Embed Size (px)
Citation preview

APMIS 109: 321-32,2001
(please use this original reference for citation) Printed in Denmark . All rights reserved
Copyright 0 APMIS 2001
APUUS ISSN 0903-4641
Epidemiology of breast cancer: an environmental disease? Review article
ANNIE J. SASCO
Unit of Epidemiology for Cancer Prevention, International Agency for Research on Cancer, and Institut National de la Santk et de la Recherche Midicale, Lyon, France
Sasco AJ. Epidemiology of breast cancer: an environmental disease? Review article. APMIS 2001;
Breast cancer is the leading cancer site in women, both in the developed and the developing world. Incidence rates are increasing in many countries, although, in some, mortality may be stable or slightly decreasing. Geographical differences exist, with high rates of disease in North America, North Europe and Oceania, intermediate rates in South and Central America as well as South and East Europe, and low rates in Africa and Asia. Most of the literature reports that genetic inherited factors account for less than 5% of cases, although some authors advance higher figures, up to about 10%. Risk factors for breast cancer are related to the reproductive life of women: early menarche, nulliparity or late age at first birth, late menopause, diet and physical exercise, as well as hormonal factors, be they endogenous (high levels of free or not bound to SHBG estrogens) or exogenous (long-term use of oral contraceptives or menopausal hormone replacement). The present review does not aim to be exhaustive and fully comprehensive, or to present in detail domains currently well known and accepted by all. On the contrary, it modestly wishes to highlight potentially controversial conditions which could in the future be recognized as new risk factors.
Key words: Breast cancer; environment; epidemiology; hormones.
Annie J. Sasco, Unit of Epidemiology for Cancer Prevention, International Agency for Research on Cancer, 150 Cours Albert Thomas, 69372 Lyon Cedex 08, France. e-mail: [email protected]
109:321-32.
Breast cancer, which for centuries has been de- scribed by clinicians as the classical cancer of women, is the present-day concern of women all over the world, first as an epidemic which plagues them, but also as a possible patholog- ical marker of general exposures to hormones and more generally to endocrine disrupters, likely to have an impact on the human species as well as on wildlife and our planet.
In this paper, we first review the descriptive epidemiology of breast cancer, evaluating the burden of disease and death for women in the world, looking at current and past figures of ab- solute numbers and rates of the disease, con-
Received March 19, 2001. Accepted March 29, 2001.
S 80
trasting mortality and incidence trends. Then we review etiological epidemiology7 searching for risk and preventive factors, briefly distin- guishing direct factors from what would better be viewed as susceptibility states, and finally we propose a synthesis corresponding to the crucial need we are facing at the dawn of the XXIst century to explain the evolution of this disease and to search for new clues as to its etiology, among which the environment clearly stands.
DESCRIPTIVE EPIDEMIOLOGY
As its name indicates, the objectives of descrip- tive epidemiology are to quantify the burden of disease and death, to describe its geography and

EPIDEMIOLOGY OF BREAST CANCER
to evaluate trends over time, either measured in secular periods or for individuals in terms of age. As disease experience may be modified by treatment, care has to be taken to distinguish mortality from incidence.
World breast cancer burden The most recently published estimates for
mortality refer to the year 1999 with 467 000 deaths attributed to breast cancer for women in the world, representing 1.7% of all female deaths (1). In terms of absolute numbers, the figure is now higher for countries with a low or middle income, where 252 000 such deaths occurred, as compared to high income countries with 160000 deaths. Yet, the percentage of deaths due to breast cancer in women is still higher in the latter countries, at 2.0%, than in the former, at 0.5% (2).
In terms of incidence, estimates for 1997 amount to 895 000 new breast cancer cases worldwide, with 505 000 in the developed and 390 000 in the developing world. Therefore, breast cancer now ranks first among cancers in
women in the whole world and not only in the Western world (3).
Geographical epidemiology According to the cancer incidence rates pub-
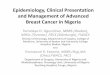
lished by population-based cancer registries, zones with a high risk of breast cancer can clearly be distinguished, with world age-stan- dardized estimated national incidence rates greater than 80 new cases per 100 000 women- years. They correspond to North America (USA and Canada), Australia, New Zealand and some countries in Europe, but also se- lected countries elsewhere, such as for example Uruguay in South America (4). Examining ac- tual data from population-based cancer regis- tries rather than national estimates, among the 30 highest rates can be counted 20 registries from North America, one from South America (Montevideo), 2 from Israel and 5 from Eur- ope. The only one from Africa is for Euro- peans in Zimbabwe (Harare), and from Oceania the registry of Hawaii for Hawaiians (Fig. 1). In contrast, among the 30 lowest
Zimbabwe, Harare:Europ. US, LA:Non Hisp. White US, SENon Hkp. Whlte
US, Hawaii : White US, Connecticut : White
Uruguay, Montevideo us. Seattle
us. DetroitWhite US, SEER:Whte
Israel: Jews born in Israel us, Atlantll:White
Israd:Jerm born in Am. w Eur. US, New 0lleans:White
US, New Mer:Non Hisp. White US, CenL Calif.:Non HIsp. Whlte
France, Wre us, Iowa
US, New 0rieans:White us, c0nnectiCUt:Biack
Canada, Britlsh Colombia US, Hawaii:Hawalian
us, sF:Black UK, Oxford
us, LABiack US, Detroit:aiack
France, Haut-Rhin Franca, Wmult
Malta The Netherbnds US, SEER:Biack
I I
0 10 20 30 40 50 60 70 80 90 100 110 120 130
New cases per 100 OOO woman-years
Fig. 1. Population-based cancer registries with the 30 highest world-age-standardized incidence rates of female breast cancer.
