Embed Size (px)
Citation preview

Eosinophilic Esophagitis: An Allergy Perspective
Daniel DeMerell, MD

Eosinophilic Esophagitis: An Allergy Perspective
• Disclosure- none

Eosinophilic Esophagitis (EoE): An Overview
• Definition of EoE• Epidemiology of EoE• Etiology of EoE• Role of allergies in EoE• Diagnosis of EoE• Treatment of EoE• Prognosis of EoE

Eosinophilic Esophagitis (EoE)
• First described as distinct entity related to foods in 1995 in 10 children with esophageal eosinophilia, refractory to acid suppression who then responded to elemental diet (Kelley et al.)
• 2007 expert panel released consensus recommendations for EoE in children and adults (Furuta GT et al.).– Presence of clinical symptoms related to esophageal dysfunction– Isolated esophageal eosinophilia
• >15 eos/hpf
– Absence of other causes of esophageal eosinophilia (especially GERD)
• Normal pH monitoring study of distal esophagus • Lack of response to high-dose PPI

Eosinophilic Esophagitis:2011 Updated Definition
• In 2011, expert panel updated consensus recommendation for children and adults
• “Eosinophilic esophagitis represents a chronic, immune/antigen mediated esophageal disease characterized clinically by symptoms related to esophageal dysfunction and histologically by eosinophil-predominant inflammation”
• Infiltration of eosinophils not affecting other areas of GI tract
Liacouras CA et al. J Allergy Clin Immunol 2011

Eosinophilic Esophagitis
• Definition is limited because mechanism(s) of EoE still not fully understood
• Challenging to design and compare studies • Diagnosis and treatment is evolving as we
learn about the mechanisms


Epidemiology of EoE
• Prevalence and incidence of EoE increasing – Prevalence of EoE ranges from 6-60 cases per 100,000 (Dohil R
et al., Prasad GA et al.- Olmstead County, MN)
– Therefore prevalence of EoE likely comparable to that of IBD, but less than that of celiac disease (Rothenberg et al 2009 )
– Not clear how much is also related to increase in endoscopy• Males: females 3:1 (genetic variant of the TSLP receptor
on the X-chromosome in males?)• Seen in all ages• More commonly diagnosed in urban and suburban areas
than rural (Spergel JM et al 2011)

Epidemiology of EoE
• Veerappan et al- found EoE in 6.5% of adults undergoing endoscopy in outpatient US military hospital (included large percentage of black patients)
• Genetics (gene locus identified on chromosome 5q22- Rothenberg M et al. 2010)
• Commonly seen in atopic individuals (approximately 75%)
• Timing of diagnosis (and exacerbations)- increased in pollen season in some patients


Symptoms of EoE
• Dysphagia and feeding dysfunction • Food impaction• GERD like symptoms • Chest pain• Abdominal pain• Vomiting• Anorexia/early satiety
Liacouras CA et al. J Allergy Clin Immunol 2011

Kapel et al. Gastroenterology 2008;134:1316

Findings Associated With EoE
Endoscopic/Radiologic• Esophageal rings• Stricture• Linear furrows• Longitudinal narrowing• Longitudinal shearing
(crepe paper esophagus)• White exudates
Histologic• Mucosal eosinophilia• Eosinophil micro abscess• Superficial layering of eos• Extracellular eos granules• Epithelial desquamation• Basal zone hyperplasia• Dilated intercellular spaces• Sub epithelial fibrosis/sclerosis• Mastocytosis and MC
degranulation• CD 8 lymphocytes and B cells
Liacouras CA et al. J Allergy Clin Immunol 2011

Differential Diagnosis of EoE
• GERD• Eosinophilic gastrointestinal diseases• Celiac disease• Crohn’s disease• Infection• Hypereosinophilic syndrome• Achalasia• Drug hypersensitivity• Vasculitis• Pemphigus vegetans• Connective tissue disease• Graft-versus-host disease
Liacouras CA et al. J Allergy Clin Immunol 2011

Differentiating EoE From GERD
• Difficult to separate into two distinct diseases • Possible relationships:
1. GERD causes esophageal injury with eosinophilia2. EoE and GERD coexist but are unrelated3. EoE causes or contributes to secondary GERD4. GERD causes or contributes to EoE
• A trial of PPIs, even when diagnosis of EoE is established, is recommended
Spechler et al. Am J Gastroenterol 2007


