Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Behaviour Research and Therapy 51 (2013) 411e416
Contents lists available
Behaviour Research and Therapy
journal homepage: www.elsevier .com/locate/brat
Effectiveness, response, and dropout of dialectical behavior therapyfor borderline personality disorder in an inpatient setting
Christoph Kröger a,*, Susanne Harbeck b, Michael Armbrust b, Sören Kliem a
a Technical University Brunswick, Department of Psychology, Humboldtstraße 33, 38106 Brunswick, Germanyb Schön Klinik Bad Bramstedt, Birkenweg 10, 24576 Bad Bramstedt, Germany
a r t i c l e i n f o
Article history:Received 11 December 2012Received in revised form23 April 2013Accepted 26 April 2013
Keywords:Borderline personality disorderDialectical behavior therapyEffectivenessDropoutClinical significance
* Corresponding author. Tel.: þ49 (0)531 391 2866;E-mail address: [email protected] (C. Kröger).
0005-7967/$ e see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.brat.2013.04.008
a b s t r a c t
To examine the effectiveness of dialectical behavior therapy for inpatients with borderline personalitydisorder (BPD), small sample sizes and, predominantly, tests of statistical significance have been used sofar. We studied 1423 consecutively admitted individuals with BPD, who were seeking a 3-month inpa-tient treatment. They completed the Borderline Symptom List (BSL) as the main outcome measure, andother self-rating measures at pre- and post-treatment. Therapy outcome was defined in three ways:effect size (ES), response based on the reliable change index, and remission compared to the generalpopulation symptom level. Non-parametric conditional inference trees were used to predict dropouts. Inthe pre-post comparison of the BSL, the ES was 0.54 (95% CI: 0.49e0.59). The response rate was 45%; 31%remained unchanged, and 11% deteriorated. Approximately 15% showed a symptom level equivalent tothat of the general population. A further 10% of participants dropped out. A predictive impact on dropoutwas demonstrated by substance use disorders and a younger age at pre-treatment. In future research,follow-up assessments should be conducted to investigate the extent to which response and remissionrates at post-treatment remain stable over time. A consistent definition of response appears to beessential for cross-study and cross-methodological comparisons.
� 2013 Elsevier Ltd. All rights reserved.
Dialectical behavior therapy (DBT; Linehan, 1993a, 1993b) iscurrently the most frequently investigated psychosocial interven-tion for borderline personality disorder (BPD). The four core ele-ments of DBT are individual therapy, which takes place once aweek; weekly skills training within the group; telephone coachingby the individual therapist; and supervision for the therapeuticteam (Linehan,1993a,1993b). The treatment concept was originallyconceived on an outpatient basis, but has been adapted to theinpatient setting (Swenson, Sanderson, Duilt, & Linehan, 2001). Theshort- and long-term effectiveness of inpatient DBT was shown byvarious work groups (Bohus et al., 2004; Fassbinder et al., 2007;Höschel, 2006; Kleindienst et al., 2008; Kröger et al., 2006; Simpsonet al., 2004). For inpatient DBT, moderate to large effect sizesemerged at the end of treatment with regard to self-reported,general, or depressive symptom severity (ES ¼ 0.56 to 0.84and ES ¼ 0.59 to 1.90, respectively), and large effect sizes werefound with regard to psychosocial functioning as rated by others(ES¼ 0.80e1.33). However, the results of these studies are based on
fax: þ49 (0)531 391 8195.
All rights reserved.
relatively small samples (N ¼ 20 to N ¼ 50), which, moreover, weretreated in university establishments.
To date, mean value comparisons and effect sizes as a bench-mark for assessing the effectiveness of a treatment are predomi-nant in the publications on DBT, whereas the clinical significanceenables an individual assessment of the change status (cf. Jacobson,Roberts, Berns & McGlinchey, 1999). Using the parameters of clin-ical significance, it can be determined whether, at post-treatment, apatient has reliably deteriorated or improved (response), orwhether the symptom level has adjusted to that of a clinicallyunimpaired sample (remission). Only in one completer sample(N ¼ 31) was the clinical significance indicated in addition to theES of 0.84 following a three-month inpatient DBT treatment:According to this, 42% of patients at post-treatment (Bohus et al.,2004) and 50% within 21 months after the end of therapy(Kleindienst et al., 2008) were remitted in terms of general symp-tom strain.
