Embed Size (px)
Citation preview

IN THE NAME OF GOD

CBC-STUDENTDr Goudarzipour

MCV:HCT/RBC,fl MCH:Hb/RBC,pg MCHC:HCT/Hb,gd RDW:anisocytosis




Neutropenia?
Anemia?
Physiologic anemia?

NL PLT? WHATS MPV?





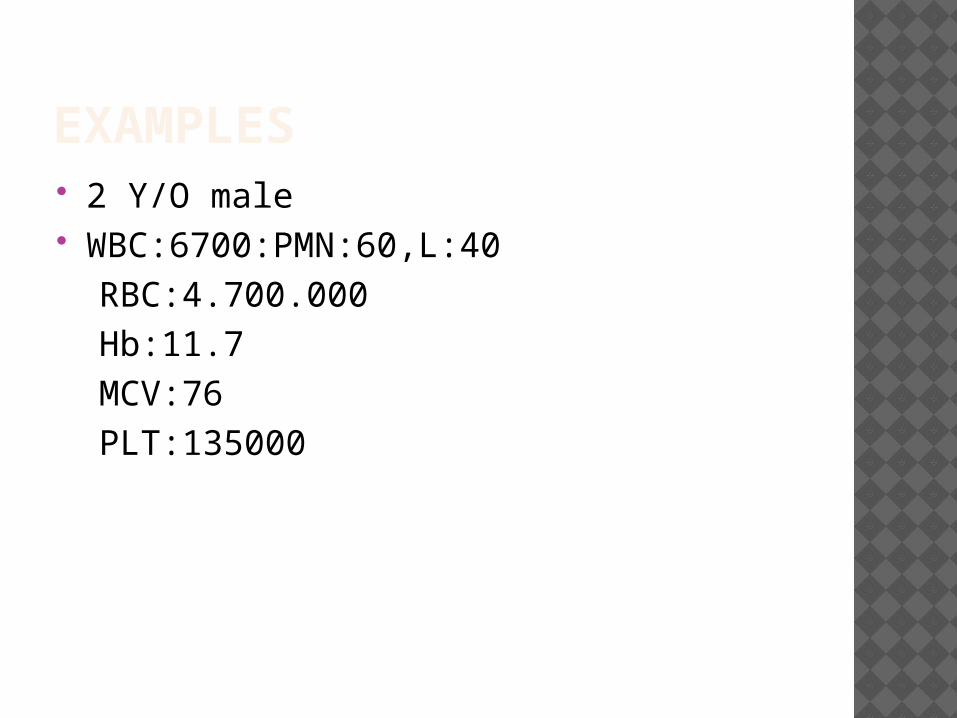
EXAMPLES 2 Y/O male WBC:6700:PMN:60,L:40 RBC:4.700.000 Hb:11.7 MCV:76 PLT:135000

CASE -2 3 month years ,female WBC:6500,L:30,P:70 Hb:8.7 MCV:90PLT:400.000

CASE-3 7 y/o,female WBC:5390,P:63,L:37 RBC:5.900.000 Hb:10.5 MCV:64 MCH:23 PLT:433.000

CASE 4 2 y/o male WBC:14500,P;78,l;22 RBC:5400 Hb;8 HCT:13 MCV:99 MCH:32 MCHC:36 PLT:78000

IRON DEFICIENCY
ANEMIA

BACK GROUND
Iron deficiency is the most common nutritional deficiency in children and is worldwide in distribuiotion.
The incidence of iron-deficiency anemia is high in infancy.
40–50% of children under 5 years of age in developing countries.

