Embed Size (px)
Citation preview

Interleukin 6 (IL-6) is a pleiotropic cytokine pro-duced by many different cell types and active upon awide range of tissues. Principal functions include the reg-ulation of the acute phase response and the stimulationof B-cell differentiation.1,2 Both growth-inhibitory andstimulatory effects of IL-6 have been reported on arange of cell types1,2 and antitumour effects have beendescribed in some murine tumour models.3–5
IL-6 exerts marked effects on haemopoiesis,including the stimulation of early myeloid progenitors
synergistically with interleukin 3 (IL-3) and stem cellfactor.6–9 In vitro IL-6 alone has little effect onmegakaryocyte progenitor cells but exerts a direct stim-ulatory effect on differentiation and maturation ofmegakaryocytes10–13 although one study reports a directstimulation of megakaryocyte colony formation by IL-6.14 IL-6 has been shown to stimulate thrombo-poiesis in vivo in murine, primate and canine modelsand to enhance recovery following chemotherapy orradiation-induced bone marrow suppression.15–23 Thelevel of action of IL-6 is not clear as some studies reportboth increased megakaryocyte number and increasedploidy. Similar thrombopoietic effects have now beenreported following administration of IL-6 to cancerpatients24–28 and additionally small but significantincreases in GM-CFC, megakaryocyte-CFC and E-BFU were found.28 An effect of IL-6 on progenitorcells would not be surprising in view of the presence of its receptor on some CD341 bone marrow blastcells.29
The present study examines the effects of IL-6 onplatelet levels and peripheral blood progenitor cells[granulocyte-macrophage colony-forming units (GM-CFU), erythroid burst-forming units (E-BFU) and themore primitive plastic-adherent (P∆) progenitor cells],
CYTOKINE, Vol. 8, No. 9 (September), 1996: pp 717–723 717
EFFECTS OF INTERLEUKIN 6 ADMINISTRATIONON PLATELETS AND HAEMOPOIETIC
PROGENITOR CELLS IN PERIPHERAL BLOODDeborah Clarke,1 Peter W.M. Johnson,1 Rosamonde E. Banks,1 Mark Storr,1
Sally E. Kinsey,2 Roderick Johnson,3 Gareth Morgan,3 Myrtle Y. Gordon,4John M. Illingworth,5 Timothy J. Perren,1 Peter J. Selby1
Platelet numbers and circulating haemopoietic progenitor cells were examined in 12 patientswith advanced malignancies who were receiving recombinant human interleukin-6 (rhIL-6)as part of an investigation of its thrombopoietic effects. Patients received recombinant glycosylated IL-6 by daily subcutaneous injection for 7 consecutive days in doses of 1, 3 or 10µg/kg/day. Platelet numbers increased reaching a peak on days 12–15 with a mean on day 15of 198.1% of pre-treatment values. This was accompanied by a significant fall in the meanplatelet volume (mean decrease of 10.6%, P 5 0.0044). No significant correlation was seenbetween the IL-6 dose and the change in platelet number. No significant differences wereobserved between pre- and post-treatment levels of circulating erythroid burst-forming units(E-BFU) and granulocyte macrophage colony-forming units (GM-CFU) but a smallsignificant increase was seen in circulating primitive progenitor cells measured in a plastic-adherent (P∆) assay (P 5 0.025). As positive controls, a group of patients treated withcyclophosphamide/G-CSF showed significant increases in GM-CFU (P 5 0.018), E-BFU(P 5 0.018) and P∆ progenitors (P 5 0.028).
These data suggest that the thrombopoietic effects of IL-6 are mediated at a relativelylate stage via effects on megakaryocyte differentiation, with a relatively small effect on cir-culating haemopoietic progenitors.
© 1996 Academic Press Limited
From the 1Imperial Cancer Research Fund Cancer MedicineResearch Fund, 2Department of Paediatric Haematology, StJames’s University Hospital, Beckett Street, Leeds LS9 7TF, UK,3Department of Haematology, Leeds General Infirmary, GreatGeorge Street, Leeds LS1 3EX, UK, 4Leukaemia Research FundCentre for Adult Leukaemia, Royal Postgraduate MedicalSchool, Hammersmith Hospital, Du Cane Road, London W120NN, UK, and 5Ares Serono, Geneva, Switzerland
Correspondence to: Peter W.M. Johnson, Imperial Cancer MedicineResearch Fund, St James’s University Hospital, Beckett Street,Leeds LS9 7TF, UK
Received 27 November 1995; accepted for publication 24 March 1996© 1996 Academic Press Limited1043-4666/96/09071717 $25.00/0
KEY WORDS: interleukin-6/stem cell mobilization/platelets/CFU-GM/BFU-E

in a group of patients with solid tumours, receiving IL-6 as part of an investigation of its effects upon therapy-related thrombocytopenia. For comparison, alsoreported are peripheral blood progenitor cell numbersin a group of patients undergoing peripheral bloodprogenitor cell harvesting following cyclophos-phamide/granulocyte colony-stimulating factor (G-CSF) mobilization, and in a group of normal healthyvolunteers.
