Embed Size (px)
Citation preview

Pharmacy
Newsletter Vol. 27 Nov-Dec 2014
Self-medication: Don’t take med-ications blindly
Drug Comparison:
Streptokinase-Alteplase-Tenectaplase
Complimentary Medicine:
Body Walking
Drug Doping
In Sport
CO
NTE
NTS
Focus
Diluents for Injectable Drugs
Topic of Current Interest
Drug Doping in Sports
Complementary medicine
Body Walking
Drug Comparison
Streptokinase vs Alteplase vs
Tenectaplase
Drug Profile
Propiverine
Counselling
Dengue: The use of papaya leaves
Drug Safety
Self-medication: Don’t take medications blindly
Activities/ Announcement
Promosi: Sahabat Farmasi
EDITORIAL BOARD
PN. SAIDATUL RAIHAN BT IBRAHIM
PN. NOORAZLINDA YAACOB
PN. AFZAN RAIHAN IZZATI HAMZAH
EDITOR:
WOON SU ANN
CONTRIBUTOR:
TANG KAH WONG
MUNAWWARAH BINTI MD KAILANI
NUR FARAHIN BINTI ABDUL JABAR
1-2
3-4
5-6
7-8
9-10
11
12
13-14

Many drugs used in sterile products, especially antibiotics, come in a dry powder form. It is extremely important that the correct diluent be selected and the appropriate calculations be performed to ensure correct concentrations and stability of the finished product. Diluent is a clinically inactive ingredient/liquid used to
dilute or reconstitute a medication. It is also used to convert a dry form of a substance to a liq-
uid form. It is typically inserted with a syringe through the rubber stopper of the medication
vial for injectable drugs.
Some medications are very unstable in liquid form. Therefore, they are supplied in a dry
form to which an inactive diluent is added just before use. The information about the specific
type and amount of diluent to be added to achieve specific concentrations is provided on the
product label. Selecting the correct diluents (liquid or solution) is important in reconstituting a
medication. Incorrect diluents used can affect the medication’s stability, efficacy and safety.
Use of the incorrect diluent may result in loss of potency of the medication, an unwanted
chemical interaction, or a shorter period of stability of the reconstituted medication. The infor-
mation regarding the correct diluent to be used is clearly written on the product label. To en-
sure that the ingredients are compatible or incompatible with the diluent, the pharmacist or
pharmacy technician should check the reference books available in the pharmacy or may con-
sult the product information leaflet.
Diluents for Injectable Drugs By: Tang Kah Wong
Normal Saline Normal saline is a term commonly used interchangeably with 0.9% sodium chloride
(NaCl) injection.
It is the concentration of sodium chloride within the human blood stream.
It is isotonic, as are most injectable formulations. By diluting with normal saline, the
tonicity of the solution is unaltered. However, it is now known that rapid infu-
sion of NS can cause metabolic acidosis.
Dextrose 5% Dextrose is a form of glucose (sugar). Dextrose 5% in water is injected into a vein
through an IV to replace lost fluids and provide carbohydrates to the body.
It may be used as a diluent (liquid) for preparing injectable medication in an IV bag.
The difference between Dextrose with others diluent that is that sugar is a rapidly
regulated and metabolized compound in the bloodstream. As the sugar is me-
tabolized, or is removed from circulation by the liver making it into glycogen,
what remains is free water, which is hypotonic and therefore tends to cross
membranes out of the vascular space until osmotic equalibrium is reachieved.
Sterile Water for
Injection
Sterile Water for Injection USP is a clear, colorless, odorless liquid. It is sterile, hypotonic, nonpyrogenic, and contains no bacteriostatic or antimicrobi-
al agents.
It is a suitable diluent for intravascular injection after first having been made ap-
proximately isotonic by the addition of suitable solute. However, The solutions
can cause fluid and/or solute overload resulting in dilution of serum electrolyte
concentrations, overhydration, congested states or pulmonary edema.
1

So, which is the best diluent?
The choice between water for injection , dextrose 5% and 0.9% sodium chloride (normal
saline) as a diluent is a matter of debate. Normal saline is most commonly used among these
three diluents. Water for injection is hypotonic; using it as a diluent will potentially produce a hy-
potonic solution, where can cause hypotonic of cells and hemolytic.
