Embed Size (px)
Citation preview
O. RODANANT, M.D.
CHULALONGKORN UNIVERSITY HOSPITAL
Enhancing Recovery
with Desflurane
outcome and Efficacy

11.8%
Morbidly
obese patients• Often have cardiopulmonary and
associated pathologies
• Vulnerable to airway complications,
sleep apnoea and hypoxia during early
recovery
• Fast emergence might benefit recovery
and patient comfort
• Rate of emergence influenced by amount
of anaesthetic deposited in adipose
tissue
• The low solubility of desflurane in blood,
fat and other tissues are key properties
for obese patients
MORBIDLY
OBESE
BMI >35kg/m2
7. Strum EM et al. Anesth Analg 2004;99:1848-1853; 18. La Colla L, Albertin A, La Colla G, et al. Br J Anaesth. 2007 Sep;99
(3):353-358; 26. Bellamy M and Struys M. Anaesthesia for the Overweight and Obese Patient, Oxford Anaesthesia Library,
Oxford University Press, 2007: p25-26
18. La Colla L, Albertin A, La Colla G, et al. Br J Anaesth. 2007 Sep;99 (3):353-358
La Colla (2007) et al - study design18 MORBIDLY
OBESE
• 28 patients, ASA status II-III, age 37.1 yrs (SD 12.9), BMI
50.6kg/m2 (SD 5.4) undergoing elective bilio-intestinal
bypass surgery
• After propofol induction, patients were randomly assigned
to receive either 6% desflurane (n=14) or 2% sevoflurane
(n=14) in O2/air for 30 minutes while sampling of inspired
and end-tidal of gases was performed
Adapted from La Colla L, Albertin A, La Colla G, et al. Br J Anaesth. 2007 Sep;99 (3):353-358 18
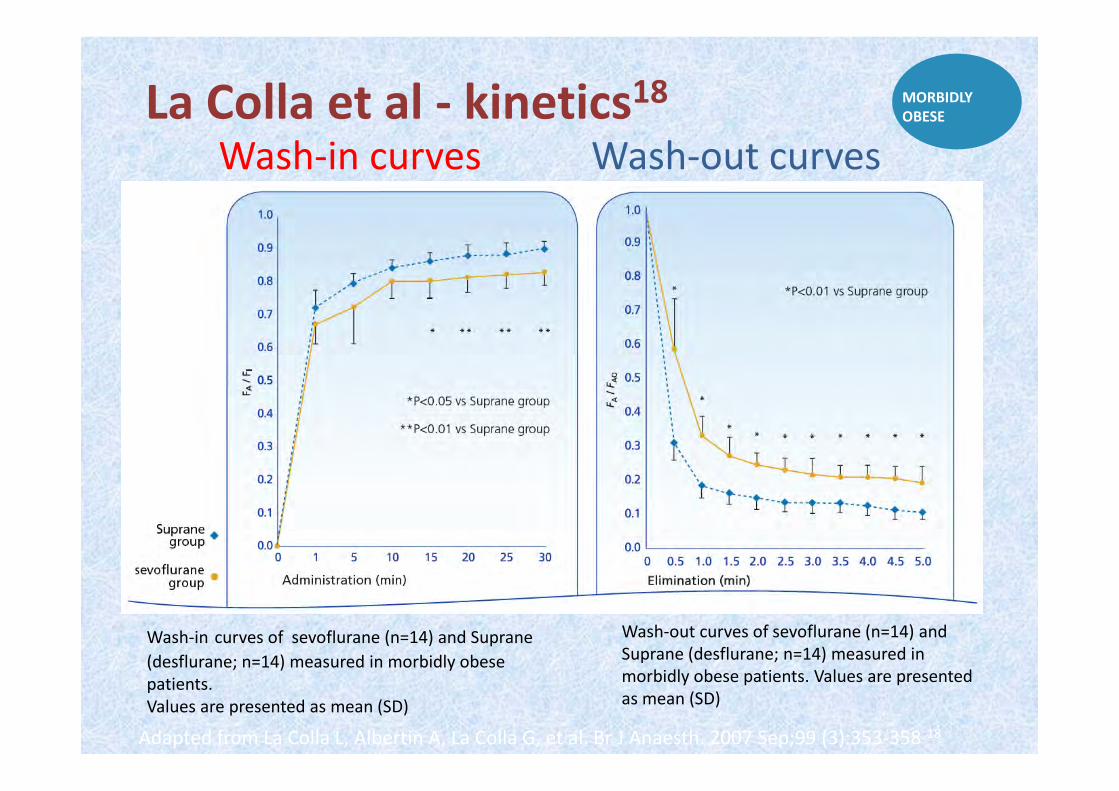
La Colla et al - kinetics18 MORBIDLY
OBESE
Wash-in curves Wash-out curves
Wash-in curves of sevoflurane (n=14) and Suprane
(desflurane; n=14) measured in morbidly obese
patients.
Values are presented as mean (SD)
Wash-out curves of sevoflurane (n=14) and
Suprane (desflurane; n=14) measured in
morbidly obese patients. Values are presented
as mean (SD)
•Cognitive impairment such as delirium and confusion can
be a problem during recovery in elderly surgical patients11
•Rapid recovery from prolonged anaesthesia may be an
advantage in the elderly11.
•Desflurane is highly lipid insoluble what makes it well
suited particularly in the elderly, because they have a
greater proportion of their body mass as fat than do
younger patients.27
Elderly (with prolonged anaesthesia) ELDERLY
(Prolonged
surgery)
11. Heavner JE, Kaye AD, Lin B-K, King T. Br J Anaesth 2003;91:502-506
27. Dodds C, Kumar C and Servin F. Anaesthesia in the Elderly Patient, Oxford Anaesthesia Library, Oxford University Press,
2007: p32,85
Heavner et al - study design11
11. Heavner JE, Kaye AD, Lin B-K, King T. Br J Anaesth 2003;91:502-506
* Inspired anaesthetic concentrations were adjusted to maintain mean arterial
blood pressure within 15% of baseline values
• 50 patients >65 years (ASA I-III) undergoing
non-emergency surgery requiring >2 hrs of
anaesthesia
• Included orthopaedic, abdominal, urogenital, skin
graft, eye, lymph node dissection, and breast surgery
• Maintainance: desflurane 2-6% or sevoflurane 0.6-
1.75% in 60% N2O / O2*; muscle relaxation was
obtained with vecuronium
• Mean duration of anaesthesia: desflurane = 154 min
sevoflurane = 159 min
ELDERLY
(Prolonged
surgery)
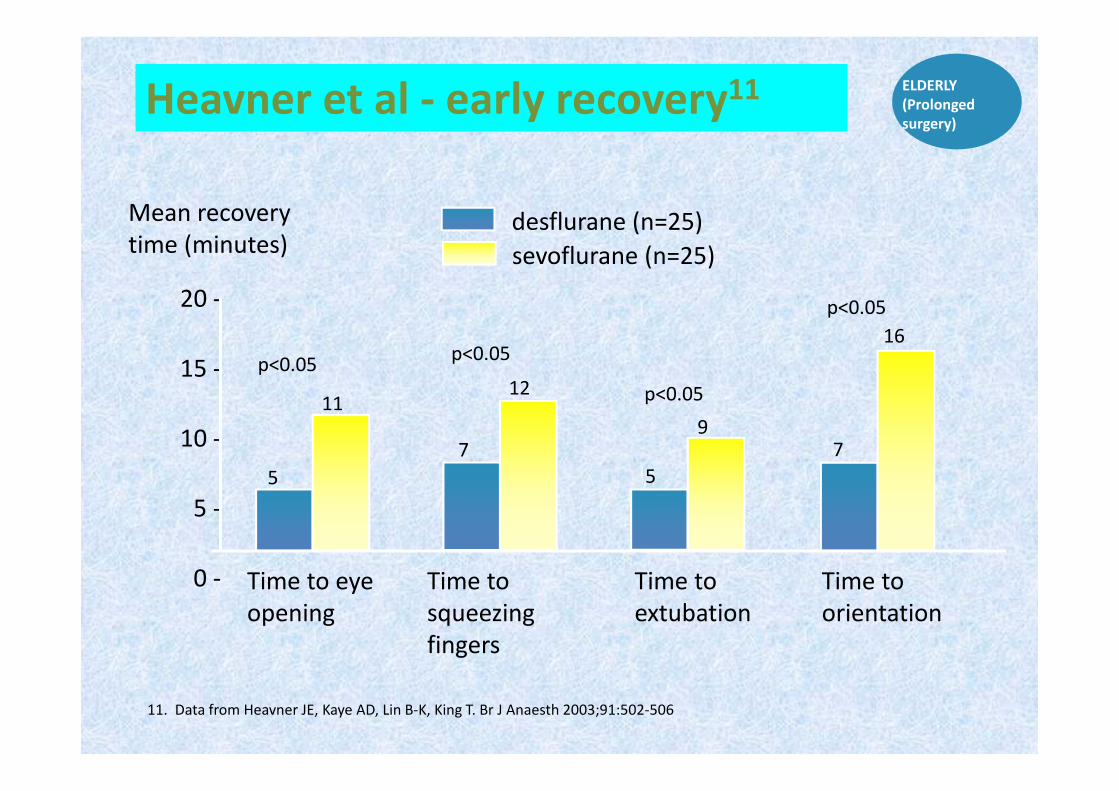
Heavner et al - early recovery11
11. Data from Heavner JE, Kaye AD, Lin B-K, King T. Br J Anaesth 2003;91:502-506
ELDERLY
(Prolonged
surgery)
Time to eye
opening
Time to
extubation
Time to
squeezing
fingers
20 -
15 -
10 -
5 -
0 -
5
11
p<0.05
Mean recovery
time (minutes) sevoflurane (n=25)
7
12
p<0.05
5
9
p<0.05
7
16
p<0.05
Time to
orientation
desflurane (n=25)
Spinal
surgery
• Surgical procedures on the
vertebral column carry a risk of
spinal cord damage, which must
be detected early so it can be
surgically revised9
• Paraplegia is one of the most
feared complications. The ‘gold-
standard’ test involves waking the
patient intraoperatively 9
