Embed Size (px)
Citation preview

DSM-5:Substance Related & Addictive
Disorders
Charles P. O’Brien, M.D., Ph.D.
University of Pennsylvania
Philadelphia, PA

• Familiar to everyone
• Criteria first published in 1994
• Text but not criteria updated in 2000
• Used worldwide for diagnosis, education, research and reimbursement purposes

Columbia University Deborah Hasin, Ph.D .
Wilson Compton, M.D.
Bridget Grant, Ph.D. , Ph.D.
Deborah Hasin , Ph.D.
Walter Ling, M.D.
Nancy Petry, Ph.D.
Marc Schuckit M.D.
Charles O’Brien, M.D., chair
Marc Auriacombe, M.D
Guilherme Borges, Ph.D.
Katherine Buchholz, Ph.D.
Alan Budney, Ph.D.
Thomas Crowley, M.D.
DSM-5 Substance Disorder Workgroup members

BUTBio-markers in psychiatry are notsufficiently reliable and availablefor clinical practice
NIMH Research Domain CriteriaRDoC
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,
(Copyright © 2013). American Psychiatric Association. All rights reserved.


Abuse Dependence Diagnostic Criteria
Failure to fulfill major role obligations X --
Hazardous use X --
Substance-related legal problems X --
Social/interpersonal substance-related problems X --
Tolerance -- X
Withdrawal -- X
Persistent desire/unsuccessful efforts to cut down -- X
Using more or over for longer than was intended -- X
Neglect of important activities -- X
Great deal of time spent in substance activities -- X
Psychological/Physical use-related problems -- X
Diagnostic Threshold 1+ criteria 3+ criteria
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000.
1+
3+
Substance Use Disorder Criteria: DSM-IV
Columbia University Deborah Hasin, Ph.D .

What should be done about abuse, specifically, should abuse be combined with dependence to create a single disorder?
Should new criteria be added, e.g., craving or old criteria (legal problems) be removed?
Can nicotine criteria be aligned with other substances?
Can cannabis and caffiene withdrawal be included?
What should be the diagnostic threshold, how should severity be indicated?
International considerations
Columbia University Deborah Hasin, Ph.D .
• Confusion about relationship of abuse to dependence because abuse is assumed to be milder than dependence
– Leads to thinking abuse is prodromal to dependence
– Leads to thinking all cases of dependence meet criteria for abuse
• Reliability and validity of dependence is excellent
• Reliability and validity of abuse much lower, more variable than dependence
• ~50% with abuse dx’ed with only 1 criterion: hazardous use
• Diagnostic “orphans” (2 dependence criteria, no dx)
Columbia University Deborah Hasin, Ph.D .

• Many factor analyses showed abuse and dependence criteria formed 1 factor, or 2 highly correlated factors
• Item Response Theory analysis extends factor analysis, provideing more information
• Item characteristic curves (graphed) show relationship of abuse and dependence criteria to each other
• Total information curves (TOC) allow comparison of two or more sets of criteria
Columbia University Deborah Hasin, Ph.D .

Sample # Studies Ns Locations
Adult general population 17 722 - 43,093 Australia, Israel, US
Adult emergency room2 5,195
Argentina, Mexico, Poland, US
Adult substance abuse treatment
5 372 - 1,511 Australia, US
Adult genetic studies 4 496 - 9,313 US
Adolescent general population
4 353 - 3,641 France, US
Adolescent substance abuse treatment
2 279 - 472 US
Adolescent mixed 2 5,587 US
Columbia University Deborah Hasin, Ph.D .

0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
-3.0
0
-2.8
0
-2.6
0
-2.4
0
-2.2
0
-2.0
0
-1.8
0
-1.6
0
-1.4
0
-1.2
0
-1.0
0
-0.8
0
-0.6
0
-0.4
0
-0.2
0
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
2.00
2.20
2.40
2.60
2.80
3.00
Severity of Alcohol Use Disorder (Latent Trait)
Pro
ba
bili
ty o
f S
ym
pto
m E
nd
ors
em
en
t
Tolerance Withdrawal Larger/longer Quit/control
Time spent Activities given up Physical/psychological problems Neglect roles
Hazardous use Legal problems Social/Interpersonal problems
Quit controlHazardous use
ToleranceWithdrawal
Saha, Grant et al., Drug and Alcohol Dependence 2007
NESARC (2001-2002) ICC Current Alcohol Abuse, Dependence (N=22,526)
Columbia University Deborah Hasin, Ph.D .

