Embed Size (px)
Citation preview

ORIGINAL RESEARCH ARTICLE l'toar~e<:>no<rOco 6 (~). 4(>4-411 . I_ II 7O-76'10194t1Xli , .04:>41 SOl.00J0
Economic Evaluation of Immunoprophylaxis in Children with Recurrent Ear, Nose and Throat Infections Kurt Banz,i David Schwickerl and A/me Marie Thomas2
HealthEcon, Health Care Consultants, Sasle, Switzerland 2 Pierre Fabre Medicament, Castres, France
Summary This study compares the costs of immunoprophylaxis versus no immunoprophylaxis in children with recurrent ear, nose and throat (ENT) infections (otitis media and rhinopharyngitis) using ribosomal immunotherapy (" RibomunyJ'). The per-patient cost of ribosomal immunotherapy (FF297) is offset by direct savings garnered through the prevention of many acule infectious episodes. The net6-month per-patient savings associated with immunoprophyJaxis range from FF272 to FFI704, depending on the indication and the type of treatment-cost estimate. Saved heahhcare resources include physician consultations and visits, laboratory tests, medicotechnical services (audiometric tests) and antibiotic ther· apy. Sensitivity analysis of efficacy and treatment-cost estimates enabled threshold ranges of incremental efficacy to be identified. Cost-equivalence between the 2 treatment options was found to exist when the incremental efficacy of immunoprophylaxis lay between 7.4 and 17.5% (recurrent otitis media), and between 8.9 and 26.1 % (recurrent rhinopharyngitis). Thus, even when clearly lower incremental efficacy rates than those reported in controlled clinical trials (approximately 40 to 60%) are assumed, ribosomal immunotherapy can still be expected to be cost effective. An analysis of the perspectives of the various payers in the French healthcare system demonstrated that net savings occurred for all payers involved. However. social security insurance would gain most from an immunoprophyJaxis programme. Based on the evidence presented here for France. physicians and payers should give increased attention to this treatment option.
Respi ratory tract infections are among the most
commonly reported diseases in children,]I -4) with
most episodes occuring duri ng the winter months.
In childhood, recurrent ear, nose and t hroat (ENT)
infections. particularly rhi nopharyngitis and otitis,
represent a major public health problem because of their prevalence and the risk of sequelae.!S.6l T he
freque ncy of these infect ions decreases as the im
mune system matures, peaki ng at age 2 years and
falling rapidly after age 7 yearsP·81 As these diseases
arc associated with substantial utilisation of health
care resources, and constitute an imponant cause
of parental absenteeism from work, they can be
expected to have a considerable economic impactJ 91
Generally, recurrent ENT infections are defined
as 3 or more acute episodes occurri ng w ithin a 6-
month time period,I7. 101 w ith up to 10 episodes
during I season having been observed.l8l Most of
these infect io ns are caused by bacterial patho
gens)3J and are therefore often successfu ll y treated

Immunoprophylaxis Against ENT Infedion
with antibiotics. However. with a risi ng number of such acute episodes. there is an increasing risk of complications and major sequelae. The long term risks in children suffe ri ng from recurrent otitis media incl ude structural middle c ar damage. entaili ng partial or permanent hearing loss as we ll as impairment of speech and language. and cogniti ve or psychosoc ial disorders. 1111
An alternative to treating repealed attacks is to prevent them through immunostimulalOry therapy. The primary c linical rational e for preven tion is the avoidance of di scomfort and, addi tionally. improvement of the long term prognosis for children who experience recurrent ENT infections. Ribosomal immunotherapy ('Ribomunyl'), which stimulates immun ity against recurrent ENT infections, contains 2 biologically acti ve fractions: ribosomes from 4 bacterial strains (StreptocoCClls pnell
mO/lioe, S. pyogenes. K lebsiella pllelllllO/liae and Haelllophi/l1$ infl"ellwe), and proteoglycans extracted from K, pllelllllolliae. In ill vilro and ill !'ivo
pharmacological studies, treatment with ribosomal immunotherapy appeared to stimulate both speci fi c and nonspecific immune rnechani sms.112. 14) In children with recurrent otit is media and rh inopharyngitis, clin ical trials have demonstrated that ribosomal immunot herapy s ignificantl y reduces the number of episodes of acute respiratory infections.17.8.I0,1 S· 181
However. clinical practice shows that prophylaxi s against recurrent ENT infections is not employed a s freque ntly as might be expected,l19) even though pat ient selection criteria. based on the number of infectious episodes,!1,8.101 a re re latively clear cut. Reasons fo r this include the fact that even after immunoprophylaxis. acu te i nfectious e pisodes still occur. albeit with reduced frequency. Connected to this is the genera l prob lem of reproducing results from controlled cli nical trials in routine practice. leading to some uncertainty concerning the achievable effi cacy. Furthermore, physic ians may feel that prophylaxis of these recurrent infections is not worthwhile, preferring instead to treat acu te epi sodes when they occur. This stems from the view that acute episodes are readily man-
465
aged. arc not life-threatening. and decrease in frequency with advancing age.
Considering the epidemiology of recurrent ENT in fections. the frequency of acute infect ious episodes in children and the potential for long term sequelae. these arguments agai nst prophylaxi s would appear to be economically quest ionable. 191
Overall. it seems that the economic importance of recurrent ENT infections and of the impact of immunoprophy laxi s is under-recognised. To our know ledge, the economics of preventive therapy in thi s fie ld have not been systematically in vesti gated. in contrast to many other prominent interventions and immuni sation programmes.120-231
Thus, this study was undertaken to compare the costs of 2 treatment options: immunoprophy lax is of recurrent ENT infections. using 'Ribom unyl', versus no immunoprophylax is.
Methods
Evaluation Framework:
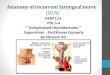
Because children with recurrent ENT infections experience acute episodes main ly during the winter. a time horizon of 6 winter months was chosen. Th is was in keeping with the design of most of the cl inical studies of ribosomal immunotherapy. and wi th the recommended treatment period. Each acute episode can lead to direct healthcare resource util isation. as well as productivity losses (fig. I). Thermal cu res1 represent an exception . as they arc not directl y related to the occ urrence of an acute episode but are prescribed to chi ldren wi th diagnosed recurrent ENT in fec tions as u general treatment.
In this contex t, the objective of this economic analysis is to invest igate whether prophylaxis wi th ribosomal immunotherapy is capable of offsetting its overall direct COStS by creating savings in other
A thennal cure is a course of lTeaunenlthallllkes advan· tage of the special propcn ies of mineral waters administered in a spa. This specia lised treatment is used for diseases s uch as ENT disorders. dermatoses and rheUlllatism. Because it is nOt usually available locally. patients are normally required to travel in order to rece i"e it.

