Embed Size (px)
Citation preview
Journal of Traumatic Stress, Vol. 14, No. I , 2001
Dreams in the Acute Aftermath of Trauma and Their Relationship to PTSD
Thomas A. Mel l rna~~ , l*~~~ Daniella David,’ Victoria Bustamante,’ Joseph Torres,’ and Ana Fins’v3
Dreams following trauma have been suggested to aid emotionul adaptation, yet trauma-related nightmares are a diagnostic symptom of Posttraumatic Stress Dis- order (PTSD). There is little published data relating dreams to PTSD soon ajler trauma. We assessed dreams and PTSD in 60 injuredpatients afer life-threatening events and obtainedfollow-up assessments in 39 of these participants 6 weeks latex Ten of 21 dream reportsfrom morning diaries were rated and described as similar to the recent traumatic event. The participants reporting these distressing “trauma dreams ’’ had more severe concurrent PTSD symptoms than those reporting other categories of dreams and had more severe initial and follow-up PTSD than those without dream recall. These findings along with our preliminary longitudinal ob- servations relating changes in dream patterns to outcome, suggest a relationship of dream characteristics and early adaptive versus maladaptive patterns of pro- cessing traumatic memory. KEY WORDS: FTSD; dreams; nightmares.
The DSM-IV criteria for Posttraumatic Stress Disorder (PTSD) include “recurrent distressing dreams of the event” and the narrative section further descri- bes dreams during which the traumatic event is “replayed” (American Psychiatric Association, 1994). Studies that relate nightmares to PTSD have relied on survey or interview items that categorically probed the occurrence of trauma-related night-
] University of Miami School of Medicine, Department of Psychiatry and Behavioral Sciences, Miami, Florida
*Dartmouth Medical School, Department of Psychiatry, Lebanon, New Hampshire. 3Nova Southeastern, Ft. Lauderdale, Florida. 4T0 whom correspondence should be addressed at Dartmouth-Hitchcock Medical Center. De- partment of Psychiatry, One Medical Center Drive, Lebanon, New Hampshire 03756; e-mail: [email protected].
241
08969867/01~1oo-O24lSl9.5~l 0 2001 Inlcmational Society forTreumalic SvUs Studies
242 Mellman, David, Bustamante, Torres, and Fins
mares (David & Mellman, 1997; Inman, Silver, & Doghramji, 1990; Mellman, Kulick-Bell, Ashlock. & Nolan, 1995; Neylan et al., 1998; Van der Kolk, Blitz, Burr, Sherry, & Hartmann, 1984). Thus, these findings do not reflect specific eval- uation of the content of dreams. Assessments were also retrospective, and recall of dreams or nightmares from the past week or month is subject to diminished or distorted recall.
We recently reported on the content of dreams elicited by morning diaries within a group with chronic combat-related PTSD and found themes of threat to predominate while representation of past trauma was more variably present (Esposito, Benitez, Barza, & Mellman, 1999). A few studies of dream content have utilized the gold standard method of eliciting mentation upon awakening a participant out of REM sleep. Findings indicate that dreams of FTSD participants are more likely to be set in the past (Dow, Kelsoe, & Gillin, 1996) and that night- mares (Kramer, Schoen, & Kinney, 1984) and degree of dream recall (Kaminer & Lavie, 1991) are associated with overall distress and psychopathology.
The aforementioned studies featured survivors decades after severe war trauma. Assessment of dream content in closer proximity to trauma has been even more limited and the studies have not included formal assessment of FTSD (Hartmann; 1998; Wood & Bootzin, 1989). Such information might help to recon- cile dreams representing or replicating trauma as a defining symptom of a disorder with the suggestion that dreams following trauma can aid emotional adaptation to trauma (Greenberg, Pearlman, & Gampel, 1972; Hartmann, 1998).
The present study features subjects exposed to life-threatening trauma with injuries requiring hospitalization. Dream reports elicited by morning diaries were obtained during initial hospitalization along with assessment of PTSD symptoms, which was reassessed approximately 2 months after the trauma. In this report we provide information on the characteristics of dreams acutely following trauma and their relationship to developing PTSD.
Method
Participants
Consecutive admissions to a regional Trauma Center were reviewed. Par- ticipants were screened if they had experienced life-threatening incidents, were conscious and alert on arrival, and had negative blood screens for alcohol and illicit drugs. Screening evaluation then determined additional inclusion criteria of having recall of the incident, having reacted with fear helplessness or horror, absence of traumatic brain injury, and absence of a psychiatric disorder during the 6 months preceding the injury. The 60 participants represent only a fraction of the Trauma Center admissions (less than 5%) during the study period and ap- proximately a thiid of eligible cases that were approached to participate. Incidents
Dreams in the Acute Aftermath of h u m a and Their Relationship to PTSD 243
included motor vehicle accidents (n = 43), industrial accidents (n = 4). and impersonal assaults (i.e., nonsexual, assailant not known to victim n = 13). All participants had serious and typically multiple injuries. The mean age of partic- ipants was 38.5 (SD = 11 -2; range = 18-54). Sixty eight percent were male (n = 41), and 52% were Hispanic (n = 31). 33% were non-Hispanic white (n = 20), and 15% (n = 9) were non-Hispanic black. Thirty five percent of partic- ipants (n = 21) were assessed in Spanish. After complete description of the study to the participants, written informed consent was obtained.
