Embed Size (px)
Citation preview

RALUCA PANAPGY-2 ADULT NEUROLOGY
JULY 17TH 2013
Emergency Lecture Series Syncope vs. Seizure

Introduction
Evaluating patients with transient loss of consciousness (TLOC) remains a challenge
These patients fall into 2 main groups: those with seizures and those with syncope
15% of transient loss of consciousness are due to seizures
Reflex syncope remains most common etiology with 58%

Case
22-year-old woman with a diagnosis of epilepsy since childhood presented to the ER after passing out during a blood draw. She recalled feeling anxious and nauseous, having a racing heartbeat, experiencing graying of vision, and then losing consciousness. Her boyfriend reported that her eyes rolled upward and her body became limp before stiffening and shaking for approximately 20 seconds. Afterward, she returned to baseline within a few minutes.
She had been diagnosed with epilepsy because of similar loss-of-consciousness events occurring since she was 4 years old. She had a total of 10 such events, and half were associated with medical procedures or orthostatic stress. She had been on anticonvulsant medications for many years.
The examination was normal, although she was pale and sweaty

Seizures OR Syncope?

Definitions
Seizure Defined as stereotyped spells caused by abnormal
electrical brain activity and can be provoked by a variety of conditions or occur spontaneously without an identifiable cause
Manifestions depend on underlying neuroanatomic substrate (spells article)

DDX of Seizure

Types of Seizures resembling syncope

Definitions
Syncope defined as an abrupt and transient loss of
consciousness associated with inability to maintain postural tone, often due to cerebral hypoperfusion

DDx of Syncope

Classification of Syncope
Examples of types of syncope
Neurocardiogenic Lack of sympathetic vasoconstriction or vagal
bradycardia Remains most common cause, look for a trigger
(pain, fear)Includes situational syncope : during straining,
coughing etc
Carotid Sinus hypersensitivityCommon in Elderly, syncope on neck turning Can reproduce with carotid sinus massage

Grey Areas
Psychogenic Presenting as seizure or apparent syncope Can account for up to 30% of refractory seizures Usually PMHx of psychiatric disorders, trauma,
abuse May sometimes document during formal video EEG
or tilt table Convulsive Syncope Myoclonic jerks during a syncope estimated to
occur between 12-46%, some reports 90% in blood donors

Clinical Approach to TLOC
In 50% of cases, it is estimated to arrive at a diagnosis by history and physical exam alone
Thorough History taking often in the presence of reliable informant/by standers
Should focus on two main elements: -Patient characteristics and past medical
history-Extremely Detailed description of the
episode of loss of consciousness

Specific Distinguishing Features
Clinical Setting: Seizures are usually unprovokedSyncope occurs in settings of strong emotional/painful
stimulirecent prolonged standing or sitting, or being able to
clearly remember the loss of consciousness.Startle : can point to hereditary long QT syndromes Aura/prodrome: pre-syncopal symtoms graying of vision, light-headedness,
muffling of sounds, sitting preceding warmth or diaphoresis, palpitation, dyspnea, chest pain
Typical Auras: rising epigastric sensation, automatisms, head turning, purpuseless movements, macropsia , dysphasia

Distinguishing Features
Associated Signs and Symptoms: -Pallor and diaphoresis strongly suggest
syncope -In syncope, fall is flaccid usually, eyes are
open and gaze is upward or straight-Tongue biting: unusual but if occurs, location
is at tip of tongue .Lateral Tongue biting is associated with epileptic seizures
-Urinary incontinence can occur in both seizures and syncope.

Specific Distinguishing Features
Motor Activity:
-brief motor activity, including tonic extension of the trunk and limbs or several clonic jerks can occur in both conditions
-Syncopal jerks are NOT rhythmic or synchronous, small amplitude, occur after LOC, last around 15 seconds
-Seizure : synchronous, large amplitude , long lasting , clearly unilateral and can occur prior to loss of consciousness. Clearly unilateral points to seizure

Specific Distinguishing Features
• Recovery Time:-Unconsciousness lasts less than 20sec in syncope unless patients are kept upright-Recovery is spontaneous and typically prompt
-Post-ictal phase can last for hours, especially in children.-Behavior and orientation usually return after 30sec -1min
-Retrograde amnesia in the elderly has been described

