Embed Size (px)
Citation preview

The how’s and why’s of asafe and effective alternative
to surgery.
JANUARY 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 117
gion. This solution, usually a 4%dilution of pure ethanol, may beused to reduce or eliminate painfulnerve lesions such as inter-metatarsal neuromas, traumaticstump neuromas, nerve entrap-
ments and painful scars. The solu-tion may also be used to treatpainful keratotic lesions on thefoot, such as porokeratosis plan-taris discreta, punctate keratotes,
By Gary L. Dockery, D.P.M.
Continued on page 118
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $17.50 per topic) or 2) per year, for the special introductory rate of $109 (yousave $66). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 128. Other than those entities cur-rently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable byany state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensurethe widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscriptsby noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podia-try Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 128).—Editor
ObjectivesAfter reading this paper
the reader should:
1) have a greater under-standing of the commonfoot condition of inter-metatarsal neuroma.
2) have an increasedability to make a differen-tial diagnosis of the footneuroma condition.
3) be able to describe al-ternative options for treat-ment of the foot neuroma.
4) have a greater under-standing of the conserva-tive treatment of 4% alco-hol injections in the treat-ment of nerve and keratot-ic foot conditions.
Continuing
Medical Education
Dilute solutions of ethyl alco-hol may be used to injectseveral types of lesions
found on the foot and ankle re-
Dilute Alcohol Injections for
Nerve Conditionsand KeratoticLesions of the Foot
C L I N I C A L P O D I A T R YC L I N I C A L P O D I A T R Y

nerve) under the deep transverseintermetatarsal ligament or a me-chanical foot imbalance that re-sults in repetitive trauma andeventually in degenerative neu-ropathy.1 This condition is oftenfound in the third intermetatarsalspace (between the third andfourth metatarsals) and is morefrequent in females than in males.Intermetatarsal neuromas aremore likely found in the exces-sively pronated foot but havebeen reported in both the rectusfoot and cavus foot as well.2 Theauthor has successfully treated in-termetatarsal neuromas with a se-ries of dilute ethyl alcohol injec-
tions and the results havebeen well-received by pa-tients and documented tobe better than other con-servative treatments or sur-gery for neuromas.
Neuroma SymptomsMost patients present
with similar complaints,which range from numb-ness in the digi ta l webspace (usually between thethird and fourth toes) tointense burning pain inthe ball of the foot or intothe toes with activities.When patients are askedto descr ibe these com-plaints they use terms,such as ‘pins and needles’,burning pain, tingling, ora sense of ful lness orcramping in the toes, espe-cial ly with activit ies or
when wearing certain shoes. Ad-ditionally, they may describe thepain as moving from the ball ofthe foot into the toes, or radiat-ing into the arch or up the leg.Walking in dress shoes or run-ning in athletic shoes tends to in-crease the symptoms and removalof the shoes or rest tends to de-crease the symptoms being exhib-ited during activities. Many pa-tients report that when they re-move their shoes and massagethe ball of the foot and toes, itprovides immediate relief of thesymptoms. However, in more ad-vanced conditions, taking theshoes off and walking barefoot onhard surfaces may be very un-comfortable.
DiagnosisThe diagnosis of inter-
metatarsal neuroma is made by avariety of different techniques;however, the clinical history andphysical examination of the fore-foot is the most reliable method
Continued on page 119
118 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2004
Dilute...
hemoma dura, helomamolle’, pinch calluses and other
hyperkeratotic lesions. In thisCME article the recommendedtechnique and uses of these injec-tions are outlined.
Nerve ConditionsIntermetatarsal neuroma (also
called interdigital neuroma, Mor-ton’s neuroma and Morton’smetatarsalgia) is a very commoncondition that is considered bymany to be caused by either anentrapment of the intermetatarsalnerve (the plantar proper digital
Contin
uing
Medica
l Edu
catio
n
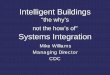
Direct examinationusually locates
the point of maximum tenderness
(PMT).
Figure 3: Direct Pressure Test for inter-metatarsal neuroma.Figure 2: Lateral Squeeze Test for intermetatarsal neuroma.
Figure 1: Pinch Test for intermetatarsal neuroma.

