Embed Size (px)
Citation preview

Early and Late Outcomes in Patients Excluded FromSame-Day Home Discharge After Transradial Stenting
and Maximal Antiplatelet Therapy
Olivier F. Bertrand,* MD, PhD, Josep Rodes-Cabau, MD, Eric Larose, DVM, MD, Guy Proulx, MD,Onil Gleeton, MD, Can Manh Nguyen, MD, Isabelle Nault, MD, Louis Roy, MD,
Paul Poirier, MD, PhD, Olivier Costerousse, PhD, and Robert De Larochelliere, MD
Background: To develop a safe practice of same-day discharge after percutaneouscoronary intervention (PCI), it is important to identify early the patients who need toremain hospitalized and potentially require more careful follow-up. In the EASY trial, alarge number of patients with acute coronary syndromes were enrolled prior to PCI tobe randomized between same-day discharge or overnight hospitalization. Based on afew angiographic criteria, suboptimal results, or clinical complications, some patientswere excluded from randomization after PCI. Objectives: We report the early and lateoutcomes of those patients, and evaluate the use of simple criteria precluding same-day discharge. Results: The rate of major adverse cardiac events including death,myocardial infarction, and target vessel revascularization in patients excluded fromrandomization (n 5 343) was significantly higher at 30 days (10.2% vs. 1.6%), 6 months(17.5% vs. 5.6%), and 12 months (24.5% vs. 9%) compared with randomized patients(n 5 1,005; P < 0.0001). At 12 months, only transient vessel closure (HR 1.78, 95%CI 1.10–2.65, P 5 0.023) and a residual dissection � grade B post-PCI (HR 1.53, 95%CI 1.11–2.05, P 5 0.011) were independent predictive factors of adverse outcomes.Conclusion: Criteria associated with angiographic suboptimal results or clinicalcomplications are useful to identify patients ineligible for same-day discharge after PCI,regardless of the clinical presentation. Patients excluded from same-day discharge afterPCI for safety concerns have worse early and late outcomes. Transient vessel closureand persisting moderate dissection after PCI remain independent predictors of lateadverse outcomes after PCI with maximal antiplatelet therapy. ' 2008 Wiley-Liss, Inc.
Key words: acute coronary syndrome; percutaneous coronary intervention; transradialcath; thrombosis; complications adult cath/intervention
INTRODUCTION
In the EArly discharge after transradial Stenting ofcoronarY arteries (EASY) study, a large number ofpatients with acute coronary syndrome representingtoday’s practice in a high-volume catheterization labo-ratory were included. After a bolus of abciximab anduncomplicated transradial coronary stenting, 1,005patients were randomized either to same-day discharge(n 5 504) or to overnight hospitalization (n 5 501).We have previously reported that the rate of majoradverse cardiovascular events (MACE) including death,myocardial infarction (MI) and target vessel revascu-larization (TVR) were similar in the two randomizedgroups at 30 days and at 1 year [1,2]. For safety con-cerns, some patients (n 5 343) were excluded fromrandomization after percutaneous coronary intervention(PCI). Although a number of angiographic and clinicalcriteria have been used to identify patients at higher-
Hopital Laval, Institut Universitaire de Cardiologie et de Pneu-mologie, Quebec, Canada
Grant sponsors: Eli-Lilly; Bristol-Myers-Squibb/Sanofi-Aventis;
Regie Regionale de Quebec; Corporation de l’Institut de cardiologie
de Quebec
Conflict of interest: Nothing to report.
*Correspondence to: Olivier F. Bertrand, MD, PhD, Interventional
Cardiology Laboratories, Hopital Laval, Institut Universitaire de
Cardiologie et de Pneumologie, affilie a l’Universite Laval, 2725
Chemin Ste Foy, Quebec, Canada G1V 4G5.
E-mail: [email protected]
Received 10 April 2008; Revision accepted 17 May 2008
DOI 10.1002/ccd.21662
Published online 20 October 2008 in Wiley InterScience (www.
interscience.wiley.com).
' 2008 Wiley-Liss, Inc.