Clues in the history
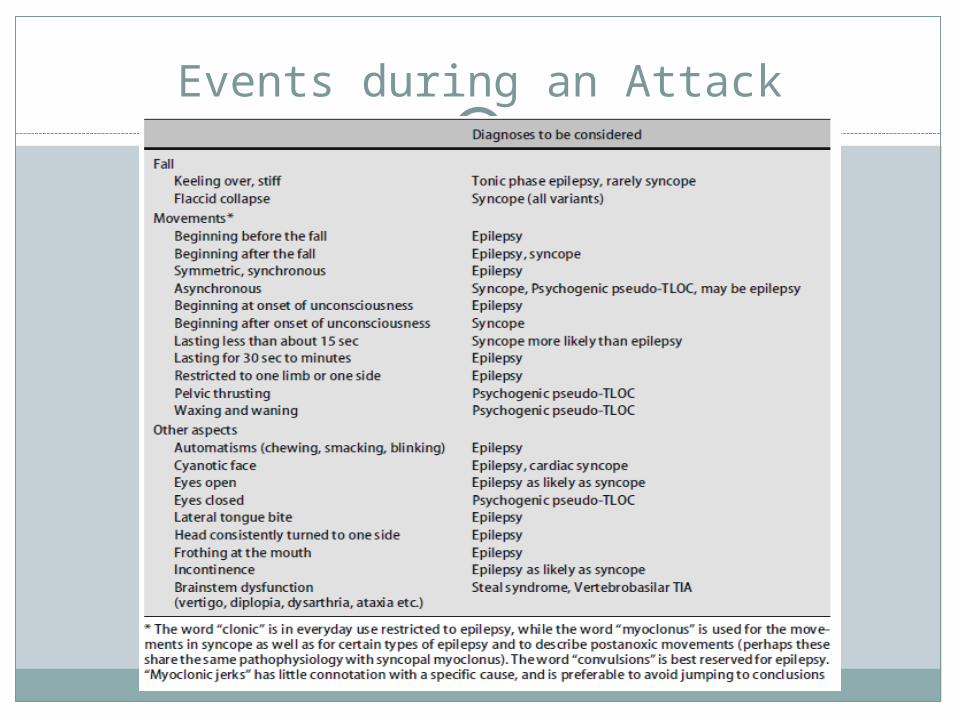
Events during an Attack

Events after an Attack

Patient caracteristics
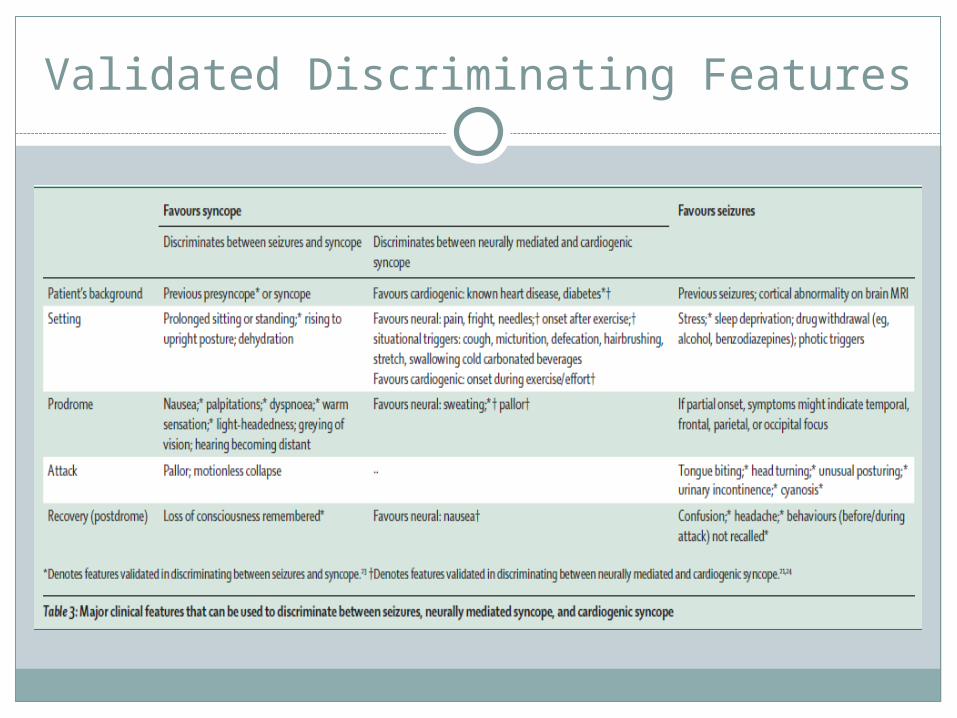
Validated Discriminating Features
What about tongue biting?
Meta-analysis by Brigo et al. In 2012 looked at clinical relevance of tongue biting in seizures and Psychogenic non epileptic events and evaluated Likelihood ratio of this physical finding
Showed a statistically significant difference in Tongue biting prevalence between epilepsy and PNEEs
More Tongue biting in Epilepsy group, even higher if it was lateral tongue biting

