Embed Size (px)
Citation preview

in partnership with
Drug development for Neuroblastoma – a preclinical hospital to drive trials and drug development for the field
Nov. 30, 2013
Ben Herring Trust
Felix White Foundation
Cole’s Family Foundation

Treatment for High-Risk Neuroblastoma(new interventions)
Prevention
Ultra-high risk
stratification
Targeted maintenance
Residual disease
eradication
X

Major Categories of New Therapeutics
• Chemotherapeutics• Small-molecule drugs
• Gene-targeted drugs• Oncoprotein-targeted drugs• Metabolic pathways• Differentiation pathways
• Immunotherapeutics – GD2, ALK, cellular• Radiotherapeutics – antibodies, metabolites

Panel Members
• Mark Gaze, UCLH, radiotherapy approaches
• John Anderson, GOSH, novel immunotherapies
• Hung Tran, CHLA, novel therapies through NANT
• Shakeel Modak, novel immune/therapies at MSKCC
• Rupert Handgretinger, Tubingen, immunotherapy/transplant

• Low number of drugs available for investigation in children • Clinical trials not optimally designed – do not Select the best drug Ask a clear scientific question Select patients who might benefit from a new drug Understand what is happening in the tumour Compare with a standard treatment
• Clinical trials take a long time to develop
Why do new drug trials take so long to develop?

Why do new drug trials take so long to develop?
• Low number of drugs available for investigation in children • Clinical trials not optimally designed – do not Select the best drug Ask a clear scientific question Select patients who might benefit from a new drug Understand what is happening in the tumour Compare with a standard treatment
• Clinical trials take a long time to develop• Pre‐clinical science and the hypotheses underpinning a therapy intervention take massive effort and funding to develop
• Without adequate science from pre‐clinical research, clinical trials are not hypothesis‐driven

New drug trials that are open
0
5
10
15
20
25
30
35
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Total number of openstudies
Molecular targeted agentstudies
First in Child

The Royal Marsden HospitalPaediatric Clinical Drug Development Team
Andy Pearson, Lucas Moreno, Lynley Marshall, Lou Chesler, Giuseppe Barone, Susanne Gatz,Dominik Schrey, Fernando Carceller, Andrea Boast, Gill James, Tracey Crowe , Beth Leach & Research Nurse Team
The Institute of Cancer ResearchBiology, Pre‐clinical Trials and Drug
Development TeamLou Chesler, Lynsey Vaughan, Teeara Berry, Evon, Poon, Sanne Kuijpers, Zai Ahmad, Xiaodun Li, Karen Barker, Lizzie Cullis, Laura Glass, Giuseppe Barone, Albert Hallsworth, Michelle Garrett (Biomarkers)Simon Robinson (Pre‐clinical Imaging)David Gonzalez (Clinical Assays)Paul Workman (Chemistry‐Drug Synthesis)

AACR Team Science Award 2012ICR/RMH Contributing of New Drugs to Cancer Trials
9
The AACR Team Science Award recognizes an outstanding interdisciplinaryresearch team for its innovative and meritorious science that has advanced orlikely will advance our fundamental knowledge of cancer or a team that hasapplied existing knowledge to advance the detection, diagnosis, prevention, ortreatment of cancer.
Major Advances in Pre-clinical Research
1. Sequencing of patients and identification of molecular targets
2. Medicinal development of targeted drugs
3. Development of pre-clinical target-driven cancer models

1. Molecular targets in neuroblastomaMutations are being rapidly identified
11
Mosse and Maris, U.Penn/CHOP NCI – TARGET, Versteeg, AMC Amsterdam
MYCN (sporadic) (Schwab et al., 1983) - “an undruggable target” ALK (familial, sporadic) (Mosse, George, et al., 2008) – “an eminently druggable target”

Drugs that target the specific molecules that are required for the growth of cancer tissue ‐ not present in normal tissue
Ideally “reduced” toxicityAdult Targets Lung Cancer – EGFR, EML4‐ALK GIST – c‐KIT Melanoma – BRAF V600E Breast + Ovarian – BRACA1/2 Breast Cancer ‐ HER2
Neuroblastoma Targets – MYCN, ALK
Centre for Cancer Therapeutics at ICR – Paul
Workman
2. Targeted Drugs for Neuroblastoma