ProductlV1ty
""
&uz tt al.
Q V
Ambula!ory services *
Fig. 1. Direc! and indirect effects 01 chronic ear, nose and throa! infections that intluence the economic evaluation 01 a prevention programme. SymOoI: ' denotes physician consulta tions andiorviSits, medicotechnical services, labora!ory services and ambulalory surgical interventions.
economicall y relevant areas . Such areas include the cOSts of ambulalOry services (e.g. physician consultations, laboratory and medicotechnical ser· vices), antibiOlics, hospitalisation. and indirect costs. The economic methodology used i s in accordance with the s tandards developed by Weinstei nl201 fo r thc economic evaluation of preventive interven· tions . The basic principle is to consider all eco· nomi c costs of prevention and thcn weigh these costs agai nst the resultant economic sav ings.
This study uses decision analysis to assess the economic impact of treating patients with ribo· somal immunotherapy as compared with no inter· vention. defined as placebo treatment or as comparable reference periods without p rophylax is. In this sense. each of the possible Ireatments of an acute infectious episode shown in fi g. I, e.g. ambu latory services or hospitali sation, characterise a specific pattern of healthcare resource utilisation and costs. The arrows represent the probabili ties with which these treatments are used in the event of an acute
episode. This eval uation framework was constructed for each of the 2 indications studied, rec urrent oti tis media and rhinopharyngitis in children.
Economic Parameters and Qualitative Considerations
Direct and indirect costs and savings were taken into accou nt . Di rect costs and sav ings include am· bulatory physician services, laboratory tests, medico· technical services. antibiotic therapy, concomi tant medication, surgi cal intervent ions. hospita li sa· lions and thermal cures. Indirect costs and savings are incurred when parents take t ime off work to care for thei r sick children.
However, major differences exist in the availabili ty a nd quality of data concerning the various cost parameters mentioned above. Whereas the in· format ion on the frequency and costs of physician consultations and visi ts. laboratory tests, medico· technical services and antibiotic therapy is deemed to be reliable, on ly sparse and inconsistent data are

Immunoprophylaxis Against ENT Infection
available fo r concomitant mcdication. surgical interve ntions (ambulatory and inpatient ). thermal cures and loss of parental productiv ity. Toall ow for thcse di fferences. a multiple step analysis was performed to avoid combining convincing data with less accurate and reliable informat ion. In the core analysis. only those direct econom ic parameters are taken inlO account where reliable data were obtainable. The remaining di rect cost factors (concomitant medication, s urgical interventions and thermal cures) as wcll as indirect costs (parental absenteeism from work) arc discussed separately in the ex/elJ(/el/ llllafysis. The analyses arc based on the therapeutic and economic env ironmen t in France. us ing 1993 costs.
Sensitiv ity analysis on the incremental efficacy of immuooprophylaxis compared with n o immunoprophylaxis. defi ned as the percemage reduct ion in the number of acute episodes over a 6-month time horizon. was perfo rmed. The sensiti vi ty analysis was done to investigate the economic effects of ribosomal immunotherapy over the wide range of therapcuticoutcomes that may be observed in daily practice. Consequently. study resu lt s are presented relat ive to the incremental effi cacy of immunoprophylax is. ranging between 2 hypothetical exIremes of zero ( product does not work) and 70% (the maxi mum reduction in infectious episodes observed with ribosomal immunOlherapy in clinical stud ies). Threshold values for the incremental effi cacy of ribosomal immu notherapy were calculated t o identi fy the point of cost-equ ivalence for the 2 treatment options. A further crucial aspect and, therefore. subject to sensi tiv ity analysis. is di sease severity. ex pressed as the number of infectious ep isodes assumed 10 occur during the 6-month study period.
Clinical Data
Table I summari ses the relevant clinical studies wit h ribosomal immunotherapy (' Ribomunyl' ), which prov ide information on clinical efficacy and key economic parameters in children. In all studies. ribosomal immu notherapy was given orall y accordi ng to the manufac turer 's recommended
C Adis tntematIonoI UrriIed. AI rlghls fe5(KVlKl
46'
dosage. i.e. 3 tablets (or I sachet) daily as a single dose on 4 days per week for 3 weeks. followed by maintenance therapy with 3 tablets on 4 days per month for the next 5 months.
Patients enrolled in these studies suffered from various ENT infect ions, includi ng recurrent otitis media and rhinopharyngitis. yet study resul ts were generally not stratified according to these different conditions. This could be considered a li mi tation for the economic st udy. in which each ind ication (recurrent otiti s media and rhinopharyngitis) is an· alysed separately. However, Hill s and colleagues18l
reported that the frequency of ac ute infec tious episodes was not substantially influenced by the type of infection studied ; thus. this limitation may not be important.
Table I indicates that the mean number of acute infectious episodes ranged between 5.6 and 8.3 in patients who did not receive r ibosomal immunotherapy. Possi ble explanations fo r this range incl ude interst udy differences with respect to patient age. disease severity. study location (urban I'S rural). climatic conditions during the study period (cold or mi ld wi nter). and the soc ial environment (day nursery, school or home care). all of which are considered to affect the incidence of acute episodes. We have based our calcul ations o n an average of 6.5 acute infectious episodes during a 6-mon th period for ch ildren with recurrent oti tis media and rhinopharyngitis who do not receive ribosomal immunotherapy (best esti mate value). Children who were treated experienced a significant reduction in the frequency of these infections, between 39 and 65% in 6-month trials. From these data. a standard incremental efficacy of immu noprophylaxis of 50% was defi ned for use as the best estimate. Le. il is assumed thai ribosomal immunotherdpy is, on average. capable of halvi ng the num ber of acute infec tious episodes.
Resource Use and Cost Assessment
The cost evaluation of the 2 indications studied is based on the healthcare resource utilisation associated ~ith these diseases. The types and amount of healthcare goods and services rendered to patients

