Embed Size (px)
Citation preview

Effect of eradication of Helicobacter pylori on geneticinstabilities in gastric intestinal metaplasiaA. TANAKA*, J . WATARI* , H. TANABE* , A . MAEMOTO* , M. FUJIYA* , T . ASHIDA* , K . M. DAS� & Y. KOHGO*
*Third Department of Internal Medi-
cine, Asahikawa Medical College, Asa-
hikawa, Japan; �Division of
Gastroenterology and Hepatology,
Department of Medicine and Pathol-
ogy, Crohn’s and Colitis Center of
New Jersey, UMDNJ-Robert Wood
Johnson Medical School, New Bruns-
wick, NJ, USA
Correspondence to:
Dr J. Watari, Third Department of
Internal Medicine, Asahikawa Medical
College, 2-1-1-1 Midorigaoka-Higashi,
Asahikawa 078-8510, Japan.
E-mail: [email protected]
Publication data
Accepted 15 March 2006
SUMMARY
BackgroundThere is little evidence of changes in genetic variations in gastric intest-inal metaplasia (GIM) after the eradication of Helicobacter pylori(H. pylori).
AimTo investigate the effects of H. pylori eradication on genetic GIM varia-bility in patients with and without gastric cancer in a one-year prospec-tive study.
MethodsWe analysed microsatellite instability (MSI) and loss of heterozygosity(LOH) in GIM. Subjects included Gr. A (n ¼ 39): chronic gastritis, andGr. B (n ¼ 53): intestinal-type early gastric cancer patients who under-went endoscopic mucosal resection (n ¼ 25) and surgical resection(n ¼ 28).
ResultsThe frequency of incidence of MSI in GIM was 10.3% and 28.3% forGr. A and Gr. B, respectively. Gr. B showed a significantly (p ¼ 0.03)higher incidence rate than Gr. A for MSI, but not for LOH. The fre-quency of MSI declined in both groups post-eradication, and patientsthat were positive for MSI before treatment were negative afterH. pylori eradication. Unfortunately, however, GIM scores did notdecline significantly post-treatment for either group.
ConclusionsMSI in GIM may be associated with gastric carcinogenesis. H. pylorieradication reduced MSI during the one-year post-treatment period,although no histological improvement in GIM was observed. These
changes in MSI may explain the decrease in gastric cancer incidenceafter the eradication of H. pylori.
Aliment Pharmacol Ther symp ser 2, 194–202
AP&T symposium series
194 ª 2006 The Authors
Journal compilation ª 2006 Blackwell Publishing Ltd

INTRODUCTION
Helicobacter pylori (H. pylori) infection is a major risk
factor for the development of gastric cancer.1–5 It has
been postulated that H. pylori infection causes the chro-
nic gastritis and gastric atrophy that are usually associ-
ated with gastric intestinal metaplasia (GIM) and gastric
dysplasia. These stepwise stages, which usually proceed
over decades, have been defined as a sequence of histo-
logical events that confer an increasing risk of malignant
transformation, as described in Correa’s hypothesis.6
Although it is widely accepted that H. pylori infection
plays a significant role in causing gastric cancer, the
mechanisms of pathogenesis have not been precisely
determined. In general, GIM is believed to be a preneo-
plastic lesion of the stomach7 which increases the risk
of gastric adenocarcinoma, especially the intestinal
type.6,8 It remains unclear, however, whether GIM is a
precancerous lesion in itself, or whether it is a marker
for an increased risk of malignancy.9,10
An important factor in the rapid accumulation of
genetic changes lies in the genetic instability11 of
these gastric lesions. It has been suggested that indi-
viduals with microsatellite instability (MSI) have a
higher tendency to accumulate alterations in their
genetic material that lead to the transformation of
normal cells into cancerous ones.12 However, a num-
ber of technical problems have been found with the
conventional methods used to analyse genetic instabil-
ity in previous investigations. For example, the accu-
racy of migration in DNA sequencing gel in which the
PCR products are electrophoresed is not sufficient to
allow accurate comparison of the two independent
lanes. Moreover, the autoradiography used has biased
detection characteristics, which means that the inten-
sity of the bands cannot be estimated with high accu-
racy.13 These problems have influenced the results of
MSI and loss of heterozygosity (LOH) analyses.14 A
high-resolution fluorescent microsatellite analysis
(HRFMA) system was recently developed to overcome
these problems.13 We previously used this assay to
investigate genetic alterations caused by gastric can-
cer.15 To date, some studies on MSI in GIM in patients
with and without gastric cancer have been reported,
but the results have been conflicting,16–21 and none
involved the use of HRFMA system analysis in MSI.
