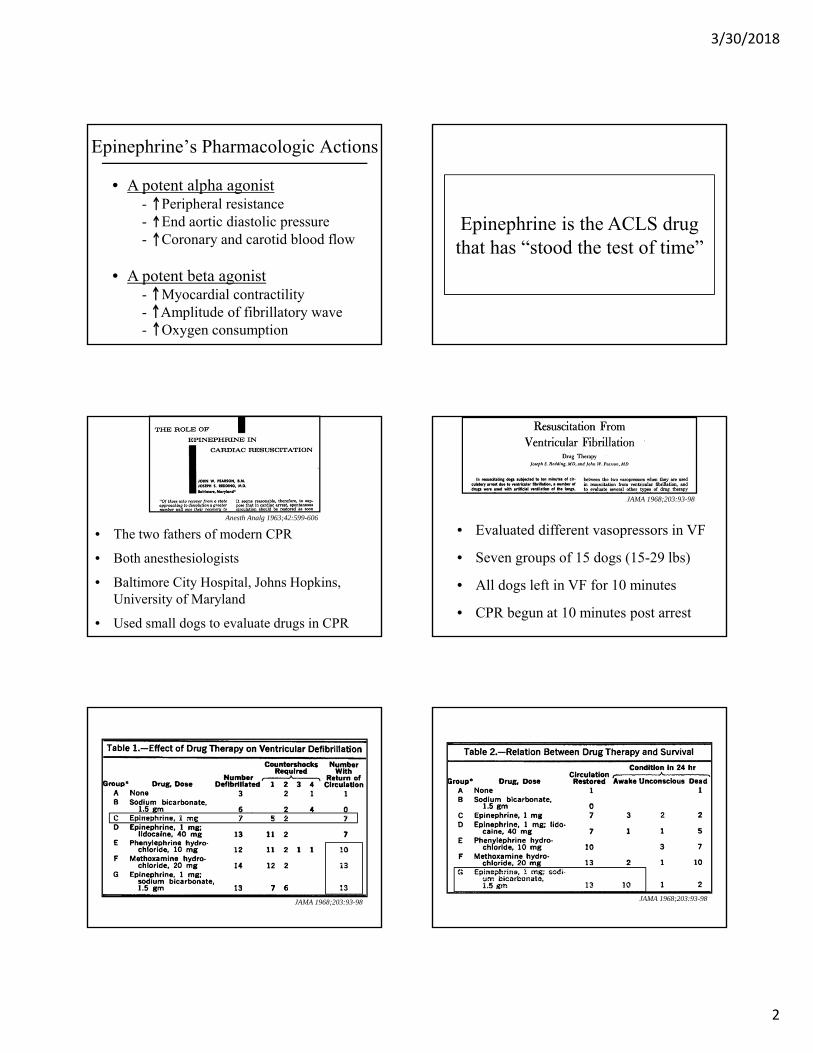
Epinephrine’s Pharmacologic Actions
• A potent alpha agonist- Peripheral resistance- End aortic diastolic pressure- Coronary and carotid blood flow
• A potent beta agonist- Myocardial contractility- Amplitude of fibrillatory wave- Oxygen consumption
Epinephrine is the ACLS drug that has “stood the test of time”
Anesth Analg 1963;42:599-606
• The two fathers of modern CPR
• Both anesthesiologists
• Baltimore City Hospital, Johns Hopkins, University of Maryland
• Used small dogs to evaluate drugs in CPR
JAMA 1968;203:93-98
• Evaluated different vasopressors in VF
• Seven groups of 15 dogs (15-29 lbs)
• All dogs left in VF for 10 minutes
• CPR begun at 10 minutes post arrest
JAMA 1968;203:93-98 JAMA 1968;203:93-98

3/30/2018
3
Anesth Analg 1965;44:746-52
• Compared early vs late epinephrine in Asystole
• 2 groups of 10 dogs using 1 mg of epinephrine
• Group 3 received epi after 1 min Asystole
• Group 4 received epi after 10 mins Asystole Anesth Analg 1965;44:746-52
Anesth Analg 1965;44:746-52
Take Home #1
Early administration of epinephrine appears to be the optimal
pharmacologic therapy in CPR based on its use in a relatively low
number of small dogs
“I question the choice of epinephrine as the emergency drug
to use in cardiac arrest”
Eastwood DW. Discussion of “Influence of peripheral vascular tone In cardiac resuscitation. Anesth Analg 1965;44:750
Corey Slovis from Clinical Essays on the Heart Vol 5.Hurst JW 1985, McGraw Hill:277-92
“Physicians should question the routine use of epinephrine in coarse ventricular fibrillation. In
this situation a pure alpha antagonist, which does not have epinephrine’s adverse myocardial effects might be significantly more beneficial”

3/30/2018
4
Epinephrine’s effectiveness has been questioned for
more than 50 years
Take Home #2
If 1 mg of epinephrine is the right dose in 10 kg dogs, are
larger doses more appropriate in 60-100 kg humans?