Why The Increase In Allergic Diseases (Atopy)?
• Genetics• Environment- allergen, pollution, chemical, pesticide,
fertilizer exposure, environmental warming?• Hygiene hypothesis - Th1 vs. Th2 lymphocytes• Increased use of GERD medications-
– Less acidic environment in gut leads to exposure to more intact proteins (altered mucosal absorption) which may affect processing of food antigens
• Food antigen processing (i.e. cooking methods of peanuts can alter allergenicity)

Hygiene Hypothesis:Why The Increase In Atopy
• Th2 cytokines- IL-4, IL-5, IL-13
• Th1 cytokines- IFN-γ, IL-2, TNF-α
www.fooddrugallergy.ucla.edu

Why The Increase In Allergic Diseases (Atopy)?
• Different routes of sensitization – Application of creams containing peanut oil to inflamed skin
can sensitize to peanut (Lack G et al.)
• Epicutaneous allergen sensitization potently primes for respiratory allergen-induced experimental EoE (Akei HS et al. Gastroenterology 2005)
– Interesting in light of high percentage of EoE patients with atopic dermatitis
• Connection between development of eosinophilic infiltration in respiratory tract and esophagus in response to external allergic triggers, but also to intrinsic Th2 cytokines (Rothenberg et al. Gastroenterology 2009)


Why Are We Seeing An Increase In EoE?
• Increased recognition• Chronic nature of EoE• Increasing atopic disease in general• Other as yet unknown factors

Seasonal Distribution in Newly Diagnosed Cases of EoE in Adults
• Retrospective review of newly diagnosed EoE patients 8/06-7/07 at Mayo Clinic
• EoE more frequently diagnosed in spring (44%) and summer (24%) than fall (17%) and winter (15%) (in light of constant number of endoscopies done year round)
• Also described in children (Wang FY et al.)
• Implicates aeroallergens (and more specifically pollens) as potential etiologic factors in EoE
• Patients with EoE have seasonal variations in symptoms (Onbasi K et al.)
Almansa C et al.

Eosinophilic esophagitis
Atopic dermatitis (eczema)
Eosinophilic gastritis
Eosinophilic gastroenteritis
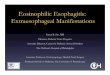
Food Allergy: Immunologic Spectrum
Anaphylaxis Urticaria Angioedema Oral Allergy
Syndrome
Celiac (IgA driven) Food Protein Induced
Proctitis Food Protein Induced
Enterocolitis Food Protein Induced
enteropathy
Sampson H. et al.
IgE Mediated Non-IgE MediatedMixed

Mechanisms of EoE
• EoE etiology- appears to be multifactorial – Immediate hypersensitivity (IgE against food/pollen
proteins)(Gell and Coombs type I reaction)– Delayed type hypersensitivity (cellular- especially
lymphocyte driven)(Gell and Coombs type IV reaction)
– Mast cells have also been shown to play role• We don’t yet fully understand the complete
mechanisms of EoE

IgE Mediated Allergic Reactions: Require Sensitization and Re-exposure

Food Allergies:The Facts On IgE Reactions
• 6-7 million in U.S. suffer from food allergies • Food allergy is #1 cause of anaphylaxis in ED (over
50,000 cases anaphylaxis per year)• Estimated 180 deaths per year (majority to
peanuts/tree nuts)• Almost a 20% increase in prevalence of food
allergies from 1997-2007• Peanut allergy affects >1% school aged children

Oral Allergy Syndrome(Also Driven By IgE)
• Oral pruritus with fresh raw fruits and vegetables (< 4% become systemic)
• Occurs in subset of pollen allergic individuals– Birch- apple, apricots, peaches, carrots, cherries,
kiwi, plums, hazelnuts– Ragweed- bananas, melons, cucumbers– Grasses- cherries, tomatoes, avocado, potatoes– Mugwort- melon, apple, peach, cherry
• Very labile proteins- heating and gastric acid denature
• Segment of EoE population has OAS (may be group with more relevant aeroallergen contribution, seasonal assoc.)

