Embed Size (px)
Citation preview

E012672D 1
Malignancy Induced Weight Loss
Malignancy Induced Weight Loss
N. Joseph Espat MD MS FACS
Associate Professor
Hepatobiliary Surgery and Pharmacology
University of Illinois at Chicago

E012672D 2
Surgery
Nutrition
Inflammation
Oncology
Surgery
Nutrition
Inflammation
Oncology
INTEGRATING SEVERAL DISCIPLINES

E012672D 3
History Of Intravenous NutritionHistory Of Intravenous Nutrition• 1628: (Harvey)-discovery of blood circulation
• 1869: (Menzel, Perco)-injection of oil into subcutaneous tissue
• 1930’s: commercial IV Fluid
• 1952: (Aubaniac) reports subclavian access
• 1968: Dudrick’s work with puppies
• 1977: HAL for radiation patients (Copeland)
• 1628: (Harvey)-discovery of blood circulation
• 1869: (Menzel, Perco)-injection of oil into subcutaneous tissue
• 1930’s: commercial IV Fluid
• 1952: (Aubaniac) reports subclavian access
• 1968: Dudrick’s work with puppies
• 1977: HAL for radiation patients (Copeland)

E012672D 4

E012672D 5
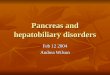
Weight Loss: Patients with CancerWeight Loss: Patients with Cancer
-80%
-60%
-40%
-20%
0%
5-10% >10%
Weight loss in previous 6 months
Colon Prostate
Lungsmallcell
Lungnon-small
cell Pancreas
Non-measurable
gastricMeasurable
gastric
14%
14%
18%
10%
20%
14%
21%
15%
28%
26%
32%
30%
29%
38%
DeWys et al. 1980. Am J Med. 69:491
% P
atie
nts
with
Wei
ght
Loss

E012672D 6
WHY DO CANCER PATIENTS DIE?WHY DO CANCER PATIENTS DIE?

E012672D 7
Causes of Cancer-Induced Weight LossCauses of Cancer-Induced Weight Loss• Mechanical obstruction of ingestion
• Treatment-related effects
• Tumor-related effects (cancer cachexia)
• Mechanical obstruction of ingestion
• Treatment-related effects
• Tumor-related effects (cancer cachexia)
Rivadeneira et al. 1998. CA Cancer J Clin. 48:69

E012672D 8
Tumor-Related Causesof Weight LossTumor-Related Causesof Weight Loss• Anorexia and early satiety
• Accelerated loss of protein and fat
• Altered energy metabolism
• Increased resting energy expenditure
• Anorexia and early satiety
• Accelerated loss of protein and fat
• Altered energy metabolism
• Increased resting energy expenditure
Rivadeneira et al. 1998. CA Cancer J Clin. 48:69

E012672D 9
Therapeutic Challenges Therapeutic Challenges • Reversible cancer-
induced weight loss– Mechanical causes
– Treatment-related causes
• Reversible cancer-induced weight loss
– Mechanical causes
– Treatment-related causes
• Tumor-related weight loss– Metabolic abnormalities
• Tumor-related weight loss– Metabolic abnormalities
Provision of energy and protein can promote
weight gain
Provision of energy and protein can promote
weight gain
No weight gain, even when added energy and
protein are provided
No weight gain, even when added energy and
protein are provided
Ottery FD. 1994. Cancer Practice. 2:123

E012672D 10
Metabolic Changes:Cachexia vs. StarvationMetabolic Changes:Cachexia vs. Starvation
Cachexia Starvation
Body Weight – /
Body Cell Mass (Lean Body Mass)
Body Fat
Caloric Intake
Total Energy Expenditure (EE)
Resting EE
Protein Synthesis /
Protein Degradation
Proteolysis-Inducing Factor (PIF) –
Adapted from Kotler DP. 2000. Ann Intern Med. 133:622

E012672D 11
Nutrition BasicsNutrition Basics

E012672D 12
GlucoseGlucose• 1 gram = 3.4 Kcals
• 1200 Kcals stored in the as glycogen– 800Kcals in muscle
– 400Kcals in liver
• Only form of energy used under usual conditions by brain and blood cells
• Enters cells under the control of insulin and trapped by phosphorylation except in the kidney and liver
• 1 gram = 3.4 Kcals
• 1200 Kcals stored in the as glycogen– 800Kcals in muscle
– 400Kcals in liver
• Only form of energy used under usual conditions by brain and blood cells
• Enters cells under the control of insulin and trapped by phosphorylation except in the kidney and liver

