Embed Size (px)
Citation preview

In May 1999 we changed our approach to the man-agement of endoleak on the basis of a review of our resultsin 114 patients who underwent elective endovascularabdominal aortic aneurysm repair over the preceding 3years. Before that time, all patients with endoleak at 2weeks underwent immediate angiographic localizationand further endovascular treatment. We now attempt tocategorize endoleaks on the basis of computed tomogra-phy (CT) findings and treat type I endoleaks immediately.Type II endoleaks are treated only if the aneurysmenlarges. This report describes the findings that promptedthese changes.
METHODS
Patient selection. Patients were selected for inclusionin this study on the basis of two sets of criteria as describedpreviously.4 Only patients considered “high risk” were eli-gible. The designation “high-risk” was based on a variableassortment of clinical and laboratory criteria. We did notapply a rigorous system of preoperative testing and riskquantification, having decided that no patient would beconsidered too sick to undergo endovascular unless their
Persistent perfusion of the space between the stent-graft and the aneurysm wall (endoleak) is the most com-mon failure mode of endovascular repair.1-13 Endoleak issometimes associated with continuing aneurysm dilation10
or rupture,12-15 but not always.11 The uncertain signifi-cance of endoleak, particularly type II or branch endoleak,is reflected in the wide variety of approaches to its man-agement. Some authors treat all types of endoleakpromptly4; others treat endoleak only if it is associatedwith an increase in aneurysm diameter.3
98
From the Division of Vascular Surgerya and Interventional Radiology,b
University of California–San Francisco.Competition of interest: TC has licensed patents on systems of endovascu-
lar aneurysm repair to both Cook Inc, Bloomington, Ind, andEndovascular Technologies Inc (now a subsidiary of Guidant Corp,Menlo Park, Calif).
Supported in part by grants from the Pacific Vascular Research foundation.Reprint requests: Tim Chuter, MD, UCSF Vascular Surgery, 505 Parnassus
Ave, M-488, Box 0222, San Francisco, CA 94143.Copyright © 2001 by The Society for Vascular Surgery and The American
Association for Vascular Surgery.0741-5214/2001/$35.00 + 0 24/1/111487doi:10.1067/mva.2001.111487
CLINICAL RESEARCH STUDIES
Endoleak after endovascular repair of abdominalaortic aneurysmTimothy A. M. Chuter, MD,a Rishad M. Faruqi, MD,a Rajiv Sawhney, MD,b Linda M. Reilly, MD,aRobert B. Kerlan, MD,b Catherine J. Canto, RN,a Gregory C. Lukaszewicz, MD,a Jean M. LaBerge,MD,b Mark W. Wilson, MD,b Roy L. Gordon, MD,b Susan D. Wall, MD,b Joseph Rapp, MD,a andLouis M. Messina, MD,a San Francisco, Calif
Purpose: We sought to assess the role of endovascular techniques in the management of perigraft flow (endoleak) afterendovascular repair of an abdominal aortic aneurysm.Method: We performed endovascular repair of abdominal aortic aneurysm in 114 patients, using a variety of GianturcoZ-stent–based prostheses. Results were evaluated with contrast-enhanced computed tomography (CT) at 3 days, 3months, 6 months, 12 months, and every year after the operation. An endoleak that occurred 3 days after operationled to repeat CT scanning at 2 weeks, followed by angiography and attempted endovascular treatment.Results: Endoleak was seen on the first postoperative CT scan in 21 (18%) patients and was still present at 2 weeks in14 (12%). On the basis of angiographic localization of the inflow, the endoleak was pure type I in 3 cases, pure type IIin 9, and mixed-pattern in 2. Of the 5 type I endoleaks, 3 were proximal and 2 were distal. All five resolved afterendovascular implantation of additional stent-grafts, stents, and embolization coils. Although inferior mesentericartery embolization was successful in 6 of 7 cases and lumbar embolization was successful in 4 of 7, only 1 of 11 pri-mary type II endoleaks was shown to be resolved on CT scanning. There were no type III or type IV endoleaks(through the stent-graft). Endoleak was associated with aneurysm dilation two cases. In both cases, the aneurysmdiameter stabilized after coil embolization of the inferior mesenteric artery. There were two secondary (delayed)endoleaks; one type I and one type II. The secondary type I endoleak and the associated aneurysm rupture were treatedby use of an additional stent-graft. The secondary type II endoleak was not treated.Conclusions: Type I endoleaks represent a persistent risk of aneurysm rupture and should be treated promptly byendovascular means. Type II leaks are less dangerous and more difficult to treat, but coil embolization of feeding arter-ies may be warranted when leakage is associated with aneurysm enlargement. (J Vasc Surg 2001;34:98-105.)