Anal Emerg Med 1989;18:1011-12
• Higher doses of epinephrine are required to better improve and end aortic diastolic pressure
• 0.1 mg/kg not 0.01 mg/kg needed to adequately perfuse the head and the heart
• 1 mg in 10-20 kg dog = 5-10 mg in 50-100 kg adult
• There are now many subjective reports of success with “high dose” epinephrine
NEJM 1992;327:1045-50
NEJM 1992;327:1051-5
JAMA 1992;268:2667-72 NEJM 2004;350:1722-30
High Dose Epinephrine
High Dose Epinephrine“Right Dose” Epinephrine
• Dramatic improvements in EMS ROSC
• Dramatic improvement in Survival to ED
• Significantly more admissions to ICUs
NO improvement in survival or good neurologic outcomes – only
more prolonged ICU stays and costs
“High-dose” epinephrine, of more than 1 mg per dose, significantly
improves ROSC but not survival to discharge
Take Home #3

3/30/2018
5
How effective is Epinephrine in Cardiac Arrest?
The first major article to question the efficacy of epinephrine and other ACLS drugs in CPR
• 773 ED and IP patients, 5 Canadian hospitals
• 34.8% 1 hour survival
• All meds including epinephrine decreased survival
Annals of Emerg Med 1998;32:544-53
When age, gender, comorbid condition controlled for along with rhythm and cause of arrest:
“A significant association between unsuccessful resuscitation and the use of epinephrine”
(OR 0.08 95% CI .04-.14)
Annals of Emerg Med 1998;32:544-53
• 851 patients, Oslo Norway, 2003-2008
• 433 got “ACLS” but no IV meds
• No Epi, Atropine, Amio
• ACLS drugs improve ROSC, not survival
JAMA 2009;302:2222-9
Do IV ACLS medications improve outcomes in cardiac arrest?