EoE Mechanisms:Delayed Type Hypersensitivity (DTH)
• Primarily lymphocyte driven (rather than antibody)
• Atopy Patch Testing (APT) is used to identify delayed reactions to foods
• Other examples of DTH include PPD used to test for TB, allergic contact dermatitis (nickel or poison oak reactions)

EoE Mechanism:Delayed Type Hypersensitivity

Mechanisms of EoE: Mast Cells
• Esophageal mastocytosis and degranulation in EoE– Lead to dysmotility in children and adults associated with
dysphagia– Produce cytokines that activate eosinophils and promote
tissue remodeling• Mast cell-associated transcriptome may distinguish EoE patients
from controls (future marker?)• Increased TGF-β1 associated with esophageal remodeling and
fibrosis as well as dysmotility– Potential therapeutic target
Aceves S et al. J Allergy Clin Immunol 2010 Abonia JP et al. J Allergy Clin Immunol 2010

Esophageal Cytokine Profile in EoE• Thus far, no reliable, noninvasive biomarkers for EoE, however: 1. Eotaxin-3 – mRNA expression increased in EoE patients vs. controls (89%
sensitivity with single biopsy)– Signals migration of eosinophils from vascular space into tissue – strongly correlated with tissue eosinophilia and mastocytosis
2. IL-13 – Tissue and serum expression levels of IL-13 correlate with tissue eosinophilia
in EoE (and disease activity)– One of the most promising potential biomarkers for the disease– Induces eotaxin-3 production
3. IL-5 – Produced by mast cells, promote maturation and activation of eosinophils– Absence leads to deficiency of eosinophil number and function
Blanchard C et al. Bhardwaj et al.


Sherill JD et al.
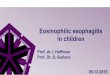
The molecular pathogenesis of EoE. An allergic insult by either food antigens or aeroallergens initiates the transition of the esophagus from a normal (NL) to an EoE phenotype through the production of TSLP by the esophageal epithelium. TSLP-activated dendritic cells induce a robust TH2 response and enhanced IL-13, which in turn mediates marked dysregulation of gene expression (the EoE transcriptome). Enhanced eotaxin-3 (CCL26) secretion by the esophageal epithelium promotes eosinophil migration from the blood into the tissue. Eosinophil- and mast cell–derived TGF-β along with IL-13 and IL-5 act on fibroblasts and mast cells and stimulate the fibrotic response. Loss of FLG expression, partially because of IL-13 overproduction, genetic variants, or both, might further enhance or even predispose patients with EoE to antigen exposure and exacerbate TH2 inflammation (and promote food allergen uptake)

Esophageal Remodeling In EoE
• Esophageal biopsies show increased TH2 cytokines (IL-5, IL-4, IL-13) and TH1 cytokines (IFN-γ)
• Also increased eosinophil chemo attractants– eotaxin-1, eotaxin-3, and TNF-α
• Esophageal remodeling in EoE is similar to allergen induced airway remodeling in patients with asthma
• EoE patients- increased fibrosis and vascularity vs. controls and patients with GERD
• TGF-β (expressed by eosinophils) promotes fibrosis and remodeling in sub epithelia in EoE
Aceves S et al. J Allergy Clin Immunol 2007

Diagnosis of Food Allergy
• Detailed history and PE– possible causal foods, quantity ingested, time course,
other contributing factors (exercise, ASA, EtOH), possible cross contamination
• Food specific IgE testing– Skin testing– Serum specific testing– Basophil activation/release assays
• Atopy patch testing (eosinophilic GI diseases, AD)• Oral Challenge (DBPCOC, Single blinded, or open)

Diagnosis Food Allergy (IgE Mediated): Skin Prick Testing
• Small amount of the allergen is placed on top of the skin – Skin is “scratched” to introduce allergen percutaneously– Wheal and flare is measured using positive and negative
controls with results in 20 minutes• Skin prick tests (SPT) generally have better sensitivity
and predictability than serum specific testing and are the preferred initial diagnostic approach (Bernstein IL et al.)– For IgE food allergy- NPV>95%, PPV 50%– For EoE- NPV 58-95%, PPV 33-95%