&lIIZ d al.
Table I. Comparison 01 efficacy and arllibiotic courses during ribosomat immunotherapy with 'Ribomunyl' (R), ptacebo period (P) Of relerence peroo (pre) in children with recurrent respiratrny infections (mainly otit is media and rhinopharyngitis)
Relerence No. 01 pat ients, Mean age of Study duration Average 00. of Average 00. Percentage of main diagllOSis patients (years) (months). inlections during of antibiotic infections treated
design study period courses with arllibiotics
2 p" 2.B4±O. 16 6 5.6 3.3 59
R" 3.09±O.18 r. db, pa 3.4 (39%) " 38 ENT infections
8 pre 492 5.6±2.7 ,,. 8.3 " 89 post 492 (R) pre/post 5.8 (30%) 2.6 " 0, RP, S
" P20 3.85 (3-5) 6 2.8 5.6 " R" 389 (3·5) r. db, pa 4.0 (49%) 2.0 50 O,RP
" P" 2 6 Not reported al 3.5 Not reported at 6 R53 r. db. pa 6 months 2.3 months O.RP
" pre 50 6.2 (1·13) 6 2.6 6.8 89 post 50 (R) pre/post 3.3 (57%) 3.0 " O,RP
" pre 137 up to 15 6 6.2 ' .8 " post 137 (R) pre/post 2.3 (63%) L2 52 O,RP
" pre 964 71% :s;15 6 6.6 5.0 " post 964 (R) 29% >15 pre/post 2.3 (65%) L6 20 O.RP.S , Ribosomal immunott1erapy duratioo ,,6 months, followed by an observation period of another 6 months.
AbtKeviatioos and symbols: db " double-blind: ENT infecuons " recurrent ear, nose, and throat infections: 0 " rBCllrrerll otitis med~: pa " parallel: pre/post" oomparison between reference period without prophylaxis (pre) and treatment period (post): r " randomise<!: RP " recurrent m i rlOpharyng~is: S" recurrent sinusitis: • " reported significant difference versus placebo or reference period (p < 0,05),
were primarily obtai ned from structured expert interviews using specific questionnaires. In total. I I face-to-face interviews with practisi ng physicians in France were conducted. Eight of Ihe II experts were resident physicians [3 otorhinolaryngology (OR L) specialists, 2 paediatricians. 2 general practit ioners (GPs) and I respiratory specialist], The remaining 3 were hospital physicians. Additional information on hea lt hertre resource usc. incl uding antibiotic treatment. concomitant medication, surgical interventions and thermal cures, was also derived from ribosomal immunotherapy cli nical studies. From these data. standard treatment algorithms were derived for each indication, reflecti ng the type and frequency of services rendered. Further data on antibiotic prescribing during acute ep isodes and concomitant medications were obtained from a representative prescriber survey and from pharmaceutical stati stics in France (1993).
o Adis intemolklnol limlted. AI rlghh re.erved
To manage observed differences in clinical outcomes, treatment algorithms and assoc iated healthcare costs, 3 main calcu lations for the core analysis were carried out. First, a 'best esti mate' calculation was done, representing acomb ination of parameter values that approximately reflect the current clini
cal and economic reality in France. From this best estimate, low and high esti mate calculations were
performed 10 provide a range of data based on ex
treme assumptions concerni ng healthcare resource use and costs,
Table II details the types and average frequency of goods and services (core analysis parameters)
associated with the treatment of a single acute infect ious episode of otitis media or rhi nopharyngitis. Fu rt her resource use data, which are discussed i n the extended analysis, are presented in table Ill.

lmmunoprophylaxi5 Against ENT Infection
Physician services, medicotechnical serv ices, laboratory tests and ambulatory surgica l in terventions were valued according to official fee -forservice tariffs, reimbursement codes and regulations set up by the French Ministry of Health,124[ and mu[tiplicd by the [993 code values. differen tiated by physician speciality [Caisse Nationale D' Assurance Maladie (CNAM) [993. personal communication]. Acqu isition costs of medication were ca[culated using the official pharmacy sales price [ist.l 251 Hospilalisation costs were based on the average length of stay (in days) multiplied by a standard hospital rate per day. Act ual figures on daily hospital rates for public and pri vate hospital s were obtained from the social security insurance (CNAM 1993. personal communication). In private hospitals, the above-mentioned tarift1 24 J applies in addition to the daily nile charged. The CNAM also prov ided exemplary cost figures for a thermal cure.
Indirect costs were valued by multiplying the number of day s off work by the average gross weekly earnings projected fo r 1993 as a proxy fo r the economic value of lost productivity.126.211
The cost of ribosomal immunotherapy comprises the acquisit ion cost of the drug only. as additional physic ian services for therapy initiation and subsequent controls are not necessary. Also.
469
adverse events leading to a possible further resource use. which would increase the total ribosomal immunotherapy costs, are rare and usually mild. Thus. additi onal costs due to adverse events which occur during ribosomal immunotherapy are considered negli gible. Following the treatment schedule outlined above. the per-patient costs for a 6-
month ribosomal immunotherapy course are FF297 (equivalent to $US53 at mean 1993 exchange rates).
For the core analysis, the results are presented in 2 ways:
• the incremental costs and savings associated with ribosomal immunotherapy;
• the total costs of the both treatment options divided into the costs to soc ial security insurance and to the patient or private insurers. The latter calculations take into accou nt the cur
rent reimbursement mechanism in France. where a proportion of the total cost (ticket moderaleur) is not reimbursed by socia l secu rity. Pat ients who choose to pay for complementary voluntary insurance (87% of the popul ation)(281 may reclaim a further proportion of Ihe tolal cost, normally the full amount of the ticket moderateur. Otherwise. the remainder must be paid by the patient. In cases of soc ial hardship. this copayment is waived (8.7% of the popu lation),l291
Tab le II . Type and average frequency 01 healthcare goods and services rendered to children with rl!<:un-ent infecbons 01 the upper respiratory tract. taken into account in the core analysis. The data relate to 1 acute inlectiotls episode
Rl!<:urrent o@smediainchildren
Ambulatory services
Physician services:
consuilatKmS/Visrts
Medicotl!<:hnical services: audiometric test
Laboratory services: bacteriologica l tests
Antibiotic therapY'
'Augmentin' (amoxicillinlctavulanic acid) 'A~atil' (celacbr) 'Cit>k)r' (amoxicillinlctavulanic acid) 'Pediazole' (erythromycin ethyl succinate)
'Oracelal' (cefadrox il)
Frequency of serv.:e
2.2
0.05
<0.05
0.'
RI!<:Ufrent rhinopharyngit is in chi ldren
Ambulatory services
PhySician services: consultationslvisrts
Laboratory services: bacteriological tests
Antibiotic therapY"
'Clamoxyl' (amoxicitl in )
'Augmentin' (amoxicillinfclavulanic aoo) 'Josocine' (josamycin) 'A~alil' (ce/aclo,) 'Oracefa l' (celadroxi l)
Frequency of
service
>'5
a Five most Irequently pmscribed antit>iotics in order of preSCliption frequency. Source : Prescriber survey in France, 1993.
C> Ad"lnTemoTional lJmiIOO. AJ rights reserved