E012672D 13
FATFAT
• 1gram =9 calories
• 15 Kg in body as fat ( 135,000 Kcals)
• Transported as free fatty acids, converted to ketones in starvation
• Released by cathecholamines and decreased release by insulin
• Made in the liver and adipose tissue-requires protein to remove from the liver
• 1gram =9 calories
• 15 Kg in body as fat ( 135,000 Kcals)
• Transported as free fatty acids, converted to ketones in starvation
• Released by cathecholamines and decreased release by insulin
• Made in the liver and adipose tissue-requires protein to remove from the liver

E012672D 14
ProteinProtein• 1 gram of nitrogen =6.25 grams protein = 30
grams of muscle
• GI absorbed protein: 57% urea, 6% plasma, 23% free AA and 14% liver
• Nitrogen balance =
gms N intake – (gms urine urea N +4)
• 1 gram of nitrogen =6.25 grams protein = 30 grams of muscle
• GI absorbed protein: 57% urea, 6% plasma, 23% free AA and 14% liver
• Nitrogen balance =
gms N intake – (gms urine urea N +4)

E012672D 15
SARCOPENIA (this is normal)SARCOPENIA (this is normal)• diminished reserves of muscle or lean body
mass leading to reduced strength , power and endurance .
• 40% of lean body mass is lost between ages 25-70.
• diminished reserves of muscle or lean body mass leading to reduced strength , power and endurance .
• 40% of lean body mass is lost between ages 25-70.

E012672D 16
Starvation (fasting)Starvation (fasting)
Simple starvation (caloric restriction) is characterized by the loss of hepatic mass with relative sparing of peripheral proteins and lean body mass.
Simple starvation (caloric restriction) is characterized by the loss of hepatic mass with relative sparing of peripheral proteins and lean body mass.

E012672D 17
Simple Starvation ( 1st phase)Simple Starvation ( 1st phase)• 2-4 days increased urine N loss
• Use of glycogen
• Insulin falls, glucagon increases– Protein-glucose
– Fat-FFA
Increased loss of Na and water (180-300 gms muscle + 150-250 gms fat )
• 2-4 days increased urine N loss
• Use of glycogen
• Insulin falls, glucagon increases– Protein-glucose
– Fat-FFA
Increased loss of Na and water (180-300 gms muscle + 150-250 gms fat )

E012672D 18
Simple Starvation ( 2nd phase)Simple Starvation ( 2nd phase)• Decreased urinary N loss over 20-40 days
• Decrease metabolic rate
• Efficient use of fat
• Decreased urinary N loss over 20-40 days
• Decrease metabolic rate
• Efficient use of fat

E012672D 19
Simple Starvation (3rd phase)Simple Starvation (3rd phase)• Keto-adaptation
• N loss falls to 2-4 grams QD
• Obligate tissues like brain adapt to ketones
• DEATH is by respiratory failure – Intercostal muscles
– pneumonia
• Keto-adaptation
• N loss falls to 2-4 grams QD
• Obligate tissues like brain adapt to ketones
• DEATH is by respiratory failure – Intercostal muscles
– pneumonia

E012672D 20
Cachexia
The loss of lean body mass, peripheral proteolysis with sparing of hepatic mass and selectively increased protein synthesis seen with trauma, sepsis, and malignancy is termed cachexia.

E012672D 21
“the failure of nutritional repletion despite adequate caloric
intake in patients with malignancy”
Or
“starvation in the midst of plenty”

E012672D 22
CachexiaCachexia• Losses are in excess of caloric restriction alone
(anorexia, inanition)
• Accompanied by other metabolic derangements such as anemia, acute-phase induction, alterations in plasma lipid profile
• Losses are in excess of caloric restriction alone (anorexia, inanition)
• Accompanied by other metabolic derangements such as anemia, acute-phase induction, alterations in plasma lipid profile

E012672D 23
Liver Cirrhosis-CachexiaLiver Cirrhosis-Cachexia• Reduction in total body nitrogen
• Reduction in total body cell mass
• Increased total body water
• PIC and endotoxemia involved
• Hypermetabolic
• TNF I and II receptors, CD14
• Reduction in total body nitrogen
• Reduction in total body cell mass
• Increased total body water
• PIC and endotoxemia involved
• Hypermetabolic
• TNF I and II receptors, CD14