JOURNAL OF VASCULAR SURGERYVolume 34, Number 1 Chuter et al 99
life expectancy was less than 2 years. We assessed the fea-sibility of endovascular aneurysm repair by use of CT scan-ning and catheter angiography. Suitable patients wereenrolled in the study after full informed consent wasobtained in accordance with the requirements of our insti-tutional committee on human research.
Stent-graft sizing. Preoperative measurements ofneck diameter and aneurysm diameter were based on CTscanning. Measurements of neck length, aneurysm length,common iliac artery length, external iliac artery diameter,and neck and iliac angulation were based on angiographyby use of calibrated catheters. In most cases, measure-ments of common iliac artery diameter were based onangiography, which we found to be more precise than CT,especially when the arteries were tortuous, heavily calci-fied, and of variable caliber. However, iliac arteryaneurysm diameters were based on the findings of CTscanning because mural thrombus precluded accurateangiographic measurement.
Anticoagulation. Eight (7%) patients were given war-farin (Coumadin) before undergoing endovascular aneurysmrepair. The Coumadin was discontinued 5 days before oper-ation and resumed before discharge. Antiplatelet therapy (inmost cases aspirin) was continued. No anticoagulants orantiplatelet agents were prescribed as part of this study.
Stent-graft insertion. These patients were treatedunder two FDA investigational device exemptions: onefor a custom-made system of our own, and the other for
the Zenith system (Cook, Inc, Bloomington, Ind). Allrepairs were performed in the operating room, and most(74%) were performed with the patients under epiduralanesthesia. We used our custom-made system of aor-tomonoiliac stent-graft implantation, together withfemorofemoral bypass and contralateral common iliacartery occlusion, in 91 cases, and an aortoaortic versionof this custom-made system in 10 cases. Zenith bifur-cated stent-grafts were implanted in 13 cases. Systemdesign and operative technique have been describedelsewhere.4
Intraoperative angiograms were studied for signs ofendoleak. Type I endoleaks were treated with a variety ofadjunctive maneuvers, including balloon dilation andreorientation of the proximal stent, additional stentimplantation, and additional stent-graft implantation.16
No patient left the operating room with angiographicsigns of type I endoleak. Intraoperative type II endoleakswere ignored.
Routine CT-based follow-up. Routine follow-upincluded contrast-enhanced CT scanning before dis-charge, which was repeated at 3 months, 6 months, 12months, and annually thereafter. When we began thisstudy, the follow-up evaluation was based on a standardabdominal CT protocol. The resulting volumetric data setwas reconstructed and displayed as a series of 10-mm axialslices. We found these studies to be insensitive, nonspe-cific, and imprecise in the diagnosis and localization of
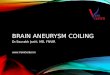
Fig 1. A, Contrast-enhanced CT scan shows area of high density (arrow), which might be read as endoleak. B, Corresponding noncontrast CT scan shows same area of high density (arrow), which cannot be result of ongoingendoleak because no contrast was present in circulating blood at time of scan.