13
Relevant clinical target
muscle‐tTA
X‐tTATRE MYCNLuc
Doxycycline
brain‐tTA
nerve‐tTA
X Medulloblastoma
Rhabdomyosarcoma
Neuroblastoma
Accurate in vivo models
OrthotopicsCell linesHT screens & pD assaysMouse hospital trials
PI103
+MYCN
-MYCN
3. Cancer models for Neuroblastoma

Drugs for MYCN and ALKThe two most common targets
1. MYCN – most common prognostically significant genetic change (gene amplification) –undruggable?
2. ALK – inherited and acquired mutations (most common single gene mutation) – druggable now (Crizotinib).
14

MYCN in neuroblastoma 15
• MYCN amplification in 25% of neuroblastoma
• MYCN amplification in infants and localised neuroblastoma – major prognostic factor –10% versus 85% survival
Years From Diagnosis
Amplified > 18 mo
Not Amplified
Overall Survival in Neuroblastoma
Amplified < 18 mo
% S
urvi
val

The MYCN driven neuroblastoma Pre-clinical model
16
Human MYCN cDNATyrosine-OH promotor
Weiss and Bishop, EMBO J, 1997 Reviewed in, Chesler, SCB, 2011
kidney
tumour

IGF-1R
PI3K AKT
Ras/Raf
MEK/ERK
mTOR
DALO
BEZ235GDC0980
AT9283CCT137690
RIDAAZD8055 AurK
GSK‐’212
GSK-’436Vemurafenib
Chesler et al. Cancer Res 2006, ANR2010, AACR2010 AACR2011, Mol Cancer Ther 2011, ANR2012, CCR2012, Cancer Cell 2012
GDC0941
Functional Imaging
Targeting MYCN protein stability

Drugs that block MYCN 18

MYCN causes resistance to PI3Ki mTORC2 inhibitors degrade MYCN
19
Mycncl. C3
pAkt473pAkt308
AktpS6
S6GAPDH
Vehicle mTOR Vehicle PI3K
200
150
100
0
-100
-150
Perc
ent V
olum
e C
hang
e
250
200
150
100
0
-100
-150
Vehicle mTOR Vehicle PI3K
mTOR PI3K
Unpublished work

Four classes of MYC/N inhibitor
Type I – transcriptional inhibitorsJQ1, iBET, Pfi1, ICR compound/s, others
Type II – stabilization inhibitors (interact with MB1)(AKT, mTORC1/2, others)
Type III – proteasome complex inhibitors (AURKA, UBC, USP inhibitors)
Type IV – synthetic lethal/functional inhibitors(CDK2 and CHK1 inhibitors, metabolic inhibitors)
20
Clin Cancer Research, Nov. 2013

ALK mutations identified in NB 2009ALK GEMM-therapeutics 2012
21
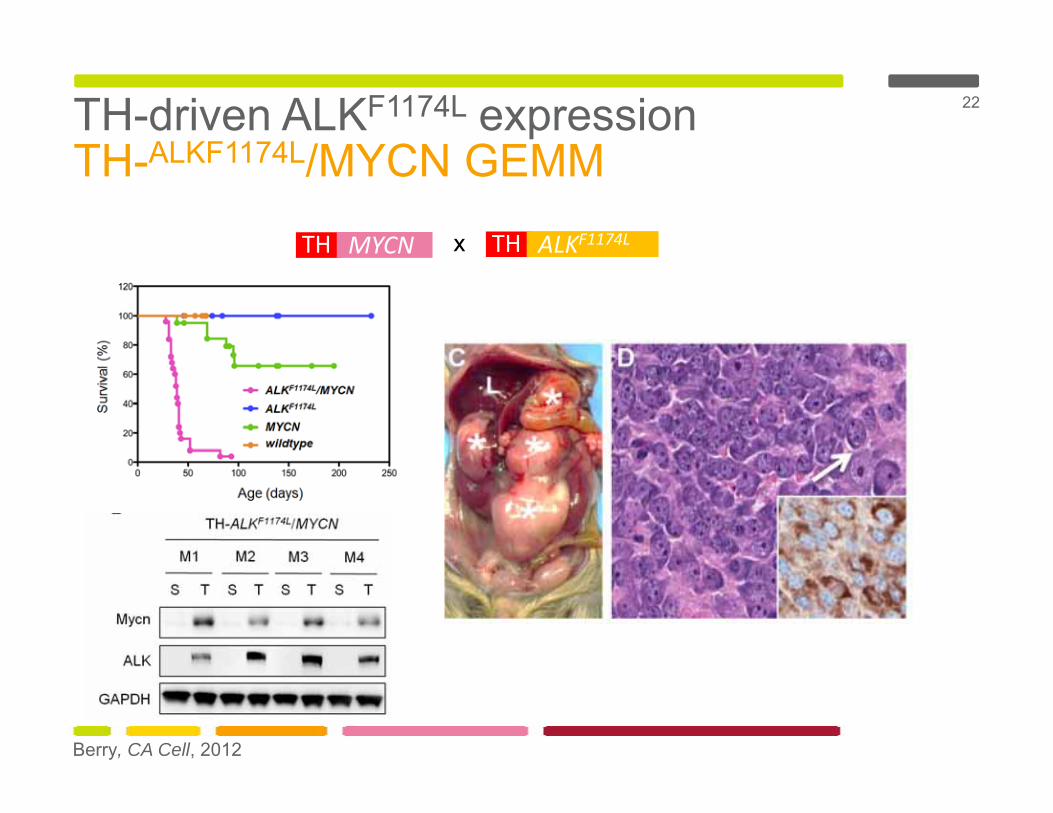
TH-driven ALKF1174L expressionTH-ALKF1174L/MYCN GEMM
22
TH MYCN TH ALKF1174Lx
Berry, CA Cell, 2012

