Embed Size (px)
Citation preview

Short Com mu ni ca tion
Jour nal of Neuroimaging Vol 11 No 2 April 2001Dubey et al: Early CT Hypodensity Pre dicts Hem or rhage
Early Com puted To mog ra phy Hypodensity Pre dicts Hem or rhage Af ter In tra ve nous Tis sue Plasminogen Ac ti va tor inAcute Ischemic Stroke
Neeraj Dubey, MD
Rohit Bakshi, MD
Mo ham med Wasay, MD
Jacek Dmochowski, PhD
A B S T R A C T
Parenchymal hypodensity is a pro posed risk fac tor for hem or -rhage after recom bi nant tis sue plasminogen acti va tor (TPA)thrombolysis for ischemic stroke. In Buf falo, NY, and Hous ton,TX, the authors reviewed 70 patients who were treated withintra ve nous TPA for acute mid dle cere bral artery (MCA) stroke.Two observ ers blinded to clin i cal out come ana lyzed ini tialnoncontrast head com puted tomog ra phy (CT) scans. Basalgan glia CT hypodensity was quantitated in Hounsfield units(HUs). Contralateral-ipsilateral dif fer ence in den sity was cal cu -lated using the asymp tom atic side as a con trol. Ictus time toTPA aver aged 2.5 hours. Six patients devel oped symp tom aticintraparenchymal hematomas (2 fatal). The hem or rhage grouphad more severe basal gan glia hypodensity (mean 7.5 ± 1.4,range 6–10 HU) than the nonhemorrhage group (2.2 ± 1.4,range 0–9 HU) (P < .0001). The hem or rhage group hadhypodensity of >5 HU; the nonhemorrhage group hadhypodensity of ≤ 4 HU, except 1 patient with hypodensity of 9HU. In pre dict ing hem or rhage, the pos i tive pre dic tive value ofhypodensity > 5 HU was 86%; the neg a tive pre dic tive value was
100%. Prethrombolysis NIH Stroke Scale (NIHSS) def i cit (P =.0007) and blood glu cose (P = .005) were also higher in the hem -or rhage group. Age, gen der, smok ing, hyper ten sion, and ictustime to TPA infu sion did not dif fer between the 2 groups. Logis -tic regres sion indi cated that basal gan glia hypodensity was thebest sin gle pre dic tor of hem or rhage. Hypodensity and NIHSSscore together pre dicted all cases of hem or rhage. The authorscon clude that basal gan glia hypodensity quan ti fied by CT maybe a use ful method of risk strat i fi ca tion to select acute MCAstroke patients for throm bo lytic ther apy.
Key words: Com puted tomog ra phy, thrombolysis, basal gan -glia, ischemic stroke, hem or rhage.
Dubey N, Bakshi R, Wasay M, Dmochowski J.Early com puted tomog ra phy hypodensity
pre dicts hem or rhage after intra ve noustis sue plasminogen acti va tor
in acute ischemic stroke.J Neuroimaging 2001;11:184–188.
Compared with other neuroimaging tech niques (eg, mag -netic res o nance imag ing, con ven tional angiography,sin gle-pho ton emis sion com puted tomog ra phy, trans-cra nial Dopp ler),1–4 com puted tomog ra phy (CT) of thehead has been most fre quently used in the set ting of acuteischemic stroke to exclude hem or rhage and other pos si -ble causes of neu ro logic symp toms. More recently, withthe use of intra ve nous (IV) recom bi nant tis sue plasmino-gen acti va tor (TPA) in acute stroke,1,4–11 CT has dem on -strated util ity as a prog nos tic and a tri age test.1,3,4,8–11
In the National Insti tute of Neu ro log i cal Dis eases andStroke (NINDS) trial, a noncontrast CT scan was man da -tory before the ini ti a tion of treat ment with IV TPA.8 Theonly exclu sion cri te rion on CT scan find ing was
184 Copy right © 2001 by the Amer i can So ci ety of Neuroimaging
Re ceived March 17, 2000, and in re vised form June 2,2000. Ac cepted for pub li ca tion June 24, 2000.
From the De part ment of Neu rol ogy, Uni ver sity of Texasat Hous ton (ND); Im aging Ser vices, Kaleida Health, andthe De part ment of Neu rol ogy, State Uni ver sity of NewYork at Buf falo (RB); the De part ment of Neu rol ogy, AgaKhan Uni ver sity, Karachi, Pa ki stan (MW); and the De -part ment of So cial and Pre ven tive Med i cine (Di vi sion ofBiostatistics and Med i cal In for ma tics), State Uni ver sity ofNew York at Buf falo ( JD).
