Embed Size (px)
Citation preview

Copies of this poster obtained through this QR code are for your personal use only and may not be reproduced
without permission from the authors.
Scan to download a reprint of this poster.
Copyright © 2020. All rights reserved.
Presented at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference; April 5, 2020; Chicago, Illinois
BACKGROUND• Abrocitinib is an oral once-daily Janus kinase 1 selective inhibitor under investigation for the treatment of
atopic dermatitis (AD)• Monotherapy with once-daily oral abrocitinib 200 mg or 100 mg was effective and well tolerated in a
dose-ranging phase 2b study (NCT02780167) in adults with moderate-to-severe AD1 – Similar results were observed in JADE MONO-1 (NCT03349060), a phase 3 trial of abrocitinib 200 mg and
100 mg versus placebo in adolescents and adults with moderate-to-severe AD2
– JADE MONO-2 (NCT03575871) was an identically designed phase 3 trial of abrocitinib 200 mg, abrocitinib 100 mg, and placebo in adolescents and adults with moderate-to-severe AD
OBJECTIVE• To characterize the efficacy and safety of once-daily oral abrocitinib 200 mg and 100 mg versus placebo in
patients aged ≥12 years with moderate-to-severe AD in the JADE MONO-2 trial
METHODSStudy Design• JADE MONO-2 (NCT03575871) was a randomized, placebo-controlled, double-blind, phase 3 study (Figure 1)
Figure 1. Study Design
! "
Eligibility Criteria• Adolescent and adult patients (≥12 years) with AD ≥1 year• Moderate-to-severe AD (IGA ≥3; EASI ≥16; %BSA ≥10; PP-NRS ≥4)• Inadequate response or intolerance to topical medication, or requirement for systemic therapy to control ADExclusion Criteria• History of conditions associated with thrombocytopenia, coagulopathy, or platelet dysfunction• Any prior use of a systemic JAK inhibitor, systemic corticosteroid use within 4 weeks, topical AD treatment use within 72 hours, dupilumab use within 6 weeks• Concomitant use of topical (corticosteroids, calcineurin inhibitors, tars, antibiotic creams, topical antihistamines) or systemic AD therapies and rescue medication use was prohibited
4-WeekFollow-Up
Abrocitinib 200 mg QDN=155
12-Week Dosing
Randomization(2:2:1) Abrocitinib 100 mg QD
N=158
Placebo QDN=78
%BSA, percentage of body surface area; AD, atopic dermatitis; EASI, Eczema Area and Severity Index; IGA, Investigator’s Global Assessment; PP-NRS, Peak Pruritus Numerical Rating Scale; QD once daily.
• Coprimary endpoints were Investigator’s Global Assessment (IGA) response (clear [0] or almost clear [1] with ≥2-grade improvement) and Eczema Area and Severity Index (EASI) ≥75% improvement (EASI-75) at week 12
• Multiplicity-controlled secondary endpoints were Peak Pruritus Numerical Rating Scale (PP-NRS; used with permission of Regeneron Pharmaceuticals, Inc., and Sanofi) response (≥4-point improvement) at week 12
• Other secondary endpoints were EASI ≥50% improvement (EASI-50) and EASI ≥90% improvement (EASI-90)• Safety was assessed via adverse event (AE) and laboratory monitoring