A B

JOURNAL OF VASCULAR SURGERY100 Chuter et al July 2001
endoleaks.17 During the course of the study, we made aseries of incremental changes in both the acquisition andprocessing of CT data. Our current practice is as follows.We acquire data in three phases: before contrast infusion,shortly after contrast infusion, and 1 to 2 minutes aftercontrast infusion. The noncontrast series is used to iden-tify areas of high density (Fig 1) present before contrastinfusion, which otherwise might lead to false-positivereporting of endoleaks.17 The delayed series is used todetect type II leaks, which often fill with contrast-enhanced blood long after contrast enhancement of theaorta. The variation in delay between contrast injectionand scanning depends on transit time, as assessed by timing the appearance of a 20-mL test bolus of contrast(320 mg/mL iohexol) at the proximal end the field ofinterest. The test bolus is administered at approximately4 mL/s. Serial density readings from the center of theaorta at the level of the celiac artery are plotted to showthe interval between peak opacification and the start ofthe contrast infusion. The contrast-enhanced phase ofthe study is performed with the same delay between thestart of contrast infusion (at approximately 4 mL/s for150 mL) and the start of data acquisition. Data areacquired from proximal to distal starting at the celiacartery level. The slice thickness is 3 mm, and the pitch is1.5 to 2.0. Three-dimensional reconstruction (shadedsurface display and multiplanar reconstruction) aids inthe localization of leaks (Fig 2). Because many of ourpatients were old, sick, and reluctant to travel long dis-tances for routine studies, we often depended on outside
institutions for late follow-up, although not all adheredto our CT protocol.
Angiograpic localization and treatment ofendoleak. Any patients with an endoleak on the first post-operative CT scan were studied again at 2 weeks. Any witha persistent leak at 2 weeks underwent catheter angiogra-phy before repeat endovascular treatment.16-19
Angiographic localization of the inflow was the solebasis for the endoleak categorization reported here. Weoften found type I or mixed-type endoleaks difficult toexclude on static CT-based images, especially early in thestudy when the CT scans had poor longitudinal resolutionand no multiplanar reconstruction. Digital angiographyprovided a more dynamic picture, in which contrast-enhanced blood could be seen entering the aneurysmthrough the site of leakage. We categorized an endoleakon the basis of identification of the site of inflow, not out-flow, for two reasons. First, there was usually only one siteof inflow, in contrast to the multiple sites of outflow.Second, we usually directed treatment toward occlusion ofthe inflow, while leaving the outflow to thrombose. Thepresence of mixed-pattern leakage was established onlyafter an additional endovascular procedure had been per-formed to eliminate the type I component.
Type I leaks were treated with embolization coils, addi-tional stents, or stent-grafts. Two proximal type I endoleaksrequired an additional stent-graft, and a third required anadditional stent to enhance the seal. In addition, one ofthese patients was treated by occlusion of the lumbar arter-ial outflow with embolization coils (Cook, Inc). Both distal
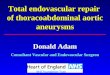
Fig 2. A, Contrast-enhanced axial CT scan show flow through lumbar artery (arrows) and resulting endoleak. B, Multiplanar reconstruction shows flow through aneurysm from one lumbar artery to another (arrows).
A B

JOURNAL OF VASCULAR SURGERYVolume 34, Number 1 Chuter et al 101
type I endoleaks occurred around the iliac occluder. In onecase this pathway was blocked by transcatheter insertion oflarge Tornado embolization coils (Cook, Inc), and in theother by insertion of an additional occluder.
Type II leaks were treated in the angiography suitewith coils to occlude the terminal arteries of the collateralpathway. We catheterized the feeding artery by followingthe collateral circulation.16-19 In some cases the pathwayled from the superior mesenteric artery to the inferiormesenteric artery (IMA) (Fig 3); in others from the inter-nal iliac arteries to the lumbar arteries (Fig 4). The goalwas always to block the route of leakage as close to theaneurysm as possible, thereby preserving perfusion of thespine, colon, and pelvis. The internal iliac and superiormesenteric arteries were catheterized by use of the coaxialtechnique. The orifice was entered with a 5F angledcatheter, and the distal branches catheterized by use of aTracker-18 catheter (Target Theraputics, Inc, MountainView, Calif) over a 0.016-in Seeker guidewire (TargetTheraputics). Embolization of the feeding artery was per-formed by use of 2- to 4-mm Tornado platinum coils(Cook, Inc).