As for LOH in gastric cancer, previous studies have
shown that LOH is common in intestinal-type but is
rare in diffuse-type,22–26 but there are only a few
reports on LOH in GIM.27,28
Gastric cancer will not develop in all individuals with
GIM, and the molecular events governing this progres-
sion remain unclear. Moreover, changes in genetic
instabilities such as MSI and LOH in GIM after H. pylori
eradication have not yet been investigated. In this study,
we evaluated the frequency of MSI and LOH, in GIM-
related H. pylori infections in patients with and without
gastric cancer. The effects of the eradication of H. pylori
on genetic changes in GIM, which is considered to be a
well-recognized precursor of gastric cancer, are also
assessed in a 1-year prospective study. Finally, we also
examined whether the eradication of H. pylori affects
the subsequent histological grading of GIM.
MATERIALS AND METHODS
All patients undergoing upper gastrointestinal endo-
scopy at Asahikawa Medical College Hospital between
January 2002 and April 2004 were invited to partici-
pate in the study. Patients who had undergone surgical
gastric resection and those taking aspirin or other non-
steroidal anti-inflammatory drugs were excluded. We
enrolled 69 patients who had been treated successfully
for H. pylori infection and had been found to have
atrophic gastritis (n ¼ 43) and intestinal-type mucosal
gastric cancer after endoscopic mucosal resection
(EMR) (n ¼ 26). In all patients, biopsy specimens were
taken to assess H. pylori infection, two each from the
greater curvature of the antrum and the greater curva-
ture of the corpus. The presence of H. pylori was deter-
mined to be present by a positive result in either or
both Wartin–Starry staining or H. pylori culture. For
eradication, patients were treated with lansoprazole
(30 mg), amoxicillin (750 mg) and clarithromycin
(400 mg), all taken twice daily for 1 week. Following
successful eradication, all patients were followed-up
with an endoscopic examination 1 year later. Of 69
patients, five patients, consisting of four chronic gastri-
tis patients and one gastric cancer patient, were exclu-
ded from this study because no GIM was seen in
biopsy samples in either before treatment or after treat-
ment or both. Finally, 64 patients who showed GIM in
gastric biopsy samples both before and after H. pylori
eradication were investigated. In these patients, the
clearance of H. pylori was also confirmed by negative
results by both Wartin–Starry staining and H. pylori
culture at a follow-up endoscopy.
The written informed consents of the patients were
obtained, and the study was approved by the Ethics
Committee of Asahikawa Medical College.
GENET IC INSTABIL IT IES IN INTEST INAL METAPLASIA 195
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

The patient pool comprised two groups, group A
(n ¼ 39): chronic gastritis and group B (n ¼ 53):
intestinal-type early gastric cancer. Group B was fur-
ther divided into group B1 (n ¼ 25): comprising EMR
cases diagnosed as mucosal cancer and group B2
(n ¼ 28): surgical resection cases, consisting of 10
mucosal cancers and 18 submucosal invasive cancers
(Table 1). In order to improve the precision of the fre-
quencies of the genetic instabilities, the number of
samples was increased. Twenty-eight intestinal-type
early gastric cancer cases that had undergone surgical
resection (group B2) were randomly selected from the
histopathology files of Asahikawa Medical College
Hospital during the same period and added to this
study. Early gastric cancer was defined as any cancer
in which invasion was limited to the submucosal
layer.29 Lauren’s classification30 was used to diagnose
all intestinal-type cancers. All patients in group B1
underwent EMR for their mucosal cancer lesions and
then received treatment for H. pylori.
DNA extraction
One antral biopsy sample embedded in paraffin for
histological examination was also used for DNA
extraction. Two 10-lm tissue sections were serially cut
from these and DNA was selectively extracted from
GIM in the cancerous area. During extraction, tissues
were precisely microdissected under a microscope
using a PixCell laser capture microdissection system
(Arcturus Engineering, Mountain View, CA, USA) to
avoid DNA contamination of inflammatory or stromal
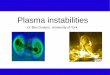
cell nuclei (Figure 1).Analysis of microsatellite instability (MSI) andloss of heterozygosity (LOH) using high-resolution fluorescent microsatellite analysis(HRFMA)
We examined five microsatellite loci on chromosomes
for MSI and LOH based on the Bethesda panel31 as fol-
lows: BAT26, D2S123, BAT25, D5S346 and D17S250.