Skin Testing

Delayed Reactions To Foods:Patch Testing (APT):
• Measures delayed type hypersensitivity (allergic contact dermatitis)
• Food slurry is prepared and placed in shallow aluminum wells (Finn Chambers) and taped on back touching the skin for.
• The patches are removed at 48 hours (preliminary read) and measured at 72 hours (final read) using standard patch test protocols.
Turjanmaa K et al. Spergal JM et al. Ann Allergy, Asthma, Immunol 2005

Patch Testing (APT)

Allergy Testing For EoE
• Skin testing (combination of SPT and APT to foods and SPT to aeroallergens best)
• General screen includes- cow’s milk, hen’s egg, soy, wheat, rice, corn, oat, barley, potato, beef, chicken, pork, turkey, peanut, peas, green beans, squash, carrots, peach, apple (+/- fish, shellfish, tree nuts, and other foods that are common part of individual's diet)
Spergel JM et al. J Allergy Clin Immunol 2007;119:509-11Bernstein IL et al. Ann Allergy Asthma Immunol 2008;100:s1-148

Food Allergy Tests That Are Unproven or Disproved
• Food specific IgG or IgG4 (IgG “RAST”)– May actually be more representative of foods
the gut has recently seen or tolerates• Provocation/neutralization• Cytotoxic tests/ hair analysis• Applied kinesiology (muscle response
testing)• Electro-dermal testing
Bernstein IL et al.

Treatment Of EoE
• What are goals of treatment?– clinical improvement– histological normalcy– reversal of fibrosis (remodeling)– prevention of disease progression
• Drugs, diet, and dilation

Treatment of EoE- Medications
• Medications– Corticosteroids– Proton pump inhibitors– Anti-IL-5 mAb- (reslizumab and mepolizumab) decreased
esophageal eosinophilia but limited clinical response (studies ongoing)
• Also suggests that eosinophilia may not be the key pathologic effector (?part of a larger Th2 response)
• Medications not recommended – Cromolyn sodium- mast cell stabilizer– Leukotriene receptor antagonists (monteleukast, zafirlukast)– Immunosuppressants (azothiaprine, 6-MP)- risks outweigh benefits
Spergel JM et al. J Allergy Clin Immunol 2012Assa’ad et al. Gastroenterology 2011Straumann et al. Gut 2010

Treatment of EoE
• Food elimination (elemental diet vs. targeted food diet)
• Esophageal dilation- can provide immediate and long-lasting relief of dysphagia in patients with stricture (doesn’t address esophageal inflammation)- more data needed

Treatment of EoE: Corticosteroids
1. Systemic corticosteroids- for severe dysphagia, hospitalization, inability to eat, weight loss– Significant long term risks- infection (esp fungal), HTN,
osteopenia/osteoporosis, glucose intolerance, cataracts, adrenal suppression
2. Localized corticosteroids– Swallowed fluticasone 220 mcg- 1-2 puffs bid or viscous
budesonide 1 mg bid– Disease recurs with drug cessation – Patients with more significant atopy may be less responsive– Steroid resistance in minority of patients (as seen with other
atopic diseases like asthma)



Treatment of EoE: Proton Pump Inhibitors
• Cohort of unselected adults referred for endoscopy due to upper GI symptoms with proximal esophageal eosinophilic infiltrate– Baseline endoscopy followed by Rabeprazole 20 mg bid for 2 months,
then endoscopy repeated– 75% achieved clinicopathological remission with PPIs– 50% of patients with EoE phenotype responded to PPIs
• Interestingly, pH monitoring was poorly predictive of PPI response.• Potential mechanisms of PPI response
– Placebo effect– Treat concurrent GERD– Acid hypersensitivity– Anti-inflammatory effect of PPIs
Molina-Infante J et al.