RESULTS
Platelets
Pre-treatment platelet counts were within the nor-mal range in 11 of the 12 patients and increasedsignificantly (P 5 0.0033) in all the patients followingtreatment with IL-6 (Fig. 1A). Half of the patients alsoshowed a slight transient decrease in platelet number24–48 h following the start of IL-6 treatment. Peak values were achieved on days 12–15 with a mean level (6 SEM) on day 15 of 198.1% 6 10.2% (range 5142.9%–249.8% median 5 189.4%, n 5 11) of the pre-treatment values. One patient was excluded from thisstatistical analysis due to an intercurrent blood trans-fusion and a marked thrombocytosis at the start of thetreatment period. There was no significant correlationbetween the IL-6 dose level and the change in plateletnumber (data not shown). The rise in platelet count wasconsistently accompanied by a significant fall in themean platelet volume (P 5 0.0044), by a mean of 10.6% + 2.1% on day 15 (Fig. 1B). A typical profile isshown in Figure 2.
In five patients, platelet aggregation tests were alsocarried out and with one exception were found to benormal with no change occurring following IL-6 ther-apy (results not shown). The one exception was thepatient who had a marked thrombocytosis prior to thestart of treatment and who exhibited pronounced spon-taneous platelet aggregation at this time.
Colony-forming assays
Normal subjects and patients before IL-6/G-CSFIThe results of the E-BFU, GM-CFU and plastic-adher-ent (P∆) progenitor assays for the nine patients prior toIL-6 therapy were not significantly different to those of12 normal subjects (Table 1). Similarly there was no dif-ference between these results and those obtained fromseven patients with haematologic malignancies beforereceiving cyclophosphamide and G-CSF. Howeversignificant intraindividual variation was apparent in the P∆ progenitor assays when examined in two or three longitudinal samples from 10 individuals, withcoefficients of variation (CVs) of between 0.2% and116% (mean 31.3%, median 28%).
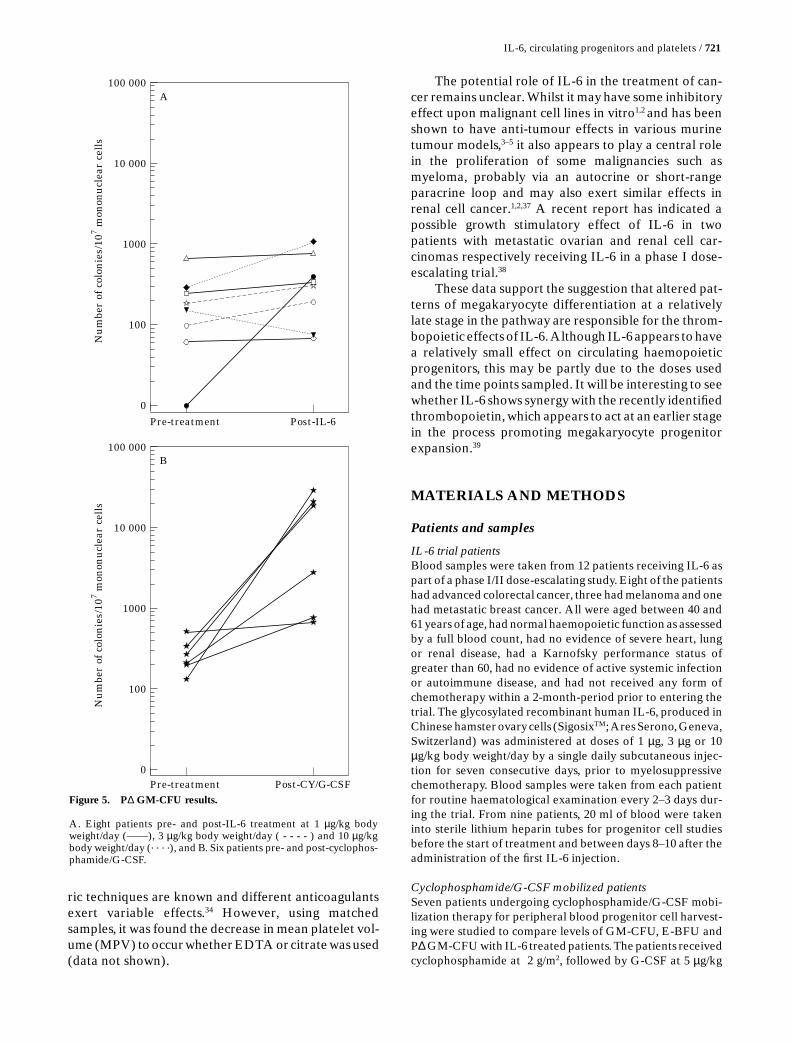
Patients treated with interleukin 6No significant difference was observed between pre-and post-treatment levels for E-BFU and GM-CFU. Asmall but significant increase was evident for P∆ pro-genitors (P 5 0.025). There was no apparent relation-ship between the dose of IL-6 and the changes seen(Table 1, Figures 3A, 4A and 5A).
