Embed Size (px)
Citation preview

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
ECMO/ECCO2R in Acute Respiratory Failure
Alain Combes, MD, PhDCardiology Institute, Hôpital Pitié-Salpêtrière, AP-HP
Inserm UMRS 1166, iCAN, Institute of Cardiometabolism and Nutrition
Sorbonne Pierre et Marie Curie University, Paris, [email protected]

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Conflict of interest
• Principal Investigator: EOLIA trial• VV ECMO in ARDS• NCT01470703 • Sponsored by MAQUET, Getinge Group
• Received honoraria for lectures from • MAQUET, XENIOS, BAXTER
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
ECMO and ECCO2R…To decrease the intensity of MV?

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
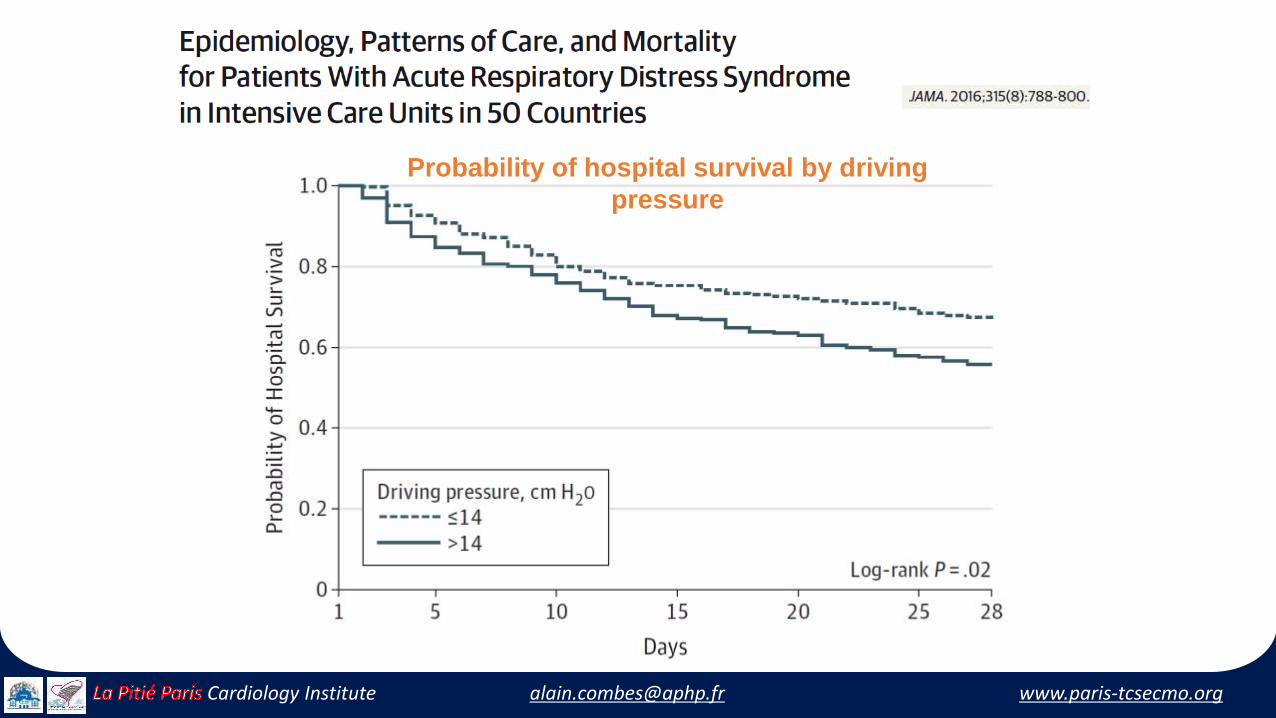
LUNG SAFEEpidemiology of ARDS
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Probability of hospital survival by driving
pressure