0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
-3 -2 -1 0 1 2 3
Severity of Alcohol use Disorder (Latent Trait)
Pro
ba
bili
ty o
f e
nd
ors
em
en
t
Neglect roles
Hazardous Use
Legal Problems
Continued use despite problems
Tolerance
Withdrawal
Larger/Longer
Quit/control
Time spent
Activities given up
Physical/psychological problems
Keyes KM…Hasin DS, Psychological Medicine 2010
Columbia University Deborah Hasin, Ph.D .

Compton, Saha, Grant et al., Drug and Alcohol Dependence 2009
NESARC ICCCurrent Cannabis Abuse, Dependence (N=1,603)
Columbia University Deborah Hasin, Ph.D .

0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
-3.0
0
-2.8
0
-2.6
0
-2.4
0
-2.2
0
-2.0
0
-1.8
0
-1.6
0
-1.4
0
-1.2
0
-1.0
0
-0.8
0
-0.6
0
-0.4
0
-0.2
0
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
2.00
2.20
2.40
2.60
2.80
3.00
Severity of Lifetime Drug Use Disorder- Cocaine/Crack (Latent Trait)
Pro
ba
bili
ty o
f S
ym
pto
m E
nd
ors
em
en
t
Tolerance Withdrawal Larger/longer Quit/control
Time spent Activities given up Physical/psychological problems Neglect roles
Hazardous use Legal problems Social/Interpersonal problems
NESARC ICCLifetime Cocaine Abuse, Dependence (N=2,528)
Saha …Grant., Drug and Alcohol Dependence, 2012
Columbia University Deborah Hasin, Ph.D .

• Tolerance
• Withdrawal
• More use than intended
• Unsuccessful efforts to cut down
• Spends excessive time in acquisition
• Activities given up because of use
• Uses despite negative effects
DSM-III 1987DSM-IV 1994
• Maladaptive use within 12 month period (one or more)
1. Failure to fulfill major role obligations
2. Recurrent use in hazardous situations3. Recurrent substance related legal problems4. Continued use despite consistent social or
interpersonal problems
• Never met dependence criteria
DSM-IV

UseUse
UseUse
UseUse
UseUse
AbuseAbuse (declarative)
AbuseAbuse
AddictionAddiction (automatic)
Abuse Abuse
AddictionAddiction