On the other hand, dextrose 5% can becomes hypotonic too after the sugar is metabolized
by body and only free water left . It also can decrease sodium and potassium level causing hypo-
natremia and hypokalemia. Moreover, prolonged use of sugar water can cause high blood sugar
(hyperglycemia). Monitoring is needed blood glucose levels carefully when using dextrose IVs,
especially if the patient is diabetic.
There no doubt normal saline is most recommended as most of the drug can be diluted
with it. Secondly, Normal saline is isotonic, as are most injectable formulations. By diluting with
normal saline, the tonicity of the solution is unaltered. Unfortunately, risk of hypernatremia and
hyperchloremic metabolic acidosis has been reported. The chloride content of isotonic saline is
particularly high relative to plasma (154 mEq/L versus 103 mEq/L, respectively). Chloride ions
can cause decrease bicarbonate ions which act as buffering agent. Without these ions, acidosis
of body will occur , this is known as hyperchloremic metabolic acidosis.
In conclusion, all pharmaceutical company and profession recommended dextrose 5% and
normal saline as a diluent, but mostly there recommended normal saline. Most importantly, be-
fore choose a good diluent drug compatibility with diluent should be considered as well as patient
condition (diabetes and fluid restriction patient ) too.
2
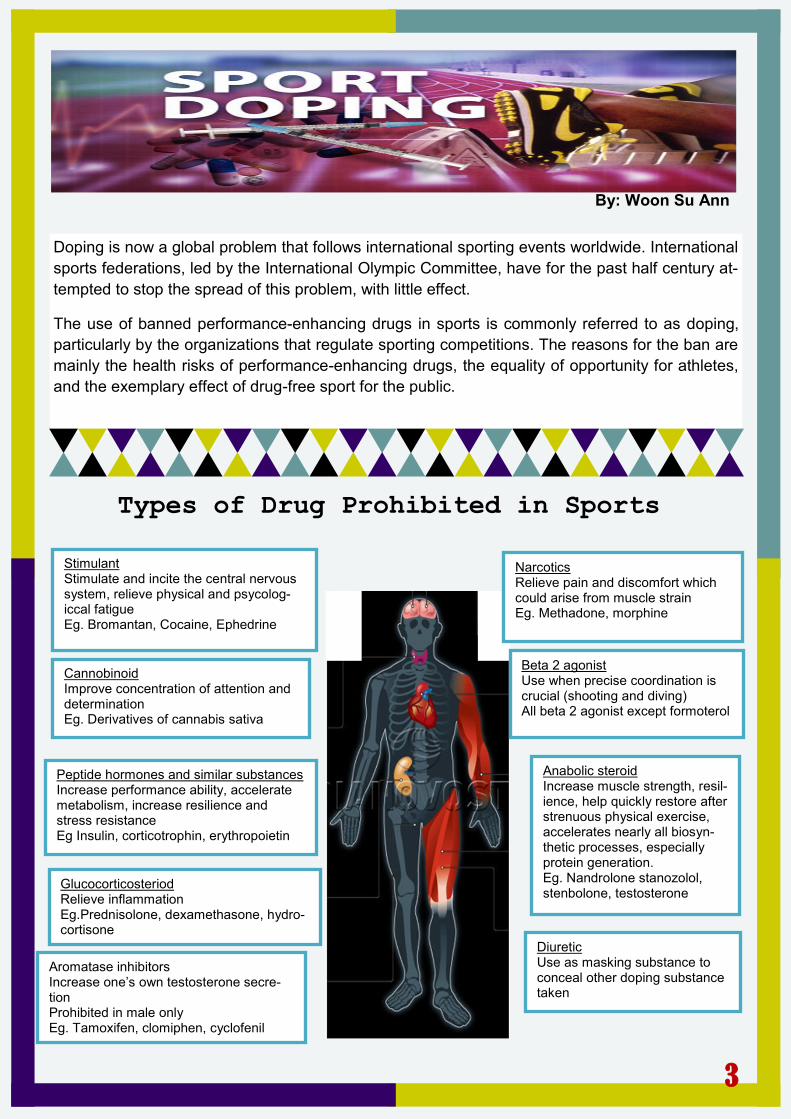
Stimulant Stimulate and incite the central nervous system, relieve physical and psycolog-iccal fatigue Eg. Bromantan, Cocaine, Ephedrine
Narcotics Relieve pain and discomfort which could arise from muscle strain Eg. Methadone, morphine
Beta 2 agonist Use when precise coordination is crucial (shooting and diving) All beta 2 agonist except formoterol
Peptide hormones and similar substances Increase performance ability, accelerate metabolism, increase resilience and stress resistance Eg Insulin, corticotrophin, erythropoietin
Diuretic Use as masking substance to conceal other doping substance taken
Glucocorticosteriod Relieve inflammation Eg.Prednisolone, dexamethasone, hydro-cortisone
Aromatase inhibitors Increase one’s own testosterone secre-tion Prohibited in male only Eg. Tamoxifen, clomiphen, cyclofenil
Anabolic steroid Increase muscle strength, resil-ience, help quickly restore after strenuous physical exercise, accelerates nearly all biosyn-thetic processes, especially protein generation. Eg. Nandrolone stanozolol, stenbolone, testosterone
Cannobinoid Improve concentration of attention and determination Eg. Derivatives of cannabis sativa
Types of Drug Prohibited in Sports
Doping is now a global problem that follows international sporting events worldwide. International
sports federations, led by the International Olympic Committee, have for the past half century at-
tempted to stop the spread of this problem, with little effect.