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
The evolving paradigm…• ARDSnet strategy might not protect against tidal hyperinflation
• When Pplat remains >28-30 cm H2O • Further decrease of Vt to reduce VILI
• From 6 to <2 ml/kg IBW• To decrease Pplat <25 cm H2O• To decrease ∆P < 12-14 cm H2O• With sufficient PEEP to prevent lung derecruitment
• Extracorporeal gas exchange for• Blood Oxygenation/Decarboxylation• Decrease the intensity of MV

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
What areECMO and ECCO2R?Same Technology
Different Objectives…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Membrane lung O2/CO2 transfer
O2 transferCO2 transfer
ECMO for oxygenation
ECCO2R for Decarboxylation

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Influence of ECMO flow
Schmidt et al, Intensive Care Med, 2013
Adequate Oxygenation
Qecmo > 60% Qco
PaO2 mmHg
SaO2, %
PaCO2 mmHg

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Influence of Sweep Gas Flow
Schmidt et al, Intensive Care Med, 2013
25
30
35
40
45
50
55
60
65
70
75
50
60
70
80
90
100
110
120
130
140
150
20
25
30
35
40
45
50
55
60
65
Pa
CO
2 (
mm
Hg
)P
AS
P (
mm
Hg
)P
aO
2 (
mm
Hg
)
10 8 6 4 2
Sweep gas flow (L.min-1 )
P < 0.001
P < 0.001
PaO2 mmHg PAPS mmHg25
30
35
40
45
50
55
60