Treatment of EoE:Dietary Intervention
1. Elemental Diet- restricted to amino-acid based formula (Elecare, Neocate, or Eo28 Splash)
2. Targeted elimination diet– Based on allergy testing (SPT/patch testing (APT))
3. Empiric elimination diet– Also called 6 Food Elimination Diet (SFED)– Avoidance of most common food allergens
• milk, egg, wheat, soy, nuts (peanuts/tree nuts), and seafood (fish and shellfish)

Treatment of EoE: Dietary Intervention
• Remember to stop topical corticosteroids before starting diet to allow recurrence of symptoms in order to document clinical effectiveness of diet
• Complete removal of the food(s) for 8-12 weeks• If possible, repeat endoscopy at end of elimination
trial (consideration of cost, coverage, risk)• If clinicopathologic improvement, then add foods back
one at a time• Clinical trials often repeat endoscopy after each food
reintroduced, but not always practical


Treatment of EoE: Elemental Diet
Advantages• Very effective
• > 95% demonstrate clinical and histologic improvement
• Allows systematic re-introduction of foods
• Removes the need for medications
Disadvantages• Expensive• Unpalatable• Need for feeding tube• Quality of life issues
Chehade M et al. Castellano M et al. Penfield JD et al.

Targeted Food Elimination (Based On SPT/APT)
• Retrospective series in 146 children treated with an elimination diet guided by the results of skin prick and patch testing
• Resolution of esophageal eosinophilia was observed in 77 percent • Egg, milk, and soy were identified most frequently with skin prick
testing, while corn, soy, and wheat were identified most frequently with atopy patch testing
• On average, 4 causative foods were identified per patient• Disease reoccurred after foods reintroduced (clinically and
histologically)• Combination of SPT/APT lead to better specificity than either test
alone
Liacouras CA et al. Clin Gastroenterol Hepatol 2005Spergel JM et al. Ann Allergy Asthma Immunol 2005

Identification of Causative FoodsIn EoE Treated With Elimination Diet
• Retrospective review in cohort of >700 patients with EoE • Definitive foods identified in 319 patients
– the rest were on elemental diet or responded to elimination diet but failed to f/u, added back multiple foods at a time, or didn’t want to add foods back in once they responded clinically
• 75% of patients were atopic, similar to other studies• SPT predictive values for EoE not as good as in patients with IgE
mediated food allergies• 70% of EoE patients allergic to 1-3 foods• Milk, egg, wheat, and soy most common allergens
– Other foods usually fell into 2 general categories- grains and meats
Spergel JM et al. J Allergy Clin Immunol 2012

Treatment Of EoE: Elimination Diet: Allergy Testing vs. SFED
• Compared removing foods based on allergy testing vs. SFED– Both had histologic response of 53% (vs. 95% with elemental diets) – NPV using SPT and APT was 80-100% for all foods (including egg,
wheat, soy) except milk (44%)• Authors Proposed 2 subsets of EoE
1. Those allergic to select major allergens 2. The other (almost 20%) group were allergic to more diverse group of
foods (many suggestive of OAS to fruits/vegetables)• Concluded that SFED or allergy testing based methods had equal success,
but one advantage of allergy testing was that fewer foods were removed.
Spergel JM et al. J Allergy Clin Immunol 2012

Targeted Diet Therapy
Spergel JM et al. J Allergy Clin Immunol 2012

Comparative Dietary Therapy Effectiveness In Remission of EoE
• Retrospective observational study in cohort from Cincinnati (CCED)• Compared effectiveness and remission rates of 3 diets- elemental
(n=49), SFED (n=26), skin test directed (n=23) • Dietary therapy is highly effective in EoE (both allergy testing and
SFED groups) – No statistical difference in remission between the 2 groups– Of note, not all of the allergy tested patients had patch testing done
• Both of the directed diets are inferior to elemental diet • Skin testing alone may not be superior to SFED, but usually involves
less foods being eliminated.– Adherence inversely related to the number of foods eliminated
• More studies needed to help determine optimal elimination diets, testing, and sensitivities/specificities/NPV/PPV Henderson CJ et al.

Comparative Dietary Therapy Effectiveness In Remission of Pediatric Eosinophilic Esophagitis
Henderson CJ et al.

Targeted Food Elimination in Adults
• 6 adults with active EoE- SPT + to grass pollen, wheat, and rye
• Elimination of wheat and rye failed to reduce disease activity and challenge with these same foods didn’t provoke EoE flare– Allergy to only wheat (or wheat and rye alone) not seen in
other studies– No APT done– Patients who are grass pollen allergic often test positive to
wheat (and other grains) due to cross-reactivity on testing without clinical significance
Simon D et al.