S81

SASCO
Peru, Trljiiio
France, la R6union *N8 =
Costa Rica US, New Mexico:Amer. lndbn
India, Bombay Japsn, Nw=M
Ecuador, Quito China, ShM@ Poland, Kielce China, Tianjin Japan, Osaka India, Madm
Japan, Yamagata US, MKoraan
lamaimon Jaws India, Bangalore
Uganda, Kvadondo Zimbabwe, Haram:Afrkw
Japan. %a India, TdMndNm
Vlet Nam, Hanoi India. Karunagappaily malland, Chlang Mai
China, Wong Mali, Bamako A i m S e ( H
India, Barshi, Paranda & Bhum Thailand, Khon Kam
Kom, K q w h a
I
0 10 20 30 40 50 60 70 80 90 100 110 120 130 New cases per 100 OOO woman-years
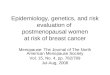
Fig. 2. Population-based cancer registries with the 30 lowest world-age-standardized incidence rates of female breast cancer.
rates, 5 are from Africa, 18 from Asia and Is- rael, 3 from South America, 2 from Eastern Europe and 2 from the United States of Amer- ica (American Indians in New Mexico and Koreans in Los Angeles, California) (Fig. 2) (5).
Potential explanations for these large geo- graphical differences may either be genetics or lifestyle and environment. In the past, the only way to distinguish these influences was to study migrant populations. In this regard, the study of Chinese migrating from the People’s Republic of China to Hong-Kong and then the United States of America showed that it took more than one generation and often more than two to progressively move towards the high rates of breast cancer of Caucasian American women compared to the very low rates of Chinese women in China (6).
Temporal epidemiology Time in epidemiology may either be debed
as calendar period or for a given individual as age.
Over time, the world breast cancer burden has
s 82
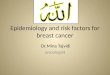
increased steadily with an almost doubling of the annual number of estimated new cases over a 20-year span, the increase being seen both in the developed as well as the developing coun- tries (Fig. 3) (7-9). Even when considering, as is more appropriate, rates rather than absolute figures, and thereby correcting for ageing of the population as well as differences in age struc- tures across countries, most cancer registries of the world still exhibit increases in breast cancer incidence. In the period 1975-1990, the largest increases, greater than 1% and sometimes 5% per year, are exhibited by registries previously having low rates of disease, mostly in Asia and Africa, as well as in some parts of Europe. In contrast, the smallest increases, in general under 0.5% per year, are usually seen in places pre- viously having high rates, mostly in North America and Europe. The picture is particularly clear when we look at the youngest age groups, below 45 years of age (5, 10). Even in countries like the USA, for the period 1975-1994, the av- erage annual change for white women was 1.4% and for black women 1.8% (1 1).
For a given individual, it can be stated that

EPIDEMIOLOGY OF BREAST CANCER
E 1000000 1 - B 'Developed' world
6
V m 'Developing' world
= m
2 500000 0 s
.- 4 d - 5
Z %
f " l . v
! - 5
0 0 - c
1980 1985 1990 1991 Year
Fig. 3. World breast cancer burden over time.
the major risk factor of breast cancer, and can- cer in general, is age. The vast majority of breast cancers appear among women older than 50 years of age. Yet such a distinction on the basis of age is crude, as for breast cancer ageing is not the sole intervening event. It is also necessary to consider what is most relevant from a physiopa- thological point of view, namely menopausal status. Particularly worrying are the increases seen among women under 45 years of age (5, 10).
A note on mortality versus incidence rates Most of what has been described above re-
lates to incidence rates. If we look at mortality rates instead, the picture for selected countries is now slightly less gloomy, with falling rates for example in the United Kingdom and in the USA (12). Even in countries such as France, where large increases in incidence rates are still seen, mortality rates have remained almost stable for the last 20 years (1 3). The discrepancy between mortality and incidence comes from better treatment, earlier diagnosis and screen- ing. For example, the impact is clearly seen in changes observed in survival in Europe (14, 15). This, of course, represents good news for women, but from an etiological as well as a pub- lic health point of view, the most relevant infor- mation derives from increases in incidence rates.
ETIOLOGICAL EPIDEMIOLOGY
The search for risk and, more recently, preven- tive factors for breast cancer is the raison dztre of epidemiological research, especially when the aim is prevention. The so-called recognized risk
factors belong to several domains: genetics, re- productive and hormonal life, diet, physical ex- ercise, and a few selected specific exposures. Yet, much is still unknown and the proportion of breast cancers that cannot be readily explained by the risk factors just listed most probably ex- ceeds the ones that can. The present review does not aim to be exhaustive and fully comprehen- sive, or to present in detail domains currently well known and accepted by all. On the con- trary, it modestly wishes to highlight potentially controversial conditions which could in the fu- ture be recognized as new risk factors. There- fore, the space devoted to each group of items is not proportional to their quantitative import- ance in terms of relative or attributable risk, but rather to our current ignorance and the ques- tions that must be asked if we want to progress.
Genetics and family history The most notable discoveries of the last 20
years regarding the etiology of breast cancer concern genetics. The roles of BRCAl and BRCA2 in the etiology of the disease are now much better understood and quantified. These gene mutations are only responsible for a tiny fraction of all breast cancers, much less than 10% overall, but they do confer on the women affected a considerable life-time risk, estimated most often at between 50 and 80% compared to the general population with a risk of under 10% (16, 17). Other mutations of greater public health, as compared to clinical, interest are likely to be found in the coming years, possibly through elucidation of the etiological roles of other genetic conditions, in particular heterozy- gotic states of more common conditions, such as ataxia telangiectasia. Well before the genetics
S 83

SASCO
of breast cancer was known, familial risk was already recognized, with many syndromes having been described, of breast cancers alone, breast and ovarian cancers associated, or also other malignancies (1 8).
Reproductive life For almost half a century now and even
longer if we refer to the pioneering work of Lane-Claypon (19), events of reproductive life have repeatedly been considered as risk factors for breast cancer in women. Cancer of the breast occurs more frequently among women who had an early menarche, remain nulliparous, or even if parous have few children with a late age at first and possibly subsequent births. In- fertility per se appears as a risk factor for breast cancer, as possibly does lack of breastfeeding. Finally, a late age at menopause increases the risk of breast cancer.