470 &lIlzeta/.
Table III. Type and average frequency 01 hea~hcare goods and services rendered to children with recurrent inlecOOns of the upper respiratory tract as diSCUssed in the e~tl!rK!ed analysis. The data relate to the stlldied 6-lT\Of1th time horizon
Recurrent otitis media in children
Concomitant medication Anl~ussives
Anti-inflammatory drugs Local anaesthet ics Ant ihistamines
Surgical procedures' Paracentesis/myringotomy Drainage Adenoidectomy/amygdalectomy
Cures Thermal cure
frequency 01 service
0.5
0' 0.' 02
<0.05
Recurrent rIlinopharyng~is in ct1ildren
Concomitant medle8tlon Antitussive! Antihistamines Decongestants MliCQ/y1ics
Su rgical procedures'
Adenoidectomy/amygdalectomy
Cures Thermal cure
Frequency of service
0.5
0.2
0' a ParacenteSis/myringotomy is generally performed on an ambulatory basis. Drainage and adenoidectomylamygdalec1omy may require
hosp~alisation for 1 day.
Results
Totol Direct Treatment Costs of ENT Infections (Core Analysis)
The results presented in this secti on are concerned with the economic parameters of the core analysis. The effects of treatment with ribosomal immunotherapy on the less reliable cost p arameters. which are part of the extended analysis. are outli ned and discussed below.
The per-patient costs correspondi ng to the core resource use for I acute infectious episode are given as bestllowlhigh esti mates in table IV. Costs for medicotechnical services are ignored, as these are not chargeable in combinati on wi th a simultaneous consultation or visit. 124J The low and high cost estimates are calculated on the basis of recorded differences in t he physician's speciality and the type of services re ndered (ambu latory services); the type. dosage and frequency of use of antibacterial therapy (antibiotic therapy); and the type and frequency of laboratory tests performed (laboratory services).
Comparing the 2 indications. table IV shows a lower total cost estimate for an acute episode of rh inopharyngitis. which can be attributed to t he lower frequency or cost of services rendered in thi s indication. These data provide ev idence that utilisat ion of healthcare goods and services during
acute infectious episodes of the upper respiratory tract is substantial. part icularly when the high frequency of recurrences is taken into account.
Moreover. it should be borne in mind that these fig ures reflect conservative estimates. as only a limited number of direct cost parameters are considered.
Incremental Direct Costs and Savings Associated with Ribosomallmmunofherapy The economic impact of treatment with ribo
somal immu notherapy on the recurrent ENT infections studied is illustrated in figures 2 and 3. These figures show that 2 major factors influence the cost effecti veness of immunoprophylaxis. Fi rstly, as incremental efficacy increases, net incremental costs decrease until cost equivalence between the treatment options (immunoprophylaxis vs no immunoprophylax is) is attained (the threshold line). The poi nt of intersection determines the threshold incremen tal efficacy of ribosomal immunotherapy. Further rises in incremental efficacy result in net incremental savings per treated patient. Thus, a decrease in the nu mber of acute infectious episodes, as expressed by increasing incremental efficacy, is associated with savings in heaJthcare resources and associated direct costs.
Secondly, the magnitude of the cost savi ngs garnered through treatment with ribosomal immunotherapy is expressed by the differences in the slope
Phormocoeconomics 6(5) 1994

