Upload
papadonik
View
238
Download
6
Embed Size (px)
Citation preview
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
1/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
DISMANTLING A MYTH:
The Role of Fat and
Carbohydrates in our Diet
by Dr. Med. Wolfgang Lutz
ISBN 3-921500-24-9 1986 by Selecta-Verlag Dr. Ildar Idris
GmbH & Co. KG Planegg V. Muenchen, West Germany
Original title "Leben ohne Brot", translated by Beatrice Idris-
Duncan and Joy Wieser. All rights reserved.
No part of this text may be reproduced in any form or by any
means electronic or mechanical, including photocopying,recording, or by any information storage and retrieval system,
without permission in writing from the publisher.
Service to Danish readers: Danish translation of certain difficultwords and medical terms
(Excerpt 2: page 125-180)
Chapter VII: GASTRO-INTESTINAL TRACT
To anyone holding the view that carbohydrates are un-natural andharmful components of our diet it is quite obvious that the gastrointestinal
http://www.scdiet.org/7archives/lutz/lutzdk.htmlhttp://www.scdiet.org/7archives/lutz/lutzdk.htmlhttp://www.scdiet.org/7archives/lutz/lutzdk.htmlhttp://www.scdiet.org/7archives/lutz/lutzdk.htmlhttp://www.scdiet.org/7archives/lutz/lutzdk.html7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
2/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
tract, being in the front line, is exposed to the most danger. The idea ofintroduction of a low-carbohydrate diet as a general mode of therapy fordisorders of this system is therefore logical, even if contrary to what hashitherto been practiced. Although it has been recommended that refinedsugar and white flour be avoided in some gastrointestinal conditions (*1-2), and gliadin-containing types of grain in another (*3-6), carbohydratesas a whole so far have not been considered as undesirable energy sources.
Too Much Acid
Distressing heartburn is often the first symptom to disappear followingwithdrawal of carbohydrates from the die However severe, and even ifmade worse by factors like the back-flow of gastric juice into theesophagus in hiatal hernia, the chances of success are good. If patientscome back with the complaint that the diet is no longer effective and theirheartburn has returned, a closer look usually reveals that some
carbohydrates have again crept into the diet. Or a gastrointestinal infectioncam be suspected - and treated.
In some way carbohydrates appear to disturb acid regulation, i.e. thenormal state of affairs in which acid is produced by the stomach onlywhen it has something to digest. Only a sick stomach produces digestivejuices when empty. This so-called 'fasting secretion' is the reason for theauto-digestion seen in gastric ulcers, or at least in ulcers near the pyloricsphincter, the duodenum or at the artificial exit of a resected stomach.Excess gastric acid is responsible for or provides the right conditions for,for development of a gastric ulcer, which is deducible from the fact that a
typical gastric ulcer is found only in sites where contact with gastric juiceis possible.
If the stomach is resected so that no more acid can be produced a gastriculcer is permanently cured. In rare cases, however, yet another ulcerdevelops even if further portions of the stomach have been removed in asecond and even third operation. Surprising quantities of acidic gastricjuice can be obtained from such patients by means of a stomach tubeeven in the absence of a test meal or any food whatsoever.
Laboratory tests on such juice reveal that the fasting secretion of acid,just as in patients with a duodenal ulcer, approaches the so-called
maximum secretion. By this, we mean the quantity of hydrochloric acidproduced by the gastric glands when they are strongly stimulated by foodor histamine. Under these circumstances the Zollinger-Ellison syndrome(*7-10), should be suspected, a condition first described many years agoby two Americans, Zollinger and Ellison. Tumors or tumor-like growthsare found either in the islet organ itself or in its immediate vicinity, andcan be removed surgically.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
3/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Gastrointestinal Hormones
In histological preparations of resected material from the above cases,cells were found closely resembling the alpha-cells of a normal islet(pancreas' Islets of Langerhans organ (*11-12). Large quantities of asubstance extracted from them proved to be highly effective in causingacid secretion, and was finally identified as 'gastrin' (*13).
Gastrin is the hormone responsible for gastric secretion. Although not thesole agent eliciting acid secretion it is certainly the most important. I donot intend to go into the physiology of gastric secretion in detail since itwould take us too far from our main theme. However, it should bementioned that apart from nervous influences, which for example causeour mouths to water at the sight or smell of food, or even at the sound ofthe dinner gong, it is gastrin which sets off the flow of gastric juice atmeal-times (*14-15). The substance is produced at the base of themucous glands of the pylorus when the latter is in contact with food. Itenters the blood stream and thus arrives at the glands in the stomach'sbody where hydrochloric acid and protein-splitting enzymes (pepsin,
cathepsin) are produced, and where it can directly and indirectly influencethe stomach movements, particularly the emptying mechanism.
Thus the stomach is provided with a kind of self-regulating mechanism.Gastrin is formed when food enters, and this leads to secretion of theenzymes and hydrochloric acid necessary for digestion in the stomach.When the stomach contents have been sufficiently acidified the sphincteropens and the acid contents enter the duodenum. Here substances areproduced (secretin, cholecystokinin, and enterogastrin for fatty foods)which stimulate the activity of the pancreas and also affect theneutralization of the acid from the stomach, at the same time arresting the
efflux of further acidic stomach contents.
The important point to note is that too much gastrin is produced in allcases of hyperacidity, in gastric ulcers and particularly duodenal ulcers,and in extreme quantities in the Zollinger-Ellison syndrome. But thisgastrin arises in the pancreas and not in the stomach (*13), (*16-23).
In recent years the so-called Verner-Morrison (*24-29), syndrome hasbeen considered to be a mirror image of the Zollinger-Ellison syndrome.The former is associated with diarrhoea, low potassium levels in theblood, and with a deficiency in free gastric acid. Small tumors containabnormally-large amounts of secretin (a hormone similar to gastrin but
with a different effect) may be found in the pancreas. The two syndromes,however, are not sharply distinguishable from one another as thisdescription would suggest. The symptoms can occur in a variety ofcombinations, and may be accompanied by disturbances of a diabetic typesuch as elevated blood sugar or too little sugar (hypos), just as in the caseof tumors of the beta-cells.
The patients often complain of headaches and hot flushes in connectionwith eating, and in fact at such times it is possible to detect abnormally-high amounts of serotonin in the blood and urine. The serotonin is ahormone believed to be formed in the so-called light cells of the islet
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
4/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
organ of the pancreas. Some investigators consider them the source of allIslet cells (*30-33).
The Pancreatic Duct Syndrome
In order to understand how the activity of the various segments of thegastrointestinal tract is controlled we have to go back to what we saidearlier about neurosecretion in connection with the hypophysis. The nervecells of the hypothalamus secrete polypeptide substances which reach thehypophysis via small blood vessels and are then either released into theblood when needed, or stimulate the hypophysis itself to produce proteinhormones such as the gonadotropins, ACTH, human growth hormone,thyrotropic hormone, etc.
The closer we delve into the problem of neurosecretion the clearer itbecomes that it is not confined to the hypothalamus and hypophysis but isin fact a widespread phenomenon. Communication between nerve cells iseffected by means of chemical substances known as neurotransmitters. Inthis way one nerve cell can contact another, its messages can beconveyed either within an organ by means of peptide hormones, or overlarger distances by means of the proteohormones which are produced incertain endocrine organs at the behest of peptide hormones. Thegastrointestinal tract seems to be especially influenced by peptidehormones formed on the spot by neurosecretion.
The neurosecretory centre is situated in the pancreas in round, glandularstructures termed "islets" (of Langerhans), which apparently secrete
insulin directly into the blood since there is no sign of effluent ducts.Insulin is an antagonist of glucagon. The large number of different typesof cells in the islets would suggest that they form still other, as yetunrecognized, incretions.
In addition to the hormones of the pancreas a larger number of more orless well-known polypeptides with their own regulatory functions isproduced in the stomach and intestine. Gastrin is one of them, andalthough normally produced in the cells of the stomach and reaching itstarget organ, the gastric mucosa, via the blood stream, it can under certaincircumstances also be produced in the small intestine and in the islets of
the pancreas. As has already been mentioned, the islets are also the sourceof secretion.