One primer for each primer pair was fluorescence-
labelled at the 5¢ end. PCR amplification was carried
out in a reaction volume of 10 lL, which contained
100 ng of genomic DNA, 1x PCR buffer (Perkin Elmer
Applied Biosystems Division, Foster City, CA, USA),
200 lmol/L of each dNTP, 600 lmol/L of each primer
and 1.5 units of AmpliTaq GOLD polymerase (Perkin
Elmer). MgCl2 concentration was 1.5 mmol/L. The fol-
lowing PCR cycle conditions were used for amplifica-
tion: 95 �C for 10 min, 30 cycles of 95 �C for 45 s,
55 �C for 1 min, 72 �C for 30 s. The PCR products
a
b
Figure 1. Metaplastic glands were isolated by laser cap-ture microdissection. (a) H&E staining and (b) Same sec-tion after the removal of metaplastic glands.
Table 1. Characteristics of patients with gastric intestinalmetaplasia
GroupNo. ofpatients Male:Female
Mean age(range)
Group A 39 26:13 55a (40–75)Group B 53 42:11 66a (42–86)Group B1 25 21:4 61b (42–79)Group B2 28 21:7 70b (51–86)
Group A, chronic gastritis; Group B, intestinal type earlygastric cancer; Group B1, intestinal type mucosal gastriccancer underwent endoscopic mucosal resection; Group B2,intestinal type early gastric cancer underwent surgical resec-tion; aP < 0.005, bP < 0.005.
196 A. TANAKA et al.
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

were evaluated for MSI and LOH by capillary electro-
phoresis using an ABI prism 310 Genetic analyzer
(Perkin Elmer) and automatic sizing of the alleles
using a GeneScan (Applied Biosystems). MSI status
was judged as positive when the presence of an
unequivocal extra peak bands in tumour DNA that dif-
fered from normal mucosal DNA by a multiple of two
dinucleotide marker base pairs or one mononucleotide
marker base pair was observed. MSI was also charac-
terized by the appearance of drastic additional alleles
in the tumour DNA. The former type of MSI was
judged to be a minor pattern and the latter type a
major pattern, as reported previously.14,15 Tumours
were defined as MSI-H when unstable loci were
observed in more than 30%, and MSI-L when unstable
loci were observed in less than 30%.31 The tumours
were declared to be MSS if no unstable loci were
found. In the literature, a sample was defined as MSI
only when MSI-H was observed. LOH was determined
to be positive when the allelic ratio (AR ¼ T1:T2/
N1:N2) was <0.7, as used by Kobayashi et al. in a gas-
tric cancer study.27 Briefly, T1 and N1 represent the
highest respective peak areas of the shorter allele in
cancerous and normal mucosa samples, and T2 and
N2 the highest respective peak areas of the longer
allele. For cases in which AR was >1.0, the ratio was
inverted (1/AR) to obtain results in the range of 0.0–
1.0. Tumours exhibiting MSI at a given locus were not
evaluated for LOH.
Histological examination of gastric intestinalmetaplasia (GIM)
All slides were scored for GIM according to the upda-
ted Sydney system32 by a single physician (AT) who
was blinded to patient identity and treatment status.
Scores were given numerically as 0 for absence, and 1,
2 or 3 for mild, moderate or severe GIM, respectively.
The GIM score was assessed in the samples obtained
from the antrum, including from patients with
mucosal cancer at a different site in the stomach. GIM
scores were evaluated before and 1-year after treat-
ment for H. pylori.
Statistics
Statistical analyses were assessed using the Mann–
Whitney U-test, the Chi-squared test and Fisher’s
exact test. Statistical significance was defined as
P < 0.05.
RESULTS
Patient characteristics
Patient characteristics are shown in Table 1. Patients
in the early stages of cancer (group B) were older
than patients with chronic gastritis (group A)
(P < 0.005). Those undergoing EMR for gastric
cancer (group B1) were significantly younger than
those in group B2 (P < 0.005) and older than those
in group A, although this latter difference was not
significant.
