Embed Size (px)
Citation preview

34 1
Embolization of a Dural Arteriovenous Malformation Using Gianturco Coils Soo Sung Han,1 Carolyn E. Parry,1 and Frederick A. Simeone2
A patient had a congenital dural arteri ovenous malformation in the supraorbital and subfrontal regions . The malformation was successfully embolized using both a percutaneous approach with transcatheter embol ization of a Gianturco co il , and a direct approach with embolization of coils through an 18 gauge needle after surgical exposure of the aneurysmal venous sac .
Case Report
A 16-year-old girl was seen by a local ophthalmolog ist because of diplopia and fullness of the right eye. Exam ination revealed visual acuity of 20/20 in both eyes with a 2-3 mm proptosis of the right eye. The right eye was also displaced downward with restri c tion of upward gaze and redness of the right canthus. There was a machine- li ke bruit over the right eye and a thrill over the right supraorbital reg ion. The patient was admitted to the hospital for further evaluation and treatment.
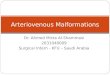
Right-sided selective internal and external angiog raphy revealed a dural arteriovenous malformation in the supraorbital and subfrontal regions. The major feed ing arteries were the middle deep temporal and middle meningeal arteries from the internal maxillary artery and , a lesser contribution, th e ethmoidal meningeal artery from a branch of the ophthalmic artery (fig . 1).
Because the external carotid artery was the major feeding artery of the large dural arteriovenous malformation, superselective catheterizat ion was done and a 3 mm mini Gianturco coil was introduced through a size 5 French catheter. Postembolization extern al carot id arteriography revealed a complete occlusion of th e middle meningeal artery as well as the distal part of the intern al maxillary artery (fig. 2A). A postembolization selecti ve internal carotid arteriogram revealed filling of the aneurysmal dilated venous sac from the ethmoidal branch of the ophthalmic artery. Ph ysical examinat ion at that time revealed a decreased orbital bruit and improvement of the diplopia.
Five days later, a frontotemporal craniotomy was performed and the residual dural arteriovenous malformation was exposed . An 18 gauge need le was direct ly inserted into the aneurysmal venous sac and 8 mm Gianturco coils were introduced . After this, the medium (5 mm) and mini (3 mm) coils were injected. A total of 18 coils were introduced until there was no blood return through the needle. The craniotomy was closed and the postoperative course was uneventful. Postoperative arteriography revealed the dural arteriovenous malformation (AVM) to be completely occluded by the coils in the
Received April 15, 198 1; accepted after revision November 25, 1981
supraorbital and subfrontal reg ions (fig. 2B). The patient was completely asymptomatic with no orbital bruits . One month later th e patient remained asymptomatic with normal vision and no diplopia.
Discussion
Interventional radiology has become increasingly important in the past decade as newer or less traumati c methods of therapy are developed for various diseases. The first neurologic embolization was performed by Brooks in 1930 when he embolized a posttraumatic carotid-carvernous fistula with a muscle embolus [1). Since that time other conditions such as AVMs, aneurysms, intractable epistax is, and vascular tumors of the head and neck have proved to be amendable to embolizati on [2-19).
The ideal transcatheter embolization material shou ld be nonantigenic, noninflammatory, noncarcinogenic , easi ly introduced, and permanent. Autologous clots , muscle embolus, and gelfoam are not permanent agents [19, 20). Silicone spheres, Ivalon, isobutyl-2-cyanoacryl ate and Gianturco co ils are permanent agents [2-1 2, 21, 22). In thi s case, Gianturco coils were used for the treatment. Although extracranial meningeal branches were embolized by the catheter technique, the ethmoidal meningeal branches of the ophthalmic artery could not be embolized. The large venous sac could also not be catheterized and embolized because the blood flow in the large ophthalmic vein would carry embolic material to the heart and result in a pu lmonary embolism. A detachable balloon [16-18] might be considered for occlusion of the meningeal arteries, but was not thought to be suitable for this patient. Surgical removal of the AVM was not considered appropriate in this case because of a large venous drainage through the ophthalmic vein.
Considerable experience in embolization of vascular lesions with Gianturco coils in extracranial locations has been reported [23-26). In our case of a large dural AVM , a combined catheter and direct approach using the coil s was used. As a first step , med ium and small branches of the extracranial meningeal arteries were occluded. The second step was a direct exposure of the venous sac and direct
I Department of Radiology, Pennsylvania Hospital , 8 th and Spruce Streets, Philade lph ia, PA 19107 . Address repri nt requests to S. S. Han. 2 Department of Neurosurgery, Pennsylvania Hospital, Philadelphia, PA 19 107.
AJNR 3:341-343, May/ June 1982 0195-6108/ 82 / 0303-0341 $00.00 © American Roentgen Ray Society

