Embed Size (px)
Citation preview
Electrical Characteristics of Channelopathies Involving
Skeletal MuscleBob Ruff, M.D., Ph.D.
Chief, SCI Service
Louis Stokes Cleveland VAMC
Barbara E. Shapiro, M.D., Ph.D.
Case Western Reserve Univ.
Jacob Levitt, M.D.
Albert Einstein College of Medicine

Objectives• To understand factors regulating membrane
excitability in skeletal muscle
• To understand how impaired Na+ channel inactivation can produce myotonia
• To appreciate how persistent depolarization produces paralysis (Myotonia vs HyperKPP)
• To learn different ways to produce a persistent depolarization (HyperKPP vs HypoKPP)
Roles of Na+, K+ and Cl- Channels in Membrane Excitability
• Kir sets resting membrane potential• Kv (delayed rectifier) repolarizes after AP• Cl- channel stabilizes membrane potential• INa drives AP

Potassium Sets Membrane Resting Potential
• K+ conductance 20% of membrane conductance - Inward or anomalous rectifier K+ channel (KIR)
• AP Termination - Delay Rectifier K+ Channel
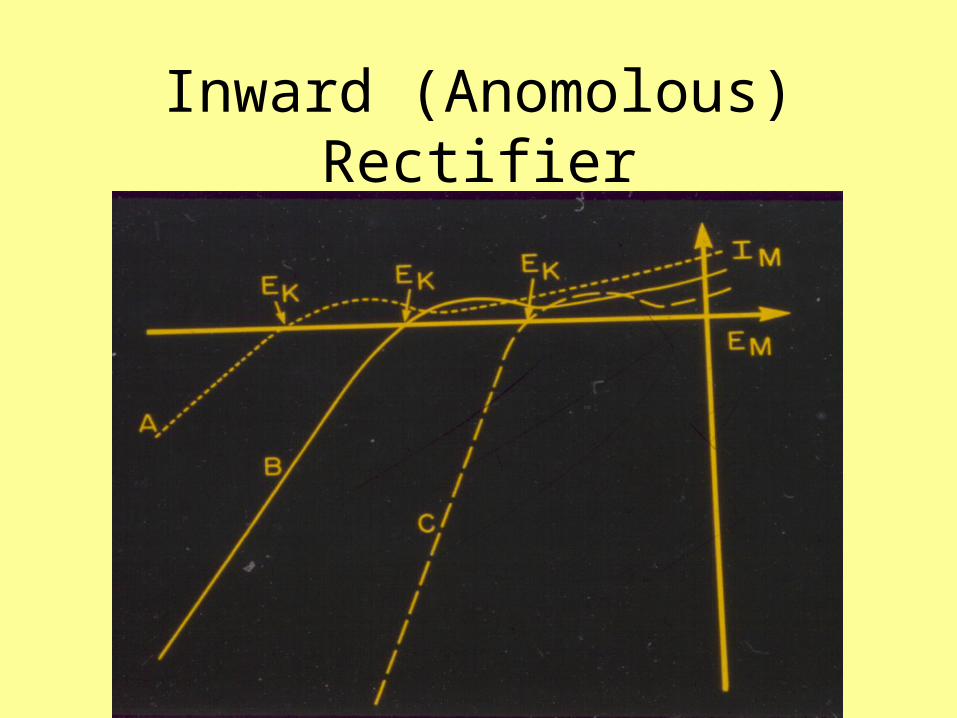
Inward (Anomolous) Rectifier

Sodium channel gating properties
• Depolarization activates Na channels - changes from a closed to an open state
• The declining portion of INa - transition of open channels to a non-conducting fast inactivated state


Two Types of Skeletal Muscle Sodium Channel Inactivation
• Fast inactivation – msec, Slow inactivation - seconds • Fast inactivation helps to terminate the AP• Slow inactivation operates at more negative potentials -
regulates the number of excitable sodium channels as a function of the membrane potential

Action Potential

Factors Determining Action Potential Threshold
• Number of excitable Na+ channels (# of channels and fraction that are excitable)
• Voltage dependence of Na+ channel opening
• Amount of Cl- conductance
• Inward rectifier K+ conductance with depolarization