One of the main aims of DBT is to lower dropout rates (Linehan,1993a), even though no significant difference in the mean dropoutrates between DBT (24.7%) and control conditions (27.3%) wasfound in a meta-analysis (Kliem, Kröger, & Kosfelder, 2010). In theface of these (partially) high dropout rates, ranging from 4.2% to

Table 1Socio-demographic characteristics and co-occurring mental disorders (N ¼ 1423).
Characteristics n %
Marital statusSingle 1026 72.1Married 200 14.1Divorced 110 7.7
School educationIn school education 28 2.0No school-leaving qualification 52 3.7
C. Kröger et al. / Behaviour Research and Therapy 51 (2013) 411e416412
61.1% (SD ¼ 15.6%), it seemed to be important to identify charac-teristics that are associated with discontinuation of treatment. Tothe best of our knowledge, four studies have examined differencescompared to completers and predictive factors for inpatients whodropped out of DBT (Bohus et al., 2004; Kröger et al., 2006; Perroud,Uher, Dieben, Nicastro, & Huguelet, 2010; Rüsch et al., 2008). Whileno differences in any aspect were found between completers anddropouts in the Bohus et al. (2004) and Kröger et al. (2006) studies,dropouts in the Rüsch et al. (2008) study reported more traitanxiety, fewer lifetime suicide attempts, and higher experientialavoidance (without error correction for multiple testing). The lattertwo characteristics were both confirmed in a stepwise logisticregression as dependent variables for dropout. However, lowereducation was found to be the only predictive characteristic in thePerroud et al. (2010) study, which did not include those charac-teristics (i.e., lifetime suicide attempts and experiential avoidance)that were found in the Rüsch et al. (2008) study.
These results were based on small sample sizes, ranging from 40to 60 mostly female participants, with the exception of the Perroudet al. (2010) study, with 447 participants. In addition, low dropoutrates were reported, ranging from 12% to 25.8%, with the exceptionof the Rüsch et al. (2008) study, with 46%. Therefore, sample sizesand dropout rates made it difficult to find any differences betweencompleters and dropouts due to a lack of statistical power. The useof a regression analysis in the Rüsch et al. (2008) study implies alarger sample size than 60 participants, and requires a confirmationin a cross-validation analysis. Since individuals with specific co-occurring mental disorders were excluded (e.g., anorexia nervosa,substance use disorders, Bohus et al., 2004; Rüsch et al., 2008),these conditions could not be included in the analyses, even thoughthey might also be suggested as risk factors for a discontinuation oftreatment (Kröger et al., 2010; Linehan et al., 2002). Hence, resultsneed to be confirmed and expanded in further analyses, whichshould be based on larger sample sizes with fewer exclusioncriteria.
The aim of the current study is, therefore, to use a largeconsecutive sample of patients admitted to a 3-month DBT pro-gram in order to draw on various parameters for assessing itseffectiveness regarding disorder-specific symptom strain andfurther complaints. For this purpose, in particular, effect sizesshould be calculated in comparison to the clinical significancethrough the RCI method (Jacobson & Truax, 1991). Moreover, afurther aim is to identify predictors of discontinuation of therapy.
Special needs or lower-track school-leaving qualification 327 22.9Medium-track school-leaving qualification 515 36.2University-entrance-level school-leaving qualification 76 5.3Other 10 0.7
Employment statusNever employed 190 13.4In training 234 16.4Military service/civilian service (in lieu of military service)/voluntary social year
22 1.5
Housewife/househusband 272 19.1Pensioner 98 6.9Laborer 77 5.4Skilled worker/craftsperson 39 2.7Employee 297 20.9Civil servant 23 1.6Self-employed 27 1.9Other 83 5.8
Prior treatmentsOutpatient psychiatric 842 59.2Outpatient psychotherapeutic 960 67.5
Mental disordersAffective disorders 1363 95.8Substance use disorders 264 18.6Anxiety disorders 588 41.3Somatoform disorders 97 6.9Eating disorders 527 37.1
Method
Participants
The participants were admitted consecutively to a psychoso-matic care hospital, which is certified according to DIN EN ISO9001:2008, in the period fromMarch 2006 to October 2011. For thediagnosis of mental disorders and personality disorders, theGerman versions of the Structured Clinical Interview for DSM-IVAxis I Disorders (SKID-I; Wittchen, Wunderlich, Gruschitz, &Zaudig, 1997) and for Axis II Disorders (SKID-II; Fydrich,Renneberg, Schmitz, & Wittchen, 1997) were used. All partici-pants had to a) be over the age of 18 years, b) show no indications ofmental retardation, dementia, or schizophrenia, c) show no acutesymptoms of a severe organic disease that are associated with thedevelopment of the mental illness, and d) show no substancedependence with current intoxication, which would indicate anadmission at a specialized unit for detoxification. Other mentaldisorders were not excluded. Each patient was informed aboutthe course of the study in writing and was required to provide
consent to it. The treatment period amounted to a maximum oftwelve weeks.
