Embed Size (px)
Citation preview

Paper ID #33167
Enhancing the Teaching of Research Ethics Through Emotional Priming withEncounters with Patients and Reflection
Dr. Ashley J. Earle, York College of Pennsylvania
Ashley is an Assistant Professor in the Mechanical and Civil Engineering department at York College ofPennsylvania. She received her B.S in Chemical and Biomolecular Engineering and B.A. in InternationalStudies from Lafayette College. She then pursued her passion for neuromuscular disease research atCornell University where she received her PhD in Biomedical Engineering. At York, she is passionateabout developing pedagogy that encourages students in reflective learning and personal self reflection inengineering classes in addition to her passion for engineering ethics and conceptual learning.
Nozomi Nishimura, Cornell UniversityProf. Isaac Smith, Brigham Young UniversityDr. David M. Small, Cornell University
c©American Society for Engineering Education, 2021

Enhancing the teaching of research ethics through encounters with patients and reflection
Introduction
Responsible conduct of research is a major element of all engineering disciplines but is especially important in biomedical engineering. Recently, there has been a movement toward more stringent research ethics practices due to the large volume of failed clinical trials that had previously shown success in animal models [1]. Further analysis of these failures pointed to a lack of strict inclusion criteria, insufficient statistical power, and other study design flaws as key culprits. In addition to these examples, there have been multiple major events of data falsification and other types of manipulations that threaten the public confidence in scientific research [2, 3]. As many engineers and scientist get their first research training at the undergraduate level through extracurricular participation in research labs [4, 5], it is important to start addressing these serious ethical concerns with students from the beginning of their training. Beyond the basics of research practice, we should also help students to develop an understanding of downstream consequences of poor research ethics decisions on the end users, who is often a patient in the biomedical context. Given the importance of biomedical engineering ethics, not only in academia but also in industry, a key question arises – what is the most effective way to teach students good ethical practices?
Research on the psychology of ethical and moral decision making has identified a variety of factors that influence people’s ethically relevant choices and behaviors. Because of the social nature of morality (i.e., many, if not most, unethical and immoral behaviors are those that seem to somehow cause harm to others in some way [4]), many of the predictors of ethical and unethical behavior relate to the way that actors and decision makers see, consider, and view the people who are affected by their actions. For example, the extent to which people can take the perspective of others and see the world through others’ eyes, can help them better calibrate all of the potential consequences of their decisions. Moreover, it has been shown that people who have a more expansive circle of moral regard--meaning that they cast a wider net in terms of the people and entities they deem worthy of moral concern--often make more ethical decisions related to the treatment of other people [5]. In short, a major motivating factor for ethical decision making is an understanding of the downstream consequences, whether personal or societal, of not upholding a high moral standing.
In biomedical engineering, the ultimate benefactor of the research is the patient. We wanted to evaluate whether an encounter with patients in conjunction with instruction on ethical conduct of research could 1) change the ethical leanings in our students or 2) make students more receptive to learning ethics as a first step to eventually shaping their actions. We exposed students to a seminar in which they met and heard from cancer patients about their experiences with the disease, and both successful and unsuccessful treatments, as well as what biomedical research meant to them. The first phase of our study focused on the reactions of undergraduate students visiting a large, private research-institution for a summer research experience. The second phase of our study focused on Biomedical Engineering students who were currently enrolled in a seminar course. We

used voluntary surveys for both phases of the study, and also analyzed assigned short essay responses to reflection questions for the seminar course students. In the summer, we allowed students to select whether they attended a research ethics seminar, and/or the cancer patient seminar based on personal preference and/or scheduling. In the summer, we considered students attending cancer patient seminar and the research ethics seminar as the treatment group compared those to who attended only the research ethics seminar (control). During the semester, we required the seminar students to attend both seminars, but split the groups so that half of the students were primed with the cancer patient experience prior to learning about research ethics (treatment), and the other half responded to the ethics seminar prior to meeting the cancer patients (control).
In the summer cohort, despite finding differences in the ethical leanings of our treatment and control group at baseline, we did not find any changes in ethical leanings after attending the research seminar regardless of whether the students also attended the cancer patient seminar. This points to the stability of the ethical landscape, and possible participation bias based on ethical leanings. The preliminary results with the ethical survey tool and its ability to detect differences between groups point to a possible use in evaluating the impact of research ethics education in the field of biomedical engineering, although it would require further confirmation in a larger study. In the semester cohort, we found that the timing of the emotional encounter with the cancer patients did not impact the ability of the students to describe bias and scientific ways to avoid bias in their own lives in short essay assignments. However, students in the treatment group were twice as likely to write about retrospection, responsibility, and a concern for downstream consequences of bias than the control group. While our group sizes are too small to make definitive conclusions on the impact of the cancer patient seminar, the possibility that emotional priming enhances a student's internalization of ethical discussion deserves further investigation. It also points to the usage of reflective essays and metacognitive analysis as a valuable tool in learning and evaluating ethics education.
Methods
Research Purpose and Question
Business has an extensive literature on ethical thought as well as practice to help teach ethics in younger generations [6, 7], but biomedical engineering has not yet seen the same depth of scholarship [8]. We wanted to investigate the effects of emotional encounters with people directly impacted by research ethics on students in biomedical engineering and scientific research. To do this, we had two student populations, sophomore level BME undergraduates in a seminar course and research experience for undergraduates (REU) students visiting our institution for the summer for lab research. Both sets of students participated in a seminar on research ethics and a discussion with cancer patients, a sample of people who would ultimately be impacted by the ethical or unethical decisions of biomedical researchers. The primary difference between the two groups was that the summer REU students could self-select which seminars to participate in, while the sophomore BME undergraduates were required to take both seminars, in randomly assigned order.
We hypothesized that having a personal and emotional interaction with people impacted by research decisions would impact interest in ethics or influence decision making toward more

ethical or inclusive behaviors. In the sophomore seminar we added an additional layer of interaction to investigate whether the timing of the emotional intervention in relation to the ethical education would impact the student outcomes. For both cases, we developed a survey on ethical tendencies and moral expansiveness which was given to the students at the start of the semester and then after the ethics and emotional interventions. In addition to the survey, we also evaluated student reflection essays from the sophomore seminar to further understand the thought process of the students regarding ethical decision.
Course and Participant Overview
For the REU portion of this study, we evaluated the 2017 cohort of students attending a mix of research programs hosted at a Cornell University which included students in REU programs about neuroscience, engineering, biology and students who were unaffiliated with a formal program, with most students being sophomore and junior undergraduates. A goal of the REU programs was to provide an intensive, hands-on, immersive research experience for students. In addition to research, students could also attend seminars and talks with topics ranging from how to apply to graduate school, ethics, research design, and novel scientific discoveries. Many of these additional panels are optional for students which naturally created groups of students who did and did not receive either a formal ethical educational experience or the emotional experience with cancer patients to serve as controls.