Periodic Paralysis• Results from persistent membrane
depolarization inactivation of normal Na+ channels membrane inexcitability
• HyperKPP – Na+ channelopathy – depolarization due to abnormal persistent INa
• HypoKPP – – Type I - Indirect Ca2+ Channelopathy– Type 2 - Na+ channelopathy – loss of function

Hyperkalemic Periodic Paralysis (HyperPP) - AD
• episodic attacks of flaccid weakness• myotonia is often present (vs HypoK-PP)• paralysis caused by membrane depolarization
Na+ channel inactivation• Overlap: Na+ Ch myotonias, paramyotonia
Lehmann-Horn, Rudel, Ricker

Impaired fast inactivation can produce myotonia
1 msec
Note: Loss of inactivation in a small % of channels → myotonia
Myotonia stopped in part due to accumulated slow inactivation
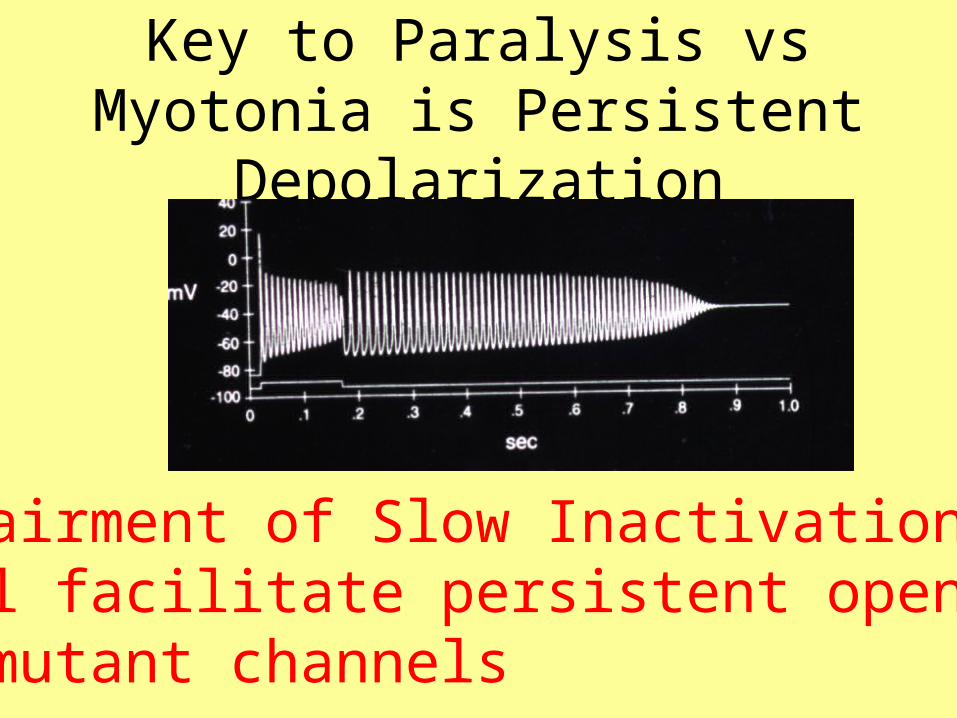
Key to Paralysis vs Myotonia is Persistent Depolarization
Impairment of Slow Inactivationwill facilitate persistent opening of mutant channels

Hypokalemic Periodic Paralysis (HypoKPP) - AD
• Episodic attacks of flaccid paralysis• Myotonia never present (vs HyperKPP)• Insulin paralytic attack without K+
• Membrane excitability impaired – low conduction velocity: Drs. Haenen, Links, Oosterhuis, Stegeman, van der Hoevan, van Weerden & Zwarts