Incidence of microsatellite instability (MSI) andloss of heterozygosity (LOH), in gastricintestinal metaplasia (GIM) and in the cancerarea before treatment
In group A, 4 of 39 (10%) patients with chronic gastri-
tis were positive for MSI in GIM. In group B, 15 of 53
(28%) were positive for MSI in GIM apart from the
cancerous lesions. The incidence of MSI in GIM was
significantly higher in group B than in group A (P ¼0.03). MSI in cancerous areas was detected 38% of the
time (20 of 53). The incidence of MSI in cancerous
areas was significantly higher than that in GIM in
group A (P < 0.005) (Table 2). Cancerous tissues from
11 of the 15 patients whose GIM lesions (at a different
area of the stomach) were positive for MSI were also
positive for MSI. The incidence of LOH in GIM from
groups A, B and cancerous areas were 10% (4 of 39),
6% (3 of 53) and 26% (14 of 53), respectively. There
was no significant difference in the incidence of LOH
Table 2. Frequency of MSI and LOH in patients withchronic gastritis and gastric cancer
GroupSamples(N)
MSI LOH
No. ofpatients (%)
No. ofpatients (%)
Group A GIM (39) 4 (10.3)a,b 4 (10.3)c
Group B GIM (53) 15 (28.3)a 3 (5.7)d
Cancerarea (53)
20 (37.7)b 14 (26.4)c,d
MSI, Microsatellite instability; LOH, loss of heterozygosity;GIM, gastric intestinal metaplasia; aP < 0.05; bP < 0.05;cP < 0.01; dP < 0.005.
GENET IC INSTABIL IT IES IN INTEST INAL METAPLASIA 197
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

in GIM between group A and group B, although the
incidence of LOH in cancerous lesions was signifi-
cantly higher than that in GIM from both group A and
group B (P < 0.01 and P < 0.005, respectively)
(Table 2).
Changes of microsatellite instability (MSI) andloss of heterozygosity (LOH) after eradication ofHelicobacter pylori
The incidence of MSI and LOH in GIM prior to
treatment was 10% (4 of 39) and 10% (4 of 39) in
group A and 24% (6 of 25) and 0% (0 of 25) in
group B1, respectively (Figures 2 and 3). There were
no significant differences in the incidence of MSI
and LOH between group A and group B1. The fre-
quency of MSI significantly declined from 10% to
3% (1 of 39) in group A, and from 24% to 4%
(1 of 25) in group B1 (P < 0.05). Interestingly, the con-
dition of four patients with MSI before eradication
changed to being microsatellite stable after H. pylori
therapy, although one patient showed MSI after
treatment in group A (Figure 2a). In the patients
from group B1, similarly, all six cases who exhibited
MSI before H. pylori treatment were negative for
MSI after treatment. One subject who had previously
been negative for MSI became positive for MSI after
treatment (Figure 2b). LOH changed from 10% to
5% (2 of 39) in group A and from 0% to 12% (3 of
25) in group B1, neither of which was significantly
different. Four patients with LOH before eradication
of H. pylori became negative for LOH after, whereas
two patients demonstrated LOH after treatment in
group A. Three individuals who were negative for
LOH before treatment became positive for LOH after
eradication (Figure 3).
Changes in the gastric intestinal metaplasia(GIM) score after eradication of Helicobacterpylori
All GIM examined in this study were diagnosed as the
incomplete type via H&E staining. In groups A and
B1, the median GIM scores before and after treatment
of H. pylori were 2.0 (range 1–3) and 2.0 (range 1–3),
respectively. Interestingly, mean GIM scores were sig-
nificantly higher in group B1 than in group A before
H. pylori therapy (P < 0.05, by Mann–Witney U-test)
but did not show a significant decline for either group
1 year after treatment.
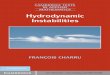
a
b
Positive
Negative
After(n=1)
Before(n=4)
Eradication (n=39)
After(n=1)
Before(n=6)
Eradication (n=25)
Positive
Negative
Figure 2. Changes in microsatellite instability (MSI) areshown in group A (a) and B1 patients (b) before and afterHelicobacter pylori (H. pylori) eradication. The incidenceof MSI declined after H. pylori eradication in both thegroups, with a significant decrease in group B1 (P < 0.05).MSI detected before treatment disappeared after treatmentof H. pylori infection. However, two patients became pos-itive for MSI after treatment, one with chronic gastritis (a)and the second with gastric cancer (b).
198 A. TANAKA et al.
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

DISCUSSION
This is the first study to examine alterations in genetic
instability in H. pylori-related GIM in patients with
and without gastric cancer before and after H. pylori
treatment. Although the decline in gastric cancer risk
after treatment for H. pylori infection has been defined
in retrospective33 and prospective studies,34 changes in
the mechanism underlying H. pylori-associated gastric
carcinogenesis following eradication remain unclear.