To investigate the impact of an emotional experience coupled with a targeted ethical intervention, we used a sophomore level Experiential Learning Seminar (ExpLS) over the course of two years, Spring 2017 and Spring 2019, for a total of 50 students with 35 participating in the survey. These students had declared or were planning to declare their major in biomedical engineering. The course met once a week for 50 minutes and was focused on building professional skills in a reflective environment including team-building, communication, and leadership. Each year the course was run, there was a slightly different line up of topics ranging from the biodesign process, personal values, listening and empathy, future career plans, and ethics based on the faculty who volunteered to lead seminar sessions. Each week, students were asked to submit a short, prompted essay describing their reactions and thoughts surrounding the topic of the week. These essays were graded primarily based on completion and not on quality, length, or other more quantitative metrics. In both years, the topics and essays related to ethics, patient experience, and graduate school were controlled and delivered in the same order in late January/February.
Demographically, the students in our sample are heavily skewed toward women in both the REU and ExpLS cohorts with >80% and 75% women in the groups, respectively. The REU cohort was significantly more racially diverse, with 25% of students identifying as Black or Other, while the ExpLS cohort was almost evenly split between White and Asian students. In addition to race, the REU group had more students with both parents with lower education levels and at lower socio-economic standing. Even with this increase in diversity, 50% of the students in the REU program had a moderate amount (six months to two years) of previous research experience. Approximately half of the students in each cohort reported having previous ethics training.
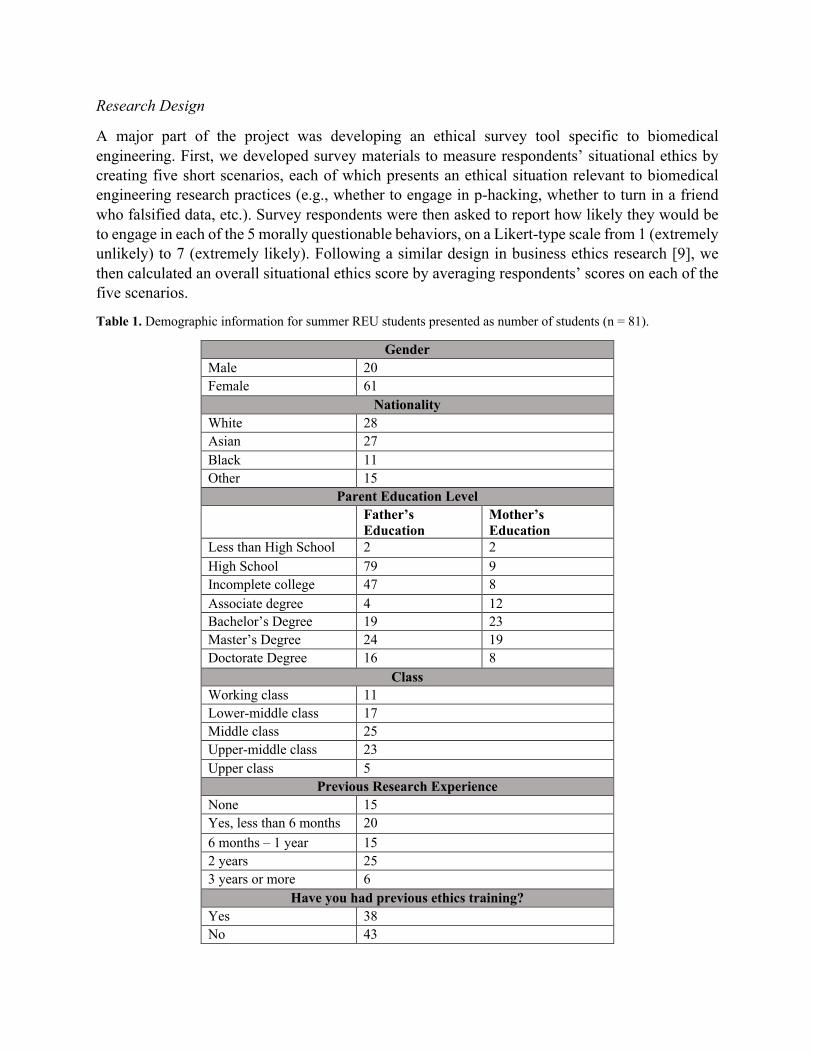
Research Design
A major part of the project was developing an ethical survey tool specific to biomedical engineering. First, we developed survey materials to measure respondents’ situational ethics by creating five short scenarios, each of which presents an ethical situation relevant to biomedical engineering research practices (e.g., whether to engage in p-hacking, whether to turn in a friend who falsified data, etc.). Survey respondents were then asked to report how likely they would be to engage in each of the 5 morally questionable behaviors, on a Likert-type scale from 1 (extremely unlikely) to 7 (extremely likely). Following a similar design in business ethics research [9], we then calculated an overall situational ethics score by averaging respondents’ scores on each of the five scenarios.
Table 1. Demographic information for summer REU students presented as number of students (n = 81).
Gender Male 20 Female 61
Nationality White 28 Asian 27 Black 11 Other 15
Parent Education Level Father’s
Education Mother’s Education
Less than High School 2 2 High School 79 9 Incomplete college 47 8 Associate degree 4 12 Bachelor’s Degree 19 23 Master’s Degree 24 19 Doctorate Degree 16 8
Class Working class 11 Lower-middle class 17 Middle class 25 Upper-middle class 23 Upper class 5
Previous Research Experience None 15 Yes, less than 6 months 20 6 months – 1 year 15 2 years 25 3 years or more 6
Have you had previous ethics training? Yes 38 No 43
Second, we adapted an established perspective-taking scale [10] to refer specifically to the context of scientific research. The items asked respondents the extent to which they considered others’ perspectives related to their research practices (e.g., “before criticizing the results of an experiment designed to test a new drug, I try to imagine how this affects the people afflicted with this disease,” “I sometimes try to understand my faculty advisor better by imagining how things look from their perspective,” “I try to communicate my methods so other scientists can repeat my experiments”). The six items were averaged to form a composite measure of perspective-taking.
Third, we also adapted a scale designed to measure the breadth of a person’s circle of moral regard [5]--that is, the extent to which they deem others worthy of moral concern. We asked subjects to rate the level of obligation they felt (1 = absolutely no obligation, 5 = very strong obligation) to show moral regard to a variety of research-related entities (e.g., other lab members, competing scientists, end user of research result, the broader research/academic community, etc.). Their responses were averaged to form a composite measure of the expansiveness of a person’s moral circle.