Depolarization not blocked by TTXInsulin Enhances Depolarization
Lehmann-Horn, Rudel, Ricker
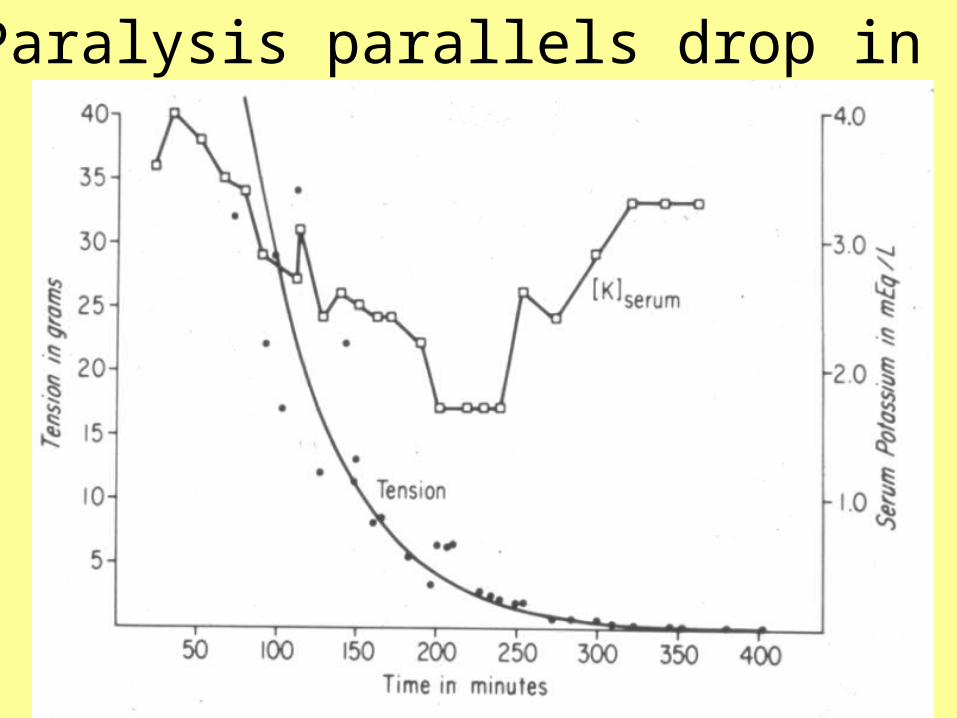
Paralysis parallels drop in K+

In HypoKPPWeaknessParallels Depolarization& Reductionin EMGAmplitude

Skeletal Muscle Membrane Excitability Is Impaired in HypoKPP (Type1)
• Muscle fibers very susceptible to depolarization-induced inexcitable
• Small depolarizations (10 mV) make HypoKPP fibers unexcitable
• Slow conduction velocity (Zwarts’ lab) suggests impaired Na+ channel function in HypoKPP
Two Genotypes - Similar Phenotype
• Type 1 HypoKPP is linked to 1Q31-32• Defective gene (CACNL1A3) encodes a
skeletal muscle dihydropyridine (DHP) sensitive or L-type calcium channel
• Mutations - segment 4 of domain 2 (R528H) and segment 4 of domain 4 (R1239H, R1239G) of the -subunit of the skeletal muscle L-type Ca+2 channel
Two Genotypes - Similar Phenotype
• Type 2 HypoK-PP has a similar phenotype to type 1 HypoK-PP
• Associated with point mutations in the Na+ channel gene (SCN4A)
• Surface membrane INa is reduced to about 50% of normal (reduced expression and increased resting inactivation)