ALK mediates resistance to CrizotinibNo efficacy as a single agent
23
Berry, Ca Cell, 2012

Combination of Crizotinib with mTOR inhibition is effective against ALK
24

Teeara Berry, Louis Chesler, Rani George, Cancer Cell 2012
Targeting ALK – Combination approach
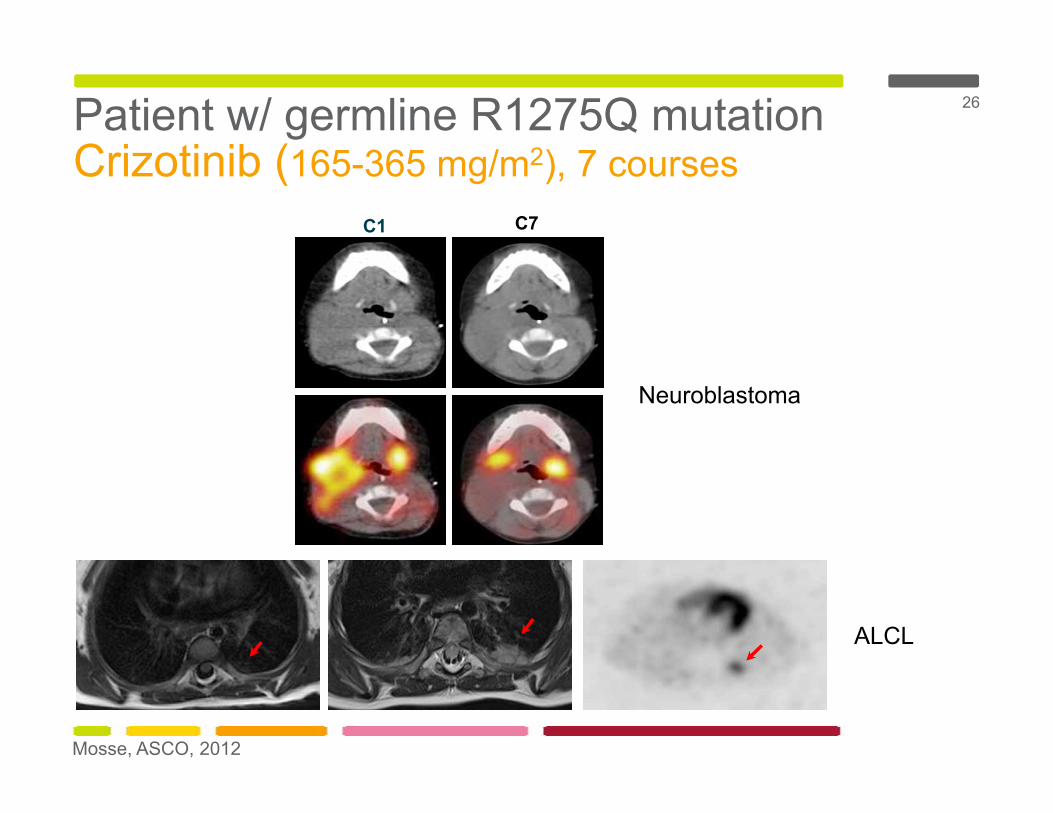
Patient w/ germline R1275Q mutation Crizotinib (165-365 mg/m2), 7 courses
26
Mosse, ASCO, 2012
C1 C7
Neuroblastoma
ALCL