The analysis included N ¼ 1423 patients with BPD, of whomn ¼ 1075 were women (75.5%). Table 1 shows the sociodemo-graphic data and comorbid mental disorders. The mean age lay at32.0 years (SD ¼ 10.27). Approximately 14% lived in a partnership.On average, each patient had 3.70 (SD ¼ 1.59) Axis I disorders and0.90 (SD ¼ 0.6) Axis II disorders, in addition to BPD. The length ofstay in the clinic amounted to an average of 63.9 days (SD ¼ 19.65).Hence, several participants were discharged with the support andpermission of the therapists before the three months were over,because these patients had legal or other obligations (e.g., lawsuit,start of school) and changes in managing their daily life (e.g.,admission at a therapeutic apartment-sharing community). Thetreatment was not ended in the standard manner by 148 (10.4%)patients (discontinuation with or without physician consent ortransfer). Of these individuals, 93 did not fill out the postal surveyquestionnaires (missing values).
Therapists and treatment
The multidisciplinary teams consisted of 5 certified DBT thera-pists, 5 certified DBT co-therapists, and 5 DBT therapists inadvanced training. Moreover, they also intermittently includedphysicians in training as specialists for psychosomatic medicine orfor psychiatry and psychotherapy, and psychotherapists in training.Also, the teams consistently included social education workers andart and movement therapists who possessed basic knowledge ofDBT through in-house and external training programs. The teamsdiscussed the individual patients on a daily basis. Moreover,recurring structural or content-based questions were tackled atleast twice yearly in a half-day workshop.

C. Kröger et al. / Behaviour Research and Therapy 51 (2013) 411e416 413
The teams were supervised by three team leaders who werestate-recognized supervisors for behavioral therapy and certifiedDBT therapists. The team leaders were available three times perweek for supervisory and structural matters. Once a year, a whole-day workshop with a licensed DBT supervisor took place.
The inpatient concept of DBT was certified by the GermanUmbrella Association of DBT and is described in detail elsewhere(Armbrust & Jungbluth, 2009). At the beginning and end of treat-ment, a team leader and the patient establish and check treatmentgoals. The target hierarchy determines that skills be set up whichenable an outpatient treatment. Hence, the treatment focus is onthe behaviors that led to the inpatient admission, to lengtheningthe clinic stay, or to readmission. The therapy components wereindividual therapy (once a week; 50 min), the psycho-educativebasic group (once a week; 50 min), the skills training in the areaof distress tolerance, emotion regulation, and interpersonal effec-tiveness (twice a week; each 100 min), the mindfulness training(once a week; 60 min), and the practice groups managed by thepatients themselves. Further components were movement therapyand art therapy (each twice a week; 100 min), which predomi-nantly served the purpose of building up skills in the area ofemotion and self-worth regulation. Furthermore, a “PatientParliament” took place weekly, and a trialogue meeting (e.g., withpatients and their relatives or friends) took place every six weeks(Link & Tilly, 2006).
Measures
The anamnesis questionnaire consisted of 52 questions aboutthe patient and his or her problems. The following outcome mea-sures were used: Borderline Symptom List (BSL; Bohus et al., 2007),Brief Symptom Inventory (BSI, Franke, 2000), Beck Depression In-ventory (BDI; Hautzinger, Bailer, Worall, & Keller, 1995), and theGlobal Assessment of Functioning Scale (GAF; APA, 1994).