Catheterization and Cardiovascular Interventions 72:619–625 (2008)

risk of early complications and exclude them fromsame-day discharge, their impact on the incidence ofMACE have not been well characterized [3]. The pur-pose of this work is to analyze early and late clinicaloutcomes in patients not randomized post-PCI in theEASY trial and assess the angiographic and clinicalcriteria used to exclude them from randomization.
METHODS
Study Population
The details of the EASY trial have been previouslydescribed [1]. Briefly, patients referred for coronaryangiography and possible PCI were enrolled at LavalHospital from October 2003 to April 2005. Patientswere excluded prior to angiography if they had sus-tained ST-elevation MI within 72 hr or had a historyof left ventricular ejection fraction �30%. Except for asecondary branch in bifurcation lesions or redilatationfor in-stent restenosis, i.e., brachytherapy, all lesionshad to be stented. The protocol was approved byHealth Canada and the Laval Hospital Ethics ReviewBoard, and the protocol was published on the ClinicalTrials Web site (NCT001169819). All patients signedan informed consent form for participation in the trialand 6-month and 1-year follow-up.
Study Design and Protocol
The study was a randomized, controlled, open-labelstudy comparing same-day home discharge and bolus-only of abciximab to overnight hospitalization andstandard bolus followed by 12-hr infusion of abcixi-mab after uncomplicated transradial coronary stenting.In case of clinical complications during PCI, i.e., ven-tricular fibrillation or hemodynamic collapse, or angio-graphic suboptimal results defined by persisting � typeB dissection of NHLBI classification, compromise orloss of �1 mm side-branch, abnormal TIMI flow, orpresence of thrombus, patients were not randomizedfor safety concerns and received standard abciximabbolus followed by 12-hr infusion. Initially, a stentedlength �25 mm was an exclusion criteria for random-ization, but the criteria was removed later by amend-ment to the protocol. Abciximab was administered as a0.25 mg/kg bolus prior to first balloon angioplasty andinfusion was given for a total of 12 hr at 0.125 lg/(kgmin) to a maximum of 10 lg/min.All patients were pretreated with aspirin and clopi-
dogrel (90% � 12 hr) prior to diagnostic angiography.After radial or ulnar sheath insertion, a bolus of 70 U/kg heparin was given intravenously as per our routine[4]. Creatine kinase (CK) and CK-myocardial band(CK-MB) were evaluated on samples collected imme-diately prior to the procedure, after PCI (4–6 hr) and
the next day (12–24 hr). An electrocardiogram wasobtained before, after, the day after PCI, at 30 6 7days, 180 6 30 days, and 365 6 30 days.
Study End Points
As reported previously, the primary composite end-point included the cumulative incidence of any of thefollowing seven events at 30 days: death from anycause, Q- and non-Q-wave MI, any unplanned revascu-larization for ischemia, major bleeding according toREPLACE-2 criteria [5], severe thrombocytopenia(<50,000/lL), access site complication, or repeat hos-pitalization. Local hematomas were graded accordingto a specific scale [1]. The MACE (death, MI, TVR)rate as secondary endpoint was calculated at 30 days,6 months, and 12 months after the index procedure.Endpoint adjudications and classifications at all timepoints were made by a clinical events committee blindedto study group allocation. Q-wave MIs were classifiedusing the Minnesota code. For non-Q-wave MIs, peripro-cedural MIs were classified when any post-PCI CK-MBvalue was �3 3 ULN, i.e., 30 lg/mL in our laboratory.After hospital discharge, non-Q MIs were classified usingthe ACC/ESC nomenclature, i.e. using any troponin Ior troponin-T value or CK/CK-MB values above upperlimits of normal [6].
