Embed Size (px)
Citation preview

J . small Anim. Pruct. (1978) 19, 363-371.
Elbow lameness in the young dog caused by a sesamoidal fragment
M A R I A V A A N A N E N A N D K A I S K U T N A B B Department of Surgery, College of Veterinary Medicine, Helsinki
A B S T R A C T
Intermittent lameness in 8 dogs was attributed to a sesamoidal fragment in the elbow joint. The clinical signs, diagnosis and treatment of the condition are described.
I N T R O D U C T I O N
Several papers dealing with injuries in the elbow joint as causes of intermittent lameness in the front leg have appeared during recent years. The main cause of arthrosis in young fast-growing dogs is considered to be the osteochondrosis syndrome (OD) (Olsson, 1974), which includes:
( I ) Osteochondrosis dissecans proc.ancon. ( 2 ) Osteochondrosis dissecans proc.coronoid.med. (3) Focal O D of the medial epicondyle of the humerus. Several authors have recognized a sesamoidal fragment on the lateral aspect of
the el bow (Tirgari, 1973; Grondalen 1973; Prole, 1973; Webbon & Clayton Jones, 1976) and queried its significance. Prole and Clayton Jones consider the fragment as being part of the normal anatomical structure which does not cause intermit- tent lameness or arthrosis. Grondalen & Braut (1976) reported the finding of a fragment bilaterally on the medial side, which they considered to be the cause of arthrosis. Long & Roger (1977) reported a similar case.
C A S E H I S T O R I E S
Eight dogs were presented a t 6 months of age with slight (2-3 degree) intermittent
0020-45 I0/78/0600-0363$02.00 0 1978 BSAVA
363

3 64 M . V A A N A N E N A N D K . S K U T N A B B
foreleg lameness. The case details are summarized in Table 1. The cause of lameness was not always apparent. Medial rotation (varus) of the forelimb occurred when the sesamoidal fragment was on the lateral side of the joint. The severity of lameness increased with time. The joint became swollen and there was pain on palpation of the lateral collateral ligament over the head of the radius. It was not usually possible to elicit crepitus in the joint nor was there pain on palpation of the proc.anc0neu.s or proc.coronoideus. The presence of the sesamoi- dal fragment was confirmed by radiographic examination and treatment was by surgical excision.
RESULTS
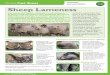
Radiographic examination Technique. The elbow is X-rayed in lateral and antero-posterior positions.
Moreover, the radius has to be rotated somewhat 50" laterally from the A-P position. The X-ray beam should pass between the head of the radius and the sesamoidal bone.
In normally used A-P position of the elbow joint the sesamoidal bone is superimposed at the lateral head of the radius. (Kv 50 MAS 10 High Speed) (Figs 1 and 2).
FIG. 1. Elbow joint, lateral radiographic anatomy.
Findings. In each case the rotated A-P view of the elbow revealed a dense fragment on the lateral side of the proximal head of the radius, (Figs 3 and 4). The surface of the fragment was smooth and the size varied between 2 x 2-5 x 5 mm in diameter. There was no radiographic evidence of arthrosis in typical places where it is seen when OD is concerned. There were no fractures on the radius and the fragment seemed to be totally independent.

TABLE
I.
Age
at
Dat
e D
ate
onse
t In
term
itten
t lam
en.
Rad
iolo
gica
lly
of
Com
plic
. Fr
ee fr
om
Cas
e of
of
sym
ptom
s 1-
4"
foun
d fr
agm
ent
oper
at:
in w
ound
- H
isto
logy
sy
mpt
oms
No.
B
reed
bi
rth
Sex
(mon
ths)
Le
ft R
ight
D
egre
e Le
ft R
ight
19
77
heal
ing
sam
ple
I wee
k 2m
onth
s
4
Rot
twei
ler
Lab
rado
r re
triev
er
Ber
nese
m
ount
ain
Ber
nese
m
ount
ain
New
- fo
undl
and
Ger
man
sh
ephe
rd
Ger
man
sh
ephe
rd
Rot
twei
ler
dog
dog
7.8
Q 75
6.
6 d
74
1-8
Q 76
7.11
Q
75
29.7
Q
28.4
d
76
76
5 17 5 5
x I
X
3
X
2
X
3
xx
3
xx
2
X
3
X 3
X
X
4.2
S.C.
oe
dem
a -
X
15.3
+
X
X
23.3
+
X
+ X
X
25
.3
-
+ x
X
X
13.4
-
X
X
noto
p.
-
-
-
X
X
2.9
S.C.
oe
dem
a in
lab
X
X
25.5
-
rn r
m 0
€ r
m
z rn m
m - Z 4
T rn .(
0
C
Z 0
U 0
Q

366 M . V A A N A N E N A N D K . S K U T N A B B
FIG. 2. The X-ray beam should pass between the head of the radius and the sesamoidal bone. This will be attained by rotating the radius from A-P position 50" laterally.
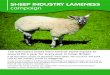
FIG. 3. The left elbow of a German Shepherd, 9 months old. The sesamoidal bone can be seen laterally a t the proximal head of the radius.