Ad dress cor re spon dence to Dr Bakshi, Neu ro sci enceCen ter, E-2, Buf falo Gen eral Hos pi tal, 100 High Street,Buf falo, NY 14203. E-mail: rbakshi@buf falo.edu.

intracranial hem or rhage.8 In the Euro pean Coop er a tiveAcute Stroke Study (ECASS),1,10 brain swell ing on the pre -treat ment CT scan pre dicted late neu ro logic wors en ing.10
Other pro found ischemic CT changes, includ inghypodensity in greater than one third of the mid dle cere -bral artery (MCA) ter ri tory and cere bral edema, may pre -dis pose to intracerebral hem or rhage (ICH), thus form inga rel a tive con tra in di ca tion in the use of thrombolysis.1,8–11
In this study, we quan ti ta tively deter mined whetherbasal gan glia hypodensity on the pre treat ment CT scanwas an inde pend ent risk fac tor for the devel op ment ofsymp tom atic hematomas in stroke patients who receivedIV TPA throm bo lytic ther apy.
Par tic i pants and Method
Sev enty ischemic stroke pa tients who were treated withIV TPA for acute MCA stroke were ran domly and ret ro -spec tively re viewed at 2 in sti tu tions (State Uni ver sity ofNew York at Buf falo and Me mo rial Hermann Hos pi tal inHous ton, TX). Base line (pre treat ment) data in clud ingage, gen der, to bacco use, hy per ten sion his tory, base lineNIH Stroke Scale (NIHSS) def i cit, se rum glu cose,prothrombin time (PT)/par tial thromboplastin time(PTT), in ter na tional nor mal ized ra tio (INR), and headCT scans were ret ro spec tively an a lyzed by 2 ex pe ri encedob serv ers blinded to the laterality of stroke symp tomsand to clin i cal out come. The same 2 ob serv ers an a lyzedfol low-up CT scans per formed 24 hours af ter TPAtreat ment.
Basal gan glia hypodensity was mea sured inHounsfield units (HUs) using pro pri etary com puter work- sta tions avail able at each site as part of the stan dard CTequip ment. The CT data were imme di ately avail ableafter the scan was com plete. No spe cial data trans fer orpost pro cess ing was nec es sary. To deter mine basal gan gliaden sity, a cir cu lar region of inter est was placed in theputamen to cover as much of the putamen as pos si ble. Anaxial slice of the noncontrast scan was cho sen that bestrevealed the midportion of the putamen. In the event ofhead rota tion, a dif fer ent slice could be used for eachhemi sphere. One mea sure ment was taken for each hemi -sphere, and the mean value was recorded. Contralateralto ipsilateral dif fer ence in den sity was cal cu lated using the nonaffected side as con trol. Mea sure ments could be per -formed rap idly (approx i mately 3 min utes per patient).The time between ictus and TPA infu sion ranged from 1to 3 hours (mean ± SD: 2.4 ± 0.4 hours). The time betweenstroke onset and CT scan ning ranged from 0.4 to 2.5hours (2.2 ± 0.4 hours). Other base line char ac ter is tics ofthe 70 patients were as fol lows: age 72 ± 8.1 years, 40 men(57%), 49 with a his tory of hyper ten sion (70%), 24 tobacco
users (34%), serum glu cose 145 ± 20 mg/dl, and NIHSSscore 11.6 ± 4.0. The base line char ac ter is tics of ourpatients are com pa ra ble to those in the NINDS trial.8 Allpatients in this study met the inclu sion and exclu sion cri -te ria for IV TPA treat ment in acute stroke from theNINDS trial.8
The 24-hour (posttreatment) CT scan was ana lyzedand com bined with clin i cal data to deter mine whether the patient had a sig nif i cant ICH related to TPA ther apy. Tobe clas si fied in the ICH group, the patient had to meetboth NINDS8 and ECASS1 cri te ria for sig nif i cant ICH.This meant that the ICH had to be asso ci ated with a2-point or greater drop in NIHSS def i cit (symp tom aticICH)8 and that the ICH had to be a frank parenchymalhematoma (not petechial).1 Six patients had sig nif i cantICH (symp tom atic parenchymal hematoma) and wereclas si fied into the ICH group. Two patients had asymp -tom atic petechial hem or rhage (hem or rhagic infarc tion)and were not placed into either the ICH group or thenon-ICH group. The remain ing 62 patients had no evi -dence of hem or rhage on the 24-hour CT scan (non-ICHgroup).