The first modern epidemiological studies on this topic were mostly done in the 1970s with the help of hormone determinations. Recent studies in general still confirm the effects of age at menarche or pregnancy history (20). The uni- fying hypothesis behind the effects on breast cancer risk of reproductive events relates to hor- monal influences, in particular estrogens. Their role is crucial not only in cancer initiation and promotion (21), but could also possibly be used for prevention (22). Hormones and reproductive life closely interact not only in the occurrence of disease but also in the development of the mammary gland and the susceptibility to car- cinogenesis (23).
Lifestyle The most important element to consider
under this heading is diet. High intake of fruits and vegetables is probably associated with a slightly reduced risk of breast cancer. In con- trast, there is convincing evidence that rapid growth and greater adult height, reflecting in part the total food intake in early years, are as- sociated with an increased risk (24). Similarly, a high body mass, also linked to a high total ca- loric intake, or at least an intake not counter- balanced by caloric expenditure, is a risk factor for postmenopausal breast cancer. Total fat as well as saturated animal fat possibly increases the risk (25). Similar conclusions have been reached by the UK Department of Health (26).
S 84
Of particular interest, also in the context of what follows, is an evaluation of the impact of meat consumption on cancer occurrence. Meat consumption is possibly associated with an in- creased risk of breast cancer. This statement is based on the fact that three out of eight pros- pective studies reported an increased risk of breast cancer with higher meat intake. A meta- analysis of seven cohort and case-control studies found a relative risk of 1.5, later con- b m e d in several other case-control studies not included in this combined analysis. Red meat was more frequently cited as a risk factor and, in fact, diets rich in poultry possibly had no links with breast cancer risk (25). A further re- view published one year later shows even clearer trends. Out of 20 case-control studies carried out in countries with different meat consump- tion levels, 17 observed higher risks associated with higher total meat, red meat or processed meat intake, although only 11 studies were stat- istically significant. One study found a nonstat- istically significant reduced risk associated with higher meat consumption, one found no associ- ation, and all others had increased relative risks ranging from 1.1 to 3.5. Among 10 cohort studies, one found no association and the other 9 had estimates above one but statistically sig- nificant in only 5 . Values of relative risks ranged from 1.2 to 2.4. In four cohort studies, a grad- ing effect associated with the number of meat servings per week was described. The con- clusion of that review was that there is consider- able and consistent evidence that higher meat consumption, particularly red or fried/browned meat, is associated with a higher risk of breast cancer (24). Although the role of N-acetyltrans- ferase genetic polymorphisms was considered to mediate the risk of breast cancer in relation to meat consumption, this was not supported by the results of a traditional case-control study (27) nor of a nested case-control study (28).
Alcohol consumption has been shown to be associated with breast cancer risk. Based on a 1997 review, 11 cohort and 36 case-control studies have examined this issue. Evidence shows an increased risk of breast cancer for consumption of alcohol and alcoholic drinks (29). In a meta-analysis of 38 studies, a dose- response was found related to number of drinks per day, including consumption in the low range (30).

EPIDEMIOLOGY OF BREAST CANCER
In contrast with alcohol, the evidence on smoking and breast cancer remains somewhat inconclusive. For a long time, tobacco was view- ed as an anti-estrogen and thereby a protective factor against breast cancer (31). Smokers on average reach menopause some 2 years earlier than nonsmokers and early menopause is as- sociated with reduced risk of breast cancer. More recent studies, in contrast, have incrimi- nated passive smoking as a risk factor for breast cancer (32) and thereby rekindled interest in the subject of smoking and breast cancer. Smoking tobacco may indeed turn out to be a risk factor, but the effect will be dependent on N-acetyl transferase 2 genetic polymorphisms (33). De- spite studies in genetically predisposed women which found a reduced risk of breast cancer among smokers (34), methodological limi- tations precluding the distinction of factors af- fecting survival rather than occurrence should make us cautious with regard to reaching de- finitive conclusions.
Physical activity has been the subject of a thorough review with respect to its effect on breast cancer. Out of a total of 21 studies then available, 15 suggested a reduced risk of breast cancer associated with physical activity, with a greater effect for women who are slim, parous and premenopausal. Four studies did not find an association and two found an increased risk (35). The relationship seems clearer for occu- pational activity than for leisure-time or nonoc- cupational activity (36). A recent study did not find that specific periods had a greater impact on recreational physical activity (37), whereas one would have been led to suspect a preferen- tial effect of peripubertal activity linked to breast susceptibility (23).
Exposure to specijic agents: physical, chemical, biological and others
Only limited data are available on specific ex- posures in relation to breast cancer. The best known and studied refer to radiation. Long- term follow-up of women exposed to the Hiro- shima or Nagasaki nuclear explosions indicates an increased risk of breast cancer, in particular for women having been exposed around pu- berty, at the time of breast development (38). Similarly, exposure as a result of treatment and surveillance of tuberculosis, is associated with risk (39). More recently, exposure to electro-
magnetic fields has been evaluated. Occu- pational cancer mortality for cancers of the breast, as well as other hormone-related cancers in women, has been found elevated in women employed in the telephone industry (40). Risks may be higher in premenopausal rather than postmenopausal women (41). Even residential exposure has been incriminated in a Swedish study, with very high risk for premenopausal, estrogen-positive tumors (42).
Specific exposures to chemicals have been evaluated in studies of mortality. Suggestive as- sociations were found for styrene, several or- ganic solvents, such as methylene chloride, car- bon tetrachloride, formaldehyde, as well as for several metals, metal oxides and acid mists (43). These data contrast somewhat with the long held view that risk of breast cancer was mostly a social class phenomenon, with higher risk for executives, administrative and clerical workers (44). Systematic reviews on occupation and breast cancer are still few (45) and much work remains to be done. This also applies to as yet to be conducted studies to evaluate the potential impact of unemployment or other sources of stress.
Based on animal experience, a viral hypoth- esis has been put forward. In mice, a retrovirus, the murine mammary tumor virus, is a recog- nized cause of mammary tumors, transmitted with milk from mother to daughters. Exposure in humans is known to occur, yet no evaluation of risk has ever been carried out (46). Another viral candidate is the Epstein-Barr virus, al- though data from the USA are not particularly supportive (47). This would be better studied in populations where inflammatory breast cancer is frequent, for example in North Africa. Other potential viral candidates remain to be investi- gated.