Measures
Spanish versions of study instruments were obtained or translated by the study team and reviewed for consistent meaning and comprehensibility by several Spanish speaking clinicians. Prior history and new onset symptoms of psychi- atric disorders were evaluated with the Structured Clinical Interview for DSM-IV (SCID; Spitzer, Williams, Gibbon, & First, 1997). PTSD symptom severity for the preceding week was rated by the Clinician Administered PTSD Scale (CAPS; Blake et al., 1990). Dream reports were elicited by a morning diary created by the first author and utilized in prior studies (Esposito et al., 1999; Mellman, Byers, & Augenstein, 1998; Mellman, David, & Barza, 1999). Items were completed as soon after awakening as possible and included instruction to describe the content of any dream remembered by the participant. This was followed by ratings of the similarity of the content of the dream to the traumatic incident and the degree to which the dream was “disturbing” on a 5-point Likert scale (0 = “not at all,” 1 = “a little bit,” 2 = “moderately,” 4 = “quite a bit,” and 5 = “exactly”P‘exwme1y”).
Assessments were performed during the initial hospitalization, just follow- ing acute medical and surgical stabilization, which was an average of 11.5 days (SD = 9.7 days; range = 1-35) after the traumatic incident. At this point 40% of participants (n = 24) remained on low dose oral narcotic analgesics (maximum of 15 mgm of oxycodon or its equivalent, per day), and none were taking psy- chotropic medication. The CAPS and SCID were readministered in 65% of the original participants (n = 39), 6 weeks after the initial evaluation at which time all participants had been discharged. The participants lost for follow-up were similar to those available with respect to demographic variables and initial PTSD severity.
Dream Caregorization
Dream diary reports were reviewed by the investigative team for consistency of the narrative description with participants’ ratings of similarity to the traumatic event and distress. Other than one report that was excluded because of ambiguity, ratings were considered consistent with descriptions by a consensus of at least two investigators. Reports that were described and rated as moderately to exactly
244 Mellman, David, Bustamante, Torres, and Fins
similar were also rated as moderately to extremely disturbing and were categorized as “trauma dreams.” The remaining dreams featured either low similarity with high distress (i.e., moderately to exmmely disturbing) or low similarity with low distress.
Results
Nature of Dream Diary Reports
Among the 60 participants filling out two to three morning diaries during the initial evaluation, 18 endorsed remembering a dream (30%) and produced descriptions of 21 dreams. Ten of the 21 reports (46%) were trauma dreams. Four of these contained deviations from the actual event such as the presence or location of passengers and the remaining six were rated and described as exact replications. Seven descriptions (33%) featured low similarity and high distress. These featured scenarios that were threatening but tended to be unrealistic. Four dreams (19%) were low for similarity and distress. References to the trauma such as representation of a person or pet present during the incident or of the injury were noted in close to half of the dream reports that were low for similarity.
Dreams and PTSD Symptoms
(For the three participants who recorded dreams in more that one category, the categorization for subsequent analyses was based on the more severe category, e.g., trauma dreams). All of the participants who produced trauma dreams were also rated positively for nightmare symptoms on the initial CAPS, and only one participant rated positively on the CAPS nightmare item did not produce a trauma dream on a diary. CAPS ratings of nightmare severity were significantly associated with dream categories from the dairy: M = 6.2 (SD = 1.6) for the participants with trauma dreams; M = 4.4 (SD = 2.9) with low similarity, high distress dreams; M = 0.67 (SD = 1.2) with low similarity, low distress dreams; and M = 1.3 (SD = 2.3) for nondreamers, F(3,56) = 11.2, p < .001.