• Desflurane is particularly useful
for spinal surgery as it gives fast
awakening times 9. Grottke O, Dietrich P J, Wiegels S, Wappler F. Anesth Analg 2004;99(5):1521-1527
SPINAL
SURGERY
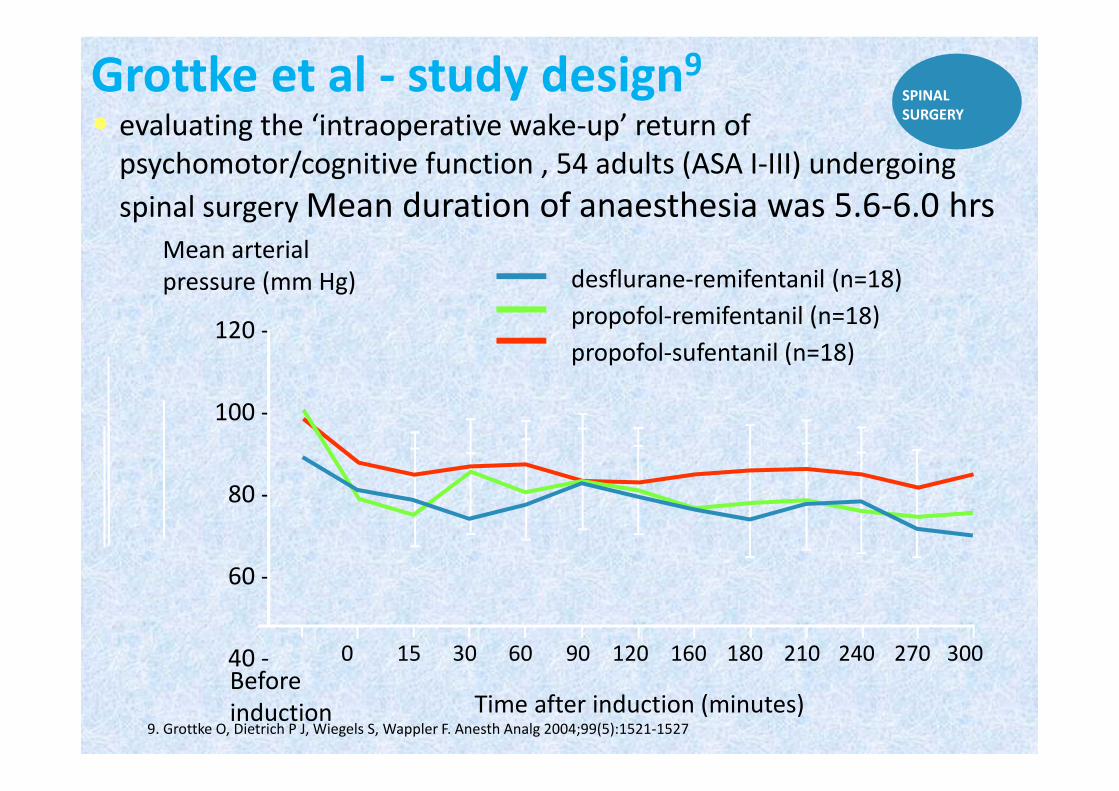
Grottke et al - study design9
• evaluating the ‘intraoperative wake-up’ return of
psychomotor/cognitive function , 54 adults (ASA I-III) undergoing
spinal surgery Mean duration of anaesthesia was 5.6-6.0 hrs
9. Grottke O, Dietrich P J, Wiegels S, Wappler F. Anesth Analg 2004;99(5):1521-1527
SPINAL
SURGERY
Before
induction
120 -
100 -
80 -
60 -
40 -
desflurane-remifentanil (n=18)
propofol-remifentanil (n=18)
propofol-sufentanil (n=18)
Mean arterial
pressure (mm Hg)
Time after induction (minutes)
0 15 30 60 90 120 160 180 240 270 300210
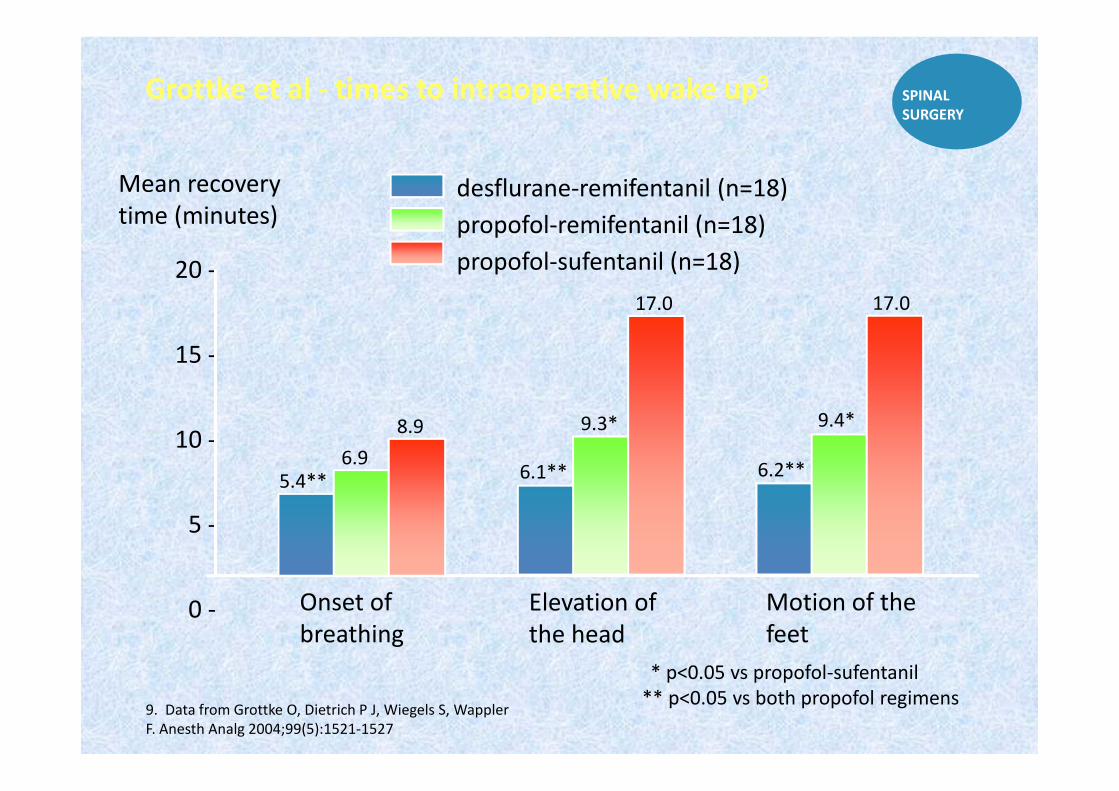
Grottke et al - times to intraoperative wake up9
9. Data from Grottke O, Dietrich P J, Wiegels S, Wappler
F. Anesth Analg 2004;99(5):1521-1527
SPINAL
SURGERY
Onset of
breathing
20 -
15 -
10 -
5 -
0 -
5.4**6.9
Mean recovery
time (minutes)desflurane-remifentanil (n=18)
propofol-remifentanil (n=18)
propofol-sufentanil (n=18)
Elevation of
the head
Motion of the
feet
* p<0.05 vs propofol-sufentanil
** p<0.05 vs both propofol regimens
8.9
6.1**
9.3*
17.0
6.2**
17.0
9.4*
Pulmonary surgery
3. Dupont J, Tavernier B, Ghosez Y, et al. Br J Anaesth 1999;82:355-359
• For example, thoracotomy,
pulmonary lobectomy or
pneumonectomy
• Rapid emergence from
anaesthesia is highly desirable
in order to allow tracheal
extubation with no residual
ventilatory depression3
• Desflurane gives rapid
emergence and early return
of cognitive function3
PULMONARY
SURGERY
Dupont et al - study design3
3. Dupont J, Tavernier B, Ghosez Y, et al. Br J Anaesth 1999;82:355-359
• Studied recovery profiles in 100 adult patients (mostly
ASA II-III) undergoing pulmonary lobectomy or
pneumonectomy
• Maintenance: desflurane, sevoflurane or isoflurane*
• The mean duration of surgery: 163-182 min
* Adjusted to maintain mean arterial pressure and heart rate within 20% of baseline values.
At the last skin suture, the volatile anaesthetic was stopped and ventilation with 100% oxygen at
10L/min was given until end-tidal volatile anaesthetic concentration was <0.1%
PULMONARY
SURGERY
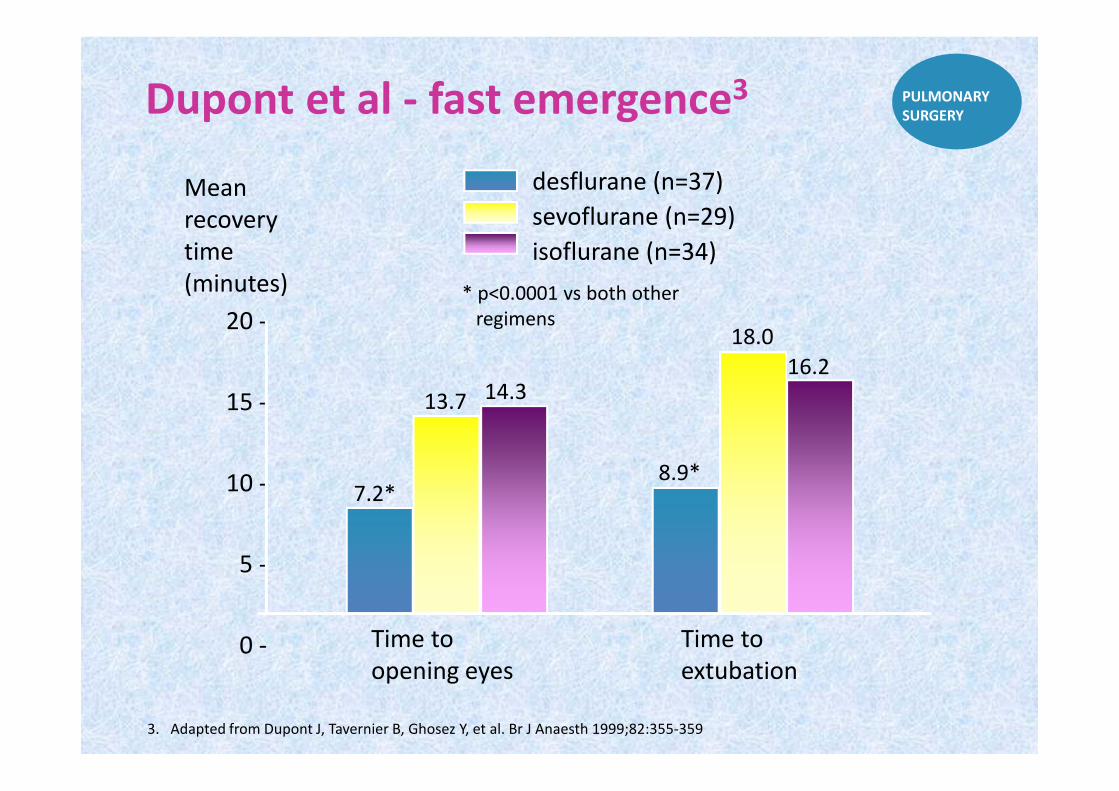
Dupont et al - fast emergence3
3. Adapted from Dupont J, Tavernier B, Ghosez Y, et al. Br J Anaesth 1999;82:355-359
PULMONARY
SURGERY
Time to
opening eyes
20 -
15 -
10 -
5 -
0 - Time to
extubation
Mean
recovery
time
(minutes) * p<0.0001 vs both other
regimens
7.2*
13.7 14.3
desflurane (n=37)
sevoflurane (n=29)
isoflurane (n=34)
8.9*
18.0
16.2
Maintenance anaesthesia in children
•Desflurane is not recommended
for induction in children, but
can be used for maintenance
after induction by other means
•Children may experience
agitation during emergence
from a potent inhaled
anaesthetic17
17. Mayer J, Boldt J, Rohm KD, et al. Anesth Analg 2006;102:400-404
CHILDREN
(Maintenance)
Mayer et al - study design17
• 38 children (1-7 yrs) undergoing minor elective ENT
surgery
• Premedication: Rectal paracetamol 60 min before
induction and midazolam 30 min before induction
• Induction: Mask induction with sevoflurane
• Maintenance: desflurane or sevoflurane (each at 1.0 ±
0.2 MAC, age-adjusted) with 50% N2O/O2 at 1L/min
• Fresh gas flow was increased to 12L/min on
discontinuation of each anaesthetic at the end of surgery
17. Mayer J, Boldt J, Rohm KD, et al. Anesth
Analg 2006;102:400-404
CHILDREN
(Maintenance)
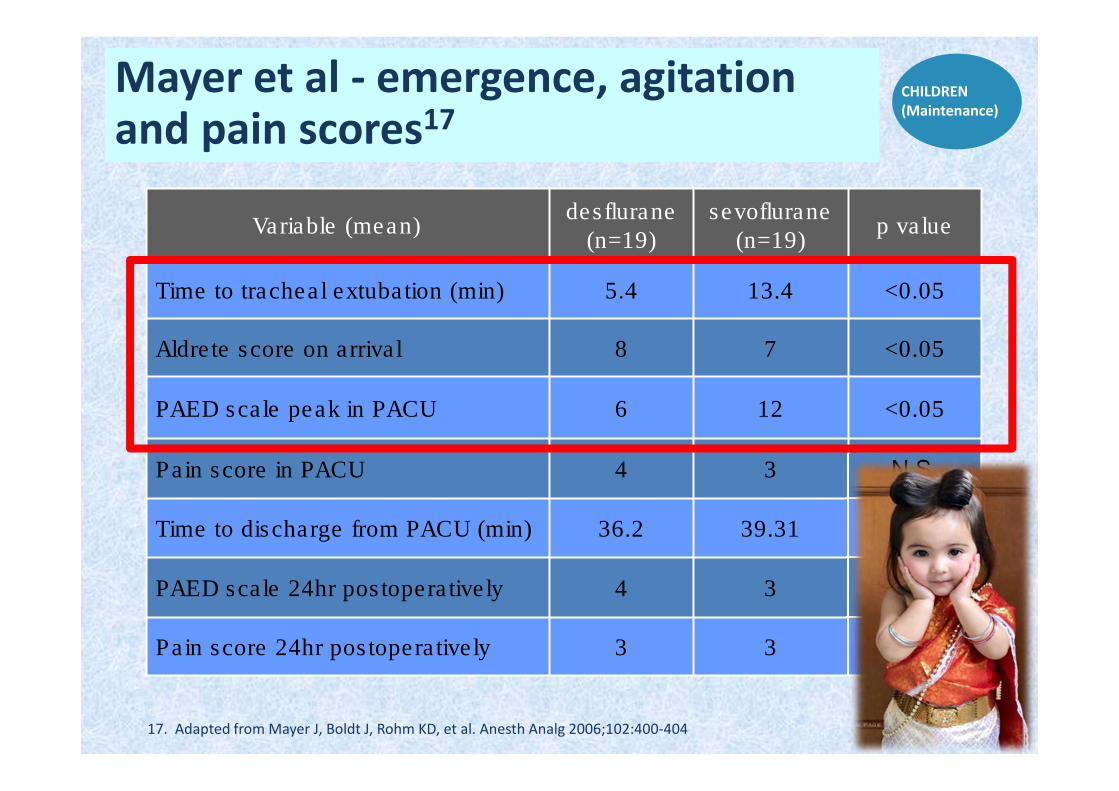
17. Adapted from Mayer J, Boldt J, Rohm KD, et al. Anesth Analg 2006;102:400-404
Variable (mean)desflurane
(n=19)
sevoflurane
(n=19)p value
Time to tracheal extubation (min) 5.4 13.4 <0.05
Aldrete score on arrival 8 7 <0.05
PAED scale peak in PACU 6 12 <0.05
Pain score in PACU 4 3 N.S.