UseUse
UseUse
AddictionAddiction SeveritySeverity
• Tolerance*
• Withdrawal*
• More use than intended
• Craving for the substance
• Unsuccessful efforts to cut down
• Spends excessive time in acquisition
• Activities given up because of use
• Uses despite negative effects
• Failure to fulfill major role obligations
• Recurrent use in hazardous situations
• Continued use despite consistent social or interpersonal problems
*not counted if prescribed by a physician
DSM-5
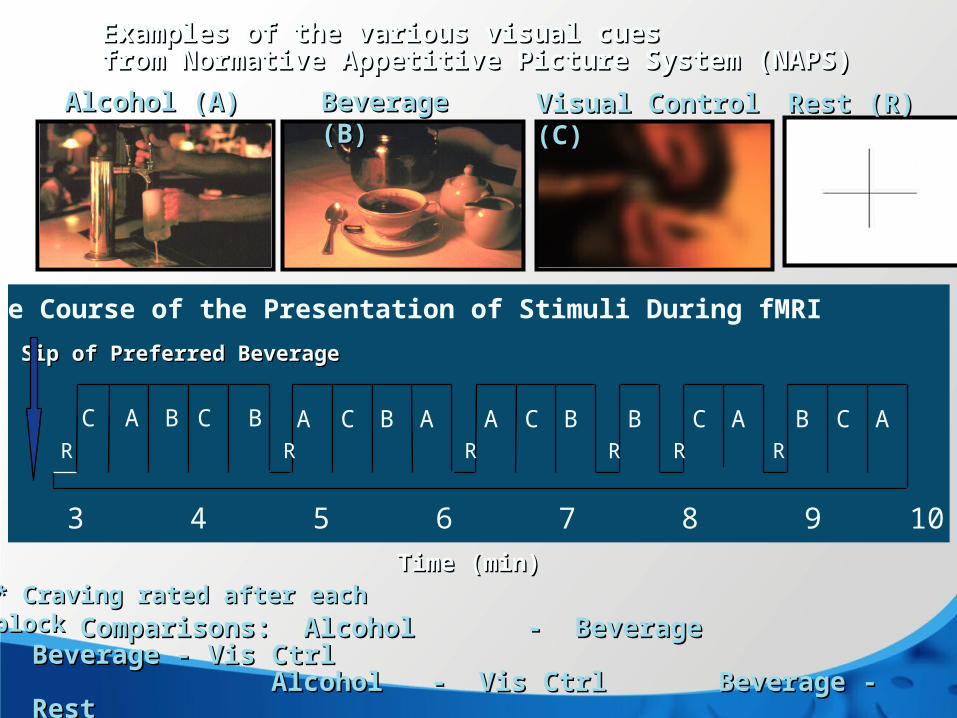
0 1 2 3 4 5 6 7 8 9 10 11 12 13
C BBAC A B C A B C AC B A A C B
Time (min)Time (min)
Alcohol (A)Alcohol (A) Beverage (B)Beverage (B) Visual Control (C)Visual Control (C)
Comparisons: Alcohol Comparisons: Alcohol - Beverage - Beverage Beverage - Vis Ctrl Beverage - Vis Ctrl AlcoholAlcohol - Vis Ctrl - Vis Ctrl Beverage - Rest Beverage - Rest Vis Ctrl Vis Ctrl - Rest - Rest
RRRRRR
Sip of Preferred BeverageSip of Preferred Beverage
Examples of the various visual cues Examples of the various visual cues from Normative Appetitive Picture System (NAPS)from Normative Appetitive Picture System (NAPS)
Rest (R)Rest (R)
* Craving rated after each block* Craving rated after each block
Time Course of the Presentation of Stimuli During fMRI
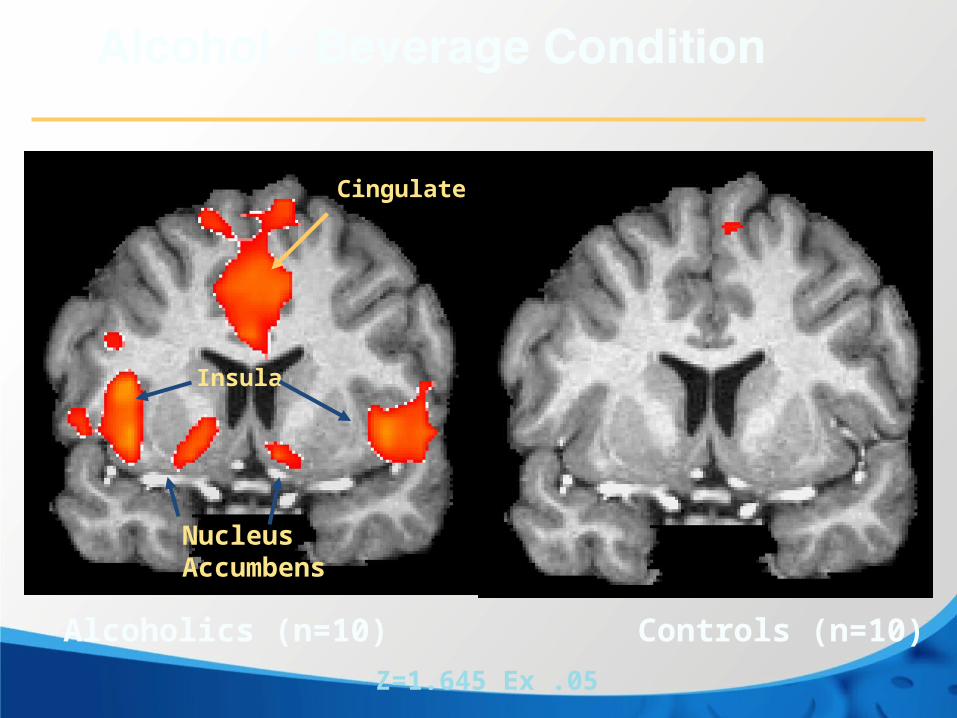
Insula
Cingulate
Nucleus Accumbens
Z=1.645 Ex .05
Alcoholics (n=10) Controls (n=10)