Conclusion
“Despite improved short term survival among patients randomized to receive IV
access and drug administration, these nearly universal interventions were not associated with a statistically significant improvement
in survival to hospital discharge”
• A relook where epi showed no benefit
• A post hoc analysis of Oslo Norway EMS data
• Now a comparison of only pts with or without epi
• 367 pts received epi vs 481 no epi
• Original study: some “epi pts” got no epi, no IV but had + ROSC
Resuscitation 2012;83:327-32
How effective is epinephrine, a re-look at prior data
3/30/2018
6
0%
10%
20%
30%
40%
Hundreds
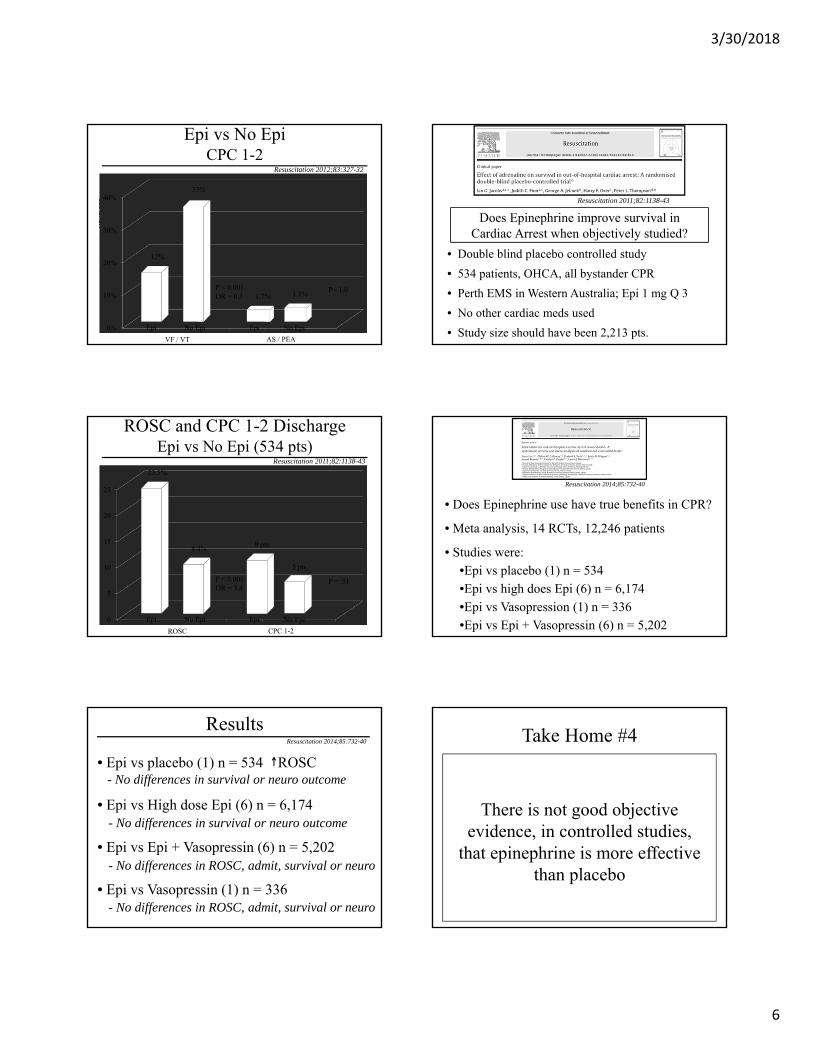
Epi vs No EpiCPC 1-2
Resuscitation 2012;83:327-32
VF / VT AS / PEA
12%
Epi No Epi Epi No Epi
P < 0.001OR = 0.3
33%
1.7% 1.8%P= 1.0
Does Epinephrine improve survival in Cardiac Arrest when objectively studied?
• Double blind placebo controlled study
• 534 patients, OHCA, all bystander CPR
• Perth EMS in Western Australia; Epi 1 mg Q 3
• No other cardiac meds used
• Study size should have been 2,213 pts.
Resuscitation 2011;82:1138-43
0
5
10
15
20
25
ROSC and CPC 1-2 DischargeEpi vs No Epi (534 pts)
Resuscitation 2011;82:1138-43
ROSC CPC 1-2
23.5%
Epi No Epi Epi No Epi
P < 0.001OR = 3.4
8.4% 9 pts.
5 pts.
P = .31
• Does Epinephrine use have true benefits in CPR?