E012672D 24

E012672D 25
Cancer- CachexiaCancer- Cachexia• Depends on the type of cancer
• Lymphoma & breast cancer vs. GI tumors
• 1/3 hypermetabolic and 1/3 hypometabolic
• Ubiquitin-proteasome pathway-(determinant?)
• Depends on the type of cancer
• Lymphoma & breast cancer vs. GI tumors
• 1/3 hypermetabolic and 1/3 hypometabolic
• Ubiquitin-proteasome pathway-(determinant?)

E012672D 26
Cytokines Mediate Acute Phase Protein Response (APPR)
Cytokines Mediate Acute Phase Protein Response (APPR)• APPR – hormonal, cytokine-mediated response
to stress, trauma, inflammation or cancer
protein synthesis in liver (CRP, haptoglobin, ceruloplasmin)
• Some of acute phase proteins are composed of amino acids derived from muscle tissue
• APPR – hormonal, cytokine-mediated response to stress, trauma, inflammation or cancer
protein synthesis in liver (CRP, haptoglobin, ceruloplasmin)
• Some of acute phase proteins are composed of amino acids derived from muscle tissue

E012672D 27
Acute Inflammatory Response• the soluble protein mediators of the acute phase
inflammatory response are termed cytokines.
• Tumor Necrosis Factor (TNF) and Interleukin-1 (IL-1) are the principal mediators of this response. Both induce IL-6, which is the key regulatory cytokine of hepatic acute phase protein synthesis.
• End organ level regulators of the inflammatory response continue to be a focus of study.

E012672D 28
Classic Pro-Inflammatory Cytokines• TNF
• IL-1
• IL-6
• INF-
Inflamatory stimuli induce these first-line mediators of the “acute inflamatory
response”.

E012672D 29
CYTOKINESCYTOKINES• small, non-structural proteins which serve as
chemical messengers between cells
• involved in processes such as normal growth and development
• Immune response to acute and chronic inflammation
• small, non-structural proteins which serve as chemical messengers between cells
• involved in processes such as normal growth and development
• Immune response to acute and chronic inflammation

E012672D 30
WHAT WE KNOWWHAT WE KNOW• Lean body mass is the most consistent predictor
of survival in cancer patients
• Hepatic uptake of nutrients is modified during inflammatory states
• Cachexia is a complex of clinical syndromes
• Inducible COX-2 enzymes are at the center of inflammation
• Lean body mass is the most consistent predictor of survival in cancer patients
• Hepatic uptake of nutrients is modified during inflammatory states
• Cachexia is a complex of clinical syndromes
• Inducible COX-2 enzymes are at the center of inflammation

E012672D 31
mRNA
NFB
NFB-IB
TNF
IL-1
IB-p
IB Phos-
26S-PEPA
NFB pathway in Macrophages
P38
IL-10

E012672D 32
2
11
3
4
5
66

E012672D 33
FIGURE 1Ubiquitin-Associated Proteolytic System
E1 Activating Enzyme
UbiquitinE2-carrier
enzyme
E3 Protein LigaseEnzyme
Protein
20S Proteasome
Peptide Fragments
PA700
ATP ADP

E012672D 34
Central Role of CytokinesCentral Role of CytokinesMalignant tumor cells Inflammatory response begins
Cytokine production IL-1, IL-6 TNF-
Metabolism of macronutrients
affectedLoss of LBM
Acute phaseprotein response
initiated( CRP)
Weight loss
REE Food intake
Proteolysis inducing
factor
Depressed Appetite

E012672D 35
Tumor-Related Weight Loss: OutcomesTumor-Related Weight Loss: Outcomes Quality of Life
Functional Status
Response to Therapy
Body Image
Hospital Length of Stay
Unscheduled Hospitalization
Complications/Infections
Quality of Life
Functional Status
Response to Therapy
Body Image
Hospital Length of Stay
Unscheduled Hospitalization
Complications/Infections

E012672D 36
Cancer and Weight Loss Current Treatments: Summary
Cancer and Weight Loss Current Treatments: Summary• Progestins: Megestrol acetate/Medroxyprogesterone
acetate
• Dronabinol: results worse
• Corticosteroids: short term appetite only
• Supplements/Dietary Counseling also not effective
• Progestins: Megestrol acetate/Medroxyprogesterone acetate
• Dronabinol: results worse
• Corticosteroids: short term appetite only
• Supplements/Dietary Counseling also not effective
Studies have not demonstrated improvement in nutritional status, LBM, quality of life, or survival.
Side effects are a major problem.
Studies have not demonstrated improvement in nutritional status, LBM, quality of life, or survival.
Side effects are a major problem.
Current interventions are unsatisfactory.Current interventions are unsatisfactory.