Ventral Tegmental Area
Cingulate
Z=1.645 Ex .05, Myrick et al,2004
Alcohol - Beverage Condition
Alcoholics (n=10) Controls (n=10)

1. No more abuse and dependence
2.Severity measured by number of symptoms, 2-3 mild, 4-6 moderate, 7-11 severe
3.? Agonist maintenance (methadone, Suboxone) requires“Moderate to severe opioid use disorder”

1. Anti-depressants
2.Opioid analgesics
3.Anti anxiety
4.Anti hypertensive

BUTBio-markers in psychiatry are notsufficiently reliable and availablefor clinical practice
NIMH Research Domain CriteriaRDoC

• (1) irritability, anger, or aggression
• (2) nervousness or anxiety
• (3) sleep difficulty (e.g., insomnia, disturbing dreams)
• (4) decreased appetite or weight loss
• (5) restlessness
• (6) depressed mood
• (7) at least one of the following physical symptoms: stomach pain, shakiness/tremors, sweating, fever, chills, headache
DSM-5
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved
• A. Daily Use of Caffeine
• B. 3 or more
(1) headache
(2) marked fatigue or drowsiness
(3) dysphoric or depressed mood, or irritability
(4) difficulty concentrating (5) symptoms of nausea, vomiting, or muscle pain/
stiffness
• C. clinically significant distress or impairment in social, occupational, or other important areas of functioning.
• D. not due to the direct physiological effects of a general medical condition
DSM-5
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

A. A problematic pattern of caffeine use leading to clinically significant impairment or distress, as manifested by all of the following three criteria occurring within a 12-month period:
1. A persistent desire or unsuccessful efforts to cut down or control caffeine use.
2. Continued caffeine use despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by caffeine.
3. Withdrawal, as manifested by either of the following:
a. The characteristic withdrawal syndrome for caffeine.
b. Caffeine (or a closely related) substance is taken to relieve or avoid withdrawal symptoms.
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved
B. Other symptoms of the disorder:1.Caffeine is often taken in larger amounts or over a longer period than was intended.2. Recurrent caffeine use resulting in a failure to fulfill major role obligations at work, school, or home (e.g., repeated tardiness or absences from work or school related to caffeine use or withdrawal).3. Continued caffeine use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of caffeine (e.g., arguments with spouse about consequences of intoxication, medical problems, cost).4. Tolerance, as defined by either of the following: a. A need for markedly increased amounts of caffeine to achieve desired effect. b. Markedly diminished effect with continued use of the same amount of caffeine.5. A great deal of time is spent in activities necessary to obtain caffeine, use caffeine, or recover from its effects.6. Craving or a strong desire or urge to use caffeine.
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

A. Persistent and recurrent problematic gambling behavior leading to clinically significant impairment or distress as indicated by four (or more) of the following in a 12-month period:
1. Needs to gamble with increasing amounts of money in order to achieve the desired excitement.2. Is restless or irritable when attempting to cut down or stop gambling.
Gambling Disorder 312.31 (F63.0) 2533. Has made repeated unsuccessful efforts to control, cut back, or stop gambling.4. Is often preoccupied with gambling (e.g., having persistent thoughts of reliving past gambling experiences, handicapping or planning the next venture, thinking of ways to get money with which to gamble).5. Often gambles when feeling distressed (e.g., helpless, guilty, anxious, depressed).6. After losing money gambling, often returns another day to get even (“chasing” one’s losses).7. Lies to conceal the extent of involvement with gambling.8. Has jeopardized or lost a significant relationship, job, or educational or career opportunity because of gambling.9. Relies on others to provide money to relieve desperate financial situations caused by gambling.
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

B. The gambling behavior is not better explained by a manic episode.
Specify if:Episodic: Meeting diagnostic criteria at more than one time point, with symptoms subsidingbetween periods of gambling disorder for at least several months.Persistent: Experiencing continuous symptoms to meet diagnostic criteria for multipleyears.In early remission: After full criteria for gambling disorder were previously met, noneof the criteria for gambling disorder have been met for at least 3 months but for lessthan 12 months.In sustained remission: After full criteria for gambling disorder were previously met,none of the criteria for gambling disorder have been met during a period of 12 monthsor longer.
Specify current severity:Mild: 4–5 criteria met.Moderate: 6–7 criteria met.Severe: 8–9 criteria met.
continued
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