Time to discharge from PACU (min) 36.2 39.31 N.S.
PAED scale 24hr postoperatively 4 3 N.S.
Pain score 24hr postoperatively 3 3 N.S.
Mayer et al - emergence, agitation and pain scores17
CHILDREN
(Maintenance)
17. Mayer J, Boldt J, Rohm KD, et al. Anesth Analg 2006;102:400-
404
28. Cole JW, Murray DJ, McAllister JD, Hirshberg GE. Paed
Anaesth 2002;12:442-447
29. Cohen IT, Finkel JC, Hannallah RS, et al. Paed Anaesth
2003;13:63-67
30. Valley RD, Freid EB, Bailey AG, et al. Anesth Analg
2003;96:1320-1324
31. Demirbilek S, Togal T, Cicek M, et al. Eur J Anaesthesiol
2004;21:538-542
32. Cohen IT, Finkel JC, Hannallah RS, et al. Anesth Analg
2002;94:1178-1181
33. Sikich N, Lerman J. Anesthesiology 2004;100:1138-1145
“ In conclusion, the use of desflurane for maintenance
of anaesthesia after sevoflurane induction in children
is associated with less severe emergence agitation and
faster emergence times.”
Mayer et al - conclusions17CHILDREN
(Maintenance)
Other studies show different results,
may be due to the usage of scores that
have never been validated for
emergence agitation and/or not
providing a validated threshold value in
the PAED scale to indicate emergence
agitation, thus no conclusions can be
drawn with respect to its incidence.
28-32
33
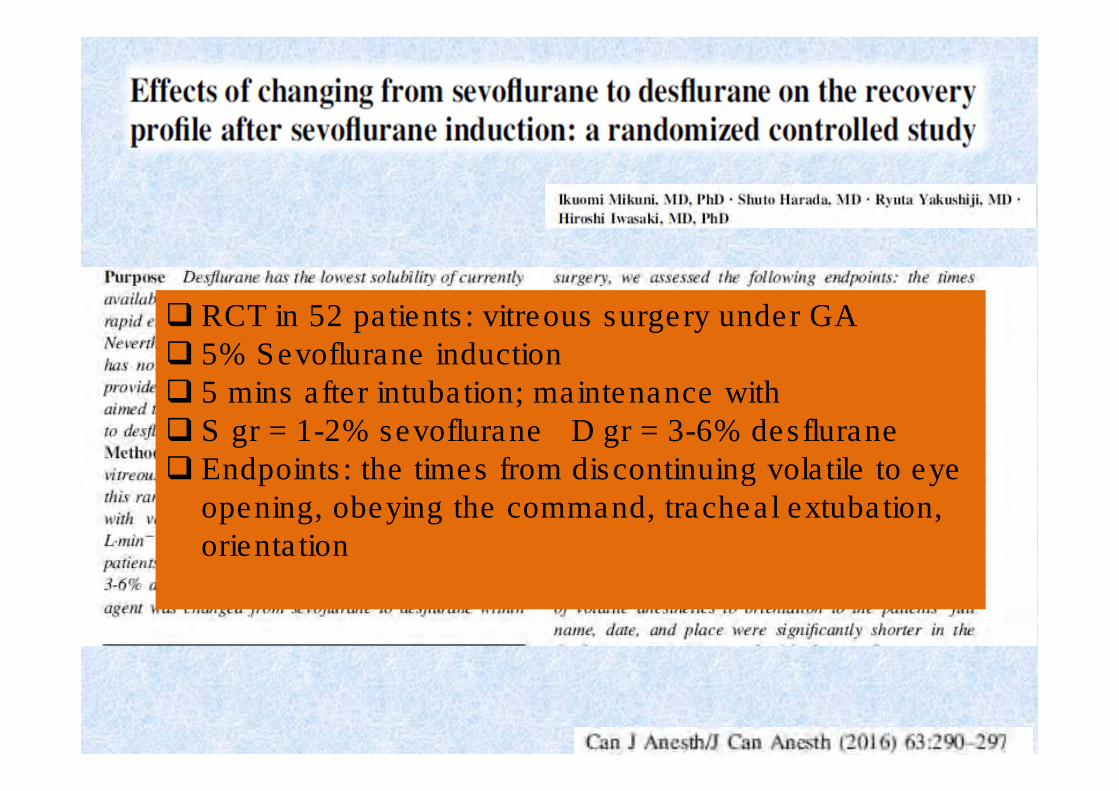
� RCT in 52 patients: vitreous surgery under GA
� 5% Sevoflurane induction
� 5 mins after intubation; maintenance with
� S gr = 1-2% sevoflurane D gr = 3-6% desflurane
� Endpoints: the times from discontinuing volatile to eye
opening, obeying the command, tracheal extubation,
orientation
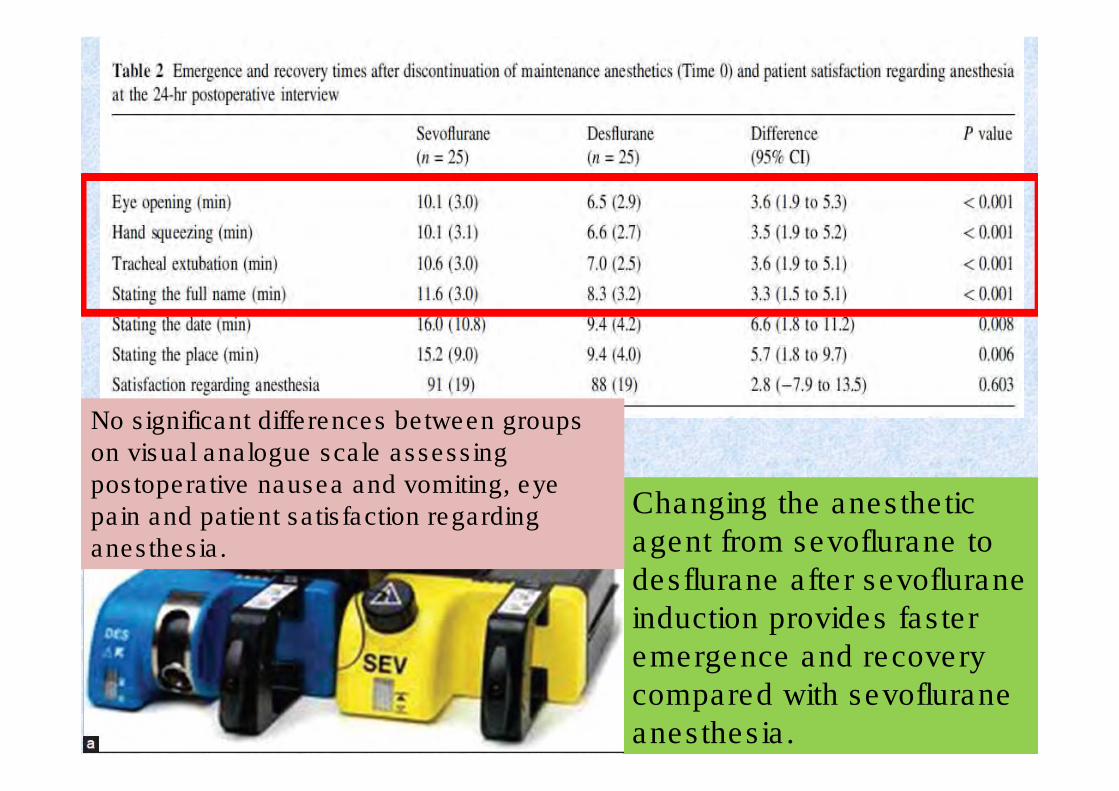
Changing the anesthetic
agent from sevoflurane to
desflurane after sevoflurane
induction provides faster
emergence and recovery
compared with sevoflurane
anesthesia.
No significant differences between groups on visual analogue scale assessing postoperative nausea and vomiting, eye pain and patient satisfaction regarding anesthesia.