The use of banned performance-enhancing drugs in sports is commonly referred to as doping,
particularly by the organizations that regulate sporting competitions. The reasons for the ban are
mainly the health risks of performance-enhancing drugs, the equality of opportunity for athletes,
and the exemplary effect of drug-free sport for the public.
By: Woon Su Ann
3

Urine
Testing
When called for a drugs test the athlete is entitled to have
a representative (such as their coach or team doctor)
present to verify that the testing occurred in accordance
to guidelines. A sample is provided (in view of an official
of the same gender) and split into two bottles and sealed
by the athlete. A code number will be attached to the bot-
tle and recorded on the relevant paperwork to ensure the
correct result is given to the athlete whilst retaining their
anonymity.
Following the sampling procedure the athlete must com-
plete a medical declaration which states all medicines,
drugs and substances taken over the last week. It is im-
portant that the athlete records everything, from over-the-
counter medicines, to supplements and prescribed drugs.
If any of these substances are on the prohibited list the
athlete must hold a Therapeutic Use Exemption (TUE).
The competitor, representative and official all check the
form before the official and athletete sign it and both par-
ties are given a copy.
The samples are then sent to a registered laboratory (if
there is not one on site) where sample A is tested using
gas chromatography (which uses separation techniques
to divide the contents of the sample) and mass spec-
trometry (which provides the exact molecular specifica-
tion of the compounds). If a positive result is found with
sample A, the athlete is notified before sample B is also
tested. The athlete or their representative is entitled to
be present at the unsealing and testing of the second
sample. If this too is positive, the relevant sporting or-
ganisations are notified whose responsibility it is to de-
cide what penalties or bans are to be imposed.
Blood Testing
Blood testing is used in the detection of drugs such
as EPO and artificial oxygen carriers by testing the
haematocrit or blood count. Over time a "blood profile" of
an athlete can be built up to help determine average
readings for each individual. This can help with blood
doping tests in the future. The same anonymity and rep-
resentative procedures apply as for urine sampling.
Again the athlete is asked to select and check the testing
and collection equipment before a phlebotomist (an indi-
vidual trained to draw blood) collects two samples of
blood directly into bottles A and B. The bottles stay in the
possession of the athlete (who is always accompa-
nied by an official) until they are sealed in the sample
collection kit. Samples are sent to a lab for testing.
The same procedure applies as in urine testing,
where if the A sample is positive, the B sample is then
tested. Another positive result means the appropriate
governing bodies are notified.
The World Anti-Doping Agency (WADA) was established in 1999 to promote, coordinate, and monitor at the interna-tional level to fight against doping in sport in all its forms. The Agency is composed and funded equally by the Sports Movement and Governments of the world. WADA works to ensure that athletes benefit from the same anti-doping pro-tocols and protections, no matter the nationality, the sport, or the country where tested. The ultimate goal is safe and fair competition worldwide for clean sport.
4

Body walking is a therapeutic massage to promote healing
within the body. The therapist use ischemic pressure that is
able to exponentially increase the therapeutic affect by uti-
lizing pinpointed pressure with various foot positions and
pressure. The result is surprisingly relaxing and rejuvinating
for the client, and easier on the therapist’s body.
Roots in Asia
What is Body Walking?
