Embed Size (px)
Citation preview

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 1/23
Endoscopy Theater
Types of Endoscopy:
There are many types of endoscopy procedures, including:
y Arthroscopy
y Bronchoscopy
y Colonoscopy
y Colposcopy
y Cystoscopy
y ERCP (endoscopic retrograde cholangio-pancreatography)
y EGD (Esophogealgastroduodensoscopy)
y Laparoscopy
y Laryngoscopy
y Proctoscopy
y Thoracoscopy
Colonoscopy Introduction
A colonoscopy is a test to look at the inside of your colon. The colon is the large intestine and the last part of your digestive system.
Its job is to dry, process, and eliminate the waste left after the small intestine has absorbed the nutrients in food. The colon is about
3-5 feet long. It travels from the lower right corner of your abdomen (where the small intestine ends) up to your liver , across your
body to the spleen in the upper left corner and then down to form your rectum and anus.
The doctor will use an instrument called the colonoscope to perform a colonoscopy. It is a long (about 3 ft), thin (about 1 in), flexible
fiberoptic camera that allows the doctor to visualize your entire colon.
Your doctor may order a colonoscopy to investigate many different diseases of the colon.
o Colonoscopy is best known for its use as a screening tool for the early detection of colorectal cancer .
Colorectal cancer is the second leading cause of cancer deaths in the United States.
Colon cancer develops from growths within the wall of the intestine such as polyps or tumors.
These growths often take 5-10 years to develop and may not cause many symptoms.
You may not have any symptoms of colon cancer, but having a close relative with the disease increases your risk for the
disease compared to the general public.
Most people who develop polyps do so after age 50, so the American College of Gastroenterology (the digestive
specialists) recommends screening examinations every 5 years for early detection and removal of these cancer-causing
growths after that age.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 2/23
o Colonoscopy is also used to investigate other diseases of the colon.
Colonoscopy may be used to find the place and cause of bleeding as well as to check areas for irritation or sores in your
colon.
These colon problems can cause unexplained changes in bowel habits.
Pain, bloody diarrhea, and weight loss can be caused by inflammation of the bowel, which may be the result of Crohn
disease or ulcerative colitis.
These inflammatory digestive diseases tend to occur in young adults and, if undetected, can produce chronic symptoms
and increase the risk of colon cancer.
Colonoscopy is used when there is concern that a disease of the colon may exist.
o Your doctor may recommend this test if other screening tests such as a manual rectal examination, a hemoccult test to find
hidden blood in your feces, or a barium enema (a test in which barium is used to make your colon visible on an x-ray) suggest
that further information is needed to make a diagnosis.
o A colonoscopy may be required when symptoms of digestive disease or other warning signs are present.
Rectal bleeding (which may appears as bright red, very dark, or black)
Pain in the lower abdomen
Changes in bowel habits
Nondietary weight loss
o Only doctors who specialize in the study of digestive disease, have special training in endoscopy, and are certified to performcolonoscopy qualify to perform this procedure.
As with any skill, performance improves with experience.
The American Society for Gastrointestinal Endoscopy suggests that a doctor perform at least 200 procedures to become
technically competent at diagnostic colonoscopy.
Risks
As with any procedure, there are risks associated with a colonoscopy. Before obtaining your consent for the procedure, your doctor
will tell you about the potential risks.
The most common side effects are cramping pain and abdominal swelling caused by the air used to inflate the colon during theprocedure. This air is expelled shortly after the procedure, and these symptoms generally go away.
If a biopsy is performed during the procedure, you may also note small amounts of blood in the bowel movements after the
examination. This may last for a few days.
Though rare, there is potential for the colonoscope to injure the intestinal wall, causing perforation, infection, or bleeding.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 3/23
Although this test is very helpful in finding the cause of many digestive diseases, abnormalities can go undetected at times.
Factors that can affect this include the completeness of your bowel preparation before the procedure, the skill of the operator of
the colonoscope, and your anatomy.
When this test is performed, you will be given sedating medications to make the test more comfortable. Whenever a medication
is given, a risk of an allergic reaction or side effect of the medication itself is present. These IV medications are given under
medical supervision, and you will be monitored during the procedure to lessen the risk of medication-related complications.
Colonoscopy Preparation
A colonoscopy can be carried out in a hospital, clinic, or in a doctor¶s office, depending on the facility. You will be given an
appointment and a set of instructions to follow before the test is performed.
Although the exact instructions given may vary from clinic to clinic, their objective is the same: to clean out the contents of the
bowel before the test.
This allows the bowel wall to be seen during the test.
This system of cleaning the bowel is often called bowel preparation.
You will be given a combination of liquid diet, laxatives, or enemas for up to 2 days prior to the test with instructions on how to
use them. Several medications are available for bowel cleansing, including polyethylene glycol 3350 (GoLYTELY, NuLYTELY),
magnesium citrate (Citroma), and senna (X-Prep).
These medications produce diarrhea, which can be uncomfortable, but unless the bowel is empty of stool, the test can be limited
and may need to be repeated at a later date.
On the night before the test is to be performed, nothing should be taken by mouth (food or liquids) until after the test is finished.
During the Procedure
On the day of the colonoscopy, you will most likely be asked to arrive at the clinic up to an hour before the test is due to begin.
This is to allow time to get ready for the test itself and to ask further questions. In addition, you will be asked the following
questions:
o When did you last eat?
o What allergies do you have?
o Did you remember to take all your bowel preparation medication?