Babies are born with iron stored in their bodies. Because they grow rapidly, infants and children need to absorb an average of 1 mg of iron per day.
Since children only absorb about 10% of the iron they eat, most children need to receive 8-10 mg of iron per day. Breastfed babies need less, because iron is absorbed 3 times better when it is in breast milk

IMPORTANCE OF IRON


TISSUE EFFECTS OF IRON DEFICIENCY
I. Gastrointestinal tract Anorexia-common and an early
symptom Pica-pagophagia (ice) geophagia Atrophic glossitis II. Central nervous system Irritability Fatigue and decreased activity

TISSUE EFFECTS OF IRON DEFICIENCY III. Cardiovascular system Cardiac hypertrophy IV. Musculoskeletal system Deficiency of myoglobin and
cytochrome C Adverse effect on fracture healing V. Immunologic system Evidence of increased propensity for
infection

TRANSPORT OF IRON

ABSORBTION OF IRON


PREVALENCE
Peak prevalence occurs during late infancy and early childhood
• Rapid growth with exhaustion of gestational iron
• Low levels of dietary iron • Complicating effect of cow’s milk-
induced exudative enteropathy

PREVALENCE
A second peak is seen during adolescence due to rapid growth and suboptimal iron intake.
This is amplified in females due to menstrual blood loss

CAUSES OF IRON-DEFICIENCY ANEMIA
I. Deficient intake Dietary (milk, 0.75 mg iron/l) II. Inadequate absorption Poor bioavailability: absorption of heme
Fe.Fe2.Fe3; breast milk iron.cow’s milk Antacid therapy or high gastric pH
(gastric acid assists in increasing solubility of inorganic iron)
Cobalt, lead ingestion

CAUSES OF IRON-DEFICIENCY ANEMIA
III. Increased demand Growth pregnancy IV. Blood loss


The best sources of iron include: Baby formula with iron Breast milk (the iron is very easily used
by the child) Infant cereals and other iron-fortified
cereals Liver

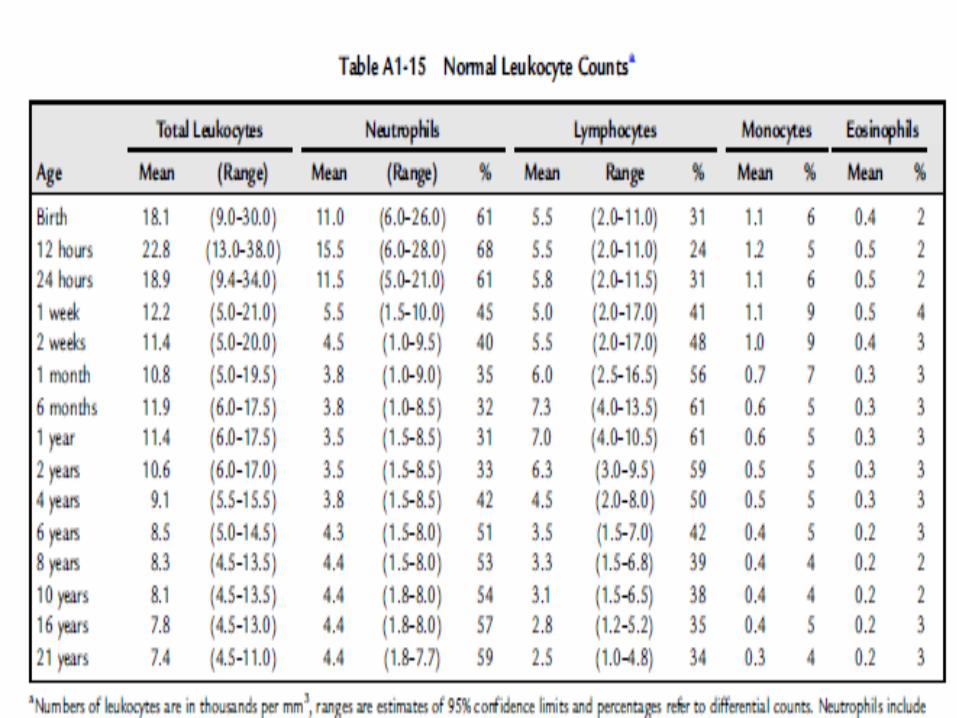
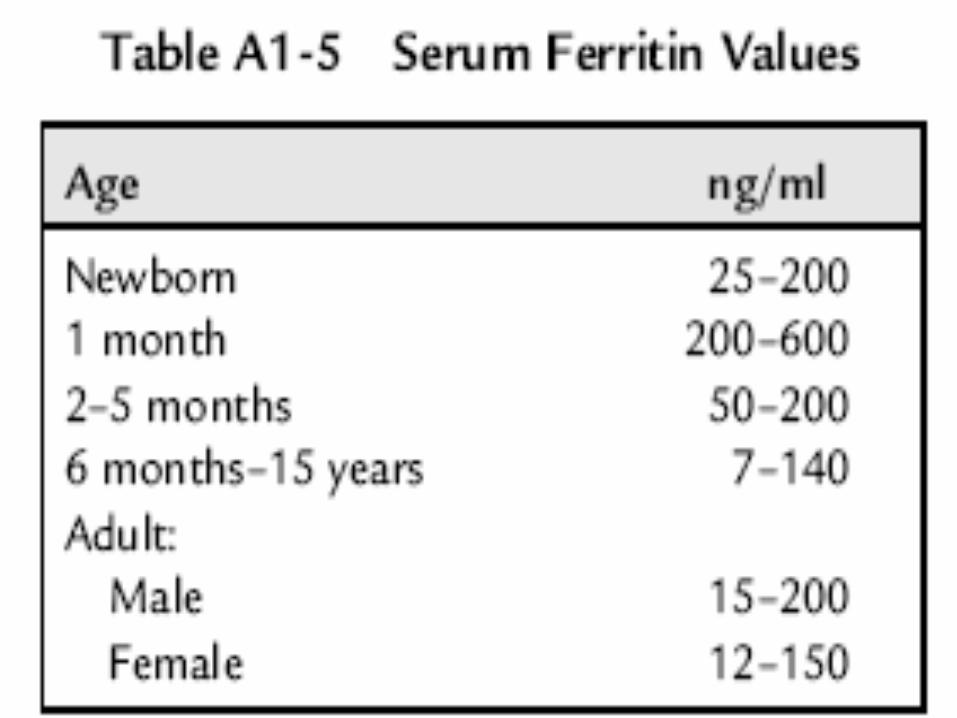
NORMAL LEVEL OF IRON,
FERRITIN ,MCV AND HB