718 / Clarke et al. CYTOKINE, Vol. 8, No. 9 (September 1996: 717–723)
11
6
Mea
n p
late
let
volu
me
(fl)
10
9
8
7
Pre-treatment Day 15
B
1000
100
Pla
tele
t co
un
t (×
109 /l)
500
900
800
700
600
400
300
200
Pre-treatment Day 15
A
Figure 1. Platelet numbers (A) and mean volumes (B) in 12 patientspre- and post-IL-6 treatment.
IL-6 was administered from days 1–7 inclusive.

Patients treated with cyclophosphamide/G-CSFThe levels of E-BFU, GM-CFU, and P∆ progenitorswere significantly increased (P 5 0.018, P 5 0.018, P 50.028 respectively) above pre-treatment values follow-ing treatment with cyclophosphamide and G-CSF(Table 1, Figures 3B, 4B and 5B).
DISCUSSION
Several phase I studies have now confirmed thethrombopoietic effects of non-glycosylated IL-6 in vivoalthough the exact mechanism underlying this effectremains far from clear. This is the fïrst report showingthat recombinant glycosylated IL-6 produces similareffects in vivo in humans and the first study examiningthe effects of IL-6 on peripheral blood progenitor cellsdetected using the plastic adherent progenitor cell assay(P∆ assay). The identification of an early plastic-adher-ent progenitor is based on the finding that removal ofplastic-adherent cells from murine bone marrow com-promises its ability to repopulate the haemopoietic sys-tem when it is transplanted into irradiated recipients.30
A small but significant increase in early haemopoieticprogenitors has been shown as measured by this assay,
which may point to an effect of IL-6 on early pluripo-tent cells. However, the changes seen with IL-6 are ofa small magnitude and there is considerable and vari-able intraindividual variation. The use of samples frompatients undergoing mobilization of peripheral bloodprogenitor cells as positive controls confirms the rele-vance of the colony assays, with the expected rises inthe numbers of progenitors, being in keeping with theresults reported in other studies.31
Previous studies examining whether the throm-bopoietic effects of IL-6 are mediated via stimulationof early progenitor cells or by differentiation ofmegakaryocytes are contradictory. In vitro, IL-6 hasbeen shown to increase megakaryocyte size and ploidywithout affecting colony numbers10–13 whilst in animalstudies examining megakaryocyte numbers or colonyforming assays, results have been inconsistent.15,17,18,21–23
A recent study in patients with cancer has reportedsignificant increases in peripheral blood GM-CFC, E-BFU and Meg-CFC, but did not demonstrate asignificant change in primitive progenitor cells.28
Megakaryocyte colony numbers in the bone marrowwere shown to increase slightly but significantly fol-lowing IL-6 treatment. However, another study failedto demonstrate changes in levels of circulating GM-CFU, E-BFU or CFU-GEMM progenitors in keepingwith our results.26
In support of IL-6 acting at the level of differenti-ation of the megakaryocyte, receptors for IL-6 havebeen found on megakaryocytes together with the pres-ence of IL-6 itself suggesting the possibility of autocrineloops.32 The majority of studies in vivo have foundincreases in megakaryocyte ploidy and/or size follow-ing treatment with IL-6.15,16,18,20–24,26 Megakaryocyteploidy has been found to be inversely related to plateletsize33 as has platelet number34 and the finding of asignificant decrease in platelet volumes is similar to thatfound in an earlier study,25 although not found in ani-mal studies.16,19,23,35 A finding of increased megakary-ocyte ploidy suggests an effect of IL-6 at the level of thedifferentiation of the megakaryocyte rather than anearlier stem cell and may be analogous to paraneo-plastic thrombocytosis in which IL-6 has been impli-
IL-6, circulating progenitors and platelets / 719
75
250
3050
0Day
Pla
tele
ts (
% o
f pr
e-tr
t)
10
175
225
200
150
125
100
2 4 6 8 14 18 22 2612 16 20 24 28
Number
Volume
IL-6 @ 1 µg/kg
Figure 2. A representative profile showing changes in platelet num-ber and mean platelet volume during and following IL-6 treatmentin a patient receiving 1 µg IL-6/kg body weight/day.