Traditional Ashiatsu massage is based
in Traditional Chinese Medicine. It is per-
formed in both China and Japan by practition-
ers who have been trained to take a whole-
body approach towellness. In addition to
offering massage to their clients, these practi-
tioners may also assess diet, prescribe herbs,
and use other treatment modalities to address
the client's health problems.
By: Nur Farahin Abdul Jabar
BODY
WALKING
This modality has its roots in Asia, but today, sev-
eral different versions of Ashiatsu massage are
practiced around the world. Learning to perform
Ashiatsu massage requires some advanced train-
ing, because indifferent technique could cause
damage to the client's back.
Ashiatsu Massage
5
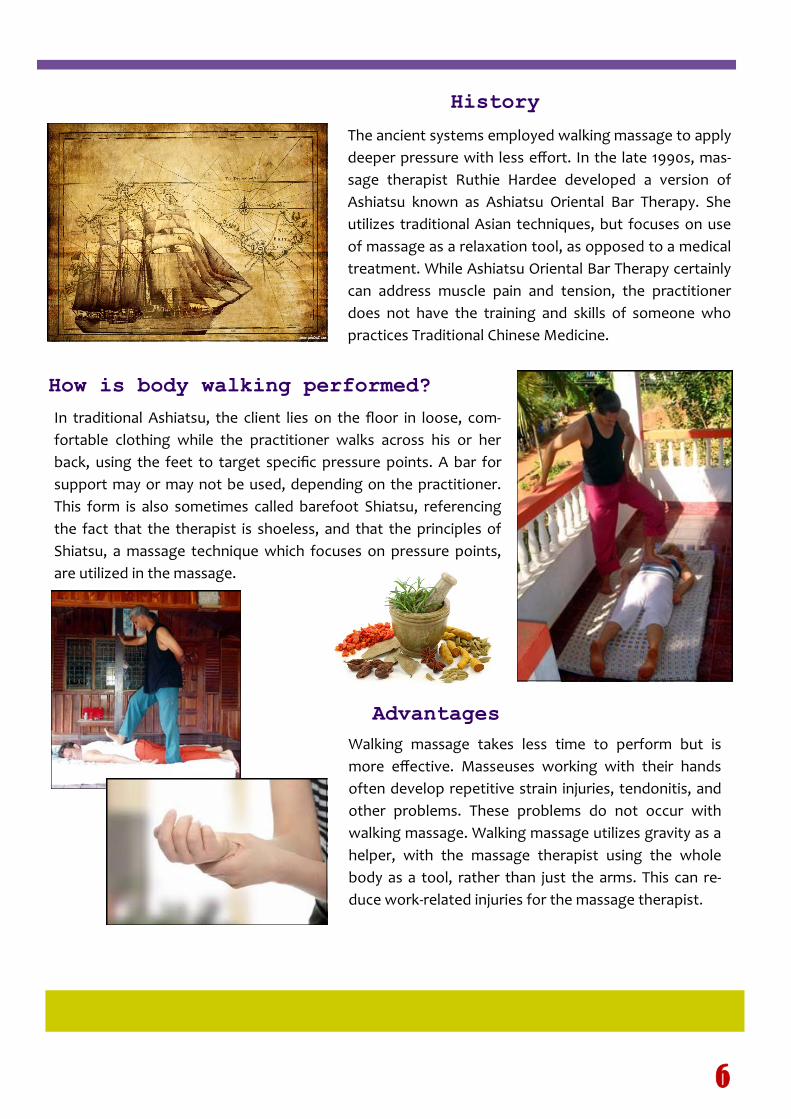
In traditional Ashiatsu, the client lies on the floor in loose, com-
fortable clothing while the practitioner walks across his or her
back, using the feet to target specific pressure points. A bar for
support may or may not be used, depending on the practitioner.
This form is also sometimes called barefoot Shiatsu, referencing
the fact that the therapist is shoeless, and that the principles of
Shiatsu, a massage technique which focuses on pressure points,
are utilized in the massage.
Advantages
History
Walking massage takes less time to perform but is
more effective. Masseuses working with their hands
often develop repetitive strain injuries, tendonitis, and
other problems. These problems do not occur with
walking massage. Walking massage utilizes gravity as a
helper, with the massage therapist using the whole
body as a tool, rather than just the arms. This can re-
duce work-related injuries for the massage therapist.
How is body walking performed?