A Comparison of Desflurane Inhalation and Propofol TCI
Regimen for Temporal Lobectomy: Early Recovery, Cognitive
Functions and Costs
Indrambarya T,et al. Thailand
aim of the study was to compare the time of
recovery, evaluate the cognitive function,
postoperative pain, PONV and costs of low flow
desflurane inhalation
and propofol TCI regimen
in patients undergoing
craniotomy for
temporal lobectomy
at Chulalongkorn
University Hospital
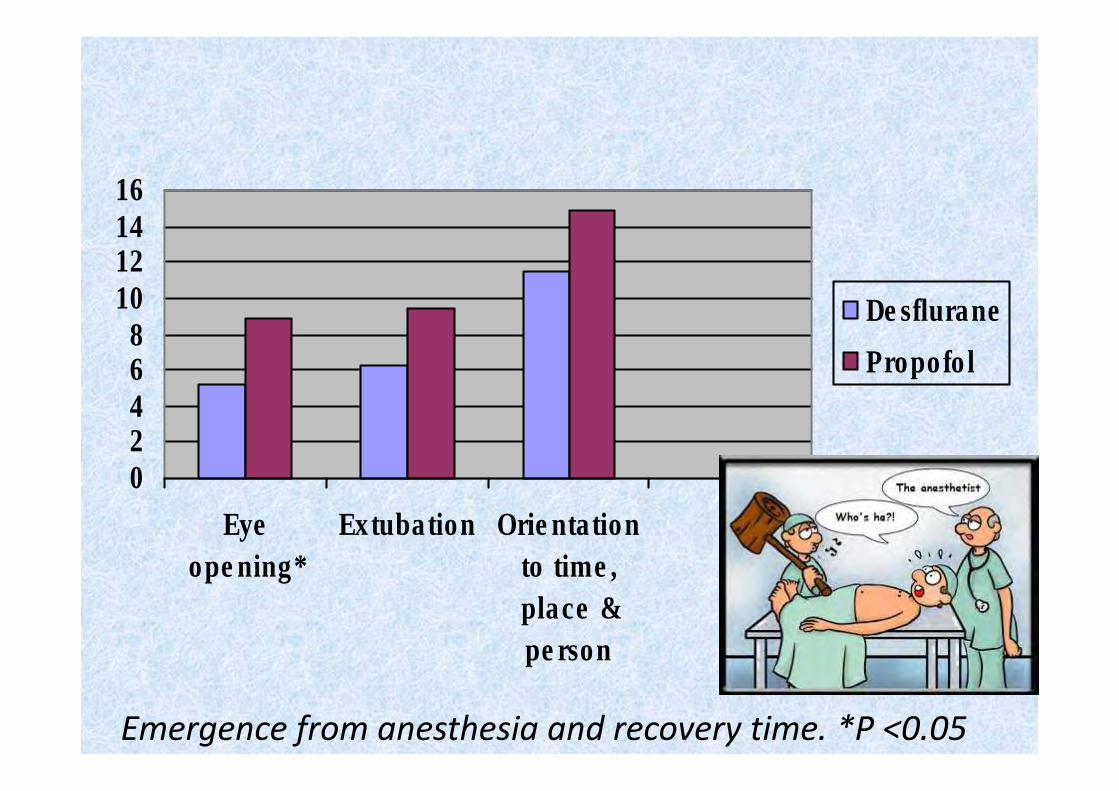
02468
10121416
Eye
opening*
Extubation Orientation
to time,
place &
person
Desflurane
Propofol
Emergence from anesthesia and recovery time. *P <0.05
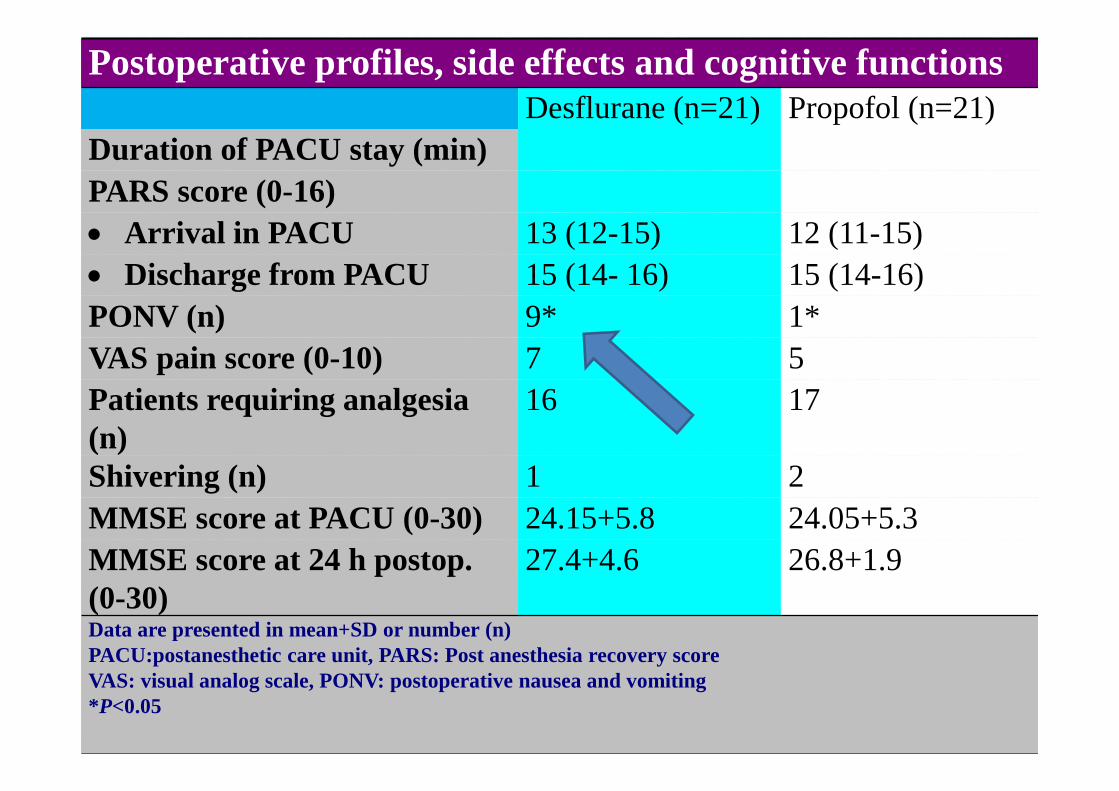
Postoperative profiles, side effects and cognitive functions
Desflurane (n=21) Propofol (n=21)
Duration of PACU stay (min)
PARS score (0-16)
• Arrival in PACU 13 (12-15) 12 (11-15)
• Discharge from PACU 15 (14- 16) 15 (14-16)
PONV (n) 9* 1*
VAS pain score (0-10) 7 5
Patients requiring analgesia
(n)
16 17
Shivering (n) 1 2
MMSE score at PACU (0-30) 24.15+5.8 24.05+5.3
MMSE score at 24 h postop.
(0-30)
27.4+4.6 26.8+1.9
Data are presented in mean+SD or number (n)
PACU:postanesthetic care unit, PARS: Post anesthesia recovery score
VAS: visual analog scale, PONV: postoperative nausea and vomiting
*P<0.05
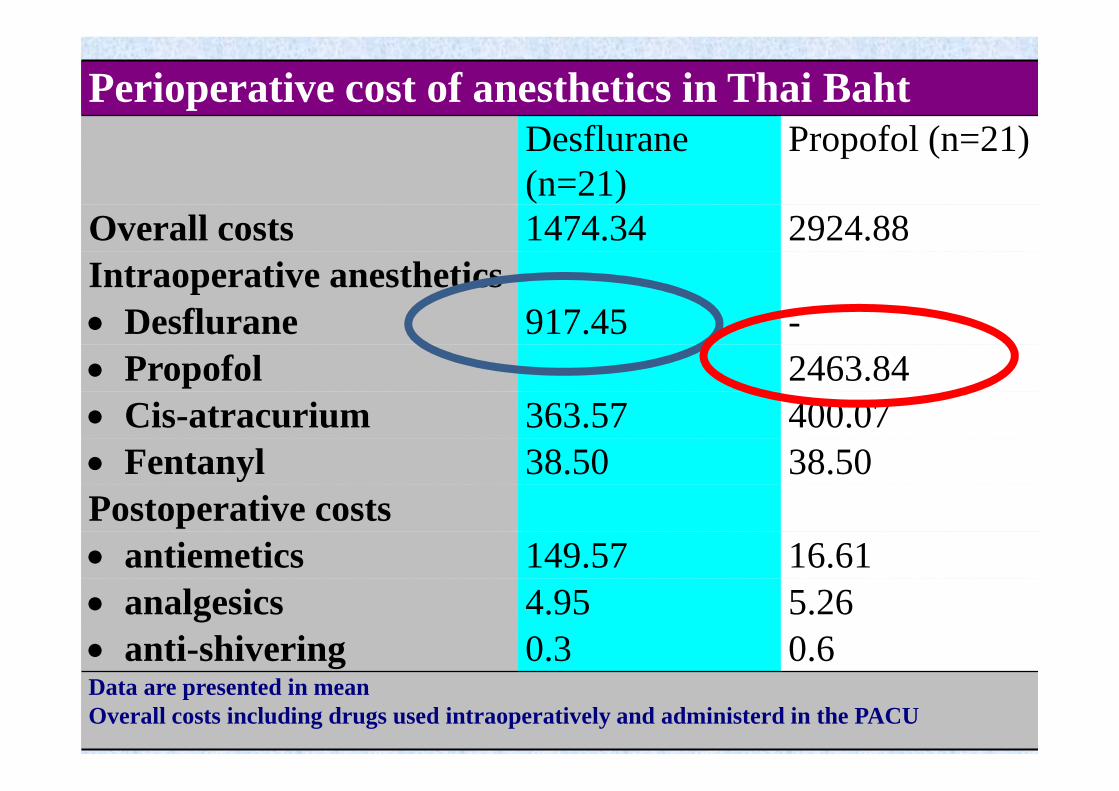
Perioperative cost of anesthetics in Thai Baht
Desflurane
(n=21)
Propofol (n=21)
Overall costs 1474.34 2924.88
Intraoperative anesthetics
• Desflurane 917.45 -
• Propofol - 2463.84
• Cis-atracurium 363.57 400.07
• Fentanyl 38.50 38.50
Postoperative costs
• antiemetics 149.57 16.61
• analgesics 4.95 5.26
• anti-shivering 0.3 0.6Data are presented in mean
Overall costs including drugs used intraoperatively and administerd in the PACU
Selection of anesthetic agents should
be based not only on safety and
efficacy, but also economic profiles.
Patients in both desflurane and propofol group
showed similar emergence and recovery profiles.
However, costs of propofol TCI regimen were
significant higher than desflurane inhalation
group.

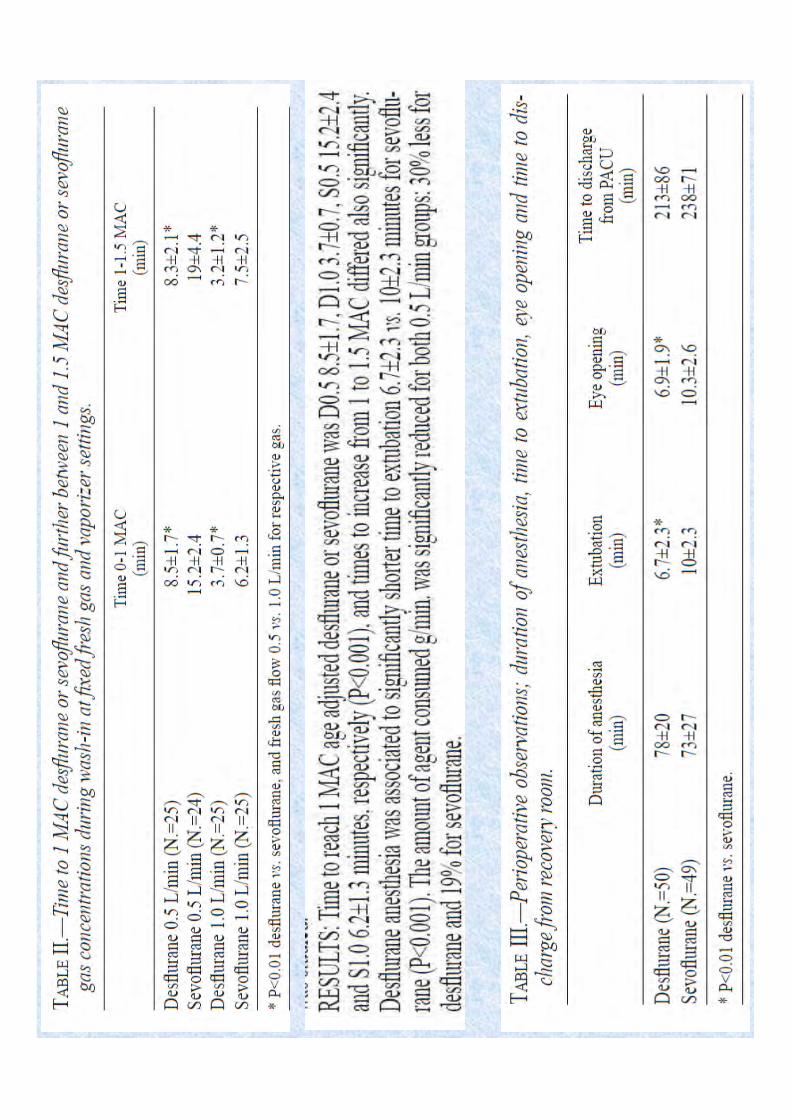
Low-flow anaesthesia is characterized by economy in the
use of anaesthetic agents and reduced atmospheric
pollution.
As the carrier gas flow rate is reduced, an
increasing disparity develops between the
fresh gas and the inspired gas mixtures. The
fresh gas composition increasingly needs to
reflect the patient’s uptake of its components.
A progressive reduction in a
practitioner’s gas flow rates permits
safe and relaxed self-learning of this
technique.