TABLE 1. Results of haemopoietic progenitor cell assays from normal and patient groups, shown as median (range)
Group GM-CFU E-BFU P∆ GM-CFU
Normals (n 5 12) 8.2 (1.7–33.3) 27.7 (15.3–114.3) 100.3 (78.5–1537.5) (n 5 10)Pre-treatment IL-6 patients (n 5 9) 15.5 (0–68.0) 49.3 (4.7–90.3) (n 5 8) 182.5 (0–658.0) (n 5 8)Post-treatment IL-6 patients (n 5 9) 17.7 (0–97.1) 49.1 (0–217.4) (n 5 8) *313.8 (67.5–1043.0) (n 5 8)Pre-treatment cyclophosphamide/
G-CSF patients (n 5 7) 3.7 (0–11.0) 32.8 (3.8–164.7) 240.0 (131.5–497.5) (n 5 6)Post-treatment cyclophosphamide/
G-CSF patients (n 5 7) *106.0 (3.8–481.0) *182.0 (22.0–284.0) *10 862.5 (665.0–28 250.0) (n 5 6)
GM-CFU and E-BFU are presented as colonies per 106 mononuclear cells. P∆ GM-CFU is expressed as GM-CFU progeny from the adherent fraction of 107 mono-nuclear cells. Numbers of patients per group are shown in the left-hand column except where otherwise indicated. Level of significance between appropriate pre-and post-treatment groups are shown as * where P , 0.05.

cated.36 This contrasts with acute thrombocytopeniawhere larger platelets are released by rapid megakary-ocyte fragmentation.
The discordant results between studies with regardto ploidy and platelet size may partly reflect differences
in dosing schedules although in many cases the incre-ments in circulating platelet numbers were similar, oralternatively may be due to species differences and the methods used for measuring platelet volumes.Differences between electronic counters and cytomet-
720 / Clarke et al. CYTOKINE, Vol. 8, No. 9 (September 1996: 717–723)
Nu
mbe
r of
col
onie
s/10
6 mon
onu
clea
r ce
lls
Mea
n n
um
ber
of c
olon
ies/
106 m
onon
ucl
ear
cell
s
1000
1
100
10
Pre-treatment Post-CY/G-CSF
B
Pre-treatment Post-IL-6
A1000
1
100
10
Nu
mbe
r of
col
onie
s/10
6 mon
onu
clea
r ce
lls
1000
1
Nu
mbe
r of
col
onie
s/10
6 mon
onu
clea
r ce
lls
100
10
Pre-treatment Post-CY/G-CSF
B
Pre-treatment Post-IL-6
A1000
1
100
10
Figure 3. E-BFU results.
A. Eight patients pre- and post-IL-6 treatment at 1 µg/kg bodyweight/day (—), 3 µg/kg body weight/day ( - - - - ) ~and 10 µg/kg bodyweight/day (. . . .), and B. Seven patients pre- and post-cyclophos-phamide/G-CSF treatment.
Figure 4. GM-CFU results.
A. Nine patients pre- and post-IL-6 treatment at 1 µg/kg bodyweight/day (——), 3 µg/kg body weight/day ( - - - - ) and 10 µg/kgbody weight/day (. . . .), and B. Seven patients pre- and post-cyclophosphamide/G-CSF treatment.
ric techniques are known and different anticoagulantsexert variable effects.34 However, using matched samples, it was found the decrease in mean platelet vol-ume (MPV) to occur whether EDTA or citrate was used(data not shown).