Once you are undressed and changed into an examination gown, your vital signs (blood pressure, heart rate, respiration rate,
and temperature) will be monitored and an intravenous line (IV) will be placed. This IV is necessary to give you sedation and pain
medication that may be required during the test. Although you will not be fully asleep during the procedure, these medications will
produce a sleepy state (sedation) and make the test more comfortable.
The procedure will begin with you lying flat on your left side. The equipment used, the colonoscope, is lubricated to allow it to
enter the anus. For a thorough investigation, air is required to gently open the folded colon. This may cause a temporary
uncomfortable bloated sensation. When the doctor applies gentle pressure, the colonoscope moves further into the colon and is
slowly advanced until the entire colon is seen.
The colonoscope has a tiny camera on the end of it, which is connected to a monitor. This allows the physician to see the colon
through the tip of the instrument even when it is far inside the body. As the scope passes the course of the colon, the normal
turns and contours of the colon may impede the passage of the scope. You may be asked to change positions for better
visualization. It is common for fluid and gas to escape through the rectum and anus; this should be expected. The entire
procedure can take from 30 minutes up to 1 hour.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 4/23
In addition to simply viewing the bowel wall, the colonoscope has special attachments that allow the doctor to collect tissue
samples or biopsies, remove small growths, and stop bleeding with laser , heat, or medication.
Af ter the Procedure
When the colonoscopy is done as an outpatient procedure (without checking into the hospital), you will go home later that
same day. But before you go home, you will be observed for some time and monitored until the effects of the medications
are gone. It is a good idea to make arrangements for someone to come to the clinic and take you home, because nausea,
bloating, and drowsiness can continue for some time after the procedure.
Irritable bowel syndrome
Irritable Bowel Syndrome Overview
Irritable bowel syndrome (IBS) is a chronic gastrointestinal disorder of unknown cause. Common symptoms include abdominal
cramping or pain, bloating and gassiness, and altered bowel habits. Irritable bowel syndrome has been called spastic colon,
functional bowel disease, and mucous colitis. However, IBS is not a true "colitis." The term colitis refers to a separate condition
known as inflammatory bowel disease (IBD).
Irritable bowel syndrome is not contagious, inherited, or cancerous. However, IBS often disrupts daily living activities. Nineteen
percent of respondents in a survey of married or cohabiting people with IBS stated that they had difficulties in their personal
relationships, and 45% stated that IBS interfered with their sex life.
Irritable Bowel Syndrome Causes
The cause of irritable bowel syndrome is currently unknown. IBS is thought to result from an interplay of abnormal gastrointestinal
(GI) tract movements, increased awareness of normal bodily functions, and a change in the nervous system communication
between the brain and the GI tract. Abnormal movements of the colon, whether too fast or too slow, are seen in some, but not all,
people who have IBS.
Irritable bowel syndrome has also developed after episodes of gastroenteritis.
It has been suggested that IBS is caused by dietary allergies or food sensitivities, but this has never been proven.
Symptoms of irritable bowel syndrome may worsen during periods of stress or menses, but these factors are unlikely to be thecause that leads to development of IBS.
Irritable Bowel Syndrome Symptoms
Irritable bowel syndrome affects each person differently. The hallmark of IBS is abdominal discomfort or pain. The following
symptoms are also common:
Abdominal cramping and pain that are relieved after bowel movements
Alternating periods of diarrhea and constipation
Change in the stool frequency or consistency
Gassiness (flatulence)
Passing mucus from the rectum
Bloating
Abdominal distension
The following are not symptoms or characteristics of IBS:

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 5/23
Blood in stools or urine
Vomiting (rare, though may occasionally accompany nausea)
Pain or diarrhea that interrupts sleep
Fever
Weight loss
Exams and Tests
Irritable bowel syndrome can be a very difficult diagnosis to make. IBS is called a diagnosis of exclusion, which means that a doctor
considers many other alternatives first, perhaps performing tests to rule out other problems. Some of these tests may include
laboratory studies, imaging studies (such as a CT scan or small intestinal x-rays), or a lower GI endoscopy (colonoscopy). An
endoscopy is a procedure in which a flexible tube with a tiny camera on one end is passed into the GI tract while the patient is under
conscious sedation.
A combination of history, physical examination, and selected tests are used to help diagnose irritable bowel syndrome.
No single blood test or x-ray study confirms a diagnosis of IBS.
Irritable Bowel Syndrome Treatment
Self-Care at Home
Many people have already modified their diets before seeing a doctor. Temporarily avoiding dairy products may help
assess whether symptoms of lactose intolerance are mimicking those of irritable bowel syndrome. Persons who avoid
dairy products should exercise and consider taking calcium supplements.
Certain foods, such as cruciferous vegetables (cauliflower, broccoli, cabbage, brussels sprouts) and legumes (beans) may
worsen bloating and gassiness.
Medical Treatment
Most people with irritable bowel syndrome have problems only occasionally. A few may experience long-lasting problems and
require prescription medications.
A common treatment for IBS is the addition of fiber to the diet. This theoretically expands the inside of the digestive tract,
reducing the chance it will spasm as it transmits and digests food. Fiber also promotes regular bowel movements, which helps
reduce constipation. Fiber should be added gradually, because it may initially worsen bloating and gassiness.
Stress may cause IBS "flares." Doctors may offer specific advice on reducing stress. Regularly eating balanced meals and
exercising may help reduce stress and problems associated with irritable bowel syndrome.
Smoking may worsen symptoms of IBS, which gives smokers another good reason to quit.
Since many patients with irritable bowel syndrome report food intolerances, a food diary may help identify foods that seem to
make IBS worse.
Next Steps
Prevention
Maintaining good physical fitness improves bowel function and helps reduce stress.