Data collection. Routine prospective data collectionincluded information on patient characteristics, preopera-tive arterial anatomy, stent-graft type, postoperative inter-ventions, postoperative changes in aneurysm diameter,
and the presence or absence of an endoleak. Before writ-ing this report, we reviewed any equivocal findings, col-lected any missing data, and called the patients and theirphysicians to update clinical status. Two patients withendoleaks died during follow-up. In both cases, the causeof death was clear from the clinical course and neitherpatient underwent an autopsy.
Statistical analysis. Cases were categorized accordingto the phase of the study (first half vs second half), the typeof device (Zenith vs custom-made), the presence orabsence of the various types of endoleak, and the presenceor absence of various types of anatomic distortion. Thedistribution of cases among these categories was assessedby use of χ2 testing. Changes in aneurysm diameter wereassessed by use of a paired t test.
RESULTS
Between June 1996 and May 1999, we performedelective endovascular repair of abdominal aorticaneurysms in 114 patients. Endoleak was seen on the firstpostoperative CT scan in 21 (18%) patients and was stillpresent at 2 weeks in 14 (12%). The patients with persis-tent endoleak underwent angiographic localization of theleak, which proved to be pure type I in 3, pure type II in9, and a mixed-pattern leak in 2. Those that resolvedspontaneously underwent routine CT-based follow-up
Fig 3. A, Selective angiogram of superior mesenteric artery shows flow through marginal arcade into IMA (arrow) andinto aneurysm. B, Selective angiogram after embolization of the IMA trunk. IMA, Inferior mesenteric artery.
A B

JOURNAL OF VASCULAR SURGERY102 Chuter et al July 2001
study, and in these cases no attempt was made to localizeor categorize the endoleak.
There was no significant difference in ultimateaneurysm size between patients with an endoleak at 2 weeks(mean, 6.5 cm) and the group of all 114 treated patients(mean, 6.3 cm). Mean follow-up in the persistent endoleakgroup was 14.3 months. This includes two patients who hadless than 3 months of follow-up; one patient declined tocontinue in the study, another died of a subdural hematomaa month after implantation of a second stent-graft. A thirdpatient died 2 years after endovascular aneurysm repair. Theimmediate cause was pneumonia complicating a stroke.
In the first half of the study, there were 2 cases of typeI endoleak, 1 case of type II endoleak, and 1 case ofmixed-type endoleak. The corresponding numbers for thesecond half of the study were 1, 8, and 1, respectively. The only significant difference between the two halves ofthe study was the number of type II endoleaks, whichoccurred more frequently in the second half (P = .037).There was no association between endoleak and the typeof device, the presence of a specific anatomic distortion, orCoumadin anticoagulation. The anatomic distortions seenmost frequently among the 114 treated patients were asfollow: neck angulation > 45 degrees (37%), neck length < 15 mm (25%), iliac angulation > 90 degrees (20%), andcommon iliac diameter > 25 mm (17%).
Aneurysm diameter increased by 3 and 9 mm in twocases of type II endoleak during an unusually long delaybetween stent-graft implantation and embolization of the
feeding arteries necessitated by other medical problems.In both cases, there were signs of persistent endoleak onsome of the subsequent CT scans but no further increasesin aneurysm diameter. No other patients demonstratedany significant (> 2 mm) increase in aneurysm diameter.
All five type I leaks (3 pure and 2 associated with typeII endoleak) resolved after endovascular treatment. In thetwo cases of mixed endoleak, the type II endoleak was notsuspected until the type I endoleak had been obliterated.One of these patients died a month later of a subduralhematoma, whereas the other patient has had a 4-mmdecrease in aneurysm diameter, in spite of the persistenceof the type II endoleak. All three patients with pure type Iendoleak had a decrease in aneurysm diameter (mean,12.3 mm) during follow-up.