In the present prospective study with 1-year follow-
up, we clearly demonstrate that H. pylori eradication
did not significantly improve GIM histologically but
did change the molecular behaviour as evidenced by
the reversion of genetic instabilities.
Microsatellite instability is a mutation phenotype
that occurs through defects in DNA mismatch repair
system in cells. The condition contributes to the gen-
eration of cancer by inducing mutations in some can-
cer-related genes.35 The separation of MSI into the
two categories of MSI-H and MSI-L or MSS is partic-
ularly important because these may arise via different
mechanisms. Leung et al. reported that MSI was detec-
ted in 27% of gastric cancers and in 9% of GIM tis-
sues, including those in patients with and without
cancer.18 In addition, MSI in GIM was more readily
detected in individuals with MSI-H tumours than in
those with MSS or MSI-L tumours.18 Because of this,
MSI is considered to play an early and significant role
in gastric carcinogenesis. Our results revealed that MSI
in GIM was detected at significant levels in patients
with gastric cancer more often than in those without
cancer. The frequency of LOH in intestinal-type gastric
cancer has been reported to be approximately 20–
40%, although a variation in the LOH rate was
observed in microsatellite markers investigated.22–26
Our data on the frequency of LOH were similar to
those of the previous reports. On the contrary, no sig-
nificant difference was found in LOH rate in GIM in
patients with and without gastric cancer. Given this, it
is evident that MSI, but not LOH, detected in GIM may
define a subset of individuals who are particularly sus-
ceptible to gastric cancer.
On the contrary, several investigators have reported
widely varying frequencies (5–46%) of MSI associated
with gastric cancer as well as GIM with and without
gastric cancer.36–38 There are several possible explana-
tions for these discrepancies. First, the findings may
be explained by the methods used for DNA extrac-
tion.21 The laser capture microdissection that we used
After(n=3)
Before(n=0)
Eradication (n=25)
Positive
Negative
Positive
Negative
After(n=2)
Before(n=4)
Eradication (n=39)
a
b
Figure 3. Changes in loss of heterozygosity (LOH) areshown in groups A (a) and B1 patients (b) before andafter Helicobacter pylori eradication. LOH detected beforetreatment disappeared after eradication in group A.However, two patients became positive for LOH aftertreatment in group A. In contrast, LOH appeared post-eradication and was not present before treatment in groupB1.
GENET IC INSTABIL IT IES IN INTEST INAL METAPLASIA 199
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

in this study allows the procurement of relatively pure
tumour cell populations from complex heterogeneous
cell mixtures.39 Therefore, the specificity of genetic
alterations in DNA extracted selectively from the area
is considered to be higher than that in the hand-
microdissected samples.40 Second, when assessing
tumours for the presence of MSI and LOH, many
investigators differ as to which and how many loci
should be analysed.20,21 Third, the methods used to
analyse MSI and LOH affected the outcome. When
conventional methods are used, the electrophoresis
profiles of PCR products may not always be reprodu-
cible.14,41 Moreover, the assessment of MSI, especially
minor patterns, using an autoradiograph is difficult, as
has been reported previously,14,15,41 with non-specific
stutter bands, seen as small fragments, often making
autoradiographs difficult to interpret and quantitate.
When all these facts are taken into consideration, it is
clear that HFRMA used in our study is superior to the
conventional method used to date.
Some reports indicated that older subjects were
more likely to experience GIM progression with a per-
sistent H. pylori infection than younger patients.42–44
Indeed, average age in the present study was signifi-
cantly higher in group B than in group A (P < 0.05).
We demonstrated that GIM in group B was in a more
advanced stage than GIM in group A. Hence, our find-
ings support the postulate that GIM grade develops
sequentially over a period of decade.7 In addition, the
severity of GIM is significantly higher in patients with
cancer than in those without cancer (group A) prior to
treatment. This finding is in agreement with Correa’s
model that intestinal-type gastric cancer arises via
GIM.6,7 Although there have been many investigations
into changes in GIM after the eradication of H. pylori,
results have been conflicting, with some reporting that
the histological grade of GIM decreased after eradica-
tion while others found no change. Several factors
have been proposed to explain the differences: incon-
sistent interpretation in histological grading, sampling
errors and different study populations.45 After 1 year,
we found that there was no significant histological
improvement in GIM, although the score was based on
the result of a single biopsy sample that was subject to
sampling error.