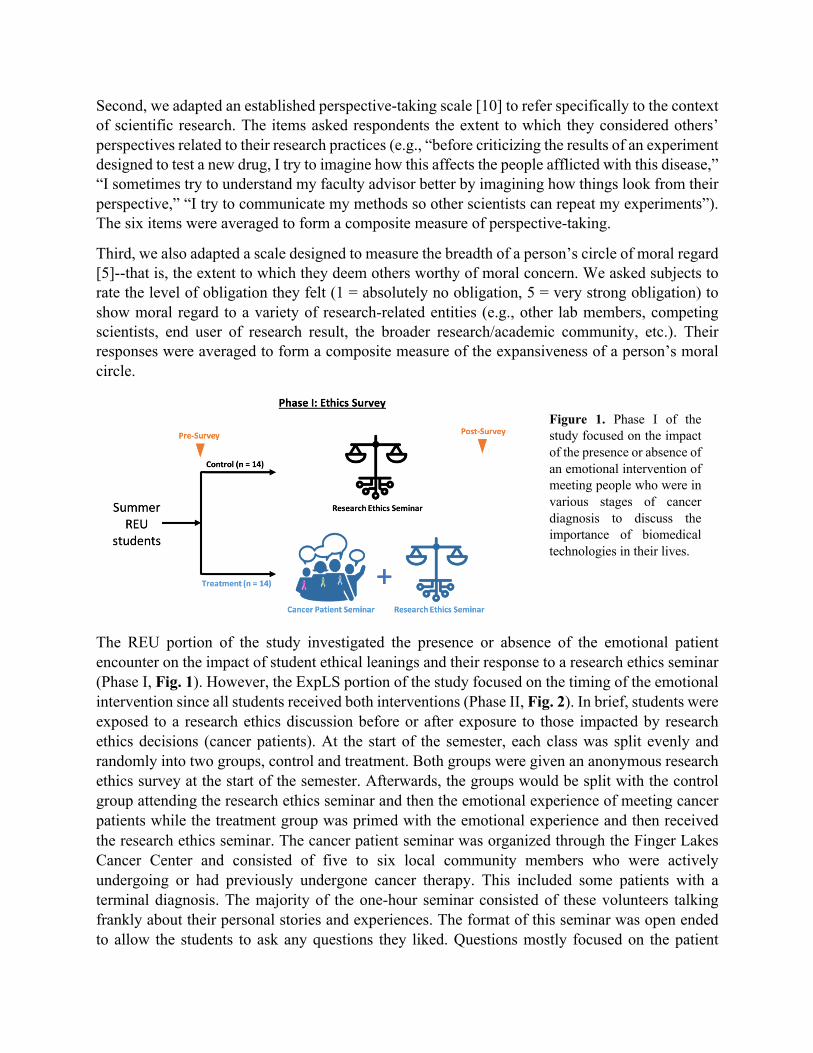
The REU portion of the study investigated the presence or absence of the emotional patient encounter on the impact of student ethical leanings and their response to a research ethics seminar (Phase I, Fig. 1). However, the ExpLS portion of the study focused on the timing of the emotional intervention since all students received both interventions (Phase II, Fig. 2). In brief, students were exposed to a research ethics discussion before or after exposure to those impacted by research ethics decisions (cancer patients). At the start of the semester, each class was split evenly and randomly into two groups, control and treatment. Both groups were given an anonymous research ethics survey at the start of the semester. Afterwards, the groups would be split with the control group attending the research ethics seminar and then the emotional experience of meeting cancer patients while the treatment group was primed with the emotional experience and then received the research ethics seminar. The cancer patient seminar was organized through the Finger Lakes Cancer Center and consisted of five to six local community members who were actively undergoing or had previously undergone cancer therapy. This included some patients with a terminal diagnosis. The majority of the one-hour seminar consisted of these volunteers talking frankly about their personal stories and experiences. The format of this seminar was open ended to allow the students to ask any questions they liked. Questions mostly focused on the patient
Figure 1. Phase I of the study focused on the impact of the presence or absence of an emotional intervention of meeting people who were in various stages of cancer diagnosis to discuss the importance of biomedical technologies in their lives.

experiences, although the faculty facilitators also prompted some discussion by the volunteers about how the scientific community, and biomedical engineers specifically, could best serve their needs. A question-and-answer panel of graduate students was used both years as a control seminar opposite the research ethics discussion. The second survey was administered to each group separately, after they attended the research ethics seminar. At the end of the semester the final ethics survey was given. As an incentive to complete all three surveys, students could self-report completion at the end of the semester to receive a gift card to the university bookstore.
The research ethics seminar was presented by the same professor for both class years. The seminar focused on best practices for rigor in lab included standard topics such as inclusion and exclusion criteria, data quality, study design and power analysis, analysis bias and p-hacking. The example of failures in many clinical trials for stroke treatments that contradicted preclinical research results was presented as motivation. Following the seminar students were asked to take a short multiple-choice quiz which was used in conjunction with the essays written after each of three course sessions to evaluate students' understanding and thoughts surrounding ethical decision making in research.
Data Collection and Analysis
All avenues of data collection were approved under the Cornell Institutional Review Board (IRB, protocol 1705007200). Surveys were completed anonymously with the student’s mother initials (Example, Elizabeth Mary Smith would be EMS) provided to link surveys together. Likert-score questions from the survey, such as “please indicate the extent to which you are likely to engage in the following behavior” with answers ranging from extremely unlikely to extremely likely, were translated into a numerical score based on the total number of answer options. In all situational cases (i.e. when there was a more ethical option), more ethical and engaged answers were given higher scores. In the case of expansiveness, a higher number indicates a broader range of people who should be considered in one’s decisions. Participants were excluded if they provided the same answer for all cases regardless of the question, incorrectly answered the attention check question,
Figure 2. Phase II of the study split a seminar course into two randomly assigned sections to test whether or not emotional priming would impact student receptivity to a lesson on research ethics. Students met people diagnosed with cancer who discussed their patient experiences and their views on biomedical research and technology either before or after a didactic research ethics seminar. An informational session on graduate school was used as the control.

or if they did not complete at least 80% of the survey. Due to low numbers of students completing the post-seminar survey, we were not able to use the survey data from the ExpLS cohort.