Data Collection and Analysis
All patients and/or family relatives were contactedby telephone at the prespecified intervals. Study per-sonnel used structured questionnaires, and data wereentered in case report forms. In case of death, generalpractitioners or treating physicians were contacted andhospital records or autopsy reports were obtained. Forother adverse cardiac events, relevant hospital recordswere obtained as source documentations. Clinical fol-low-up was performed at 12 months in 100% of thestudy population.Categorical variables were expressed as numbers
and percentages, and continuous variables as mean 6SD. Baseline and procedural characteristics were com-pared between groups using Fischer’s exact test orPearson chi-square test for categorical variables andStudent’s t-test or Wilcoxon rank-sum test for continu-ous variables. Survival curves were constructed usingKaplan–Meier techniques, and comparisons were madeusing log-rank test. Cox proportional hazard modelwas used to assess the relative risks of adverse out-comes at 30 days and 12 months. A probability value<0.05 was considered significant. Statistical tests wereperformed using JMP 5.1 (SAS Institute, Cary, NC).
620 Bertrand et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

RESULTS
Clinical Outcomes in Patients Not-RandomizedPost-PCI Compared With Randomized Patients
The baseline characteristics of patients randomized
and not-randomized after PCI were similar except for
more with previous CABG in patients not-randomized
(Table I). The majority of patients presented with
acute coronary syndrome, 67% in unstable angina, and
25% with non-ST elevation MI. More patients not-
randomized had two- and three-vessel disease, and
more lesions were dilated in these patients when
compared with the randomized groups (P < 0.0001;
Table I). There were more type-B2/C lesions in
not-randomized patients compared with randomized
patients (80% vs. 52%, P < 0.0001). Reflecting morecomplex PCI, the mean duration of procedures wasalso longer in patients not-randomized after PCI (68 631 min vs. 42 6 20 min, P < 0.0001).At 30 days, the primary composite endpoint was
higher in not-randomized compared with randomizedpatients (21.0% vs. 10.3%, P < 0.0001; Table II).Overall, ischemic and bleeding events occurred signifi-cantly more often in patients not randomized. Simi-larly, the MACE rate was significantly higher inpatients not-randomized at 30 days, 6 months, and12 months (P < 0.0001) compared with randomizedpatients (Table III).The cumulative incidence of events for patients in not-
randomized post-PCI compared with randomized patients
TABLE I. Baseline and Procedural Characteristics
Patients All (n 5 1,348) Randomized (n 5 1,005) Not randomized (n 5 343) P*
Age, years 60 6 10 60 6 10 61 6 11 0.20
Male 1050 (78)a 789 (79) 261 (76) 0.37
Diabetes 233 (17) 165 (16) 68 (20) 0.16
Previous CABG 85 (6) 54 (5) 31 (9) 0.02
ACS: unstable angina 903 (67) 669 (67) 234 (68) 0.60
ACS: non-ST elevation MI 333 (25) 248 (25) 85 (25) 1.00
1 Dilated site 843 (63) 688 (68) 155 (45)
2 Dilated sites 370 (27) 260 (26) 110 (32) <0.0001
�3 Dilated sites 135 (10) 57 (6) 78 (23)
LAD n/N 771 (38) 512 (37) 259 (41)
RCA n/N 696 (34) 497 (36) 199 (31)
Cx n/N 513 (25) 352 (25) 161 (25) 0.18
LM n/N 16 (1) 9 (1) 7 (1)
Vein graft n/N 25 (1) 15 (1) 10 (2)
DES/total stents 518/2,300 (22) 358/1,539 (23) 160/761 (21) 0.24
Stented length (mm) 18 6 6 18 6 5 19 6 6 0.0013
Data are mean 6 SD or number (percent of total). ACS, acute coronary syndrome; MI, myocardial infarction; CABG, coronary artery bypass grafting;
LAD, left anterior descending coronary artery; RCA, right coronary artery; Cx, left circumflex coronary artery; LM, left main coronary artery; DES,
drug-eluting stent.aValues in parentheses indicate percentages.
*P value for the comparison between randomized and not-randomized patients.