Type 1 HypoKPP – Altered Inward (Anomolous) Rectifier
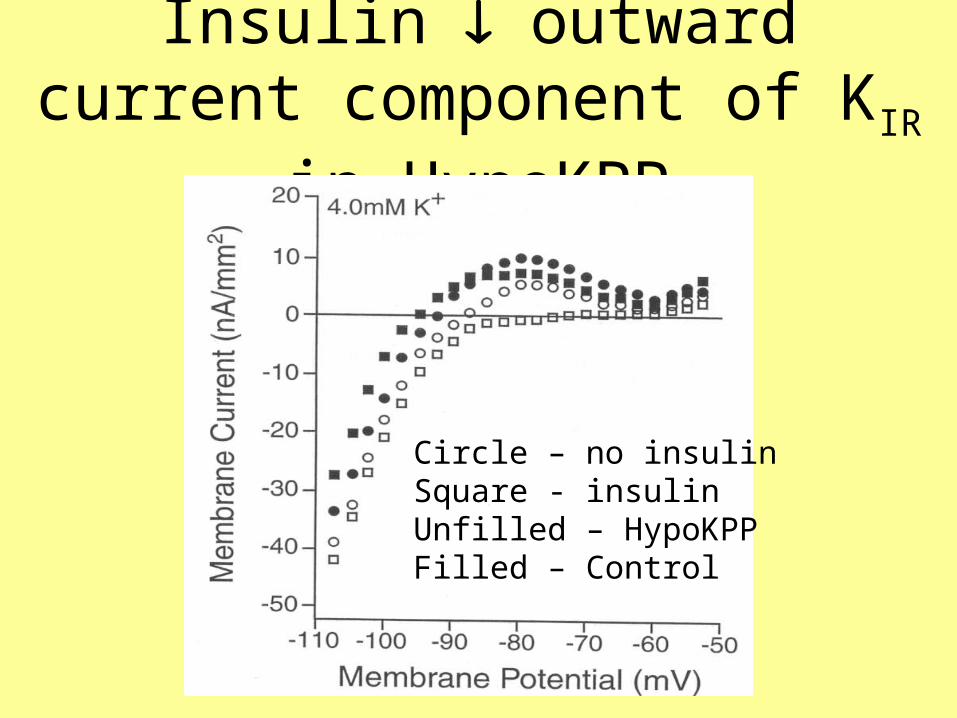
Insulin outward current component of KIR in HypoKPP
Circle – no insulinSquare - insulinUnfilled – HypoKPPFilled – Control
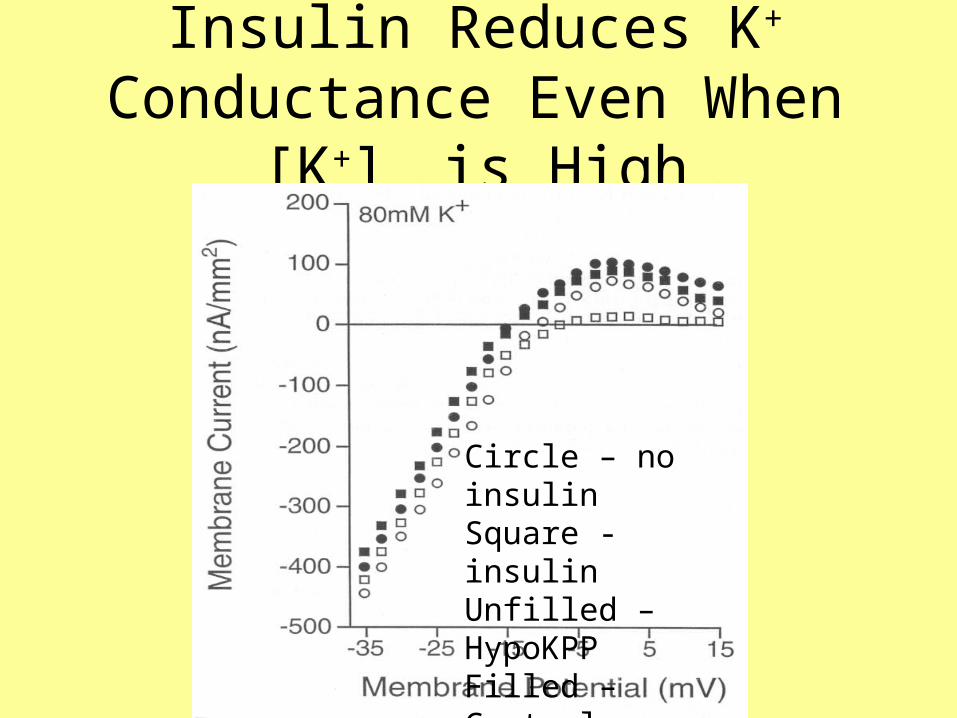
Insulin Reduces K+ Conductance Even When [K+]o is High
Circle – no insulinSquare - insulinUnfilled – HypoKPPFilled – Control

Summary of Alterations of Inward Rectifier K+ Channel in HypoKPP
• Baseline Inward Rectifier Conductance Including KATP Channels is Reduced
• Insulin selectively reduces the K+ conductance for outward currents
• Lowering [K+]o causes depolarization due to TTX- and DHP-insensitive depolarizing current (low Kir conductance for outward current facilitates depolarization)
• Note: Andersen-Tawil Syndrome due to Kir mutation