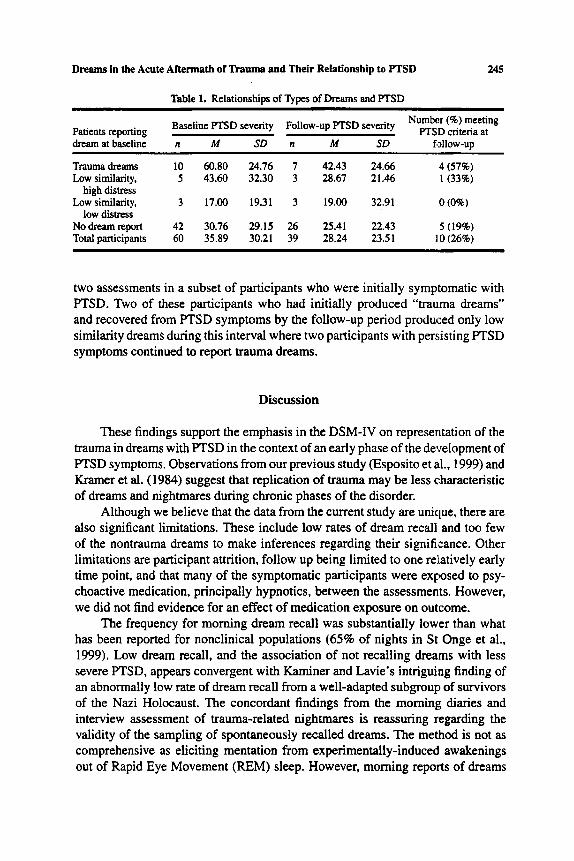
Relationships between the initial dream categorization and concurrent and follow-up PTSD severity, and PTSD diagnostic status at follow up, are presented in Table 1. ANOVA comparing initial PTSD severity across dream categories was significant, F(3,56) = 3.60, p < .05. Post hoc testing by the least significant difference (LSD) method revealed significant differences ( p < .05) between those reporting trauma dreams and dreams with low similarity and distress, and trauma dreams and not dreaming. Small numbers within categories precluded this analysis for follow-up F’TSD. PTSD was significantly more severe at follow up in the group initially reporting trauma dreams compared to those not reporting dreams by t-test (one-tailed), t(33) = 1.68, p < .05. Additional diaries were obtained between the
Dreams in the Acute Anennath of h u m a and Their Relationship to PTSD 245
Table 1. Relationshios of Tvoes of Dreams and PTSD
Baseline PTSD seventy Patients reporting dream atbaseline n M SD
Trauma dreams 10 60.80 24.76 Low similarity, 5 43.60 32.30
Low similarity, 3 17.00 19.31
Nodreamreport 42 30.76 29.15 Total participants 60 35.89 30.21
high distress
low distress
FOIIOW-UP PTSD severity (‘) meeting PTSD criteria at n M SD fdlow-up
7 42.43 24.66 4 (57%) 3 28.67 21.46 1(33%)
3 19.00 32.91 0 (0%)
26 25.41 22.43 5 (19%) 39 28.24 23.51 10 (26%)
two assessments in a subset of participants who were initially symptomatic with PTSD. Two of these participants who had initially produced “trauma dreams” and recovered from PTSD symptoms by the follow-up period produced only low similarity dreams during this interval where two participants with persisting PTSD symptoms continued to report trauma dreams.
Discussion
These findings support the emphasis in the DSM-IV on representation of the trauma in dreams with PTSD in the context of an early phase of the development of PTSD symptoms. Observations from our previous study (Esposito et al., 1999) and Kramer et al. (1984) suggest that replication of trauma may be less characteristic of dreams and nightmares during chronic phases of the disorder.
Although we believe that the data from the current study are unique, there are also significant limitations. These include low rates of dream recall and too few of the nontrauma dreams to make inferences regarding their significance. Other limitations are participant attrition, follow up being limited to one relatively early time point, and that many of the symptomatic participants were exposed to psy- choactive medication, principally hypnotics, between the assessments. However, we did not find evidence for an effect of medication exposure on outcome.
The frequency for morning dream recall was substantially lower than what has been reported for nonclinical populations (65% of nights in St Onge et al., 1999). Low dream recall, and the association of not recalling dreams with less severe PTSD, appears convergent with Kaminer and Lavie’s intriguing finding of an abnormally low rate of dream recall from a well-adapted subgroup of survivors of the Nazi Holocaust. The concordant findings from the morning diaries and interview assessment of trauma-related nightmares is reassuring regarding the validity of the sampling of spontaneously recalled dreams. The method is not as comprehensive as eliciting mentation from expenmentally-induced awakenings out of Rapid Eye Movement (REM) sleep. However, morning reports of dreams
246 Mellman, David, Bustamante, Torres, and Fins
have been found to have similar characteristics as mentation elicited from REM periods occurring later in the sleep cycle (St Onge et al., 1999).
The association of dreams depicting the traumatic event with minimal alter- ation or representation of other events or settings seems consistent with emotional processing theory as applied to PTSD. In this model, recovery is dependent on al- teration of the cognitions and emotional valence linked to a traumatic experience (Foa et al., 1999). Dreaming and its physiologic correlate, REM sleep, appear to offer an opportunity for experiencing threat in a physically relaxed state, and for images from different temporal and physical contexts to coexist. How the activation of a relatively unaltered trauma memory, possibly in conjunction with disruption of the E M state by awakening, contributes to the early pathogenesis of PTSD, and can be targeted by intervention, warrants further investigation.