Immunoprophylaxis Against ENT Infection
of the 3 calculated cost estimates (bestlhigh/low). The higher the esti mated costs per acute infectious episode. the s teeper the slope of the line determining the net incremental costs or sav ings per patient. in relation to the incremental efficacy of immunoprophylaxis. The points of intersect ion of the low and high estimate lines with the threshold li ne th us demarcate the range of th reshold incremental effi cacy of ribosomal immunotherapy, in relation to the cost estimate chosen. in conclusion, i f in clinical practice an increme ntal effi cacy of prophylaxis higher than the documented maximum threshold value can be achieved, net d irect savi ngs per treated patient will resul t.
The s haded area in figures 2 and 3 represents the range of cost savings which can be achieved through immunoprophylaxis over a 6-month time period. dependi ng on the incremental efficacy of immunoprophylax is.
For otiti s medi a and rhinopharyngiti s, the i ncre· mental cost analysis demonstrates that ribosomal immunotherapy has clear potential to achieve net savi ngs over a period of 6 months, when the efficacy rates reponed in clinical studies arc considered (see table I). The cost ofribosomal immunotherapy is equal to the cost of no immunoprophylaxis when the former reduces the rate of acute infectious episodes by at least 17.5% (otitis media) or 26.1% (rhinopharyngiti s) in low esti mate cases. Since the incremental efficacy of immunoprophylaxis was between 30 and 65% in cli nical tr ial s, it may be assu med that ribosomal immunoprophylaxi s of rec urrent ENT infections is economically worthwhile, i.e. th is preventive treatment is ca-
471
pable of generati ng net per-patient savings in both indications.
Sensitivlfy Analysis Apart from the incremental efficacy of im
munoprophyl axi s and the magnitude of treatment costs per acute in fectious episode, the number of acute recurrences experienced duri ng a 6-month time period without preventive therapy is also crucial in determining the cost effect iveness of ribosomal immunotherapy treatment. Therefore, a 2-way sensitivity analysis on this central parameter and incremental efficacy of immu noprophylaxis was performed to determine the threshold incremental efficacy when the frequency of acute epi sodes was varied (table V). These ca lcu lat ions were based on the best estimate treatment costs. incremental efficacy values in cl inical practice hi gher than the threshold values are associated with net direct cost sav ings per treated patient. in recurrent otitis media, an average effi cacy of ribosomal immunotherapy of 50% is the poi nt of cost equivalence between the 2 treatment option s, for patients who experience 2 infections in a 6-month period.
Poyer Perspective of Study Results The different perspectives and cost shares taken
up by the vari ous possible payers, i.e. socia l security insurance, private insurer or the pat ient , are shown in table VI. Social security insurance covers between 35 and 70% of the costs of treatment. depending o n the types of services and medications rendered.
Table IV. Total per-patient cost estimates 01 hea~hcare resource use (in FF) for core analysis parameters. Oala relale to t acute inlectious episode
Parameter Ae<:urrenl OIrtis in ch ildren Recurrent rhil'lOpharyngitis in children
best estimate Iow--high estimate best estimate Iow--high estimate
Ambulatory services' 2;> 22()-308 170 150-210
Antibiotic therapy· " 4H02 " 25· t02
Laboratory services " 0-200 " 0200
Total 328 261-616 227 175-518 a Ambulatory services irlCtude phySician consultations and/or visits: costs are based on the f,equency 01 services rendered arn:llhe
physician speciality (general practitioner. paedialrician. otorhinolaryngology specia list. ,espiratory specialist),
b Costs ,elate to the type of antibiotics pres<:ribed. dosage and duration 01 treatment
e Adi$ lnlemolionol limited, AI lights ,eserved , PhormocoEc~6 (5) 1994

472
500
0
'" " E , -500 & ~ • ~ -"'00 < , m 0 < ~ -1500 • 8 ~ ~ - 2000
• ~ - 2500
- 3000
0
Area 01 net
Range 01, • threshold ~ : efficacy
1~4% 17.5%
'"
Area of net saving re5(J~s
50
Bml: e/ at.
Threshold
Low estimate case
Best est,mate case
HIgh estimate case
60 70
Incremental efficacy of vaccination (%)
Fig. 2. Incremental per-patient costs and savings of immunoprophylaxis with ribosomal immunotherapy versus no treatment in children with recurrent otitis media (based on a 6-mon\h t ime horizon and 6.5 acute inlectious episodes in untreated patients).
The data presented in tabl e V I are based on an
incremental efficacy of immunoprophylaxis of 50%, 6.5 acute episodes in 6 months (in patients who do not receive immunoprophylaxis) and the best estimate treatment costs, Using recurrent otitis media as an example, the results show that the social security's per-patient investment of FFlO4 in ribosomal immunotherapy (35% of FF297) leads to net direct savings for that institution of FF630 (FF1468 minus FF838). In contrast. the patients or their complementary insurance cover the majority of the ribosomal immunotherapy costs (65% = FFI93), while profiti ng only from a relatively small proportion of the overall direct savings (FF140 = FF666 mi nus FF526).
Therefore. under current reimbursement regulation s, social security insurance gains substantially from an immunoprophylaxis programme, whi le pa
tients and pri vate insurers profit only marginally. Nonetheless, using the assumptionsdescribcd above,
() Ad~ Inlemolionol lImiled. AJ rlghl'$ reoorved.
ribosoma l immunotherapy treatment of recurrent otit is media and rhinopharyngitis in chi ldren results in net savings for all payers involved .
Extended Analysis
The results of the core analysis discussed above included on ly those economic parameters for which rel iable data were obtainable. However, the evaluation framework includes a nu mber of further direct effects as well as indirect effects (fi g. I).
First, other medi cations arc often prescribed in addition t o antibiotic therapy. Based on the literature, pharmaceutical statistics, and information from the expert survey (see Resource Use and Cost Assessment), we estimated the frequency of patients receiving concomitant medication for symptomatic treatment of their ENT infections to be 50%, Approximate frequency and per-patient costs of concomitant medication for the 6-month period are indicated in tables II I and VII. Hu ls et a1.l 81
PhormocoEconorrics I;, (5) 191M

lmmunoprophylaxis Against ENT Infection
reported a reducti on of up to 35% in the need fo r concomitant medication in patients receivi ng ribosoma l immunotherapy. compared with patients who did not receive preventive treatment. Similarly. Perruchetl191 reported a reduct ion in medical treatment in 63% of patients who received ribosomal immunotherapy.
Second ly. su rgical procedures arc performed in a number of children with recurrent ot itis media and rhinopharyngitis. These interventions are gencraJly carried out in the ambulatory setting. but hospitali sation may be necessary in some cases. Costs for these procedures in ambu latory care amount to FFl 24 (paracentesis/myringotomy). FF372 (transtympanic drainage) and FF270 (adenoidectomyl amygda1cctomy). When performed in an inpatient setting. estimated costs increase to between FF900 and FF2200 (transtympan ic drai nage) and FF800 and FF2200 (adenoidectomy/amygdalectomy). based on a mean length of admission of 1 day. These data
500
- 2500
~ :
! Range 01 threshold ' efficacy
8.g% 26 ~~ %
473
depend on the type of hospital (private or public). However, considering the frequency of these surgical procedures, the mean 6-month per-patient costs are minimal, particularly when perfonned in ambulatory care (table VII). Lacommel15] reported fewer surgical interventions within a 3-lllonth treatment period in patients receiving ribosomal immunotherapy (4%) compared to patient s receiving placebo ( 17%).
Third, treatment of the ENT infections studied may also include thermal cures, which, from the viewpoint of prescription freq uency, playa relati vely important role in France. The cost of a thermal cure varies. dependi ng on the specialisation of the spa, the extra services rendered to the patient during his/her stay, the travel costs to and from the spa. etc. Determining the average cost of such treatment in France is practica((y impossible because of the wide variation i n services, applicable tari ffs and charges. The only common denominator
Low estImate case
Best eSllmate case
saVIng results
HIgh est,mate case
Incremental efficacy of vaccinal"'n (%)
Fig. 3. Incremental per-patient costs and savings 01 treatment with ribosomal immunotherapy versus no immunotherapy in children with recurrent rhinopharyng itis (based on 6-mooth time horizoo and 6.5 acute infectious episodes in untreated patients).
PhormocoEconomic$ /) (5) 191M