TABLE II. 30-Day Events
Patients All (n 5 1,348) Randomized (n 5 1,005) Not randomized (n 5 343) P*
Composite 176 (13.1)a 104 (10.3) 72 (21.0) <0.0001
Death 2 (0.1) 0 (0) 2 (0.6) 0.065
MI 46 (3.4) 16 (1.6) 30 (8.7) <0.0001
Urgent revascularization 14 (1.0) 5 (0.5) 9 (2.6) 0.002
PCI 7 5 2 –
CABG 7 0 7 –
Repeat hospitalization 64 (4.7) 41 (4.1) 23 (6.7) 0.056
Access site complication 75 (5.6) 50 (5.0) 25 (7.3) 0.13
Major bleeding 19 (1.4) 5 (0.5) 14 (4.1) <0.0001
Thrombocytopenia 8 (0.6) 6 (0.6) 2 (0.6) 1.0
Events are expressed as numbers of patients (percent of total). Composite endpoint: death, MI, unplanned revascularization, major bleeding, repeat
hospitalization, severe thrombocytopenia, access site complications. No other access site complications than local hematomas occurred.aValues in parentheses indicate percentages.
*P value for the comparison between randomized and not-randomized patients. MI, myocardial infarction; PCI, percutaneous coronary intervention;
CABG, coronary artery bypass grafting.
Outcomes in Registry Patients 621
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

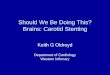
is shown in Fig. 1. Most events in not-randomized patientswere related to the index PCI and occurred early, whereasthe curve remained flat up to 60 days. Later, MACEevents slowly recurred and the curve remained steeper innot-randomized when compared with the randomizedpatients (log rank P< 0.0001).Within 30 days, two not-randomized patients died,
whereas no death occurred in the randomized patients.These two deaths occurred as PCI-related complica-tions while the patients were still hospitalized. The firstpatient developed aortic dissection during attempts to
dilate a right coronary artery. He underwent urgentCABG but sustained a massive stroke and died. Theother patient had a failed attempt to dilate a vein graftto a marginal branch and later died during repeat-CABG 2 days after PCI. At 12 months, there was nosignificant difference in the rates of death between therandomized and not-randomized patients (0.6% vs.1.5%, P 5 0.16). Similarly, although the cumulativeincidence of MI was significantly higher at 12 monthsin not-randomized patients (2.5% vs. 9.3%, P <0.0001), few MIs occurred beyond 30 days. In con-trast, TVR and revascularization rates in not-random-ized patients remained significantly higher than in the
TABLE III. Major Adverse Cardiac Events
Patients All (n 5 1348) Randomized (n 5 1005) Not randomized (n 5 343) P*
MACE
30 days 51 (3.8)a 16 (1.6) 35 (10.2) <0.0001
6 months 116 (8.6) 56 (5.6) 60 (17.5) <0.0001
1 year 174 (12.9) 90 (9.0) 84 (24.5) <0.0001
Death
30 days 2 (0.1) 0 (0) 2 (0.6) 0.065
6 months 4 (0.3) 1 (0.1) 3 (0.9) 0.053
1 year 11 (0.8) 6 (0.6) 5 (1.5) 0.16
MI
30 days 46 (3.4) 16 (1.6) 30 (8.7) <0.0001
6 months 50 (3.7) 19 (1.9) 31 (9.0) <0.0001
1 year 57 (4.2) 25 (2.5) 32 (9.3) <0.0001
TVR
30 days 9 (0.7) 1 (0.1) 8 (2.3) 0.0001
6 months 72 (5.3) 39 (3.9) 33 (9.6) 0.0001
1 year 120 (8.9) 65 (6.5) 55 (16.0) <0.0001
Revascularization at 1 year
PCI 108 (8.0) 70 (7.0) 38 (11) 0.02
CABG 40 (3.0) 12 (1.2) 28 (8.2) <0.0001
Events are expressed as numbers of patients (percent of total). MACE, death, MI, or target vessel revascularization.aValues in parentheses indicate percentages.
*P value for the comparison between randomized and not-randomized patients. MI, myocardial infarction; TVR, target vessel revascularization; PCI,
percutaneous coronary intervention; CABG, coronary artery bypass grafting.