There were nine cases of pure type II endoleak. Inaddition to the two patients described above, whose leaksseemed to appear and disappear after IMA and lumbarembolization, only one other patient has shown signs ofendoleak resolution. This patient underwent IMAembolization within a month of stent-graft implantation.Although embolization was an effective means of IMAocclusion in another three cases, an endoleak was seen ona subsequent CT scan in all three because of the persistenceof lumbar collateral routes to the aneurysm. The IMAappeared to be part of the endoleak circuit in seven cases,including a case of mixed-type endoleak. Embolizationfailed to achieve IMA occlusion in only one of sevenattempts. In this case, there were multiple connections
Fig 4. A, Selective angiogram of internal iliac artery shows ascending flow (arrows) into pair of lumbar arteries and fromthere into aneurysm (arrow). B, Angiography after embolization of endoleak cavity, junction between lumbar arteries, andone of ascending internal iliac artery branches (arrows).
A B

JOURNAL OF VASCULAR SURGERYVolume 34, Number 1 Chuter et al 103
between the SMA and IMA branches, none of which waslarge enough to admit a catheter.
In contrast, lumbar embolization failed in four ofseven attempts, usually because the ascending pathways,from the internal iliac arteries to the lumbar arteries, weresmall and multiple. Moreover, all three “angiographicallysuccessful” lumbar artery embolizations can be assumedto have been incomplete, because subsequent CT scan-ning showed persistence of the endoleak through otherlumbar arteries.
All in all, there were eight cases with unresolved, orintermittently resolved endoleaks, after 3 or more monthsof follow-up. There was no statistically significant change inaneurysm diameter in these cases. Mean aneurysm diameterdecreased only 0.5 mm (P = .66) during a mean follow-upof 13.8 months. Even if one excludes the period beforeembolization, the mean decrease in aneurysm diameter was only 2 mm (P = .12) during a mean follow-up of 12 months. There were no signs of type III or type IVendoleaks through defects in the fabric of the stent-graft.
In addition to the 14 cases of primary endoleak, therewere two cases of secondary (delayed) endoleak. In onecase, proximal stent migration caused secondary type Iendoleak and aneurysm rupture a year after stent-graftimplantation. This patient was treated by implantation of asecond stent-graft. At last follow-up, his aneurysm diame-ter had decreased by more than 1 cm. A second patientdeveloped a secondary type II endoleak when he began toreceive Coumadin as prophylaxis against cardiogenicembolism. Two patent lumbar arteries were seen adjacentto the distal aneurysm at the level of the endoleak. Onreview of the earlier CT scans, it appears these lumbararteries were patent all along. They were probably part ofa circuit, which involved some of the aneurysm sac, but notenough to produce a positive CT finding of endoleak. Thisaneurysm has not changed in diameter.
DISCUSSION
These results prompted several changes in our proto-col (Table), most of which relate to the detection andmanagement of type II endoleaks. We still take a fairly
aggressive approach to type I endoleaks, treating all ofthem early in the postoperative course, but we have startedto observe type II endoleaks.
We found that pure type I endoleaks were relativelyuncommon and easy to treat. We treated all primary typeI endoleaks within a month of the initial operation in thebelief that this type of leakage represents a high risk ofaneurysm dilation and rupture. We cannot assess thisbelief on the basis of our own experience. However,reported cases of aneurysm rupture after incompleteendovascular aneurysm exclusion attest to the risk.13-15
Even when type I endoleaks resolve spontaneously, theymay reappear, and when they do the risk of rupture is evenhigher.3,12 In our experience, the high risk of rupture wasdemonstrated by the sole case of secondary type Iendoleak. This patient had no endoleak on any of thescans performed in the first year after endovascular repair,yet he returned 3 months later with a type I endoleak anda ruptured aneurysm. Fortunately, the rupture was con-tained, and we were able to eliminate the endoleak with anadditional stent-graft.