Why do Type I and Type II HypoKPP have similar phenotypes?
• The effects of the Na+ channel mutations in Type II HypoKPP are to reduce membrane channel density and to increase the amount of resting inactivation - both lead to INa
• Susceptibility of Type I HypoKPP fibers to depolarization-induced inactivation and lower AP conduction velocities suggest reduced INa
in HypoKPP (Zwarts’ lab)

Small Depolarizations Produce Paralysis in HypoKPP

Comparison of Na+ Channel Properties and Action Potential (AP) Thresholds in Fast Twitch, Type IIb, Skeletal Muscle Fibers from Five Patients with HypoKPP and Seven Controls.
Controls HypoKPPNa+ Channel PropertiesMax INa (mA/cm2) 23.7 15.4
±1.3 ±1.9 (p<0.001)
Action Potential (AP) ThresholdsAP Threshold (mV) -58.7 -53.4
±1.5 ±1.1 (p<0.001)

Which Membrane Change Correlates Best with Paralytic Attacks in Type 1 HypoKPP?
•INa correlated inversely with frequency of paralytic attacks (Pearson’s correlation coefficient, r = -0.996)
•AP threshold correlated with the frequency of paralytic attacks (r=-0.921)
•Peak outward K+ conductance of the inward rectifier K+ channel correlated weakly with the frequency of paralytic attacks (r = -0.121).
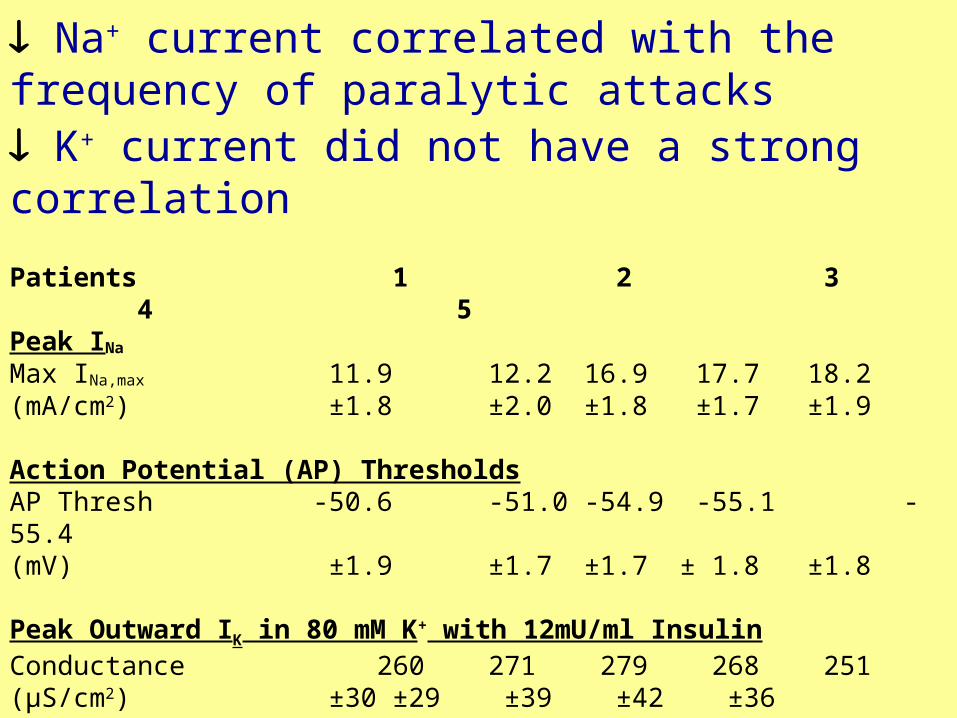
Na+ current correlated with the frequency of paralytic attacks K+ current did not have a strong correlation
Patients 1 2 3 4 5Peak INa
Max INa,max 11.9 12.2 16.9 17.7 18.2(mA/cm2) ±1.8 ±2.0 ±1.8 ±1.7 ±1.9
Action Potential (AP) ThresholdsAP Thresh -50.6 -51.0 -54.9 -55.1 -55.4(mV) ±1.9 ±1.7 ±1.7 ± 1.8 ±1.8
Peak Outward IK in 80 mM K+ with 12mU/ml InsulinConductance 260 271 279 268 251(µS/cm2) ±30 ±29 ±39 ±42 ±36 Number of Paralytic Attacks (lasting >1 hour) in one year 15 13 3 2 1

