Embed Size (px)
Citation preview

Emergency Lecture SeriesEmergency Lecture Series:Brain Death and Organ Donation
Robert Altman, R5McGill NeurologyAugust 10th 2011
Outline
• Pre-Test• Brain death exam in context of “prognostication”
skills• Definition and standardized exam for brain death
– Canadian + Transplant Quebec guidelines– AAN guidelines (recently updated 2010)
• Organ donation; Transplant Quebec• Neuro-otology reinforcement• Post-test

Pre-Test
1. How many criteria are there to establish NDD? 2. Explain which side the MLF is lesioned if I instil
cold water into the pt’s L ear and you get this response.
– Is this compatible with NDD?3. What are the apnea test parameters?4. What are the 2 “ancillary tests” that should be
used when clinical grounds for NDD cannot be established? • Transcranial
doppler• Conventional angio• MRA/I
• Tc99HMPAO nuc. med. Scan• EEG• SSEP

AAN 2006 Practice
Parameter
Remember...

Vancouver, 2003
• In all Canadian provinces and territories, the legal definition of brain death is “according to accepted medical practice.” – Practices are largely determined by individual
hospitals or regions. – Guidelines established by the Canadian Congress
Committee on Brain Death in 1986 and the Canadian Neurocritical Care Group in 1997 initiated clarification of the criteria, but have not led to uniform practice.

• “Severe Brain Injury to Neurological Determination of Death,” held in Vancouver from 9 to 11 April 2003, was to initiate the development of a national agreement on the processes of care, commencing with severe brain injury and culminating with NDD


Overarching Recommendations
• NDD = Neurological Determination of Death– Confirmation of NDD = legal time of actual death
• Even if there is intact cardiac functions (assumed this will be temporary, and non-sustained)
• No clear medical basis for 2 independent exams– Can be performed by 2 MD’s concurrently– If performed at different times, a full clinical examination,
including apnea testing, must be performed at each determination
– No fixed interval of time is recommended for the second determination, except where age-related criteria apply

NDD (Neurological Determination of Death)
• Aetiology established that can cause irreversible death• No confounders
• Deep coma– Absence of motor responses to stimuli, no spontaneous or
abnormal movements (dyskinesia, posturing) or seizures– N.b. spinal reflexes may exist
• Absence of brainstem reflexes– No spontaneous breathing during apnea test
• Infants (≥30d and <1yr); repeat exam recommended

R/O These Confounders1. Unresuscitated shock2. Hypothermia (core temperature <34 °C)3. Severe metabolic disorder capable of causing a potentially
reversible coma– Glucose, E+ (PO4, Ca, Mg), IEM, LFT, creatinine, BUN
• Should correct any abnormality that could possibly influence decision
4. Peripheral nerve / muscle or NMJ blockade5. Drug intoxications
– ETOH, barbituates, sedatives, hypnotics• Should calculate 5 ½ lives to clear drug; longer if cooled.
– NB therapeutic levels of AED, sedatives or analgesics do not preclude the diagnosis

Irreversible Cause of Death• Neurological assessments may be unreliable in
the acute post-resuscitation phase after cardiorespiratory arrest. In cases of acute hypoxic-ischemic brain injury, clinical evaluation for NDD should be delayed for 24 h subsequent to the cardiorespiratory arrest or an ancillary test could be performed.
• Core temperature MUST be ≥ 34°C to proceed with formal testing.– Central blood, rectal or esophageal–gastric– Previously was 32.2°C

Brain Death Exam• Brainstem
– Pupils• ≥4-9mm, unresponsive to light* (enquire about Rx given)
– Corneals• Movement of jaw or lids excludes NDD
– Vestibulo-ocular responses• OCR (Doll’s)
– Caution if trauma
• Cold calorics– Pharyngeal
• Stimulate posterior pharynx• Suction the ETT• Depress larynx, swallow reflex
– Apnea test

Vestibulo-ocular Response

Oculocephalic and caloric response.
Bateman D E J Neurol Neurosurg Psychiatry 2001;71:i13-i17©2001 by BMJ Publishing Group Ltd