The analysis for the ExpLS cohort focused on the in-class ethics quiz and numerous reflective essays. Quiz grades were compared between groups for cohorts in both years. Students were required to write reflective essays throughout the seminar, and we asked students to self-score the amount of effort they felt they put into their reflections on a scale of 1-5 with five being the most effort. We compared the self-rated effort put into these essays for the research ethics, cancer patient, and graduate school essays. For the ethics essay in particular, we wanted to evaluate if the cancer patient seminar improved the sophistication or depth of students’ response to the question, “Describe a situation in which unconscious bias may have influenced your assessment or conclusion and what measures were taken or should have been taken to avoid these biases.” These essays were analyzed blindly by three independent researchers on 1) the level of detail and specificity in the description of the situation, 2) quality of analysis on the role of or the cause of bias, 3) level of detail and specificity in the description of the measures, and 4) justification or analysis of the measures. All three independent scores were averaged to produce the final score for each category.
In addition, we also performed phrase analysis on the research ethics essay for topics that were covered in the seminar as well as student interpretation of their own actions. Essays were blinded and then coded by a single researcher. The pre-determined codes were shared with two other independent researchers who assigned codes to the essays based on the themes present. Final tallies of the codes used were based on at least two of three researchers interpreting the written work as the same code. Individual codes were grouped into categories and then unblinded for analysis of treatment effect.
Statistical analysis
All statistical analysis was completed in Prism 9.0. Data collected from the survey tracking multiple groups across time was analyzed with a 2-way ANOVA with paired subjects and Sidak test for multiple comparisons. T-tests were used to compare the control and treatment groups for ExpLS quiz grade, essay word count and essay grades. One-way ANOVA was used to evaluate the word count and student self-rating of effort put into essays between the semester average, research ethics, and cancer essays. Alpha values were set to 0.05 for statistical significance.
Results
Phase I: Use of the Research Ethics Survey Instrument
Likert questions on the survey were transitioned to a numerical scale such that higher numbers indicated increased reporting of engagement in the behavior in question. Predominantly, there were very few differences between the treatment (n=15) and control (n=17) group, especially in the areas of perspective taking (Fig. 3A). The treatment group seemed at baseline to indicate a decreased likelihood of exposing ethical issues in a research setting at baseline than the control group from 5.8/7 to 5.1/7 where 7 indicated that the subject would always report a possible ethical violation. This result remained stable after the cancer discussion (Fig. 3B). A similar trend was
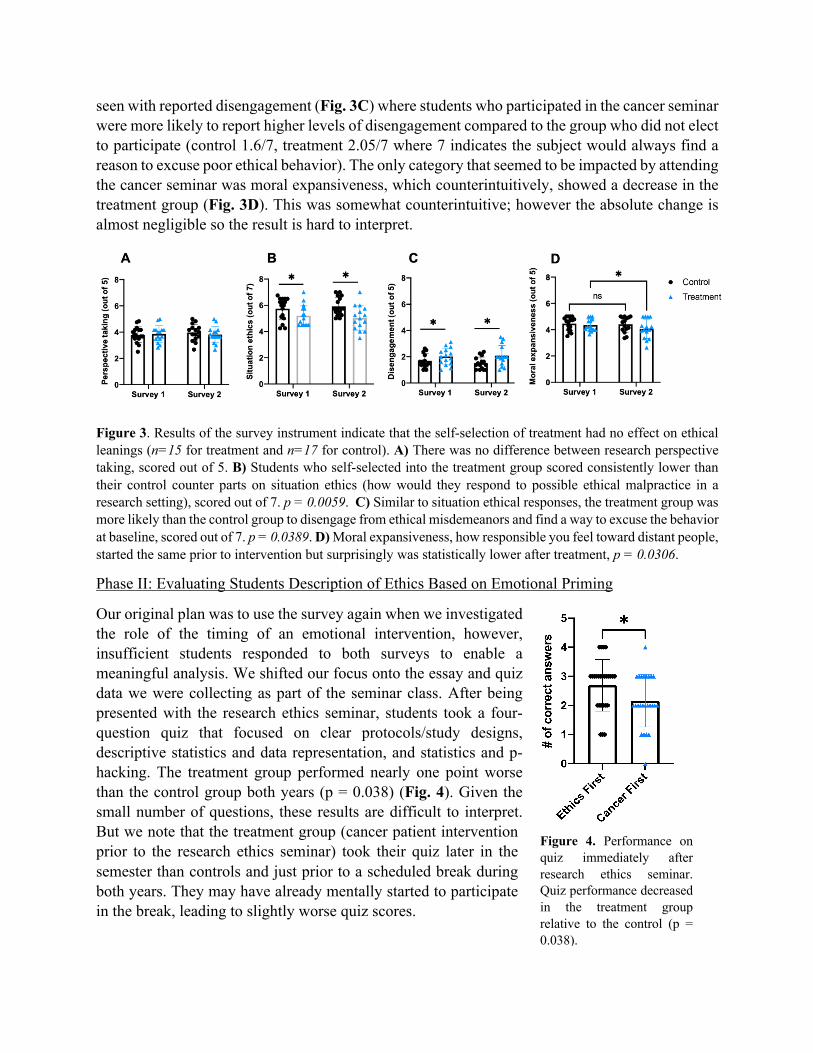
seen with reported disengagement (Fig. 3C) where students who participated in the cancer seminar were more likely to report higher levels of disengagement compared to the group who did not elect to participate (control 1.6/7, treatment 2.05/7 where 7 indicates the subject would always find a reason to excuse poor ethical behavior). The only category that seemed to be impacted by attending the cancer seminar was moral expansiveness, which counterintuitively, showed a decrease in the treatment group (Fig. 3D). This was somewhat counterintuitive; however the absolute change is almost negligible so the result is hard to interpret.
Figure 3. Results of the survey instrument indicate that the self-selection of treatment had no effect on ethical leanings (n=15 for treatment and n=17 for control). A) There was no difference between research perspective taking, scored out of 5. B) Students who self-selected into the treatment group scored consistently lower than their control counter parts on situation ethics (how would they respond to possible ethical malpractice in a research setting), scored out of 7. p = 0.0059. C) Similar to situation ethical responses, the treatment group was more likely than the control group to disengage from ethical misdemeanors and find a way to excuse the behavior at baseline, scored out of 7. p = 0.0389. D) Moral expansiveness, how responsible you feel toward distant people, started the same prior to intervention but surprisingly was statistically lower after treatment, p = 0.0306.
Phase II: Evaluating Students Description of Ethics Based on Emotional Priming
Our original plan was to use the survey again when we investigated the role of the timing of an emotional intervention, however, insufficient students responded to both surveys to enable a meaningful analysis. We shifted our focus onto the essay and quiz data we were collecting as part of the seminar class. After being presented with the research ethics seminar, students took a four-question quiz that focused on clear protocols/study designs, descriptive statistics and data representation, and statistics and p-hacking. The treatment group performed nearly one point worse than the control group both years (p = 0.038) (Fig. 4). Given the small number of questions, these results are difficult to interpret. But we note that the treatment group (cancer patient intervention prior to the research ethics seminar) took their quiz later in the semester than controls and just prior to a scheduled break during both years. They may have already mentally started to participate in the break, leading to slightly worse quiz scores.