Empiric Elimination Diet:Six Food Elimination Diet (SFED)
• Prospective, uncontrolled study in 50 adults with EoE on SFED for 6 weeks • History of bid PPI or normal pH study• 78% had greater than 50% reduction in peak eosinophils in esophagus
(64% had < 5 eos/hpf)• Decrease in dysphagia scores by 94%• Most common food allergies- wheat and milk, followed by soy, nuts, and
egg• Reintroduction of foods led to return of previous pathology and symptoms
confirming food allergies• SPT predicted only 13% of foods associated with EoE • Authors concluded SPT may not be as helpful in adults as in kids, but APT
not done, and aero-allergens were not treated/addressed
Gonsalvez et al. Gastroenterology 2012

Empiric Elimination DietSix Food Elimination Diet (SFED)
• Observational study of 2 cohorts of Children • 35 put on SFED for 6 weeks
– Histologic improvement in 74% and symptomatic improvement in 97%
• Second cohort of 27 children (similar population) treated with elemental diet– Histologic improvement in 88%– Cost $900-$1500/month for a 20 Kg child(2006)
Kagalwalla AF et al. Clin Gastroenterol Hepatol 2006


Important Considerations of Dietary Treatment
• Registered dietician- provide ongoing dietary counseling, watch for cross-contamination, adequate caloric intake, vitamins, etc.
• Selection of diet- should be based upon severity of disease, patient’s lifestyle and quality of life, as well as family resources
• Importance of being realistic and upfront with the patient from the start– Many patients hope for a quick and easy fix and it usually is not– Patients need to be ready to commit to diet (or encouraged to
wait/treat with meds until they are)• If the offending food is found and improvement is attained with
elimination, the elimination appears life-long at this time (tolerance to the food(s) doesn’t occur)

Other Dietary Tips In Treatment Of EoE
• Caution with:• Highly textured foods (meats)• Bulky foods (certain breads, potatoes)
• Cut food into small pieces• Chew extensively • Eat slowly• Wash foods down with liquids

Prognosis of EoE• EoE cohort had decreased quality of life and persistent
symptoms 15 years after presentation • EoE leads to persistent dysphagia, food impaction and
structural esophageal alterations (including stricture)• Patients with increased esophageal eosinophil counts and
food allergy (as well as atopy in general) have increased risk for food impaction and persistent symptoms and therefore should be treated and monitored more aggressively
• No malignant potential has been associated with this disease
DeBrosse C et al. Straumann A et al. Rothenberg M. 2009

Future of EoE• Critical to better understand mechanisms to help guide diagnosis and therapy
– Need to continue to evolve EoE definition• In spite of clear food allergy role, need to determine utility of food testing,
especially in adults (and role of aeroallergens)• Need to clearly define optimal treatment endpoints (histologically and
clinically)– Define what histological “normalcy” is (i.e. <5 eos/hpf)
• Need for relevant biomarkers (eotaxin-3 and IL-13 may be the most promising Bhardwaj et al.)
• Guidelines for evaluation and management of the asymptomatic patient with esophageal eosinophilia
• Determine optimal frequency of endoscopy in follow-up (as well as guidelines on number and locations of esophageal biopsies)
• Validated measurements of symptoms, endoscopic findings, histology, and quality of life

Summary of EoE
• EoE has shown increasing incidence and prevalence (paralleling that of atopy in general)
• Most EoE patients are also atopic (and control of these diseases may play role in EoE control)
• Mechanism of EoE still not definitive, but is at least in part antigen driven (especially food antigen)
• Diagnosis remains clinicopathologic– Allergy evaluation and testing is currently recommended but further
studies needed to clarify utility and best approach, especially in adults • Treatment options include use of medications
– Trial of PPI is recommended as some EoE patients respond– Swallowed corticosteroids are effective but carry risk of adverse
effects

Summary of EoE
• Dietary interventions eliminating food antigens are effective– Elemental diet is most effective dietary intervention(but also
extremely prohibitive)– Targeted elimination of diet based on allergy testing and SFED are
both effective– Relevance of aero-allergens should be assessed, especially in
hard to treat patients • Long term therapy must be individualized for each patient• Prognosis consistent with chronic process requiring ongoing
treatment • Coordination of gastroenterology, allergy/immunology,
pathology, and certified nutritionists

Eat Dirt!