Fig. 1. Major adverse cardiac events at 1 year: Kaplan–Meierestimates of the patients with the composite endpoint (death,MI, TVR) after study entry according to group assignment.[Color figure can be viewed in the online issue, which is avail-able at www.interscience.wiley.com.]
TABLE IV. Reasons for Exclusion to RandomizationPost-PCI (n 5 343)
Procedural data
Stented length >25 mm in one vessel 152 (44)a
PCI without stent implantation 56 (16)
Compromised or suboccluded branch with diameter �1 mm 55 (16)
Residual dissection of grade �B of NHBLI classification 33 (9.6)
Persisting chest pain 29 (8.5)
TIMI flow <3 poststenting 26 (7.6)
In-cath lab transient vessel closure 12 (3.5)
Entry site complication upon investigator decision 9 (2.6)
Thrombus post-PCI 4 (1.2)
Resuscitation pre-PCI 4 (1.2)
PCI, percutaneous coronary intervention. Numbers of patients (percent of
total). More than one reason per patient could be given.aValues in parentheses indicate percentages.
622 Bertrand et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

randomized at 30 days, 6 months, and 12 months (P <0.0001). After 30 days and after adjustment by multi-variate analysis for differences in baseline characteris-tics, exclusion from randomization remained an inde-pendent predictive factor for MACE at 12 months (HR1.41; 95% CI: 1.17–1.71, P 5 0.0005).
Assessment of Exclusion Criteria in PatientsNot Randomized Post-PCI
Exclusion criteria for same-day discharge used inpatients after PCI are given in Table IV. The onlyangiographic criteria were related to a stented length�25 mm. This criteria was in the original protocolapproved by Health Canada at study initiation but wasremoved later by amendment. This criteria was notidentified as a predictive factor for adverse outcomesat 30 days (HR 0.94, 95% CI 0.78–1.13, P 5 0.54) orfor MACE at 12 months (HR 1.04, 95% CI 0.86–1.24,P 5 0.67) in not-randomized when compared withrandomized patients.In patients not-randomized post-PCI, only transient
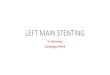
vessel closure during PCI was associated with anincreased risk of worse outcomes at 30 days (HR 1.63,95% CI 1.02–2.38, P 5 0.044). At 12 months, two cri-
teria were independent predictive factors of anincreased incidence of MACE, transient vessel closureduring PCI (HR 1.78, 95% CI 1.10–2.65, P 5 0.023)and a residual dissection grade � B of NHLBI classifi-cation after PCI (HR 1.53, 95% CI 1.11–2.05, P 50.011) (Fig. 2).
DISCUSSION
In this study, we show that simple criteria can beapplied in patients with acute coronary syndrome toidentify subjects, who require to remain hospitalizedafter transradial PCI and maximal antiplatelet therapy.Importantly, only criteria related to angiographic sub-optimal results or clinical complications were associ-ated with worse acute and late outcomes, albeit mostevents beyond the initial hospitalization phase con-sisted of repeated revascularization. These are impor-tant findings, which suggest that the most importantfactor to determine whether patients can be dischargedthe same day relates to PCI results, regardless of theclinical presentation of patients and associated risk.Indeed, in the EASY trial, the majority of patients hadacute coronary syndrome prior to the procedure. Other
Fig. 2. Clinical risk for patients not-randomized (hazard ratio and 95% confidence intervals):Hazard ratios and 95% CI for (A) the composite primary end point at 30 days and (B) MACEat 12 months after study entry in not-randomized patients according to exclusion criteriapost-PCI.