The potential role of IL-6 in the treatment of can-cer remains unclear. Whilst it may have some inhibitoryeffect upon malignant cell lines in vitro1,2 and has beenshown to have anti-tumour effects in various murinetumour models,3–5 it also appears to play a central rolein the proliferation of some malignancies such asmyeloma, probably via an autocrine or short-rangeparacrine loop and may also exert similar effects inrenal cell cancer.1,2,37 A recent report has indicated apossible growth stimulatory effect of IL-6 in twopatients with metastatic ovarian and renal cell car-cinomas respectively receiving IL-6 in a phase I dose-escalating trial.38
These data support the suggestion that altered pat-terns of megakaryocyte differentiation at a relativelylate stage in the pathway are responsible for the throm-bopoietic effects of IL-6. Although IL-6 appears to havea relatively small effect on circulating haemopoieticprogenitors, this may be partly due to the doses usedand the time points sampled. It will be interesting to seewhether IL-6 shows synergy with the recently identifiedthrombopoietin, which appears to act at an earlier stagein the process promoting megakaryocyte progenitorexpansion.39
MATERIALS AND METHODS
Patients and samples
IL-6 trial patientsBlood samples were taken from 12 patients receiving IL-6 aspart of a phase I/II dose-escalating study. Eight of the patientshad advanced colorectal cancer, three had melanoma and onehad metastatic breast cancer. All were aged between 40 and61 years of age, had normal haemopoietic function as assessedby a full blood count, had no evidence of severe heart, lungor renal disease, had a Karnofsky performance status ofgreater than 60, had no evidence of active systemic infectionor autoimmune disease, and had not received any form ofchemotherapy within a 2-month-period prior to entering thetrial. The glycosylated recombinant human IL-6, produced inChinese hamster ovary cells (SigosixTM; Ares Serono, Geneva,Switzerland) was administered at doses of 1 µg, 3 µg or 10µg/kg body weight/day by a single daily subcutaneous injec-tion for seven consecutive days, prior to myelosuppressivechemotherapy. Blood samples were taken from each patientfor routine haematological examination every 2–3 days dur-ing the trial. From nine patients, 20 ml of blood were takeninto sterile lithium heparin tubes for progenitor cell studiesbefore the start of treatment and between days 8–10 after theadministration of the first IL-6 injection.
Cyclophosphamide/G-CSF mobilized patientsSeven patients undergoing cyclophosphamide/G-CSF mobi-lization therapy for peripheral blood progenitor cell harvest-ing were studied to compare levels of GM-CFU, E-BFU andP∆ GM-CFU with IL-6 treated patients. The patients receivedcyclophosphamide at 2 g/m2, followed by G-CSF at 5 µg/kg
IL-6, circulating progenitors and platelets / 721
100 000
100 000
0
Nu
mbe
r of
col
onie
s/10
7 mon
onu
clea
r ce
lls
10 000
1000
100
Pre-treatment Post-CY/G-CSF
B
Pre-treatment Post-IL-6
A
0
Nu
mbe
r of
col
onie
s/10
7 mon
onu
clea
r ce
lls
10 000
1000
100
Figure 5. P∆ GM-CFU results.
A. Eight patients pre- and post-IL-6 treatment at 1 µg/kg bodyweight/day (——), 3 µg/kg body weight/day ( - - - - ) and 10 µg/kgbody weight/day (. . . .), and B. Six patients pre- and post-cyclophos-phamide/G-CSF.

by daily subcutaneous injection up to and including the day(s)of harvesting. Peripheral blood (20 mls) was taken into ster-ile lithium heparin tubes before the commencement of treat-ment and on the first day of leukapheresis after 8–10 daysfollowing G-CSF administration.
Normal volunteersFive male and seven female adult donors (age 23–53) wererecruited in order to determine a normal range of circulatingGM-CFU, E-BFU and plastic-adherent (P∆) progenitors.Samples were obtained at two to three time points in orderto determine intra-individual variability.
Clonogenic assays
Preparation of cellsPeripheral blood was obtained from consenting subjects andthe mononuclear cell fraction from each source was separatedusing Lymphoprep (Nyegaard, Oslo, Norway) and washed inα-medium (GIBCO BRL, Paisley, Scotland). Mononuclearcells (107) from each subject were plastic adhered at a con-centration of 106/ml in α-medium containing 15% V/V foetalcalf serum (FCS) (Sera Lab Ltd., Sussex, UK) in a 25 cm2 tis-sue culture flask (Nunc, Denmark) at 37°C in an atmosphereof 95% humidified air/5% CO2. After 2 h the non-adherentcells were transferred to a separate flask to incubate overnightbefore plating into GM-CFU and E-BFU assays as describedbelow.40 The plastic adherent cells were then used for the P∆assay, in order to detect progenitor cells indirectly by mea-suring the clonogenic progeny they produce in vitro.41–43
Delta assay of plastic-adherent (P∆) progenitor cellsThe plastic-adherent cells were washed free of any remainingnon-adherent and loosely-adherent cells by washing threetimes in α-medium. After the final rinse, the adherent cellswere immersed in α-medium containing 10% V/V FCS, 10%V/V horse serum (Sera Lab Ltd.), 10% V/V 5637 cell-condi-tioned medium,44 2 mM L-glutamine and 2 µM methylpred-nisolone (Upjohn Ltd., Crawley, UK). These plastic adherentcells were then incubated for seven days at 37°C in an atmos-phere of 95% air/5% CO2. The non-adherent progenyreleased into the supernatant was pipetted from the flask andthe cells harvested by centrifugation at 450 g for 5 min andresuspended in α-medium. The progeny were then assayed inthe GM-CFU assay. The numbers of GM-CFU derived fromthe adherent fraction of 107 mononuclear cells were deter-mined from the numbers of colonies scored.