Development of Biomarkers
Yap et al, Nature Rev Cancer 2010; Yap , JCO 2011; Garrido‐Laguna Nat Rev Clin Onc 2011
MK2206
MK2206
Predictive ‐What is the best drug for an individual patient?
Vemurafenib
Pharmacodynamic ‐ Is the drug working in the way we expected?
MK2206

Future imaging – anatomic correlationTranslational imaging for clinical use
28
tk
TH-ALKF1174LMYCN
TH-MYCN
TH-ALKF1174L
MYCN
TH-MYCN
PET MRI MRI perfusion imaging
Simon Robinson Laboratory, ICR

Pharmacodynamic Biomarker
Ganglioneuroblastoma (7 years old)
Miyazaki, et al. ISMRM 2011
Glioblastoma (10 years old)
Implemented in the Beacon –Neuroblastoma Trial
Is the drug tumour targeting tumour blood vessels?
DCE MRI

Models with multiple mutationsRepresentative of relapse patients
30
XTH MYCN
XMYCNTP53
ALK/ALKF1174L
p53ERTAMTH‐ALK/ALKF1174L
MYCNPhox2b
THPhox2B Sox2/10 dHand2Promotors:
Trial designs (single agent/combinations):• Intervention (induction)• Prevention• Survival extension• Chemo/Relapse• Chemo/MRD• Imaging is a key driver to all of these trials
Chemoresistant relapse mouse

Brain Tumour Cancer Models 31
D
Control NeuN Ki67 MYCN
0.E+00
5.E+09
1.E+10
2.E+10
2.E+10
3.E+10
1 8 15 22 28 32 39
Days post-implantation
500dox/CD133-
50 CD133+
500 CD133+
100 CD133+

Pre-clinical Drug Trials An Equivalent “HR” Trial
32
Models – Imaging – pK – online pathology – genomics - integrative dataflow – formalised reporting
Induction Consolidation Retrieval(phase I/II/III trial)
Chemo combinations
Targeted single / combinations
MRI/US BIOPSY MRD “biopsies”
Tumour Board
refractory
remission
MRD
XRT
HD-chemo
Surgery
Immunotherapy
Differentiation
Anatomic/functional imagingPharmacokinetics
Toxicity
Mol. PathologyGross and traditional Path
Genomics/sequencing
Chemo backbone
-/+ targeted agents
XRT
Relapse
Progression
A1
A2
A1
A2GEMM

Pre-clinical Drug PipelineFrom Mouse hospital trials
33
GENE TARGET/S COMPOUND/S COMPLETED CLINICAL TRIALPROPOSED
CLINICAL TRIAL INITIATION
MYCN PI3K ZSTK474, GDC0941 XPI3K/mTOR NVPBEZ235
GDC0980, Torin1/2XX
20122012
mTOR(kinase)
(rapalogue)
WY132AZD8055, AZD2014INK128RapamycinTemsirolimus
XX
XX
X
AURKA/B MLN8054MLN8237CCT690 (ICR)CCT736 (ICR)VX689AT9283
XXXXXX
XX
USA 2010
Spring 2010CDK2 AT7519 XBRD4 JQ1, iBET, Pfi1CHK1 CCT244747 X 2012PARP AZD2281 X 2012
ALK ALK crizotinib XLDK378 X X Feb 2013undisclosed
ALK immunotherapeuticALK/mTOR Crizotinib/temsirolimus
Critozinib/AZD2014XX
Late 2013
ALK/HSP90 AUY922 XVEGFR2 VEGFR2 mAb
VEGFR2 kinaseAvastinAZD2171
XX
Jan 2013
MDM2 MDM2 Roche pipeline X X Late 2014