Figure 4. Performance on quiz immediately after research ethics seminar. Quiz performance decreased in the treatment group relative to the control (p = 0.038).
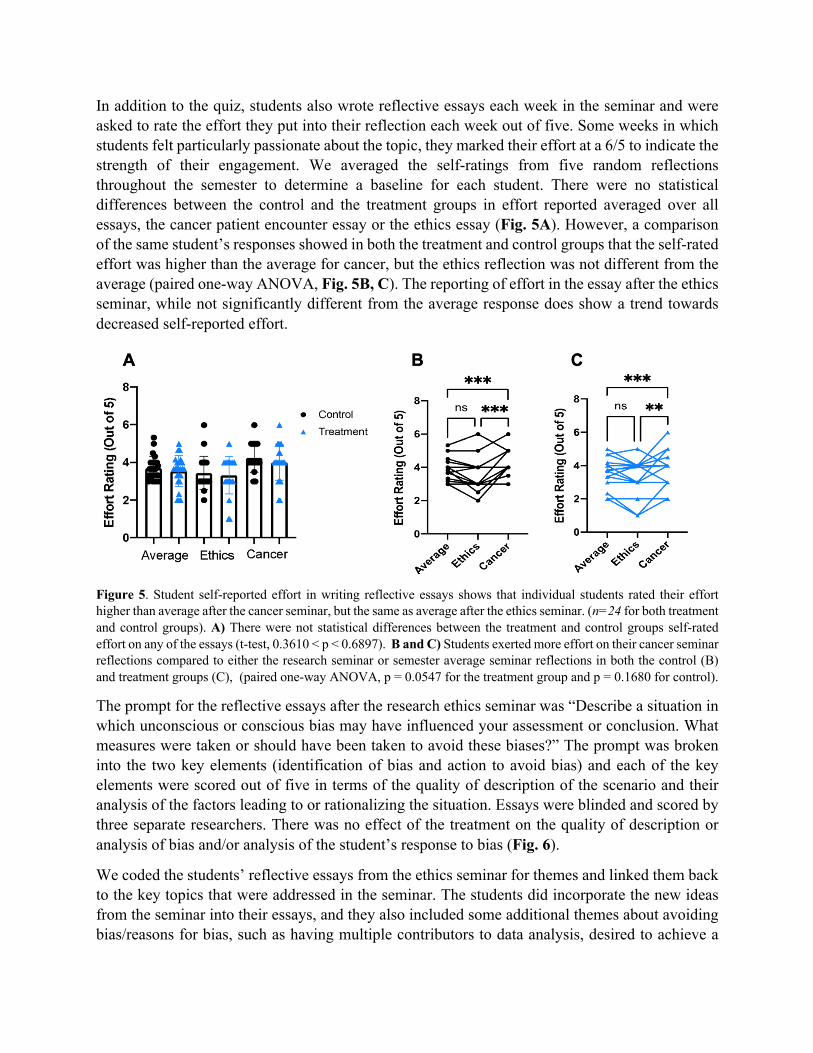
In addition to the quiz, students also wrote reflective essays each week in the seminar and were asked to rate the effort they put into their reflection each week out of five. Some weeks in which students felt particularly passionate about the topic, they marked their effort at a 6/5 to indicate the strength of their engagement. We averaged the self-ratings from five random reflections throughout the semester to determine a baseline for each student. There were no statistical differences between the control and the treatment groups in effort reported averaged over all essays, the cancer patient encounter essay or the ethics essay (Fig. 5A). However, a comparison of the same student’s responses showed in both the treatment and control groups that the self-rated effort was higher than the average for cancer, but the ethics reflection was not different from the average (paired one-way ANOVA, Fig. 5B, C). The reporting of effort in the essay after the ethics seminar, while not significantly different from the average response does show a trend towards decreased self-reported effort.
Figure 5. Student self-reported effort in writing reflective essays shows that individual students rated their effort higher than average after the cancer seminar, but the same as average after the ethics seminar. (n=24 for both treatment and control groups). A) There were not statistical differences between the treatment and control groups self-rated effort on any of the essays (t-test, 0.3610 < p < 0.6897). B and C) Students exerted more effort on their cancer seminar reflections compared to either the research seminar or semester average seminar reflections in both the control (B) and treatment groups (C), (paired one-way ANOVA, p = 0.0547 for the treatment group and p = 0.1680 for control).
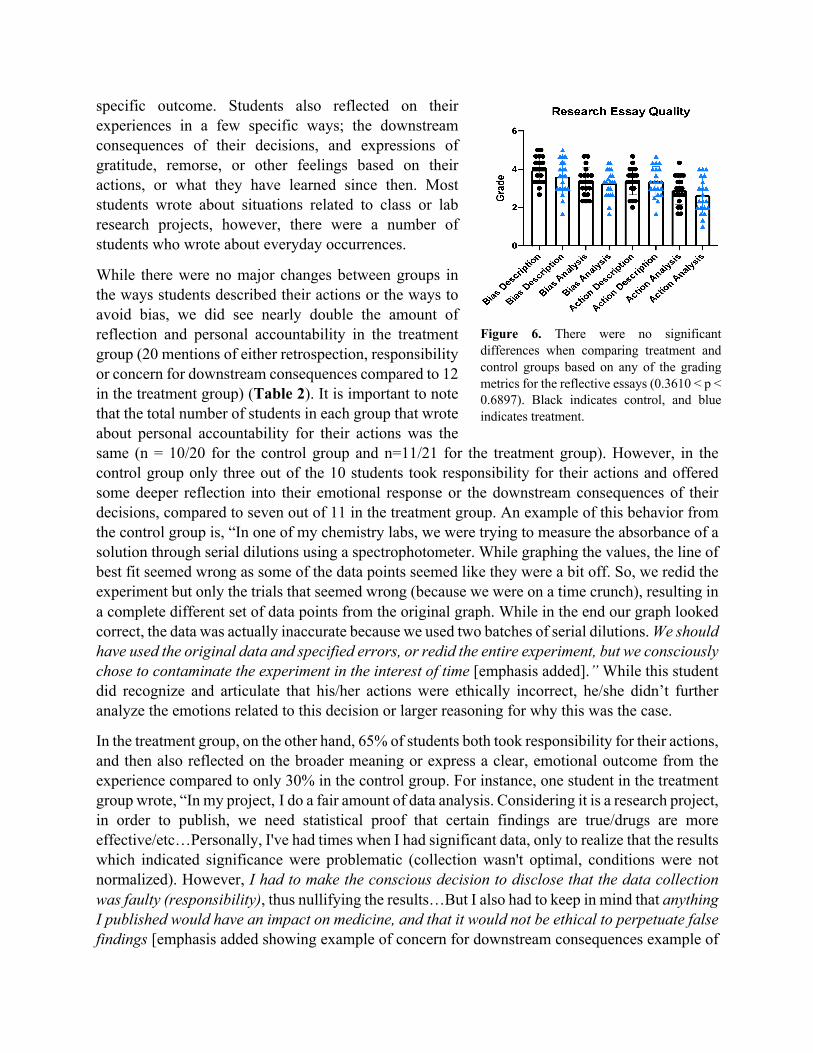
The prompt for the reflective essays after the research ethics seminar was “Describe a situation in which unconscious or conscious bias may have influenced your assessment or conclusion. What measures were taken or should have been taken to avoid these biases?” The prompt was broken into the two key elements (identification of bias and action to avoid bias) and each of the key elements were scored out of five in terms of the quality of description of the scenario and their analysis of the factors leading to or rationalizing the situation. Essays were blinded and scored by three separate researchers. There was no effect of the treatment on the quality of description or analysis of bias and/or analysis of the student’s response to bias (Fig. 6).