Outcomes in Registry Patients 623
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

randomized studies with same-day discharge typicallyexcluded acute coronary syndrome patients and the useof glycoproteins IIb/IIIa [7–9].Patients not randomized had more events, primarily
procedure-related, during the first 30 days comparedwith the randomized groups. However, our resultsshow that, even after 30 days, patients not-randomizedand who received maximal antiplatelet therapyremained a selected group at higher cardiovascularrisk, especially of repeat revascularization. It should beemphasized that our study population represent allcomers in a high volume catheterization laboratorywith limited exclusion criteria and that the MACE rateat 1 year in this study compares favorably with that ofother recent large trials involving abciximab [10–12].Our early and late results compare also favorably withother same-day discharge experience in lower-riskpatients and no use of glycoproteins IIb-IIIa receptorinhibitors [7]. Indeed, it should be reminded that allpatients underwent PCI through a transradial approachand that this approach was associated with anextremely low incidence of bleeding [1]. This mighthave played a role, considering the increasingly recog-nized importance of periprocedural bleeding as a riskfactor for MACE after PCI [13]. Our results also com-pare favorably with other PCI trials using bivalirudin,which have been shown to lessen the risk of bleedingafter PCI at least with the traditional femoral approach[14]. Whether bivalirudin could reduce even furtherthe risk of bleeding after PCI using a transradialapproach and hence, influences late outcomes, remainspresently unknown.Simple clinical and angiographic criteria were used
to exclude patients from randomization after PCI.Since patients had to be eligible for same-day homedischarge, exclusion criteria were related to safety con-cerns. A number of criteria have been previouslyreported in studies with same-day discharge [3]. Mostcriteria are related to suboptimal angiographic resultspost-PCI such as abnormal coronary flow, suspicion ofthrombus, or persisting dissection [7,8,15–17]. Theseabnormalities are known to be associated with adverseoutcomes within the first 24 hr after PCI and justifymaintaining patients under close clinical observation.Although surprising considering today practice, coro-nary stenting was initially proposed as an exclusioncriteria for same-day discharge [3]. In early studies,longer stented length had been identified as a risk fac-tor for stent thrombosis [18]. In this study, stentedlength �25 mm was initially an exclusion criteria, butthe protocol was later amended on the request of oper-ators who felt that PCI result was more important thanstented length. More recent studies involving thieno-pyridines had shown similar excellent early outcomes
with longer stents [19–23]. Indeed, our results showthat randomized and not-randomized patients withstented length �25 mm had similar early and late out-comes. Therefore, stented length by itself should notpreclude same-day discharge after maximal antiplatelettherapy. In patients not randomized, only transient ves-sel closure per-PCI and persisting � grade B dissectionpost-PCI remained significant independent predictivefactors of worse outcomes at 30 days and at 12 months.Persisting dissections after bare metal stents and drug-eluting stents have been previously recognized as riskfactors for adverse outcomes early after PCI, but itremains more controversial at later stages [24,25].Other procedural complications do not appear to jeop-ardize late outcomes of patients not randomized afterPCI.
Limitation
This is a post hoc analysis, which may have intro-duced some bias. However, these simple criteria areeasy to apply and, therefore, represent a first step toidentify patients requiring closer clinical follow-up.
Conclusion
Patients not randomized after PCI to same-day dis-charge for safety concerns in the EASY trial showedworse outcomes than randomized patients at 30 days,and 6 and 12 months. Simple clinical and angiographiccriteria are useful to identify patients at higher risk ofcardiovascular complications at the end of the proce-dure, regardless of the clinical presentation. Transientvessel closure and persisting moderate dissectionremain independent predictors of late adverse outcomesafter PCI with maximal antiplatelet therapy.
ACKNOWLEDGMENTS
This study was designed as an investigator-initiatedtrial. O.F. Bertrand and P. Poirier are research scholarsof the Quebec Foundation for Health Research. We aregrateful to Mr. S. Simard, MSc for statistical advice.
REFERENCES
1. Bertrand OF, De Larochelliere R, Rodes-Cabau J, Proulx G,
Gleeton O, Nguyen CM, Dery JP, Barbeau G, Noel B, Larose E,
et al. A randomized study comparing sameday home discharge
and abciximab bolus only to overnight hospitalization and abcix-
imab bolus and infusion after transradial coronary stent implan-
tation. Circulation 2006;114:2636–2643.
2. Bertrand OF, Rodes-Cabau J, Larose E, Nguyen CM, Roy L,
Dery JP, Courtis J, Nault I, Poirier P, Costerousse O, et al. One-
year clinical outcomes after abciximab bolus-only compared to
abciximab bolus and 12-hour infusion in the randomized early
discharge after transradial stenting of coronary arteries (EASY)
study. Am Heart J 2008.