It has been reported that molecular changes, i.e.
mutations of the p5346,47 or K-ras genes,48,49 in
patients with H. pylori-related gastritis after eradica-
tion do occur. To our knowledge, however, analyses of
genetic instabilities in GIM, a precancerous lesion,
before and after H. pylori treatment in a single patient
have not been reported. Our result shows that the
elimination of DNA damage, characterized by MSI,
may be more important in the prevention of gastric
cancer than the actual reversal of GIM.45 In the pre-
sent study, MSI detected before treatment disappeared
after treatment of H. pylori infection. However, two
patients became positive for MSI after treatment, one
with chronic gastritis and the second with gastric can-
cer. Those lesions may have passed the ‘point of no
return’.34 Wong et al. has reported that the eradication
of H. pylori did not decrease the development of gas-
tric cancer in participants with precancerous lesions
such as gastric atrophy, intestinal metaplasia or gastric
dysplasia by a prospective, randomized, placebo-con-
trolled, population-based study.34 In contrast to their
report, our results may provide an important clue to
the pathogenesis of the observed reduction of gastric
cancer following H. pylori eradication even in patients
with precancerous lesions such as GIM. Recently, it
has been reported that promoter hypermethylation of
hMLH1, a mismatch repair gene, is associated with
gastric cancer in premalignant lesions with MSI.31,50,51
Thus, investigation may be required on changes in
epigenetic alterations in other genetic markers in the
same patients.
In conclusion, the results of this prospective study
suggest that MSI in H. pylori-related GIM plays a role
in the early events leading to gastric carcinogenesis.
Helicobacter pylori eradication reduced MSI during the
1-year post-treatment period, although no histological
improvement in GIM was observed. Hence, patients
with precancerous lesion such as GIM should be trea-
ted and cured of their H. pylori infection. Further
investigation is required using a larger series of sam-
ples with a longer term follow-up to determine the
possible role of H. pylori-associated GIM as a precan-
cerous lesion.
ACKNOWLEDGEMENTS
No external financial support was received for this
study. The authors would like to thank Ms. H. Suzuki
for providing the tissue specimens.
200 A. TANAKA et al.
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

REFERENCES
1. Correa P, Fox J, Fontham E, et al. Heli-cobacter pylori and gastric carcinoma:
serum antibody prevalence in popula-
tions with contrasting cancer risks. Can-
cer 1990; 66: 2569–74.
2. Shipponen P, Hyvarinen H. Role of
Helicobacter pylori in the pathogenesis
of gastritis, peptic ulcer and gastric can-
cer. Scand J Gastroenterol Suppl 1993;
196: 3–6.
3. Infection with Helicobacter pylori. In:
IARC monographs on the evaluation of
the carcinogenic risks to humans. Vol.
61. Schistosomes, liver flukes and Heli-cobacter pylori. Lyon, France: Interna-
tional Agency for Research on Cancer,
1994: 177–240.
4. Graham DY. Helicobacter pylori infec-
tion is the primary cause of gastric can-
cer. J Gastroenterol 2000; 35: 90–7.
5. Uemura N, Okamoto S, Yamamoto S,
et al. Helicobacter pylori infection and
the development of gastric cancer.
N Engl J Med 2001; 345: 784–9.
6. Correa P, Shiao YH. Phenotypic and
genotypic events in gastric carcinogene-
sis. Cancer Res 1994; 54: 1941s–3s.
7. Correa P. Helicobacter pylori and gastric
carcinogenesis. Am J Surg Pathol 1995;
19: S37–43.
8. Correa P. A human model of gastric
carcinogenesis. Cancer Res 1988; 48:
3554–60.
9. Filipe MI, Munoz N, Matko I, et al.
Intestinal metaplasia types and the risk
of gastric cancer: a cohort study in Slo-
venia. Int J Cancer 1994; 57: 324–9.
10. Miehlke S, Hackelsberger A, Meining A,
et al. Severe expression of corpus gas-
tritis is characteristic in gastric cancer
patients infected with Helicobacterpylori. Br J Cancer 1998; 78: 263–6.
11. Loeb LA. Mutator phenotype may be
required for multistage carcinogenesis.
Cancer Res 1991; 51: 3075–9.
12. Lee HS, Lee BL, Kim SH, et al. Microsat-
ellite instability in synchronous gastric
carcinomas. Int J Cancer 2001; 91:
619–24.