We coded the students’ reflective essays from the ethics seminar for themes and linked them back to the key topics that were addressed in the seminar. The students did incorporate the new ideas from the seminar into their essays, and they also included some additional themes about avoiding bias/reasons for bias, such as having multiple contributors to data analysis, desired to achieve a
specific outcome. Students also reflected on their experiences in a few specific ways; the downstream consequences of their decisions, and expressions of gratitude, remorse, or other feelings based on their actions, or what they have learned since then. Most students wrote about situations related to class or lab research projects, however, there were a number of students who wrote about everyday occurrences.
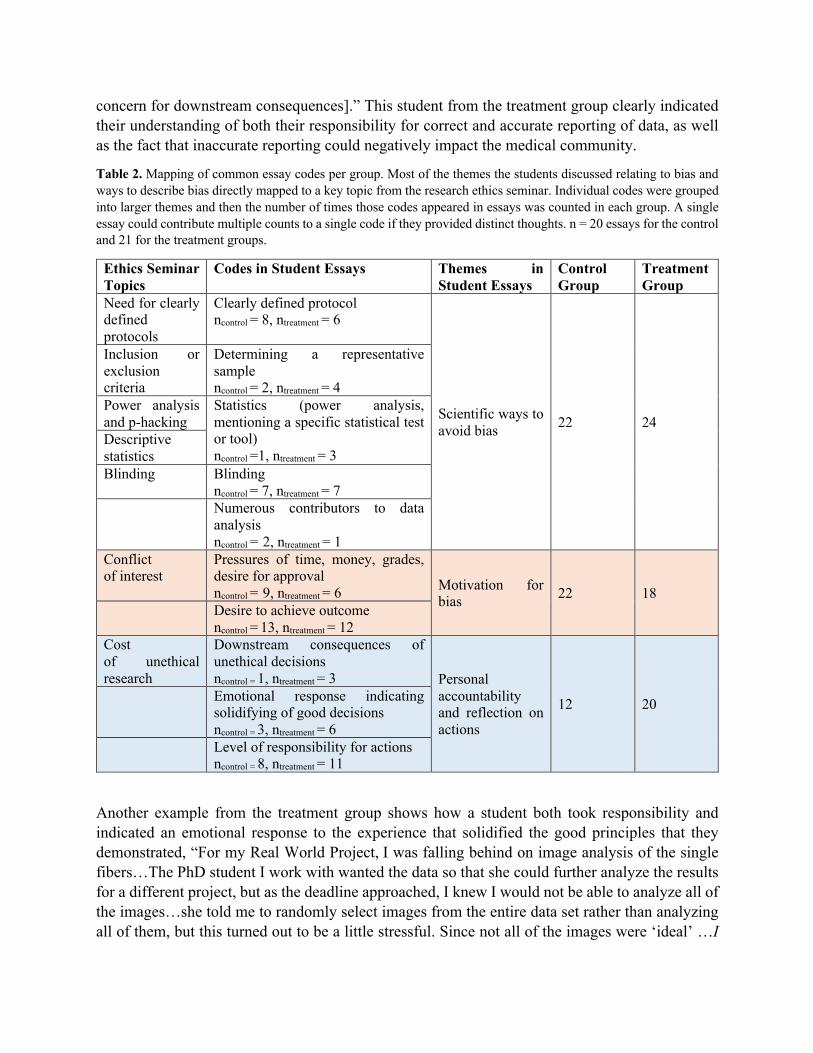
While there were no major changes between groups in the ways students described their actions or the ways to avoid bias, we did see nearly double the amount of reflection and personal accountability in the treatment group (20 mentions of either retrospection, responsibility or concern for downstream consequences compared to 12 in the treatment group) (Table 2). It is important to note that the total number of students in each group that wrote about personal accountability for their actions was the same (n = 10/20 for the control group and n=11/21 for the treatment group). However, in the control group only three out of the 10 students took responsibility for their actions and offered some deeper reflection into their emotional response or the downstream consequences of their decisions, compared to seven out of 11 in the treatment group. An example of this behavior from the control group is, “In one of my chemistry labs, we were trying to measure the absorbance of a solution through serial dilutions using a spectrophotometer. While graphing the values, the line of best fit seemed wrong as some of the data points seemed like they were a bit off. So, we redid the experiment but only the trials that seemed wrong (because we were on a time crunch), resulting in a complete different set of data points from the original graph. While in the end our graph looked correct, the data was actually inaccurate because we used two batches of serial dilutions. We should have used the original data and specified errors, or redid the entire experiment, but we consciously chose to contaminate the experiment in the interest of time [emphasis added].” While this student did recognize and articulate that his/her actions were ethically incorrect, he/she didn’t further analyze the emotions related to this decision or larger reasoning for why this was the case.
In the treatment group, on the other hand, 65% of students both took responsibility for their actions, and then also reflected on the broader meaning or express a clear, emotional outcome from the experience compared to only 30% in the control group. For instance, one student in the treatment group wrote, “In my project, I do a fair amount of data analysis. Considering it is a research project, in order to publish, we need statistical proof that certain findings are true/drugs are more effective/etc…Personally, I've had times when I had significant data, only to realize that the results which indicated significance were problematic (collection wasn't optimal, conditions were not normalized). However, I had to make the conscious decision to disclose that the data collection was faulty (responsibility), thus nullifying the results…But I also had to keep in mind that anything I published would have an impact on medicine, and that it would not be ethical to perpetuate false findings [emphasis added showing example of concern for downstream consequences example of
Figure 6. There were no significant differences when comparing treatment and control groups based on any of the grading metrics for the reflective essays (0.3610 < p < 0.6897). Black indicates control, and blue indicates treatment.
concern for downstream consequences].” This student from the treatment group clearly indicated their understanding of both their responsibility for correct and accurate reporting of data, as well as the fact that inaccurate reporting could negatively impact the medical community.