A Mann-Whit ney U test and Fisher exact test wereused to com pare con tin u ous and nom i nal vari ablesbetween the ICH and non-ICH groups. Univariate logis -tic regres sion was used to deter mine which vari ablescould inde pend ently pre dict ICH. A P value <.05 wascon sid ered sta tis ti cally sig nif i cant. Mul ti ple logis ticregres sion and multivariate dis crim i nate anal y sis wereused to clas sify ICH cases. The rela tion ship betweenbasal gan glia hypodensity and con tin u ous clin i cal vari -ables (the time of CT scan ning after stroke onset and thetime to TPA treat ment after stroke onset) was deter minedby Spearman cor re la tion coef fi cient.
Re sults
A com par i son of rel e vant pre treat ment data be tweenICH and non-ICH groups is shown in Ta ble 1. Base lineNIHSS def i cit (P = .0007), se rum glu cose (P = .005), andbasal gan glia hypodensity (P < .0001) were higher in theICH group. The PT, PTT, INR, and time from ic tus to CT scan ning were not sig nif i cantly dif fer ent be tween the 2groups (all Ps > .05). Lo gis tic re gres sion anal y sis re vealedthat basal gan glia CT hypodensity was a sig nif i cant in de -pend ent pre dic tor of ICH (P = .0018). A step wise lo gis ticre gres sion in di cated that only the ad di tion of NIHSS tothe model im proved its pre dic tive ca pa bil i ties. The ad di -tion of NIHSS led to to tal sep a ra tion of ICH fromnon-ICH cases (Fig 1), prob a bly due to the rel a tivelysmall num ber of ICH cases in the study. The lo gis tic re -gres sion model is not valid when to tal sep a ra tion is pres -
Dubey et al: Early CT Hypodensity Pre dicts Hem or rhage 185
ent (when hypodensity and NIHSS score were in themodel). Thus, for fur ther clar i fi ca tion, we sum ma rizedmultivariate re sults us ing discriminant anal y sis. The fol -low ing discriminant func tion based on CT hypodensityand NIHSS can serve as a pre dic tor of ICH:
Discriminant = 2.85 * DEN SITY + 0.65 * NIHSS – 23.1.
Pos i tive val ues cor re spond to ICH cases and neg a tive val -ues to non-ICH cases. Such discriminant func tion mis-clas si fies only 1 non-ICH case as ICH.
A cut off of 5 HU hypodensity was use ful in sep a rat ingICH from non-ICH groups. All patients in the ICH group had basal gan glia hypodensity of >5 HU. All patients inthe nonhemorrhage group had basal gan glia hypodensityof ≤ 4 HU, except 1 patient with hypodensity of 9 HU. If 5 HU had been used as a cut off for deliv er ing TPA, allsymp tom atic hem or rhages could have been pre vented(neg a tive pre dic tive value 100%) and 2 deaths might havebeen avoided. Only 1 patient who qual i fied for this treat -ment and did not develop ICH would have had TPAtreat ment with held using this cut off (pos i tive pre dic tivevalue 86%). A post hoc review of the ini tial CT scans of the ICH patients revealed that 50% (n = 3) had >33% MCAter ri tory ischemic changes and 33% (n = 2) had a denseMCA sign.12 Thus, >33% MCA ter ri tory ischemicchanges and dense MCA sign had a lower neg a tive pre -dic tive value than our basal gan glia hypodensity tech -nique in pre dict ing ICH.
Age, gen der, time between ictus and TPA infu sion,coag u la tion pro file (PTT, PT), and his tory of cig a rettesmok ing did not sig nif i cantly dif fer between the 2 groups.Across all 70 patients, basal gan glia hypodensity did notcor re late sig nif i cantly with the time of CT scan ning afterstroke onset (ρ = 0.158, P = .10) or the time to TPA treat -ment after stroke onset (ρ = 0.107, P = .21).
