Embed Size (px)
Citation preview

Epilepsy guideline
พ.ญ.พรรณปพรโคนพนธ
ประสาทแพทย
โรงพยาบาลสรรพสทธประสงค


Outline
การวนจฉยอาการชก
การจ าแนกประเภทของอาการชกและโรคลมชก
แนวทางการสบคนในผ ปวยทมอาการชกและโรคลมชก
การวนจฉยแยกอาการชกและโรคลมชกจากภาวะอนๆ

Outline
การสงตอผ ปวยเพอการรกษา
แนวทางการรกษาผ ปวยชกครงแรกและชกซ า
แนวทางการบรหารยากนชก
แนวทางการดแลผ ปวยโรคลมชกชนดไมตอบสนองตอการรกษา

การวนจฉยอาการชก

History taking
• Preictal symptoms
– prodomes
– aura
• Seizure symptoms
– level of consciousness
– abnormal movement
– automatism
– respiration

History taking
• Seizure symptoms
– Phonation
– ANS dysfunction
• ลกษณะของอาการชก
– Sudden onset, paroxysm
– Brief duration
– Involuntary
– Stereotype
– Spontaneous remission

History taking
• Postictal symptoms
– Alteration of consciousness: confusion,
drowsiness, sleepiness
– Psychosis: visual/auditory hallucination
– Headache
– Todd, s paralysis
• Precipitating/provoking factors
– Alcohol
– Medications
– infection

History taking
• Underlying disease
– Previous CNS infection
– Brain trauma
– Diabetes, hypertension
• Psychosocial history
– Occupation
• Family history
– Epilepsy
– Genetic disease

Tuberous sclerosis complex

Sturge-Weber syndrome

Physical examination
• General examination
– Vital signs: atrial fibrillation, hypertension
– Head contour
– Skin
• Neurological examination
– Consciousness
– Focal neurological deficit
– Meningeal irritation sign

การจ าแนกประเภทของอาการชกและโรคลมชก

Seizure
• Definition
– อาการทเกดจากภาวะทมการเปลยนแปลงอยางเฉยบพลนของการท างานของเซลลสมอง โดยมการปลดปลอยคลนไฟฟาทผดปกต (epileptiform
activity) ออกมาจากเซลลสมองจ านวนมากพรอมๆกน
จากสมองจดใดจดหนงหรอทงหมด

Seizure classification (ILAE1981)
1. Partial seizure
Simple partial seizure
Complex partial seizure
Partial seizure evolving to secondarily
generalized clonic tonic seizure
2. Generalized seizure
Absence seizure
Generalized tonic-clonic seizure
Generalized tonic seizure

Seizure classification (ILAE1981)
2. Generalized seizure
Absence seizure
Generalized tonic seizure
Generalized clonic seizure
Atonic seizure
Myoclonic seizure
3. Unclassified seizure
Absence seizure
Generalized tonic seizure

Epilepsy (โรคลมชก)
• Definition
– โรคทผ ปวยมอาการชกซ า> 1 ครงทไมไดเกดในชวงเวลาเดยวกนโดยไมมปจจยกระตน (provoking
factor) ทชดเจน

Epilepsy classification (ILAE1989)
1. Localization related (focal) epilepsy
partial seizure
2. Generalized epilepsy
Absence seizure
3. Undetermined epilepsy
Absence seizure
4. Special syndrome
Febrile convulsion

Classification by etiology and
pathology
1. Idiopathic
2. Symptomatic
Brain tumor
Stroke
3. Cryptogenic

Acute symptomatic seizure
Cerebral venous sinus thrombosis with venous infarction
and hemorrhagic transformation

Acute symptomatic seizure
Viral encephalitis

Acute symptomatic seizure
Cerebral abscess Neurocysticercosis

แนวทางการสบคนในผปวยทมอาการชกและโรคลมชก

วตถประสงคในการสบคน
1. ชวยการวนจฉยอาการชกและโรคลมชก
2. ชวยจ าแนกชนดของอาการชกและโรคลมชก
3. หาสาเหตของการชก
4. ตดตามการด าเนนโรคและผลการรกษา