Stopping smoking is important for overall good health.
Avoiding coffee, gas-producing foods, and spicy foods may help.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 6/23
Reducing or eliminating alcohol consumption may help.
Diverticulitis
Diverticulosis and Diverticulitis Overview
Diverticula are small pouches in the wall of the digestive tract. They occur when the inner layer of the digestive tract bulges through
weak spots in the outer layer. (This is similar to what happens when an inner tube bulges through a tire.)
Although these pouches can occur anyplace from the mouth to the anus, most occur in the large intestine (colon), especially the
left (lower) portion of the colon just before the rectum.
These marble-sized pouches usually occur where blood vessels run through the intestinal wall.
Individuals who have these pouches are said to have diverticulosis.
Because this condition typically does not cause symptoms, most people are unaware that they have diverticulitis.
Diverticulitis is inflammation of diverticula. Diverticulitis occurs when one or more of these pouches becomes inflamed or infected.
Some people with diverticulosis become aware of the condition only when diverticulitis occurs.
Diverticulosis is a very common condition in the United States.
Diverticulosis is mainly a condition of older people.
Approximately 10% of Americans over the age of 40 have diverticulitis. As we age, the condition becomes more prevalent. Over
half of people older than 60 years of age develop the condition, and about two-thirds of individuals older than 80 years of age are
believed to have diverticulosis.
Only about 10% to 25% of people with diverticulosis will develop diverticulitis.
Diverticulosis is more common in developed or industrialized countries.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 7/23
In places such as the United States, England, and Australia, where the typical diet is low in fiber and high in highly processed
carbohydrates, diverticulosis is common. The current theory is that a low-fiber diet may cause increased incidence of diverticular
disease.
Diverticulosis first appeared in the United States in the early 1900s. This was the same time that processed foods were first
introduced into the U.S. daily diet.
Diverticulosis is much less common in countries of Asia and Africa, where the typical diet is high in fiber.
Most people recover from diverticulitis without complications if they receive appropriate treatment. Diverticulitis can lead to some
very serious conditions if it is not detected and treated promptly. To a great extent, diverticulosis and diverticulitis can be prevented
by changes in lifestyle and habits.
Diverticulosis and Diverticulitis Causes
Diverticulosis is thought to be caused by increased pressure on the intestinal wall from inside the intestine.
As the body ages, the outer layer of the intestinal wall thickens. This causes the open space inside the intestine to narrow. Stool
(feces) moves more slowly through the colon, increasing the pressure.
Hard stools, such as those produced by a diet low in fiber or slower stool "transit time" through the colon can further increasepressure.
Frequent, repeated straining during bowel movements also increases pressure and contributes to formation of diverticula.
Diverticulosis in developed countries is blamed largely on a diet low in fiber.
Fiber is found in fruits and vegetables, whole grains, and legumes (dried beans, peas, and lentils).
There are two types of fiber, soluble (dissolves in water) and insoluble.
Soluble fiber forms a soft gel-like substance in the digestive tract.
Insoluble fiber passes through the digestive tract nearly unchanged.
Both are necessary to keep stool soft and moving easily through the digestive tract, which helps prevent constipation.
This is how fiber prevents constipation.
Diverticulosis and Diverticulitis Symptoms
Most people with diverticulosis have no symptoms. When symptoms do occur, they are usually mild and include the following:
pain in the belly (abdomen),
bloating,
constipation (less often, diarrhea), and
cramping.
These symptoms are nonspecific. This means that they are symptoms of many different digestive disorders. They do not necessarily
mean that a person has diverticulosis. If an individual has these symptoms, he or she should see a health care practitioner.
Diverticulitis is a more serious condition and causes symptoms in most people with the condition that include:

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 8/23
pain in the abdomen, usually in the lower left side;
bleeding, bright red or maroon blood may appear in the toilet, on toilet paper, or in the stool. Bleeding is often mild and usually
stops by itself; however, it can become severe;
fever ;
nausea;
vomiting;
chills; and
constipation (less often, diarrhea).
If diverticulitis is not treated promptly it can develop some very serious complications. A complication is suggested by any of the
following symptoms:
worsening abdominal pain;
persistent fever;
vomiting (no food or liquid can be tolerated);
constipation for an extended period of time;
burning or pain during urination; and
bleeding from the rectum.
Exams and Tests
The health care practitioner will ask the patient questions about his or her symptoms, lifestyle and habits, and medical and surgical
history.
The physical exam will probably include a "digital rectal examination" in which a health care practitioner inserts a gloved finger
into the rectum to try to find a cause for bleeding or pain.
Blood tests may be performed to access signs of blood loss or infection, evaluate the function of the kidneys and liver, or to rule
out other medical conditions that could be causing similar symptoms.
X-rays of organs in the abdomen may be ordered to assist in identifying the cause of the patient's symptoms.
CT scans are similar to an X-ray except they are able to visualize the organs better and often provide the health care practitioner
with more useful information. One drawback with CT scans is they are more expensive, and take longer to perform.
A colonoscopy is a procedure performed using a flexible tube with a tiny camera on the end, called an endoscope. Theendoscope is inserted into the rectum and further up into the colon. The endoscope provides a direct view of the inner lining of
the colon and rectum. The procedure is relatively painless and usually takes 30 to 45 minutes. Patients may be given a sedative
medication to relax during the procedure.