Dis cus sion
The re li abil ity of early CT changes in the de tec tion ofacute ischemic stroke, as well as the reproducibility of CT
186 Jour nal of Neuroimaging Vol 11 No 2 April 2001
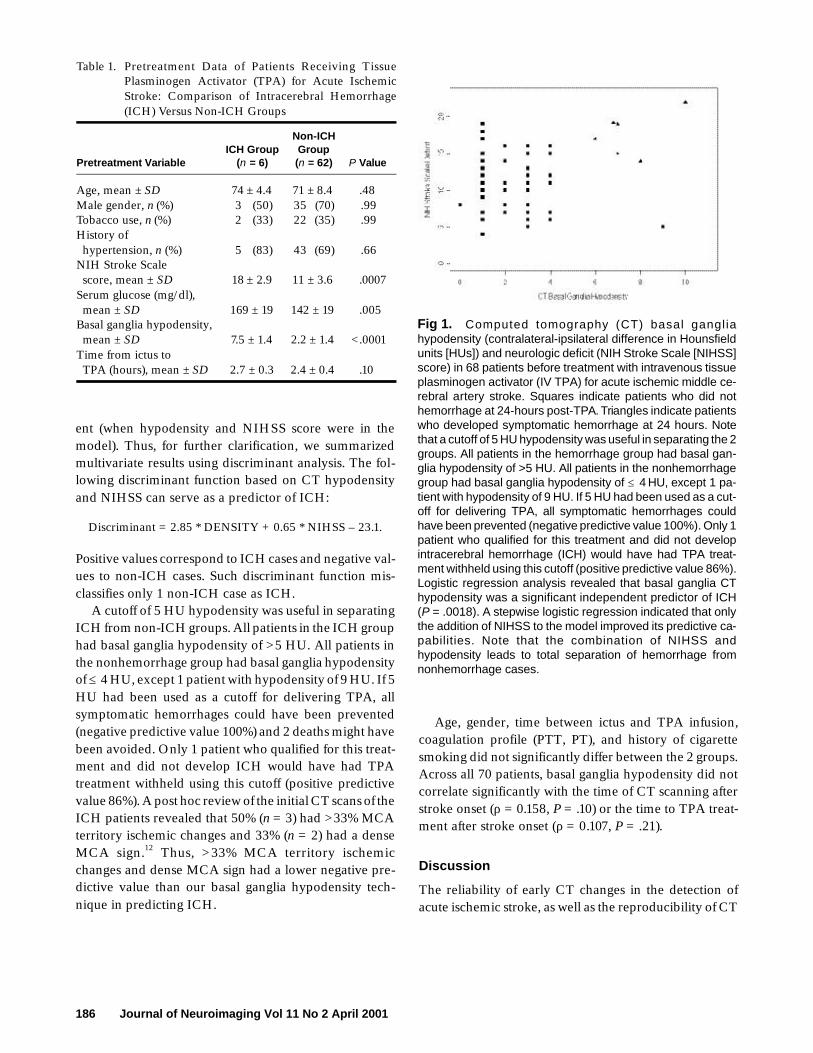
Fig 1. Com puted to mog ra phy (CT) basal gan gl iahypodensity (contralateral-ipsilateral dif fer ence in Hounsfieldunits [HUs]) and neu ro logic def i cit (NIH Stroke Scale [NIHSS]score) in 68 pa tients be fore treat ment with in tra ve nous tis sueplasminogen ac ti va tor (IV TPA) for acute ischemic mid dle ce -re bral ar tery stroke. Squares in di cate pa tients who did nothem or rhage at 24-hours post-TPA. Tri an gles in di cate pa tientswho de vel oped symp tom atic hem or rhage at 24 hours. Notethat a cut off of 5 HU hypodensity was use ful in sep a rat ing the 2 groups. All pa tients in the hem or rhage group had basal gan -glia hypodensity of >5 HU. All pa tients in the nonhemorrhagegroup had basal gan glia hypodensity of ≤ 4 HU, ex cept 1 pa -tient with hypodensity of 9 HU. If 5 HU had been used as a cut -off for de liv er ing TPA, all symp tom atic hem or rhages couldhave been pre vented (neg a tive pre dic tive value 100%). Only 1 pa tient who qual i fied for this treat ment and did not de velopintracerebral hem or rhage (ICH) would have had TPA treat -ment with held us ing this cut off (pos i tive pre dic tive value 86%). Lo gis tic re gres sion anal y sis re vealed that basal gan glia CThypodensity was a sig nif i cant in de pend ent pre dic tor of ICH(P = .0018). A step wise lo gis tic re gres sion in di cated that onlythe ad di tion of NIHSS to the model im proved its pre dic tive ca -pa bil i ties. Note that the com bi na tion of NIHSS andhypodensity leads to to tal sep a ra tion of hem or rhage fromnonhemorrhage cases.