Hormones and endocrine disrupters Since the 1960s, numerous studies have been
conducted on the influence of hormones on breast cancer risk. Estrogens, female hormones par excellence, have been measured in various body fluids, urine, blood, and more recently breast tissue, either tumorous or in the vicinity of tumors. Estrogens in the body exist in several forms, estradiol, estrone and estriol being the three main ones. Differences in levels of these hormones exist from country to country and
S 85

SASCO
have been linked to different risks of breast can- cer. Women with high levels of estrogens, in par- ticular free estrogens, not linked to the sex-hor- mone-binding globulin, have long been recog- nized as being at a high risk of cancer development (48). This demonstrates that even in the absence of exogenous hormones, risk of cancer is influenced by the endogenous hor- monal milieu. In fact, future cancer risk is in part also determined by conditions of exposure in utero. The preventive effect of gravidic toxe- mia is recognized (49) and since the 1950s studies have incriminated high birth weight as a risk factor for cancer and in particular for breast cancer (50). Similarly, a very recent study concluded that, among twins, the risk of breast cancer may be affected by the type of twinning (dizygotic versus monozygotic) and sex of the dizygotic twin (51).
Exogenous hormones have been evaluated for carcinogenicity in humans using the IARC Monographs programme, for some of them sev- eral times and most recently in 1999 (52-55).
More than 10 cohort and 50 case-control studies have assessed the relationship between use of combined oral contraceptives and risk of breast cancer. The evidence suggests a small in- crease in the relative risk of breast cancer espe- cially among current and recent users, which is, however, unrelated to duration of use and type or dose of preparation, and may be partly linked to detection bias (55). Data on injectable progestogen-only contraceptives come from two case-control studies and a pooled analysis of original data. Relative risks vary between 1.0 and 1.3, and are not statistically significant (55).
In contrast, information on the relationship between postmenopausal estrogen therapy and risk of breast cancer is available from many epi- demiological studies. A pooled analysis of the original data from 51 of these studies and a re- view of data from 15 cohort and 23 case-control studies showed that in the majority of the studies there is a small increase in risk with longer duration of use in current and recent users (55). Separate information on the effects of use of postmenopausal estrogen-progestogen therapy was provided in only a minority of the studies on the risk of breast cancer. The results of nine cohort and five case-control studies that did include such information and the findings of a pooled analysis of the original data from
S 86
these and other studies indicate that the in- creased relative risk observed with long-term use of postmenopausal estrogen-progestogen therapy is not materially different from that for long-term use of estrogens alone (55) .
If evidence for other cancer sites, in addition to the breast is also considered, as well as evi- dence from experimental animals, several hor- monal compounds belong to categories of car- cinogens for humans. In group 1 (carcinogenic to humans), one finds diethylstilbestrol(53, 54), postmenopausal estrogen therapy ( 5 9 , nonster- oidal estrogens (53, 54), steroidal estrogens (53, 54), combined oral contraceptives ( 5 9 , sequen- tial oral contraceptives (53, 54) and tamoxifen (56). In group 2A (probably carcinogenic to humans), one finds androgenic anabolic steroids (54). In group 2B (possibly carcinogenic to humans) , we have medr ox yproges terone acetate (53, 54), progestins (53, 54), postmenopausal es- trogen-progestogen therapy (55) , progestin - only oral contraceptives (55). Finally, in group 3 (not classifiable as to carcinogenicity to humans), one finds clomiphene citrate (53, 54), estradiol mustard (52), toremifene (56) and dro- loxifene (56).
Some data implicate a polymorphism in cat- echol-o-methyl transferase (COMT) in breast cancer risk. Methylation by COMT is an im- portant pathway for inactivation of catechol es- trogens. The allele encoding low-activity COMT may be a contributor in particular to post- menopausal breast cancer (57), although this was not confirmed by another study (58). In fact, menopausal status, as well as weight, may modify this association (59). Even physical exer- cise and training have an impact on 4-hydroxy catechol estrogen metabolism (60).
The knowledge currently available on the car- cinogenicity of hormones as well as on the im- pact in various disease risks of small variations, remaining within the physiological range, as may occur in utero or at other susceptible life periods, helps us provide answers to exceedingly difficult questions, such as for example the po- tential impact on human health of hormone residues in bovine meat and meat products, re- sulting from the use in beef, as growth pro- moters, of natural hormones (17p estradiol, tes- tosterone, progesterone) or synthetic com- pounds (zeranol, trembolone acetate, melengestrol acetate). Of course, no study is

EPIDEMIOLOGY OF BREAST CANCER
available, nor more importantly is ever likely to be available, where two strictly identical popula- tions are compared, one consuming meat from hormone-treated animals and the other con- suming exactly the same types and quantities of similarly prepared and cooked meat but from animals not having been treated with hormones for growth-promotion purposes, the allocation between the two groups being decided by ran- domization. Therefore, we can only rely on in- direct evidence. From an etiological point of view, we can also rely on studies conducted on vegetarian populations. The overall cancer risk and, in particular, breast cancer risk is generally lower among non-meat eaters. The evidence is more marked in North America than in Europe (25, 29). Finally, better knowledge of the hor- mone receptors, a and p, with more accurate information on their functions would also be helpful. Genotoxic effects, independent of the hormonal receptors, have been recognized for metabolites of the parent compounds. These essentially concern catechol estrogens and cor- responding quinones, in particular 4-hy- droxylated derivatives (61). An international symposium on “Estrogens as endogenous car- cinogens in breast and prostate” was recently re- ported in Monograph 27 of the Journal of the National Cancer Institute (62). Papers demon- strating the developmental basis of breast can- cer (63) are of specific relevance, as well as the carcinogenic role of oxidative metabolites of es- trogens (64), the possibility of obtaining DNA adducts and mutations (65), the recognition of the huge variability in tissue-specific synthesis and oxidative metabolism (66), the role of con- jugation (67) and genetic polymorphisms (68), and finally the role of estrogen-receptor-me- diated processes (69). All this points towards the possibility of the coexistence of several path- ways in the development of the breast and later on breast cancer, involving both hormonal en- docrine events and genotoxicity.