The ancient systems employed walking massage to apply
deeper pressure with less effort. In the late 1990s, mas-
sage therapist Ruthie Hardee developed a version of
Ashiatsu known as Ashiatsu Oriental Bar Therapy. She
utilizes traditional Asian techniques, but focuses on use
of massage as a relaxation tool, as opposed to a medical
treatment. While Ashiatsu Oriental Bar Therapy certainly
can address muscle pain and tension, the practitioner
does not have the training and skills of someone who
practices Traditional Chinese Medicine.
6

Streptokinase Tenecteplase Alteplase
Indications Acute myocardial infarction, ar-
terial thrombosis, arteriovenous
cannula occlusion clearance,
deep venous thrombosis, pul-
monary embolism
Acute myocardial infarction Acute myocardial infarction, cere-
brovascular accident(acute & is-
chemic), pulmonary embolism, cen-
tral venous catheter occlusion
Dose Acute myocardial infarction (IV):
1500000 IU infused over 60
min
Acute myocardial infarction
(intracoronary): 20000 IU
bolus, then 2000 to 4000
IU / min for 10 to 90 min
Arterial thrombosis: loading
dose 250000 IU IV over 30
min, then 100000 IU / hr for
24hr
Arteriovenous cannula occlusion
clearance: instill 250000 IU /
2ml into each occluded limb
of the catheter
Deep vein thrombosis: loading
dose 250000 IU IV over 30
min, then 100000 IU / hr for
72hr
Pulmonary embolism: : loading
dose 250000 IU IV over 30
min, then 100000 IU / hr for
24hr (72hr if concurrent DVT
is suspected)
Acute myocardial infarction:
administer IV bolus over
5sec,
weight < 60kg: 30mg,
weight 60-69kg: 35mg,
weight 70-79kg: 40mg,
weight 80-89kg: 45mg,
weight > 90kg: 50mg
Acute myocardial infarction
(accelerated infusion): weight >
67kg: give 15mg IV bolus, 50mg
over 30min, then 35mg over
60min.
Acute myocardial infarction
(accelerated infusion): weight ≤
67kg: 15mg IV bolus, then
0.75mg/kg over 30min, then
0.5mg/kg over 60min.
Acute myocardial infarction (3hr
infusion): weight < 65kg,
1.25mg/kg IV administered over
3hr, give 60% in the first hour
(10% of which to be given as
bolus), give remaining 40% over
the next 2hr
Acute myocardial infarction (3hr
infusion): weight ≥ 65kg, 60mg
in the first hour (6-10mg of
which to be given as bolus),
20mg over the second hour, and
20mg over the third hour
Cerebrovascular accident: 0.9mg/kg
IV (not to exceed 90mg total
dose), infused over 60min with
10% of the total dose give as an
initial bolus over 1min
Pulmonary embolism: 100mg IV in-
fused over 2hr
Cost RM 901.80/ vial (1 vial =
1500000 IU)
RM 3630.00/ vial (1 vial =
10000 IU or 50mg)
RM 5106.35/ 2 vials (1 vial = 50mg)
Comparison between Streptokinase, Tenecteplase & Alteplase
By: Munawwarah Md Kailani
7

Pharma-
cokinetic
(ADME)
Onset & duration: the effect of
hyperfibrinolytic effect disap-
pears within a few hours,
however the effect on coag-
ulation may persist for up to
12 to 24hr after discontinua-
tion of streptokinase
Absorption (Bioavailability): not
absorbed orally and rectally
Distribution: volume of distribu-
tion is 5.68L
Excretion: by renal, with rate of
7.08L/hr
Elimination half-life: 18min due
to the action of antibodies,
or 83min which is operative
in the absence of antibodies
Onset & duration: the time to
reperfusion approximately
11min
Metabolism: mainly in liver, but
extent unknown, and some in
plasma
Excretion: total body clearance is
99 to 119ml/min, and plasma
clearance is approximately
105ml/min
Elimination half-life: 20 to 24min
Onset & duration: time to
initial response is
30min and time to peak
response approximate-
ly 60min
Distribution: volume of dis-
tribution is 8.1L
Metabolism: metabolized at
liver, with the metabo-
lites degraded to con-
stituent amino acids
Excretion: total body clear-
ance is 380 to 570ml/
min
Elimination half-life: 26.5 to
46min
Pharma-
codyna-
mic
Streptokinase and plasminogen
form a complex, exposing plas-
minogen-activating site, and
then, cleavage of peptide bond
converts plasminogen to plas-
min. In treatment of acute MI,
streptokinase prevents primary
or secondary thrombus for-
mation in microcirculation sur-
rounding the necrotic area.