E012672D 37
Cancer and Weight LossCancer and Weight Loss
• Current interventions have only been able to influence appetite but notmajor clinical outcomes
• There is a critical need to identify new interventions which can favorably influence clinically relevant outcomes
Treatment should address the underlying mechanism

E012672D 38
Inflammatory
Immune suppressive
Appropriate response to “primary pathway” stimulus)
Exaggerated of prolonged“appropriate” response to “primary pathway” stimulus)
Inflammation: Good or Bad ?
Anti-inflammatory

E012672D 39
EPAEPA
• Long-chain polyunsaturated fatty acid of the -3 family
-3 fatty acids are essential dietary components
• Main source is oily fish
• Typical intake around 0.1 g per day
• Long-chain polyunsaturated fatty acid of the -3 family
-3 fatty acids are essential dietary components
• Main source is oily fish
• Typical intake around 0.1 g per day
Eicosapentaenoic Acid (EPA)
C OHO

E012672D 40
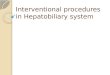
Reprinted from Nutrition Vol. 12, Wigmore SJ, Ross JA, Falconer JS, et al. The effect of polyunsaturated fatty acids on the progress of cachexia in patients with pancreatic cancer, p. S27-S30, 1996, with permission from Elsevier Science.
Fatty Acids and Cancer CachexiaFatty Acids and Cancer Cachexia
Weight change before and after a median of 3 months supplementation with fish oil in patients with unresectable pancreatic cancer (n=18)
Cha
nge
in W
eigh
t kg
/mon
th
-8
-7
-6
-5
-4
-3
-2
-1
0
1
2
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Before EPA
EPA

E012672D 41
Wigmore. 2000. Nutrition and Cancer. 36:177
EPA: Clinical Trials in Cancer PatientsEPA: Clinical Trials in Cancer Patients
EPAStarted
Time (months)
25
20
15
10
5
0
-5
-10
-15
-20
Wei
ght
Cha
nge
(kg)
-10 -8 -6 -4 -2 0 108642 12 14 16 18

E012672D 42
Summary: Roles of EPASummary: Roles of EPA Inflammatory response
Pro-inflammatory cytokine production
• Attenuates APPR
Level/activity of proteolysis-inducing factor (PIF)
• Attenuates tumor-related weight loss
• Increases survival
Inflammatory response
Pro-inflammatory cytokine production
• Attenuates APPR
Level/activity of proteolysis-inducing factor (PIF)
• Attenuates tumor-related weight loss
• Increases survival

E012672D 43
HypothesisHypothesis
If fish oil (EPA) stabilizes weight by suppressing metabolic changes in
cancer, EPA in combination with energy and protein will result in weight gain.

E012672D 44
“Effect of an oral nutritional supplement enriched with fish oil
on weight loss in patients with pancreatic cancer.”
“Effect of an oral nutritional supplement enriched with fish oil
on weight loss in patients with pancreatic cancer.”
Barber et al. Brit J Nutr. 1999;81:80

E012672D 45
Experimental ProductExperimental Product• 240 mls per serving
• 301 kcal (1.26 kcal/ml)
• Protein: 16 g
• Carbohydrate: 44 g
• Fiber: 5 g (2.4 g FOS)
• Fat: 6 g– EPA: 1.09 g– DHA: 0.44 g
• Enhanced with antioxidants (vitamins A, C, E and Se)
• 240 mls per serving
• 301 kcal (1.26 kcal/ml)
• Protein: 16 g
• Carbohydrate: 44 g
• Fiber: 5 g (2.4 g FOS)
• Fat: 6 g– EPA: 1.09 g– DHA: 0.44 g
• Enhanced with antioxidants (vitamins A, C, E and Se)