การสบคน
1. การตรวจทางหองปฏบตการ CBC, blood sugar, BUN/Cr, electrolyte, LFT,
Ca, Mg,toxicology screening, AEDs level
LP: meningitis, SAH, leptomeningeal
metastasis
2. การตรวจการท างานของสมอง EEG
3. การตรวจกายภาพของสมอง (brain imaging):
CT brain or MRI brain

ขอบงชของการสงตรวจ brain imaging
1. Localization related epilepsy
2. Adult onset epilepsy
3. Intractable epilepsy
4. Evaluate for epilepsy surgery

การวนจฉยแยกอาการชกและโรคลมชกจากภาวะอนๆ

การวนจฉยแยกอาการชกและโรคลมชกจากภาวะอนๆ
1. Migraine headache
2. Syncope
3. Hyperventilation syndrome
4. Movement disorder
5. Transient ischemic attack (TIA)
6. Transient global amnesia (TGA)
7. Psychogenic disorder

Migraine versus temporal lobe epilepsy
Clinical feature Migraine Temporal lobe
epilepsy
Aura duration 2-5min 5-30sec
Aura type Visual phenomenon
most common
Aura often difficult to define
and consists of fear,
detachment, or abdominal
sensation
Impairment of
consciousness
None Impaired consciousness in
complex partial seizure
Postictal
impairment
No Postictal impairment in
complex partial seizure

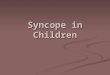
Seizure versus syncope
Clinical feature Syncope Seizure
Relation to posture Common No
Muscle tone Flaccid Increased in tonic-clonic and
complex partial seizure
Duration 10sec 1-2min (tonic-clonic)
Sleep Rarely occurs in sleep May occur during sleep
Incontinence Rarely Often
Tongue biting or
injury
Not likely May occur
Skin color Pale Flushed
Diaphoresis Common Rare

แนวทางการรกษาผปวยชกครงแรกและชกซ า

Seizure
recurrence rate
76%
73%
Fourth seizure
Third seizure
Second seizure
First unprovoked seizure
Seizure recurrence rate in a
population-based study
33%

Factors predicting a higher recurrence risk
following a single unprovoked seizure
Abnormal neurologic examination
Abnormal electroencephalogram
Abnormal brain imaging
Partial seizure
Status epilepticus
Remote symptomatic etiology
Family history of epilepsy
ควรพจารณาเรมยากนชกตงแตชกครงแรก

แนวทางการบรหารยากนชก

หลกการบรหารยากนชก
1. เรมยาเมอแนใจวาผ ปวยเปนโรคลมชกจรง
2. เลอกใชใหเหมาะสมกบชนดของอาการชก
3. การเรมใหยากนชก
เรมดวยยาตวเดยวกอน
กรณผ ปวยชกแบบstatus epilepticus ควรใหยาทางหลอดเลอดด า

หลกการบรหารยากนชก
4. การปรบยากนชก
เรมขนาดนอยๆคอยๆปรบขนทละนอยจนกระทงควบคมอาการชกได ในขนาดยาทผ ปวยทนตอผลขางเคยงได (maximal tolerated dose)
5. ควรอธบายแนวทางการรกษา

หลกการบรหารยากนชก
6. บรหารยาตามคณสมบตทางเภสชวทยา
Half life
Steady state
preparation
7. การตรวจระดบยากนชกในเลอด
ใหยาในขนาดและปรมาณทเหมาะสมแลวแตยงควบคมอาการชกไมได
ผปวยมอาการทสงสยวายาเกนขนาด

AED
Half-life (hours) Short:≤10
Intermediate:>10 to<30
Long:≥30
Phenobarbital long
Phenytoin Intermediate
Valproate Intermediate
Carbamazepine Intermediate
Gabapentin Intermediate
Topiramate Intermediate
Levetiracetam Short