Persistent and recurrent use of the Internet to engage in games, often with other players. Use of the Internet for required activities in a business or profession is not included in this disorder, and it also is not intended to apply to other recreational or social Internet use. Afflicted individuals show clinically significant impairment or distress as indicated by five (or more) of the following in a 12-month period:
1. Preoccupation with Internet games. (The individual thinks about previous gaming activity or anticipates playing the next game; Internet gaming becomes the dominant activity in daily life). Note: This disorder is distinct from Internet gambling, which is included under gambling disorder.2. Withdrawal symptoms when Internet gaming is taken away. (These symptoms are typically described as irritability, anxiety, or sadness, but there are no physical signs of pharmacological withdrawal.)3. Tolerance—the need to spend increasing amounts of time engaged in Internet games.4. Unsuccessful attempts to control the participation in Internet games.5. Loss of interests in previous hobbies and entertainment as a result of, and with the exception of, Internet games.6. Continued excessive use of Internet games despite knowledge of psychosocial problems.7. Has deceived family members, therapists, or others regarding the amount of Internet gaming.8. Use of Internet games to escape or relieve a negative mood (e.g., feelings of helplessness, guilt, anxiety).9. Has jeopardized or lost a significant relationship, job, or educational or career opportunity because of participation in Internet games.Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

Note: For this disorder, gambling sites on the Internet are excluded. Only non-gambling Internet games are included. Similarly, this disorder excludes sexual Internet sites. Use of the Internet for required activities in a business or profession is not included in this disorder, and the disorder is not intended to include other recreational or social Internet use.
Specify current severity:Internet gaming disorder can be mild, moderate, or severe depending on the degreeof disruption of normal activities. Individuals with less severe Internet gaming disordermay exhibit fewer symptoms and less disruption of their lives. Those with severe Internetgaming disorder will have more hours spent on the computer and more severe lossof relationships or career or school opportunities
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

A. More than minimal exposure to alcohol during gestation, including prior to pregnancy recognition. Confirmation of gestational exposure to alcohol may be obtained from maternal self-report of alcohol use in pregnancy, medical or other records, or clinical observation.
B. Impaired neurocognitive functioning as manifested by one or more of the following:1. Impairment in global intellectual performance (i.e., IQ of 70 or below, or a standard score of 70 or below
on a comprehensive developmental assessment).2. Impairment in executive functioning (e.g., poor planning and organization; inflexibility; difficulty with behavioral inhibition).3. Impairment in learning (e.g., lower academic achievement than expected for intellectual level; specific learning disability).4. Memory impairment (e.g., problems remembering information learned recently; repeatedly making the same mistakes; difficulty remembering lengthy verbal instructions).5. Impairment in visual-spatial reasoning (e.g., disorganized or poorly planned drawings or constructions; problems differentiating left from right).
C. Impaired self-regulation as manifested by one or more of the following:1. Impairment in mood or behavioral regulation (e.g., mood lability; negative affect or irritability; frequent behavioral outbursts).2. Attention deficit (e.g., difficulty shifting attention; difficulty sustaining mental effort).3. Impairment in impulse control (e.g., difficulty waiting turn; difficulty complying with rules).
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved

D. Impairment in adaptive functioning as manifested by two or more of the following, one of which must be (1) or (2):
1.Communication deficit (e.g., delayed acquisition of language; difficulty understanding spoken language).2.Impairment in social communication and interaction (e.g., overly friendly with strangers; difficult reading social cues; difficulty understanding social consequences).3.Impairment in daily living skills (e.g., delayed toileting, feeding, or bathing; difficulty managing daily schedule).4.Impairment in motor skills (e.g., poor fine motor development; delayed attainment of gross motor milestones or ongoing deficits in gross motor function; deficits in coordination and balance).E. Onset of the disorder (symptoms in Criteria B, C, and D) occurs in childhood.F.The disturbance causes clinically significant distress or impairment in social, academic, occupational, or other important areas of functioning.G.The disorder is not better explained by the direct physiological effects associated with postnatal use of a substance (e.g., a medication, alcohol or other drugs), a general medical condition (e.g., traumatic brain injury, delirium, dementia), another known teratogen (e.g., fetal hydantoin syndrome), a genetic condition (e.g., Williams syndrome, Down syndrome, Cornelia de Lange syndrome), or environmental neglect.
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright © 2013). American Psychiatric Association. All rights reserved
1. 1. Neuroscience based diagnosis2.150,000 diagnostic interviews3.Bio markers not yet reliable4.Heredity important, but no genetic impact on treatment5.Relapse prevention meds show efficacy but rarely used6.New findings if replicated > DSM 5.17.Potential pharmacogenetic indication,
Genotype, then select medication