Statistical Analysis• The familywise type 1 error rate for testing the coprimary and key secondary endpoints was controlled at 5%
using a sequential, Bonferroni-based procedure; all other secondary endpoints were performed at the nominal 5% significance level and were not controlled for multiplicity
• Coprimary, key secondary, and other binary endpoints were analyzed using the Cochran-Mantel-Haenszel test, adjusted by randomization strata (age group [<18 years, ≥18 years] and baseline IGA)
• All continuous endpoints were analyzed using a mixed-effects model with repeated measures based on all observed data
RESULTSPatients• Overall, 155, 158, and 78 patients were treated in the abrocitinib 200-mg, abrocitinib 100-mg, and
placebo groups (Figure 2); demographics and baseline characteristics were balanced between treatment groups (Table 1)
Figure 2. Patient Disposition
26 (33.3)8 (10.3)
01 (1.3)
9 (11.5)
7 (9.0)
1 (1.3)0
Discontinued, n (%) AE Death Lost to follow-up No longer willing to participate Insufficient clinical response Protocol violation Other
14 (9.0)5 (3.2)
01 (0.6)
1 (0.6)
4 (2.6)
1 (0.6)2 (1.3)
Discontinued, n (%) AE Death Lost to follow-up No longer willing to participate Insufficient clinical response Protocol violation Other
21 (13.3)5 (3.2)1 (0.6)1 (0.6)
6 (3.8)
5 (3.2)
1 (0.6)2 (1.3)
Discontinued, n (%) AE Death Lost to follow-up No longer willing to participate Insufficient clinical response Protocol violation Other
Abrocitinib 100 mgN=158
RandomizedN=391
Assessed for EligibilityN=554
Abrocitinib 200 mgN=155
PlaceboN=78
Completed treatmentn=137 (86.7%)
Completed treatmentn=141 (91.0%)
Completed treatmentn=52 (66.7%)
AE, adverse event.
Table 1. Demographics and Baseline Disease Characteristics
Placebo N=78
Abrocitinib 100 mg N=158
Abrocitinib 200 mg N=155
TotalN=391
Age, mean (SD), y 33.4 (13.8) 37.4 (15.8) 33.5 (14.7) 35.1 (15.1)
Age group, n (%)<18 y 8 (10.3) 17 (10.8) 15 (9.7) 40 (10.2)
Male, n (%) 47 (60.3) 94 (59.5) 88 (56.8) 229 (58.6)
Race, n (%)WhiteAsian
40 (51.3)29 (37.2)
101 (63.9)46 (29.1)
91 (58.7)54 (34.8)
232 (59.3)129 (33.0)
Disease duration, mean (SD), y 21.7 (14.3) 21.1 (14.8) 20.5 (14.8) 21.0 (14.7)
Prior systemic AD treatment,a n (%) 32 (41.0) 70 (44.3) 60 (38.7) 162 (41.4)
IGA, n (%)Moderate (3)Severe (4)
52 (66.7)26 (33.3)
107 (67.7)51 (32.3)
106 (68.4)49 (31.6)
265 (67.8)126 (32.2)
EASI, mean (SD) 28.0 (10.2) 28.4 (11.2) 29.0 (12.4) 28.5 (11.5)
PP-NRS, mean (SD) 6.7 (1.9) 7.1 (1.6) 7.0 (1.6) 7.0 (1.7)
DLQI,b mean (SD) 15.0 (7.1) 15.4 (7.3) 14.8 (6.0) 15.0 (6.8)
CDLQI,c mean (SD) 10.1 (3.8) 13.8 (5.8) 12.9 (5.7) 12.7 (5.4)AD, atopic dermatitis; CDLQI, Children’s Dermatology Life Quality Index; DLQI, Dermatology Life Quality Index; EASI, Eczema Area and Severity Index; IGA, Investigator’s Global Assessment; PP-NRS, Peak Pruritus Numerical Rating Scale.aIncluded mycophenolate mofetil, methotrexate, azathioprine, corticosteroids, ciclosporin, and dupilumab. bFor patients aged ≥18 years. cFor patients aged <18 years.