624 Bertrand et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

3. Bertrand OF, Larose E, De Larochelliere R, Proulx G, Nguyen
CM, Dery JP, Gleeton O, Barbeau G, Noel B, Rouleau J, et al.
Outpatient percutaneous coronary intervention: Ready for prime
time? Can J Cardiol 2007;23:58B–66B.
4. Mangin L, Bertrand OF, De La Rochelliere R, Proulx G, Lemay
R, Barbeau G, Gleeton O, Rodes-Cabau J, Nguyen CM, Roy L.
The transulnar approach for coronary intervention: A safe alter-
native to transradial approach in selected patients. J Invas Car-
diol 2005;17:77–79.
5. Lincoff AM, Bittl JA, Harrington RA, Feit F, Kleiman NS, Jack-
man JD, Sarembock IJ, Cohen DJ, Spriggs D, Ebrahimi R, et al.
Bivalirudin and provisional glycoprotein IIb/IIIa blockade com-
pared with heparin and planned glycoprotein IIb/IIIa blockade
during percutaneous coronary intervention: REPLACE-2 rando-
mized trial. JAMA 2003;289:853–863.
6. Cannon CP, Battler A, Brindis RG, Cox JL, Ellis SG, Every
NR, Flaherty JT, Harrington RA, Krumholz HM, Simoons ML,
et al. American College of Cardiology key data elements and
definitions for measuring the clinical management and outcomes
of patients with acute coronary syndromes. A report of the
American College of Cardiology Task Force on Clinical Data
Standards (Acute Coronary Syndromes Writing Committee).
J Am Coll Cardiol 2001;38:2114–2130.
7. Heyde GS, Koch KT, de Winter RJ, Dijkgraaf MG, Klees MI,
Dijksman LM, Piek JJ, Tijssen JG. Randomized trial comparing
same-day discharge with overnight hospital stay after percutane-
ous coronary intervention: Results of the Elective PCI in Outpa-
tient Study (EPOS). Circulation 2007;115:2299–2306.
8. Kiemeneij F, Laarman GJ, Slagboom T, van der Wieken R. Out-
patient coronary stent implantation. J Am Coll Cardiol 1997;29:
323–327.
9. Slagboom T, Kiemeneij F, Laarman GJ, van der Wieken R. Out-
patient coronary angioplasty: Feasible and safe. Catheter Cardio-
vasc Interv 2005;64:421–427.
10. Anderson KM, Califf RM, Stone GW, Neumann FJ, Montalescot
G, Miller DP, Ferguson JJ III, Willerson JT, Weisman HF,
Topol EJ. Long-term mortality benefit with abciximab in
patients undergoing percutaneous coronary intervention. J Am
Coll Cardiol 2001;37:2059–2065.
11. Lincoff AM, Kleiman NS, Kereiakes DJ, Feit F, Bittl JA, Jack-
man JD, Sarembock IJ, Cohen DJ, Spriggs D, Ebrahimi R, et al.
Long-term efficacy of bivalirudin and provisional glycoprotein
IIb/IIIa blockade vs heparin and planned glycoprotein IIb/
IIIa blockade during percutaneous coronary revascularization:
REPLACE-2 randomized trial. JAMA 2004;292:696–703.
12. Mukherjee D, Topol EJ, Bertrand ME, Kristensen SD, Herrmann
HC, Neumann FJ, Yakubov SJ, Bassand JP, McClure RR, Stone
GW, et al. Mortality at 1 year for the direct comparison of tirofi-
ban and abciximab during percutaneous coronary revasculariza-
tion: Do tirofiban and ReoPro give similar efficacy outcomes at
trial 1-year follow-up. Eur Heart J 2005;26:2524–2528.