• Meta analysis, 14 RCTs, 12,246 patients
• Studies were:
•Epi vs placebo (1) n = 534
•Epi vs high does Epi (6) n = 6,174
•Epi vs Vasopression (1) n = 336
•Epi vs Epi + Vasopressin (6) n = 5,202
Resuscitation 2014;85:732-40
• Epi vs placebo (1) n = 534 ROSC
• Epi vs High dose Epi (6) n = 6,174
• Epi vs Epi + Vasopressin (6) n = 5,202
• Epi vs Vasopressin (1) n = 336
- No differences in survival or neuro outcome
- No differences in survival or neuro outcome
- No differences in ROSC, admit, survival or neuro
- No differences in ROSC, admit, survival or neuro
ResultsResuscitation 2014;85:732-40
There is not good objective evidence, in controlled studies,
that epinephrine is more effective than placebo
Take Home #4

3/30/2018
7
Maybe if epinephrine was given sooner it would work better
• 686 pts, retrospective review, Royal Oak, Michigan
• 911 to Epi < 10 min vs > 10 min
• Evaluated rhythm and ROSC and survival to discharge
Resuscitation 2013.;84:915-20
Does giving epinephrine sooner improve outcomes in out of hospital arrests?
• Witnessed arrests: Early Epi increased ROSC by 3.2 X
• Early Epi did not improve survival to discharge
JAMA 2015;314:802-10
• 1,558 pediatric patients
• Average age = 9 mos
• 31.3% overall survival rate
• 17.1% favorable neurologic status
• Matched rhythm and numerous variables
Does time to epinephrine affect outcomes innon-VF-VT pediatric arrests?
0
5
10
15
20
25
30
35