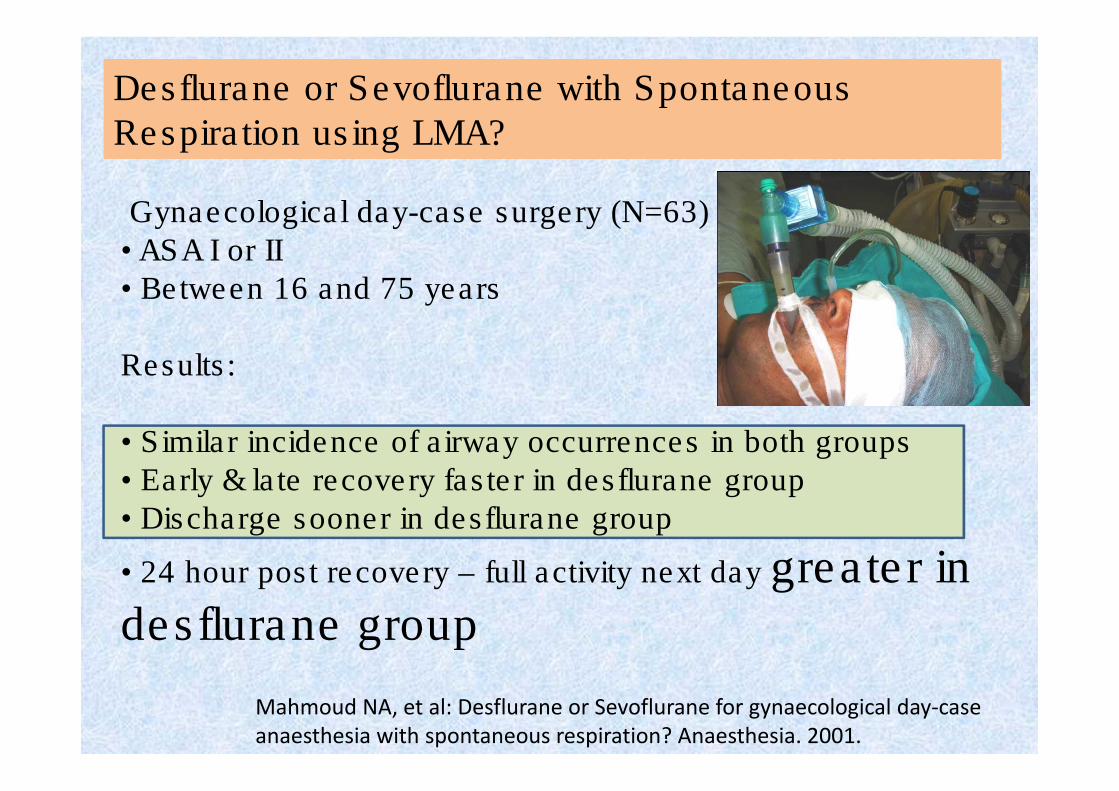
Gynaecological day-case surgery (N=63)
• ASA I or II
• Between 16 and 75 years
Results:
• Similar incidence of airway occurrences in both groups
• Early & late recovery faster in desflurane group
• Discharge sooner in desflurane group
• 24 hour post recovery – full activity next day greater in
desflurane group
Mahmoud NA, et al: Desflurane or Sevoflurane for gynaecological day-case
anaesthesia with spontaneous respiration? Anaesthesia. 2001.
Desflurane or Sevoflurane with Spontaneous
Respiration using LMA?
Low levels of pressure support ventilation well
tolerated without leak;
decrease end-tidal CO2, increase SaO2 slightly
LMA and Ventilation
Work of breathing lower than
breathing
spontaneously through 8.0 ETT
Joshi GP et al. J Clin Anes; 10:268, 1998
• Brimacombe J et al. Anesthesiology; 92:1621, 2000
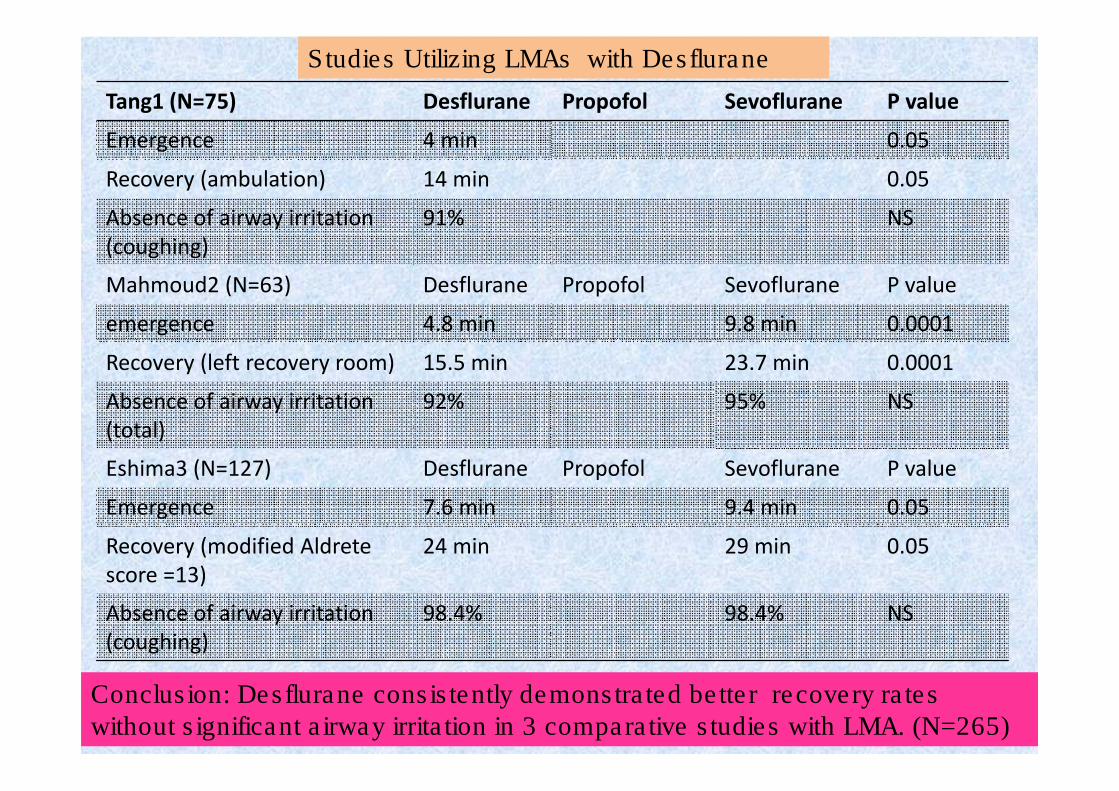
Studies Utilizing LMAs with Desflurane
Tang1 (N=75) Desflurane Propofol Sevoflurane P value
Emergence 4 min 0.05
Recovery (ambulation) 14 min 0.05
Absence of airway irritation
(coughing)
91% NS
Mahmoud2 (N=63) Desflurane Propofol Sevoflurane P value
emergence 4.8 min 9.8 min 0.0001
Recovery (left recovery room) 15.5 min 23.7 min 0.0001
Absence of airway irritation
(total)
92% 95% NS
Eshima3 (N=127) Desflurane Propofol Sevoflurane P value
Emergence 7.6 min 9.4 min 0.05
Recovery (modified Aldrete
score =13)
24 min 29 min 0.05
Absence of airway irritation
(coughing)
98.4% 98.4% NS
1. Tang et al. Anesth Analg 2001;92:95-99.2. Mahmoud et al. Anes. 2001;56:171-182.3. Eshima et al. Analg. 2003;96:701-705.
Conclusion: Desflurane consistently demonstrated better recovery rates without significant airway irritation in 3 comparative studies with LMA. (N=265)
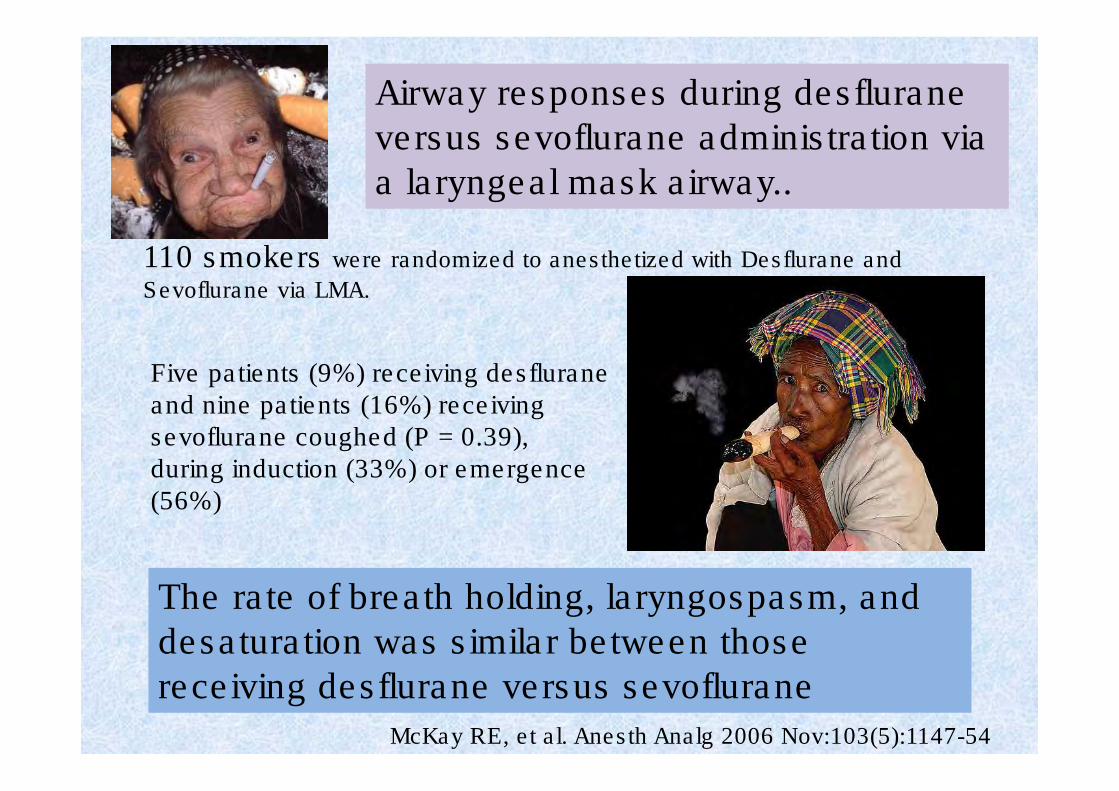
Airway responses during desflurane
versus sevoflurane administration via
a laryngeal mask airway..
110 smokers were randomized to anesthetized with Desflurane and
Sevoflurane via LMA.
Five patients (9%) receiving desfluraneand nine patients (16%) receiving sevoflurane coughed (P = 0.39), during induction (33%) or emergence (56%)
McKay RE, et al. Anesth Analg 2006 Nov:103(5):1147-54
The rate of breath holding, laryngospasm, and
desaturation was similar between those
receiving desflurane versus sevoflurane
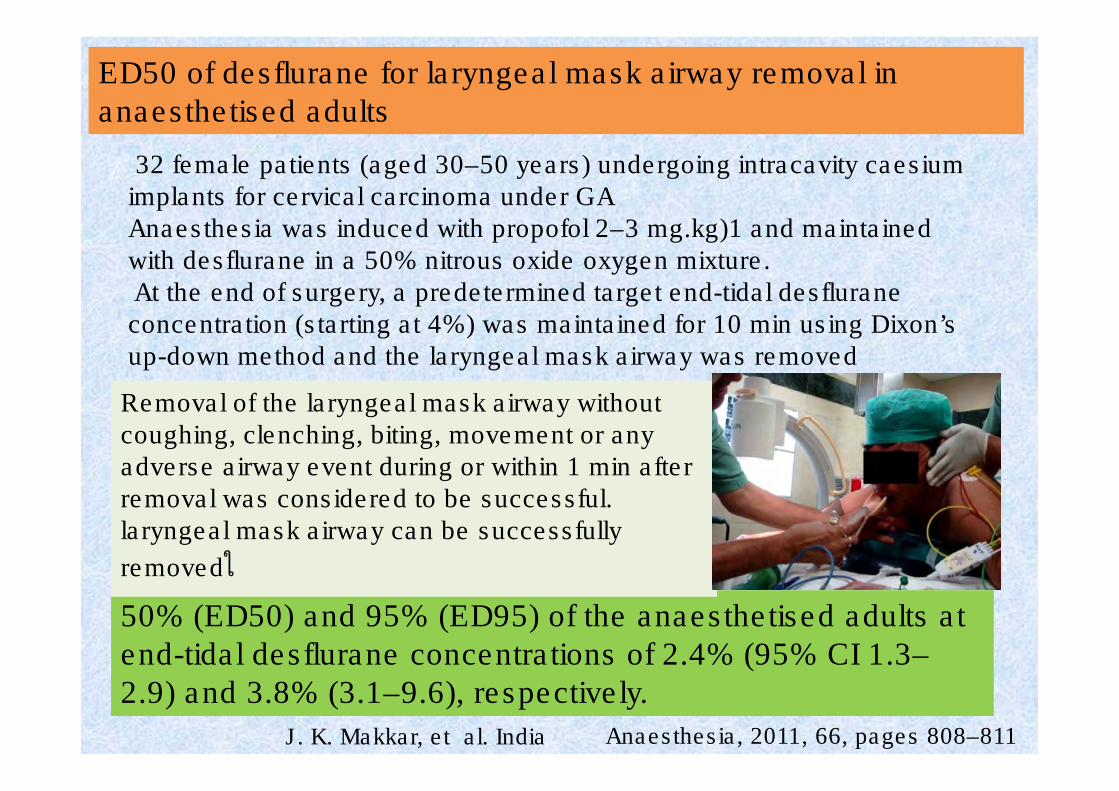
32 female patients (aged 30–50 years) undergoing intracavity caesiumimplants for cervical carcinoma under GAAnaesthesia was induced with propofol 2–3 mg.kg)1 and maintained with desflurane in a 50% nitrous oxide oxygen mixture.At the end of surgery, a predetermined target end-tidal desfluraneconcentration (starting at 4%) was maintained for 10 min using Dixon’s up-down method and the laryngeal mask airway was removed
ED50 of desflurane for laryngeal mask airway removal in
anaesthetised adults
Anaesthesia, 2011, 66, pages 808–811 J. K. Makkar, et al. India
50% (ED50) and 95% (ED95) of the anaesthetised adults at
end-tidal desflurane concentrations of 2.4% (95% CI 1.3–
2.9) and 3.8% (3.1–9.6), respectively.