1. No intermediate state-abuse, dependence; only a single dimension,
mild, moderate, severe
2. Two symptoms is diagnostic threshold for the combined disorder
3. “Dependence” only used for pharmacological dependence which is
not a disorder
4. Delete legal symptom and add craving
5. Group gambling disorder with substance use disorders
6. Add cannabis withdrawal.
7. Add Internet gaming disorder to section 3
8. Add Neurobehavioral Disorder Associated with Prenatal Alcohol
Exposure to Section 3
9. Add caffeine use disorder to section 3
Impact of Changes in DSM-5 on SUDs
• Interviewed 7,543 subjects for genetic studies of substance dependence
• Modestly increased prevalence largely due to DSM-IV “diagnostic orphans” receiving DSM-5 diagnoses
• Vast majority of switches to DSM-5 due to reduced threshold and increased number of criteria
• Support for omission of the legal criterion due to limited diagnostic impact
• Little impact of the addition of craving
Peer et al., Drug Alcohol Depend, 2013

Impact of Changes in DSM-5 on SUD Prevalence
Peer et al., Drug Alcohol Depend, 2013
Why Classify Gambling Disorder with SUDs?
• Strong comorbidity of the two disorders
• Measurable phenotype with high heritability that underlies SUD and GD: Different manifestations of an underlying predisposition
• Evidence for shared neurobiology: Imbalance between motivation/reward systems and inhibitory systems
Why Classify Gambling Disorder with SUDs?
• Strong comorbidity of the two disorders
• Measurable phenotype with high heritability that underlies SUD and GD: Different manifestations of an underlying predisposition
• Evidence for shared neurobiology: Imbalance between motivation/reward systems and inhibitory systems

DSM-IV Pathological Gambling(5 or more required for diagnosis)
1. Preoccupation with gambling
2. Need to gamble in increasing amounts
3. Unsuccessful efforts to control gambling
4. Restlessness or irritability when attempting to stop
5. Gambling as a way to escape problems

DSM-IV Pathological Gambling(5 or more required for diagnosis)
6. After losing, returns another day to get even (“chasing losses”)
7. Lies to conceal extent of gambling
8. Commits illegal acts to finance gambling
9. Jeopardized or lost relationship, job, education, or career because of gambling
10. Relies on others to relieve desperate financial situation caused by gambling

DSM-5 Gambling Disorder (GD)
• Included in Substance-Related and Addictive Disorders
• “Illegal Acts” criterion dropped, leaving a total of only 9 criteria
• Number of criteria required for the diagnosis reduced to 4
Impact of Changes in DSM-5 GD
• Interviewed 6,613 subjects from genetic studies of substance dependence
• 1,507 had ever gambled $10 at least monthly and were the focus of analyses
• Three subgroups: “No Diagnosis” (n=829, 55.0%), a “DSM-5-Only” (n=115, 7.6%), and a “Both-Diagnoses” (n=563, 37.4%)
Rennert et al., Exp Clin Psychopharmacol, in press

Impact of Changes in DSM-5 GD
• Prevalence of DSM-5 GD was 20.4% higher than DSM-IV Pathological Gambling (PG)
• DSM-5-Only group was intermediate on the prevalence of comorbid substance use disorders, distribution of DSM-IV PG criteria endorsed, types of gambling reported, and acknowledgment of a gambling problem
• DSM-5 appears to identify problem gamblers who were not diagnosed under DSM-IV
Rennert et al., Exp Clin Psychopharmacol, in press

Other Changes
• Eliminated Polysubstance Dependence
• Added Cannabis and Caffeine Withdrawal and include them as criteria for Cannabis Use and Caffeine Use Disorders
• Aligned criteria for Tobacco Use Disorder with criteria for other Substance Use Disorders