65
70
75
50
60
70
80
90
100
110
120
130
140
150
20
25
30
35
40
45
50
55
60
65
Pa
CO
2 (
mm
Hg
)P
AS
P (
mm
Hg
)P
aO
2 (
mm
Hg
)
10 8 6 4 2
Sweep gas flow (L.min-1 )
P < 0.001
P < 0.001
25
30
35
40
45
50
55
60
65
70
75
50
60
70
80
90
100
110
120
130
140
150
20
25
30
35
40
45
50
55
60
65
Pa
CO
2 (
mm
Hg
)P
AS
P (
mm
Hg
)P
aO
2 (
mm
Hg
)
10 8 6 4 2
Sweep gas flow (L.min-1 )
P < 0.001
P < 0.001
25
30
35
40
45
50
55
60
65
70
75
50
60
70
80
90
100
110
120
130
140
150
20
25
30
35
40
45
50
55
60
65
Pa
CO
2 (
mm
Hg
)P
AS
P (
mm
Hg
)P
aO
2 (
mm
Hg
)
10 8 6 4 2
Sweep gas flow (L.min-1 )
P < 0.001
P < 0.001
25
30
35
40
45
50
55
60
65
70
75
50
60
70
80
90
100
110
120
130
140
150
20
25
30
35
40
45
50
55
60
65
Pa
CO
2 (
mm
Hg
)P
AS
P (
mm
Hg
)P
aO
2 (
mm
Hg
)
10 8 6 4 2
Sweep gas flow (L.min-1 )
P < 0.001
P < 0.001
PaCO2 mmHg
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
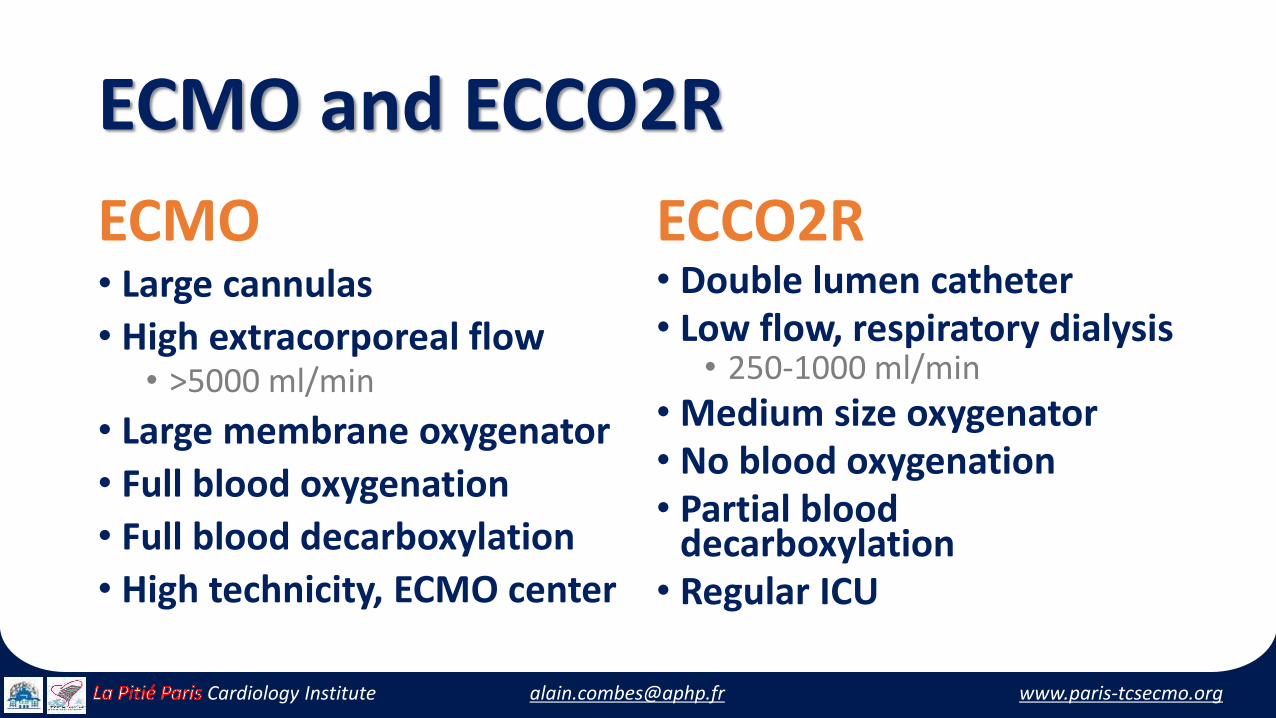
ECMO and ECCO2R
ECMO• Large cannulas
• High extracorporeal flow• >5000 ml/min
• Large membrane oxygenator
• Full blood oxygenation
• Full blood decarboxylation
• High technicity, ECMO center
ECCO2R• Double lumen catheter• Low flow, respiratory dialysis
• 250-1000 ml/min
• Medium size oxygenator• No blood oxygenation• Partial blood
decarboxylation• Regular ICU