Removal of the laryngeal mask airway without coughing, clenching, biting, movement or any adverse airway event during or within 1 min after removal was considered to be successful. laryngeal mask airway can be successfully
removedใ
25 children aged 2-10 years, undergoing elective cataract surgery.. A subtenon block was administered in all children before surgical incision. Desflurane was used for maintenance of anesthesia. Predetermined end tidal concentration of desflurane was maintained for 10 min at the end of surgery before LMA removal was attempted Patient responses to LMA removal were classified as “movement” or “no movement.”
.Effective dose 50 of desflurane for laryngeal mask airway removal in anaesthetized children in cataract surgeries
with subtenon block
Sameer Sethi, Saudi Journal of Anesthesia Vol. 9, Issue 1, January-March 2015
Laryngeal mask airway
removal can be
successfully accomplished
in 50% and 95%
anesthetized children at
3.6% and 4.65% end-tidal
desflurane concentration
Desflurane/fentanyl compared with sevoflurane/fentanyl
on awakening and quality of recovery in outpatient
surgery using a laryngeal mask airway: A randomized, double-blinded controlled trial
to compare time to awakening and upper airway morbidity between desflurane and sevoflurane using a Laryngeal Mask Airway (LMA) and a balanced anesthetic regimen inclusive of opioids. Desflurane retains faster awakening properties than does sevoflurane when used in combination with fentanyl as part of anesthetic maintenance in outpatient surgery with a LMA
Journal of Clinical Anesthesia, 2013
De Oliveira GS, et al.
. The balanced anesthetic maintenance regimen seems to reduce the potential airway reactivity properties of desflurane.
A systematic review of RCTs of patients receiving general
anesthesia with a LMA was performed. Sevoflurane and
desflurane were used for maintenance of anesthesia in the
RCTs. A wide search was performed to identify RCTs
comparing desflurane with sevoflurane on the incidence of
upper respiratory adverse events in patients undergoing
surgery with a LMA. The primary outcomes were incidence of
cough and laryngospasm. A random-effects model was used
to perform quantitative analysis.
The effect of sevoflurane versus desflurane on the
incidence of upper respiratory morbidity in patients
undergoing general anesthesia with a Laryngeal Mask Airway: a meta-analysis of randomized controlled trials☆
Gildasio S. de Oliveira Jr.
Journal of Clinical Anesthesia 25(6),September 2013, Pages 452–458
Main ResultsData originating from 7 studies comprising 657 subjects were analyzed. The confidence interval (CI) was large relative to a clinically significant difference in the incidence of overall cough and laryngospasm in patients receiving desflurane versus sevoflurane (odds ratio [OR; 95% CI] of 1.44 [0.49 - 4.1] and 3.06 [0.43 - 21.62]), respectively. The incidence of cough at emergence was greater in subjects receiving desflurane compared with sevoflurane (OR [95% CI] of 2.43 [1.2 - 4.7], number needed to harm [NNH] = 9.0); however, the analysis was limited
by the presence of an asymmetric funnel plot suggesting the
possibility of publication bias.
Journal of Clinical Anesthesia 25(6),September 2013, Pages 452–458
There is a lack of evidence that
desflurane causes a greater
incidence of upper airway
adverse events than sevoflurane
in patients undergoing general
anesthesia with a LMA.
A systematic review and meta-analysis of randomised controlled trials (RCTs).
13 RCTs were included and analysed.
There was no difference in the rates of upper airway events between
desflurane and sevoflurane or between desflurane and a control group consisting of
all the other anaesthetics combined.
Comparing desflurane (n = 284) with all other anaesthetic groups (n = 313), the risk ratio [95% confidence interval (95% CI)] was 1.12 (0.63 to 2.02, P = 0.70).
Cough at emergence was only measured in patients receiving desflurane (n = 148) and sevoflurane (n = 146): the risk ratio (95% CI) was 1.49 (0.55 to 4.02, P = 0.43).
Laryngospasm was rare and there was no significant difference in its incidence
when desflurane (n = 262) was compared with all other anaesthetics combined (n = 289; risk ratio 1.03; 95% CI 0.33 to 3.20, P = 0.96).
Desflurane's short emergence time supports fast track anaesthesia. Data on the rate of upper airway complications and emergence time when desflurane is used with laryngeal mask airway (LMA) are controversial and limited.
Afshari A, Wetterslev J. When may systematic reviews and meta-analyses be considered reliable? Eur J Anaesthesiol 2015; 32:85–87.
The times of all emergence variables were significantly
faster in the desflurane group than in all other groups.
When using an LMA, upper airway adverse reactions in
association with desflurane anaesthesia were no different from those noted with sevoflurane, isoflurane or propofol
anaesthesia. Emergence from general anaesthesia with
desflurane is significantly faster than all the other
anaesthetics. Due to interstudy variations and the small size
of the trials, further large-scale, multicentre studies are
required to confirm or refute the results of this meta-analysis.
Afshari A, Wetterslev J. When may systematic reviews and meta-analyses be considered reliable? Eur J Anaesthesiol 2015; 32:85–87.
Pharyngeal Function: The Little ‘Big’ Problem
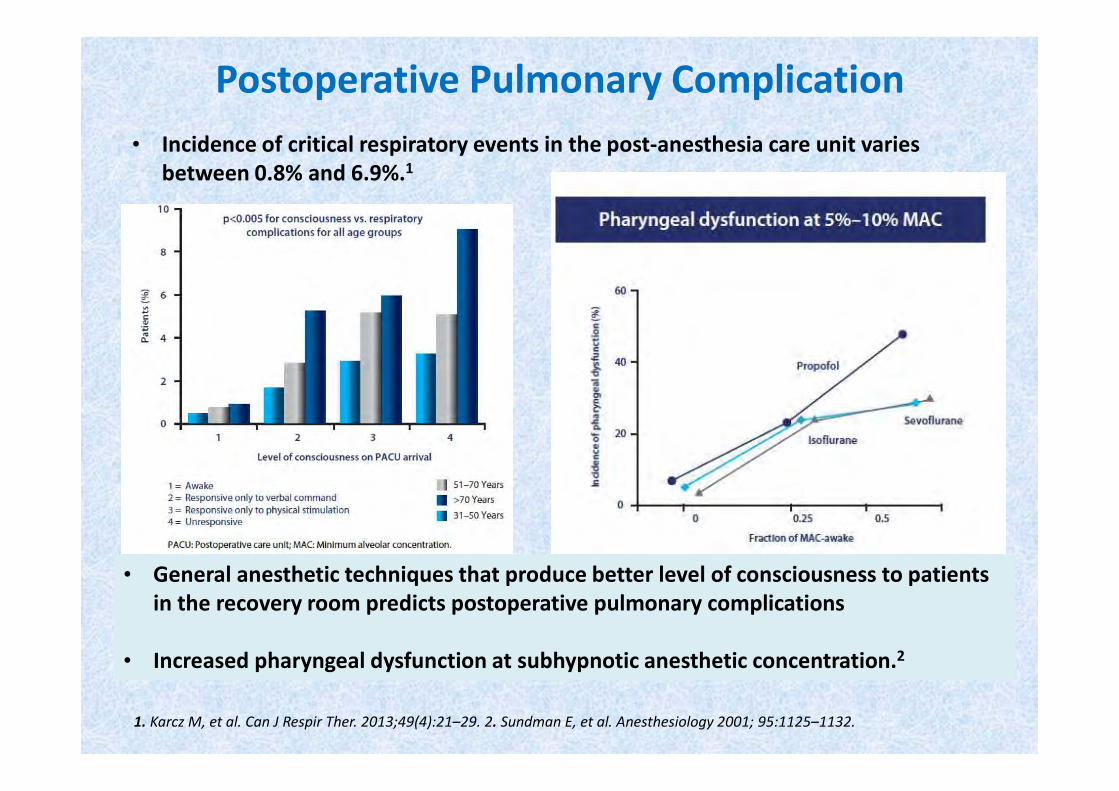
Postoperative Pulmonary Complication
• General anesthetic techniques that produce better level of consciousness to patients
in the recovery room predicts postoperative pulmonary complications
• Increased pharyngeal dysfunction at subhypnotic anesthetic concentration.2
• Incidence of critical respiratory events in the post-anesthesia care unit varies