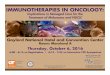
Efficacy• IGA and EASI-75 responses for both abrocitinib doses (200 mg and 100 mg) were significantly greater than
for placebo at the first postbaseline assessment (week 2) and continued to increase until week 12 (Figure 3) – Differences from placebo in IGA response were 28.7% (95% CI, 18.6-38.8; P<0.0001) for abrocitinib 200 mg
and 19.3% (95% CI, 9.6-29.0; P=0.0008) for abrocitinib 100 mg – Differences from placebo in EASI-75 response were 50.5% (95% CI, 40.0-60.9; P<0.0001) for
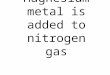
abrocitinib 200 mg and 33.9% (95% CI, 23.3-44.4; P<0.0001) for abrocitinib 100 mg• Proportions of patients achieving PP-NRS response increased from weeks 2 to 12 for both abrocitinib doses
(Figure 4); significant differences (P<0.05) in PP-NRS scores between both doses of abrocitinib and placebo were observed within 24 hours of the first dose of treatment (day 2) (data not shown)
• EASI-50 and EASI-90 responder rates were significantly (P<0.0001) greater for both abrocitinib doses than for placebo at all time points (Figure 4)
Figure 3. Coprimary Endpoints
0 2 4 8 120
20
40
60
80
100
Patie
nts
(95%
CI),
%
Week
IGA Response (FAS, NRI) EASI-75 Response (FAS, NRI)
200 mg (N=155)100 mg (N=158)Placebo (N=78)
0 2 4 8 120
20
40
60
80
100
Patie
nts
(95%
CI),
%
Week
10.4%9.1%*
** 28.4%*
*
*
** 44.5%**
**
**** 61.0%**
*
** ** 38.1%**
EASI-75, ≥75% improvement in Eczema Area and Severity Index; FAS, full analysis set; IGA, Investigator’s Global Assessment; NRI, nonresponder imputation.IGA response defined as clear (0) or almost clear (1) with ≥2-grade improvement.*P<0.05; **P<0.0001 versus placebo. Conclusion of statistical significance was controlled for multiplicity only at week 12.
Figure 4. Secondary Endpoints
Key Secondary Endpoint:PP-NRS Responder Rate
(≥4-Point Improvement; FAS, NRI + MI)
0 7 15 29 57 85 113
Time to PP-NRS Response (FAS)
0 2 4 8 120
20
40
60
80
100
Patie
nts
(95%
CI),
%
Week
EASI-50 (FAS, NRI) EASI-90 (FAS, NRI)
0 2 4 8 120
20
40
60
80
100
Patie
nts
(95%
CI),
%
Week
0 2 4 8 120
20
40
60
80
100
Patie
nts
(95%
CI),
%
Week
0
20
40
60
80
100
Prob
abili
ty, %
Days
200 mg (N=155)100 mg (N=158)Placebo (N=78)
11.5%23.1%*
33.4%****
45.2%**
3.9%*
* 23.9%*19.5%**
68.4%****
**
**
** ** 79.9%**
***
** 37.7%**
35.3%**52.8%** ** 55.3%**
29.0(16.0-31.0)**
58.0(56.0-83.0)**
112.0(112.0-NE)
EASI-50, ≥50% improvement in Eczema Area and Severity Index; EASI-90, ≥90% improvement in Eczema Area and Severity Index; FAS, full analysis set; IGA, Investigator’s Global Assessment; MI, multiple imputation; NRI, nonresponder imputation; PP-NRS, Peak Pruritus Numerical Rating Scale.*P<0.05; **P<0.0001 versus placebo. Conclusion of statistical significance was not controlled for multiplicity at week 8 for PP-NRS responder rate or for time to PP-NRS response, EASI-50, or EASI-90 at any time point.