Table 2. Mapping of common essay codes per group. Most of the themes the students discussed relating to bias and ways to describe bias directly mapped to a key topic from the research ethics seminar. Individual codes were grouped into larger themes and then the number of times those codes appeared in essays was counted in each group. A single essay could contribute multiple counts to a single code if they provided distinct thoughts. n = 20 essays for the control and 21 for the treatment groups.
Ethics Seminar Topics
Codes in Student Essays Themes in Student Essays
Control Group
Treatment Group
Need for clearly defined protocols
Clearly defined protocol ncontrol = 8, ntreatment = 6
Scientific ways to avoid bias 22 24
Inclusion or exclusion criteria
Determining a representative sample ncontrol = 2, ntreatment = 4
Power analysis and p-hacking
Statistics (power analysis, mentioning a specific statistical test or tool) ncontrol =1, ntreatment = 3
Descriptive statistics Blinding Blinding
ncontrol = 7, ntreatment = 7 Numerous contributors to data
analysis ncontrol = 2, ntreatment = 1
Conflict of interest
Pressures of time, money, grades, desire for approval ncontrol = 9, ntreatment = 6 Motivation for
bias 22 18 Desire to achieve outcome
ncontrol = 13, ntreatment = 12 Cost of unethical research
Downstream consequences of unethical decisions ncontrol = 1, ntreatment = 3 Personal
accountability and reflection on actions
12 20 Emotional response indicating solidifying of good decisions ncontrol = 3, ntreatment = 6
Level of responsibility for actions ncontrol = 8, ntreatment = 11
Another example from the treatment group shows how a student both took responsibility and indicated an emotional response to the experience that solidified the good principles that they demonstrated, “For my Real World Project, I was falling behind on image analysis of the single fibers…The PhD student I work with wanted the data so that she could further analyze the results for a different project, but as the deadline approached, I knew I would not be able to analyze all of the images…she told me to randomly select images from the entire data set rather than analyzing all of them, but this turned out to be a little stressful. Since not all of the images were ‘ideal’ …I

was tempted to analyze only the ‘good’ images. I knew that I had enough time to perform image analysis on the single fibers that showed what I was looking for and that the standard deviation would be low if I did this, but after thinking about the ethical consequences of doing this, I decided not to. I ended up randomly analyzing a sample of the entire image set by using a random number generator because I did not want to risk publishing inaccurate--or biased--results. Although our data turned out to have a high standard deviation, I felt better about showing these results than if I had only analyzed the images I thought would give us the best results [emphasis added].” Another theme that appeared in more than one essay was gratitude for having experienced a situation that brought to light how easy it was to introduce bias, whether by mistakes or by not properly carrying out a protocol. This type of reflection that indicated the reports of an emotional to elements of bias and the downstream consequences occurred in 80% of treatment group essays but only in 40% of control group essays.
There was also an interesting subpopulation of students who avoided taking personal responsibility for their actions. A treatment group student wrote, “When doing lab experiments for classes, it is common to look for results based on the results that are theoretically expected. This monitoring of data and manipulation is further motivated by the fact that some classes grade based on your experimental results. To avoid this, one can set parameters for data gathering and statistical analysis before looking at the results [emphasis added].” While this student accurately determined reasons for introducing bias (desired outcome, wanting a good grade), and ways to collect accurate data (set parameters for data gathering, and likely the idea of blinding), they actually avoided their own personal accountability by discussing the actions that could be taken in the abstract “one” instead of using personal pronouns. The way in which this student, and others that dodged taking responsibility, discuss the practice of manipulating data is also underscoring a general attitude of moral disengagement by saying it is “common”. This specific behavior occurred twice out of all 41 students and both students were in the treatment group.
Discussion
We investigated the ways in which an emotional patient focused seminar could impact the way our students responded to learning about research ethics. Using a novel survey instrument, we found that students ethical leanings remain constant despite intervention. We piloted the use of textual analysis on reflective essays. We saw that the primary outcome of receiving emotional priming from the patient seminar prior to learning about research ethics was an increased likelihood to reflect on personal accountability and discuss the emotional response to ethical decisions and the downstream consequences of unethical decisions. In these studies, our sample sizes were small, limiting conclusiveness of our observations. However, this instruments and methods are practical for future implementation to follow up on these and other studies.
For Phase I of the study which used the survey instrument to evaluate the effect of having an emotional experience with patients in conjunction with learning about research ethics. The primary finding is the stability of student’s ethical leanings despite either kind of intervention. However, it is interesting that the group that self-selected to see the cancer patients scored statistically lower on the situational ethics and moral disengagement elements of the survey instrument (Fig 3B and C). The data between these two responses both trend toward those who elected to attend both the

research ethics seminar and the cancer seminar where less likely to make the most ethical choices in these two scenarios. Interestingly, the only metric to show a significant change was the morale expansiveness, which measures how far a person’s sense of ethical responsibly extends beyond their immediate community. The treatment showed a decrease in this metric, maybe because students realized that there were people in their local community who needed their attention who they had not previously felt connected with. However, the small sample size means that this could have been within the variation of noise. Although we generally saw null effects in terms of the survey instrument, the baseline characteristics of the self-selected groups could indicate that students who do not score as highly on the instrument were more willing to engage in situations that may challenge their ethical underpinnings. Again, the small sample size precludes strong conclusions, but whether or not student’s perception of their ethical correctness makes them more or less willing to engage in challenging experiences could be an interesting area for further investigation.
The most striking finding was that students who received emotional priming in the form of the cancer patient seminar prior to learning about research ethics showed nearly a doubling in the number of students who engaged in deeper reflective practices in their essays (Table 2) despite the general ability to describe ethical scenarios being unchanged compared to the control group (Fig. 6). This positive increase in deeper thought may be an important first step to producing long term ethical change and understanding. Social and emotional learning theory has been applied to ethics education at both the primary, secondary, and higher education levels with the aim of improving perspective taking, empathy and an understanding of the consequence of an individual’s actions on others [11, 12]. Previous work highlighted the need for clear and explicit ethics education that is contextualized in real experiences. Exposing students to people who have and continue to be impacted by research ethics in tangible ways, and who are willing to talk candidly about how their lives have been impacted, provides a clear motivation for why ethics matters. People matter. The level of emotional engagement that students had with the cancer seminar is unusual compared to many courses that also focus on ethics [8], especially since the panel of current or previous patients focused included what biomedical technology means to them. The most common types of learning techniques used for biomedical engineering ethics courses are in-class discussions, case studies, lectures, and examples of professional scenarios. The increase in student engagement with the cancer seminar (Fig. 5) is not surprising given the emotional nature of the experience. After the seminar some students were even moved to tears.