13. Manoukian SV, Feit F, Mehran R, Voeltz MD, Ebrahimi R,
Hamon M, Dangas GD, Lincoff AM, White HD, Moses JW,
et al. Impact of major bleeding on 30-day mortality and clinical
outcomes in patients with acute coronary syndromes: An analy-
sis from the ACUITY Trial. J Am Coll Cardiol 2007;49:1362–
1368.
14. Stone GW, White HD, Ohman EM, Bertrand ME, Lincoff AM,
McLaurin BT, Cox DA, Pocock SJ, Ware JH, Feit F, et al. Biva-
lirudin in patients with acute coronary syndromes undergoing
percutaneous coronary intervention: A subgroup analysis from
the Acute Catheterization and Urgent Intervention Triage strat-
egy (ACUITY) trial. Lancet 2007;369:907–919.
15. Kiemeneij F, Laarman GJ, Slagboom T, Stella P. Transradial
palmaz-schatz coronary stenting on an outpatient basis: Results
of a prospective pilot study. J Invas Cardiol 1995;7:5A–11A.
16. Koch KT, Piek JJ, Prins MH, de Winter RJ, Mulder K, Lie KI,
Tijssen JG. Triage of patients for short term observation after
elective coronary angioplasty. Heart 2000;83:557–563.
17. Slagboom T, Kiemeneij F, Laarman GJ, van der Wieken R,
Odekerken D. Actual outpatient PTCA: Results of the OUT-
CLAS pilot study. Catheter Cardiovasc Interv 2001;53:204–208.
18. Cutlip DE, Baim DS, Ho KK, Popma JJ, Lansky AJ, Cohen DJ,
Carrozza JP Jr, Chauhan MS, Rodriguez O, Kuntz RE. Stent
thrombosis in the modern era: A pooled analysis of multicenter
coronary stent clinical trials. Circulation 2001;103:1967–1971.
19. Antoniucci D, Valenti R, Santoro GM, Bolognese L, Trapani M,
Fazzini PF. Preliminary experience with stent-supported coro-
nary angioplasty in long narrowings using the long freedom
force stent: Acute and six-month clinical and angiographic
results in a series of 27 consecutive patients. Cathet Cardiovasc
Diagn 1998;43:163–167.
20. Cheneau E, Leborgne L, Mintz GS, Kotani J, Pichard AD, Satler
LF, Canos D, Castagna M, Weissman NJ, Waksman R. Predic-
tors of subacute stent thrombosis: Results of a systematic intra-
vascular ultrasound study. Circulation 2003;108:43–47.
21. Kobayashi Y, De Gregorio J, Kobayashi N, Akiyama T, Reimers
B, Finci L, Di Mario C, Colombo A. Stented segment length as
an independent predictor of restenosis. J Am Coll Cardiol
1999;34:651–659.
22. Kornowski R, Bhargava B, Fuchs S, Lansky AJ, Satler LF,
Pichard AD, Hong MK, Kent KM, Mehran R, Stone GW, et al.
Procedural results and late clinical outcomes after percutaneous
interventions using long (> or 5 25 mm) versus short (<20 mm)
stents. J Am Coll Cardiol 2000;35:612–618.
23. Le Breton H, Bedossa M, Commeau P, Boschat J, Huret B,
Gilard M, Brunel P, Crochet D, Grollier G, Douillet R, et al.
Clinical and angiographic results of stenting for long coronary
arterial atherosclerotic lesions. Am J Cardiol 1998;82:1539–
1543.
24. Alfonso F, Hernandez R, Goicolea J, Segovia J, Perez-Vizcayno
MJ, Banuelos C, Silva JC, Zarco P, Macaya C. Coronary stent-
ing for acute coronary dissection after coronary angioplasty:
Implications of residual dissection. J Am Coll Cardiol 1994;24:
989–995.
25. Biondi-Zoccai GG, Agostoni P, Sangiorgi GM, Airoldi F, Cos-
grave J, Chieffo A, Barbagallo R, Tamburino C, Vittori G, Fal-
chetti E, et al. Incidence, predictors, and outcomes of coronary
dissections left untreated after drug-eluting stent implantation.
Eur Heart J 2006;27:540–546.
Outcomes in Registry Patients 625
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).