A flexible sigmoidoscopy is a procedure performed with a flexible sigmoidoscope that has a tiny camera on the end of the
sigmoidoscope. The patient lays on their left side while the instrument is inserted through the anus and advanced through the
rectum and colon. This procedure is relatively painless and takes about five minutes.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 9/23
Sometimes diverticulosis is discovered during a screening colonoscopy. The current recommendations from the American Cancer
Society, the United States Multi-Society Task Force on Colorectal Cancer recommend colonoscopies every 10 years for people
older than 50 years to detect early signs of colon cancer . If an individual's family medical history includes a close relative diagnosed
with colon cancer, they may need to begin screening at an earlier age. Consult a gastroenterologist for guidelines.
Self-Care at Home
These measures can help heal existing diverticula and prevent new diverticula from forming.
Eat a high-fiber diet. High-fiber foods include fruits, vegetables, whole grains, and dried beans, peas, and lentils. These foods
contain elements that your body cannot digest and are passed through your colon.
Drink plenty of fluids to help keep stools soft and prevent constipation.
Get plenty of physical activity to keep bowels functioning properly.
Medical Treatment
Diverticulosis with symptoms is usually treated as follows. This therapy is designed to soften stools and help them pass faster,
which removes the conditions that cause diverticula in the first place.
High-fiber diet: Some health care practitioners recommend a fiber supplement to prevent constipation.
Clear fluids
Mild pain medications
Treatment for diverticulitis depends on the severity of the condition.
Simple cases can be treated by a health care practitioner at his or her office.
Treatment for uncomplicated cases usually consists of antibiotics and bowel rest. This usually involves two to three days of bowel
rest, taking in only clear fluids (no food at all), so the colon may heal without having to work.
Complicated cases typically involve severe pain, fever, or bleeding. If an individual has any of these symptoms, he or she will
probably be admitted to the hospital. Treatment consists of IV antibiotics, bowel rest, and possibly surgery.
Surgery
If diverticulitis attacks are frequent or severe, the doctor may suggest surgery to remove part of the patient's colon.
As with any surgery, there are risks that the patient should discuss with his or her physician.
Sometimes the operation requires at least two separate surgeries on different occasions.
Prevention
A high-fiber diet is the mainstay of diverticulosis and diverticulitis prevention.
Starting a high-fiber diet may not make the diverticula a patient has go away, but it will decrease the risk of complications and the
accompanying symptoms.
Foods high in fiber include whole-grain cereals and breads, fruits (apples, berries, peaches, pears), vegetables (squash, broccoli,
cabbage, and spinach), and dried beans, peas, and lentils.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 10/23
Drinking plenty of fluids will also help the stool stay soft and pass quickly, decreasing the risk for diverticulosis.
In the past, those with diverticulosis or diverticulitis were advised to avoid nuts, corn, and popcorn. However, a 2008 study from
The Journal of the Amer ican Medical Association found these foods may actually lower risk of the condition because of their high
fiber content. Consult a health care practitioner for their dietary recommendations.
Rectal Cancer
Rectal Cancer Overview
The rectum is the lower part of the colon that connects the large bowel to the anus. The rectum's primary function is to store formed
stool in preparation for evacuation. Like the colon, the 3 layers of the rectal wall are as follows:
Mucosa: This layer of the rectal wall lines the inner surface. The mucosa is composed of glands that secrete mucus to help the
passage of stool.
Muscularis propria: This middle layer of the rectal wall is composed of muscles that help the rectum keep its shape and contract
in a coordinated fashion to expel stool.
Mesorectum: This fatty tissue surrounds the rectum.
In addition to these 3 layers, another important component of the rectum is the surrounding lymph nodes (also called regional lymph
nodes). Lymph nodes are part of the immune system and assist in conducting surveillance for harmful materials (including viruses
and bacteria) that may be threatening the body. Lymph nodes surround every organ in the body, including the rectum.
Of the 150,000 cases of colorectal cancer diagnosed each year in the United States, more than 40,000 people are diagnosed with
rectal cancer. The most common type of rectal cancer is adenocarcinoma, which is a cancer arising from the mucosa. Cancer cellscan also spread from the rectum to the lymph nodes on their way to other parts of the body.
Like colon cancer , the prognosis and treatment of rectal cancer depends on how deeply the cancer has invaded the rectal wall and
surrounding lymph nodes. However, although the rectum is part of the colon, the location of the rectum in the pelvis poses additional
challenges in treatment when compared with colon cancer.
Rectal Cancer Causes
Rectal cancer usually develops over several years, first growing as a precancerous growth called a polyp. Some polyps have the
ability to turn into cancer and begin to grow and penetrate the wall of the rectum.
The actual cause of rectal cancer is unclear. However, the following are risk factors for developing rectal cancer:
Increasing age
Smoking
Family history of colon or rectal cancer
High-fat diet and/or a diet mostly from animal sources
Personal or family history of polyps or colorectal cancer

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 11/23
Family history is a factor in determining the risk of rectal cancer. If a family history of colorectal cancer is present in a first-degree
relative (a parent or a sibling), then endoscopy of the colon and rectum should begin 10 years before the age of the relative's
diagnosis or at age 50 years, whichever comes first.
An often forgotten risk factor , but perhaps the most important, is the lack of screening for rectal cancer. Routine cancer screening of
the colon and rectum is the best way to prevent rectal cancer.
Rectal Cancer Symptoms
Rectal cancer can cause many symptoms that require a person to seek medical care. However, rectal cancer may also be present
without any symptoms, underscoring the importance of routine health screening. Symptoms to be aware of include the following:
Bleeding
y Seeing blood mixed with stool is a sign to seek immediate medical care. Although many people bleed due to hemorrhoids, a
doctor should still be notified in the event of rectal bleeding.
y y Prolonged rectal bleeding (perhaps in small quantities that is not seen in the stool) may lead to anemia, causing fatigue,
shortness of breath, light-headedness, or a fast heartbeat.