Since the development of a highly sensitive method for detectingpolypeptides, the RIA or Radio Immune Assays, more of this group ofsubstances have been discovered. They are apparently concerned withgoverning the activity of the gastrointestinal tract and its glands, andinclude cholecystokinin or pancreokinin, enteroglucagon (an insulinantagonist like pancreatic glucagon), and the gastroinhibitory polypeptide(GIP) from the duodenum and upper small intestine, which is chemicallyvery similar to secretin and glucagon. GIP inhibits the formation of
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
5/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
gastric acid and promotes insulin production in carbohydrate digestion,and is thus insulinotropic. It has already been mentioned as representingthe probable starting point of diabetes and the reason for hyper-insulinismin carbohydrate eaters. Yet another gastrointestinal hormone is the so-called Vasoactive Intestinal Polypeptide (VIP). It leads to hot flushes anddiarrhoea if produced in excessive amounts.
Originally, i.e. in primitive forms of life, the entire gastrointestinal tractwas probably able to produce these regulatory polypeptides. In the course
of further developments, however, the various parts took on a specializedfunction.
Esophagus, stomach, duodenum, small and large intestine, differ not onlyin structure but also in function, so as to serve the body in the bestpossible way. In the course of this transition glandular organs have fused,in order to produce the liver and pancreas, whose only present connectionwith the intestine is via the ducts through which their secretions enter itslumen. As has already been mentioned, the neurosecretory portion of thepancreas is concentrated in the islets.
Neurosecretion is nevertheless not confined to the pancreas and its isletorgan, but still plays a role over the whole of the gastrointestinal tract.Even though insulin and glucagon are apparently produced exclusively inthe islets the other gastrointestinal hormones can be produced elsewheretoo, like gastrin, at least under pathological conditions.
In the embryo the primitive pancreatic duct from which the pancreasdevelops appears to harbour the primitive form of every kind of cellproducing gastrointestinal hormones. With this in mind I suggested theterm "pancreatic duct syndrome" for all disorders triggered bygastrointestinal peptides.
The cells producing gastrointestinal hormones can be thought of asbelonging to a clan dating back to primitive times. Some members of theclan have built larger houses (the islets of the pancreas) whereas othersstill live in the open or in very primitive shelters.
Nonetheless the clan sticks together through thick and thin, and theirsense of loyalty is such that if one of the members is injured, an outcrywill be heard from the rest. Emanation or irradiation is a familiar idea tomembers of the medical profession.
Apparently a strong stimulus to one gastrointestinal polypeptide or to its
site of production involves to greater or lesser extent all of the others. Notonly is insulin or glucagon produced, but gastrin, secretin, serotonin, GIP,VIP, as well, and probably others as yet unrecognized.
That the disturbances already discussed are due to the carbohydrates inthe diet, and that they disappear if carbohydrates are restricted, isprobably due to the fact that the two chief hormones of the islet organ,insulin and glucagon, primarily regulate carbohydrate metabolism. Theyrespond to too much or too little blood sugar, and the presence ofcarbohydrates in the intestine. And least one of the gastrointestinalpolypeptides (GIP, VIP) has an insulinotropic action.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
6/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
It was previously assumed that sugar injected direct into the bloodnecessarily has a greater effect than the same quantity administeredorally. Surprisingly, the opposite holds true and sugar in fact is muchmore effective if it enters the body via the intestines, i.e. insulinproduction is stepped up much more rapidly and is more persistent than ifthe sugar is given intravenously.
The reason for this is I think that when sugar enters the intestine
insulinotropic substances are produced the mucosa and as their namesuggests they stimulate the pancreas to produce insulin. They are theoutposts which serve to warn the headquarters that sugar is on its way,and that insulin has to be produced for its breakdown.
It might be that these outposts represent the seat of our civilIzationdiseases (see also chapter XIII). Our primitive ancestors learned to livewithout carbohydrate over the course of millions of years and now ourbody, via the above-mentioned outposts, reacts "allergically" to the kindof food that was introduced with grain cultivation, and even more to thelarge quantities of sugar that we have consumed since the development of
sugar-beet cultivation.
The 'clan' reacts as to an enemy against which it is in fact no longerarmed. It throws in all the resources at its command even if the weaponsinvolved are not suited to the purpose. The body produces not only insulinand glucagon but secretin, pancreozymin, vasoactive intestinalpolypeptides, and above all gastrin as well. Like a beleaguered garrison itfinally resorts to producing ammunition in workshops originally intendedfor quite different purposes. Similarly, as a result of prolonged excessiveintake of carbohydrates, gastrin is finally produced by the pancreas aswell as by the stomach.
That this somehow describes the situation is clearly borne out by theobservation that all symptoms connected with the pancreatic-ductsyndrome disappear upon withdrawal of carbohydrates from the diet.Although I have not yet had the opportunity to put my idea into practice Iam convinced that the Zollinger-Ellison syndrome would, if not the resultof a malignant tumor, eventually respond to a low-carbohydrate diet ifcontinued long enough, just as does Morbus Cushing.
There is little doubt that in addition to GIP or VIP the typical fluctuationsin the blood-sugar level and the attendant counter-regulation so typical orcarbohydrate consumers play a special role. This was discussed in the
chapter on diabetes and hypoglycemia. It is striking that in cases ofhyperacidity and duodenal ulcer the maximum acid production inconnection with eating is the same as in normal subjects, whereas the so-called basal secretion in the fasting state is higher than normal. And it isin this fasting state that the tendency to hypoglycemia becomes manifest,with its resultant need for increased glucagon (and gastrin) production.
HIstological similarities between the gastrin-producing cells in tumoursfrom Zollinger-Ellison patients and the glucagon-producing alpha-cells ofthe islet organ support this theory. Viewed in the light of suchobservations it would appear that gastric surgery is being performed in the
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
7/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
wrong place. The removal of the lower part of the stomach (antrum)deprives the organism of a gastrin production geared to the requirementsof the digestive tract, whilst leaving the cells that are active betweenmeals to produce the fasting secretion and ulcers.
I am convinced that we would spare many of our patients the need ofundergoing surgery if we were to put them on a low-carbohydrate diet.An operation is, after all, only a form of mutilation leaving the root of thetrouble untouched.
Gastritis, Enteritis, Ulcers
The above ideas have been fully confirmed by my experience on theeffect of a low-carbohydrate diet in patients with hyperacidity andduodenal ulcers. Both gastritis and ulcers heal if carbohydrates arerestricted. A so-called callous gastric ulcer, however, should not betreated immediately by simple restriction of carbohydrates. These ulcersare stress-induced and a transition to a new diet entails further stress.Therefore one has to give small amounts of cortisol first until the ulcerhas healed and then slowly introduce a low-carbohydrate diet.
In my experience the only permanent relief for an ulcer lies in consistentadherence to a low-carbohydrate diet. Lack of discipline in this respectusually leads to the operating table.
The frequent mention of ulcers in connection with gastro-intestinaldisorders does not necessarily mean the condition is as commonly
encountered in a physician's practice as in a hospital, where there issimply an accumulation of cases that cannot be treated at home. Even theduodenal ulcer is a relatively rare condition, at any rate less common thangastritis, enteritis and colitis.
It was originally believed that mucosal irritations could be detected bymeans of an X-ray. More recently, however, biopsy methods have beendeveloped in which small pieces of mucosa are removed from thestomach or intestine. Their histological examination has provided us withmore detailed knowledge as well as some surprises.
We know that the story begins with excessive irritation of the mucosa andincreased production of gastric acid and digestive enzymes.
At this stage the mucosa presents a fairly normal aspect under themicroscope. X-ray pictures show the so-called fasting secretion, i.e. evenan 'empty' stomach, is full of juice. The mucosal folds are either normalor swollen, indicating that adequate substance is still available. That thistype of gastritis represents the initial stages of the disease and is notanother variation of it is demonstrated by the observation that it is thecommon form in children and young subjects where the disorder is notlong-standing. X-ray pictures of children with gastritis almost invariably
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
8/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
reveal normal or enlarged mucosal folds and a copious fasting secretion.
The longer the process has time to develop the less fasting secretion isseen. The sphincter is open and the stomach is seen to empty its contentsprematurely into the small intestine. In the end, what was initially anexcess of gastric acid and pepsin is now too little and in some cases NOgastric acid can be demonstrated at all. An experienced eye recognizesthis in an X-ray picture, but it becomes very obvious in pieces of mucosaexamined under the microscope that atrophy of the mucosal layers has set
in and large numbers of mucosal cells have perished. Heartburn and othersymptoms of hyperacidity should not be allowed to mislead one. Evenwith such a thin mucosa the stomach can still produce acid in quantitiessufficient to cause a severe burning sensation in the lower oesophagus,whereas the normal stomach moves its contents in a downward direction(except in vomiting), a diseased stomach can in some cases regurgitate itscontents into the oesophagus.