40 33.1%
Survival and Time to Epi
< 5 min > 5 min
21.0%
%
JAMA 2015;314:802-10
JAMA 2015;314:802-10
• Longer time to epi = decreased ROSC
• Longer time to epi = worse survival
• time to epi = neurologic outcomes
ResultsAm J Emerg Med 2017;35:676-80
Does timing of epinephrine affect neurologic outcome in cardiac arrest?
• 13,326 pts, retrospective Japanese database
• 2011-2014 data; divided pts into 2 groups
• 8 min from 911 to arrival and 8-16 min from 911
• Evaluated if epi given within 10 min of arrival
3/30/2018
8
0
1
2
3
4
5
6
7
8
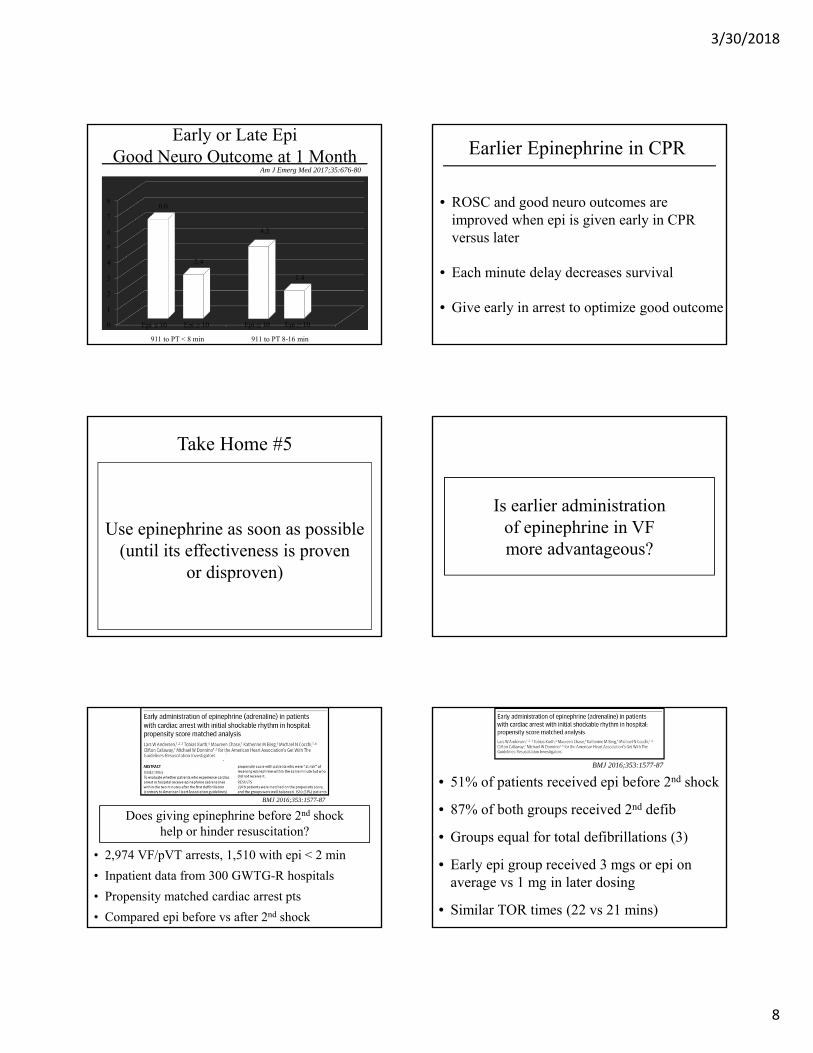
2.4
1.4
Early or Late EpiGood Neuro Outcome at 1 Month
Am J Emerg Med 2017;35:676-80
911 to PT < 8 min 911 to PT 8-16 min
6.0
Epi ≤ 10 Epi ≥ 10 Epi ≤ 10 Epi ≥ 10
4.2
Earlier Epinephrine in CPR
• ROSC and good neuro outcomes are improved when epi is given early in CPR versus later
• Each minute delay decreases survival
• Give early in arrest to optimize good outcome
Use epinephrine as soon as possible (until its effectiveness is proven
or disproven)
Take Home #5
Is earlier administration of epinephrine in VF more advantageous?
• 2,974 VF/pVT arrests, 1,510 with epi < 2 min
• Inpatient data from 300 GWTG-R hospitals
• Propensity matched cardiac arrest pts
• Compared epi before vs after 2nd shock
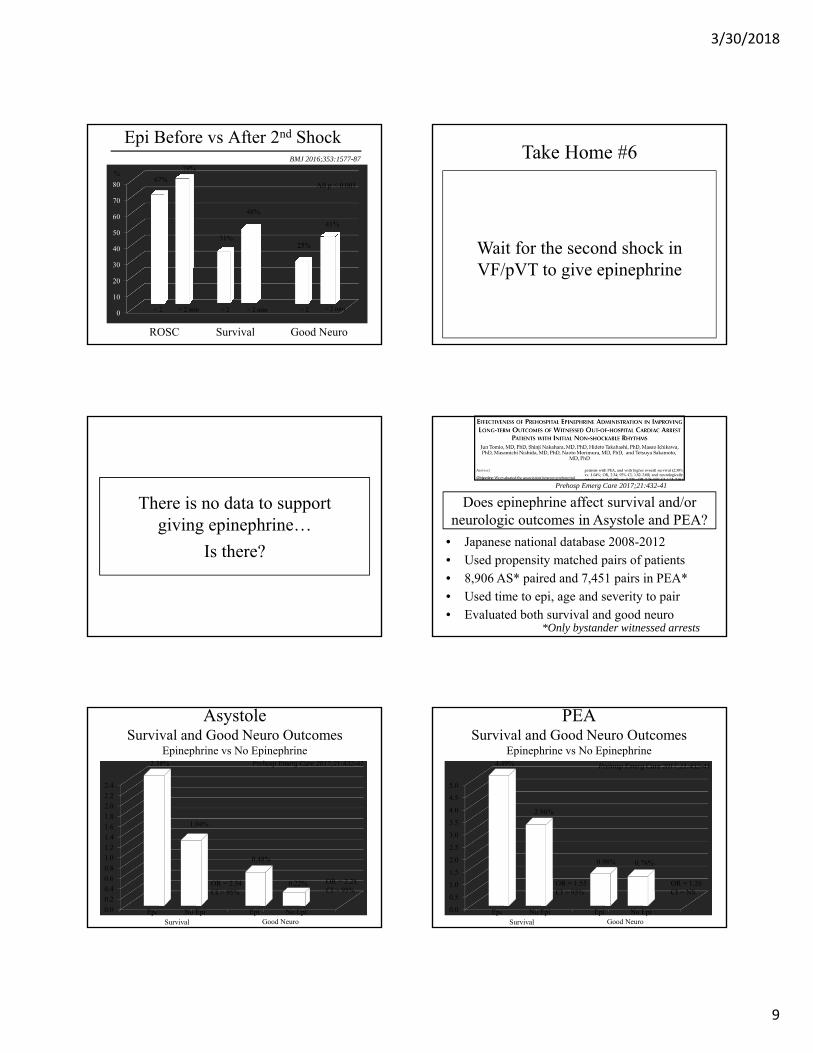
BMJ 2016;353:1577-87
Does giving epinephrine before 2nd shock help or hinder resuscitation?