Ta ble 1. Pre treat ment Data of Pa tients Re ceiving Tis suePlasminogen Ac ti va tor (TPA) for Acute IschemicStroke: Com par i son of Intracerebral Hem or rhage(ICH) Ver sus Non-ICH Groups
Non-ICHICH Group Group
Pre treat ment Vari able (n = 6) (n = 62) P Value
Age, mean ± SD 74 ± 4.4 71 ± 8.4 .48Male gen der, n (%) 3 (50) 35 (70) .99To bacco use, n (%) 2 (33) 22 (35) .99His tory of hy per ten sion, n (%) 5 (83) 43 (69) .66NIH Stroke Scale score, mean ± SD 18 ± 2.9 11 ± 3.6 .0007Se rum glu cose (mg/dl), mean ± SD 169 ± 19 142 ± 19 .005Basal gan glia hypodensity, mean ± SD 7.5 ± 1.4 2.2 ± 1.4 <.0001Time from ic tus to TPA (hours), mean ± SD 2.7 ± 0.3 2.4 ± 0.4 .10

scan read ing, has been a mat ter of con tro versy in screen -ing for throm bo lytic ther apy in acute ischemic stroke.ECASS in ves ti ga tors sug gested that sub tle changes on the ini tial CT scan might help iden tify the best can di dates forthrombolysis.1,10,11 ECASS data sug gest that pa tients withrel a tively few early CT changes ap peared to ben e fit mostfrom TPA.1,10,11 Few stud ies have at tempted to look at there li abil ity of early CT changes and the role of quan ti ta tivede tec tion of hypodensity. There is con sid er able lack ofagree ment even among ex pe ri enced cli ni cians in rec og -niz ing and quan ti fy ing early CT changes.3,4 Thus, im -proved meth ods of rec og niz ing and quan ti fy ing earlyischemic brain dam age are needed.4
Sub tle changes of cere bral ischemia includehypoattenuation (hypodensity) of the CT sig nal.3 Slighthypoattenuation of gray mat ter may man i fest as a loss ofdis tinc tion between gray and white mat ter, espe ciallybetween the basal gan glia and inter nal cap sule orbetween the insu lar or frontoparietal cor tex and under ly -ing white mat ter.3 These changes, along with greater than33% MCA dis tri bu tion hypodensity,3,4,11 dense MCAsign,12 and cere bral edema (swell ing),9 are col lec tivelyreferred to as early ischemic CT changes in the dis cus sionbelow.
The impor tance of our obser va tion obvi ously dependson the pathophysiologic and clin i cal sig nif i cance of earlyCT hypodensity. It is likely that early CT changes such ashypoattenuation rep re sent cytotoxic edema andincreased tis sue water con tent, which may or may not rep -re sent irre vers ible injury.4 The asso ci ated tis sue soft en ingand dis rup tion of the blood-brain bar rier may pre dis poseto ICH.4
Major early CT changes so far have been defined as>33% MCA ter ri tory involve ment or cere braledema/mass effect.1,3,4,8–11 Hypodensities involv ing morethan one third of the MCA dis tri bu tion are fre quently dueto ter mi nal inter nal carotid artery or MCA mainstemocclu sions in IV TPA angiographic stud ies,6,7 which areasso ci ated with worse out comes and increased hem or -rhagic trans for ma tion. Edema and mass effect have alsobeen linked to higher rates of ICH in TPA-treated strokepatients.1,8
This study dif fers from pre vi ous stud ies in that we havepre sented a com puter-assisted quan ti ta tive mea sure mentof hypoattenuation on ini tial head CT scans rather than amea sure ment based on a visual (sub jec tive) deter mi na -tion. One strength of this method is the ease of per form ing these mea sure ments in the clin i cal set ting. Data can beobtained rap idly on the pro pri etary work sta tion that ispro vided with most mod ern CT scan ners. This should not cause an undue delay in acute stroke tri age. The den sity