หลกการบรหารยากนชก
7. การตรวจระดบยากนชกในเลอด
ประเมนความสม าเสมอในการรบประทานยาของผ ปวย
เฝาระวงระดบของยากนชกในภาวะทมการเปลยนแปลงของโปรตนในเลอด เชน ตงครรภ
เฝาระวงระดบยา กรณไดรบยาหลายชนดทอาจจะมปฏกรยาระหวางยา

Generalised-onset seizure
Broad- spectrums AEDs for all seizure types
Valproic acid
Lamotrigine
Topiramate
Levetiracetam
Zonisamide
Phenobarbital
Benzodiazepines
Partial-onset seizure
Absence Myoclonus Tonic-atonic Primary
tonic-clonic
Simple
partial Complex
partial
Secondary tonic-clonic
Lancet Neurol 2004;3: 729-35.
Restricted-spectrums AEDs
Carbamazepine
Phenytoin
Vigabatrin
Gabapentin
Ethosuximide

Seizure type
Initial choice
Second line
Tonic-clonic
Valproate,
Phenytoin
Carbamazepine
Lamotrigine,
Oxcarbazepine
Myoclonic Valproate
Topiramate,
Levetiracetam,
Zonisamide
Partial
Carbamazepine,
Phenytoin
Valproate,
Lamotrigine,
Oxcarbazepine,
Levetiracetam
Absence Valproate Ethosuximide,
Lamotrigine
Unclassifiable Valproate Lamotrigine

Special population
1. Elderly patients
Gabapentin
Lamotrigine
Topiramate
Avoid enzyme inducing AEDs: Phenytoin,
Carbamazepine, Phenobarbital
2. Women of childbearing age
Avoidance of highly teratogenic AEDs:
Valproate have major congenital
malformation rate 10% esp. at high dose

Comorbid conditions
1. Depression
Lamotrigine
2. Bipolar disorder
Valproate
3. Kidney stone/ Glaucoma
Avoid topiramate
4. Migraine headache
Topiramate
Valproate

Comorbid conditions
5. Chronic pain
Gabapentin
Pregabalin
Carbamazepine
6. Obesity
Topiramate
Zonisamaide
Avoid Valproate, Pregabalin, Gabapentin

Administration of AEDs in adults
AEDs Starting
dose (mg/d)
Maintenance
dose (mg/d)
Frequency of
administration
Carbamazepine 100-200 400-1600 2-3 times daily
Clobazam 10 10-40 Once or twice daily
Ethosuzimide 250 500-1500 2-3 times daily
Gabapentin 300-900 900-1800 2-3 times daily
Lamotrigine 25 100-300 Twice daily
Levetiracetam 500 1000-3000 Twice daily
Lancet Neurol 2011; 10: 446–56

Administration of AEDs in adults
AEDs Starting
dose (mg/d)
Maintenance
dose (mg/d)
Frequency of
administration
Oxcarbamazepi
ne
300 600-2400 2-3 times daily
Phenobarbital 30-50 50-200 Once daily
Phenytoin 100 200-400 Once daily
Pregabalin 50-75 150-600 2-3 times daily
Topiramate 25 100-400 Twice daily
Valproate 500 500-2500 Once or twice daily
Lancet Neurol 2011; 10: 446–56

แนวทางการดแลผปวยโรคลมชกชนดทไมตอบสนองตอการรกษา

โรคลมชกทรกษายาก (Difficult-to-treat
epilepsy)
ผ ปวยลมชกทรกษามานานแตยงไมสามารถควบคมอาการชกได
โดยผ ปวยไดรบยาพนฐานไดแก CBZ, PHT,
VPA, PB อยางนอย 2ชนด ในขนาดและระยะเวลาทเหมาะสมแตยงควบคมอาการชกไมได