JANUARY 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 119
tion); weight bearing x-rays of theinvolved forefoot area; computedaxial tomography scan (CAT); mag-netic resonance imaging (MRI); ul-trasonographic imaging (USI); orsensory nerve conduction testing.These diagnostic studies are notwell standardized or popular be-cause of increased costs, unreliabili-ty of studies due to operator sensi-tivities, or lack of availability of theequipment. The clinical examina-tion and review of the patient’s his-tory of symptoms are still the mostcommon methods for diagnosis ofintermetatarsal neuroma.
Differential DiagnosisIntermetatarsal neuroma may
be mimicked by several differentclinical findings including any con-dition that causes forefoot pain,numbness, nerve-like pain,metatarsalgia symptoms or discom-fort into the toes. Specific condi-tions in the differential can befound in Table 1. Most of the con-ditions listed in the differential di-agnosis can be confirmed by carefulhistory and physical examination,as well as with the more sophisti-
cated diagnosticstudies mentionedpreviously.
TreatmentOptions
There are nu-merous treatmentoptions availablefor intermetatarsalneuroma rangingfrom leaving italone with no treat-ment to conserva-tive methods oftreatment or surgi-cal care. The conser-vative alternativesinclude tape-strap-ping of the foot toprovide additionalsupport, applicationof intermetatarsalpads to help sepa-rate the metatarsalheads on weightbearing, and the useof functional or-thotic devices tohelp stabilize thefoot. Most of theseapproaches are less
of making the diagnosis. Directexamination usually locates thepoint of maximum tenderness(PMT) by reproducing the symp-toms during a pinch test involv-ing dorsal and plantar compres-sion of the intermetatarsal space(Figure 1) or with the lateralsqueeze test using medial and lat-eral compression of the forefootarea (Figure 2). Also, direct pres-sure placed at the plantar distalintermetatarsal space may repro-duce the patient’s symptoms andidentify increased thickness or anerve enlargement (Figure 3). Acombination of the physical ex-aminations of the lateral squeezetest and the pinch test may repro-duce an audible and/or palpablecl ick in the involved inter-metatarsal space, often referred toas a positive Mulder’s sign.3
Other diagnostic techniquesmay be used to identify inter-metatarsal neuromas, such as theanesthetic nerve block injectionperformed proximal to the suspect-ed neuroma site (diagnostic injec-
Dilute... than successful in thelong-term correction of theproblem. Other conservativetreatments involve the injectionof vitamin B12,4 corticosteroid in-jections,5 and dilute alcohol injec-tions.6,7
Surgical options include a num-ber of different approaches includ-ing the most obvious, surgical exci-sion of the involved nerve. Othervariations consist of transection ofthe intermetatarsal ligament withor without neurectomy, external orinternal neurolysis, with transloca-tion of the involved nerve, endo-scopic decompression or other de-
structive measures, such as laser ab-lation or cryogenic denervation.8-12
All of the surgical techniqueshave the potential for failures andcomplications. The major problemsfollowing the surgical treatmentsinclude return of the condition,worsening of the pain, creation oftraumatic or stump neuromas, ex-cessive deep or superficial scar for-mation, damage to adjacent soft-tissue structures, wound dehiscenceand infection. Less serious compli-cations include numbness in thetoes or ball of the foot area, a feel-ing of fullness or swelling, and per-sistent paresthesias.
Chemical Neurolysis ofIntermetatarsal Neuroma
In an unpublished study per-formed from 1977 through 1985,over 150 patients were evaluatedwho underwent weekly injectionsof 0.5-mL of the 4% alcohol solu-tion for clinical symptoms of inter-metatarsal neuromas. The resultsshowed that over 80% received res-olution of their neuroma symp-toms after three or more weekly in-
Continued on page 120
Continuing
Medical Education
All of the surgical techniques have the potential
for failures andcomplications.
TABLE 1Differential Diagnosis of Intermetatarsal Neuroma
in the Foot
Bursitis
Distal Neuropathy
Flexor Tendinopathy
Freiberg's Disease
Metatarsal Bone Tumors
Metatarsal Plantar Plate Rupture
Metatarsal Stress Fractures
Peripheral Neuritis
Plantar Capsulitis
Rheumatoid Arthritis
Rheumatoid Nodules
Soft-tissue Tumors
Synovitis
Tarsal Tunnel Syndrome