Studies Included

Meta-Analysis for Tongue Bite in Epilepsy

Normogram:LR for Lateral TB vs TB no precise
localization

Clinical Approach
Another useful tool to help distinguish syncope from seizures
Bedside questionnaire developed by Sheldon et al in 2002 that is validated to identify seizures in 94% of cases
Validated Historical Criteria
Prospectively analyzed data from 617 patients with loss of consciouness who completed a 118 item questionnaire
Developped Diagnostic criteria by correlating these historic features with their final diagnosis
They then tested the decision rule on 268 patients
Overall accuracy in test sample was 94% with a sensitivity of 94% for seizures
The presence of negative criteria solves the diagnostic problem of convulsive syncope


Bedside Questionnaire

Physical Exam
Vital signs: orthostatic VS, irregular HR Performing a carotid massage to identify
carotid sinus hypersensitivity can be useful
Cardiovascular examination: look for murmurs suggestive of aortic stenosis, increased size and altered location of PMI , Pericardial rub (restrictive pericarditis), etc

Physical exam
Thorough Neurological exam: - VS : febrile for seizures,
meningitis/encephalitis- ENT: Tongue lacerations - Altered mental status, post-ictal confusion- Looks for focal neuro signs - Previous scars (Neurosurgical)- Signs of Neuro dx associated with Autonomic
dysfunction (PD, MSA)

To summarize...

Investigations
Should not be guided by the specialty under which the patient is admitted
Rather should be guided by elements gathered in history taking
Recent review by Krahn et. al looked at evidence supporting different investigation modalities in patients with “collapse”.
In general it is recommended to start with EKG in all patients (can give prognostic information if underlying structural cardiac disease)

Investigations
Standard blood test CBC, chem 7, trops +/-toxicology depending on clinical history
Dx yield is about 2-3% Prolactin levels are not usefulCK levels are usually elevated in seizure
patients, but not alwaysEEG in undifferentiated patients with TLOC
yield of 1.5% similar to general population

Investigations
EEG: interictal EEG useful when there is a clinical suspicion of epilepsy (focal neuro findings or hx suggestive of epilepsy)
Timing of EEG is crucial: 50 % of patients who present after generalized convulsion have abnormlities on EEG within 24hours.
Within 48hrs, only 21-34% have epileptiform activity
Younger patients have higher yield Sleep deprived EEG may increase dx yield
by 30%

Investigations
Tilt table to detect neuro-cardiogenic syncope
Mainly in atypical storiesHolter diagnostic yield of about 10% when worn for
24hrsElectrophysiologic studies

Investigations
Imaging (CT, MRI)Diagnostic yield is about 5% for CT scan in
undifferentiated patients with collapseshould be done if there is a traumaIn the presence of focal neurological deficitsHigh suspicion of first seizure

What about our case...
This case illustrates several prototypical features of reflex syncope, including the temporal association with a painful event, the characteristic prodromal symptoms, and the rapid return to baseline.
The association of the event with abnormal movements is not inconsistent with the diagnosis of convulsive syncope, and the association of her prior losses of consciousness with medical procedures suggests that these events might also be due to convulsive syncope.
The patient underwent video-EEG monitoring, and one of her typical events was elicited by venipuncture and associated with a prolonged (40-second) asystolic pause, consistent with malignant reflex syncope .
ECG, cardiac telemetry, and echocardiography were normal, and the patient underwent pacemaker placement to prevent further prolonged asystoles. While the diagnosis of epilepsy could not be completely excluded, the patient has since been able to gradually wean antiepileptic medications and has remained seizure free.

In Summary

References McKeon, Vaughan, Delanty. Seizures versus Syncope. 2006,
Lancet 5; 171-80 Dijk, Thijs, Benditt et Wieling. A guide to Transient loss of
consciouness van . Nat. Rev. Neurol. 5, 438–448 (2009) Thijs, Dijk and Bloem. Falls, Faints, Fits and funny Turns
(2009) J Neurol (2009) 256:155–167 Kaplan, Nguyen, Non epileptic Paroxysmal disorders in
Adults and Adolescents (2012). Uptodate.com Krahn, Andrew et Dewell, Selecting Appropriate diagnostic
Tools for Evaluating the patient with Syncope/collapse 2013, Progress in Cardiovascular Diseases 402-409.



























![Syncope AHD[1]](https://img.dokumen.tips/doc/110x75/577d36611a28ab3a6b92ec10/syncope-ahd1.jpg)