Over the last 10 years, there has been increas- ing concern regarding the potential risks linked to exposures, not only to hormones, but to arti- ficial products, mimicking hormonal activities. This has led to the concept of xenohormones, largely represented so far by xenoestrogens. The exact role they play is still unknown. Most of the epidemiological studies available so far deal with various pesticides, essentially organochlor-
ides, which remain in the environment for a long period of time and the residues of which may be found in adipose tissues of various spe- cies, including humans (70). Old studies, mostly dealing with polychlorinated biphenyls (PCBs) and dichlorodiphenyldichloroethylene (DDE), found higher levels in cancer cases compared to controls (71), as did a nested case-control study which looked at estrogen-receptor-positive cases (72). Yet other studies were negative, in particu- lar for specific population groups, such as Asian women in the USA (73). Three studies even found that levels of organochloride residues were lower among cases than among controls (7676). One of these studies was conducted in Mexico, a country where DDT was still in use (74). Specific products may carry a higher risk than others (77). Such could be the case for diel- drin (78), which could also play a role not only for occurrence of cancer but also for survival (79). Yet, exact quantification of the risk re- mains to be done on a larger scale. For the time being, many consider these links as speculative and unfounded (80) or as markers of suscepti- bility (81). Similarly, studies on the role of phta- lates and other contaminants in plastics remain to be done, at least in epidemiological terms.
A note on risk versus vulnerability factors The major problem when discussing effects of
exposure to low levels of hormones is that many questions remain unanswered regarding the identification of all metabolites, mechanisms of action, and knowledge of all effects. Whether hormones are true “causes” of cancer or crucial agents in the causal pathway is not known. Yet, we may wonder from the point of view of pre- vention how relevant this is. If one excludes radiation and inherited mutations which can easily be seen as direct carcinogens for the breast, all the other so-called risk factors re- garding, in particular, reproductive life may better be considered as vulnerability factors. Having an early menarche, a late menopause, or no pregnancy will render the woman more susceptible to other potential contributing fac- tors, such as alcohol or exogenous hormones and possibly xenoestrogens (82).
The other important aspect is that besides de- fining individual susceptibility in terms of gen- etic background, metabolic profile and sex, there is a crucial need to better define time win-
S 87

SASCO
dows of exposure. Vulnerability periods corre- spond to in utero life, as well as prepubertal period both for girls and boys. In women, per- imenopause may also be particularly relevant.
CONCLUSION
Only a small proportion of all breast cancers can currently be explained by traditional risk factors, leaving most of the recent and world- wide increases in incidence unsolved. Given the crucial role of the hormonal pathway in the oc- currence and development of tumors, better knowledge of the determinants of endocrine events such as puberty and fertility is needed. Too much is still unknown and yet too little is studied with respect to the etiology of breast cancer, in particular premenopausal disease. We need to assess the impact of continuous, low- level, yet cumulative exposures over a lifetime. In the mean time, the precautionary principle (83) should, whenever possible, be enacted to prevent unnecessary exposures, notably at spe- cific periods of vulnerability.
REFERENCES
1. World Health Organization. Annex. Table 3. Deaths by cause, sex and mortality stratum in WHO regions, estimates for 1999. In: The World Health Report 2000. Health systems: improving performance. Geneva: World Health Organiza- tion, 2000:1669.
2. World Health Organization. Annex. Table 2. Mortality by sex, cause and WHO region, esti- mates for 1998. In: The World Health Report 1999. Making a difference. Geneva: World Health Organization, 1999:98-9.
3. World Health Organization. Cancer. In: The World Health Report. Life in the 21st century. A vision for all. Geneva: World Health Organiza- tion, 1998:88-90.
4. Ferlay J, Bray I, Pisani P, Parkin DM. Globocan 2000. Cancer incidence, mortality and prevalence worldwide. Lyon: IARC Press, 2001.
5. Parkin DM, Whelan SL, Ferlay J, Raymond L, Young J, editors. Breast cancer. In: Cancer inci- dence in five continents. Vol VII. IARC Scientific Publication No. 143. Lyon: International Agency for Research on Cancer, 1997:858-9.
6. Sasco AJ. Migrations et cancers. Rev Med Int
7. Parkin DM, Laara E, Muir CS. Estimates of the 1989; 10:341-8.
S 88
worldwide frequency of sixteen major cancers in 1980. Int J Cancer 1988;41:184-97.
8. Parkin DM, Pisani P, Ferlay J. Estimates of the worldwide incidence of eighteen major cancers in 1985. Int J Cancer 1993;54:594-606.
9. Parkin DM, Pisani P, Ferlay J. Estimates of the worldwide incidence of 25 major cancers in 1990. Int J Cancer 1999;80:82741.
10. Waterhouse J, Muir CS, Shanmugaratnam K, Powell J, editors. Breast cancer. In: Cancer inci- dence in five continents. Vol. IY IARC Scientific Publication No. 42. Lyon: International Agency for Research on Cancer, 1982:73&5.
11. Dime GE, Umbach DM, Sasco AJ, Hoe1 DG, Davis DL. Unexplained increases in cancer inci- dence in the United States from 1975 to 1994: possible sentinel health indicators? Annu Rev Public Health 1999;20:173-209.
12. Pet0 R, Boreham J, Clarke M, Davies C, Beral Y UK and USA breast cancer deaths down 25% in year 2000 at ages 20-69 years. Lancet 2000; 355:1822.
13. Menegoz F, Cherie-Challine L. Cancer du sein. In: Le cancer en France: incidence et mortalitt. Situation en 1995. Evolution entre 1975 et 1995. Paris: La documentation franGaise, 1998:7&8 1.