Doll’s Eyes• Normal response = eyes always
gaze up towards roof• Rapid, but steady movements and
observe for direction of gaze– Activates vestibular system
ipsilateral to head thrust (same principal for HIT)
• Communicates with contralateral horizontal gaze center (CN VI) “orchestrating” the action of the eyes
• Simultaneously dampens contralateral vestibular tone, etc.
Left vestibular tone
L CN VI (HGC) Right vestibular tone
R CN VI (HGC)
Turn to left + - - +
Turn to right - + + -

Cold Calorics
• 30° to the horizontal• Minimum of 50cc of ice cold water into the inner
ear canal– Ensure no perforated tympanic membrane before
instilling water– Use kidney basin, prop up beside ear
• Start observing for eye deviation rapidly; eye movements should be absent for 1 minute
• Minimum of 5 minutes before evaluating contralateral side

Cold Caloric TestingCold Caloric TestingVestibulo-Ocular Reflex (VOR)
Attenuates resting state vestibular tone
Pearl: COWS mneumonic implies intact cortex (frontal eye fields). If on coma / sedated, will not get corrective nystagmus.

Warm Caloric TestingWarm Caloric Testing(Rarely done in
neurology...)
Increases resting state vestibular tone
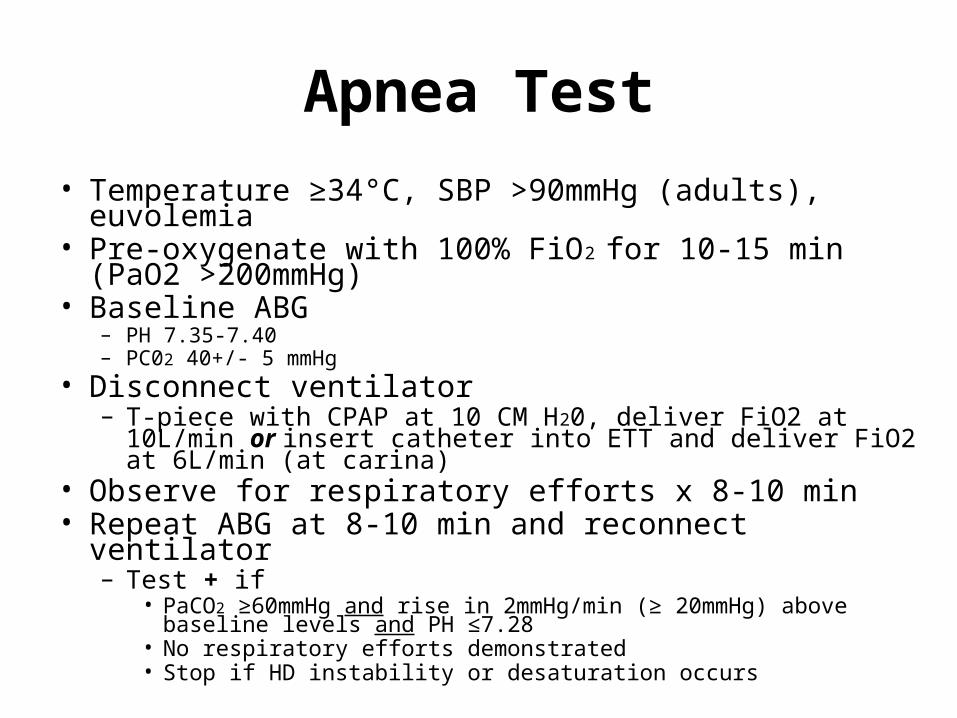
Apnea Test• Temperature ≥34°C, SBP >90mmHg (adults), euvolemia• Pre-oxygenate with 100% FiO2 for 10-15 min (PaO2
>200mmHg)• Baseline ABG
– PH 7.35-7.40– PC02 40+/- 5 mmHg
• Disconnect ventilator– T-piece with CPAP at 10 CM H20, deliver FiO2 at 10L/min or insert
catheter into ETT and deliver FiO2 at 6L/min (at carina)• Observe for respiratory efforts x 8-10 min• Repeat ABG at 8-10 min and reconnect ventilator
– Test + if• PaCO2 ≥60mmHg and rise in 2mmHg/min (≥ 20mmHg) above baseline
levels and PH ≤7.28• No respiratory efforts demonstrated• Stop if HD instability or desaturation occurs