474
Table V. Two-way sef1siti~ily analysis to esla~ish the threshold incremental efficacy 01 ribosomal immunotherapy required to achieve cost equivalence, compared to no immur.oprophyfa~is. CalCIJ lations were based on best estimate treatment costs
No. 01 inlec\OouS episodes Threshold incremental efficacy 01
in 6 months (w~houl immunoprophylaxis (%) versus no
immunoprophylaxis) immunoprophylaxis
recurrent ot~is recurrent media m i nopharyng~is
" NAb NAb ,. " 66
3 30 .. • 23 33
5 18 " 6 " 22
7 13 " 8 " 16
9 10 " 10 9 13 a These data are provided for completeness only, as recurrent
disease is defined as :1 01" more infectious episodes in a 6-month peliod.
b Immunoprophylaxis is always more cosily than no immunoprophylaxis where only 1 acute inlectious episode occurs in
a 6·month period.
Abbreviation: NA = not assessable.
is the length of the cure, wh ich is set by law at 21 days. The COSI of a thermal cure in 1993 was. therefore, based on an exemplary case provided by the CNAM (persona l commu nication) a nd was calculated 10 be FF3365. Th is includes the costs for medical surveillance (FF420), extra serv ices (FF225), hydrotherapy (FFI300), bed and board (FF950) and travel (FF470). Table VII shows the estimated per-patient average thermal cure cost for the studied time horizon of 6 months, taking into account the prescription freq uency of thermal cures in both indications (see table Ill ).
Although not directly related to the occurrence of an acute episode itse lf, thermal cures appear to be less often prescribed in ribosomal immunotherapy-treated patients. Lacommel151 fou nd that 26% of placebo patients required a therma l cure. compared with only 10% in the Ireated group. The interpretation of thi s finding is that, with a reduced frequency and a milder course of acute ENT infections in immunised patients, physicians may
Blmz e/ ai,
tend to prescribe thermal cures less often. If this is the case, the resu ltant sav ings in the cost of thermal cures can be attributed to ribosomal immunotherapy.
Finally, indirect cost savings with ribosomal immunotherapy derive from a reduced need for parents to stay off work to care for their children during acute infectious episodes. Two studies show that parental productivity loss ranges on average from I to 2.5 days per acute ep isode. 19.lOl Thi s translates into approximate indirect costs of FF390 10 FF975. based on average 1993 gross week ly earnings of FF 1960. The reduced freq uency of acute recurrences associated with immunoprophylaxis thus correlates directly with indirect savings, which can be quite substantial considering the magnitude of direct costs and savi ngs.
In summary. all the above-mentioned addi tional direct and indirect effects of ribosomal immunotherapy can be assumed 10 further augment the cost effectiveness of ribosomal immu notherapy in recurrent ENT infections. The quality of the presently available data is. however. insu fficient to alIowa conclusive presentation of results for these parameters. Overall . the extended analysis indi cates that the resu lts of the core analysis are conservative estimates.
Discussion
The study found wide variation in the avai lability and quality of data concerning the various economic parameters relevant to the immunoprophylax is of children with recurrent ot itis media or rhinopharyngitis. To allow for these differences, a mu ltiple-step analysis (core and ex tended) was performed; this avoided combining convinc in g data with less acc urate and reliable information.
In both indications st udied, the core ana lysis demonstrated that prophy lax is with ribosomal immunotherapy was associated with substantial net direct savi ngs over 6 months. Overall . the net savings of immunoprophylaxis, at a set incremental efficacy rate of 50% and assuming an average of 6.5 acute infectious episodes during a winter season, are calculated to range between FF272 and
PhormocoEconomics 6(5) 1994