Our failure to demonstrate any anatomic risk factorsfor type I endoleak probably reflects a lack of data. We hadonly three leaks around the proximal end of the stent-graftand two around the distal end. A high rate of type I leak-age has been seen in cases with a short proximal implanta-tion site.9 Although 25% of our patients had necks of 15mm or less in length, we were careful to avoid cases inwhich a short neck was associated with other unfavorablefeatures, such as angulation, thrombus lining, or conicalshape, and we ensured stable implantation by placing anuncovered stent over the renal arteries whenever the neckwas shorter than 15 mm. Both cases of distal type Iendoleak had irregular, calcified common iliac arteries. Yetthere were many cases with these findings and no endoleak.
Type II endoleaks became more common as the studyprogressed. We attribute this increasing incidence to moresensitive diagnosis; type II endoleaks are easily missedunless the scan is performed a minute or more after injec-tion of intravenous contrast.11 The 16% rate seen in thesecond half of this study probably represents the true inci-
Endoleak management
Study Finding Response
Intraoperative angiogram No endoleak 1-month CTType I endoleak Endovascular treatmentType II endoleak 1-month CT
1-month CT No endoleak 6-month CTType I endoleak Endovascular treatmentType II endoleak 3-month CT
3-month CT No endoleak 6-month CTType II endoleak (with < 3 mm AAA diameter increase) 6-month CTType II endoleak (with > 3 mm AAA diameter increase) Endovascular treatment
6-month CT No endoleak 12-month CTType II endoleak (with < 3 mm AAA diameter increase) 12-month CTType II endoleak (with > 3 mm AAA diameter increase) Endovascular treatment
AAA, Abdominal aortic aneurysm; CT, computed tomography.

dence. Other studies1-13 have reported rates of type IIendoleak ranging from 0% to 25%. We think these varyingrates reflect differences in diagnostic sensitivity. Perhapsthe underdiagnosis of type II endoleak is responsible forthe phenomenon of “endotension,” whereby aneurysmsremain pressurized and dilate, in spite of CT evidence ofcomplete exclusion.10,20
We found type II endoleaks difficult to eliminatebecause the communicating arteries were often small andmultiple. Perhaps a more aggressive approach would haveyielded a higher success rate. When faced with multipleascending internal iliac branches to the lumbar arteries wecould have attempted to embolize them all, although thismaneuver has been known to cause paraplegia.11 Whenfaced with collateral vessels that would not admit acatheter, we could have attempted to reach the lumbarand inferior mesenteric arteries from the aneurysm side.There are two possible routes into an aneurysm afterendovascular repair. One is around the end of a self-expanding stent-graft and the other is translumbar. Wehave obtained perigraft access to the aneurysm forembolization of lumbar outflow from a type I endoleak intwo cases (one elective and one urgent), both of whichwere successful. We have no experience with the translum-bar route, which theoretically risks inducing aneurysmrupture.
Perhaps it would be better to prevent type IIendoleaks by occluding potential collateral routes into theaneurysm before or during stent-graft implantation.However, selective catheterization of multiple small aorticbranches is sometimes difficult, and even dangerous, inthe presence of a thrombus-lined aneurysm. Moreover, inthe absence of a reliable basis for selecting which branchesto embolize, many patients would have to be treatedbefore operation for every postoperative treatment thatwould be prevented. Packing the aneurysm with thombo-genic material at the time of operation appears to be morepromising. The group from Nottingham, UnitedKingdom, has reported a zero rate of endoleak after selec-tive application of this technique.21
We take the view that if a collateral connectionbetween two arterial beds is too small to admit a catheter,it is probably too small to sustain flow or contribute muchto the pressure in the recipient arterial bed. Conversely, alarge connection would maintain a high pressure environ-ment within the aneurysm, making dilation likely, andhigh flow through the aneurysm, making spontaneous res-olution unlikely. In this series, the most troublesome typeII endoleaks were fed through the large marginal arcadebetween the superior mesenteric and inferior mesentericterritories. The only instances of aneurysm enlargementoccurred when IMA embolization had to be delayed bythe patients’ other medical problems. Once the IMA wasembolized, the aneurysm ceased to dilate.