References• Liacouras CA et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol 2011;128:3-
20• Furuta GT et al. EoE in children and adults: a systematic review and consensus recommendations for diagnosis and treatment.
Gastroenterology 2007;133:1342-63• Straumann A et al. Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years.Gastroenterology
2003;125:1660-69• Gonsalvez et al. Elimination diet effectively treats EoE in adults; food reintroduction identifies causative factors. Gastroenterology
2012;142(7):1451-59• Spergel JM et al. Identification of causative foods in children with EoE treated with an elimination diet. J Allergy Clin Immunol 2012;130:461-7• Abonia JP et al. Involvement of mast cells in eosinophilic esophagitis. J Allergy Clin Immunol 2010;126:140-9.• Abonia JP et al. TGF-B1: mediator of feedback loop in EoE- or should we really say mastocytic esophagitis. J Allergy Clin Immunol
2010;126:1205-07• Spergel JM et al. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch
tests Ann Allergy Asthma Immmunol 2005;95:336-43• Spechler et al. Thoughts on the complex relationship between gastroesophageal disease and eosinophilic esophagitis. Am J Gastroenterol
2007;72:1312-16• Merwat SN et al. Might the use of acid-suppressive medications predispose to the development of EoE. Am J Gastroenterol 2009;104:1897-
1902.• Rothenberg et al. Biology and treatment of EoE. Gastroenterology 2009;137:1238-49• Spergel JM et al. Predictive values for skin prick test and atopy patch test for eosinophilic esophagitis. J Allergy Clin Immunol 2007;119:509-11• Dellon ES et al. Clinical, endoscopic, and histologic findings distinguish EoE from GERD. Clin Gastroenterol Hepatol 2009;7(12):1305-13• Fiorentino R et al. Cross-sector sponsorship of research in eosinophilic esophagitis: A collaborative model for rational drug development in
rare diseases. J Allergy Clin Immunol. 2012;130(3):613–6• Penfield JD et al. The Role of Allergy Evaluation in Adults With EoE. J Clin Gastroenterol 2010;44:22-7.• Castellano M et al. Defining the role of food allergy in a population of adult patients with eosinophilic esophagitis. Inflamm Allergy Drug
Targets. 2010;9:257–262• Kagalwalla AF et al. Effect of 6 food elimination diet on clinical and histologic outcomes in EoE. Clin Gastroenterol Hepatol 2006;4:1097-1102• Henderson CJ et al. Comparative dietary therapy effectiveness in remission of pediatric EoE. J Allergy Clin Immunol 2012;129:1570-8• Chehade M et al. Food allergy and eosinophilic esophagitis. Curr Opin Allergy Clin Immunol. 2010;10:231–237

References• Aceves S et al. Mast cells infiltrate the esophageal smooth muscle in patients with EoE, express TGF-B1, and increase esophageal smooth
muscle contraction. J Allergy Clin Immunol 2010;126:1198-204• Spergel JM et al. Variation in prevalence, diagnostic criteria, and initial management options for eosinophilic gastrointestinal diseases in the
United States. J Pediatr Gastroenterol Nutr. 2011 Mar;52(3):300-6• Aceves S et al. Esophageal remodeling in eosinophilic esophagitis. J Allergy Clin Immunol 2007;119:206-12• Kelley KJ et al. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula.
Gastroenterology 1995;109:1503-12• Almansa C et al. Seasonal distribution in newly diagnosed cases of eosinophilic esophagitis in adults. Am J Gastroenterol 2009;104:828-33• Rodrigo S et al. High intraepithelial eosinophil counts in esophageal squamous epithelium are not specific for eosinophilic esophagitis in
adults. Am J Gastroenterol 2008;103:435-42• Kapel RC et al. Eosinophilic esophagitis: a prevalent disease in the United States that affects all age groups. Gastroenterology 2008;134:1316-
21• Abu-Sultaneh SM et al. Fluticasone and food allergen elimination reverse sub-epithelial fibrosis in children with eosinophilic esophagitis. Dig
Dis Sci. 2011;56:97–102• Akei HS et al. Epicutaneous antigen exposure primes for experimental eosinophilic esophagitis in mice. Gastroenterology 2005;129:985-94 • Dohil R et al. Oral viscous budesonide is effective in children with eosinophilic esophagitis in a randomized, placebo-controlled trial.
Gastroenterology 2010;139:418-29• Veerappan GR et al. Prevalence of eosinophilic esophagitis in an adult population undergoing upper endoscopy: a prospective study. Clin
Gastroenterol Hepatol. 2009;7:420–426• Sherill JD et al. Genetic dissection of eosinophilic esophagitis provides insight into disease pathogenesis and treatment strategies. J Allergy Clin
Immunol 2011;128(1):23-32• Molina-Infante J et al. EoE infiltration responds to proton pump inhibition in most adults. Clinical Gastroenterology and Hepatology
2011;9:110-17• Simon D et al. Eosinophilic esophagitis in adults--no clinical relevance of wheat and rye sensitizations. Allergy 2006;61:1480-83• Lack G et al. Factors associated with the development of peanut allergy in childhood. N Engl J Med 2003;348:977-85• Blanchard C et al. A striking local esohpageal cytokine expression profile in EoE. J Allergy Clin Immunol 2011;127:208-17• Prasad GA et al. Epidemiology of eosinophilic esophagitis over three decades in Olmsted County, Minnesota. Clin Gastroenterol Hepatol.
2009;7:1055–1061• Bernstein IL et al. Allergy diagnostic testing: an updated practice parameter. Ann Allergy Asthma Immunol 2008;100:s1-148