Obstruction
y A rectal mass may grow so large that it prevents the normal passage of stool. This blockage may lead to the feeling of severe
constipation or pain when having a bowel movement. In addition, abdominal pain or cramping may occur due to the blockage.
y
y The stool size may appear narrow so that it can be passed around the rectal mass. Therefore, pencil-thin stool may be
another sign of an obstruction from rectal cancer.
y y A person with rectal cancer may have a sensation that the stool cannot be completely evacuated after a bowel movement.
Weight loss: Cancer may cause weight loss. Unexplained weight loss (in the absence of dieting or a new exercise program)
requires a medical evaluation.
Medical Treatment
The treatment and prognosis of rectal cancer depend on the stage of the cancer, which is determined by the following 3
considerations:
How deeply the tumor has invaded the wall of the rectum
Whether the lymph nodes appear to have cancer in them
Whether the cancer has spread to any other locations in the body (Organs that rectal cancer commonly spreads to include the
liver and the lungs.)
The stages of rectal cancer are as follows:
Stage I: The tumor involves only the first or second layer of the rectal wall and no lymph nodes are involved.
Stage II: The tumor penetrates into the mesorectum, but no lymph nodes are involved.
Stage III: Regardless of how deeply the tumor penetrates, the lymph nodes are involved with the cancer.
Stage IV: Convincing evidence of the cancer exists in other parts of the body, outside of the rectal area.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 12/23
Localized rectal cancer includes stages I-III. Metastatic rectal cancer is stage IV.
The goals of treating localized rectal cancer are to ensure the removal of all the cancer and to prevent a recurrence of the cancer,
either near the rectum or elsewhere in the body.
If stage I rectal cancer is diagnosed, then surgery is likely to be the only necessary step in treatment. The risk of the cancer coming
back after surgery is low, and, therefore, chemotherapy is not usually offered.
Sometimes, after the removal of a tumor, the doctor discovers that the tumor penetrated into the mesorectum (stage II) or that the
lymph nodes contained cancer cells (stage III). In these cases, chemotherapy and radiation therapy are offered after recovery from
the surgery to reduce the chance of the cancer returning. Chemotherapy and radiation therapy given after surgery is called adjuvant
therapy.
If the initial exams and tests show a person to have stage II or III rectal cancer, then chemotherapy and radiation therapy should be
considered before surgery. Chemotherapy and radiation given before surgery is called neoadjuvant therapy. This therapy lasts
approximately 6 weeks. Neoadjuvant therapy is performed to shrink the tumor so it can be more completely removed by surgery. In
addition, a person is likely to tolerate the side effects of combined chemotherapy and radiation therapy better if this therapy is
administered before surgery rather than afterward. After recovery from the surgery, a person who has undergone neoadjuvant
therapy should meet with the oncologist to discuss the need for more chemotherapy.
If the rectal cancer is metastatic, then surgery and radiation therapy would only be performed if persistent bleeding or bowel
obstruction from the rectal mass exist. Otherwise, chemotherapy alone is the standard treatment of metastatic rectal cancer. At this
time, metastatic rectal cancer is not curable. However, average survival times for people with metastatic rectal cancer have
lengthened over the past several years because of the introduction of new medications.
Celiac Disease
What is celiac disease?
Celiac disease is a digestive disease that damages the small intestine and interferes withabsorption of nutrients from food. People who have celiac disease cannot tolerate gluten, a
protein in wheat, rye, and barley. Gluten is found mainly in foods but may also be found in
everyday products such as medicines, vitamins, and lip balms.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 13/23
The small intestine is shaded above.
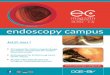
When people with celiac disease eat foods or use products containing gluten, their immunesystem responds by damaging or destroying villi²the tiny, fingerlike protrusions lining the
small intestine. Villi normally allow nutrients from food to be absorbed through the walls of thesmall intestine into the bloodstream. Without healthy villi, a person becomes malnourished, no
matter how much food one eats.
Villi on the lining of the small intestine help absorb nutrients.
Celiac disease is both a disease of malabsorption²meaning nutrients are not absorbed properly²and an abnormal immune reaction to gluten. Celiac disease is also known as celiac
sprue, nontropical sprue, and gluten-sensitive enteropathy. Celiac disease is genetic, meaning itruns in families. Sometimes the disease is triggered²or becomes active for the first time²after
surgery, pregnancy, childbirth, viral infection, or severe emotional stress.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 14/23
[Top]
What are the symptoms of celiac disease?
Symptoms of celiac disease vary from person to person. Symptoms may occur in the digestive
system or in other parts of the body. Digestive symptoms are more common in infants and youngchildren and may include
y abdominal bloating and pain
y chronic diarrhea
y vomiting
y constipation
y pale, foul-smelling, or fatty stool
y weight loss
Irritability is another common symptom in children. Malabsorption of nutrients during the years
when nutrition is critical to a child¶s normal growth and development can result in other problems such as failure to thrive in infants, delayed growth and short stature, delayed puberty,and dental enamel defects of the permanent teeth.
Adults are less likely to have digestive symptoms and may instead have one or more of thefollowing:
y unexplained iron-deficiency anemia
y fatigue
y bone or joint pain
y arthritis
y bone loss or osteoporosis
y depression or anxiety
y tingling numbness in the hands and feet
y seizures
y missed menstrual periods
y infertility or recurrent miscarriage
y canker sores inside the mouth
y an itchy skin rash called dermatitis herpetiformis
People with celiac disease may have no symptoms but can still develop complications of the
disease over time. Long-term complications include malnutrition²which can lead to anemia,osteoporosis, and miscarriage, among other problems²liver diseases, and cancers of the
intestine.