• 51% of patients received epi before 2nd shock
• 87% of both groups received 2nd defib
• Groups equal for total defibrillations (3)
• Early epi group received 3 mgs or epi on average vs 1 mg in later dosing
• Similar TOR times (22 vs 21 mins)
BMJ 2016;353:1577-87
3/30/2018
9
0
10
20
30
40
50
60
70
8067%
79%
Epi Before vs After 2nd Shock
ROSC
31%
48%
BMJ 2016;353:1577-87
%
< 2 < 2> 2 min > 2 min
25%
41%
Good Neuro
< 2 > 2 min
Survival
All p < 0.001
Wait for the second shock in VF/pVT to give epinephrine
Take Home #6
There is no data to support giving epinephrine…
Is there?
Prehosp Emerg Care 2017;21:432-41
Does epinephrine affect survival and/or neurologic outcomes in Asystole and PEA?
• Japanese national database 2008-2012
• Used propensity matched pairs of patients
• 8,906 AS* paired and 7,451 pairs in PEA*
• Used time to epi, age and severity to pair
• Evaluated both survival and good neuro *Only bystander witnessed arrests
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
0.48%
1.04%
0.22%
Asystole Survival and Good Neuro Outcomes
Epinephrine vs No EpinephrinePrehosp Emerg Care 2017;21:432-41
Survival Good Neuro
2.38%
Epi No Epi Epi No Epi
OR = 2.34CI > 95%
OR = 2.28CI > 95%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
0.98%
2.96%
0.78%
PEA Survival and Good Neuro Outcomes
Epinephrine vs No EpinephrinePrehosp Emerg Care 2017;21:432-41
Survival Good Neuro
4.49%
Epi No Epi Epi No Epi
OR = 1.55CI > 95%
OR = 1.26CI = NS

3/30/2018
10
But…
• 1,556 patients from 2000 – 2012
• 1,134 (73%) received epinephrine
• 422 (27%) did not receive epinephrine
• Evaluated frequency of CPC 1 - 2 survival
JACC 2014;64:2360-7
Does prehospital epinephrine improve functional outcome post OOH cardiac arrest?
• Study from Paris, France
• All patients had ROSC
• All were admitted
• + Epi patients: older, less witnessed
• + Epi patients: longer resuscitation, less VF/VT
JACC 2014;64:2360-7
Study compared 228 pairs of Epi vs non-Epi matched samples
0
10
20
30
40
50
60
70
30%
61%
Epi vs No-Epi: CPC 1 - 2Matched Pairs Evaluation
Epi Used No Epi
P < 0.001
68/228
138/228
Epi vs No-EpiAdditional Results
• Longer delay to epi = worse outcomes
• Negative effects of epi across subgroups
• Rhythm, TH, length of CPR, PCI
• The more the epi, the worse the outcome
JACC 2014;64:2360-7
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0.48
0.30
Epi Dosing and SurvivalCPC 1 - 2
1 Mg 2 - 5 Mgs
0.23
> 5 Mgs
OR
JACC 2014;64:2360-7

3/30/2018
11
Epinephrine’s role remains unclear.
The more you look, the more higher does of epinephrine look bad
Take Home #7
Maybe we are just giving too much epinephrine?
Resuscitation 2014;85:350-8
Does dosing interval of epinephrine affect survival in CPR?