The mucosal atrophy, whether due to chronic damage, or --- as mentionedearlier --- to excessive secretin (GIP, VIP) production which might to beresponsible for the deficiency of acid, leads to a series of consequences
for the digestive apparatus. Raw connective tissue, in the absence ofadequate amounts of acid or pepsin, is insufficiently broken down andeven the juices from the liver and pancreas in the small intestine areunable to complete the process. Such patients often suffer from diarrhoeaif they eat raw or smoked meat. This is no great misfortune and thepatient can easily avoid such foods if made aware of the necessity.
The deficiency of acid, however, results in malfunction of the emptyingmechanism of the stomach. Normally the gastric sphincter shuts as soonas the acid content in the duodenum rises. In this manner the passage offurther acid contents is delayed until the acid has been neutralized by thealkaline juices of the duodenum (bile and pancreatic juice). If the stomachproduces too little acid the point of neutralization is reached sooner, withthe result that it empties too rapidly. The stomach thus loses its functionas a depot and the rest of the digestive tract is overburdened by receivinginsufficiently-digested food.
But breakdown of food is not the only function of the stomach. Forexample, it produces a substance, the Intrinsic Factor, which bycombining with vitamin B-12 (Cobalamine) in the food, and perhaps withother so far unknown substances, renders it absorbable. If the mucosa isatrophic and unable to form intrinsic factor, the vitamin is not absorbedbut is lost in the stool. Since vitamin B12 is essential for growth of the
entire organism as well as for maturation of the red blood corpuscles it isunderstandable that patients of this type suffer from a variety of disordersincluding pernicious anaemia.
Although no-one believes today that gastritis and enteritis are expressionsof bacterial or viral irritations, we still have no exact idea as the cause ofthese common complaints. In my opinion we are dealing with nutritionaldiseases provoked by the high carbohydrate content of the diet ofcivilized man. Carbohydrates elicit production of gastrin, secretin and soon, and in the initial stages the mucosa is stimulated to produce excessivequantities of digestive enzymes, and this at the wrong time, until finally it
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
9/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
succumbs. The process is enhanced by the tendency to tissue deteriorationseen in carbohydrate-eaters. Every organ has to make a contribution tothe toll of protein that is constantly demanded of carbohydrate-eaters bythe mechanism of the adrenocortical hormone. The process is the same asthat already discussed in connection with the striae.
I have described these processes in detail because their understanding isof vital importance in treating such patients. The more recent the processthe earlier the patient comes for treatment, the more fasting secretion,
enlarged mucosal folds and other signs of mucosal swelling andhyperacidity, the sooner can the patient expect to be relieved of hiscomplaint by means of a low-carbohydrate diet. The better-established theprocess, the thinner the mucosa and the more rapid the stomach emptyingthe longer it takes to effect a cure, and in some cases the less completewill this cure be. But an improvement can be expected in any case.
Chronic inflammation of the stomach (gastritis), the duodenum and smallintestine (enteritis), and large intestine (colitis), often occur together,although in most cases the symptoms of one or another of the organs orhormones of the pancreatic duct system usually dominate the picture. The
characteristic symptoms of gastritis are a feeling of sickness, nausea andvomiting in the fasting state, usually tine morning and followingbreakfast, choking, a lump in the throat and a burning sensation thestomach. Fasting pains that are usually improved by food to return asafter-pains a couple of hours later suggest disease of the gastric pylorusor duodenum. Enteritis is usually accompanied by a full feeling aftermeals, rumblings. gas, inability to digest fats and colicky stomach pains.
Fat is not the Culprit
Because fat in the diet evokes unpleasant symptoms in many patients, theopinion has arisen that a gastric diet has to be low in fat. But a low-fatdiet never brings about a cure. In fact the diet that I recommend forpatients can later include large quantities of fat. The patients feeldistinctly better even within a few days and usually are completely wellagain within a couple weeks. But if they attempt to eat carbohydrates theyquickly notice that these were responsible for the discomfort and not thefat or other foods.
In very severe cases of enteritis the small intestinal loops are knotted andswollen, and the patients have a pot-belly similar to that seen in primitivepeoples whose diet consists mainly of carbohydrates. The children oftenalready suffer from Kwashiorkor, a disease characterized by a state ofmalnutrition, swollen belly and oedema, and resulting from their one-sided, low-protein diet. Even in civilized countries we find equivalents tothis disease in which, for unknown reasons, dietary fat cannot be utilizedbut is eliminated in the stool.
A typical disorder of this kind is celiac disease in infants which resultsfrom oversensitivity to the protein gliadin (*3-5), a substance present in
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
10/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
wheat, rye, barley and oats. Since corn, rice and potatoes contain none ofit, it is quite a simple matter to rear the patients on a gliadin-free diet andat the same time ensure their normal development.
The absence of the necessary enzyme for splitting gliadin from theintestinal villi suggests that the gliadin sensitivity is of genetic orimmunological origin. A gliadin-sensitive type of enteritis is alsoencountered in adults in the condition known as endemic (as opposed totropical) sprue (*5). In this disorder, as in other forms of chronic enteritis,
not only can antibodies to gliadin or its individual fractions (e.g. fractionIII) be demonstrated, but also antibodies to hens' eggs, milk, and even torabbit protein (*34-36).
It can hardly be assumed that the defect is of genetic origin in thesepatients but rather that the damaged mucosa permits the passage ofantigens which elicit the production of antibodies in the blood. Thiswould mean that the mucosal damage represents the first step in thedisease and can thus be regarded as the cause and not the effect of auto-immunization.
Itching (Pruritus)
I have another reason for believing that this is indeed the situation. Alarge number of patients visit the doctor on account of itching, which theyreport as occurring after wetting of the skin (bathing or sweating), andalso after eating certain food. If these patients are put onto a low-carbohydrate diet the itching usually disappears after a couple of months.
My explanation is that the diet gives the intestine a chance to heal, themucosa recovers and no longer lets through (or completely breaks down)the food constituents that could previously enter the blood and elicit anallergy.
Since I have been so much concerned with the clinic and radiologicalsigns of enteritis I have come to realize just how many apparentlyclinically healthy patients suffer in this way. Only when closelyquestioned do they admit their discomfort, and for this reason theargument that such antibodies are found in 'healthy' subjects and hasnothing to do with enteritis does not hold water.
It is small wonder that the gliadin-free diet automatically prescribed foradult enteritis is not particularly successful.
When the condition due to low-carbohydrate has improved to the pointwhere the patients can safely begin to add again some carbohydrate totheir diet it is bread and other flour-containing foods that are least-welltolerated. I believe that this is not because gliadin is responsible for theenteritis but because it has a greater allergic effect than other unsplitproteins if it gets into the blood. Therefore bread Is forbidden to suchpatients. They may replace the carbohydrate with fruits, vegetables,potatoes and pulses.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
11/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
The fact that carbohydrates have something to do with gastro-intestinalailments was already known to Prof. H. Lampert, who recommendedrestricted carbohydrate intake for the so-called fermentation dyspepsia(when stools are acidic and smell peculiarly acidulous), and forabdominal flatulence (*36). Had he continued on this path, he surelywould have observed that not only "fermentation dyspepsia" but also"putrescent dyspepsia" responds to carbohydrate restriction.
For the latter disorder he recommended other diets.
Colon Disorders
Constipation
On the whole, constipation is the most common illness of the colon, but itis mostly restricted to the female gender since the female hollow organs,which include the uterus, tend to retain their contents in order to preservethe fetus, instead of expelling them. Therefore women are also moresusceptible to enervation and infections of the urinary tract, but lesssusceptible to ureteric colics.
Without laxatives the stool of chronically constipated patients is brokendown by putrefaction bacteria. The gases produced during this processcan he taken up by the blood and detoxified in the liver. Or the tormentedgut finally rids itself of the stools by the so-called paradox diarrhoea.
Billions of dollars are realized by producers of laxatives but the ailment istreated only very superficially. Experience shows that the effect oflaxatives diminishes with time so that the dosage has to be increased orthe preparation has to be changed. In the long run they are most likelyhealth-detrimental since they cause an evacuation of the bowel byirritating it, and because they have been demonstrated to disturb themineral metabolism (loss of potassium). This constant irritation of themucosa finally leads to the most predominant complaint amongchronically constipated patient: they feel constipated although their colonis totally empty and laxatives would not be necessary.