Summary of Major Changes
• Replaced Abuse/Dependence with SUD
• Increased criteria to 11 for SUD– Omitted legal criterion and added craving– Mild = 2-3, Moderate = 4-5, Severe = 6-11
• Renamed and moved Gambling Disorder to Substance-Related and Addictive Disorders
• Reduced criteria to 9 for Gambling Disorder– Omitted illicit acts – Lowered threshold to 4 criteria required for diagnosis

Minimal Skills:Detox
• Sedatives– Alcohol, barbs, benzos
(gabapentin)– Opioids
Clonidine
Lofexidine
Stimulants
Anti-depressants-TCA. SSRI
Cannabis

Relapse Prevention
• Naltrexone– Alcohol, – Opioids
Suboxone
Opioids
Stimulants, cocaine
Modafinil
Methamphetamine ?
Treatment of Alcoholism in USATreatment of Alcoholism in USA
<10% receive treatment<10% receive treatment
• Medications only for treatment of withdrawalMedications only for treatment of withdrawal
• Relapse prevention medication rareRelapse prevention medication rare
• CNN Special on addiction: RelapsesCNN Special on addiction: Relapses
• Interviews with counselors at famous programsInterviews with counselors at famous programs
CNN Special CNN Special Addiction: Life on the edgeAddiction: Life on the edge
5 patients followed for one year5 patients followed for one yearDifferent parts of countryDifferent parts of country
• AdmissionsAdmissions
• GraduationsGraduations
• RelapsesRelapses
• Interviews with counselors at famous programsInterviews with counselors at famous programs•Interview with the one patient who did NOTInterview with the one patient who did NOT relapserelapse

GUPTA: And so he tried again. He checked himself into an experimental program run by Brown University. This time he got This time he got counseling once a week and a daily pill, a medicine called counseling once a week and a daily pill, a medicine called naltrexone. About two months into it, Walter Kent naltrexone. About two months into it, Walter Kent suddenly noticed the world around him looked and felt suddenly noticed the world around him looked and felt different. different.
KENT: And I had just turned around and I said, this is really something for the first time in my life that I never had this for the first time in my life that I never had this sensation where I didn’t want a drinksensation where I didn’t want a drink. And this, to me, was like a godsend because of the fact that for someone who had to have a drink, now all of a sudden I don't need that -- I don't have that feeling anymore.
GUPTA: He hasn’t had a drink in more than eight years. He hasn’t had a drink in more than eight years. Even after his doctor stopped the medication. He’s healthy, back He’s healthy, back at work, fixing up carburetors.at work, fixing up carburetors.. And now he's part of a running debate. Is addiction an illness you can treat with a pill or a character flaw to be tackled with therapy and self-help?
Addiction: Life on the Edge – CNN Correspondent Dr. Sanjay Gupta aired April 19, 2009Addiction: Life on the Edge – CNN Correspondent Dr. Sanjay Gupta aired April 19, 2009

GUPTA: Despite the evidence, most fancy rehab centers use Despite the evidence, most fancy rehab centers use medication only rarely, if at all. The focus is much more on medication only rarely, if at all. The focus is much more on therapy. therapy.
Head Counselor Minnesota: With the health care professional With the health care professional staff here at Hazelden, our experience tells us having that staff here at Hazelden, our experience tells us having that network of support in recovery is what really makes the network of support in recovery is what really makes the difference. difference.
GUPTA: More so than medication?
CLARK: More so than just medication, exactly.
GUPTA: And that's the conventional wisdom.
Addiction: Life on the Edge – CNN Correspondent Dr. Sanjay Gupta aired April 19, 2009Addiction: Life on the Edge – CNN Correspondent Dr. Sanjay Gupta aired April 19, 2009
California Program
GUPTA: What about medications?What about medications?
Head Counselor California Program: We do not use them at the We do not use them at the Betty Ford Center.Betty Ford Center.
No comment from the interviewer, no follow up questions.
Addiction: Life on the Edge – CNN Correspondent Dr. Sanjay Gupta aired April 19, 2009Addiction: Life on the Edge – CNN Correspondent Dr. Sanjay Gupta aired April 19, 2009
Evidence-based treatments not Evidence-based treatments not often used in US programsoften used in US programs
• Medication only for detoxification
• Few programs prescribe relapse prevention medication
• Affordable Care Act, 2014 will cover all FDA approved medications for substance use disorders.