Studies on the natural history of type II endoleak haveproduced varying conclusions.10,11 However, these differ-ences are probably attributable to a combination of smallstudy size, variation in diagnostic (CT) technique, and the
underlying heterogeneity of type II endoleaks. On thebasis of experience in surgically excluded aneurysms,22 itappears that continuing perfusion, dilation, pulsatility, andrupture risk (endoleak) is quite rare (4%), even if oneincludes the cases in which persistent aneurysm perfusionwas treated at the time of the original operation.
Returning to the endovascular literature, type IIendoleaks are generally associated with less pulsatility ofthe aneurysm wall than type I endoleaks.23 On the otherhand, recent transcatheter measurements of aneurysmpressure at the time of embolization for type II endoleakshow values close to systemic.24 Of course, these readingscould not have been taken if the collateral connection hadnot been large enough to admit a catheter, which is cer-tainly not the case in all instances of endoleak.
Our policy of observation depends not only on theanticipated behavior of type II endoleak, but also on theability to distinguish type II from type I without anangiogram. This in turn depends on the quality of CT dataacquisition and processing. If the distinction betweenthese types cannot be made by CT scanning, it may benecessary to obtain an angiogram to be certain that a typeI endoleak is not present. Having obtained selectiveangiograms, we find it hard to argue against attemptingembolization. If the feeding arteries can be catheterizedeasily and occluded close to the aneurysm, there is littlerisk of inducing ischemia in the lumbar or IMA territory.
We conclude that type I endoleaks represent a techni-cal failure of endovascular repair that should be correctedpromptly by endovascular means. On the other hand, typeII endoleaks are generally benign enough to warrant aperiod of observation. In these cases, immediateembolization of feeding collateral vessels is often difficult,futile, and unnecessary. However, these conclusions arebased on a relatively short period of observation in a smallnumber of cases. We still recommend early angiographywith embolization when the aneurysm is very large, theCT scan does not exclude the possibility of type Iendoleak, or regular CT-based follow-up is problematic.
REFERENCES1. Blum U, Voshage G, Lammer J, Beyersdorf F, Tollner D, Kretschmer
G, et al. Endoluminal stent-grafts for infrarenal abdominal aorticaneurysms. N Engl J Med 1997;336:13-20.
2. Deaton D, Bogey W, Chiang K, Brigham D, Powell S. Bifurcatedendovascular grafting for abdominal aortic aneurysm. Ann Vasc Surg1999;13:23-31.
3. Matsumura JS, Moore WS. Clinical consequences of periprostheticleak after endovascular repair of abdominal aortic aneurysm:Endovascular Technologies Investigators. J Vasc Surg 1998;27:606-13.
4. Chuter TA, Reilly LM, Faruqi RM, Kerlan RB, Sawhney R, Canto CJ,et al. Endovascular aneurysm repair in high-risk patients. J Vasc Surg2000;31:122-33.
5. Yusuf SW, Whitaker SC, Chuter TA, Ivancev K, Baker DM, GregsonRH, et al. Early results of endovascular aortic aneurysm surgery withaortouniiliac graft, contralateral iliac occlusion, and femorofemoralbypass. J Vasc Surg 1997;25:165-72.
6. van Schie GP, Sieunarine K, Lawrence-Brown MMD, Hartley D. ThePerth endovascular graft for infrarenal aortic aneurysms. Seminars inInterventional Radiology 1998;15:63-9.
JOURNAL OF VASCULAR SURGERY104 Chuter et al July 2001

JOURNAL OF VASCULAR SURGERYVolume 34, Number 1 Chuter et al 105
7. Zarins CK, White RA, Schwarten D, Kinney E, Dietrich EB, HodgsonKJ, et al. AneuRx stent graft versus open surgical repair of abdominalaortic aneurysm: Multicenter prospective clinical trial. J Vasc Surg1999;29:292-308.