When these patients come to the physician, he justly recommends thediscontinuation of the medication. But without laxatives the patients haveno stool. If they are put on a low-carbohydrate diet then they definitelyhave no evacuation. Now the last motivating force for the bowelabolished because the fermentation process stops and the entire gastro-intestinal tract calms down. Even the female patients who are notnormally constipated react to a low-carbohydrate diet with an indolentbowel. That is why I have not initially treated constipation with this diet.However, over the years I solved this problem by instructing my patientsto continue the laxatives and by prescribing them instead daily cleansingenema with one and a half litres of warm water without additives in order
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
12/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
to bridge the period of initial change for the worse.
Under the continued diet, sooner or later the stool will normalize. Inchildren it can take one or two days, in young adults one or two weeks,and in older persons a few months, but undoubtedly it will be successfulsooner or later.
Diverticulosis
The wall of the colon consists of several muscle 1 which cross each otherand, like a lattice, leave open spaces through which blood vessels andnerves pass. When these muscle layers weaken, the spaces enlarge to thepoint that mucosa can protrude through the meshwork. These finger-likemucosa protrusions get under the peritoneum, which covers most of thecolon and becomes deformed into button shapes. These "buttons" arecovered by peritoneum on the outside and are therefore fixed in place so
that they can no longer retract. On the inside they contain stool or otherbowel contents.
The number of these so-called diverticula can vary greatly. There arepatients with one or two diverticula and others with 20 to 50. Theygenerally do not cause typical symptoms. Only when they becomeinflamed does the resulting peritonitis create problems; at times itnecessitates immediate surgery. The diverticula are most-commonlylocalized in an area of the large bowel called the pelvic colon, an S-shaped loop between the rectum and descending colon on the left side.Here an inflammation creates symptoms like an like an appendicitis
would be on the right.
Usually a diet rich in fibers is recommended for the treatment ofdiverticulosis because years ago scientists observed that African Negroeswho eat fiber-rich diets have no diverticulosis and also get few othercolon diseases (cancer).
I, however, do not believe in this fiber hypothesis which has become verypopular over the last few years. Man is a hunter and gatherer and not aherbivore. although his original diet may have contained somewhat more-undigestable food residues. Therefore, I also treat diverticulosis with alow-carbohydrate diet very successfully. Here the prevention of an initial
constipation through the regular application of cleansing enemas asdescribed in the previous chapter on constipation is particularlyimportant.
After a few months the patients will have normal stools and no furthercomplaints relating to their diverticulosis. The existing diverticula will notdisappear but no new ones will form. Most of all, the inflammation,which very often exists in the gastro-intestinal canal of consumers ofnormal diets, and which spreads to the diverticula, will heal. Finally, thebowel musculature will strengthen and the original cause of thediverticula, namely the muscular weakness with the enlarged spaces
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
13/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
between the bundles, disappears.
Diarrhoea
I am not talking about the short periods of liquid stool which occur
several times a year due to infections with various bacteria or viruses.Particularly viruses multiply in the gut, enter the blood stream, and finallylead to a general illness.
A frequent traveller knows that "Montezuma's Revenge" is not restrictedto Mexico. On long trips one enters regions with unfamiliar germs towhich one is not yet resistant and promptly becomes ill.
Here I mean the chronic diarrhoea, which is much more common than isgenerally assumed. One just has to visit larger toilet facilities in arestaurant or train station to hear the familiar noise in one of the
neighboring stalls. However, this illness is evaluated differently byvarious people. Some have had diarrhoea for years and have become soused to it that they do not perceive their condition as unusual anymore.
I remember one patient, the foreman of a Mercedes-Re service station,who came to me years ago and told me that he has had diarrhoea for over15 years now and that he had consulted at least ten physicians withoutany success. He did not dare to leave his house anymore; when he had toout anyway, he would immediately look for a rest stop since at times hecould hold his stool not even for one minute.
I prescribed him a low-carbohydrate diet and told him to see me again ina fortnight, because I was sure that the problem would have resolved bythen.
This was indeed the case. He came, thanked me and told me that of themany doctors he consulted previously, not one knew how to help him. Hedid not quite understand that, because if there is mechanical trouble withone the Mercedes-Benz models, all service stations in the whole worldwould be informed and instructed how to repair the defect. Whether thiswas not so in medicine? No, I had to admit: we have the so-calledscholarly medicine with certain dogmatic views, and other views are nottolerated. The many "outsiders" among the medical scientists will surely
agree with me wholeheartedly.
When chronic constipation is to be understood as disturbed motility of thebowel due to an insufficiently-developed colon musculature, which isunable to move its contents ahead (which Is hardly the heart of theproblem), then chronic diarrhoea surely cannot be considered solely asmotility disturbance. Rather, the bowel evacuates because it does notwant to contain tts contents; it is not able to absorb water and to producestool of a normal consistency; therefore it releases the contents of thesmall intestine in a more or less unaltered form.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
14/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
In my experience, acute diarrhoea is followed by a lengthy period ofliquid or soft stool, although through therapy and the elapsed time intervalthe Infectious organism has been killed off and the Infection has beenovercome. Furthermore, this type of diarrhoea can be halted by givinggold or cortisone for several days, i.e. by subduing the immune reaction;therefore we are dealing here with a so-called "auto-aggressive disease".
For reasons which are not yet known in detail, the body starts to mount animmune reaction not only against the infectious organisms but also
against the affected organ. I got the Impression that initially thismechanism does not necessarily have to be considered morbid, that theattack against the affected organ is part of the immune reaction itself. Thebody tries not only to fight the infectious organism, but also to destroy itsbasis for existence, the affected organ, by weakening it with its defensiveforces. One can hardly understand the multitude of existing auto-immunediseases in any other way. These affect not only the gastro-intestinal tractbut also the nervous system (multiple sclerosis, see page 239) and, mostof all, the heart. The myocardial inflammations, which frequently occureven among young people, can most easily be explained in this way.
When diarrhoea after an acute gastrointestinal inflammation does not healand persists for years, one not only has to restrict carbohydrate intake, butalso to slow down the immune reaction. This can be done with cortisoneor gold preparations. The former is less harmful and therefore should betried first. I prescribe 10 mg Prednisolon or 8 mg Triamcinolon (early inthe morning for eight to ten days) and repeat the same treatment in caseof a relapse.
Frequently an immunosuppressive therapy is not even necessary. Afterone or two weeks the stools normalize although often accompanied byabdominal pain. One has to know this in order not to break off the diet,believing it to be inappropriate. Apparently the large bowel, which hasnot actively worked for months or years as it has discharged the contentscoming from the small intestine in a more or less unaltered form, rebelsagainst having to work again.
Sometimes even a period of constipation follows, which should be treatedwith cleansing enemas, since laxatives should be avoided at all cost.Ultimately, chronic diarrhoea will always heal under the above-mentionedcircumstances and with a low-carbohydrate diet.
Crohn's Disease
Why chronic diarrhoea, as described above, develops into a MorbusCrohn (English: Crohn's Disease), named after the American physicianDr. Crohn (*37) is not clear. Apparently there are connections betweenthe two, because in my experience, a "Crohn's" always has a pro-dromalphase in which the patient has diarrhoea over some period. It is, so tospeak, nothing else but the extrapolation of the chronic enterocolitis. Herethe illness is not limited to the mucosa alone but Involves all levels of the
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
15/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
bowel, the mesentery, and the lymph nodes; the gall bladder, theduodenum, and the stomach can be affected as well. A form ofInflammatIon, called granulomatous, is characteristic. Infiltrations aroundthe bowel in the peritoneal cavity can result, but they also can melt down,form abscesses, and leave fistulas, through which the bowel contents canenter the bladder, the vagina, or, most frequently, exit next to the rectumor through the abdominal wall. Often they can only be removed surgicallyand often without ideal results.
Crohn's disease becomes more common from year to year. When I startedto treat my colon-patients with a low-carbohydrate diet 25 years ago,there was no Crohn's patient among them. Lately they have becomealmost as frequent as patients with ulcerative colitis.
Morbus Crohn differs from ulcerative colitis in that there often is nointestinal bleeding, and in its different localization. Crohn's rarely occursin the rectum; its frequency Increases upward; often it affects only thelower small intestine. Ulcerative colitis, on the other hand, prefers therectum; its frequency decreases continually toward the small intestine; atleast sporadic bleeding occurs and no fistulas form. There are
intermediate forms between ulcerative colitis and Crohn's disease:patients with intestinal bleeding and fistulas, those with involvement ofthe large and small Intestine.