Early Phase Studies Early 2013 Neuroblastoma
2013 2014 2015 2016 2017
• Ph I LEE011 CDK inhibitor (Novartis)
• Ph I/II Lutetium dotatate NBL (CR CTU)
• Ph IIb Beacon‐NBL (CR CTU)
• Ph I Abraxane (Celgene)
• Ph I Volasertib I (BI)
• Ph I/II Trametinib MEK inhibitor (GSK)
• Ph I LDK 378 ALK inhibitor (Novartis)
• Ph I/II Abraxane (Celgene)
• Ph I/II Crizotinib + temsirolimus ‐ ALK (CTU)
• Ph I/II trial GD2‐CAR transduced T‐cells (UCLH)
• Ph I /II study CI ch14.18/cho antibody and IL2 (CR CTU)
• Ph I/II Regorafenib (Bayer)
• PI3K Inhibitors• TORC1/2 Inhibitors• HSP90 Inhibitors• PARP Inhibitors
• Fusion Protein IL2 + GD2• ALK Vaccines• ALK CAR • Alk Antibodies
Earlier stages of planning

in partnership with
x
Centre for Pre-Clinical Drug Development, July 1 2011

in partnership with
x
x
Centre for Pre-Clinical Drug Development, Opens, July 1 2014
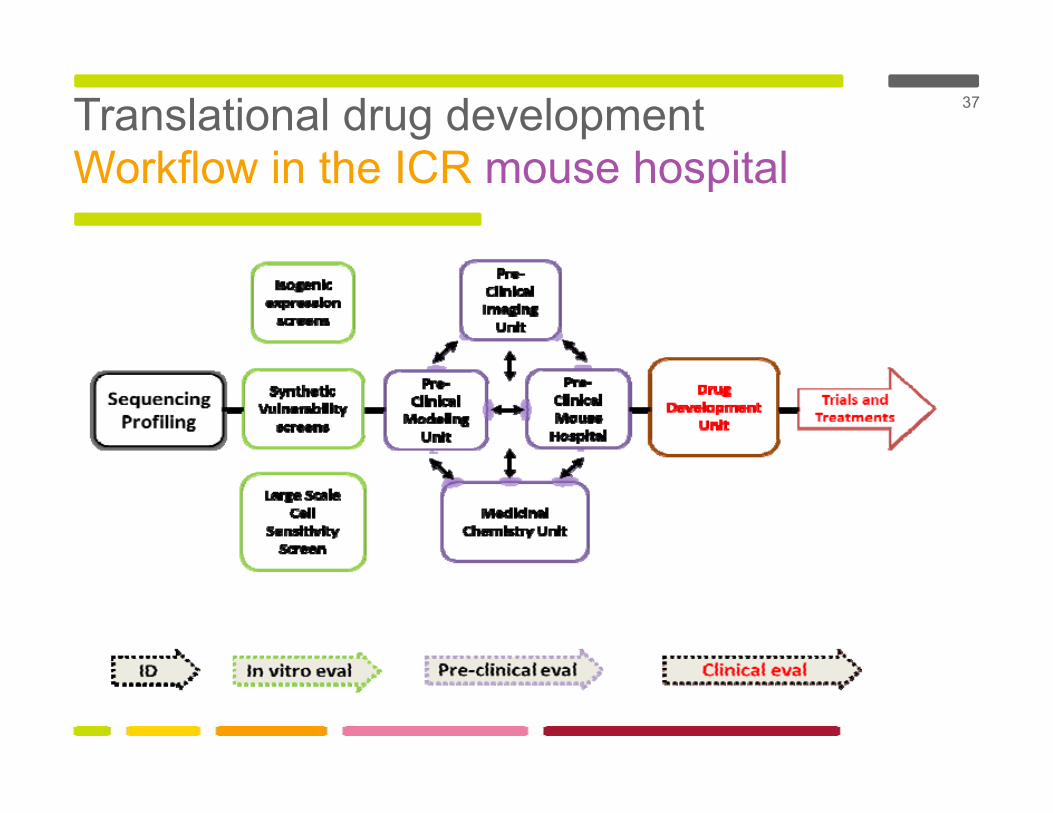
Translational drug developmentWorkflow in the ICR mouse hospital
37

in partnership with
Paul WorkmanAndrew PearsonPaul ClarkeJulian BlaggSpiros LinardopolousAlan AshworthChris LordMichelle GarrettSimon RobinsonSue EcclesJanet ShipleyChris JonesSergey PopovKhin Thway
Chesler labLynsey Vaughan Teeara BerryEvon PoonSanne Kuijpers
Clay GustafsonWilliam WeissYvan Chanthery
Fred Swartling
Martin Eilers
Rani GeorgeNathanael GrayNai-Kong Cheung (MSKCC)Wenchao WantScott RodigBandana Sharma
John MarisYael Mosse





