GM-CFU assayThe non-adherent fraction from 5 3 106 mononuclear cellswere diluted in α-medium containing 20% V/V FCS and 10%V/V 5637 cell-conditioned medium and warmed to 37°C.Finally molten agar (Agar Noble, Difco Laboratories, Detroit,MI) was added to an overall concentration of 0.3% W/V in atotal volume of 5 ml. After mixing the cell mixture by pipet-ting, 4 3 1 ml aliquots were dispensed into 35 mm Petri dishesand incubated at 37°C in an atmosphere of 95% air/5% CO2.Colonies were scored on day 14 using an inverted microscopewhere an individual colony was defined as being 50 cells ormore.
E-BFU assayThe non-plastic adherent cells from 5 3 106 mononuclear cellswere cultured in a total volume of 5 ml containing 30% V/VFCS, 1% W/V bovine serum albumin (BSA) (fraction V pro-vided as a 35% W/V solution, Sigma Chemical Company Ltd.,Poole, UK), 1.5 U/ml erythropoietin (Stem Cell TechnologiesInc., Metachem Diagnostics Ltd., Northampton, UK), 100 µM2-mercaptoethanol (Sigma) and 2% W/V methylcellulose(made up in Iscove's modified Dulbecco’s medium, GIBCOBRL) as support matrix. After vortexing, 3 3 1 ml aliquotswere dispensed into 35 mm Falcon 3001 Petri dishes using a1 ml syringe and a blunt needle. The Petri dishes were thenincubated tor 14 days and both unicentric and multiple burstswere scored.
Statistical analysis
The data was tound to be non-normally distributed andaccordingly the non-parametric Mann–Whitney U andWilcoxon matched pairs tests and Spearman rank correlationswere used throughout.
Acknowledgements
This work was supported by the Imperial CancerResearch Fund and the Yorkshire Cancer ResearchCampaign. We also thank Ares Serono for the provi-sion of the recombinant interleukin 6.
REFERENCES
1. Akira S, Taga T, Kishimoto, T (1993) Interleukin-6 in biol-ogy and medicine. Adv Immunol 54:1–77.
2. Borden EC, Chin P (1994) Interleukin-6: a cytokine withpotential diagnostic and therapeutic roles. J Lab Clin Med123:824–829.
3. Mule JJ, Custer MC, Travis WD, Rosenberg SA (1992)Cellular mechanisms of the antitumor activity of recombmant IL-6in mice. J Immunol 148:2622–2629.
4. Katz A, Shulman LM, Porgador A, Revel M, Feldman M,Eisenbach L (1993) Abrogation of B16 melanoma metastases by long-term low-dose interleukin-6 therapy. J Immunother 13:98–109.
5. Yoshizawa K, Okamoto T, Moriya K, Izawa A, Satoh Y,Naruto M, Ida N (1994) Effects of natural human interleukin-6 onthrombopoiesis and tumour progression in tumour-bearing mice.Cancer Lett 79:83–89.
6. Ikebuchi K, Wong GG, Clark SC, Ihle JN, Hirai Y, OgawaM (1987) Interleukin 6 enhancement of interleukin-3-dependent pro-liferation of multipotential hemopoietic progenitors. Proc Natl AcadSci USA 84:9035–9039.
7. Leary AG, Ikebuchi K, Hirai Y, Wong G, Yang Y, Clark SC,Ogawa M (1988) Synergism between interleukin-6 and inerleukin-3in supporting proliferation of human hematopoietic stem cells: com-parison with interleukin-1a. Blood 71:1759–1763.
8. Bertoncello I, Bradley TR, Hodgson GS, Dunlop, JM (1991)The resolution, enrichment and organization of normal bone marrowhigh proliferative potential colony-forming cells subsets on the basisof rhodamine-123 fluorescence. Exp Hematol 19:174–178.