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
ECMO and ECCO2R…What is the Evidence?

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Results of series of VV-ECMO in ARDS patients

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
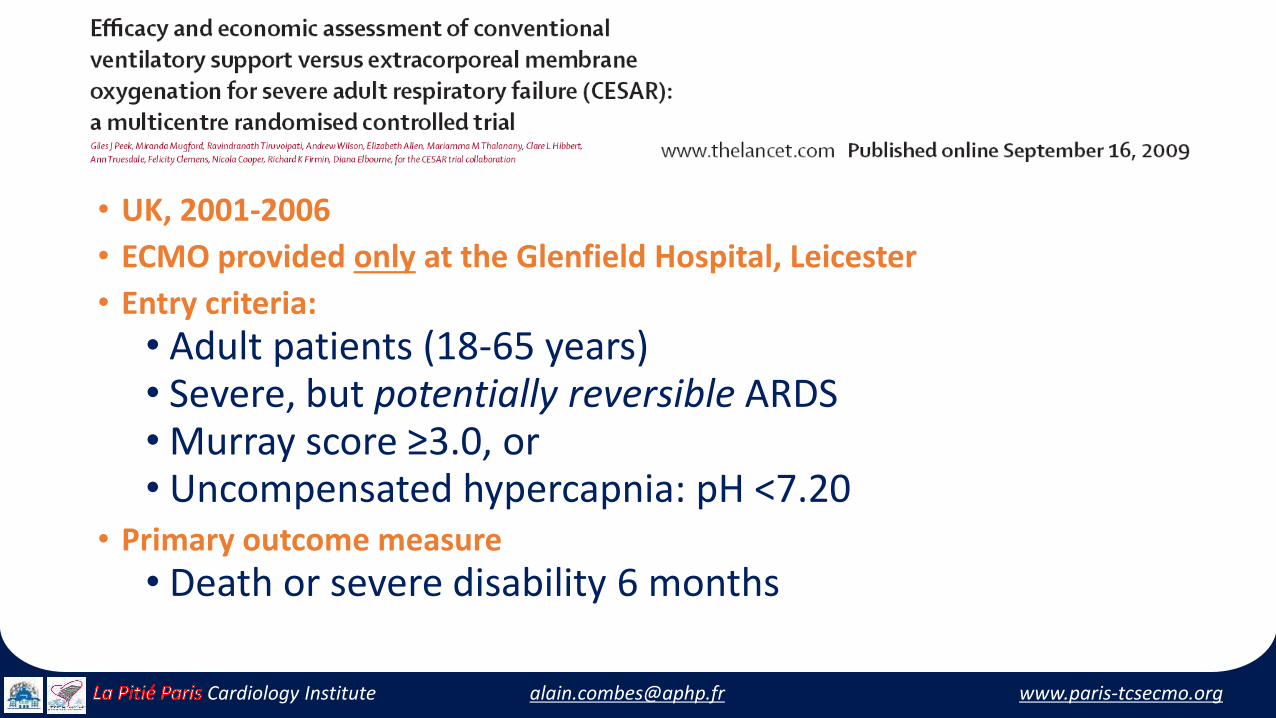
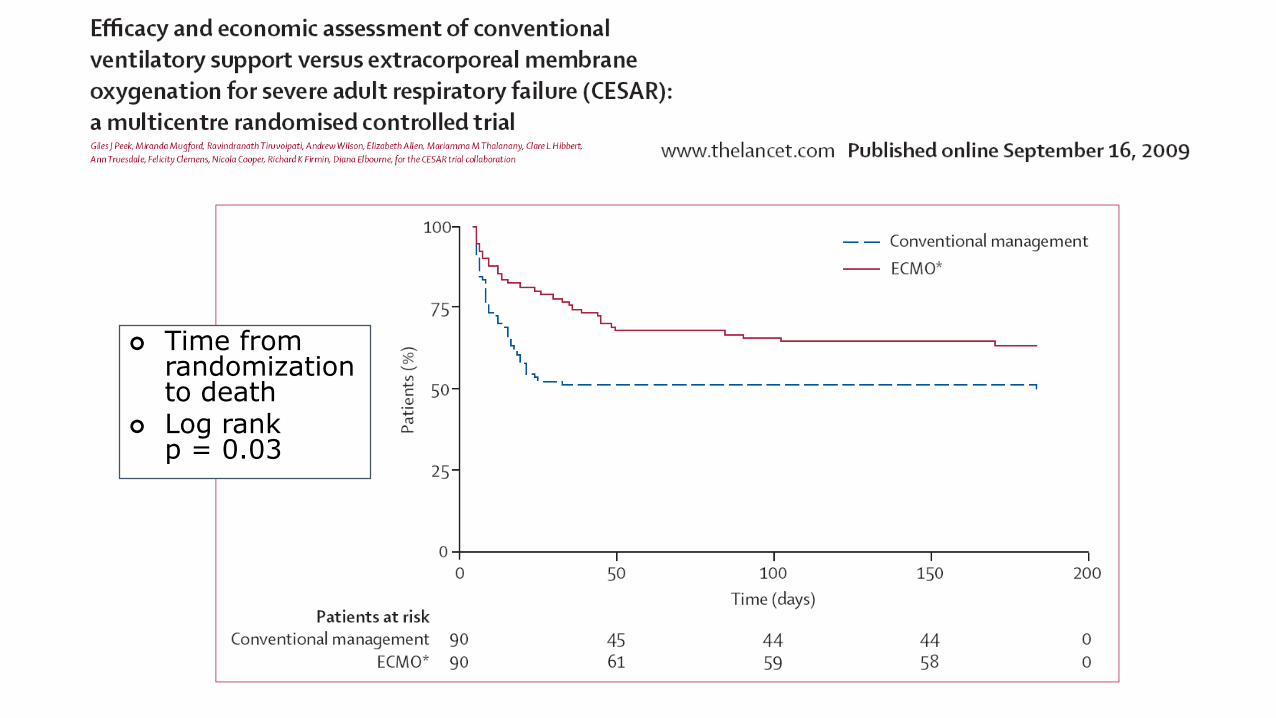
The CESAR trial
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
• UK, 2001-2006
• ECMO provided only at the Glenfield Hospital, Leicester
• Entry criteria:
• Adult patients (18-65 years) • Severe, but potentially reversible ARDS• Murray score ≥3.0, or • Uncompensated hypercapnia: pH <7.20
• Primary outcome measure
• Death or severe disability 6 months