14. Berrino F, Sant M, Verdecchia A, Capocaccia R, Hakulinen T, Esteve J , editors. Breast. In: Sur- vival of cancer patients in Europe. The Eurocare study. IARC Scientific Publication No. 132. Lyon: International Agency for Research on Cancer, 199525345.
15. Berrino F, Capoccia R, Esttve J, Gatta G, Haku- linen T, Micheli A, et al. Breast. In: Survival of cancer patients in Europe: the Eurocare-2 study. IARC Scientific Publication No. 15 1. Lyon: In- ternational Agency for Research on Cancer, 1999:30&13.
16. Easton D, Narod S, Ford, D, Steel M. The gen- etic epidemiology of BRCAl . Breast Cancer Linkage Consortium. Lancet 1994;344:761.
17. Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J, et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995;
18. Sobol H, Stoppa-Lyonnet D. Predisposition gtnetique aux cancers du sein et de l’ovaire: gen- tralites et aspects cliniques. In: Institut National de la Santt et de la Recherche Mtdicale. Risques hereditaires de cancers du sein et de l’ovaire. Quelle prise en charge? Paris: INSERM, 1998:
19. Lane-Claypon JE. A further report on cancer of the breast with special reference to its associated antecedent conditions. In: Report on public health and medical subjects No. 32. Ministry of Health, London, 1926:l-189.
20. Magnusson CM, Persson IR, Baron JA, Ekbom A, Bergstrom R, Adami HO. The role of repro-
3781789-92.
81-91.

EPIDEMIOLOGY OF BREAST CANCER
ductive factors and use of oral contraceptives in the aetiology of breast cancer in women aged 50 to 74 years. Int J Cancer 1999;80:231-6.
21. Russo IH, Russo J. Role of hormones in mam- mary cancer initiation and progression. J Mam- mary Gland Biol Neoplasia 1998;3:49-61.
22. Russo IH, Russo J. Hormonal approaches to breast cancer prevention. J Cell Biochem 2000;
23. Russo J, Russo IH. Cellular basis of breast can- cer susceptibility. Oncol Res 1999;ll: 169-78.
24. Department of Health. Energy balance, obesity and the development of cancer. Breast cancer. In: Report on health and social subjects No. 48. Nu- tritional aspects of the development of cancer. Norwich: The Stationary Office, 1998: 154-60.
25. World Cancer Research Fund in association with American Institute for Cancer Research. Breast. In: Food, nutrition and the prevention of cancer: a global perspective. Washington: American In- stitute for Cancer Research, 1997:252-87.
26. Department of Health. Epidemiology of diet in relation to specific cancers. Breast cancer. In: Re- port on health and social subjects No. 48. Nu- tritional aspects of the development of cancer. Norwich: The Stationary Office, 1998:8 1-94.
27. Ambrosone CB, Freudenheim JL, Sinha R, Gra- ham R, Marshall JR, Vena JE, et al. Breast can- cer risk, meat consumption and N-acetyltransfer- ase (NAT2) genetic polymorphisms. Int J Cancer 1998;75:825-30.
28. Gertig DM, Hankinson SE, Hough H, Spiegel- man D, Colditz GA, Willett WC, et al. N-acetyl transferase 2 genotypes, meat intake and breast cancer risk. Int J Cancer 1999;80:13-7.
29. World Cancer Research Fund in association with American Institute for Cancer Research. Alco- hol. In: Food, nutrition and the prevention of cancer: a global perspective. Washington: Ameri- can Institute for Cancer Research, 1997:403.
30. Longnecker MI? Alcoholic beverage consump- tion in relation to risk of breast cancer: meta- analysis and review. Cancer Causes Control 1994;
3 1. Baron JA. Smoking and estrogen-related disease. Am J Epidemiol 1984: 1 19:9-22.
32. Morabia A, Bernstein AM, Heritier S, Khatch- atrian N. Relation of breast cancer with passive and active exposure to tobacco smoke. Am J Epi- demiol 1996;143:918-28.
33. Welp EA, Weiderpass E, Boffetta P, Vainio H, Vasama-Neuvonen K, Petralia S, et al. Environ- mental risk factors of breast cancer. Scand J Work Environ Health 1998;24:3-7.
34. Brunet JS, Ghadirian P, Rebbeck TR, Lerman C, Garber JE, Tonin PN, et al. Effect of smoking on breast cancer in carriers of mutant BRCAl or BRCA2 genes. J Natl Cancer Inst 1998;90:761-6.
35. Friedenreich CM, Thune I, Brinton LA, Albanes
Suppl341-6.
5~73-82.
D. Epidemiologic issues related to the association between physical activity and breast cancer. Can- cer 1998;83 Suppl:600-10.
36. Kramer MM, Wells CL. Does physical activity reduce risk of estrogen-dependent cancer in women? Med Sci Sports Exerc 1996;28:322-34.
37. Verloop J, Rookus MA, van der Kooy K, van Leeuwen FE. Physical activity and breast cancer risk in women aged 20-54 years. J Natl Cancer Inst 2000;92: 128-35.
38. Tokunaga M, Land CE, Yamamoto T, Asano M, Tokuoka S, Ezaki H, et al. Incidence of female breast cancer among atomic bomb survivors, Hi- roshima and Nagasaki, 1950-1980. Radiat Res
39. Boice JD Jr, Preston D, Davis FG, Monson RR. Frequent chest X-ray fluoroscopy and breast cancer incidence among tuberculosis patients in Massachusetts. Radiat Res 199 1 ;125:2 14-22.
40. Dosemeci M, Blair A. Occupational cancer mor- tality among women employed in the telephone industry. J Occup Med 1994;36:1204-9.
41. Coogan PF, Clapp RW, Newcomb PA, Wenzl TB, Bogdan G, Mittendorf R, et al. Occupational ex- posure to 60-hertz magnetic fields and risk of breast cancer in women. Epidemiology 1996;7: 459-64.
42. Feychting M, ForssCn U, Rutqvist LE, Ahlbom A. Magnetic fields and breast cancer in Swedish adults residing near high-voltage power lines. Epidemiology 1998;9:392-7.