The distinction between Crohn's and ulcerative colitis is of significance.Crohn's disease, in contrast to ulcerative colitis, heals with greatprobability within six months to one year and usually withoutcomplications. There are individual patients who have difficultieschanging from the high-carbohydrate standard diet to the low-carbohydrate diet; they worsen acutely, have diarrhoea, fever and so on.However, this rarely lasts longer than a few weeks. Potential remnants(fistulas, etc.) must be removed surgically if they do not healspontaneously; also narrowings in the bowel may require surgicalintervention. However, if possible, one should wait until the underlyingillness has resolved, until iron level, erythrocyte sedimentation and stoolshave normalized.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
16/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
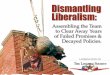
Fig. 16:103 patients suffering from Crohn's disease were treated by a low-carbohydrate diet. Aftera quarter of year most patients (85 percent) showed remarkable improvement in theirhealth. After half a year, more than 60 percent were asymptomatic, after one year morethan 70 percent and after one and a half year about 85 percent. This is in contrast withulcerose colitis, which Is shown in the lowest line, improvement of which runs much
slowlier on the same diet and often is interrupted by relapses.
Crohn's disease generally thought of being incurable can so be shown to be very wellaccessable to dietary measures.
In March 1985 I published 103 Crohn's patients (Fig. 16) which I hadtreated up to then (*74-75), and with this information I hope to be able toconvince my colleagues to first try to treat these unfortunate patients withdiet instead of cortisone and scalpel. Perhaps then also a breakthroughregarding other diseases can be reached. In recent years German andEnglish authors (*38-39) have found that Crohn's patients experience acertain improvement after relinquishment of sugar and so-called refinedcarbohydrates. This corresponds to today's widespread conception thatonly the refined carbohydrates are harmful, i.e. sugar and white flour.
I do not believe this. To the contrary, I am convinced and have seen againand again that bread and particularly whole meal bread is not toleratedwell by patients with gastro-intestinal ailments. Starch turns into sugar inthe bowel anyhow, perhaps somewhat slower than if one eats sugar andonly dextrose, but in principle the result is the same. At least this
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
17/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
recommendation points in the right direction: restriction of carbohydrates.
Often a gluten-free diet is tried, particularly for chronic diarrhoea andCrohn's disease, because the alcohol-soluble fraction of the grain proteincauses the so-called Celiac Disease in children, which is accompanied bypulpy, flat-cake-shaped stools, and impaired development. But I haveseen many times that grain protein is not the cause of this colon disease.Again and again patients were on a gluten-free diet for months or years,unsuccessfully, but responded to carbohydrate restriction despite of
gluten.
Recently the consumption of margarine and other artificial fats as causefor Crohn's disease has been discussed, based on the fact that in Franceand in the WalIonic part of Belgium, where less artificial fat and morebutter is consumed, Crohn's disease occurs less frequently (*40-41).
Indeed, the increase in Crohn's disease in the German-speaking countriesin the last years correlates with an increase in margarine consumption.One speculates that the artificial fats are not broken down and absorbedproperly, so that their metabolites enter the lymphatic vessels and cause
the described granulomatous inflammations. This could be quite true.Artificial fats are, considering human evolution, definitely less naturalthan carbohydrates, but I have among my patients cases of Crohn'sdisease who have only eaten natural fats and never artificial fats, but Ihave none who has eaten no carbohydrates. Yet I can imagine that theconsumption of artificial fats supports the tendency to develop thedisease, when carbohydrates are consumed in large quantities.
Ulcerative Colitis
Ulcerative colitis is located at the lower end of the continuum "chronicdiarrhoea ---> Crohn's Disease". It may begin one day quite harmlesslywith the appearance of blood in the stool. The physician diagnoseshemorrhoids which cannot be found with the rectoscope. Instead he seesa reddened mucosa which starts bleeding at the slightest touch or whenthe overlying purulent layer is removed. In mild cases this process isrestricted to the rectum; the more severe the disease the further it extendsupward. In contrast to Crohn's Disease the small intestine, the gallbladder,the duodenum, and the stomach are never involved. There are no
infiltrates, no perforations, and no flstulas. Only the mucosa and theunderlying muscle layer are affected. However, in time both are destroyedto an extent that the whole colon contracts into a short cylinder, which iscompletely motionless and has lost most of its function.
At least these patients still have their natural anus and not an artificialabdominal one. All this is bad enough but the patients would and actuallydo put up with their bloody stools, abdominal pain, and diarrhoea, if thedisease would not become life-threatening by turning into the so-calledtoxic megacolon or by degenerating malignantly. A toxic megacolon candevelop at any time as long as the ulcerative colitis is active. Only three
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
18/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
patients of a total of 285 that I have treated up to the end of 1984 havedied. One was a relatively young man who had recovered quite wellunder a low-carbohydrate diet and had gained 20 kg of weight. Suddenlyhe became acutely ill with high fever and abdominal pain. He wasadmitted to a clinic but was operated on too late because he had fiercelyrefused this operation. Another one underwent surgery without myapproval; the third, a very old lady, died two months after operation ofthrombo-embolism.
Surgical Therapy
Of all patients with ulcerative colitis 20 to 30% sooner or later have to beoperated on if they do not eat a low-carbohydrate diet. The constant lossof blood and iron and the continuously-deteriorating general healthnecessitate the removal of the colon and the creation of an artificial anus(*42). Only two of my patients had to have their colon removed. Of
course I cannot be certain that one or the other who was lost to follow up(who did not answer my repeated inquiries) did not have to have hiscolon removed after all. Certainly there is a limit even to what a low-carbohydrate diet can do, a stage of the disease so advanced that thetransition to a new diet is not tolerated or effective anymore. Maybe thepatients gave up after months or years of dieting, or other reasonsnecessitated surgical intervention.
With the surgical removal of the entire colon the disease is finallyovercome. Not only the colitis is resolved because the diseased organ isgone, but with it all other symptoms of a chronic colitis which can occur
in the eyes, skin, and the joints. They manifest due to an outwardradiation of the immune reaction from the colon to other organs.
There is still one other possibility before the operation, and that is goldtherapy. Gold is a well-known anti-rheumatic drug which was usedextensively to treat joint inflammations before the newer non-steroidalanti-inflammatory drugs and cortisone preparations became available.Gold is directly taken up by the immune-competent cells, the white bloodcells and their progeny; it inhibits their activity and thereby improvesimmune diseases. The leukocytes are not able to attack the colon'smucosa anymore.
Gold therapy should only be applied to severe cases of ulcerative colitisbecause sometimes it causes side-effects like week-long fever or urticarialskin rashes. It can also alter the hormonal status. I have observed that thegonadotropin secretion decreases (see page 94), which can compromisesexuality. In women this is not so bad, sometimes even advantageous,because menstrual breast pain disappears. However, in men sexualpotency often declines. Of course, in severe cases of ulcerative colitis onewill have to ignore these side- effects, since usually the question iswhether the colon can be preserved or not. The side effects usuallydisappear with time.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
19/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Low-Carbohydrate Nutrition
I can only report positive about my ulcerative colitis patients (*43-47).Alone the number of more than 200 patients is unusual for a practitioner.It indicates that one patient recommends him to another. Many patients
came to me from hospitals, where these unlucky people congregate andare told "There is no diet for ulcerative colitis or Crohn's Disease. Eatwhatever you can tolerate. Take your medication and come back to uswhen you have a relapse. Eventually you may have to be operatedanyway."
Of the first 74 patients, whom I have treated until 1979 with a low-carbohydrate diet (*46), approximately 60% were without complaintsafter two years, had normal laboratory values, and a normal-lookingrectal mucosa (figure 17, see also color plate following page 348). Theremaining 40% took longer, four, six, eight years, until the bleeding
stopped, iron levels normalIzed, diarrhoea and abdominal pain subsided. Ihad only two patients who took longer than eight years until their diseasecalmed down.
protein fat carbohydrate kcal kilojoule
sum of 12 cases 1241 1866 868 25422 106391
average per case 103 156 72 2118 8866kcal per 24 hours 422 1395 295 - -
Percent calories of mainnutrient sources
20 66 14 - -
Table 1:
Values for actually consumed nutrient componentsof twelve patients with ulcerative colitis after a low-
carbohydrate diet for several months, (*48).
Flashlight photographs yield interesting findings (color plate followingpage 348, top). One commonly sees yellow spots at the beginning oftreatment, which are interpreted as superficial mucosal ulcers; theydisappear after several months of a low-carbohydrate diet. Then theintestinal mucosa looks like that of healthy individuals.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
20/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
The same can be seen on fine-grained pictures of small pieces of mucosaremoved during rectoscopy. One can see that the inflammatory process,the many white blood cells in the mucosa, disappear, when patients liveon the diet for some time.