References• Kagalwalla, et al; Clin Gastroenterol Hepatol 2006; 117(2Suppl):S470• Onbasi K et al. Eosinophil infiltration of the oesophageal mucosa in patients with pollen allergy during the season. Clin Exp Allergy
2005;35:1423-31• Bhardwaj N et al. Biomarkers for eosinophilic esophagitis: a review. Ann Allergy, Asthma & Immunol 2012;109(3):155-159• Sampson H. Update on food allergy. J Allergy Clin Immunol 2004;113:805-9• Rothenberg ME et al. Common variants at 5q22 associate with pediatric eosinophilic esophagitis. Nat Genet 2010;42(2):289-91• Kagalwalla AF et a. EoE: epithelial mesenchymal transitition contributes to esophageal remodeling and reverses with treatment. J Allergy
Clin Immunol. 2010;129:1387-96.• Straumann A et al. Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years.
Gastroenterology 2003;125:1660-69• Spergel JMet al. Reslizumab in children and adolescents with EoE: results of a double-blind, randomized, placebo-controlled trial. J Allergy
Clin Immunol 2012;129:456-63• Blanchard, C. et al. EoE: pathogenesis, genetics, and therapy. J. Clin. Invest. 2006;116:536-547• Onbasi K et al. Eosinophil infiltration of the oesophageal mucosa in patients with pollen allergy during the season.Clin Exp Allergy
2005;35:1423-31• Wang FY et al. Is there a seasonal variation in the incidence or intensity of allergic eosinophilic esophagitis in newly diagnosed children? J
Clin Gastroenterol 2007;41:451-3• DeBrosse C et al. Long-term outcomes in pediatric onset EoE. J Allergy Clin Immunolog 2011;128:132-8• Sampson HA et al. AGA technical review on the evaluation of food allergy in gastrointestinal disorders. American Gastroenterological
Association. Gastroenterology. 2001;120:1026 –1040• Vickery et al. Mechanisms of immune tolerance relevant to food allergy. JACI 2011;127:576• Turjanmaa K et al. EAACI/GA2LEN position paper: present status of the atopy patch test. Allergy 2006;61:1377• Assa’ad et al. An antibody against IL-5 reduces numbers of esophageal intraepithelial eosinophils in children with eosinophilic esophagitis.
Gastroenterology 2011;141:1593-604• Straumann et al. Anti-interleukin-5 antibody treatment (mepolizumab) in active eosinophilic oesophagitis: a randomised, placebo-
controlled, double-blind trial. Gut 2010;59:21-30• American Partnership for Esoinophilic Disorders www.apfed.org• American Academy of Allergy, Asthma, and Immunology www.aaaai.org• Food Allergy and Anaphylaxis Network www.foodallergy.org• The International Gastrointestinal Eosinophilic Researchers (TIGER)