Apnea Test (if lung disease)
• If severe lung disease– Caution must be exercised in considering the validity
of the apnea test– If in the physician’s judgment, there is a history
suggestive of chronic respiratory insufficiency and responsiveness to only supranormal levels of carbon dioxide, or if the patient is dependent on hypoxic drive.
– If the physician cannot be sure of the validity of the apnea test, an ancillary test should be administered.

Ancillary Testing
• The term “ancillary” should be understood to mean an alternative test to one that otherwise, for any reason, cannot be conducted. – No longer called “confirmatory” or “supplemental”– Different connotations
• Gold standard = global absence of intracerebral blood flow (only 2 tests support)– Cerebral angiography or radio-isotope scan

Accepted Ancillary Test(s)
Normal Brain Death

Insufficient Ancillary Testing

Special Circumstances• Children ≥ 1 yr (including adolescents)
– Same criteria– Mandates a second exam
• No fixed time interval– Physician qualified with working with critically ill children (i.e, not an adult
neurology resident doing an elective at the MCH)
• 30 days to 1 year old (corrected for GA)– Minimum clinical criteria = OCR (more reliable due to external auditory canal
anatomy)– Repeat exam recommended by another physician / at another time (lack of
collective experience and research on brain death in this age group)– If uncertain or confounders factoring in, extend time interval or perform
ancillary testing– Specialists with skill and knowledge in management of infants with severe
brain injury

NDD recommendations for term newborns aged <30d
• Standards apply for all those >36wks gestation*• NDD is clinical
– Absence of OCR and suck reflex– Temp (core) ≥ 36°C
• Min time from birth to first determination is 48h• 2 determinations required, minimum interval 24h • Ancillary testing:
– Should be performed when any of the minimum clinical criteria cannot be established or confounding factors remain unresolved
• “specialists with skill and knowledge in the management of newborns with brain injury and the determination of death based in neurological criteria.”

Other tidbits
• NDD can be determined (in adults)– any physician licensed by the college of physicians
and surgeons or licensing authority in that jurisdiction.
– excludes physicians who are only on an educational register.
– does not require a particular level of specialty certification;
– nonspecialists can declare NDD if they have the requisite skill and knowledge.

Organ Donation• 3 pronged approach
– Environment• Caring attitude; be open and honest• Ask if family members around, or if there is a family spokesperson• Take family to private room• Offer pastoral services• Offer phone, tissue, etc.
– Knowledge• Assess loved-ones comprehension of the situation• Emphasize irreversibility of brain death• Repeat the information as many times as necessary• Grant enough time to assimilate the new knowledge
– The Question (at a future time-point)• Verify wished of deceased (organ donor signature on RAMQ card)• Be attentive to apprehension; answer questions +++• Offer possibility of communication with T-Q• Emphasize possibility of giving the gift of life to another
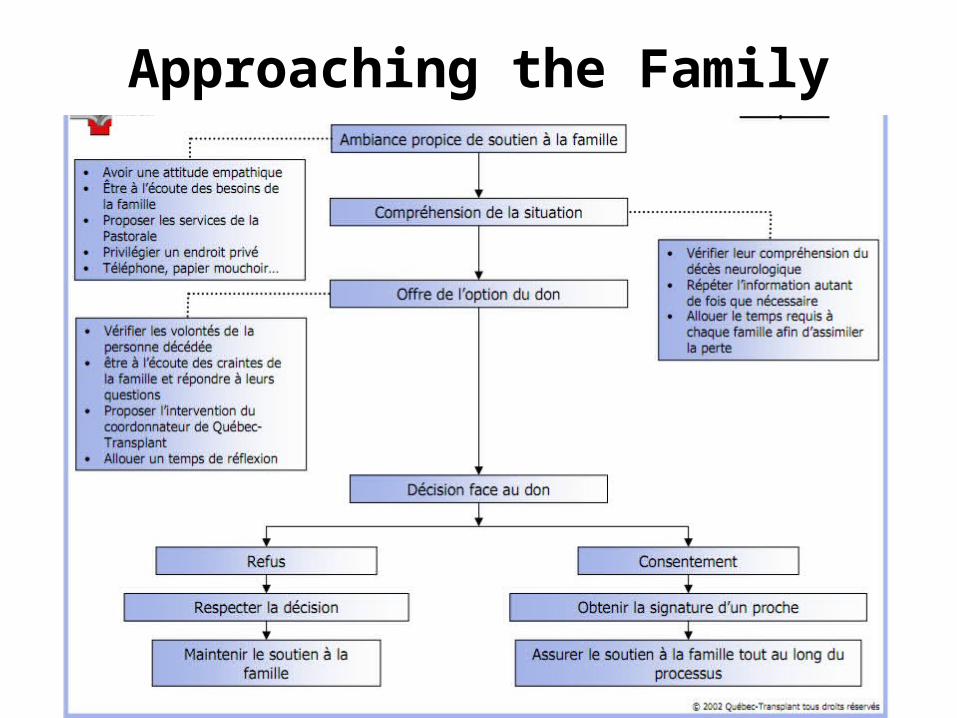
Approaching the Family