• 20,909 adult pts, 505 GWTG hospitals
• Looked at survival vs dosing interval
• Adjusted via multi-variate analysis
• Most common intervals were 4-5 and 5-6 min 0.00
0.25
0.50
0.75
1.00
1.25
1.50
1.75
2.00
2.25
2.50
2.75
3.00
5-6
0.780.96
Epinephrine Dosing Intervals (min)Adjusted Odds Ratio for Survival
1-3 3-4
Resuscitation 2014;85:350-8
1
4-5
OR
6-7 7-8 8-9 9-10
0.96
1.41 1.30
1.79
2.17
Resuscitation 2017;117:18-23
Does spacing out epinephrine more than PALS/ACLS recommends affect pediatric
CPR outcomes?
• 1,630 pediatric in-hospital arrests
• Intervals of 1-5, 5-8 min and 8-10 min evaluated
• Multi-variate analysis used to control co-morbidities
• Separately analyzed vasopressor use pre-arrest 0.00
0.25
0.50
0.75
1.00
1.25
1.50
1.75
2.00
2.25
2.50
2.75
3.00
1.0
1.99
Epinephrine Dosing Intervals (min)Adjusted Odds Ratio for Survival
1-5 5-8
Resuscitation 2017;117:18-23
2.67
8-10

3/30/2018
12
Epinephrine Dosing Interval
• Although ACLS guideline say Q 3-5, it appears that spacing epinephrine doses out to up to 8-10 minutes may be optimal
• This is a violation of current guidelines
• No randomized study exists
• Give less not more
Try to space your repeat doses of epinephrine by longer intervals
not shorter ones
Take Home #8
Maybe then, reduced dose epinephrine in cardiac arrest
is the answer?
Resuscitation 2018;124:43-48
Could less than 1.0 mg be better dose of epinephrine?
• 2,255 pts from Seattle, 2008-2016
• 554 (24.6%) VF/VT; 1,701 (75.4%) AS/PEA
• Before and after type study
• VF/VT: 0.5 mg min 4, 8; AS/PEA: 0.5 mg Q 2 min
• Evaluated ROSC, Discharge, CPC 1-2
0
10
20
30
40
50
60
56.4% 54.2%
VF/VT Outcomes0.5 mg vs 1.0 mg Epinephrine
ROSC
35% 34.2%
Resuscitation 2018;124:43-48
%
Std StdLow Low
32.9% 30.5%
Good NeuroStd Low
Discharged
0
10
20
30
40 34.7% 35.8%
AS / PEA Outcomes0.5 mg vs 1.0 mg Epinephrine
ROSC
4.2% 5.1%
Resuscitation 2018;124:43-48
%
Std StdLow Low
3.1% 3.5%
Good NeuroStd Low
Discharged
3/30/2018
13
Low Dose Epinephrine
• Not a randomized trial
• Cross overs from either group
• 3.4 mg vs 2.6 mg in VF/VT; 3.5 mg vs 2.8 mg in AS/PEA
Reducing the dose of epinephrine in OOH cardiac arrests does not affect ROSC, hospital discharge frequency or neurologic outcomes in
either shockable or non-shockable rhythms
Reduced dose epinephrine offers no benefits
Take Home #9
The case for or against epinephrine in CPR is embarrassingly not based on large randomized
double-blind studies
Final Take HomeTake Home #10
Epinephrine in Cardiac ArrestSummary
• Use appears to decrease functional neurological status in survivors
• More epi = worse outcomes
• May increase ischemic-reperfusion and post-anoxic injury
• PCI and hypothermia do NOT attenuate Epi’s negative effects
Epinephrine Biases 2018
• The more epi, the more likely the patient will do worse – but the more epi, the longer the code
• High quality BCLS, later intubation, and selective application of ECLS seems more likely to save selected patients
• Earlier administration of epinephrine, not later, is well supported by multiple studies
• One dose after second shock for VF
Epi improves ROSC
Summary
Survival benefits unproven
Give early, not late
Give after second shock
Await London study

3/30/2018
14