Tenecteplase binds to fibrin rich
clots and cleaves the Arg/Val
bond in plasminogen to form
plasmin. Plasmin in turn de-
grades the fibrin matrix of the
thrombus, thereby exerting its
thrombolytic action. This helps
eliminate blood clots or arterial
blockages that cause myocardial
infarction.
Alteplase binds to fibrin in
a thrombus and converts
the entrapped plasminogen
to plasmin. It also produces
limited conversion of plas-
minogen in the absence of
fibrin.
Mecha-
nism of
Action
Streptokinase forms a highly
specific 1:1 enzymatic complex
with plasminogen which con-
verts inactive plasminogen mol-
ecules into active plasmin. Plas-
min degrades fibrin clots as well
as fibrinogen and other plasma
proteins. This in turn leads to
the degradation of blood clots.
Genetically engineered variant of
alteplase with multiple point mu-
tations of tPA molecule resulting
in longer plasma half-life, en-
hanced fibrin specificity & in-
creased resistance to inactivation
by plasminogen activator inhibitor
1 (PAI-1) compared to alteplase.
Promotes thrombolysis by con-
verting plasminogen to plasmin
which degrades fibrin & fibrino-
gen
Recombinant human tissue
-type plasminogen activa-
tor (t-PA), produces local
fibrinolysis. . Promotes
thrombolysis by converting
plasminogen to plasmin
which degrades fibrin &
fibrinogen
8

Propiverine By: Tang Kah Wong
Propiverine hydrochloride is used to treat people who have urinary problems caused by an overac-tive bladder or by spinal cord injuries. It works by pre-venting spasms of the bladder muscle. This can help to reduce the episodes of urinary incontinence or reduce the feeling of urgency that bladder spasms can cause.
Dose:
Adult: 15mg 2 to 3 times daily, increase to 4 times daily if required.
Max dose: 60mg .
Children more than 5 years old: 0.2 –0.4 mg/kg per day in 2 divided doses.
(MOH Drug Formulary (Blue Book)
Before you take Propiverine
Do not take Propiverine if you are allergic (hypersensitive) to propiverine hydrochloride or to any of the other ingredients content inside the drug.
Do not take Propiverine if you suffer from any of the following conditions:
obstruction of the bowel obstruction to the bladder outlet (difficulty in passing urine) myasthenia gravis (a disease causing muscle weakness) a loss of function of the muscles controlling your bowel movements (intestinal atony) severe inflammation of the bowel (ulcerative colitis) that may lead to diarrhoea containing blood and mucus and stomach pains toxic megacolon (a condition involving enlargement of the bowel) increased pressure in the eye moderate or severe liver disease fast and irregular heart beat (arrhythmia) you are pregnant or breast-feeding
Mictonorm® 15 mg Coated
Tablets
9
Possible side effects
Drug interaction
The following medicines as they may interact with Propeverine:
Other precautions
Any sudden wheeziness, difficulty in breathing or dizziness, swelling of the eye-lids, face, lips or throat
Peeling and blistering of the skin, mouth, eyes and genitals
Rash affecting your whole body.
antidepressants (e.g. imipramine, clomipramine and amitriptyline), sleeping tablets (e.g. benzodiazepines), anticholinergics taken by mouth or injection (usually used to treat asthma, stomach cramps, eye problems or urinary incontinence), amantadine (used to treat flu), neuroleptics (eg. promazine, olanzapine, quetiapine) (drugs used to treat psy-
chotic disorders like schizophrenia or anxiety), beta stimulants (drugs used to treat asthma), isoniazide (a treatment for tuberculosis)
metoclopramide (used to treat nausea and vomiting)
Taking Propervine with food and drink The tablets should be swallowed whole before meals. Pregnancy and breast-feeding Do not take Propervine if you are pregnant, likely to become
pregnant or are breast-feeding. Driving and using machines Propervine can sometimes cause sleepiness and blurred vision. You should not drive or operate machinery if you suffer from
sleepiness and blurred vision
10

The Use of Papaya
Leaves in Dengue Fever
By: Munawwarah Md Kailani
Dengue is the most common arthropod-
borne viral illness in humans. It is transmitted
by mosquitoes of the genus Aedes, which are
widely distributed in subtropical and tropical are-
as of the world. It is afebrile illness that affects
all ages with symptoms appearing 3-14 days
after the infective bite. Symptoms range from
mild fever, to incapacitating high fever, with se-
vere headache, pain behind eyes, muscle and
join pain, rash. Severe dengue, also known as
dengue haemorrhagic fever (DHF) is a specific
syndrome that mainly affects children. It causes
abdominal pain, bleeding and circulatory col-
lapse (shock). Since dengue fever is caused by
a virus, there is no specific medicine or antibiotic
to treat it. For a typical dengue fever, the treat-
ment is directed toward relief of the symptoms.