SYMPTOMS Blue-tinged or very pale whites of eyes Blood in the stools Brittle nails Decreased appetite (especially in children) Fatigue Headache Irritability Pale skin color (pallor) Shortness of breath Sore tongue Unusual food cravings (called pica) Weakness Note: There may be no symptoms if anemia is mild.

P/E AND LAB 1. Hemoglobin: Hemoglobin is below the
acceptable level for age 2. Red cell indices: Lower than normal
MCV, MCH and MCHC for age. 3.Increase RDWBlood smear: Red cells are hypochromic
and microcytic with anisocytosis
hemoglobin level falls below 10 g/dl.

P/E AND LAB Basophilic stippling can also be present
but not as frequently The RDW is high (.14.5%) Reticulocyte count: The reticulocyte
count is usually increase in bleeding).)normal
Platelet count: The platelet count varies from thrombocytopenia to thrombocytosis.
free erythrocyte protoporphyrin (FEP) levels. increase

P/E AND LAB The normal FEP level is 15.56 +-8.3
mg/dl. The upper limit of normal is 40 mg/dl
Serum ferritin: The level of serum ferritin reflects the level of body iron stores (below than 12).
Normal ferritin levels, however, can exist in iron deficiency when bacterial or parasitic infection, malignancy or chronic inflammatory conditions co-exist .because ferritin is an acute-phase reactant

P/E AND LAB Serum iron and iron saturation
percentage: limitations: • Wide normal variations (age, sex,
laboratory methodology) • Time consuming • Subject to error from iron ingestion • Diurnal variation • Falls in mild or transient infection.

STAGES OF IRON DEPLETION
1. Iron depletion:tissue stores are decreased without a change in hematocrit or serum iron level2. Iron-deficient erythropoiesisIron decrease reticuloendothelial macrophage
TIBC increase With out change in HCT3. Iron-deficiency anemia: Anemia Increase RDW Increase FEP