Fig. 17:
Graphic depiction of the values of table 2. The most severe symptomsdisappear first, contact hemorrhaging last. Simultaneous increase ofpercentages of symptom-free patients_____ = without findings;. . . . = only contact hemorrhaging;- - - = spontaneous hemorrhaging;- . - . = ulcers and fibrin
Absolute Percent
years 0 2 4 6 8
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
21/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Progress of ulcerative colitis of 74 patients' on a low-carbohydratediet. Criteria: rectoscopic findings. Decline of hemorrhage and ulcers
during two to eight years. Increase of rate of healing to over 90percent.
Certainly this is not an easy form of therapy. It requires cooperation andsacrifice from the side of the patient, patience from side of the physician,and time. Whoever believes he can get rid of his colitis in a few monthsis mistaken. But one has to see the success of the diet in relation to itsalternatives.
Psychotherapy
For one there Is psychotherapy. Every other one of my patients hadundergone previous psychiatric treatment. Due to the lack of success ofconventional therapies it was commonly assumed that colitis must be apsychosomatic disorder.
These patients asked me how they had given the impression ofpsychological difficulties. They thought they were happily married, hadno problems, sufficient income, by no means the feeling that somethingpsychological had Influenced or even caused their disease. The followingletter of a doctor is characteristic for this situation.
October 23, 1980
I want to thank SELECTA for referring me to Dr. WolfgangLutz in Salzburg and his methods of treating ulcerativecolitis, and for his book "Leben ohne Brot (life withoutbread), which I became acquainted with in November 1974. Atthat time I had suffered from this disease for severalyears. I had rectal ulcers and crypt abscesses. None wasable to help me. I was allergic to drugs and experiencedunpleasant side effects from cortisone, swollen knee joints,edemas of the legs, nocturnal sweating, sleeplessness andCushing's symptoms. The commonly-recommended diets did nothelp at all. I felt I was stuck on a dead-end road.
Now, after two-and-a-half years of low-carbohydrate diet,everything has changed. Not only the colitis has healed butalso the stomach problems have disappeared. I am totallyconvinced now that this illness is in no respectpsychosomatic but purely a nutritional problem. I only regretthat most colitis patients will go on to be consideredpsychosomatically ill and will not be treated with the onlyeffective therapy, that is carbohydrate restriction, justbecause doctors do not believe in it."
The second alternative is the removal of the entire colon and the creationof an artificial anus. Certainly there are cases where this is finally the last
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
22/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
possibility to cure a chronic colon illness. Patients are usually capable toput up with anything their fate imposes on them, but whoever has had anartificial anus, knows what that means. As mentioned before, I have lostone patient who was operated on too late because he absolutely refused tohave an artificial anus. Resides this one, however, I did not have to referone single patient of mine to surgery and I hope this will be so in thefuture.
In contrast to Crohn's Disease, even after the resolution of an ulcerative
colitis there can be a relapse. From year to year these relapses becomeless probable and less severe. Two of my patients have had a relapse afterten years, one after six, and one after four. The recurrent disease wasusually mild and lasted only a few weeks.
An Immune Disease
This is because ulcerative colitis is distinctly an immune disease (*49-57). Immune reactions are supposed to protect us from external enemies.Let us consider the hemolytic streptococci which are dangerous germs.The first encounter with them causes scarlet fever. During the progressionof the disease the organism develops immunity toward the pathogen. Nowthe immune system, represented by white blood cells and bone marrowcells, knows the germs. The immune person will never fall ill of scarletfever again. Most other childhood diseases proceed similarly; a child willonly contract them once and then never again.
The immune system never forgets; it also does not forget if it ever has
been sensitized to the body's own organs. Basically what Prof. LudwigDemIing, a specialist of gastrointestinal diseases, said, still holds true:"Once colitis, always colitis." Demling meant this in a different context,namely that once a person has ulcerative colitis, he will never get rid ofthe disease again. Rut this is different under a low-carbohydrate diet.Once a person has colitis, his immune system will remain primed towardhis colon, but his colon becomes more resistant and can cope better withthe immune system's attacks. After a while the immune system losesinterest in such attacks. Because the colon does not bleed or otherwisereact to the attacks, the immune system is less stimulated and its reactionsare less intense.
There is a good analogy to this: we all contract chicken-pox duringchildhood. Some develop a typical rash, others just have fever buteverybody has had chicken-pox. With increasing age the immunityagainst this pathogen wears off, so that we can be infected with it again.This time the infection manifests itself in the form of shingles. Sometimesthis reinfection can be very extensive; however, usually it passes withoutfever and is restricted to small areas of the skin.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
23/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Lactose Intolerance
There have been claims that milk may be harmful for a patient withulcerative colitis (*42), (*49). I have never observed anything of thiskind. Certainly a patient with an undiagnosed lactose intolerance willhave diarrhoea after drinking milk. In these cases the enzyme lactase,which splits the milk sugar molecules, is missing. Therefore milk sugarcannot be absorbed by the intestine and transferred to the blood. It
reaches the colon in an undigested form and causes diarrhoea. But thishas nothing to do with ulcerative colitis.
Another danger, that a patient with ulcerative colitis has to face, ismalignant degeneration, i.e. the development of colon cancer. Usually ittakes ten to fifteen years for a cancer to develop. Generally these patientshave had their colitis since their youth; often cancer develops at multiplesites. Whether or not patients who have been on a low-carbohydrate dietdevelop cancer, I cannot say. Among my first 100 patients I had two casesof cancer. One woman simultaneously had leukemia, a malignant blooddisease, and colon cancer. She was operated in 1980 and is well now, also
regarding her leukemia. The second case was an older man. After he hadbeen well for over a decade, hemorrhages recurred. We found asuspicious area in his colon but a biopsy taken at that site was negative.Eventually we operated anyway; it was cancer. The surgeon told me laterthat he had not found any indication of ulcerative colitis in the colon.This was after more than ten years of the diet; the disease had resolved tothat extent under the diet. Postoperatively the patient started to eateverything again, just to come back to me with a relapse of his colitis.Now his surgeon also uses a low-carbohydrate diet for colitis patients inhis hospital.
Medication
The medication cannot be discontinued immediately since it takes a littlewhile until the diet takes effect. First one should try to wean the patientfrom cortisone since these artificial adrenal cortex preparations generallyinhibit protein synthesis. That means they do not only suppress theproduction of immune cells and thereby subdue the symptoms, but alsointerfere with the healing of the mucosa. Eventually one will be able to
discontinue all medication. Should there be a relapse in the first fewyears, one can temporarily take up the medication again. A mild relapsedoes not require medication.
I have a whole file of thank-you letters from patients who had tried everypossible therapy unsuccessfully and finally were left with surgery as theonly option, before they came to me. Certainly there are more than 50,080cases of Crohn's disease and ulcerative colitis alone in the German-speaking countries. Why are they not put on a low-carbohydrate diet?Why does not this method become established? I can only say that I havetried everything. Between 1965 and 1981 I published five scientific
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
24/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
papers in respectable medical journals, I have written over 40 letters toeditors of scientific journals, I contacted the societies for patients ofCrohn's disease and ulcerative colitis and have not even received a reply.
I do not believe that, of all the letters the postal service handles, it has lostexactly these. There Is no limit to the arrogance of orthodox medicinetoward all outsider methods, toward acupuncture, neural therapy,chiropractic, homeopathy. Caution is partially justified but none even hadthe courage to use these precise methods of this orthodox medicine to
prove the outsiders wrong. To ignore something that comes from outside,from a physician who "only" practices and does not teach at a university,in my opinion is irresponsible. In my office I have posted a saying byMark Twain: "A person with a new idea is a crank until the idea turns outto be right." I hope this will happen for the sake of the many ten-thousands of colon patients who today can still "eat what they cantolerate".
Irritable Colon
This entails complaints which the patient associates with his colon,because they commonly pertain to bowel movements and are felt alongthe colon. The well-known Swedish physician Axel Munthe a long timeago associated this kind of colitis with a whole variety of hysterical traitsand thereby turned it into a fashionable disease. The term "colitis" slowlybecame removed from the colon and became a disease of those socialcircles who were able to afford to have it.
However, the irritable colon actually exists as a mixture of all theconditions which have been discussed so far: constipation, diarrhoea,abdominal cramps, irritations, and the like. Some patients excrete withtheir stools large amounts of mucus. They are worried because the mucuslooks like pieces of tissue and they believe they are excreting the actualmucosa.
For this condition the term colitis or colica mucosa was coined. Butsurely it is not an isolated disease but rather an irritation of the colonwhich leads to an excessive stimulation of the mucous glands and theexcretion of the mucus. All these conditions are caused by an excessiveintake of carbohydrates.