Possibilities of Donation• <70 yo; any tissues• Any age; eyes / cornea
– Transplant Québec (24/7)Tel: 514-286-0600
Web: www.quebec-transplant.qc.ca• Heart, lungs, pancreas, liver, kidneys, intestines
– Héma Quebec • Cardiac valves, bone, skin, tendons
– Banque d’yeux• Cornea

Resources
• http://www.quebec-transplant.qc.ca• CMAJ: Brain arrest: the neurological
determination of death and organ donor management in Canada
• AAN 2010 Clinical practice guidelines on brain death– Including PowerPoint presentation

Post-Test1. How many criteria are there to establish NDD? (4)
• Death by something known to be able to kill you.• No confounders.• Deep coma with absent motor responses; except local spinal reflexes.• Brainstem death: absent corneals, gag, VOR, pupils midposition and areactive, +
apnea test.
2. Explain which side the MLF is lesioned if I instil cold water into the pt’s L ear and you get this response.
– Is this compatible with NDD?3. What are the apnea test parameters?4. What are the 2 “ancillary tests” that should be used
when clinical grounds for NDD cannot be established?• Transcranial
doppler• Conventional angio• MRA/I
• Tc99HMPAO nuc. med. scan• EEG• SSEP



Vestibular apparatus
Vestibular nucleus
PPRF
VI
“HORIZONTAL GAZE CENTER”
Lateral rectus
MLF = Medial Longitudinal Fasciculus
Medial rectus
III
Normal Vestibular Physiology

JGH ER, July 2011
• 65M, felt abrutly unwell one evening, then literally “flung off his couch,” illusion of spinning around his room.– a/w nausea and vomiting, no other craniobulbar
symptoms.
• Exam demonstrates a right beating nystagmus in primary gaze, worsened on R gaze, dampened on L gaze, but nontheless present...
• Remainder of exam normal (including TOS).

Which vestibule is hypofunctioning?

Vestibular nucleus
PPRF
VI
L Vestibular Neuronitis
Dampened
Dampened
Slow tonic deviation L
Left FEF
PPRF
VI
Rules1. Hypofunctioning
implies fast phase away (vestibular neuronitis) OR eyes tonically drift to impaired side
2. Hyperfunctioning (BPPV), fast phase towards dysfunctional vestibular apparatus
III
Vestibular apparatus
slow
fast fast
slow
LR

Vestibular apparatus
Vestibular nucleus
PPRF
VI
R Irritative phase of neuritis
Irritated
Irritated
Slow tonic deviation L
Slow Slow
L FEF
PPRF
VI
Rules1. Hyperfunctioning (BPPV), fast
phase towards dysfunctional vestibular apparatus
III
fast fast
LR