Statistical analyses
EffectivenessThe problem of missing data was corrected using multiple im-
putations, as recommended by Schafer and Graham (2002). Theindependent variables age, gender, baseline measurements, andpost-treatment measurements were included in the generation of10 complete data sets by chained equations modeling (White,Royston, & Wood, 2011). Variables with missing data werecompleted following the imputation method of predictive meanmatching. The R package “MICE” (Multivariate Imputation byChained Equations; Buuren & Groothuis-Oudshoorn, 2011) wasapplied for this procedure. To complete the process, the 10 imputeddata sets were used to compare the mean values before and afterthe treatment. In accordance with Rubin’s rule (1987), the calcu-lation of the standard errors of the pooled coefficients considers thevariations within each imputation (common uncertainty of esti-mation) as well as between imputations (uncertainty of imputa-tion). Subsequently, pooled dependent t-tests with Bonferronicorrection (two-sided) were carried out. In order to quantify theeffect of the treatment, we estimated the pooled effect sizes (ES;Hedges & Olkin, 1985). In accordance with Cohen’s convention(1988), ES > 0.2 is regarded as a small, ES > 0.5 as a medium, andES > 0.8 as a large effect size.
ResponseFollowing Jacobson and Truax (1991), we calculated the RCI to
determine the percentage share of patients who remained un-changed or reliably improved or deteriorated. The calculation wasmade according to the following formula:
RCI ¼ Xpre � Xpost
Sdiff; whereby Sdiff ¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2*
�SE
�2rand
SE ¼ SD*ffiffiffiffiffiffiffiffiffiffiffiffiffiffi1� rtt
p
with:
Xpre ¼ BSL total score at beginning of therapyXpost ¼ BSL total score at end of therapySD ¼ Standard deviation of the clinical norm sample,rtt ¼ Reliability of the measurement instrument, which corre-sponds here to Cronbach’s alpha.
In order to calculate the standard error (SE), we referred to areference population of inpatients with BPD (Kröger et al., 2010:SD ¼ 0.66, a ¼ 0.94). An RCI above the 95% confidence limits �1.96counts as evidence of a reliable change (p � 0.05). A critical value of0.45must beexceededby thedifferencebetweenpre- andpost-meanvalue of a patient for the patient to be counted as having responded.
RemissionTo establish whether responders can also be seen as remitted,
the cut-off point C was calculated, the use of which was favoredbecause it takes into account the overlapping of the two distribu-tions of normal and impaired population (Jacobson et al., 1999). Thecalculation was made according to the following formula:
Cut� off point C ¼�MDys*SDNorm þMNorm*SDDys
�ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi�SDDys*SDNorm
�q
For the impaired population, the data of the inpatient samplewith BPD were also used (Kröger et al., 2010: M ¼ 1.89, SD ¼ 0.66).As a frame of reference with respect to the normal population, thedata of a general population (Bohus et al., 2007:M¼ 0.4; SD¼ 0.22)were drawn on in order to operationalize remission as theachievement of the symptom level of a clinically unimpairedsample. To calculate the remission rates, a cut-off point of C ¼ 0.80emerged. If a responded patient falls below the respective cut-offpoint C with his or her BSL post-value, he or she is seen as remitted.
DropoutNon-parametric conditional inference trees (C-Trees; Hothorn,
Hornik, & Zeileis, 2006; Strobl, Malley, & Tutz, 2009) based on theprinciple of recursive partitioning were applied to analyze associ-ations between pre-treatment measurements and risk of dropout.An exact permutation testwill assess the strength of the associationbetween response and input variable (Strasser & Weber, 1999).Since permutation tests derive the p-values from sample-specificpermutation distributions of the test statistics, only p-values arereported. In the following analysis, gender, age, social, educational,and employment status, treatment history, as well as the level ofmean pre-treatment scores of outcome measures (BSL, BDI, GSI,and GAF, respectively), co-occurring mental disorders, and psy-chosocial stress factors were selected for testing the associationwith dropout (no ¼ 0; yes ¼ 1). The R package “party” (a laboratoryfor recursive partitioning; Hothorn, Hornik, Strobl, & Zeileis, 2011)was used for this analysis.
Results
Outcome
Table 2 displays the means and standard deviation of the fouroutcome measures based on the 10 imputed data sets, usingRubin’s rule for the pooling procedure. The mean pre-treatment

Table 2Means (M), standard deviations (SD) and effect sizes (ES) at pre- and post-treatment.