9. Williams N, Bertoncello I, Kavnoudias H, Zsebo K,McNiece I (1992) Recombinant rat stem cell factor stimulates theamplification and differentiation of fractionated mouse stem cell populations. Blood 79:58–64.
722 / Clarke et al. CYTOKINE, Vol. 8, No. 9 (September 1996: 717–723)

10. Ishibashi T, Kimura H, Uchida T, Kariyone S, Friese P,Burstein SA (1989) Human interleukin 6 is a direct promoter of mat-uration of megakaryocytes in vitro. Proc Natl Acad Sci USA86:5953–5957.
11. Imai T, Koike K, Kubo T, Kikuchi T, Amano Y, Takagi M,Okumura N, Nakahata T (1991) Interleukin-6 supports humanmegakaryocytic proliferation and differentiation in vitro. Blood78:1969–1974.
12. Williams N, De Giorgio T, Banu N, Withy R, Hirano T,Kishimoto T (1990) Recombinant interleukin 6 stimulates immaturemurine megakaryocytes. Exp Hematol 18:69–72.
13 Kimura H, Ishibashi T, Uchida T, Maruyama Y, Friese P,Burstein SA (1990) Interleukin 6 is a differentiation factor for humanmegakaryocytes in vitro. Eur J Immunol 20:1927–1931.
14. Quesenberry PJ, McGrath HE, Williams ME, Robinson BE,Deacon DH, Clark S, Urdal D, McNiece IK (1991) Multifactor stimulation of megakaryocytopoiesis: effects of interleukin 6. ExpHematol 19:35–41.
15. Asano S, Okano A, Ozawa K, Nakahata T, Ishibashi T,Koike K, Kimura K, Tanioka Y, Shibuya A, Hirano T, Kishimoto T,Takaku F, Akiyama Y (1990) In vivo effects of recombinant humaninterleukin-6 in primates: stimulated production of platelets. Blood75:1602–1605.
16. Stahl CP, Zucker-Franklin D, Evatt BL, Winton EF (1991)Effects of human interleukin-6 on megakaryocyte development andthrombocytopoiesis in primates. Blood 78:1467–1475.
17. Patchen ML, MacVittie TJ, Williams JL, Schwartz GN,Souza LM (1991) Administration of interleukin-6 stimulates multi-lineage hematopoiesis and accelerates recovery from radiation-induced hematopoietic depression. Blood 77:472–480.
18. Ryffel B, Car BD, Woerly G, Weber M, DiPadova F,Kammüller M, Klug S, Neubert R, Neubert D (1994) Long-term inter-leukin-6 administration stimulates sustained thrombopoiesis andacute-phase protein synthesis in a small primate—the marmoset.Blood 83:2093–2102.
19. Burstein SA, Downs T, Friese P, Lynam S, Anderson S,Henthron J, Epstein RB, Savage K (1992) Thrombocytopoiesis in nor-mal and sublethally irradiated dogs: response to human interleukin-6. Blood 80:420–428.
20. Zeidler C, Kanz L, Hurkuck F, Rittmann KL, Wildfang I,Kadoya T, Mikayama T, Souza L, Welte K (1992) In vivo effects ofinterleukin-6 on thrombopoiesis in healthy and irradiated primatesBlood 80:2740–2745.
21. Ishibashi T, Kimura H, Shikama Y, Uchida T, Kariyone S,Hirano T, Kishimoto T, Takatsuki F, Akiyama Y (1989) Interleukin-6 is a potent thrombopoietic factor in vivo in mice. Blood74:1241–1244.
22. Carrington PA, Hill RJ, Stenberg PE, Levin J, Corash L,Schreurs J, Baker G, Levin FC (1991) Multiple in vivo effects of inter-leukin-3 and interleukin-6 on murine megakaryocytosis. Blood77:34–41.
23. Hill RJ, Warren MK, Stenberg P, Levin J, Corash L,Drummond R, Baker G, Levin F, Mok Y (1991) Stimulation ofmegakaryocytopoiesis in mice by human recombinant interleukin-6.Blood 77:42–48.
24. Weber J, Gunn H, Yang J, Parkinson D, Topalian S,Schwartzentruber D, Ettinghausen S, Levitt D, Rosenberg SA (1994)A phase I trial of intravenous interleukin-6 in patients with advancedcancer. J Immunother 15:292–302.
25. Van Gameren MM, Willemse PHB, Mulder NH, LimburgPC, Groen HJM, Vellenga E, De Vries EGE (1994) Effects of recom-binant human interleukin-6 in cancer patients: a phase I-II study.Blood 84:1434–1441.