between 0.8% and 6.9%.1
1. Karcz M, et al. Can J Respir Ther. 2013;49(4):21–29. 2. Sundman E, et al. Anesthesiology 2001; 95:1125–1132.
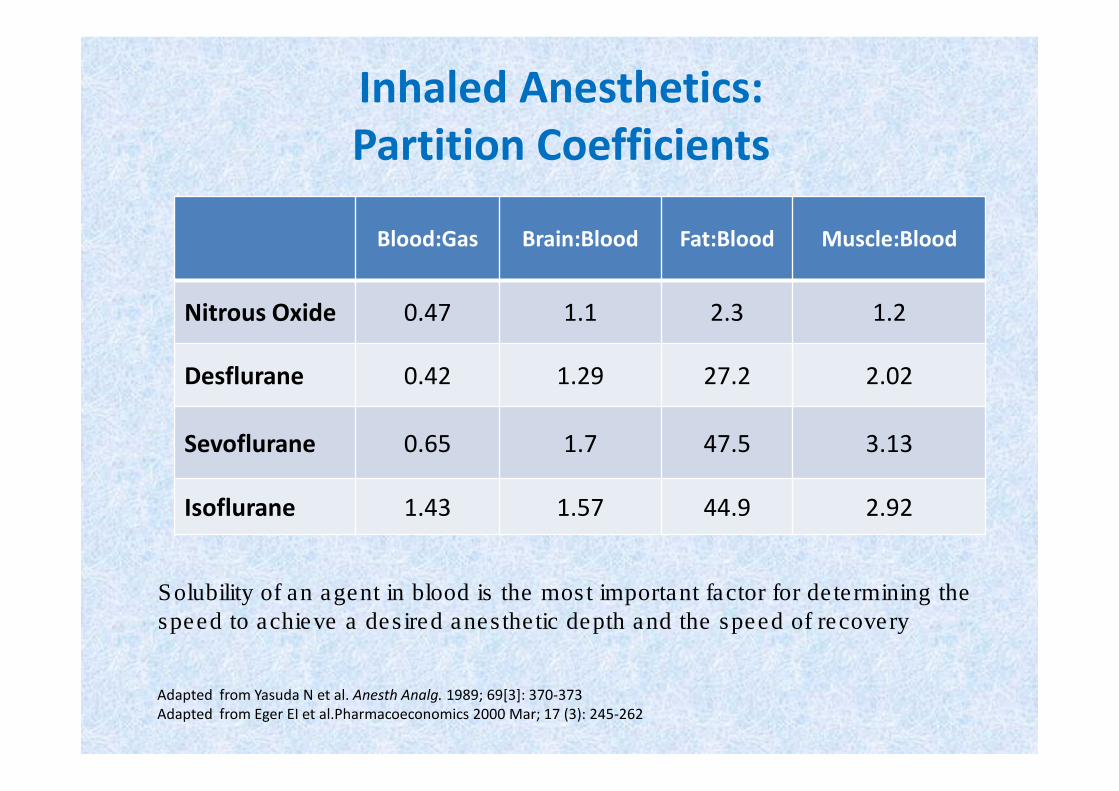
Inhaled Anesthetics:
Partition Coefficients
Blood:Gas Brain:Blood Fat:Blood Muscle:Blood
Nitrous Oxide 0.47 1.1 2.3 1.2
Desflurane 0.42 1.29 27.2 2.02
Sevoflurane 0.65 1.7 47.5 3.13
Isoflurane 1.43 1.57 44.9 2.92
Adapted from Yasuda N et al. Anesth Analg. 1989; 69[3]: 370-373
Adapted from Eger EI et al.Pharmacoeconomics 2000 Mar; 17 (3): 245-262
Solubility of an agent in blood is the most important factor for determining the
speed to achieve a desired anesthetic depth and the speed of recovery
Key Pivots Affecting Airway Reflex Response
• Opioids
• Inhalational Anesthetics
• Neuromuscular Blockers
Desflurane vs Sevoflurane
DAY-CASE SURGERY
• 60 gynaecological day-case patients 16-75 yrs (ASA I-II)
• Induction: metoclopramide, fentanyl, propofol
• Maintenance: desflurane (initially 2-6%) or sevoflurane (initially 0.5-2.0%) in N2O / O2 given by laryngeal mask airway (LMA) in spontaneously breathing patients. Vapour concentrations were adjusted to meet the surgical requirements*
• The mean duration of maintenance anaesthesia in each group
was 18 min
4. Mahmoud NA, Rose DJA, Laurence
AS. Anaesthesia 2001;56:171-174
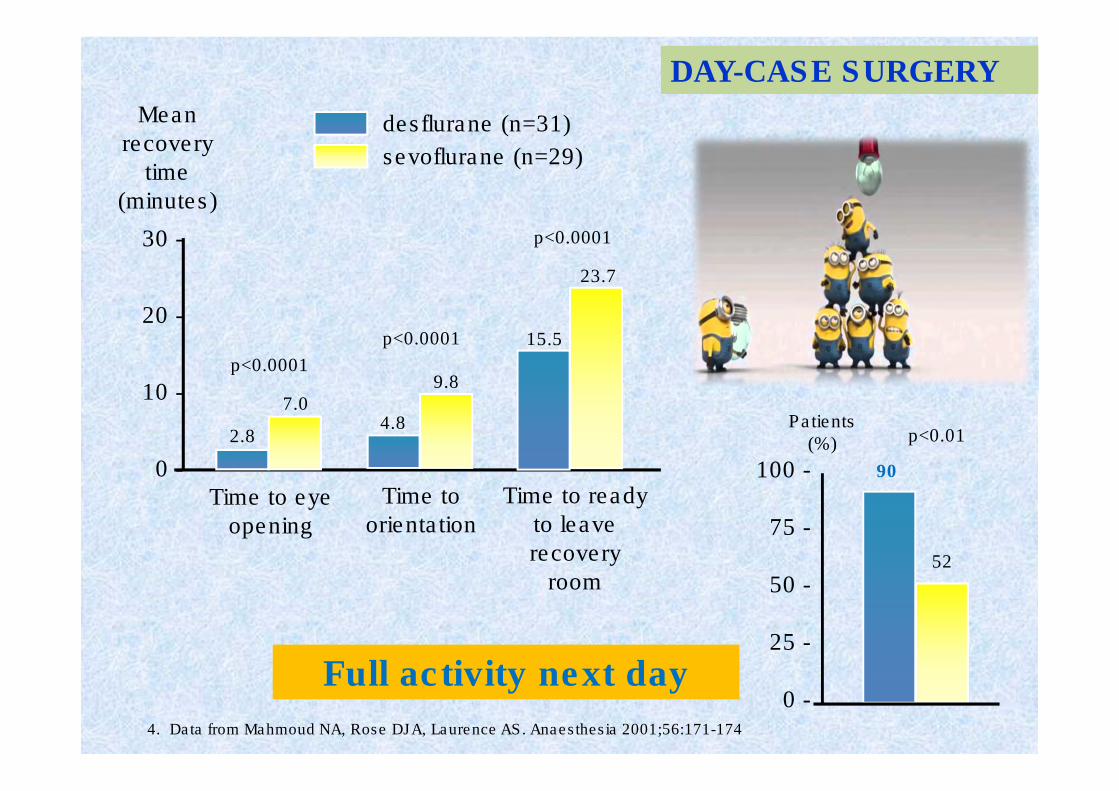
4. Data from Mahmoud NA, Rose DJA, Laurence AS. Anaesthesia 2001;56:171-174
DAY-CASE SURGERY
Time to eye
opening
Time to ready
to leave
recovery
room
Time to
orientation
30 -
20 -
10 -
0 -
2.8
7.0
p<0.0001
Mean
recovery
time
(minutes)
desflurane (n=31)
sevoflurane (n=29)
4.8
9.8
p<0.0001 15.5
23.7
p<0.0001
90
52
Patients(%) p<0.01
100 -
75 -
50 -
25 -
0 -Full activity next day
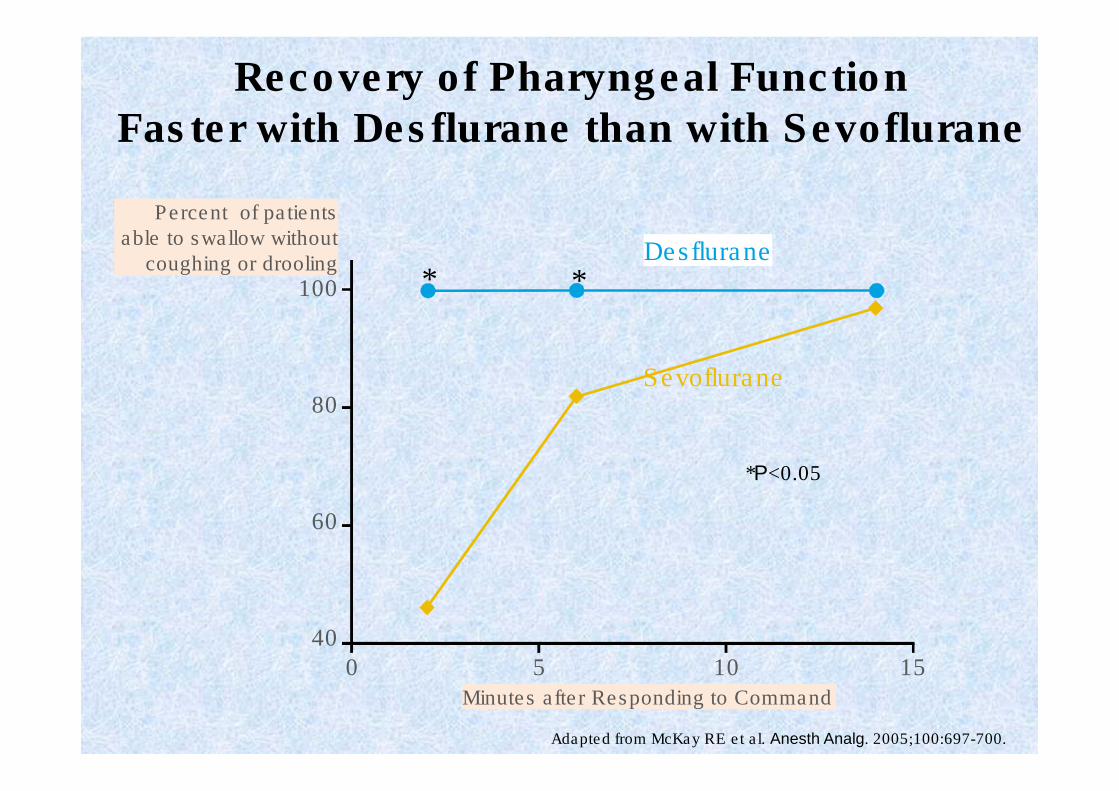
Recovery of Pharyngeal Function Faster with Desflurane than with Sevoflurane
Percent of patients
able to swallow without
coughing or drooling
Adapted from McKay RE et al. Anesth Analg. 2005;100:697-700.
100
80
60
40
0 5 10 15
Minutes after Responding to Command
Desflurane
Sevoflurane
* *
*P<0.05
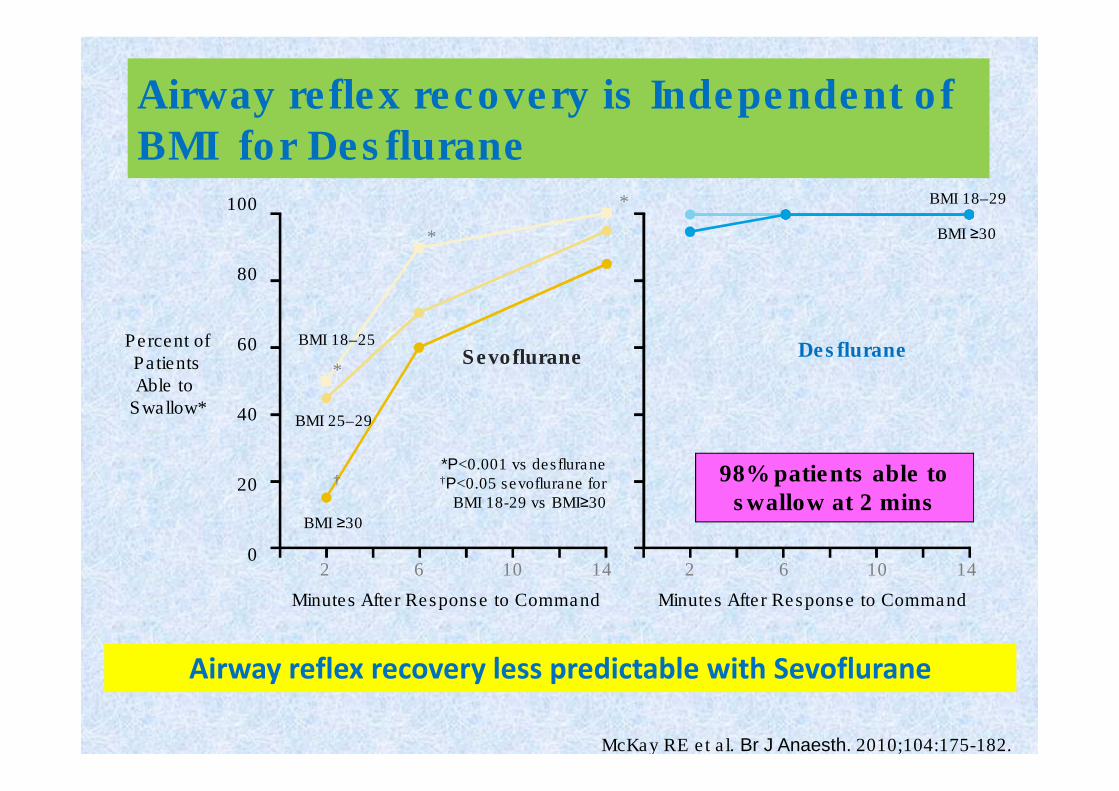
Airway reflex recovery is Independent of BMI for Desflurane
†
Percent ofPatientsAble to
Swallow*
100
80
60
40
20
02 6 10 14 2 6 10 14
*P<0.001 vs desflurane†P<0.05 sevoflurane for
BMI 18-29 vs BMI≥30
Minutes After Response to Command Minutes After Response to Command
Sevoflurane Desflurane
BMI ≥30
BMI 18–29
*
*
*
BMI 18–25
BMI 25–29
BMI ≥30
McKay RE et al. Br J Anaesth. 2010;104:175-182.