13. Tokunaga E, Oki E, Oda S, et al. Fre-
quency of microsatellite instability in
breast cancer determined by high-reso-
lution fluorescent microsatellite analy-
sis. Oncology 2000; 59: 44–9.
14. Oda S, Oki E, Maehara Y, et al. Precise
assessment of microsatellite instability
using high resolution fluorescent
microsatellite analysis. Nucleic Acids
Res 1997; 25: 3415–20.
15. Shibata N, Watari J, Fujiya M, et al. Cell
kinetics and genetic instabilities in dif-
ferentiated type early gastric cancers
with different mucin phenotype. Hum
Pathol 2003; 34: 32–40.
16. Semba S, Yokozaki H, Yamamoto S,
et al. Microsatellite instability in pre-
cancerous lesions and adenocarcinomas
of the stomach. Cancer 1996; 77: 1620–
7.
17. Ottini L, Palli D, Falchetti M, et al.
Microsatellite instability in gastric can-
cer is associated with tumor location
and family history in a high-risk popu-
lation from Tuscany. Cancer Res 1997;
57: 4523–9.
18. Leung WK, Kim JJ, Kim JG, et al.
Microsatellite instability in gastric intes-
tinal metaplasia in patients with and
without gastric cancer. Am J Pathol
2000; 156: 537–43.
19. Kashiwagi K, Watanabe M, Ezaki T,
et al. Clinical usefulness of microsatel-
lite instability for the prediction of gas-
tric adenoma or adenocarcinoma in
patients with chronic gastritis. Br J Can-
cer 2000; 82: 1814–8.
20. Jin Z, Tamura G, Satoh M, et al.
Absence of BAT-26 instability in gastric
intestinal metaplasia. Pathol Int 2001;
51: 473–5.
21. Garay J, Bravo JC, Correa P, et al. Infre-
quency of microsatellite instability in
complete type and incomplete gastric
metaplasia. Hum Pathol 2004; 35: 102–
6.
22. Choi SW, Park SW, Lee KY, Kim KM,
Chung YJ, Rhyu MG. Fractional allelic
loss in gastric carcinoma correlates with
growth patterns. Oncogene 1998; 17:
2655–9.
23. Choi SW, Choi JR, Chung YJ, Kim KM,
Rhyu MG. Prognostic implications of
microsatellite genotypes in gastric carci-
noma. Int J Cancer 2000; 89: 378–83.
24. Tamura G, Sato K, Akiyama S, et al.
Molecular characterization of undiffer-
entiated-type gastric carcinoma. Lab
Invest 2001; 81: 593–8.
25. Kim KM, Kwon MS, Hong SJ, et al.
Genetic classification of intestinal of
intestinal-type and diffuse-type gastric
cancers based on chromosomal loss and
microsatellite instability. Virchows Arch
2003; 443: 491–500.
26. Jiao YF, Sugai T, Habano W, Suzuki M,
Takagane A, Nakamura S. Analysis of
microsatellite alterations in gastric car-
cinoma using the crypt isolation tech-
nique. J Pathol 2004; 204: 200–7.
27. Kobayashi K, Okamoto T, Takayama S,
Akiyama M, Ohno T, Yamada H. Genetic
instability in intestinal metaplasia is a
frequent event leading to well-differen-
tiated early adenocarcinoma of the
stomach. Eur J Cancer 2000; 36:
1113–9.
28. Li YL, Tian Z, Wu DY, Fu BY, Xin Y.
Loss of heterozygosity on 10q23.3 and
mutation of tumor suppressor gene
PTEN in gastric cancer and precancer-
ous lesions. World J Gastroenterol 2005;
11: 285–8.
29. Japanese Research Society for GastricCancer. The general rules for gastric
cancer study, 12th edn. Tokyo: Kinbara
Publication, 1993.
30. Lauren P. The two histological main
types of gastric carcinoma: diffuse and
so-called intestinal type carcinoma. An
attempt at a histo-clinical classification.
Acta Pathol Microbiol Scand 1965; 64:
31–49.
31. Boland CR, Thibodeau SN, Hamilton SR,
et al. A National Cancer Institute Work-
shop on Microsatellite Instability for
cancer detection and familial predispo-
sition: development of international cri-
teria for the determination of
microsatellite instability in colorectal
cancer. Cancer Res 1998; 58: 5248–57.
32. Dixon MF, Genta RM, Yardley JH, et al.
Classification and grading of gastritis.
The updated Sydney System. Interna-
tional Workshop on the Histopathology
of Gastritis, Houston 1994. Am J Surg
Pathol 1996; 20: 1161–81.