Questions to ask when things are not
going well: the 8C
1. Correct diagnosis?
2. Correct classification?
3. Correct drug/dosage?
4. Correct lesion?
5. Compliance?
6. Comorbidity?
7. Clarifying triggers?
8. Consistent with the truth?
Pract Neurol 2009; 9: 27–32

การรกษาดวยยากนชกรนใหม(Novel AEDs)
ขอบงช
– โรคลมชกทไมตอบสนองตอการรกษาดวยยากนชกพนฐาน
– ผปวยแพหรอมผลขางเคยงรนแรงตอยากนชกพนฐาน
– เพอหลกเลยง drug interaction กรณผ ปวยรบประทานยาหลายชนด

Factor influencing choice of add-on
treatment
1. Epilepsy classification
2. Drug interaction (AEDs, oral pill, etc)
3. Adverse effects
4. Side benefits

Adverse effect and unexpected benefit of AEDs
Aggravated No effect Helpful
Weight gain Carbamazepine
Pregabalin
Gabapentin
Valproate
Levetiracetam
Lamotrigine
Levetiracetam
Oxcarbamazepine
Topiramate
Zonisamide
Anxiety Levetiracetam Oxcarbamazepine
Valproate
Pregabaline
?Carbamazepine
?Lamotrigine
Depression Topiramate
?Levetiracetam
Oxcarbamazepine Pregabaline
?Lamotrigine
?Carbamazepine
Migraine Lamotrigine
Oxcarbamazepine
Gabapentin,Pregabalin
Topiramate
Valproate Pract Neurol 2009; 9: 27–32

Nature review 2009;10:68-82
Excitatory synapse
Excitatory synapse

หลกการเลอกยากนชกรนใหม
1. ผ ปวย partialและgeneralized tonic clonic
seizure
– Gabapentin, pregabalin
– Lamotrigine
– Levetiracetam
– Oxcarbamazepine
– Topiramate
– Zonisamide
– Vigabatrin

หลกการเลอกยากนชกรนใหม
2. ยาทใชเปน monotherapyได
– Gabapentin
– Oxcarbamazepine
– Topiramate
– Lamotrigine
3. ยาทเปน broad spectrum
– Lamotrigine
– Topiramate
– Levetiracetam, Zonisamide

การสงตอผปวยเพอการรกษา

การสงตอผ ปวยไปยงร.พ.ทมศกยภาพสงกวา
1. ไมแนใจการวนจฉยวาเปนโรคลมชก
2. จ าเปนตองตรวจคนหาสาเหตเพมเตม
3. ไมสามารถควบคมอาการชกได
4. ผ ปวยทจ าเปนตองไดรบยารกษาทเฉพาะ

หลกการหยดยากนชก

Should AEDs be discontinued in
seizure-free patients?
Might be considered after at least 2-4
years of seizure freedom
Discussion with the patient about
associated risk versus potential benefit
possibility of relapse

หลกการหยดยากนชก
1. ลดขนาดลงชาๆทก 4-8 สปดาห ตอยากนชก 1
ชนดตอครง จนกวาจะหมด
2. กรณรบประทานยากนชกหลายชนด ใหหยดทละชนดโดย
หยดยาเสรมกอนยาหลก
หยดยาทมผลขางเคยงสงกอน
หยดยาทมราคาแพงกอน

หลกการหยดยากนชก
3. หากชกระหวางลดหรอหยดยา ควรพจารณาเลอกยาเดมทใชไดผลในขนาดต าสดกอนทจะลดหรอหยดยา

Conclusions
AED monotherapy is indicated after 2
seizures
Considered initiation of AED in high risk
patients after one seizure
AED choice is determined by
Seizure type
Adverse-effect profile
Patient-specific features (age, sex and
comorbidities)

Conclusions
Dose titration and dosing regimens need
to be carefully individualised
Failure to achieves seizure freedom
should prompt diagnostic reassessment
Discontinuation of AEDs after at least2-4
years of seizure freedom should be
considered