Pre Post t p* jESj 95% CI
M SD M SD
BSL total score 1.83 0.70 1.44 0.76 20.22 <0.001 0.54 0.49; 0.59BSL-Subscales Self-perception 1.56 0.87 1.11 0.86 19.68 <0.001 0.52 0.47; 0.57
Affect regulation 2.18 0.87 1.74 0.93 17.39 <0.001 0.46 0.41; 0.51Self-destruction 1.71 1.01 1.34 1.08 14.05 <0.001 0.37 0.32; 0.42Dysphoria 3.05 0.49 2.69 0.66 20.47 <0.001 0.54 0.49; 0.59Loneliness 1.65 0.86 1.14 0.87 20.02 <0.001 0.53 0.48; 0.58Intrusions 0.95 0.70 0.77 0.71 10.94 <0.001 0.29 0.24; 0.34Hostility 1.47 0.90 1.28 0.84 7.37 <0.001 0.20 0.15; 0.25
BDI 28.98 14.49 20.79 13.65 25.29 <0.001 0.67 0.62; 0.72GSI 1.72 0.69 1.25 0.73 26.82 <0.001 0.71 0.66; 0.76GAF 46.99 8.85 54.33 9.07 �38.38 <0.001 1.02 0.94; 1.08
Note. BSL¼ Borderline Symptom List; BDI¼ Beck Depression Inventory; GSI¼ Global Severity Index of the Brief Symptom Inventory; GAF¼ Global Assessment of FunctioningScale; p* ¼ p-value, corrected for multiple testing.
C. Kröger et al. / Behaviour Research and Therapy 51 (2013) 411e416414
BSL score of 1.83 (SD ¼ 0.70) was comparable to the level ofborderline-specific symptoms of the BPD subsample that was re-ported in Bohus et al. (2007). The mean BDI score of 28.98(SD ¼ 14.49) and the mean pre-treatment GSI score of 1.72(SD¼ 0.69) were comparable to other inpatient samples (see Bohuset al., 2004; Kröger et al., 2006: mean BDI scores ¼ 31.3, SD ¼ 9.4,and 31.96, SD ¼ 11.03; mean GSI scores ¼ 1.74, SD ¼ 0.48, and 1.80,SD ¼ 0.68, respectively), indicating a very high level of symptomstrain and depression at pre-treatment. The GAF score of 46.99(SD ¼ 8.85) was similar to the Bohus et al. study (2004; mean GAFscore ¼ 48.5, SD ¼ 8.4), but higher than the Kröger et al. study(2006, mean GAF score ¼ 35.16, SD ¼ 10.11), indicating a moder-ate impairment in psychosocial adaptation.
EffectivenessAs shown in Table 2, the scores of the BSL, BDI, and GSI of the BSI
decreased significantly over time, while the score of the GAFincreased significantly. The ES was small to moderate in the self-rating measures (ES ¼ 0.20e0.71) and large in the GAF Scale(ES ¼ 1.02).
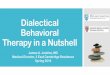
Response and remission ratesForty-five percent of the participants were classified as
responded. A symptom level corresponding to that of a generalpopulation was shown by 14.8%. About 11% deteriorated, and 30.6%remained unchanged despite the treatment. Fig. 1 illustrates theresponse and remission rates.
Dropout
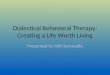
Participants with co-occurring substance use disorders showeda significantly higher risk of discontinuing treatment. Moreover,patients whowere additionally aged�20 years were particularly atrisk. Fig. 2 illustrates the risk of dropout in the C-Tree.
Discussion
The ES of 0.54 for the reduction of the BSL total score lies in therange of a current meta-analysis (Kliem et al., 2010), reporting aglobal ES of 0.50 (95% CI [0.43, 0.57]) based on various outcomemeasures. In linewith previous studies (Bohus et al., 2004; Höschel,2006; Kröger et al., 2006; Simpson et al., 2004), the non-disorder-specific and depressive symptoms were reduced and the psycho-social functioning was increased.
In accordance with the RCI, approximately a third of the treatedindividuals remained unchanged and about 11% deteriorated. Asymptom level like that of a general population was reached by
approximately 15%. Compared to the Bohus et al. (2004) study, theremission rate (42%) thus emerged as clearly lower, although bothinpatient staffs were certified by the German Umbrella Associationof DBT. Again, it should be noted that the results of the Bohus et al.study were based on a small completer sample (N ¼ 31), excludingall substance use disorders and using the general symptom strain asthe main outcome, but no borderline-specific measure.