Immunoprophy!axis Against ENT Infection 475
Table VI. Total6·month treatmeot costs Iwith or without ribosomal immunotherapy (Rll per patent (in FF) and the cost share pa>d by the social secUlity and that pa>d by the patient or plivate insurer. These data assume a mean lff~Quency 016.5 inlectious episodes and a mean
incremental efficacy 01 50%
Cost factors Percentage 01 Totaf core treatment costs Costs reimbursed by Costs Iell to patient or
costs reimoorsed (6 months' treatment) social security private insurer
by social security wilh R
Recurrent otitis media
Cost 01 physic~n services " 835
CoSI 01 laboratory services 60 33
Cost of antibiotics 65 '" Cost of R 35 2"
Total "64
Recurrent rhinopharyngitis
Cost 01 physician services " 553 Cost 01 laboratory services 60 33 Cost of antibiotics 65 '" Cost 01 R 35 297
Total '03'
FFl 704 (figs. 2 and 3). dependi ng on the indication and the type of treatme nt-cost estimate (low or high). This favourable outcome is mainly attributable to the relatively low per- patient cost of ribosomal immunotherapy (FF297), which is recouped through savi ngs in direct treatment costs due to the prevention of a substamial number of acute infectious episodes. Saved healthcare resources include physician consultations and visi ts, laboratory tests, medicotechnical services and antibiotic therapy.
Major factors innuencing the economic results in this study are:
• the incremental efficacy of immunoprophylaxis;
• the magni tude of estimated treatment costs per ac ute episode;
wrthout R withR wrthout R with R without R
1670 585 1170 250 500 66 2<J " " 26
". '" 258 " '" 0 '" 0 ' 93 0
"" '" "" 526 '" "'" 387 '" '66 3J2
66 2<J " " 26
302 98 ,,. 53 '''' 0 '" 0 '93 0
1474 609 1010 425 '64
• the number of acute infectious episodes which occur in untreated individuals during a 6-month time period . Therefore, a sensitivi ty analysis was performed
to study the economic effects of immunoprophyla xis under varyi ng assumptions. Threshold values of incremental effi cacy were calculated to determine points of cost equivalence between the immunoprophy lax is and no preventive treatment options. The sensi ti vity analysis on efficacy and treatment-cost est imates showed that net direct sav ings with ribosomal im munotherapy result even with a relati vely low incremental efficacy of immunoprophyiaxis. Threshold ranges of incremental efficacy were found to extend between 7.4
Table VII. Per-patiB!11 cost estimates 01 hea~hcare resource use {in FF) lor parameters included in the extended analys is. Cost data re1ate
to a &-mooth time horizon
Parameter Approximate costs
recurrent otitis media
Concomitant medication" ")() Thermal curesb '" Surgical procedures As outpatient
paracentesis/myringotomy " drainage (middle ear tubes) 37 adenoidectomy/amygdalec1omy 54
As inpatienl
90·220 16()..440
rBCurrent rhinoptlaryngitis
")() 340
Asoutpatieot As inpatiB!1t
a Costs are based on the 2 most frequently prescribed ciasses 01 drugs lor each indication and the estimated prescription lrequency.
b Costs are calcu lated according to a thermal cure duration of 21 days and to the prescription frequency of thermal cures.
" Ads InTemolic>r".ollimited AI righTS rewovOO.

476
and 17.5% for children with recurrent ot iti s media, and 8.9 and 26.1 % for child ren with recurrent rhinopharyngitis. If the incremental efficacy observed in clinical practice is higher than the upper threshold limits defined for each indication, net per-patient cost savings wi ll resuit from ribosomal immunotherapy. The clinical studies carri ed ou t in these indications report consistently higher incremental effi cacy rates than those necessary to achieve net direct savings (table J). A further 2-way sensitivi ty analysis, which investigated the effects of varying the number of acute infectious episodes during 6 months on the threshold incremental effi cacy (table V), showed thaI thi s conclusion withstands changes in disease severity.
From the above data it can be concluded that there is a comfortable margin between the reported efficacy results of controlled trials and the actual efficacy thai may be achieved in daily practice for ribosomal immu notherapy. Th is is important in view of possible uncertainty concern ing the true efficacy of irmnunoprophylaxis. The results show that even when assuming clearly lower increme ntal efficacy rates in routi ne practice, ribosomal immunotherapy can st ill be expected to be cost effecti ve. In this sense, the present analysis prov ides a framework within which individual readers can orient themselves relevant 10 their personal views on the efficacy of ribosomal immunotherapy and treatment costs of ENT infection .
An analysis of the perspectives o f the various payers in the French healthcare system showed that social security insurance stands 10 gain substantially from the implementation of an appropriate immunoprophylaxis programme. Per pat ient, an initial investment of FFI04 leads 10 approximate net savi ngs for this institution of FF630 (based on a standard set of assumptions). Nonetheless, the patients or their complementary insumnce also benefit from (albeit much lower) net sav ings (FFI40), despite the fact that they must cover 65% of the costs of the immunotherapy itself.
In conclusion, net savings occur for all payers involved, and the shown effects are therefore not simply due 10 redistributi on of the costs from one
Ball! el at.
payer to another. Based on the results of this study. the ' no immunoprophylaxis' o ption clearly represents an economically suboptimal solution. Additionally, the likelihood that social security will benefit su bstan tially from ribosomal immunoprophylaxis, yet bears a minor share of the treatment cost, could be an issue for heal!hcare po licy discussion.
The extended analysis showed that a number of further di rect savings could be att ributable to immunoprophy laxis. Specifically. this includes potential sav ings in concomitant medication, surgical intervent ion and thermal cures. Indirect savings were also identified, in terms of product ivity gai ns of parents cari ng for their sick children. Based on the avai lable data. indirect savings could be a major contributor in determining the economic value of ribosomal immunotherapy. However. the existi ng information is insufficient for a concl usi ve presentation of results in this area. Thi s is also the reason we chose not to combine the resu lt s of the core and extended analyses. Nevertheless, the extended analysis enables the conclusion to be made that a number of fun her direct and ind irect econo mic benefits o f immunoprophylaxis exist and. therefore. the core analysis results can be considered conservative.
This study was prompted by the hypothesis that immunoprophylaxis against recurrent ENT in fections is somewhal under-recognised. Thi s may be att ributabl e in part to cl ini cal uncertainties surrounding the efficacy of immunost imulants in routine practice and in pan to economic considemtions. as physicians seem to prefer to treat acute episodes rather than prevent them. The results of this study show thai. both clinically and economically, immunoprophy laxis with ribosomal immunotherapy can be considered preferable 10 the no imm unoprophylaxis option for children with recurrent otitis media or rhi nopharyngitis. Further, prevention can contribute 10 reducing parental anx iety, maintaining normal activities for both parent and child. and avoiding possible long term sequelae and associated costs. Based on the evidence presented for France, physicians as well as payers should give increased attention to thi s treatment option.
Pharmoco£COI">CI<'rics 6 (5) 1994