This can simply be concluded from the fact that they resolve quickly on alow-carbohydrate diet. Too bad, we do not live during Axe Munthe'stimes, although the hysterical connotation would not have convinced theupper class at that time, that this is simply a carbohydrate-associateddisease. One would have clung to the hysterical symptoms and wouldhave looked for another physiological substrate.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
25/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Iron and Calcium
I have observed that the low iron levels in the blood of patients withcolitis ulcerosa may return to normal an a low-carbohydrate diet. Thefrequent intestinal haemorrhages in ulcerous colitis cause large losses ofiron, an important component of the red blood pigment haemoglobin. 100
mL (1/10 L) of blood contains 14 to 16 grams of haemoglobin, of which0,34% is iron. Our approximately 5 litres of blood therefore contain about2.8 g of iron (an additional gram is present as tissue iron in enzymes andiron depots). It is therefore not surprising that the iron levels in the bloodrise when the haemorrhages associated with colitis ulcerosa are stopped.
In many cases, however, the haemorrhages do not stop at once, but theblood iron values nevertheless begin to rise. They even return to normalin patients who have never had haemorrhages and never suffered fromcolitis ulcerosa (*62).
What is the reason for this improvement in the blood iron on a low-carbohydrate diet? Cessation of haemorrhage is certainly not the onlyreason because we have seen that the diet is also effective in cases whereno bleeding occurred.
If the stools are chemically analysed for blood (e.g. by means of thebenzidine reaction) it turns out that on a normal diet some patients show apositive and some a negative reaction. But even the former have blood-negative stools on a meatless diet so that it can be concluded that theblood-positive reaction previously obtained was due to the meat in theirdiet. On a low-carbohydrate diet such patients lose their blood-positivestool, even though they now are eating meat. The process of meat
digestion must have improved in some way.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
26/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Fig. 18:The behaviour of (a) hypo- and (b) hypersideroseson a low-carbohydrate diet (72 g) without othertherapeutic measures. The figures of "n =" showhow many pations were investigated at each point.
a: 38 cases with manifest hyposiderosis. In inaverage a normal iron level is attained after sixmonths.
b: 38 cases with hypersiderosis approaching normalwithin 10 weeks. The main effect of thecarbohydrate restriction is seen in the first fourweeks, in which the mean value drops to 140 mu.
We can thus partially explain the rise in iron in the blood of iron-
deficient patients on a low-carbohydrate diet. The iron contained in ourfood varies in quantity and absorbability. Vegetable matter is relativelylow in iron and even this is not readily digestible, whereas meat containslarge amounts of iron, both in the blood remaining in the blood vessels aswell as in myoglobin, an iron-containing pigment of the muscle cells.Further, iron is present in meat in combination with the organic complexprotoporphyrin, a substance known as haeme. Whereas iron is normallycompletely dissolved out of the food in the intestines and traverses theintestinal mucosa in molecular form, it is absorbed as a complex inhaeme, a fact that considerably facilitates its uptake by the body (*58-61).Thus the iron in meat is in this respect superior to that in vegetable
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
27/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
foodstuffs.
The elevation of low iron levels in the blood which results from a low-carbohydrate diet may be brought about in three ways:
a) The food contains more iron (meat)b) This iron is more readily absorbed.c) Improvement of meat digestion in the intestine, thus leading toincreased uptake of iron. A diseased intestine permits the loss of
undigested food and thus of the iron in it, whereas the healthy intestinebreaks down the food, takes up the iron, and the stools give a blood-negative reaction.
Although these three factors undoubtedly play am important role I believethat still another factor, as yet unrecognized, is involved.
Among my patients were cases that had already received large quantitiesof iron, some by injection, without any improvement having beenachieved. Lack of iron therefore cannot have been the reason for the lowiron levels in the blood. The low-carbohydrate diet must exert its effect at
some other site (*62).
Too Much Iron in the Blood (Hyper-siderosis)
The same diet also has a beneficial effect on abnormally high iron levels(*62). Fig. 18 includes 38 cases in which an elevated iron level respondedto restriction of carbohydrate intake. Cases of siderosis (too much iron in
the blood) are even more common than sideropenia (too little iron) andare important since they may lead to deposition of iron in the tissue andthus to severe metabolic disturbances (haemochromatosis).
The Bantus use only iron vessels for cooking and their diet thereforecontains adequate quantities of iron. Anyone, like the Bantus, eating foodfrom iron pots, accompanied by large amounts of carbohydrate, maysuffer from siderosis.
The Bantus could probably change this, either by giving up their iron potsor their carbohydrates.
Joking apart, the fact that one and the same measure, in this case a low-carbohydrate diet, can restore abnormal to normal from both directionsstrongly suggests a common causal effect. It appears that carbohydratesare cause of both disorders and, in a manner as yet unknown to us, rob usof our ability to keep our iron balance in order. As will be seen the sameholds for calcium.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
28/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
An Example Provided by the Kung
Iron deficiency disease serves as an example emphasizing that we wereoriginally hunters and meat-eaters, that our metabolism is geared to thepreferential treatment of the iron from meat and has neglected theutilization of iron from vegetable matter. As long as we consume meateverything is all right, but if we go against our nature and eat onlyvegetable matter we get into difficulties. Although these troubles canoften be circumvented by means of iron pills the solution is not an ideal
one.
Recent reports on investigations made among the Knng, a primitive tribeinhabiting the Kalahari desert In South Africa, seen to confirm the ideasput forward above. For 11,000 years the Kung lived a nomadic existencein the same region. In recent decades, however, some of them havechanged to a sedentary way of life and have taken on the nutritionalhabits of the neighbouring Bantus (but not their iron cooking pots). Thenomadic Kung live as they always have done on neat, vegetables and nutswhereas those who have settled down live on cereals and soya milk. Thelatter show signs of iron deficiency (as well as obesity and high blood
pressure), conditions which are not found among the nomads (*63). Thedifference between the two groups, just as between us and ourforefathers, is in the meat and carbohydrate content of their diet.
The general improvement in intestinal function on a low-carbohydratediet is reflected not only in the normalization of the low iron levels in theblood but also of calcium levels. I have observed a number of such casesof idiopathic hypocalcaemia (for which no particular cause could bediscovered) over a number of years. They are shown in Fig. 19.
Low blood calcium levels are mainly seen in disorders of the thyroid or
parathyroid glands. If the parathyroids, of which we usually possess six,three on each side, are damaged or erroneously removed during a goitreoperation the blood calcium level may drop radically and so-called tetanywith muscular spasm may ensue. In my patients, however, the situation isdifferent and cannot be alleviated by administering parathyroid hormone --- which usually has the same effect --- the so-called calcinosis factor orvitamin D. In most cases it looks as if the ability of the Intestine to takeup calcium from the food is impaired.
My first case of this kind was a colleague suffering from chronicinflammation of the pancreas and the small intestine. He came to me withthe symptoms of tetany and blood calcium values of 6 mg/dL (instead of
the normal 10.5 mg/dL. On a low-carbohydrate diet he recovered within afew months, the blood calcium values returned to normal although nomedicinal calcium had been prescribed. Several of my patients hadalready tried treatment of various kinds in clinics or hospitals without anysuccess, and not until I put them on a low-carbohydrate diet did theirblood calcium levels become normal.
If we think back to the cases of low iron levels discussed above it istempting to adopt the view that here, too, it is the intestine that isresponsible for the disorder.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
29/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Fig. 19:Abnormal low calcium levels normalize withcarbohydrate restriction.
Bile and Liver
In 1960, when I began to use a low-carbohydrate diet in treating patientswith abdominal complaints, I excluded those with gall bladder troubles. It
was an accepted fact that fat and roasted products were bad for them, andwithout fat it is impossible to prescribe a low-carbohydrate diet. In fact,experience shows that gastritis does not heal without the addition of fat tothe low-carbohydrate nutrition. When a patient tells me (which is rarelythe case) that the prescribed diet has brought no relief to hisgastrointestinal troubles I look not only for chronic constipation but alsotry to discover whether, supposedly for slimming purposes, (or on accountof the cholesterol level, see later) the fat intake had been kept down.
Among my successfully-treated gastrointestinal patients more and morecases have later turned out to have been suffering from gall bladder
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
30/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
disease as well. In spite of this they had responded well to the low-carbohydrate diet and its accompanying additional fat.