342 HAN ET AL. AJNR: 3 , May I June 1982
A B
Fig. 1.-Lateral view arteriog rams. A, Extern al ca rotid artery. Dura l arteriovenous malformation (AVM) fed by middle meningeal artery (arrows) and middle deep temporal artery (arrowheads ). B, Superselective view of middle
A B
introduction of large coi ls that were trapped in the malformation.
REFERENCES
1 . Brooks B. The treatment of traumatic arteriovenous fistu la. South Med J 1930;23: 1 00-1 06
c deep temporal artery. Dural AVM filled. C, Intern al carotid artery. Dural AVM filled by ethmoidal meningeal artery (arrowheads ) originating from ophthalmic artery.
Fig. 2. - A, Postembolizati on external ca rotid arte riog ram. Lateral view. Meningeal arteri es and intern al max illary artery completely occluded using single 3 mm Gianturco coil (arrows) with no filling of dural arteriovenous malformati on. B, Postoperative intern al carot id arteriogram. Lateral view. Aggregated co ils introduced after exposure of dural venous sac. Dural arteriovenous malformation no longer fill s from ethmoidal branch of ophthalmic artery.
2. Luessenhop AJ , Velasquez AC. Observations on the to lerance of the intracranial arteries to catheterization . J Neurosurg 1964;2 1 :85-91
3. Krichelf II , Madayag M. Braunstein P. Transfemoral catheter embolization of cerebral and posterior fossa arteriovenous malformations. Radiology 1972; 103 : 1 07 -111
4. Wolpert SM, Stein BM . Catheter embolization of intracranial arteriovenous malformations as an aid to surgical excision.

AJNR :3 , May / June 1982 EMBOLIZATION OF DURAL AVM 3 4 3
Neuroradiology 1975; 10 : 73- 85 5. Hilal SK, Michelsen JW. Therapeutic percutaneous emboliza
tion for extraaxial vascular lesions of the head, neck, and spin e. J Neurosurg 1975;43: 275-287
6 . Doppman JL, Zapol W, Pierce J. Tran scatheter embolization with a silicone rubber preparation experimental observat ions. Invest Radio/1971 ;6 : 304-309
7. Zanetti PH , Sherman FE . Experimental evaluation of a ti ssue adhesive as an agent for the treatment of a aneurysms and arteriovenous anomalies. J Neurosurg 1972;36: 72-79
8. Dotter CT, Goldman ML, Rosch J . Instant selective arterial occ lusion with isobutyl 2-cyanoacrylate. Radiology 1975;114:227-230
9 . Kerber CW, Cromwell LD, Sheptak PE. Intraarterial cyanoacrylate: an adjunct in the treatment of spinal / paraspinal arteriovenous malformations. AJR 1978; 1 30 : 99-1 03
10. Kerber C. Intracranial cyanoacrylate: a new catheter therapy for arteriovenous malformations (letter). Invest Radiol 1975; 10 : 536-538
11. Berenstein A, Kricheff II. Catheter and material selection for transarterial embolization: technical considerations. II. Materials. Radiology 1979;132:631-639
12. Zollikofer C, Castaneda-Zuniga WR, Galliani C, Rysavy JA, Formanek A, Amplatz K. Therapeutic blockade of arteries using compressed Ivalon. Radiology 1980; 136 : 635-640
13 . Sokoloff J, Wickbom I, McDonald D, Brahme F, Goergen TG, Goldberger L. Therapeutic percutaneous embolization in intractable epistaxis . Radiology 1974;111 :285-287
14. Djindjian R, Theron CJ , Merland JJ , Houdart R. Embolization by superselective arteriography from the femoral route in neuroradiology review of 60 cases. Neuroradiology 1973;6 : 20-26
15. Ruggiero G, Grillo BA, Santora G. Two cases of glomus tumors
treated by unusual embolization. Neuroradiology 1976 ;11 : 265- 269
16. Serbinenko FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg 1974;41 : 1 25-145
17. Debrun G, Lacour P, Caron JP, et al. An Experimental approach to the treatment of carotid cavernous fistulas with an inflatable and isolated balloon. Neuroradiology 1975;9 : 9-1 2
18. Laitinen L, Servo A. Embolization of cerebral vessels with inflatable and detachable balloons. J Neurosurg 1978;48: 307 - 308
19. Stanley RJ , Cubillo E. Nonsurgical treatment of arteriovenous malformations of the trunk and limb by transcatheter arterial embolization. Radiology 1975;11 5 : 609-612
20 . Osterman FA, Bell WR , Montali RJ, Novak GR, Wh ite RJ . Natural history of autologous blood clot embolization in swine. Invest Radio/1976 ; 11 : 267 -276
21. White RI Jr, Strandberg JV, Gross GS, Barth KH. Therapeutic embolization with long-term occluding agents and their effects on embolized tissues. Radiology 1977; 125 : 677 - 687
22. Kerber C. Experimental arteriovenous fi stula c reation and percutaneous catheter obstruction with cyanoacrylate. Invest Radio/1975 ;10 :10-17
23. Gianturco C, Anderson JH , Wallace S. Mechanical devices for arterial occlusion. AJR 1975; 124 : 428-435
24 . Wallace S, Gianturco C, Anderson JH , Goldstein HM , Davis LJ, Bree RL. Therapeutic vascular occlusion utilizing steel co il technique: c linical applications. AJR 1976; 127 : 381 -387
25. Goldstein HM, Wallace S, Anderson JH , Bree RL, Gian turco C. Transcatheter occ lusion of abdominal tumors. Radiology 1976; 120 : 539-545
26. Chuang VP, Wallace S, Gianturco C. A new improved coil for tapered-tip cath eter for arterial occlusion. Radiology 1980; 135: 507 - 509