26. D’Hondt V, Humblet Y, Guillaume, T, Baatout S, ChatelainC, Berlière M, Longueville J, Feyens AM, De Greve J, Van OosteromA, Von Graffenried B, Donnez J, Symann M (1995) Thrombopoietic
effects and toxicity of interleukin-6 in patients with ovarian cancerbefore and after chemotherapy: A multicentric placebo-controlled,randomized phase Ib study. Blood 85:2347–2353
27. Weber J, Yang JC, Topalian SL, Parkinson DR,Schwartzentruber DS, Ettinghausen SE, Gunn H, Mixon A, Kim H,Cole D, Levin R, Rosenberg SA (1993) Phase I trial of subcutaneousinterleukin-6 in patients with advanced malignancies. J Clin Oncol11:499–506.
28. Pettengell R, Luft T, De Wynter E, Coutinho L, Young R,Fitzsimmons L, Scarffe JH, Testa NG (1995) Effects of interleukin-6on mobilization of primitive haemopoietic cells into the circulation.Br J Haematol 89:237–242.
29. Wognum AW, Van Gils FCJM, Wagemaker G (1993) Flowcytometric detection of receptors for interleukin-6 on bone marrowand peripheral blood cells of humans and rhesus monkeys. Blood81:2036–2043.
30. Bearpark AD, Gordon MY (1989) Adhesive properties dis-tinguish sub-populations of hemopoietic stem cells with differentspleen colony-forming and marrow-repopulating capacities. BoneMarrow Transplant 4:625–628.
31. Jones HM, Jones SA, Watts MJ, Khwaja A, Mills W, FieldingA, Goldstone AH, Linch DC (1994) Development of a simplified single-apheresis approach for peripheral-blood progenitor-cell trans-plantation in previously treated patients with lymphoma. J Clin Oncol12:1693–1702.
32. Navarro S, Debili N, Le Couedic J-P, Klein B, Breton-GoriusJ, Doly J, Vainchenker W (1991) Interleukin-6 and its receptor areexpressed by human megakaryocytes: in vitro effects on proliferationand endoreplication. Blood 77:461–471.
33. Penington DG, Streatfield K, Roxburgh AE. (1976)Megakaryocytes and the heterogeneity of circulating platelets. Br JHaematol 34:639–653.
34. Threatte GA (1993) Usefulness of the mean platelet vol-ume. Clinic Lab Med 13:937–951.
35. McDonald TP, Cottrell MB, Swearingen CJ, Clift RE (1991)Comparative effects of thrombopoietin and interleukin-6 on murinemegakaryocytosis and platelet production. Blood 77:735–740.
36. Blay J-Y, Favrot M, Rossi JF, Wijdenes J (1993) Role ofinterleukin-6 in paraneoplastic thrombocytosis. Blood 81:2261–2262.
37. Koo AS, Armstrong C, Bochner B, Shimabukuro T, Tso C-L, de Kernion JB, Belldegrun A (1992) Interleukin-6 and renal cellcancer: production, regulation and growth effects. Cancer ImmunolImmunother 35:97–105.
38. Ravoet C, De Grève J, Vandewoude K, Kerger J, Sculier J-P, Lacor P, Stryckmans P, Piccart M (1994) Tumour stimulatingeffects of recombinant human interleukin-6. Lancet 344:1576–1577.
39. Kaushansky K, Lok S, Holly RD, Broudy VC, Lin N, BaileyMC, Forstrom JW, Buddle MM, Oort, PJ, Hagen FS, Roth GJ,Papayannopoulou T, Foster DC (1994) Promotion of megakaryocyteprogenitor expansion and differentiation by the c-Mpl ligand thrombopoietin. Nature 369:568–571.
40. Gordon MY (1993) Human haemopoietic stem cell assays.Blood Rev 7:190–197.
41. Gordon MY, Riley GP, Greaves MF (1987) Plastic-adher-ent progenitor cells in human bone marrow. Exp Hematol 15:772–778.
42. Gordon MY, Clarke D, Healy LE (1989) An in vitro modelfor the production of committed haemopoietic progenitor cells stim-ulated by exposure to single and combined recombinant growth fac-tors. Bone Marrow Transplant 4:353–358.
43. Gordon MY (1994) Plastic-adherent cells in human bonemarrow generate long-term hematopoiesis in vitro. Leukemia8:865–870.
44. Myers CD, Katz FE, Joshi G, Millar JL (1984) A cell linesecreting stimulating factors for CFU-GEMM culture. Blood64:152–155.
IL-6, circulating progenitors and platelets / 723





