I gradually began to include gall-bladder patients in my dietaryprogramme. A patient with any kind of gall bladder complaint, e.g. gallstones, ought in fact to experience some symptoms as a result of eatingfat. The function of the gall bladder is, after all, to make available a largequantity of concentrated bile at the beginning of the digestive process.This involves contraction and the expulsion of its contents, a process
which is inevitably painful if gall stones are present since the latter cannotbe expelled (otherwise they would no longer be inside the gall bladder).
Apparently a low-carbohydrate diet leads to an improvement in thesituation along the entire length of the digestive tract, and thus also in theregion of the bile ducts, so that a colic becomes less likely. It should beborne in mind that the size of the gall bladder and the quantity ofconcentrated bile stored within it are adapted to a human being in hisnatural state, where he often ate nothing for days on end and then quitesuddenly consumed large amounts of meat and fat. For us, eating threetimes daily, the organ is in fact oversized and even the volume of bile at
the disposal of a gall bladder containing stones, and of the so-called liverbile secreted by the liver, suffices for the process of digestion. This is whyit is possible to live comfortably after operative removal of the gallbladder.
When to Operate
Instead of recommending patients with a pathological X-ray diagnosis ofthe bile system to consider an operation in the immediate future, I nowprescribe a low-carbohydrate diet plus medication aimed at slightlysubduing the intestinal flora. I endeavour to see the patients through thefirst couple of weeks, which is not usually difficult, and if they feel animprovement then they no longer press for an operation.
All patients who in the end had to have an operation despite a low-carbohydrate diet, had stones in a partially-functioning gall bladder,which filled with contrast agent during the X-ray examination and wascapable of contraction at the appropriate stimulus. I cannot recall a singlecase in which a gall bladder already totally out of action (i.e. in which no
contrast shadow appeared) had to he operated upon. It appears that, givena low-carbohydrate diet, it is the contractile gall bladder with stones andnot one totally tilled with stones and unable to contract and empty thatrequires operation.
Post-Operative Complaints
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
31/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
A further point seems to me to be of importance. Sometimes patients arenot satisfied with the result of a gall bladder operation, and complaints ofpost-operative complications are frequent. They have been termed the"post-cholecystectomy syndrome". It is known that common enteritisoften leads to colicky sensations in the upper right abdomen. If a patientwho has had an operation to alleviate symptoms of this kind or for gallbladder trouble tries to eat anything he likes, the enteritis or inflammationof the bile ducts and thus the accompanying symptoms often persist.Alleviation is to be found solely in a restriction of dietary carbohydrates,
supplemented at first by the above-mentioned antibiotic measures.
Inflammation of the Bile Ducts (Cholangitis)
Since liver and gall bladder are to a large degree functionally involvedwith one another it is to he expected that the same success obtained bydietary treatment of patients with diseases of the gall bladder and bile
ducts can also be achieved in diseases of the liver. In cases of a swollenliver resulting from an infection (by bacteria etc.) in the smaller bile ductswithin the liver, diet and antibiotics in fact bring relief as readily as in thecase of gall bladder disease. Such cases are by no means rare. In contrastto a chronic hepatitis, in which the liver cells themselves are inflamed,the enlarged liver is remarkably sensitive to pressure. The infection of thebile ducts probably comes from the inflamed and infected small intestine,and heals when the enteritis itself is cured.
Inflammation of the Liver (Hepatitis)
It was to be expected that the situation would not turn out to be so simplein hepatitis (termed "infectious jaundice" in its acute stage). And at thispoint I am obliged to digress considerably.
We know that animals and humans possess a small depot of carbohydratein the form of glycogen in the liver and musculature. An unhealthy livertends to lose its glycogen and to store fat in its place, from which wasconcluded years ago that patients with liver complaints require plenty ofsugar and other carbohydrates but little fat, in order to maintain a normalglycogen content. In the meantime, however, it has become clear that thisstrategy is not successfulI. Professor Eppinger, a well-known Viennesephysician, was already of the opinion that sufferers from liver diseaseshould not be put on a very low-fat diet even if they had jaundice. Duringthe Second World War Patek in the USA propagated a high-calorie, high-protein diet for patients with cirrhosis of the liver and abdominal dropsy(*64). The Patek diet nevertheless contained large amounts ofcarbohydrate so that in the long run it was not successful. If a patient isgiven more protein, then some other foodstuff has to be cut down, e.g.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
32/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
carbohydrates, and additional fat has to be permitted.
A variety of observations suggest that, contrary to what has previouslybeen accepted, restriction of carbohydrates in favour of more protein andfat is also beneficial to a diseased liver. Statistics from infectious jaundicehave revealed that a high-protein, high-fat diet brings somewhat betterand in no case worse results than a high-carbohydrate, low-fat type ofnutrition (*65-72). As a rule acute hepatitis almost always subsides, atleast for a time, so that it is not easy to judge the advantages and
disadvantages of a particular type of diet, the more so since drasticnutritional measures are not considered necessary in routine cases. If itwere to be borne in mind, however, that chronic hepatitis often developsfrom an incompletely healed acute condition, perhaps more importancewould be attached to the treatment of the latter.
In the chronic stage, which has a poor prognosis due to its tendency todevelop into cirrhosis and for which all measures so far tried, particularlyall types of medication, have proved to be fairly ineffective, dietarytherapy seems to warrant closer attention.
Fat is not Harmful
The question as to whether a low-carbohydrate, high-fat, high-proteindiet would be more beneficial than the general practice of prescribing alow-fat nutrition has recently been taken up again: at least a fatty liverresponds favourably, and for this reason it has been suggested that theprinciple of treating liver diseases with a low-fat, high-carbohydrate diet
should be discontinued (*69-72).
I have personal access to many patients with pathological liver tests. Thetests in regular use are the so-called GOT (glutamate-oxalate-transaminase), the LAP (leucine-arylamidase), the serum bilirubin (bilepigment in blood) and the electrophoretic separation of the serum into itsindividual fractions (serum electrophoresis).
The GOT which is found in the liver cells and their energy sources, themitochondria, serves as an indicator of the extent of the inflammation ofthe liver cells (hepatitis). The LAP (like alkaline phosphatase) indicatesthe degree of involvement of the bile capillaries, whilst electrophoresis
gives a measure of the individual protein fractions, and above all of thegamma globulins. The proportion of the blood proteins accounted for bythe gamma globulins shows to what degree the organism has so farmobilized immune reactions against its own organs, in this case the liver.We have already encountered these immune reactions on severaloccasions and in view of the size of the organ involved it is not difficultto conceive of their playing a particularly important role in liver diseases.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
33/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Enzyme Reactions Improve
If a patient with a diseased liver is put onto a low-carbohydrate diet notonly does he soon begin to feel better, but the laboratory values also showan improvement. I already have 190 cases in which the GOT has beenconsistently recorded, so that the results are statistically significant (Fig.20). The slighter cases (GOT up to 20 mU) returned to normal within twoweeks, but even in more severe cases a response is generally seen
although this understandably requires longer.
Fig. 20:The behaviour of GOT (ASAT), a parameter indicative of the state of the liver. The speedwith which a normal value is obtained on a low-carbohydrate diet depends upon the initialvalue (A,B,C). Even in severe cases (C) the results are impressive."n" = number of cases investigated at each date.
In 23 of the cases LAP was also determined. These values, too, returnedrapidly to normal, as Fig. 21 shows. Following jaundice the two above-mentioned liver tests often remain positive and, in addition, the bloodfrequently contains elevated quantities of bile pigments. This is a disorderwhich is usually considered to be very resistant and for which so far noeffective mode of treatment has been devised. As can be seen from Figure22 however, a low-carbohydrate diet is successful.
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
34/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scdiet.org/7archives/lutz/lutz7.html [24/1/2013 1:49:49 ]
Fig. 21:The LAP level (leucine-arylamidase) is characteristic of the function of the bile capillariesand the unimpeded flow of bile. Even elevated LAP values rapidly returned to normal on alow-carbohydrate diet.
Chronic hepatitis is the classical example of an auto-aggressive disease.Even if electrophoresis does not indicate that the gamma fraction of theblood proteins Is higher than normal it can be assumed that the failure ofInfectious jaundice to heal, or --- in its absence --- the development of achronic inflammatory process in the liver, is due to the production ofantibodies by the organism to its own liver. Just as has been observed indiseases of other organs, particularly the heart, thyroid andgastrointestinal tract, the body reacts to one of its own parts as if theywere foreign and tries to reject it. A similar situation is encountered inheart transplants. Defence reactions of this kind are being attributed an
7/29/2019 Dr. Med. Wolfgang Lutz_ Dismantling a Myth_ Chapter VII
35/42
med. Wolfgang Lutz: Dismantling a Myth: Chapter VII
//www.scd