While not part of the study design, we observed an interesting discrepancy between self-reported completion of surveys and actual completions of surveys. In the summer research study, students were asked to provide information so that they could claim a reward (gift certificate) for participation in the study. This information was decoupled from the surveys so that that the data could remain separate from the information needed to send the reward. In this, students were asked to self-report whether they had completed all three of three surveys for a slightly larger gift certificate amount. We found that 42 claimed the completion of all three surveys, although there were only 33 that actually completed all three surveys in entirety. We found that this is an interesting case of over reporting favorable outcomes, even in the context of having just answered survey questions related to ethical issues in research data collection, data rigor, and moral

perspective. Unfortunately, this just emphasizes the difficulty of this type of teaching and the need for further study for effective ways of producing ethical behaviors.
Additional modifications to the course structure in the form of scaffolding and contextualizing could enhance the linkage in student minds between the patient seminar and the research ethics seminar. As mentioned before, the ability to take the perspective of others, and specifically those who will be impacted by their actions, is a primary predictor of ethical decision making [4], and hearing first hand from those who would be impacted is a wonderful way to understand their perspective. There are some simple ways our seminar could be modified to strengthen the connection between patient and ethics; 1) the patients spoke in the context of cancer whereas the ethics discussion was primarily in the context of strokes and thus not direct connection as made for the students by the professors, 2) the seminar primarily focused on patient experiences with a secondary focus on their relationship to biomedical science and research, 3) there was no follow-up discussion of the student reflective essays. Providing additional scaffolding could help students more consciously make the connection between their decisions, their jobs/research experiences, and the end-beneficiaries of their current or future work. Interestingly, all of students who discussed the downstream consequences were personally engaged in research and reflected on their personal experiences instead of a class experiment or everyday life scenario. It could be that student find it easier to engage in deeper reflection when the decisions happen in a real-life context, instead of one that is contrived (such as a lab course where they are graded on their outcome). This could point to this emotional priming having a larger effect on seniors engaged in design projects where research is not available, or possibly integrating this reflection into Co-op or internship opportunities where students have the opportunity to interact with clients. Regardless, the use of reflective practices in teaching engineering education [13-15], and engineering ethics specifically [16, 17], has been gaining momentum in recent years and our study adds to those that see enhanced outcomes of reflective practices, with a new emphasis on the power of an emotional encounter to trigger deeper and more meaningful reflection.
Acknowledgements
We would like to thank Finger Lakes Cancer Resource Center, the participants of the patient panel and Bob Ritter for their extraordinary generosity in presenting their stories to the students. We thank Amita Verma, Laurel Southard, Ryan Sauvé, Jonathan Butcher for their work in seeding and completing this study. This work was supported by Cornell’s Office of Engagement Initiatives and the National Science Foundation (1453339).
References
[1] S. A. Iqbal, J. D. Wallach, M. J. Khoury, S. D. Schully, and J. P. A. Ioannidis, "Reproducible Research Practices and Transparency across the Biomedical Literature," (in eng).
[2] M. R. Munafò et al., "A manifesto for reproducible science," Nature human behaviour, vol. 1, no. 1, pp. 1-9, 2017.
[3] J. Lenzer, The Danger Within Us: America's Untested, Unregulated Medical Device Industry and One Man's Battle to Survive It. Hachette UK, 2017.
[4] C. Schein and K. Gray, "The theory of dyadic morality: Reinventing moral judgment by redefining harm," Personality and Social Psychology Review, vol. 22, no. 1, pp. 32-70, 2018.
[5] A. Reed II and K. F. Aquino, "Moral identity and the expanding circle of moral regard toward out-groups," Journal of personality and social psychology, vol. 84, no. 6, p. 1270, 2003.
[6] E. P. Jonson, L. McGuire, and B. Cooper, "Does teaching ethics do any good?," Education+ Training, 2016.
[7] R. R. Sims and E. L. Felton, "Designing and delivering business ethics teaching and learning," Journal of Business Ethics, vol. 63, no. 3, pp. 297-312, 2006.
[8] A. R. Bielefeldt, N. E. Canney, C. Swan, M. Polmear, and D. Knight, "Microethics and macroethics education of biomedical engineering students in the United States," Ethics in Biology, Engineering and Medicine: An International Journal, vol. 7, no. 1-2, 2016.
[9] J. R. Detert, L. K. Treviño, and V. L. Sweitzer, "Moral disengagement in ethical decision making: a study of antecedents and outcomes," Journal of Applied Psychology, vol. 93, no. 2, p. 374, 2008.
[10] M. H. Davis, "A multidimensional approach to individual differences in empathy," 1980. [11] M. D. Burroughs and N. J. Barkauskas, "Educating the whole child: Social-emotional
learning and ethics education," Ethics and Education, vol. 12, no. 2, pp. 218-232, 2017. [12] L. Goralnik, K. F. Millenbah, M. P. Nelson, and L. Thorp, "An environmental pedagogy
of care: Emotion, relationships, and experience in higher education ethics learning," Journal of Experiential Education, vol. 35, no. 3, pp. 412-428, 2012.
[13] J. Colomer, M. Pallisera, J. Fullana, M. P. Burriel, and R. Fernández, "Reflective learning in higher education: A comparative analysis," Procedia-Social and Behavioral Sciences, vol. 93, pp. 364-370, 2013.
[14] M. Minnes, J. Mayberry, M. Soto, and J. Hargis, "Practice makes deeper? Regular reflective writing during engineering internships," Journal of Transformative Learning, vol. 4, no. 2, 2017.
[15] P. Wallin and T. Adawi, "The reflective diary as a method for the formative assessment of self-regulated learning," European Journal of Engineering Education, vol. 43, no. 4, pp. 507-521, 2018.
[16] J.-H. Kim, "Exploring Ways to Develop Reflective Engineers: Toward Phronesis-Centered Engineering Education," in Proceedings of the American Society for Engineering Education (ASEE) Annual Conference, 2019.
[17] L. G. Kisselburgh, J. Hess, C. Zoltowski, J. Beever, and A. Brightman, "Assessing a scaffolded, interactive, and reflective analysis framework for developing ethical reasoning in engineering students," in Proceedings of the American Society for Engineering Education Annual Conference & Exposition, 2016.





