Acknowledgments
The authors thank Jeffrey Augenstein, M.D., and Steven Cohn, M.D., for facilitating access to trauma patients and Karin Esposito, Ph.D., M.D., for her review of the manuscript. This study was supported by NIMH Grant MH54006.
References
American Psychiatric Association (1994). Diagnostic and staristical manual of mental disorders (4th ed.). Washington DC: Author.
Blake, D. D.. Weathers, F. W., Nagy, L. M., Kaloupek, D. G.. Klauminzer. G.. Charney, D. S., & Keane. T. M. (1990). A clinician rating scale for assessing current and lifetime F'TSD The CAPS-I. Behavior Thempist. 3. 187-188.
David, D.. & Mellman. T. A. (1997). Dreams following Hurricane Andrew. Dreaming, 7, 209-214. Dow, B. M., Kelsoe, J. R.. & Gillin J. C. (1996). Sleep and dreams in Viemam PT'SD and depression.
Biological Psychiatry. 39, 42-50. Esposito, K., Benitez, A., B a a , L., & Mellman, T. A. (1999). Journal of Traumatic Stress, Z2,681-
687. Foa, E. B., Dancu, C. V.. Hembree, E. A., Jaycox, L. H., Meadows, E. A., & Street G. P. (1999).
A comparison of exposure therapy, stress inoculation mining. and their combination for reduc- ing posttraumatic stress disorder in female assault victims. Journal of Consulting and Clinical Psychology, 67, 194-200.
Greenberg. R. Pearlman, C. A.. & Gampel. D. (1972). War neurosis and the adaptive function of REM sleep. Brirish Journal of Medical Psychology. 45, 27-33.
H m a n n . E. (1998). Nightmare after trauma as paradigm for all dreams: A new approach to the nature and function of dreaming. Psychiatry, 61,223-238.
Inman, D. J.. Silver, S. M., & Doghramji, K. (1990). Sleep disnubance in post-traumatic stress disorder: A comparison with non-FTSD insomnia Journal of Traumatic Stress, 3,429437.
Kaminer, H.. & Lavie, P. (1991). Sleep and dreaming in Holocaust survivors. Journal of Nervous And Mental Disorders, 179, 664469.
Kramer. M.. Schoen, L. S., & Kinney. L. (1984). The dream experience in dreamdisturbed Vietnam veterans. In Van der Kolk (Ed.), Post-traumatic stress disorders: Psychological and biological sequefac (pp. 82-95). Washington, DC: American Psychiatric Association.
Mellman. T. A.. David, D., & Barza. L. (1999). Nefazodone treatment and dream repom in chronic F'I'SD. Depression and Anxiety. 9, 146-148.

Dreams in the Acute Aftermath of Trauma and Their Relationship to PTSD 247
Mellman, T. A., Byers. P. M., & Augenstein, J. S. (1998). Pilot evaluation of hypnotic medication during acute trauma response. Journal of Truumric Stress, I I , 563-569.
Mellman, T. A.. Kulick-Bell, R., Ashlock, L. E.. & Nolan, B. (1995) Sleep events among veterans with combat-related posttraumatic smss disorder. American Journal of Psychiatry, 152. 1 10-1 15.
Neylan, T. C., Marmar, C. R., Metzler, T. J., Weiss, D. S.. Zatzick, D. F., Delucchi. K. L., Wu, R. M.. & Schoenfeld, F. B. (1998). Sleep disturbances in the Vietnam generation Findings from a nationally representative sample of male Vietnam Veterans. American Journa: of Psychiatry,
Spitzer, R. L., Williams, J. B. W., Gibbon, M., & First, M . B. (1997). Instruction ikf4nUalfOr the Structured Clinical lnterveiw for DSM-IV (SCID 1997 Revision). New York, NY Biornevics Research Department, New York State Psychiatric Institute.
St Onge, M. A.. Grenier, J., Vinette, S., Vachon, J., Dupuis-Roy. N.. Roussy, F., & de Koninck, J. (1999). A comparison of visual imagery in laboratory and home dreams. Sleep, 221'Suppl. 1). 170.
Van der Kolk, B., Blitz, R., Burr, W., Sherry, S., & Hartmann E. (1984). Nightmares and trauma: A comparison of nightmares after combat with lifelong nightmares in veterans. American J o u m l
Wood, J. M., & Bootzin, R. R. (1989). Effects of the 1989 San Francisco earthquake on frequency and
155.929-933.
of P~ychiatty, 141. 87-90.
content of nightmares. Journal of A b n o m l Psychology. 101.219-224.