Airway reflex recovery less predictable with Sevoflurane
98% patients able to
swallow at 2 mins
Enhanced Recovery:
From Concept to Clinical Practice
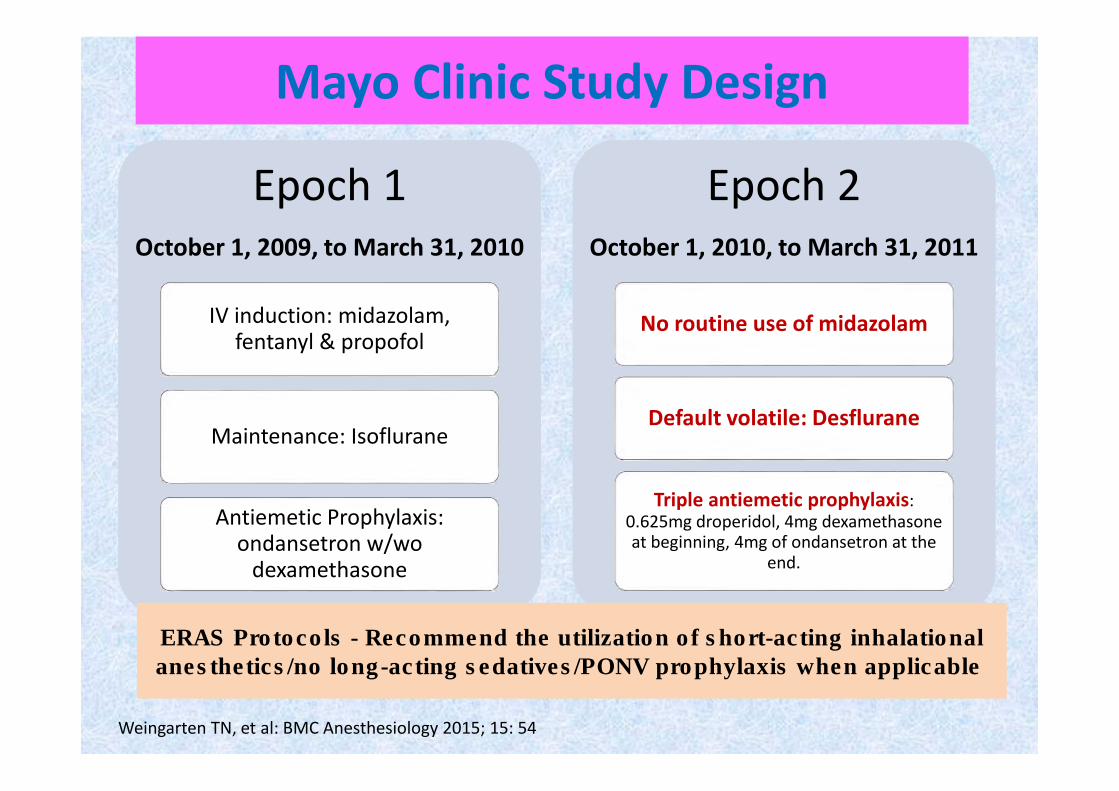
Mayo Clinic Study Design
Epoch 1
October 1, 2009, to March 31, 2010
Epoch 1
October 1, 2009, to March 31, 2010
IV induction: midazolam, fentanyl & propofol
Maintenance: Isoflurane
Antiemetic Prophylaxis: ondansetron w/wo
dexamethasone
Epoch 2
October 1, 2010, to March 31, 2011
Epoch 2
October 1, 2010, to March 31, 2011
No routine use of midazolam
Default volatile: Desflurane
Triple antiemetic prophylaxis:
0.625mg droperidol, 4mg dexamethasone at beginning, 4mg of ondansetron at the
end.
Weingarten TN, et al: BMC Anesthesiology 2015; 15: 54
ERAS Protocols - Recommend the utilization of short-acting inhalational
anesthetics/no long-acting sedatives/PONV prophylaxis when applicable
Weingarten TN, et al: BMC Anesthesiology 2015; 15: 54
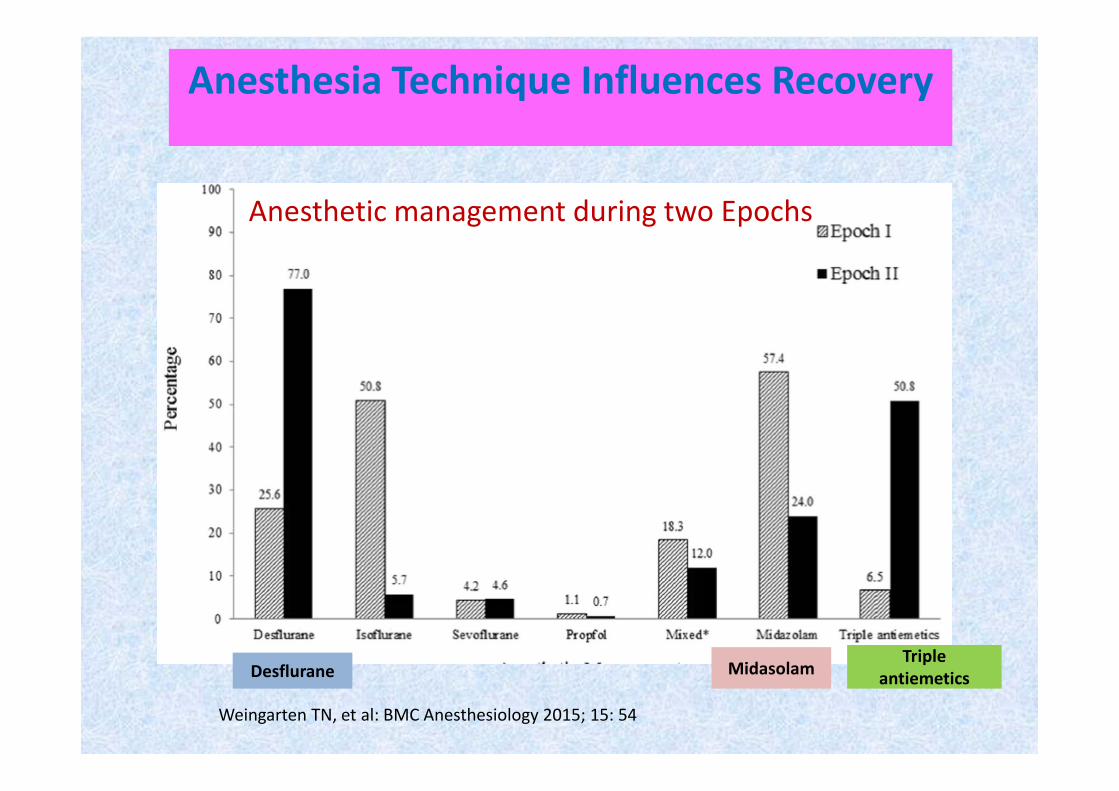
Anesthesia Technique Influences Recovery
Anesthetic management during two Epochs
Desflurane MidasolamTriple
antiemetics
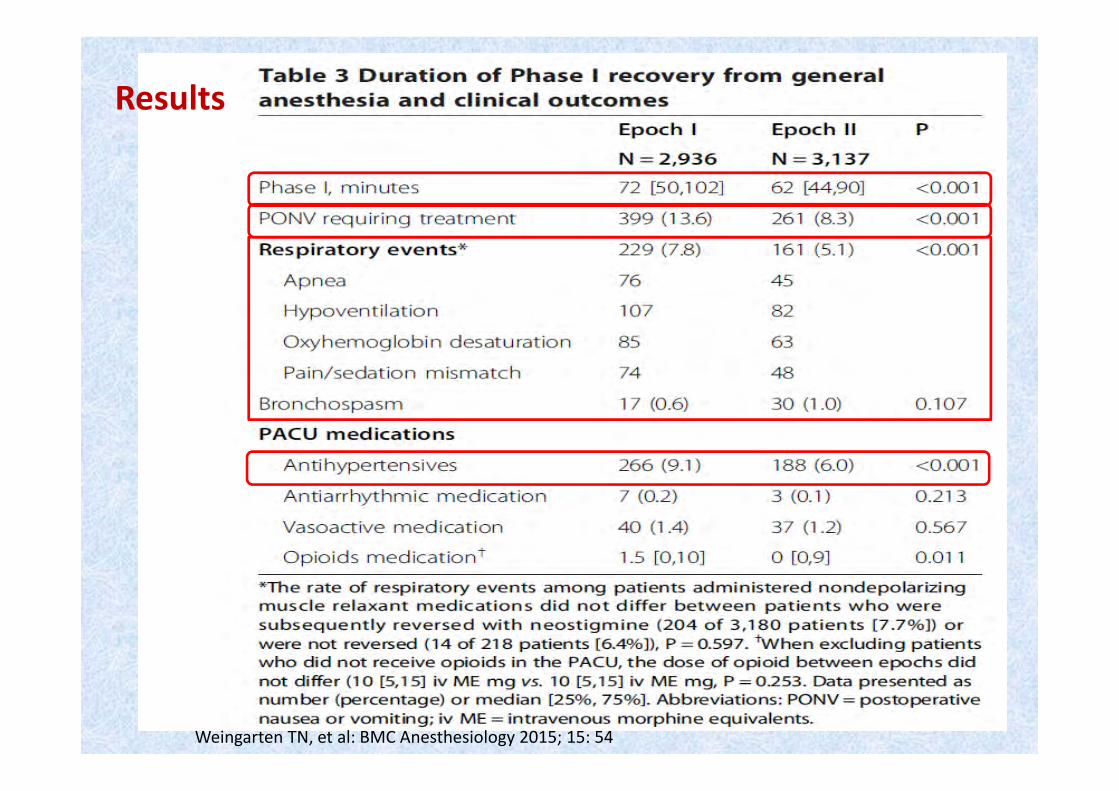
Results
Weingarten TN, et al: BMC Anesthesiology 2015; 15: 54
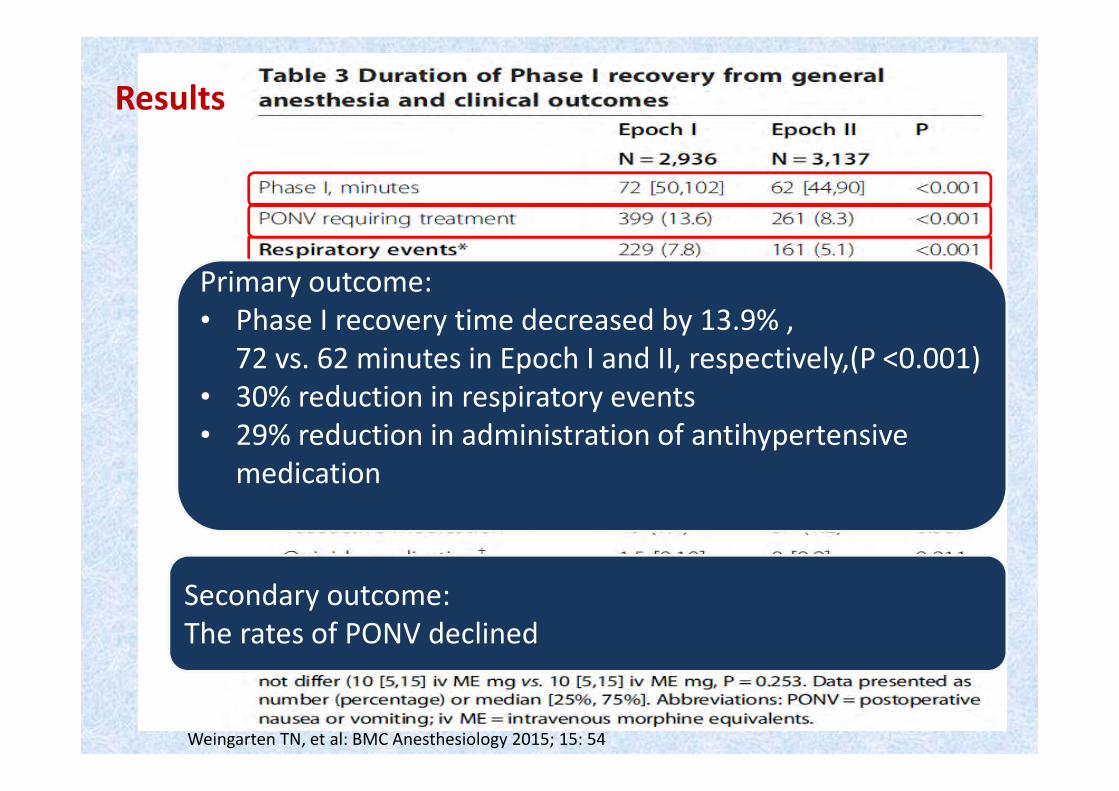
Secondary outcome:
The rates of PONV declined
Results
Primary outcome:
• Phase I recovery time decreased by 13.9% ,
72 vs. 62 minutes in Epoch I and II, respectively,(P <0.001)
• 30% reduction in respiratory events
• 29% reduction in administration of antihypertensive
medication
Weingarten TN, et al: BMC Anesthesiology 2015; 15: 54