E L B O W L A M E N E S S I N T H E Y O U N G D O G 367
FIG. 4. In normally used A-P position of the elbow joint the sesamoidal bone is superim- posed at the lateral head of the radius.
S U R G I C A L P R O C E D U R E
Approach to the elbow joint A skin incision 2 cm long is made over the lateral surface of the elbow joint and
extended through the subcutaneous fascia (Fig. 5) . The skin and the fascia are undermined and retracted. The deep antebrachial
fascia is bluntly dissected and cut between the common and lateral digital extensor muscles. The muscles are separated over the joint to expose the joint capsule and lig. collaterale lat. The sesamoidal bone can be palpated cranially to the ligament (Fig. 5) .
A cut is made in front of the sesamoidal bone with a tenotomy blade and/or small scissors. The sesamoidal bone is then dissected from the collateral ligament and the joint capsule to which it is attached (Fig. 5).
The joint capsule is closed with absorbable synthetic suture material 2-0, (Dexon@). The deep antebrachial fascia and subcutaneous tissue are closed by the same means with interrupted sutures. The skin wound is sutured with Wolf-U, using nonabsorbable suture material. The joint can be flushed with dihydrostrep- tomycin 250 mg/ml before closure.

368 M. V A A N A N E N A N D K. S K U T N A B B
(C)_
Lq. col bterole loterolis
Epicondylus humeri loterolis
I
Surgical results Clinically, intermittent lameness decreased clearly one week after the operation
and lameness has resolved in five patients so far. The follow-up has been rather short but up to now the results are encouraging.
P A T H O L O G Y
The fragments were bony, 2 x 2-5 x 5 mm in diameter. The area towards the joint was covered with smooth cartilage. The opposite side was usually covered with connective tissue originating from the joint capsule and the ligament from which

E L B O W L A M E N E S S I N T H E Y O U N G DOG
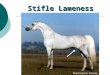
FIG. 6. Magnification of the sesamoidal bone showing the lamellar bone centre.
FIG. 7. Magnification of the bone, showing the articulating surface.
369

370 M . V A A N A N E N A N D K . S K U T N A B B
it was removed. The fragments were decalcified and stained by haematoxylin (H and E) and van Gieson methods.
Histology The fragments were covered by fibrous articular cartilage that resembled hyalin
cartilage in places. The centre of a fragment consisted of lamellar bone. A small, more or less necrotic, focus inside the centre was found in the case of the patient which developed arthrosis. There were no signs of necrosis or degeneration in any of the other fragments. Nor could callus-formation be shown on any of the fragments. All of the specimens contained small amounts of connective tissue, possibly originating from the joint capsule, (Figs 6-8).
FIG. 8. Magnification of the bone showing the nonarticulating side.
DISCUSSION
Obviously fragments of this kind must be considered, together with the osteo- chondrosis-syndrome, which Olsson ( 1977) has so widely described, as causes of intermittent lameness in the elbow joint. The occurrence of the fragment does not necessarily cause lameness but symptoms may become apparent through some external stimulus.
There has been no arthrosis and the fragments have been shown, both histolo- gically and radiographically, to be of a non-fracture origin. (Therefore they cannot be considered avulsion-fracture from an osteophyte.)

E L B O W L A M E N E S S I N T H E Y O U N G D O G 371
At the operation typical OD-foci were not encountered, nor was there any radiological evidence of OD. Histologically, the fragments did not resemble typical OD-fragments. Therefore neither O D of the proc.anconaeus nor of pro- cxoronoideus can be the cause.
It is difficult to determine the origin of the fragments, but i t cannot be excluded that they could be sesamoidal by nature. They are attached to the joint capsule and in a certain phase of the joint movement (flexion) they may be interposed between the joint surfaces and thereby cause intermittent lameness. This view is supported by the clinical observation that the patients try to move in such a way that the joint-space is as wide as possible.
A C K N O W L E D G M E N T
The authors wish to thank the Department of Anatomy at the College of Veterinary Medicine of Finland for technical and scientific assistance.
R E F E R E N C E S GRONDALEN, J. Malformationoftheelbowjoint inan Afghan hound litter. J.smallAnim. Pract. 14,2. GRONDALEN, J. & BRAUT, T. (1976) Lameness in two young dogs caused by a calcified body in the
LONG, R.D. & ROGER, A.J. (1 977) Letter to the editor, J. small Anim. Pract. IS, 157. OLSSON, S.-E. (1974) En ny typ av armbagsleds dysplasi hos hund? Svensk vet tidskrift. 26, 152. OLSSON, S.-E. (1977) Osteochondros hos hund. Svensk Vel . tidskrift 13-14, 547. PROLE, J.H.B. ( I 973) Letter to the editor. J. small anim. Pract. 14,309. TIRGARI, M. (1 974) Clinical radiographical and pathological aspects of arthritis of the elbow joint in
WEBBON, P.M. & CLAYTON JONES, D.G. (1976) Radiological refresher-6. The elbow. J . small
joint capsule of the elbow. J . small Anim. Pract. 17,681.
dogs. J . small Anim. Pract. 15,671.
Anim. Pract., 17, 395.