With the recent dengue outbreak, the use
of papaya (carica papaya) leaves as natural
remedy for dengue has become more popular.
According to the recent newspaper articles, the
Institute for Medical Research (IMR) will soon
release pamphlets on the correct use of papaya
leaf extract in the treatment of dengue. This is
based on the clinical studies that showed the
use of papaya leaves may increase blood plate-
let count and assist in the recovery of those with
less severe complications. Animal studies sug-
gest that papaya leaf extracts have potential
therapeutic effects on disease process, which
results in destabilization of biological mem-
branes as they inhibit haemolysis in vitro and
may cause elevated platelet and red blood cell
counts. There is a trial from Malaysia demon-
strated significantly higher platelet count after 40
to 48 hours of first dose of papaya leaves’ juice.
According to the Evidence-Based Com-
plementary and Alternative Medicine Volume
2013, consumption of Carica papaya leaf juice
induced rapid increase in platelet count in pa-
tients with grade one and two dengue fever and
the fatal dengue haemorrhagic fever. A random-
ised controlled trial that was carried out by IMR
and Hospital Tengku Ampuan Rahimah found
out patient that were administered with 50gm of
fresh Carica papaya juice for 3 consecutive
days showed a significant increase in platelet
count compared to those who received standard
management.
Basically the methods to prepare the
juice were already shared widely in the internet
and social media. The most commonly used
method is to prepare 2 pieces of raw papaya
leaves, then clean the leaves and pound and
squeeze with a filter cloth. You will only get one
tablespoon of juice per leaf, so take two table
spoons of papaya leaf juice once a day. The leaf
cannot be boiled, cooked or rinsed with hot wa-
ter, because it will lose its strength. Only the
leafy part of the papaya plant is being used, not
the stem or sap. The juice is very bitter and you
have to swallow it.
However, the role of Carica papaya leaf
juice cannot be scientifically substantiated
based on a few positive preliminary reports. Alt-
hough herbal products are assumed to be safe
because they are natural, this assumption can-
not be valued more than just conventional wis-
dom. The science must provide evidence to dis-
pel myths and focus efforts on more evidence-
based management of dengue fever using pa-
paya leaf juice.
11
Self medication is an act of consuming drugs without the ad-
vice of healthcare professionals. It also includes taking more
than the prescribed dosage, consuming medicine for a longer
duration than required, consuming medication prescribed for
a prior illness, sharing medicine among family members or
switching from Western to herbal medicines without consult-
ing a doctor. Shallow Self-
Diagnosis
What is self medication?
According to a study done in Malaysia, aimed to explore the
awareness and attitude among urban population towards self
medication, it was found that 83.9% of participants consumed
OTC medications, most commonly were supplements and vita-
mins, followed by painkillers, flu/cough remedies and sore throat
products. Easy access, convenience and time saving were the
most frequent reasons for self-medication.
Most people do it because they want to eliminate the cost and time of seeing a doctor. Others assume their condition is too mild for a doctor’s intervention and some believe they have ac-quired enough information to self-diagnose and self-medicate.
Common illnesses which lead to self-medication include head-
ache, flu, cough, joint pain, constipation and flatulence. Men-
strual pain, stomach discomfort and food poisoning are also
often self-medicated and painkillers and antibiotics are the two
drugs which are most commonly misused.
By: Nur Farahin Abdul Jabar
In Malaysia
12
Bermula dari: 26 Nov 2012
Fungsi: Menyediakan medium perantara yang merapatkan jurang antara Cawangan Penguat-kuasa Farmasi Negeri Melaka dengan masyara-kat.
Facebook: Sahabat Farmasi
Misi:
Menyampaikan informasi terkini mengenai penguatkuasaan farmasi dan penggunaan ubat-ubatan.
Menjamin keselamatan masyarakat dari segi ubat-ubatan.
13
Tarikh: 20 November 2014
Lokasi: Auditorium Sri Baiduri
14