The dropout rate of approximately 10% was low in comparison toprevious studies in the inpatient setting (from 12.0%, Kröger et al.,2006; to 25.8%, Bohus et al., 2004). Substance use disorders andyounger age were found to be predictive of dropout. Hence, theremight be evidence of an adaptation, including more validating andmotivating strategies (Linehan et al., 2002) as well as multifamilyskills training and interventions addressing family members andsocial environment (Katz, Cox, Gunasekara, & Miller, 2004;Woodberry & Popenoe, 2008). However, we did not include factorsthat have shown their predictive significance in other studies (i.e.,trait anxiety, experiential avoidance; Rüsch et al., 2008). On a furthercritical note, the sociodemographic characteristics were onlyassessed through self-disclosure. To measure family burden as apossible predictor, an interaction diagnosis or an interview withfamily members, for instance, would be desirable (cf. Hooley &Hoffman, 1999).
The major limitation of the study is that it uses an uncontrolled,nonrandomized design, thus making it impossible to determinewhether any changes that were found were a result of treatmentversus other factors (e.g., the passage of time, regression to themean). Furthermore, the main outcome measure was only a self-rating instrument and not one of the recommended disorder-specific interviews (Zanarini et al. 2010). Under the conditions ofa standard care hospital, the treatment providers’ adherence to themanual could not be evaluated by external assessors. The phar-macological treatment was not systematically recorded and couldtherefore not be controlled for as an additional predictor of drop-outs. However, the effects of the pharmacological treatment onthe target symptoms can be assumed to be low (e.g., Simpsonet al., 2004).
To the best of our knowledge, this is the first study that uses alarger, gender-mixed sample in order to evaluate the treatmentsuccess of inpatient DBT using group- and individual-specific pa-rameters. In our view, including indices of statistical and clinicalsignificance results in a realistic basis for treatment evaluation. Toconduct comparisons across studies and procedures, uniform def-initions of response and remission appear to be necessary. In thefuture, follow-up assessments should be implemented in order toexamine the extent to which the rates at the end of treatmentremain stable over time.

60 %
substance use disorder
ageno yes
20 years > 20 years
100 %
0 %
20 %
40 %
60 %
80 %
subgroup 1 (n = 121)
0 %
subgroup 3 (n = 135)
0 %
subgroup 2 (n = 1167)100 % 100 %
20 %
40 %
80 %
20 %
40 %
60 %
80 %
Fig. 2. The risk of dropout in a non-parametric conditional inference tree. (The percentaged share of dropouts in each subgroup is marked in black.)
Fig. 1. Clinically significant change in accordance with the RCI for the total score of the Borderline Symptom List. In the area between the dotted diagonal lines are patients in whomno change occurred (black). Above the upper dotted line are patients whose symptoms worsened (red). All patients below the lower dotted line showed a response to the treatment.Patients who responded to the treatment but were still burdened after the treatment are found between the dotted line and above the cut-off point (yellow). Below the green line(cut-off point C) are patients whose symptom level at the end of treatment corresponded to that of a healthy sample (Bohus et al., 2007). (For interpretation of the references tocolor in this figure legend, the reader is referred to the web version of this article.)
C. Kröger et al. / Behaviour Research and Therapy 51 (2013) 411e416 415

C. Kröger et al. / Behaviour Research and Therapy 51 (2013) 411e416416
The response and remission rates also give rise to questions ofindication for inpatient DBT. The non-responding patients mightpossibly benefit from interventions other than inpatient treatment(e.g., a partial-inpatient treatment). The adaptation of the thera-peutic relationship through a feedback system for therapists (e.g.,Lutz, Tholen, Kosfelder, Tschitsaz, Schürch & Stulz, 2005) could alsoexert an impact on the disorder-specific symptoms. So far, however,process-oriented aspects have received little investigation (Bedics,Atkins, Comtois, & Linhan, 2012).
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mentaldisorders (DSM-IV) (4th ed.). Washington. D.C: APA.
Armbrust, M., & Jungbluth, G. (2009). Stationäre Verhaltenstherapie für MenschenmitPersönlichkeitsstörungen in einem psychosomatischen Versorgungskrankenhaus.In E. Fabian, B. Dulz, & P. Martius (Eds.). Therapiespektrum und klinikspezifischeBehandlungskonzepte: Stationäre Psychotherapie der Borderline-Störungen (pp. 51e70). Stuttgart: Schattauer.