data are quan ti ta tive and likely to be less vul ner a ble to thevari abil ity that is seen with sub jec tive or semiquantitativevisual anal y ses.3,4 Our find ings must be viewed with lim i -ta tions. Because of the ret ro spec tive nature of the anal y sis, we did not sys tem at i cally eval u ate many of these early CT changes on all patients. How ever, in the patients whodevel oped ICH, the find ings of >33% MCA ter ri toryhypodensity changes and dense MCA signs had a lowerneg a tive pre dic tive value than basal gan glia CThypodensity. Future stud ies should con firm and extendthese pre lim i nary data with pro spec tively col lected data.Intrarater and interrater reli abil ity of this method shouldbe deter mined. Finally, the prog nos tic value of basal gan -glia hypodensity should be com pared with other pro -posed CT mark ers such as >33% MCA ter ri toryhypodensity,3,4,11 dense MCA sign,12 and cere bral edema(swell ing).9
Our study also showed that ini tial clin i cal def i cit asassessed by the NIHSS was use ful in pre dict ing ICH.When NIHSS score was com bined with basal gan gliahypodensity, all cases of ICH were pre dicted. This is inagree ment with pre vi ous data show ing that severe acuteneu ro logic impair ment is a risk fac tor for ICH after TPA.9
Thus, in acute MCA stroke patients, early severe braininjury (reflected by clin i cal exam i na tion and CT hypo-atten u a tion) is asso ci ated with ICH after TPA ther apy.
Ref er ences
1. Hacke W, Kaste M, Fieschi C, et al. Intra ve nousthrombolysis with recom bi nant tis sue plasminogen acti va -tor for acute hemi spheric stroke. The Euro pean Coop er a -t ive Acute Stroke Study (ECASS). JAMA1995;274:1017–1025.
2. Bakshi R, Kamran S, Kinkel PR, et al. Fluid-atten u atedinver sion-recov ery MR find ings in acute and sub acute cere -bral intraventricular hem or rhage. AJNR Am J Neuroradiol1999;20:629–636.
3. Marks MP, Holmgren EB, Fox AJ, et al. Eval u a tion of earlycom puted tomographic find ings in acute ischemic stroke.Stroke 1999;30:389–392.
4. Grotta JC, Chiu D, Lu M, et al. Agree ment and vari abil ity inthe inter pre ta tion of early CT changes in stroke patientsqual i fy ing for intra ve nous rtPA ther apy. Stroke1999;30:1528–1533.
5. Demchuk AM, Morgenstern LB, Krieger DW, et al. Serumglu cose level and dia be tes pre dict tis sue plasminogen acti -va tor-related intracerebral hem or rhage in acute ischemicstroke. Stroke 1999;30:34–39.
6. del Zoppo GJ, Poeck K, Pessin MS, et al. Recom bi nant tis sue plasminogen acti va tor in acute throm botic and embolicstroke. Ann Neurol 1992;32:78–86.
7. Sasaki O, Takeuchi S, Koike T, et al. Fibrinolytic ther apy foracute embolic stroke: intra ve nous, intracarotid, and intra-arte rial local approaches. Neu ro sur gery 1995;36:246–252.
Dubey et al: Early CT Hypodensity Pre dicts Hem or rhage 187

8. National Insti tute of Neu ro log i cal Dis or ders and Strokert-PA Stroke Study Group. Tis sue plasminogen acti va tor foracute ischemic stroke. N Eng J Med 1995;333:1581–1587.
9. NINDS t-PA Stroke Study Group. Intracerebral hem or -rhage after intra ve nous t-PA ther apy for ischemic stroke.Stroke 1997;28:2109–2118.
10. Davalos A, Toni D, Iweins F, et al. Neu ro log i cal dete ri o ra -tion in acute ischemic stroke: poten tial pre dic tors and asso -
ci ated fac tors in the Euro pean Coop er a tive Acute StrokeStudy (ECASS). Stroke 1999;30:2631–2636.
11. von Kummer R, Allen KL, Holle R, et al. Acute stroke: use -ful ness of early CT find ings before throm bo lytic ther apy.Radi ol ogy 1997;205:327–333.
12. Bakshi R, Mazziotta JC. Acute mid dle cere bral arterythrom bo sis dem on strated by cra nial com puted tomog ra -phy: the “dense MCA” sign. Arch Neurol 1998;55:1577.
188 Jour nal of Neuroimaging Vol 11 No 2 April 2001





