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Time from randomization to death
Log rank p = 0.03

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
17 (25%)

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Et al…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Et al…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Et al…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
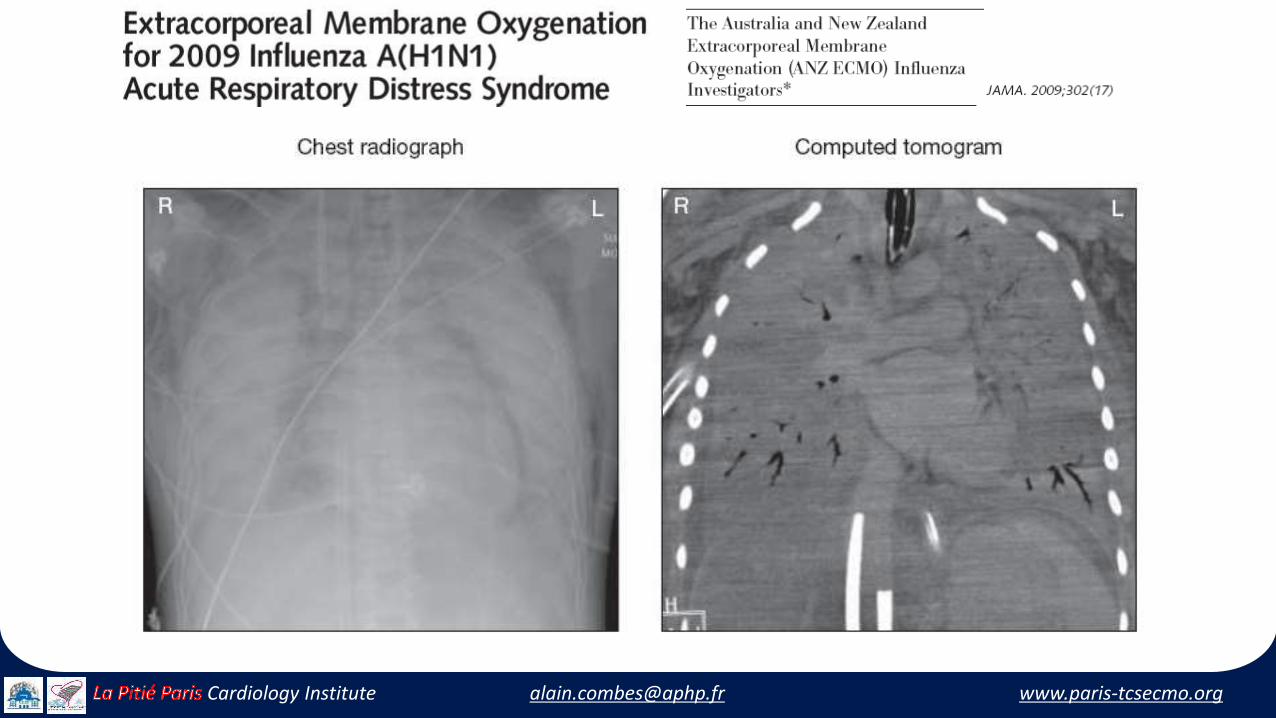
• The French REVA Registry collected data of patients hospitalized in ICUs
• For H1N1-associated ARDS
• Analysis of factors associated • With death among 123 patients who received ECMO
• Case-control study with • Matching on a propensity score to receive ECMO

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Why early ECMO?