8. Stelter W, Umscheid T, Siegler P. Three-year experience with modu-lar stent-graft devices for endovascular AAA treatment. J EndovascSurg 1997;4:362-9.
9. Wain RA, Marin ML, Ohki T, Sanchez LA, Lyon RT, Rozenblit A, etal. Endoleaks after endovascular graft treatment of aortic aneurysms:classification, risk factors, and outcome. J Vasc Surg 1998;27:69-80.
10. Armon MP, Yusuf SW, Whitaker SC, Gregson RH, Wenham PW,Hopkinson BR. Thrombus distribution and changes in aneurysm sizefollowing endovascular aortic aneurysm repair. Eur J Vasc EndovascSurg 1998;16:472-6.
11. Resch T, Ivancev K, Lindh M, Nyman U, Brunkwall J, Malina M, etal. Persistent collateral perfusion of abdominal aortic aneurysm afterendovascular repair does not lead to progressive change in aneurysmdiameter. J Vasc Surg 1998;28:242-9.
12. White GH, Yu W, May J, Chaufour X, Stephen MS. Endoleak as acomplication of endoluminal grafting of abdominal aortic aneurysms:classification, incidence, diagnosis and management. J Endovasc Surg1997;4:152-68.
13. Chuter TA, Wendt G, Hopkinson BR, Scott RA, Risberg B, Kieffer E,et al. European experience with a system for bifurcated stent-graftinsertion. J Endovasc Surg 1997;13-22.
14. Torsello GB, Klenk E, Kazprzak B, Umscheid T. Rupture of abdomi-nal aortic aneurysm previously treated by endovascular stentgraft. JVasc Surg 1998;28:184-7.
15. Lumsden AB, Allen RC, Chaikof EL, Resnikoff M, Moritz MW,Gerhard H, et al. Delayed rupture of aortic aneurysms followingendovascular stent-grafting. Am J Surg 1995;170:174-8.
16. Chuter TA, Reilly LM, Kerlan RK, Sawhney R, Canto CJ, Ring EJ, etal. Endovascular repair of abdominal aortic aneurysm: getting out oftrouble. Cardiovasc Surg 1998;6:232-9.
17. Sawhney R, Kerlan RK, Wall SD, et al. Analysis of computed tomo-graphic findings following endovascular repair of abdominal aorticaneurysms. Radiology. In press.
18. Ivancev K, Chuter T, Lindh M, Lindbladt B, Brunkwall J, Risberg B.Options for treatment of persistent aneurysm perfusion after endovas-cular repair. World J Surg 1996;20:673-8.
19. van Schie G, Sieunarine K, Holt M, Lawrence-Brown M, Hartley D,Goodman MA, et al. Successful embolization of persistent endoleakfrom a patent inferior mesenteric artery. J Endovasc Surg 1997;4:312-5.
20. Schurink GW, Aarts NJ, Wilde J, vanBaalen JM, Chuter TAM,Schultze Kool LJ, et al. Endoleakage after stent-graft treatment ofabdominal aneurysm: implications on pressure and imaging–an invitro study. J Vasc Surg 1998;28:234-41.
21. Walker SR, Macierewicz J, Hopkinson BR. Prevention of lumbarartery endoleaks with selective use of absorbable gelatin sponge. JEndovasc Surg 1999;6:180-213.
22. Resnikoff M, Darling RC 3rd, Chang BB, Lloyd WE, Paty PS,Leather RP, et al. Fate of the excluded abdominal aortic aneurysm sac:long-term follow-up of 831 patients. J Vasc Surg 1996;24:851.
23. Malina M, Lanne T, Ivancev K, Lindblad B, Brunkwall J. Reducedpulsatile wall motion of abdominal aortic aneurysm after endovascularrepair. J Vasc Surg 1998;27:624-31.
24. Fairman RM, Velazquez OC, Criado FJ, Pyerson AM, Barker CF.Endovascular repair of aortic aneurysms: critical events and adjunctprocedures. J Vasc Surg 2001;33:1226-32.
Submitted Sep 28, 1999; accepted Dec 13, 1999.