Immunoprophylaxis ASi"linst ENT Infection
Acknowledgements
This study was supponed by a grant from Pierre Fabre Medicament. Castres. France. The authors would lii.:e to thani.: the starr at the CNAM and Union des Caisses Nationale~ de Securite Sociale (UCANSS) for providing cost and other dma on the French healthcare system. and M~ Be\'erly Steams for her helpful comments in preparation of th is manuscript.
References I. Andre MJ. Infections of th~ ear. nose. and throat ESM'ntial o f
infecti ous diseases. Bhlc~wcll Scicntific Publications. 1985: 155-73
2. Feigi" RD. Kline MW. Spector G. Oti tis media. In : Feigin RD. Cherry JO. edi tnrs. T~xtbook of pcdi;ltrie in{cctiousdisea." '''' 2nd cd. Philadelph ia: WB Saunders Co. 1987: 197-2 15
3. Liu e. Sinusil is. In: Hocprich I'D. Jordan Me. editors. In fec· lious diseases. 41h cd. Philadelphia: J6 LippiIKolt Co. 1989: 293-5
4. Mocknin ML. Respi r~tory infectio!)< in children. PO!itgrad Mcd 1992; 2: 235-S(}
5. Aust in DF. Aculc innal11matOf)' diseases of tlK' middle ear. In: Balkngcr JJ . edilor. Diseases o f lhe nose. throat. ear. head. and neck . 141h cd. Lea &: Febigcr. 1991: 11(»-8
6 . Giebin~ GS. Otit is media updale : palhoge~sis and Ireatment. Ann 0101 Rhinol t aryngoll992: 101 : 21-3
7. Vaulc1 JM. Cauqui l J. PerructICt AM. el aJ. Prevenlion o f TeCUf
renl car. no.;c. and IhlWl infections in young children wit h Ribomunyl: double-blind . plxebo<ontrollcd s tudy. Curr Ther Res 1993; 6 : 722-9
8. Hills G. Hirehe I~ . Lindemann II . Kl inische Effil.ienl eines neucn muhioo~Iericllcn Il11mUnlhel"'lll'Cutikums ( Ribomunyl) bei Kindern lind JIIgcndlichcn mit re:(idivicrenden respiralor· iSChen Infekten. J ~Iros Padiatr 1991; 9: 3-14
9 . Bunin P. ElUde prospecth'c des infections des oourrissons en cm:he. l yon: ~~. Universili Claude Bernard. 199 1
10. Haguenaucr JP. Pfi!"ention des episodes infectiellX ricid ivant'i de la sp-hCre ORl par Ribomunyl comprimtsche •. I·cnfanide moins de Sans. In1lllunol Med 1987: IS: 36-9
II . Par~di.o;e JL. Antimicrobial prophylaxis forr.!currenl aculeO! ili s media. Ann Otol Rhinol l~ryngol 1992: 101: 33-6
12. Bt ne Me. Kahl l. Perruchel AM. ct al. Bacterial lySlltes and ribosOl~s as induce rs o f specific immuM response: a comp;lralive s lud y. Scan J Im"'uno l 1993; 3S: 496_S
477
13. Faure GF. BaIKr S. Mole C. ct al. Pcripbct:ll blood spc-cific antibody-forming ce lls afler oral stimulalion wilh 0 -53. a ribosom~1 vaccine. lXv Bioi Siand 1992: 77: 175-SI
14. Hb;lbi L Roqucs C. Michel G. el al. In ~ilro slimulation of polymorphonuclear a ll adhesion by Ribomunyl and antibiOIie ... Ribomunyl combinalions: effeclson CDI8. CD35.~nd CDI6 upression. Inl J Immunopharmarol 1993; 15: 163-73
IS. Lacommc Y. Prr.·cnlion par immullOlhhapic ribosom.Jle des ipisodes de surinf« Iion ricidivante de 13 sp-hCre ORl chn I" enfant. l mmunol ~ Ied 1985: II : 73·~
16. Grimfdd A. In feclions rcspirJloires n!eidivantes de: I"enfant: inlml de Ribomunyl. Tempo Med 1988: 299: 57·61
17. Castel Y. Pn.'wnt;on des ricidi"es infcclieuses des voies respiraloircs chez I"enfanl par Ri bomun yl comprimts. 1m· munol Med 1986; 14: 34-40
18. COlin G. Le5bro~ D. "re.·cnlion <lcs rec idi,·cs infect icuses des voies rcspiratoire, par Ribomunyl comprimes. lmmunol Mcd 1986; 14: 28-33
19. Perruchel AM. Bilan cpidCmiologiquc de r otile s..' romuque usc chez 45S ORL fram;ais. Rev Soc Fr ORt t99 l ; 7; 59-62
20. Weinste in MC. Economics of ptC'·cniio n. J Gen Intern Mcd 1990; 5 Suppl. : SS9·92
2 1. JQM. .... n B .Horishergcr B. Bruguc ra /I. !. (I al. CO!iI·benefil anal· ysis of hepalilis·B vaccinal ion . A compulNiud decision model for Spain. Inl J Techno l Asscss Heallh Care 1991 ; 3: 379-4Q2
22. Lieu TA. Cochi SL. Black SB. ct al. CO!it·dfo:eli\·cncss of rou· line varicella vaccinal ion progrJm for US chi ldren . JA MA 1994; 5: 375-81
23. Gable C, Holzer S. Engclhan l . el al. Pneumococcal \·acci~. JAMA 1990; 22: 2910-5
24. UCANSS (Union des Cais.~s Nationales de S«urit~ Soci"le). Nomenclalure: generale des acles professionnels. Paris. 1993
25. Dictionnaire Vidal. Editions du Vidal. Paris. t993 26. Statis tical Yearbook. 38th issuc . I):panmo:nt of Economic and
Social l n fonn~tion and Policy Analysis. StatistICal Division. New York: United Nation~. 1993
27. Year Book o f Labour St~t i$t ic$. 52nd ed. Geneva: International labour Office. 1993
28. BocognallO A. Gl"'lndfils N. L..c Fur P. e t al. Sanle. soins et protection socialc en 1992. Paris: Cenlrc de Recherche D'Elude el de Documo:nlalion en Econornie de I~ Sanle. 1993
Correspondence and reprin ts: Dr AIl/Je MllrieTholltll5, Pierre
Fabre Medicame nt , Ll ChartT·cusc, 811 06 Caslres Cedcx, France.







![Bond University Research Repository Antibiotics for ...€¦ · [Intervention Review] Antibiotics for preventing recurrent sore throat Gareth JY Ng1, Stephanie Tan 2, Anh N Vu , Chris](https://img.dokumen.tips/doc/110x75/5f67352d9cc1843cb35c5500/bond-university-research-repository-antibiotics-for-intervention-review-antibiotics.jpg)