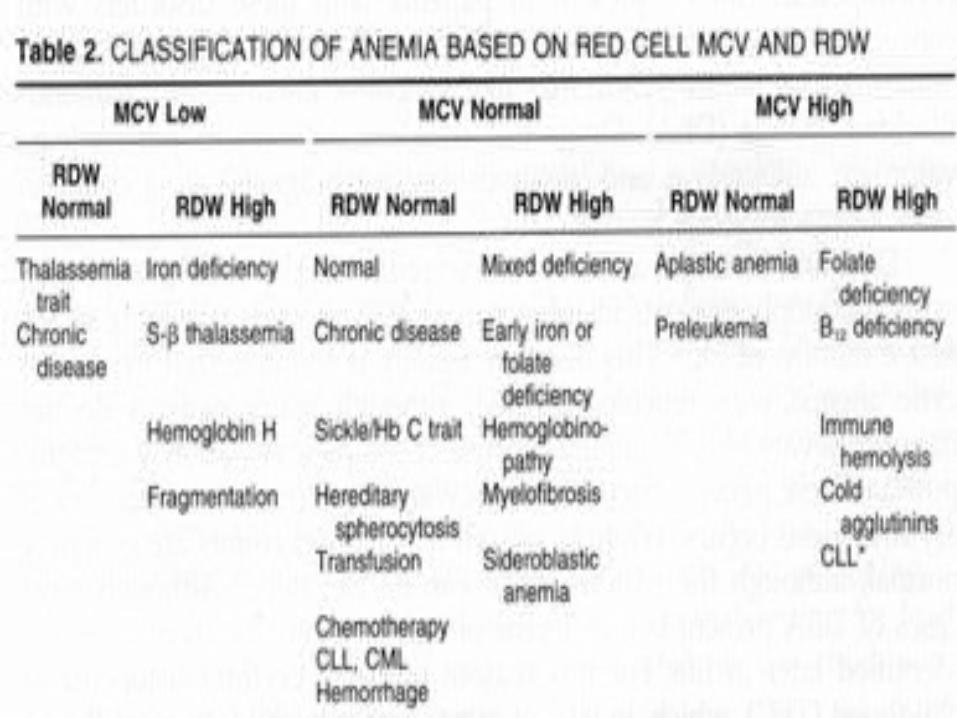
DIFFERENTIAL DIAGNOSIS

DIFFERENTIAL DIAGNOSIS

TREATMENT
Oral Iron Medication Dose: 1.5–2.0 mg/kg elemental iron
three times daily. In children with gastrointestinal side
effects, iron once every other day Duration: 6–8 weeks after hemoglobin
level and the red cell indices return to normal.

RESPONSE:
Peak reticulocyte count on days 5–10 following initiation of iron therapy.
Following peak reticulocyte level, hemoglobin rises on average by 0.25–0.4 g/dl/
hematocrit rises 1%/day during first 7–10 days.
Thereafter, hemoglobin rises slower: 0.1–0.15 g/dl/day.
FAILURE TO RESPOND TO ORAL IRON:
Poor compliance – failure or irregular administration of oral iron;
Inadequate iron dose Ineffective iron preparation Insufficient duration Persistent or unrecognized blood loss Incorrect diagnosis – thalassemia,
sideroblastic anemia Coexistent disease that interferes with
absorption or utilization of iron Impaired gastrointestinal absorption due
to high gastric pH

PARENTERAL THERAPY
Noncompliance or poor tolerance of oral iron.
Severe bowel disease (e.g., inflammatory bowel disease)
Chronic hemorrhage Rapid replacement of iron stores is
needed. Erythropoietin therapy is necessary, e.g.
renal dialysis.

BLOOD TRANSFUSION
In children with sever infection specially with cardiac dysfunction or Hb less than 4 g/dl.






References Glader B. Iron-deficiency anemia. In:
Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia, Pa: Saunders Elsevier; 2007: chap 455.
Heird WC. The feeding of infants and children. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th Ed. Philadelphia, Pa: Saunders Elsevier; 2007: chap 42.
O'Connor NR. Infant formula. Am Fam Physician. 2009;79:565-570.
THE END

THANK YOU
















![FIS for the RBC/RBC Handover...4.2.1.1 The RBC/RBC communication shall be established according to the rules of the underlying RBC-RBC Safe Communication Interface [Subset-098]. Further](https://img.dokumen.tips/doc/110x75/5e331307d520b57b5677b3fa/fis-for-the-rbcrbc-handover-4211-the-rbcrbc-communication-shall-be-established.jpg)