43. Cantor Kp, Stewart PA. Brinton LA, Dosemeci M. Occupational exposures and female breast cancer mortality in the United States. J Occup Environ Med 1995;37:33&48.
44. Calle EE, Murphy TK, Rodriguez C, Thun MJ, Heath CW Occupation and breast cancer mor- tality in a prospective cohort of US women. Am J Epidemiol 1998;148:191-7.
45. Goldberg MS, Labrkche E Occupational risk factors for female breast cancer. Occup Environ Med 1996;53:145-56.
46. Dion AS, Girandi AJ, Williams CC, Pomenti AA. Serologic responses to murine mammary tu- mor virus (MuMTV) in MuMTV-exposed lab- oratory personnel. J Natl Cancer Inst 1986;76:
47. Glaser SL, Ambinder RF, Di Guisseppe JA, Horn-Ross PL, Hsu JL. Absence of Epstein-Barr virus EBER- 1 transcripts in an epidemiologically diverse group of breast cancers. Int J Cancer
48. Henderson BE, Ross R, Bernstein L. Estrogens as a cause of human cancer: the Richard and Hinda Rosenthal Foundation award lecture. Cancer Res 1988; 48:24&53.
49. Innes KE, Byers TE. Preeclampsia and breast cancer risk. Epidemiology 1999; 10:722-32.
50. Michels KB, Trichopoulos D, Robins JM, Rosn-
1987;112:243-72.
61 1-9.
1998;75:555-8.
S 89

SASCO
er BA, Manson JE, Hunter DJ, et al. Birth weight as a risk factor for breast cancer. Lancet 1996;348: 15426.
51. Cerhan R, Kushi LH, Olson JE, Rich SS, Zheng W, Folsom AR, et al. Twinship and risk of post- menopausal breast cancer. J Natl Cancer Inst
52. International Agency for Research on Cancer. IARC Monographs on the evaluation of carcino- genic risk of chemicals to man. Volume 9. Some aziridines, N-S and 0-mustards and selenium. Lyon: International Agency for Research on Cancer, 1975:268 pp.
53. International Agency for Research on Cancer. IARC Monographs on the evaluation of carcino- genic risk of chemicals to humans. Volume 21. Sex hormones (11). Lyon: International Agency for Research on Cancer, 1979583 pp.
54. International Agency for Research on Cancer. Overall evaluations of carcinogenicity: an updat- ing of LARC Monographs Volumes 1 to 42. Supplement No 7. Lyon: International Agency for Research on Cancer, 1987:440 pp.
55. International Agency for Research on Cancer. IARC Monographs on the evaluation of carcino- genic risk of chemicals to humans. Volume 72. Some hormones, postmenopausal hormone ther- apy, and hormonal contraception. Lyon: Interna- tional Agency for Research on Cancer, 1999:660 PP.
56. International Agency for Research on Cancer. IARC Monographs on the evaluation of carcino- genic risk of chemicals to humans. Volume 66. Some pharmaceutical drugs. International Agency for Research on Cancer, Lyon, 1996:514 PP.
57. Lavigne JA, Helzlsouer KJ, Huang HY, Strick- land PT, Bell DA, Selmin 0, et al. An associ- ation between the allele coding for a low activ- ity variant of catechol-0-methyltransferase and the risk for breast cancer. Cancer Res
58. Millikan RC, Pittman GS, Tse CK, Duel1 E, Newman B, Savitz D, et al. Catechol-O-methyl- transferase and breast cancer risk. Carcino- genesis 1998;19: 1943-7.
59. Thompson PA, Shields PG, Freudenheim JL, Stone A, Vena JE, Marshall JR, et al. Genetic polymorphisms in catechol-0-methyltransferase, menopausal status, and breast cancer risk. Can- cer Res 1998;58:2107-10.
60. De Cree C, Van Kranenburg G, Geurten P, Fuji- mori Y, Keizer HA. 4-hydroxycatecholestrogen metabolism responses to exercise and training: menstrual cycle irregularities and breast cancer. Fertil Steril 1997;67:505-16.
61. Service RE New role for estrogen in cancer? Science 1998;279: 1631-3.
62. Estrogens as endogenous carcinogens in the
s 90
2000;92:261-5.
1997;57:5493-7.
breast and prostate. J Natl Cancer Inst Monogr
63. Russo J, Hu YF, Yang X, Russo IH. Develop- mental, cellular and molecular basis of human breast cancer. J Natl Cancer Inst Monogr 2000;
64. Yager JD. Endogenous estrogens as carcinogens through metabolic activation. J Natl Cancer Inst Monogr 2000;27:67-73.
65. Cavalieri E, Frenkel K, Liehr JG, Rogan E, Roy D. Estrogens as endogenous genotoxic agents - DNA adducts and mutations. J Natl Cancer Inst Monogr 2000;27:75-93.
66. Jefcoate CR, Liehr JG, Santen RJ, Sutter TR, Yager JD, Yue W, et al. Tissue-specific synthesis and oxidative metabolism of estrogens. J Natl Cancer Inst Monogr 2000;27:95-112.
67. Raftogianis R, Creveling C, Weinshilboum R, Weisz J. Estrogen metabolism by conjugation. J Natl Cancer Inst Monogr 2000;27: 1 13-24.
68. Thompson PA, Ambrosone C. Molecular epi- demiology of genetic polymorphisms in estrogen metabolizing enzymes in human breast cancer. J Natl Cancer Inst Monogr 2000;27:125-34.
69. Dickson RB, Stance1 GM. Estrogen-receptor me- diated processes in normal and cancer cells. J Natl Cancer Inst Monogr 2000;27: 13545.
70. Davis DL, Bradlow HL, Wolff M, Woodruff T, Hoe1 DG, Anton-Culver H. Medical hypothesis: xenoestrogens as preventable causes of breast can- cer. Environ Health Perspect 1993;101:372-7.