Bedics, J. D., Atkins, D. C., Comtois, K. A., & Linhan, M. M. (2012). Treatment dif-ferences in the therapeutic relationship and introject during a 2-year ran-domized controlled trial of dialectical behavior therapy versus nonbehavioralpsychotherapy experts for borderline personality disorder. Journal of Consultingand Clinical Psychology, 80, 66e77.
Bohus, M., Haaf, B., Simms, T., Limberger, M. F., Schmahl, C., Unckel, C., et al. (2004).Effectiveness of inpatient dialectical behavioral therapy for borderline person-ality disorder: a controlled trial. Behaviour Research and Therapy, 42, 487e499.
Bohus, M., Limberger, M. F., Frank, U., Chapman, A., Kühler, T., & Stieglitz, R. D.(2007). Psychometric properties of the borderline symptom list (BSL). Psycho-pathology, 40, 126e132.
Buuren, S., & Groothuis-Oudshoorn, K. (2011). Multivariate imputation by chainedequations in R. Journal of Statistical Software, 45, 1e67.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).Hillsdale, NJ: Lawrence Earlbaum Associates.
Fassbinder, E., Rudolf, S., Bussiek, A., Kröger, C., Arnold, R., Greggersen, W., et al.(2007). Effektivität der dialektischen Verhaltenstherapie bei Patienten mitBorderline-Persönlichkeitsstörung im Langzeitverlauf e Eine 30-Monats-Katamnese nach stationärer Behandlung. Psychotherapie Psychosomatik Medi-zinische Psychologie, 57, 161e169.
Franke, G. H. (2000). Brief symptom inventory (BSI). Göttingen: Beltz.Fydrich, T., Renneberg, B., Schmitz, B., & Wittchen, H.-U. (1997). Strukturiertes Kli-
nisches Interview für DSM-IV, Achse II (SKID II). Göttingen: Hogrefe.Hautzinger, M., Bailer, M., Worral, H., & Keller, F. (1995). Das Beck depressions-
inventar (BDI) (2.Auflage).. Bern: Huber.Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. San Diego, CA:
Academic Press.Hooley, J. M., & Hoffman, P. D. (1999). Expressed emotion and clinical outcome in
borderline personality disorder. American Journal of Psychiatry, 156, 1557e1562.Höschel, K. (2006). Dialektisch Behaviorale Therapie der Borderline Persön-
lichkeitsstörung in der Regelversorgung e Das Saarbrücker DBT-Modell. Ver-haltenstherapie, 16, 17e24.
Hothorn, T., Hornik, K., Strobl, C., & Zeileis, A. (2011). A laboratory for recursive parti-tioning. Retrieved from http://cran.r-project.org/web/packages/party/party.pdf.
Hothorn, T., Hornik, K., & Zeileis, A. (2006). Unbiased recursive partitioning: aconditional inference framework. Journal of Computational and Graphical Sta-tistics, 15, 651e674. http://dx.doi.org/10.1198/106186006X133933.
Jacobson, N. S., Roberts, L. J., Berns, S. B., & McGlinchey, J. B. (1999). Methods fordefining and determining the clinical significance of treatment effects.Description, application, and alternatives. Journal of Consulting and ClinicalPsychology, 67, 300e307.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: a statistical approach todefining meaningful change in psychotherapy research. Journal of Consultingand Clinical Psychology, 59, 12e19.
Katz, L. Y., Cox, B. J., Gunasekara, S., & Miller, A. (2004). Feasibility of dialecticalbehavior therapy for suicidal adolescent inpatients. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 43, 276e282.
Kleindienst, N., Limberger, M. F., Schmahl, C., Steil, R., Ebner-Priemer, U. W.,Linehan, M. M., et al. (2008). Do improvements after inpatient dialectialbehavioral therapy persist in the long term? A naturalistic follow-up in patientswith borderline personality disorder. Journal of Nervous and Mental Disease, 196,838e843.
Kliem, S., Kröger, C., & Kosfelder, J. (2010). Dialectical behavior therapy forborderline personality disorder: a meta-analysis using mixed-effects modeling.Journal of Consulting and Clinical Psychology, 78, 936e951.