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100 120 140 160 180
MV <7 days before ECMO
MV >7 days before ECMO
P <0.005, log-rank

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
10
15
20
25
30
20
25
30
35
40
0
100
200
300
400
500Before ECMO After ECMO
0 0
Driving Pressure Tidal Volume Plateau Pressure

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Results ECCO2R seriesin ARDS patients

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Morris AH, et al. Am J Respir Crit Care 1994;349:295−305.
Randomised clinical trial of pressure-controlled inverse ratio ventilation and ECCO2R for ARDS
Study design
• Randomised controlled clinical trial
• 40 patients with severe ARDS
• ECCO2R versus MV
– Low-flow veno-venous ECCOR2 device
Results
• No significant difference in survival at 30 days (p = 0.08):
– 42% in the MV group (n = 19)
– 33% in the ECCO2R patients (n = 21)
– All deaths occurred within 30 days of randomization
• Study stopped for futility
• >30% patients with severe haemorrhage
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Techniques of the 2000’s…
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Novalung, ILA, Pumpless AV shunt

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Novalung, ILA pumpless AV shunt
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Frequency of complications and adverse effects
Complication / side effect Patients (n)
Ischemia of lower limb after cannulation 9
Cannula thrombosis 4
Compartmental syndrome in a lower limb 4
Haematoma / aneurysm at cannulation site 2
Haemolysis 1
Intracerebral haemorrhage 1
Diffuse bleeding / shock syndrome during cannulation 1
All 22 (24.4%)
Limb ischemia
due to arterial
cannulation +
need for IV
norepinephrineOverall frequency
of complications
and side effects
was 24%

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Hemodec DECAP
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Individual and average (horizontal bar) respiratory variables
before and after initiating CO2 removal
VT (mL/kg PBW) Pplat (cm H2O) PEEP (cm H2O) PaO2 / FiO2)
[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Techniques of the 2010’s…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
NOVALUNG

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
• iLA activve, Novalung, ILA membrane • 22 French double lumen cannula• Ten patients hypercapnic respiratory failure• Step 1:
• Sweep gas flow increased from 1 to 14 L/min• At constant blood flow
• Step 2: • Blood flow gradually increased at constant sweep gas flow
• At each step measurement of • Arterial blood gas AND • Membrane gas transfer

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Hemolung, Alung Technologies

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Feasibility and safety of low-flow extracorporeal carbon dioxide
removal to facilitate ultra-protective ventilation in patients with
moderate ARDS

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Time course of CRS Time course of driving pressure
Feasibility and safety of low-flow extracorporeal carbon dioxide
removal to facilitate ultra-protective ventilation in patients with
moderate ARDS

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
PALP, MAQUET®

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
PrismaLung (Baxter)

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Anesth Crit Care Pain Med 2014
Mean CO2 removal rates at FsO2 1
Preclinical study in 5 adult hypercapnic pigs to investigate the performance of thePrismaLung system with different flow rates (blood flow/ sweep gas flow)

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
More to come…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
A new paradigm…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Mild ARDS Severe ARDSModerate ARDS
Incre
asin
g I
nte
nsit
y o
f In
terv
en
tio
n
300 200250 0100150 50
PaO2/FiO2
Low Tidal Volume Ventilation
Higher PEEP
Low-Moderate PEEP
Prone Positioning
NIV
Neuromuscular Blockade
Inhaled NO
ECCO2R
ECMO
HFOV
The ARDS Definition Taskforce. JAMA 2012;307:2526-2533.