71. Wolff M, Toniolo PG, Lee EW, Rivera M, Dubin N. Blood levels of organochlorine residues and risk of breast cancer. J Natl Cancer Inst 1993;85:
72. Dewailly MS, Dodin S, Verrault R, Ayotte P, Sauve L, Morin J, et al. High organochloride body burden in women with estrogen-receptor positive breast cancer. J Natl Cancer Inst 1994; 86:232-4.
73. Krieger N, Wolff MS, Hiatt RA, Rivera M, Vog- elman J, Orentreich N. Breast cancer and serum organochlorines: a prospective study among white, black and Asian women. J Natl Cancer Inst 1994;86:589-99.
74. Lopez-Carrillo L, Blair A, Lopez-Cervantes M, Cebrian M, Rueda C, Reyes R, et al. Dichlorodi- phenyl trichloroethane serum levels and breast cancer risk: a case-control study from Mexico. Cancer Res 1997;57:3728-32.
75. Hunter DJ, Hankinson SE, Laden F, Colditz GA, Manson JE, Willett WC, et al. Plasma or- ganochlorine levels and the risk of breast cancer. N Engl J Med 1997;377:1253-8.
76. van’t Veer P, Lobbezoo IE, Martin-Moreno JM, Guallar E, Gomez-Aracena J, Kardinaal AF, et al. DDT (dicophane) and post-menopausal breast cancer in Europe: case-control study. BMJ
2000;27: 1-1 59.
27:17-37.
648-52.
1997;3 1518 1-5.

EPIDEMIOLOGY OF BREAST CANCER
77. Aronson KJ, Miller AB, Woolcott CG, Sterns EE, McCready DR, Lickley LA, et al. Breast adi- pose tissue concentrations of polychlorinated bi- phenyls and other organochlorines and breast cancer risk. Cancer Epid Biomarkers Prev 2000;9:5 543 .
78. Hsyer AP, Grandjean P, Jsrgensen T, Brock Jw, Hartvig HB. Organochlorine exposure and risk of breast cancer. Lancet 1998;352: 18 1 G20.
79. Hsyer AP, Jsrgensen T, Bruck Jw, Grandjean I? Organochlorine exposure and breast cancer sur- vival. J Clin Epidemiol 2000;53:323-30.
80. Safe SH. Xenoestrogens and breast cancer. N Engl J Med 337: 13034
8 1. Musgrave MA, Aronson KJ, Narod S , Hanna W, Miller AB, McCready DR. Breast cancer and or- ganochlorines: a marker for susceptibility? Surg Oncol 1998;7:14.
82. Davis DL, Axelrod D, Bailey L, Gaynor M, Sas- co AJ. Rethinking breast cancer risk and the en- vironment: the case for the precautionary prin- ciple. Environ Health Perspect 1998; 106523-9.
83. Horton R. The new new public health of risk and radical engagement. Lancet 1998;352:25 1-2.
DISCUSSION
Elsebeth Lynge (Copenhagen, Denmark) What is known about the interaction between genes and the environment in women known to be carriers of BRCAl or 2?
Annie Susco (Lyon, France) Colleagues at the International Agency for Research on Cancer are studying that aspect of interaction of gene and environment at present. There are other large studies looking at the populations of women carrying BRCA 1 or BRCA 2, including EORTC studies. The influence of taking exoge- nous oestrogens, of physical exercise and of diet in changing the risk of developing breast cancer will be assessed among these women who are starting with a very high background incidence. We do not have a comprehensive picture in a large population because many countries will need to be involved in recruiting a sufficiently large cohort for analysis. There is one contro- versial result concerning BRCA l women and smoking in which there was a reduced incidence of breast cancer amongst smokers in that speci- fic population, but there are criticisms about the design of that study. The study group was limited to survivors of breast cancer and that may have introduced bias because incident cases were not used as a starting point.
Jose Russo (Philadelphia, USA) It was en- couraging to hear that you emphasise the im- portance of puberty as a susceptible window for environmental exposure. Do you recommend any interventional measures that could apply to pubertal girls in an attempt to protect them from developing breast cancer?
Annie Susco At the present time, given our
state of knowledge, we can only recommend general health promotion such as avoiding obesity and taking much physical activity. This can be achieved by consuming an adequate diet to maintain a good energy balance. Avoiding obesity will prevent early puberty except in pathological conditions, and late puberty re- duces the risk of breast cancer. In my opinion, delaying puberty in girls by drug therapy or hormonal manipulation should be avoided be- cause we do not know the longterm conse- quences.
Sabine de Muinck Keizer-Schrama (Rotter- dam, The Netherlands) What is the biological explanation for the increase in breast cancer re- lating to alcohol consumption even at low levels?
Annie Sasco A dose-response effect has been seen in a meta-analysis indicating higher risk due to higher dose of alcohol (Longnecker, Cancer Causes Control 1994;5:73-82). This may be due to the impact of alcohol on the liver, and its effect on changing metabolism, which may have consequences on the hormonal pathways, perhaps by enhancing oestrogens. We also know that alcohol itself has a carcinogenic effect in humans, but usually at much higher doses than is seen for breast cancer. We often hear that low levels of alcohol are good for our health, espe- cially in the cardiovascular system, but there is less beneficial cardiovascular effect in women than in men, and women have the added risk of breast cancer. Perhaps we should not be pro- moting even moderate amounts of alcohol in women.
S91

SASCO
Manolis Kogevinas (Barcelona, Spain) There are a few studies comparing women with breast cancer in low incidence countries and high inci- dence countries, and there is a difference in the distribution of oestrogen receptor (ER) and progesterone receptor positive tumours. In the USA, there are a higher proportion of ER +ve cases. Is receptor positivity related to the aeti- ology?
Annie Sasco I do not know of any study which has assessed ER status world wide, and we know very little on the aetiology of breast
cancer in Africa. The incidence of breast cancer among young women is not negligible in North Africa. These women tend to have many children at an early age, which should be protec- tive according to data from Western countries. The North African incidence may be associated with a virus such as the Epstein Barr Virus (EBV), which is in keeping with animal models of the murine mammary tumour viruses. The African tumour is more frequently an inflam- matory type of breast cancer, which suggests differences from Western Countries.
S 92