[Top]
Why are celiac disease symptoms so varied?
R esearchers are studying the reasons celiac disease affects people differently. The length of time
a person was breastfed, the age a person started eating gluten-containing foods, and the amount

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 15/23
of gluten-containing foods one eats are three factors thought to play a role in when and howceliac disease appears. Some studies have shown, for example, that the longer a person was
breastfed, the later the symptoms of celiac disease appear.
Symptoms also vary depending on a person¶s age and the degree of damage to the small
intestine. Many adults have the disease for a decade or more before they are diagnosed. Thelonger a person goes undiagnosed and untreated, the greater the chance of developing long-termcomplications.
[Top]
What other health problems do people with celiac disease have?
People with celiac disease tend to have other diseases in which the immune system attacks the body¶s healthy cells and tissues. The connection between celiac disease and these diseases may
be genetic. They include
y type 1 diabetes
y autoimmune thyroid disease
y autoimmune liver disease
y rheumatoid arthritis
y Addisons disease, a condition in which the glands that produce critical hormones are damaged
y S jögrens syndrome, a condition in which the glands that produce tears and saliva are destroyed
[Top]
How common is celiac disease?
Celiac disease affects people in all parts of the world. Originally thought to be a rare childhoodsyndrome, celiac disease is now known to be a common genetic disorder. More than 2 million
people in the United States have the disease, or about 1 in 133 people.1 Among people who havea first-degree relative²a parent, sibling, or child²diagnosed with celiac disease, as many as 1
in 22 people may have the disease.2
Celiac disease is also more common among people with other genetic disorders including Down
syndrome and Turner syndrome, a condition that affects girls¶ development.
1Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk
groups in the United States. Archives of Internal Medicine. 2003;163(3):268±292.2I bid.
[Top]
How is celiac disease diagnosed?

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 16/23
R ecognizing celiac disease can be difficult because some of its symptoms are similar to those of other diseases. Celiac disease can be confused with irritable bowel syndrome, iron-deficiency
anemia caused by menstrual blood loss, inflammatory bowel disease, diverticulitis, intestinalinfections, and chronic fatigue syndrome. As a result, celiac disease has long been
underdiagnosed or misdiagnosed. As doctors become more aware of the many varied symptoms
of the disease and reliable blood tests become more available, diagnosis rates are increasing.
Blood Tests
People with celiac disease have higher than normal levels of certain autoantibodies²proteins
that react against the body¶s own cells or tissues²in their blood. To diagnose celiac disease,doctors will test blood for high levels of anti-tissue transglutaminase antibodies (tTGA) or anti-
endomysium antibodies (EMA). If test results are negative but celiac disease is still suspected,additional blood tests may be needed.
Before being tested, one should continue to eat a diet that includes foods with gluten, such as
breads and pastas. If a person stops eating foods with gluten before being tested, the results may be negative for celiac disease even if the disease is present.
Intestinal Biopsy
If blood tests and symptoms suggest celiac disease, a biopsy of the small intestine is performedto confirm the diagnosis. During the biopsy, the doctor removes tiny pieces of tissue from the
small intestine to check for damage to the villi. To obtain the tissue sample, the doctor eases along, thin tube called an endoscope through the patient¶s mouth and stomach into the small
intestine. The doctor then takes the samples using instruments passed through the endoscope.
DermatitisH
erpetiformis
Dermatitis herpetiformis (DH) is an intensely itchy, blistering skin rash that affects 15 to 25
percent of people with celiac disease.3
The rash usually occurs on the elbows, knees, and buttocks. Most people with DH have no digestive symptoms of celiac disease.
DH is diagnosed through blood tests and a skin biopsy. If the antibody tests are positive and the
skin biopsy has the typical findings of DH, patients do not need to have an intestinal biopsy.Both the skin disease and the intestinal disease respond to a gluten-free diet and recur if gluten is
added back into the diet. The rash symptoms can be controlled with antibiotics such as dapsone.Because dapsone does not treat the intestinal condition, people with DH must maintain a gluten-
free diet.
Screening
Screening for celiac disease means testing for the presence of autoantibodies in the blood in
people without symptoms. Americans are not routinely screened for celiac disease. However, because celiac disease is hereditary, family members of a person with the disease may wish to be

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 17/23
tested. Four to 12 percent of an affected person¶s first-degree relatives will also have thedisease.
4
3R odrigo L. Celiac disease. W orld Journal of Gastroenterology. 2006;12(41):6585±6593.
4
I bid.
[Top]
How is celiac disease treated?
The only treatment for celiac disease is a gluten-free diet. Doctors may ask a newly diagnosed person to work with a dietitian on a gluten-free diet plan. A dietitian is a health care professional
who specializes in food and nutrition. Someone with celiac disease can learn from a dietitianhow to read ingredient lists and identify foods that contain gluten in order to make informed
decisions at the grocery store and when eating out.
For most people, following this diet will stop symptoms, heal existing intestinal damage, and prevent further damage. Improvement begins within days of starting the diet. The small intestine
usually heals in 3 to 6 months in children but may take several years in adults. A healed intestinemeans a person now has villi that can absorb nutrients from food into the bloodstream.
To stay well, people with celiac disease must avoid gluten for the rest of their lives. Eating evena small amount of gluten can damage the small intestine. The damage will occur in anyone with
the disease, including people without noticeable symptoms. Depending on a person¶s age atdiagnosis, some problems will not improve, such as short stature and dental enamel defects.