Safety• A summary of AEs is presented in Table 2• Serious infections were infrequent (0%, 1.9%, and 1.3% in the 200-mg, 100-mg, and placebo groups,
respectively)• No malignancy or venous thromboembolism was reported• Hemoglobin, neutrophils, and lymphocytes showed no clinically significant changes• Platelet counts reached a nadir at week 4 (decreases of 26%, 19%, and <1% in the abrocitinib 200-mg,
abrocitinib 100-mg, and placebo groups, respectively) and trended toward baseline thereafter despite continued therapy
– 1 patient in the abrocitinib 200-mg group discontinued treatment because of thrombocytopenia – No clinical sequelae or hemorrhagic events were reported
• Dose-related changes in lipid levels were observed, including ~10% increases in low-density lipoprotein and high-density lipoprotein
• ~10% of patients in the 200-mg and 100-mg abrocitinib groups had >2× the upper limit of normal in creatine kinase
Table 2. Summary of Adverse Events
n (%) Placebo
N=78
Abrocitinib 100 mg N=158
Abrocitinib 200 mg N=155
≥1 TEAE 42 (53.8) 99 (62.7) 102 (65.8)
≥1 serious AE 1 (1.3) 5 (3.2) 2 (1.3)
Discontinuations because of AEs 10 (12.8) 6 (3.8) 5 (3.2)
Deaths 0 1 (0.6)a 0
TEAEs in ≥5% of patients in any groupNauseab
NasopharyngitisHeadacheUpper respiratory tract infectionDermatitis atopicAcneVomiting
2 (2.6)5 (6.4)2 (2.6)3 (3.8)
12 (15.4)0
1 (1.3)
12 (7.6)20 (12.7)
9 (5.7)14 (8.9)9 (5.7)2 (1.3)2 (1.3)
22 (14.2)12 (7.7)12 (7.7)5 (3.2)6 (3.9)9 (5.8)8 (5.2)
AE, adverse event; NE, not estimable; TEAE, treatment-emergent adverse event. aSudden cardiac death in a 73-year-old woman 3 weeks after end of therapy with abrocitinib 100 mg. b Median (95% CI) days to cessation of nausea were 7.0 (1.0-14.0), 2.5 (1.0-7.0), and 1.0 (NE-NE) in the abrocitinib 200-mg, abrocitinib 100-mg, and placebo groups, respectively. One patient in the abrocitinib 200-mg group discontinued treatment because of nausea.
CONCLUSION• Abrocitinib significantly improved signs and symptoms of moderate-to-severe AD compared with placebo in
adolescents and adults – IGA and EASI-75 responses for both abrocitinib doses were significantly greater than placebo as early as
week 2 and continued to increase until week 12 – Significant, rapid itch relief was observed with both abrocitinib doses compared with placebo starting at
day 2 of treatment• Abrocitinib was well tolerated and showed an acceptable short-term safety profile
REFERENCES 1. Gooderham MJ et al. JAMA Dermatol. Published online ahead of print October 2, 2019.
doi: 10.1001/jamadermatol.2019.2855.
2. Simpson E et al. Poster presented at: 28th EADV Congress; October 9-13, 2019; Madrid, Spain.
ACKNOWLEDGMENTSThe authors thank the patients and the JADE MONO-2 investigators for making this study possible. Medical writing support under the guidance of the authors was provided by Robert Schoen, PharmD, and Jennifer C. Jaworski, MS, at ApotheCom, San Francisco, CA, USA, and was funded by Pfizer Inc., New York, NY, USA, in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med. 2015;163:461-464).
This study was funded by Pfizer Inc.
Efficacy and Safety of Abrocitinib in Patients With Moderate-to-Severe Atopic Dermatitis: Results From the Phase 3 JADE MONO-2 Study
Jonathan I. Silverberg,1 Eric L. Simpson,2 Jacob P. Thyssen,3 Melinda J. Gooderham,4 Gary Chan,5 Claire Feeney,6 Pinaki Biswas,7 Hernan Valdez,7 Marco DiBonaventura,7 Chudy Nduaka,8 Ricardo Rojo5
1The George Washington University School of Medicine and Health Sciences, Washington, DC; 2Oregon Health & Science University, Portland, OR; 3Herlev-Gentofte Hospital, University of Copenhagen, Hellerup, Denmark; 4SKiN Centre for Dermatology, Queen’s University and Probity Medical Research, Peterborough, ON, Canada; 5Pfizer Inc., Groton, CT; 6Pfizer Ltd., Surrey, United Kingdom; 7Pfizer Inc., New York, NY; 8Pfizer Inc., Collegeville, PA