E012672D 46
Clinical StudyClinical StudyDesign
• Patients with unresectable pancreatic cancer (n=20)
• 2 servings per day for up to 7 weeks
Design
• Patients with unresectable pancreatic cancer (n=20)
• 2 servings per day for up to 7 weeks
Outcome Measures
• Patients weighed at baseline, and wks 3 and 7
• Nutritional intake
• Performance and appetite
• Resting energy expenditure
• C-reactive protein
Outcome Measures
• Patients weighed at baseline, and wks 3 and 7
• Nutritional intake
• Performance and appetite
• Resting energy expenditure
• C-reactive protein
Barber et al. Brit J Nutr. 1999;81:80

E012672D 47
Weight Change After SupplementationWeight Change After Supplementation
-5
0
5
10
15
20
25
30
35
supplementstarted
Time (months)
-10 -8 -6 -4 -2 0 2 4 6 8 10
Barber et al. Brit J Nutr. 1999;81:80
Mean Intake 1.9 servings/dMean Intake 1.9 servings/d
Wei
ght C
hang
e (k
g)

E012672D 48
Results of Multicenter Clinical Trial in Pancreatic
Cancer
Results of Multicenter Clinical Trial in Pancreatic
Cancer
Fearon KCH. 2001; Eur J Cancer 37:27S

E012672D 49
Why Study Pancreatic Cancer Patients?Why Study Pancreatic Cancer Patients?• Dramatic weight loss• Smaller sample size• Shorter study duration
• Dramatic weight loss• Smaller sample size• Shorter study duration
-35
-30
-25
-20
-15
-10
-5
0
Wei
ght L
oss
(kg)
PancreaticCancer
LungCancer
Wigmore SJ. British J Cancer 1997;75:106 Staal-van den Brekel AJ. Cancer Research 1994;54:6430
-4 -3 -1-2 10 2 43 65 Time (months)

E012672D 50
Study DesignStudy Design• Prospective, double-blind, randomized,
multi-center trial
• Unresectable pancreatic cancer (n=200)
• High protein, energy dense oral supplement with or without EPA and enhanced antioxidants
• Prospective, double-blind, randomized, multi-center trial
• Unresectable pancreatic cancer (n=200)
• High protein, energy dense oral supplement with or without EPA and enhanced antioxidants
Fearon KCH. 2001; Eur J Cancer 37:27S

E012672D 51
Outcome Measures for StudyOutcome Measures for Study1. Body weight and body composition (LBM)
2. Quality of Life
3. Change in Acute Phase Proteins
4. Appetite and total dietary Intake
5. Functional status– Grip strength
– Karnofsky performance status
1. Body weight and body composition (LBM)
2. Quality of Life
3. Change in Acute Phase Proteins
4. Appetite and total dietary Intake
5. Functional status– Grip strength
– Karnofsky performance status

E012672D 52
Study Supplement Comparison Study Supplement Comparison Control/Experimental
• 300 kcal per serving
• Protein – 16 g
• Carbohydrate – 50 g
• Fiber – 5 g (2.6 g FOS)
• Fat – 6 g
Control/Experimental
• 300 kcal per serving
• Protein – 16 g
• Carbohydrate – 50 g
• Fiber – 5 g (2.6 g FOS)
• Fat – 6 g
Experimental Product
• EPA – 1.09 g
• DHA – 0.46 g
• Enhanced antioxidants (vitamins A, C, E and Se)
Experimental Product
• EPA – 1.09 g
• DHA – 0.46 g
• Enhanced antioxidants (vitamins A, C, E and Se)

E012672D 53
Effect on Weight ChangeEffect on Weight Change
Wei
ght (
kg/m
onth
)
Fearon KCH. 2001. Eur J Cancer. 37:27S
-4
-3
-2
-1
0
1
2
Baseline 4 Weeks 8 Weeks
Control
ProSure
n=96 n=88 n=78 n=70 n=60 n=50
-3.18-2.92
-0.13 -0.09-0.38 -0.26
p=NS

E012672D 54
Change in Lean Body MassChange in Lean Body Mass
Lean
Bod
y M
ass
(kg/
mon
th)
-3
-2
-1
0
1
2
Baseline 4 Weeks 8 Weeks
Control
ProSure
n=90 n=80
n=68 n=630 n=56 n=41
-2.35
-2.01
0.380.74
0.12 0.27
p=NS