Some people with celiac disease show no improvement on the gluten-free diet. The mostcommon reason for poor response to the diet is that small amounts of gluten are still beingconsumed. Hidden sources of gluten include additives such as modified food starch,
preservatives, and stabilizers made with wheat. And because many corn and rice products are produced in factories that also manufacture wheat products, they can be contaminated with wheat
gluten.
R arely, the intestinal injury will continue despite a strictly gluten-free diet. People with thiscondition, known as refractory celiac disease, have severely damaged intestines that cannot heal.
Because their intestines are not absorbing enough nutrients, they may need to receive nutrientsdirectly into their bloodstream through a vein, or intravenously. R esearchers are evaluating drug
treatments for refractory celiac disease.
The Gluten-free Diet
A gluten-free diet means not eating foods that contain wheat, rye, and barley. The foods and
products made from these grains should also be avoided. In other words, a person with celiacdisease should not eat most grain, pasta, cereal, and many processed foods.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 18/23
Despite these restrictions, people with celiac disease can eat a well-balanced diet with a varietyof foods. They can use potato, rice, soy, amaranth, quinoa, buckwheat, or bean flour instead of
wheat flour. They can buy gluten-free bread, pasta, and other products from stores that carryorganic foods, or order products from special food companies. Gluten-free products are
increasingly available from mainstream stores.
³Plain´ meat, fish, rice, fruits, and vegetables do not contain gluten, so people with celiac diseasecan freely eat these foods. In the past, people with celiac disease were advised not to eat oats.
New evidence suggests that most people can safely eat small amounts of oats, as long as the oatsare not contaminated with wheat gluten during processing. People with celiac disease should
work closely with their health care team when deciding whether to include oats in their diet.Examples of other foods that are safe to eat and those that are not are provided in the table.
The gluten-free diet requires a completely new approach to eating. Newly diagnosed people and
their families may find support groups helpful as they learn to adjust to a new way of life. Peoplewith celiac disease must be cautious about what they buy for lunch at school or work, what they
purchase at the grocery store, what they eat at restaurants or parties, and what they grab for asnack. Eating out can be a challenge. When in doubt about a menu item, a person with celiac
disease should ask the waiter or chef about ingredients and preparation or if a gluten-free menu isavailable.
Gluten is also used in some medications. People with celiac disease should ask a pharmacist if prescribed medications contain wheat. Because gluten is sometimes used as an additive in
unexpected products²such as lipstick and play dough²reading product labels is important. If the ingredients are not listed on the label, the manufacturer should provide a list upon request.
With practice, screening for gluten becomes second nature.
N
ew Food Labeling
The Food Allergen Labeling and Consumer Protection Act (FALCPA), which took effect onJanuary 1, 2006, requires food labels to clearly identify wheat and other common food allergens
in the list of ingredients. FALCPA also requires the U.S. Food and Drug Administration todevelop and finalize rules for the use of the term ³gluten free´ on product labels.
[Top]
The Gluten-free Diet: Some Examples
In 2006, the American Dietetic Association updated its recommendations for a gluten-free diet.The following chart is based on the 2006 recommendations. This list is not complete, so people
with celiac disease should discuss gluten-free food choices with a dietitian or physician whospecializes in celiac disease. People with celiac disease should always read food ingredient lists
carefully to make sure the food does not contain gluten.
Allowed Foods

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 19/23
amaranth
arrowroot
buckwheat
cassava
corn
flax
Indian rice grass
Jobs tears
legumes
millet
nuts
potatoes
quinoa
rice
sago
seeds
sorghum
soy
tapioca
teff
wild rice
yucca
Foods To Avoid
wheat
y including einkorn, emmer, spelt, kamut
y
wheat starch, wheat bran, wheat germ, cracked wheat,hydrolyzed wheat protein
barley
rye
triticale (a cross between wheat
and rye)
Other Wheat Products
bromated flour
durum flour
enriched flour
farina
graham flour
phosphated flour
plain flour
self-rising flour
semolina
white flour
Processed Foods that May Contain Wheat, Barley, or Rye*
bouillon cubes
brown rice syrup
candy
chips/potato chips
cold cuts, hot dogs, salami,
sausage
communion wafers
French fries
gravy
imitation fish
matzo
rice mixes
sauces
seasoned tortilla chips
self-basting turkey
soups
soy sauce
vegetables in sauce
*Most of these foods can be found gluten-free. When in doubt, check with the food
manufacturer.
S ource: Thompson T. Celiac Disease Nutrition Guide, 2nd ed. Chicago: American DieteticAssociation; 2006. © American Dietetic Association. Adapted with permission. For a complete
copy of the Celiac Disease Nutrition Guide, please visit www.eatright.org.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 20/23
[Top]
Points to Remember
y People with celiac disease cannot tolerate gluten, a protein in wheat, rye, and barley.
y
Untreated celiac disease damages the small intestine and interferes with nutrient absorption.y Without treatment, people with celiac disease can develop complications such as osteoporosis,
anemia, and cancer.
y A person with celiac disease may or may not have symptoms.
y Diagnosis involves blood tests and, in most cases, a biopsy of the small intestine.
y Since celiac disease is hereditary, family members of a person with celiac disease may wish to be
tested.
y Celiac disease is treated by eliminating all gluten from the diet. The gluten-free diet is a lifetime
requirement.
y A dietitian can teach a person with celiac disease about food selection, label reading, and other
strategies to help manage the disease.