33. Uemura N, Mukai T, Okamoto S, et al.
Effect of Helicobacter pylori eradication
on subsequent development of cancer
after endoscopic resection of early gas-
tric cancer. Cancer Epidemiol Biomark-
ers Prev 1997; 6: 639–42.
34. Wong BC-Y, Lam SK, Wong WM, et al.
Helicobacter pylori eradication to pre-
vent gastric cancer in a high-risk region
of China: a randomized controlled trial.
JAMA 2004; 291: 187–94.
35. Loeb LA. Microsatellite instability: mar-
ker of a mutator phenotype in cancer.
Cancer Res 1994; 54: 5059–63.
36. Halling KC, Harper J, Moskaluk CA,
et al. Origin of microsatellite instability
in gastric cancer. Am J Pathol 1999;
155: 205–11.
GENET IC INSTABIL IT IES IN INTEST INAL METAPLASIA 201
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd

37. Kang GH, Shim YH, Ro JY. Correlation
of methylation of the hMLH1 promoter
with lack of expression of hMLH1 in
sporadic gastric carcinomas with repli-
cation error. Lab Invest 1999; 79: 903–
9.
38. Fleisher AS, Esteller M, Wang S, et al.
Hypermethylation of the hMLH1 promo-
ter in human gastric cancers with
microsatellite instability. Cancer Res
1999; 59: 1090–5.
39. Bonner RF, Emmert-Buck M, Cole K,
et al. Laser capture microdissection:
molecular analysis of tissue. Science
1997; 278: 1481–3.
40. Dillon D, Zheng K, Costa J. Rapid, effi-
cient genotyping of clinical tumor sam-
ples by laser-capture microdissection/
PCR/SSCP. Exp Mol Pathol 2001; 70:
195–200.
41. Cawkwell L, Li D, Lewis FA, et al.
Microsatellite instability in colorectal
cancer: Improved assessment using
fluorescent polymerase chain reaction.
Gastroenterology 1995; 109: 465–71.
42. Sung JJY, Lin S, Ching JYL, et al. Atro-
phy and intestinal metaplasia one year
after cure of H. pylori infection: a pros-
pective, randomized study. Gastroenter-
ology 2000; 119: 7–14.
43. Sakaki N, Kozawa H, Egawa N, et al.
Ten-year prospective follow-up study
on the relationship between Helicobact-er pylori infection and progression of
atrophic gastritis, particularly assessed
by endoscopic findings. Aliment Phar-
macol Ther 2002; 16: 198–203.
44. Asaka M, Sugiyama T, Nobuta A, et al.
Atrophic gastritis and intestinal meta-
plasia in Japan: results of a large multi-
center study. Helicobacter 2001; 6:
294–9.
45. Leung WK, Sung JJ. Review article:
intestinal metaplasia and gastric carcin-
ogenesis. Aliment Pharmacol Ther 2002;
16: 1209–16.
46. Hibi K, Mitomi H, Koizumi W, et al.
Enhanced cellular proliferation and p53
accumulation in gastric mucosa chron-
ically infected with Helicobacter pylori.Am J Clin Pathol 1997; 108: 26–34.
47. Jones NL, Shannon PT, Cutz E, et al.
Increase in proliferation and apoptosis
of gastric epithelial cells early in the
natural history of Helicobacter pyloriinfection. Am J Pathol 1997; 151:
1695–703.
48. Gong C, Mera R, Bravo JC, et al.
KRAS mutations predict progression of
preneoplastic gastric lesions. Cancer
Epidemiol Biomarkers Prev 1999; 8:
167–71.
49. Hiyama T, Haruma K, Kitadai Y, et al.
K-ras mutation in Helicobacter pylori-associated chronic gastritis in patients
with and without gastric cancer. Int J
Cancer 2002; 97: 562–6.
50. Kang GH, Shim YH, Jung HY, et al. CpG
island methylation in premalignant
stage of gastric cancer. Cancer Res
2001; 61: 2847–51.
51. To KF, Keung WK, Lee TL, et al. Promo-
ter hypermethylation of tumor-related
genes in gastric intestinal metaplasia of
patients with and without gastric can-
cer. Int J Cancer 2002; 102: 623–8.
202 A. TANAKA et al.
ª 2006 The Authors, Aliment Pharmacol Ther symp ser 2, 194–202
Journal compilation ª 2006 Blackwell Publishing Ltd