Kröger, C., Schweiger, U., Sipos, V., Arnold, R., Kahl, K. G., Schunert, T., et al. (2006).Effectiveness of dialectical behaviour therapy for borderline personality disor-der in an inpatient setting. Behaviour Research and Therapy, 44, 1211e1217.
Kröger, C., Theysohn, S., Hartung, D., Vonau, M., Lammers, C.-H., & Kosfelder, J.(2010). Die Skala zur Erfassung der Impulsivität der Borderline-Persön-lichkeitsstörung (IS-27). Ein Beitrag zur Qualitätssicherung in der Psychother-apie. Diagnostica, 56, 178e189.
Linehan, M. M. (1993a). Cognitive-behavioral treatment of borderline personalitydisorder. New York, NY: Guilford Press.
Linehan, M. M. (1993b). Skills training manual for treating borderline personalitydisorder. New York, NY: Guilford Press.
Linehan, M. M., Dimeff, L. A., Reynolds, S. K., Comtois, K. A., Shaw-Welch, S.,Heagerty, P., et al. (2002). Dialectical behavior therapy versus comprehensivevalidation therapy plus 12-step for the treatment of opioid dependent womenmeeting criteria for borderline personality disorder. Drug and Alcohol Depen-dence, 67, 13e26.
Link, A., & Tilly, C. (2006). Borderline-Trialog und Peer-Support. In C. Kröger, &C. Unkel (Eds.), Borderline-Störung. Wie mir DBT geholfen hat (pp. 157e169).Göttingen: Hogrefe.
Lutz, W., Tholen, S., Kosfelder, J., Tschitsaz, A., Schürch, E., & Stulz, N. (2005). DieEvaluation des therapeutischen Fortschritts als Baustein eines störungss-pezifischen Rückmeldesystems zur Qualitätssicherung in der Psychotherapie.Verhaltenstherapie, 3, 168e175.
Perroud, N., Uher, R., Dieben, K., Nicastro, R., & Huguelet, P. (2010). Predictors ofresponse and drop-out during intensive dialectical behavior therapy. Journal ofPersonality Disorders, 24, 634e650.
Rubin, D. B. (1987). Multiple imputation for nonresponse in surveys. New York: JohnWiley & Sons.
Rüsch, N., Schiel, S., Corrigan, P. W., Leihener, F., Jacob, G. A., Olschewski, M., et al.(2008). Predictors of dropout from inpatient dialectical behavior therapy amongwomen with borderline personality disorder. Journal of Behavior Therapy andExperimental Psychiatry, 39, 497e503.
Schafer, J. L., & Graham, J. W. (2002). Missing data: our view of the state of the art.Psychological Methods, 7, 147e177.
Simpson, E. B., Yen, S., Costello, E., Rosen, K., Begin, A., Pistorello, J., et al. (2004).Combined dialectical behavior therapy and fluoxetine in the treatment ofborderline personality disorder. Journal of Clinical Psychiatry, 65, 379e385.
Strasser, H., & Weber, C. (1999). On the asymptotic theory of permutation statistics.Mathematical Methods of Statistics, 8, 220e250.
Strobl, C., Malley, J., & Tutz, G. (2009). An introduction to recursive partitioning:Rationale, application and characteristics of classification and regression trees,bagging and random forests. Psychological Methods, 14, 323e348.
Swenson, C. R., Sanderson, C., Duilt, R., & Linehan, M. M. (2001). The application ofdialectical behavior therapy for patients with borderline personality disorderon inpatient units. Psychiatric Quarterly, 72, 307e324.
White, I. R., Royston, P., & Wood, A. M. (2011). Multiple imputation using chainedequations: issues and guidance for practice. Statistics in Medicine, 30, 377e399.
Wittchen, H.-U., Wunderlich, U., Gruschitz, S., & Zaudig, M. (1997). StrukturiertesKlinisches Interview für DSM-IV, Achse I (SKID-I). Göttingen: Hogrefe.
Woodberry, K. A., & Popenoe, E. J. (2008). Implementing dialectical behavior ther-apy with adolescents and their families in a community outpatient clinic.Cognitive and Behavioral Practice, 15, 277e286.
Zanarini, M. C., Stanley, B., Black, D. B., Markowitz, J. C., Goodman, M.,Pilkonis, P., et al. (2010). Methodological considerations for treatment trialsfor persons with borderline personality disorder. Annals of Clinical Psychi-atry, 22, 75e83.