From mouth
Hiatus HerniaAuthor: Frank W. Jackson, M.D.
Prebiotics in your diet or in a supplement naturally restore digestive
balance and health. Learn more . . .
The hiatus hernia is one of the most
misunderstood and maligned conditions inmedicine. People blame this hernia for much
more than it ever does. Patients with a hiatushernia need to understand what it is and what
might occur with it. Most importantly, theyneed to know it is unusual for serious
problems to develop from this type of hernia.
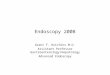
Anatomy
The diaphragm is a sheet of muscle thatseparates the lungs from the abdomen. When a person takes a deep breath, the dome-shaped
diaphragm contracts and flattens. In doing this, the diaphragm pulls air into the lungs. The leftdiaphragm contains a small hole through which passes the tube-shaped esophagus that carries
food and liquid to the stomach. Normally this hole, called a hiatus, is small and fits snuglyaround the esophagus. The J-shaped stomach sits below the diaphragm.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 21/23
What Causes a Hiatus Hernia?
In some people, the hiatus or hole in the diaphragm weakens and enlarges. It is not known whythis occurs. It may be due to heredity, while in others it may be caused by obesity, exercises such
as weightlifting, or straining at stool. Whatever the cause, a portion of the stomach herniates, or moves up, into the chest cavity through this enlarged hole. A hiatus hernia is now present. Hiatus
hernias are very common, occuring in up to 60 percent of people by age 60.
What Are the Different Types of Hiatus Hernia?1. Sliding Hiatus Hernia -- In this most common type of hiatus hernia, the herniated portion of the stomach
slides back and forth, into and out of the chest. These hernias are normally small and usually cause no
problems or even symptoms.
2. Fixed Hiatus Hernia -- In this case, the upper part of the stomach is caught up in the chest. Even with thishernia, there may be few symptoms. However, the potential for problems in the esophagus is increased.
3. Complicated or Serious Hiatus Hernia -- Fortunately, this type of hernia is uncommon. It includes a variety
of patterns of herniation of the stomach, including cases in which the entire stomach moves up in thechest. There is a high likelihood that medical problems will occur with this hernia and that treatment,
frequently involving surgery, will be required. Complicated hernias are uncommon.
Symptoms
In most patients, hiatus hernias cause no symptoms. This is especially true of sliding hernias.When symptoms occur, they may only be heartburn and regurgitation, when stomach acid
refluxes back into the esophagus. Some patients with fixed hiatus hernias experience chronicreflux of acid into the esophagus, which may cause injury and bleeding. Anemia, or low red
blood cell count, can result. Further, chronic inflammation of the lower esophagus may producescarring and narrowing in this area. This, in turn, makes swallowing difficult, and food does not
pass easily into the stomach.
Does Hiatus Hernia Cause Pain and Indigestion?
It is wrong to always blame a hiatus hernia for pain and indigestion. Hiatus hernias generally donot cause acute pain. This symptom may result from other disorders, such as peptic ulcers or even heart disease. Some patients with coronary heart disease fool themselves into believing
their discomfort is due to a hiatus hernia. If upper-abdominal pain or indigestion occurs, peopleshould not mislead themselves into thinking the cause is a hiatus hernia. Instead, the patient
should seek medical advice.
Diagnosis
Diagnosis of a hiatus hernia is typically made through an upper GI barium x-ray. A

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 22/23
complementary test is gastroscopy, or upper-intestinal endoscopy, in which the physicianvisually examines the esophagus and stomach using a flexible scope while the patient is lightly
sedated.
What Are the Complications?
The complications of hiatus hernia are:
Chronic heartburn and inflammation of the lower esophagus, called reflux esophagitis
Anemia due to chronic bleeding from the lower esophagus
Scarring and narrowing of the lower esophagus causing difficulty in swallowing
While sleeping, stomach secretions can seep up the esophagus and into the lungs causing chronic cough,
wheezing, and even pneumonia
In addition, the complicated hernia can cause serious problems such as difficulty in breathing or severe chest pain, especially in the elderly.
Treatment
Treatment is called for only when the hernia results in symptoms, such as persistent heartburn or difficulty in swallowing. Acid inflammation and ulceration of the lower esophagus also require
treatment.
General guidelines for treating heartburn and esophagitis (inflammation of the esophagus) are:
Avoid (or use only in moderation) foods and substances that increase reflux of acid into the esophagus,such as:
y nicotine (cigarettes)
y caffeine
y chocolate
y fatty foods
y peppermint
y alcohol
y spearmint
Eat smaller, more frequent meals and do not eat within 2-3 hours of bedtime. Avoid bending, stooping, abdominal exercises, tight belts, and girdles all of which increase abdominal
pressure and cause reflux.
If overweight, lose weight. Obesity also increases abdominal pressure.
Prescription medications. Certain drugs, such as intestinal antispasmodics, calcium channel blockers, and
some antidepressants weaken the muscle strength of the lower espohagus.
Elevate the head of the bed 8 to 10 inches by putting pillows or a wedge under the upper part of themattress. Gravity then helps keep stomach acid out of the esophagus while sleeping.

8/7/2019 Endoscopy Theater
http://slidepdf.com/reader/full/endoscopy-theater 23/23
Other Treatments
Drugs -- Some medicines effectively reduce the secretion of stomach acid, while others increasethe muscle strength of the lower esophagus, thereby reducing acid reflux.
Surgery -- The complicated hiatus hernia requires surgery occasionally on an emergency basis.
Surgery otherwise is reserved for those patients with complications that cannot be handled withmedications. The mere presence of a hiatus hernia is not a reason for surgery.