How Can Ca2+ Channel Mutations Alter Na+ & K+ Channel Properties?
• The Ca2+ channel mutations may disturb intracellular [Ca2+]
• Intracellular Ca2+ is known to regulate Na+ channel expression and can alter the expression and properties of other channels

Intracellular [Ca2+] is increased in HypoKPP Fibers
Intracellular [Ca2+] Determined with a Calcium Sensitive Electrode in Type I, IIa and IIb Control and HypoKPP Human Intercostal Muscle Fibers
Intracellular [Ca2+](µM) According to Fiber Type Type I Type IIa Type IIb Controls 0.113±0.005 0.094±0.005 0.081±0.003 n=27 n=22 n=58
HypoPP 0.129±0.009 0.112±0.008 0.100±0.006 n=11 n=12 n=16
p<0.05 p<0.05 p<0.01

Indirect Channelopathy -Intracellular [Ca2+] may Down Regulate Na+ and KIR
(incl. KATP) Channels
Ca2+ mutations in HypoKPP may reduce Na+ channel density (and perhaps alter Inward Rectifier K+ Channel Function) by elevating intracellular [Ca2+], which reduces the level of the Na+ channel -subunit mRNA (and perhaps reduces expression of KATP Channels)

Thyrotoxic Periodic Paralysis: the brother of Hypokalemic
Periodic Paralysis
Bob Ruff, M.D., Ph.D.
Chief, SCI Service
Louis Stokes Cleveland VAMC
Director Rehabilitation Research & Development Department of Veterans Affairs.
Objectives• To understand distinguishing features of
Thyrotoxic Periodic Paralysis (TPP)
• To compare channel defects in TPP with HypoKPP
• To consider how thyrotoxicosis contributes to the pathogenesis of TPP
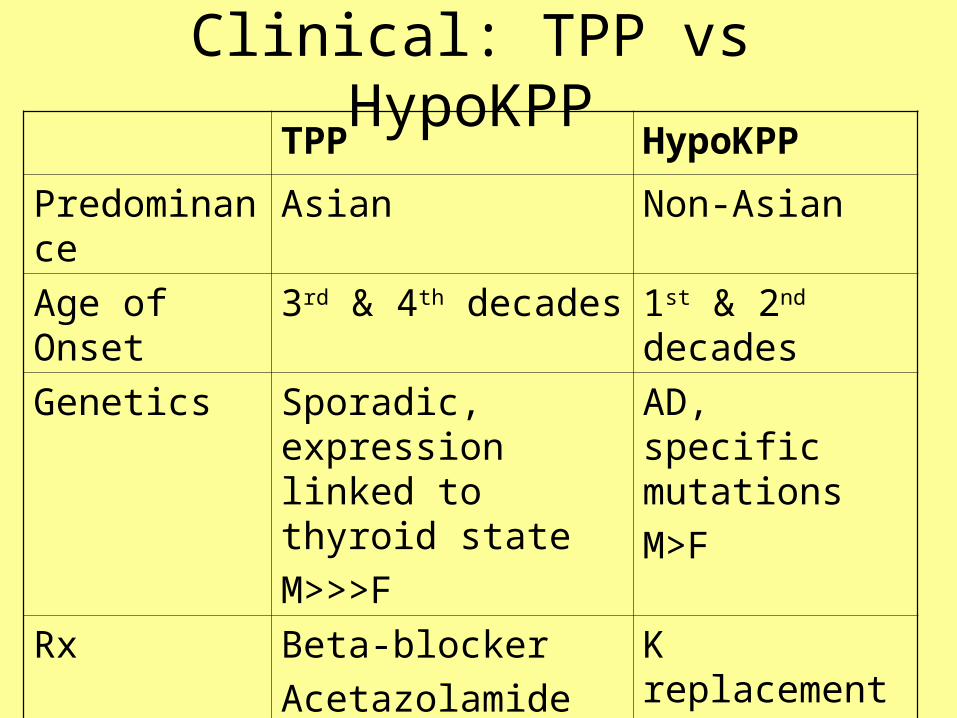
Clinical: TPP vs HypoKPPTPP HypoKPP
Predominance Asian Non-Asian
Age of Onset 3rd & 4th decades 1st & 2nd decades
Genetics Sporadic, expression linked to thyroid state
M>>>F
AD, specific mutations
M>F
Rx Beta-blocker
Acetazolamide may worsen
K replacement
Acetazolamide
Prevents