E012672D 55
Change in Weight and Lean Body Mass at 8 WeeksChange in Weight and Lean Body Mass at 8 Weeks
kg (
chan
ge)
-6
-5
-4
-3
-2
-1
0
1
2
0-0.5 can 0.5-1.0 can 1.0-1.5 can 1.5-2.0 can
Weight
Lean Body Mass
n=6 n=3 n=8 n=8 n=10
n=8 n=26 n=22

E012672D 56
Recommended Intake (1.5-2.0 cans/day) Change in Wt and LBM at 8 Weeks
Recommended Intake (1.5-2.0 cans/day) Change in Wt and LBM at 8 Weeks
0.46
0.09
1.21
1.46
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Wt LBM
Control
ProSure
0.46
0.09
1.21
1.46
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Wt LBM
Control
ProSure
p=NS
Kilo
gram
s
n=30 n=28n=26 n=22

E012672D 57
Consumption vs. Lean Body MassConsumption vs. Lean Body Mass
-10-8-6-4-202468
10
0 0.5 1 1.5 2
-10-8-6-4-202468
10
0 0.5 1 1.5 2
Fearon KCH. 2001; Eur J Cancer 37:27S
Unit Intake (cans)
Lea
n B
ody
Mas
s (k
g)
Unit Intake (cans)
Lea
n B
ody
Mas
s (k
g)
P=0.036 r=0.332
P=NS
Experimental
Control

E012672D 58
Parallel Study of Physical Activity Level As an Objective Measure of Quality of Life
Parallel Study of Physical Activity Level As an Objective Measure of Quality of Life
• Total energy expenditure/Resting energy expenditure = Physical activity level
• TEE – measured using doubly labeled water
• REE – measured by indirect calorimetry
• Physical activity level– ~1.1 Morbid– ~1.5 Normal– ~1.8 Active
• Total energy expenditure/Resting energy expenditure = Physical activity level
• TEE – measured using doubly labeled water
• REE – measured by indirect calorimetry
• Physical activity level– ~1.1 Morbid– ~1.5 Normal– ~1.8 Active

E012672D 59
Effect on Physical Activity LevelEffect on Physical Activity Level
TE
E/R
EE
Phy
sica
l Act
ivity
Lev
el
Control Group (n=12) Experimental Group (n=7)
1.23
1.321.29
1.48
1.0
1.1
1.2
1.3
1.4
1.5
1.6
Baseline 8 Weeks Baseline 8 Weeks
NormalSedentary
Level
Confinedto Bed
p=NS p=0.005
Moses et al. 2001 Clin Nutr 20:21

E012672D 60
Weight Change vs. QLQ-C30 Physical FunctionWeight Change vs. QLQ-C30 Physical Function
-60
-40
-20
0
20
40
60
-10 -5 0 5 10
-60
-40
-20
0
20
40
60
-10 -5 0 5 10
Weight Change (kg)
QL
Q-C
30 P
hysi
cal F
unct
ion
n=49, r=0.33, p=0.02

E012672D 61
Total Energy and Protein Intake (experimental group)Total Energy and Protein Intake (experimental group)
0
500
1000
1500
2000
Baseline 8 Weeks
p=0.001
Bauer et al. Nutrition Week. 2002
p=0.001
Cal
orie
s (k
cal)
0
20
40
60
80
Baseline 8 Weeks
Pro
tein
(g)
78
63
1800
1465

E012672D 62
ConclusionConclusion• It appears to be the combination of energy and
protein with EPA and antioxidants is effective in improving nutritional status in patients with cancer-induced weight loss
• Need for biological markers of oral supplement consumption
• Need for further randomized trials
• It appears to be the combination of energy and protein with EPA and antioxidants is effective in improving nutritional status in patients with cancer-induced weight loss
• Need for biological markers of oral supplement consumption
• Need for further randomized trials

E012672D 63
QUESTIONSQUESTIONS




![Clinical and Therapeutic Implications of Aeromonas Bacteremia: … · 2016-12-28 · Aeromonas bacteremia are malignancy and hepatobiliary dis-eases [5]. Aeromonas spp. tend to produce](https://img.dokumen.tips/doc/110x75/5ec79db8c2bd727c0b32cc58/clinical-and-therapeutic-implications-of-aeromonas-bacteremia-2016-12-28-aeromonas.jpg)