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
“In God we (may) trust; all others
must bring data…”W. Edwards Deming
(1900-1993)

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
We need EOLIA… A new trial of
ECMO for severe pneumonia/ARDS241 patients randomized so far…
YESWECAN
YESWECAN

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
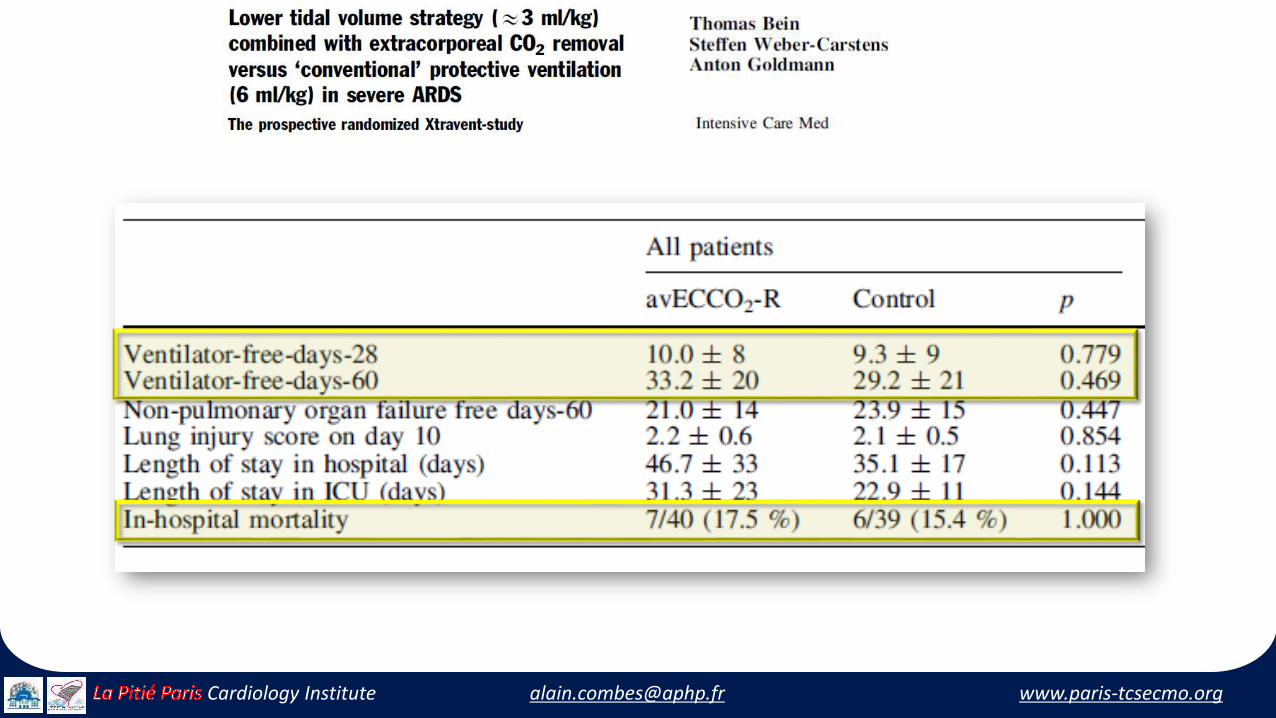
A Strategy of UltraProtective lung ventilation
With Extracorporeal CO2 Removal for
New-Onset moderate to seVere ARDS
The SUPERNOVA trial

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute
Conclusion
• ECMO/ECCO2R: Potential for use in moderate to severe ARDS patients
• To allow further reduction of Vt/Pplat/∆P, to limit VILI…
• ExtraCorporeal CO2 Removal
• “Respiratory dialysis” for moderate ARDS
• VV-ECMO
• For refractory hypoxemia
• For severe ARDS?
• Before large diffusion, (re)test the concept in large randomized clinical trials…

[email protected] www.paris-ecmo.orgCardiology Institute [email protected] www.paris-tcsecmo.orgCardiology Institute










![TCS - ECMO - [Bow]€¦ · The Paris International Congress on ECMO will therefore become the TCS-ECMO ... Ethics: end of life and ECMO FRIDAY 1 ... TCS for the right ventricle M](https://img.dokumen.tips/doc/110x75/5aef5ebd7f8b9a8b4c8c350f/tcs-ecmo-bow-the-paris-international-congress-on-ecmo-will-therefore-become.jpg)


