Periodic Paralysis• Results from persistent membrane depolarization
inactivation of normal Na+ channels membrane inexcitability
• HyperKPP – Na+ channelopathy – depolarization due to abnormal persistent INa
• HypoKPP – – Type I - Indirect Ca2+ Channelopathy– Type 2 - Na+ channelopathy – loss of function
• TPP – Not Associated with HypoKPP channel defects

Common Features of TPP & HypoKPP
• Episodic attacks of flaccid paralysis• Myotonia never present (vs HyperKPP)• Insulin paralytic attack without K+
• Membrane excitability impaired – low conduction velocity, low CMAP amplitude, CMAP reduction with exercise

Genetics of TPP• Familial cases increasingly recognized
• HypoKPP Na channel mutations not found
• HypoKPP Ca channel mutations not found
• Reports of selective single nucleotide polymorphisms (SNP) in regulatory region of Ca channel gene – region of thyroid hormone binding sites

Methods - Patient with TPP• 32 yo man with TPP in the T-toxic state and 4
months later when euthyroid & asymptomatic
• Measured INa with a loose patch voltage clamp, inward rectifier IK with a 3-electrode voltage clamp, action potential (AP) threshold with a 2 electrode clamp and intracellular [Ca2+] using Ca2+-sensitive electrodes
• Intercostal type IIb muscle fibers from patient with TPP, 5 patients with Type I HypoKPP (R528H mutation) and 7 controls(C).

Summary of Alterations of Inward Rectifier K+ Channel in HypoKPP
• Baseline Inward Rectifier Conductance Including KATP Channels is Reduced
• Insulin selectively reduces the K+ conductance for outward currents

KIR in TPP (nA/mm2)
0
20
40
60
80
100
120
Control HypoKPP T-toxic Euthyroid
no Insulin+ Insulin

Max INa (mA/cm2)
0
5
10
15
20
25
Control HypoKPP T-toxic Euthyroid

AP Threshold (mV)
-59-58-57-56-55-54-53-52-51-50-49
Control HypoKPP T-toxic Euthyroid

Intracellular [Ca2+] (nM) in TPP & HypoKPP
0102030405060708090
100
Control HypoKPP T-toxic Euthyroid
IIb

TPP & HypoKPP- Indirect Channelopathies -[Ca2+] may Down
Regulate Na+ and KIR Channels
• Ca2+ mutations in HypoKPP may reduce Na+ channel density and alter KIR function by elevating intracellular [Ca2+]
• In TPP - SNPs at the thyroid hormone responsive element may affect the binding affinity of the thyroid hormone responsive element and modulate the stimulation of thyroid hormone on the Ca(v)1.1 gene

Summary – HyperKPP• Paralysis produced by prolonged membrane
depolarization
• Difference between mutations that produce myotonia vs paralysis is probably that paralysis is associated with prolonged pathological INa
• Impairment of slow inactivation will facilitate prolonged pathological INa
• Mutations that impair slow inactivation associated with paralysis

Summary – HypoKPP• INa is reduced in both types of HypoKPP• Inward Rectifier K+ conductance is altered
in Type I HypoKPP and Andersen-Tawil Syndrome
• Type I HypoKPP - Frequency of paralytic attacks correlates with decrease of INa
• Type I HypoKPP – indirect Channelopathy - alteration of Na+ and K+ channel function may be mediated by intracellular [Ca2+]
Supported by the Clinical Research and Development Service, Office of Research and Development, Department of Veterans Affairs

Rx of HyperKPP
• REDUCE PARALYTIC ATTACK FREQUENCY
– 1) Eat regular meals high in carbohydrates and low in K
– 2) Avoid strenuous exercise followed by rest, emotional stress and cold

Rx of HyperKPP
• ABORT PARALYTIC ATTACKS –
– 1) Ingest high carbohydrate food such as candy bar
– 2) use beta-adrenergic agonist inhaler. For severe attacks I.V. glucose and insulin can be administered in a carefully monitored environment

Rx of HyperKPP
• IF PARAMYOTONIA AND STIFFNESS ARE PRESENT – – 1) Mexiletine 150 mg twice a day
increasing to 300 mg three times a day to reduce stiffness
– 2) Tocainide is a second line agent if mexiletine fails; however blood counts must be monitored due to the risk of bone marrow suppression. The dose of tocainide is 400-1200 mg per day

Rx of HypoKPP
• REDUCE PARALYTIC ATTACK FREQUENCY –
– 1) Follow a low carbohydrate and sodium restricted diet
– 2) Avoid precipitating factors such as strenuous exercise followed by rest, high carbohydrate meals or alcohol.

Rx of HypoKPP• MEDICATION TO REDUCE ATTACK FREQUENCY• 1) Initiate carbonic anhydrase inhibitor. Usual agent is
acetazolamide. Initial dose of 125 mg twice a day and increasing as needed to final dose of 250 mg four times a day (some will need a total daily dose of 1500mg). An alternative carbonic anhydrate inhibitor is dichlorphenamide starting at 25 mg twice a day and increasing to 25-50 mg two to three times a day. Note that some HypoPP patients worsen with carbonic anhydrase inhibitors.
• 2) If carbonic anhydrase inhibitors are not successful, a K-sparing diuretic such a triamterene or spironolactone may help.
• 3) Supplemental oral K alone or combined with a carbonic anhydrase inhibitor may prevent paralytic attacks

Rx of HypoKPP
• ABORT PARALYTIC ATTACKS –
• 1) Oral KCl 0.25 mEq/kg repeating every half hour until the weakness improves. Carefully monitor electrolytes and EKG in an intensive care setting. Avoid intravenous KCl unless KCl cannot be given orally. Avoid giving glucose and insulin as this will worsen paralysis.

Rx of Anderson-Tawil Syndrome
• MEDICATION TO REDUCE ATTACK FREQUENCY – Initiate an oral carbonic anhydrase inhibitor. The usual agent is acetazolamide, with the initial dose of 125 mg twice a day and increasing as needed to final dose of 250 mg four times a day. An alternative carbonic anhydrate inhibitor is dichlorphenamide starting at 25 mg twice a day and increasing to 25-50 mg two to three times a day. Monitor cardiac function.
Rx of Anderson-Tawil Syndrome
• TREATMENT OF ARRHYTHMIAS - Arrhythmias may respond poorly to anti-arrhythmic agents. Imipramine may be useful. Manage with a cardiologist.

Rx of ThyrotoxicPP
• PRIMARY TREATMENT IS TO CORRECT HYPERTHYROIDISM. When it is not possible to correct thyrotoxicosis, treatment with propranolol may reduce the frequency of paralytic attacks as may the treatments used to reduce the frequency of paralytic attacks in patients with HypoPP. Carbonic anhydrase inhibitors are not effective for treating TPP.

Rx of ThyrotoxicPP
• ABORT PARALYTIC ATTACKS - Administer oral KCl 0.25 mEq/kg repeating every half hour until the weakness improves. Carefully monitor electrolytes and EKG in an intensive care setting. Avoid intravenous KCl unless KCl cannot be given orally. Avoid giving glucose and insulin as this will worsen paralysis. Intravenous propranolol, given with EKG monitoring may be useful in treating acute paralytic attacks in TPP when hyperthyroidism has not yet been addressed.

Rx of HyperKPP• IF PARALYTIC ATTACKS REMAIN FREQUENT –
1) Start oral HCTZ diuretic, with initial dose of 12.5 mg/day and increasing slowly in increments of 12.5 mg to a final dose of 100-200mg/day
• 2) If HCTZ alone is not sufficient initiate an oral carbonic anhydrase inhibitor. The most common agent is acetazolamide, with the initial dose of 125 mg twice a day and increasing as needed to final dose of 250 mg four times a day (some will need a total daily dose of 1500mg). An alternative carbonic anhydrate inhibitor is dichlorphenamide starting at 25 mg twice a day and increasing to 25-50 mg two to three times a day. Note that carbonic anhydrase inhibitors may precipitate weakness in patients with HyperPP and paramyotonia.





