formed a detailed prospective studyto evaluate the treatment results ofa conservative technique involvingthe chemical neurolysis of isolatedintermetatarsal space neuromasusing a dilute 4% alcohol solution.The patients chosen for the studyhad clinical symptoms of a singleintermetatarsal space neuroma on
one foot only. None of the patientshad undergone previous therapyfor their neuromas and all agreed torefrain from receiving additional al-ternative treatments while in thestudy program. The patients all hada minimum of three to a maximumof seven weekly injections com-posed of 0.5-mL of the 4% ethyl al-cohol solution placed proximal tothe point of maximal tenderness.The results of this 10-year study in-volving 100 patients showed that
82 patients reported complete reso-lution of their symptoms followingtreatment and another 7 patientsreported 60-85% improvement. Theresults of this study were publishedin the Journal of Foot and AnkleSurgery in 1999.7 Overall, the long-term results of this prospectivestudy of injection therapy for inter-metatarsal neuromas appear to besuperior to most reported forms oftreatment, including cortisone in-jections and surgical care.
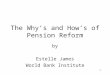
The 4% Dilute Alcohol MixtureThe 4% alcohol solution used
for chemical neurolysis in thisstudy and in all subsequent treat-ments of intermetatarsal neuromas,nerve entrapments, stump neuro-mas and all keratotic lesions wasprepared by mixing 48-ml of 0.5%bupivacaine HCl (Marcaine™) withepinephrine (1:200,000) with 2-ml(two 1-ml vials) of dehydrated ethylalcohol for injection, USP, for anew total volume of 50-mL (Figure4). The use of epinephrine appearsto aid in the results of neuroma in-jections perhaps due to the factthat it potentiates the local anes-thetic agent, confines the sclerosingsolution to a smaller area, preventsthe rapid absorption of the solutioninto the adjacent tissues, and mayhave some neurolytic action on thenerve tissue itself.
The new mixture is kept in theoriginal bupivacaine bottle and re-
labeled to identifythe solution as 4%sclerosing, ratherthan local anesthet-ic, to prevent inad-vertent misuse (Fig-ure 5). The mixturedate should also beincluded on the newlabel and I recom-mend replacing thesolution after 6months even thoughthe solution is proba-bly stable for alonger period oftime. I also make abottle of the 4% so-lution using bupiva-caine HCl withoutepinephrine for usein those patients thathave untoward reac-
Continued on page 121
120 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2004
Dilute...
jections. The compilation ofdata and format of tracking ad-
ditional therapeutic measures inthis study was faulty and therewere so many variables and othertreatments provided that the re-sults were not publishable. Manypatients had multiple interspacecomplaints, had undergone previ-ous cortisone injections, werewearing functional orthotic devicesor had received some other formsof treatment before or during thestudy time. In 1986, the techniquefor mixing the 4% solution and thedifferent clinical conditions re-sponsive to sclerosing alcohol in-jections was published.6 The mix-ture was initially composed of 48-mL of 2% lidocaine withepinephrine (1:100,000) and 2-mLof dehydrated ethyl alcohol, whichresulted in a 4% dilute solution.13
However, I began to note thatusing 0.5% bupivacaine HCl withepinephrine (1:200,000) combinedwith the dehydrated ethyl alcoholprovided more consistent resultsand longer-lasting anesthesia afterinjection. Based upon this experi-ence, this became the mixture ofchoice for all additional futuretreatments. Further studies werethen developed to help controlmost of the problems and variablesnoted in the earlier study design.
From 1986 through 1996, I per-
Contin
uing
Medica
l Edu
catio
n
The use of corticosteroid in the
mixture is notrecommended since it has an
anti-inflammatoryresponse.
Figure 5: Placing a new label on the4% alcohol to clearly identify it.
Figure 4: Mixture of two 1 ml. vials of dehydrated ethylalcohol and 48 ml. of local anesthetic agent.

JANUARY 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 121
It is not necessary to try to enterthe nerve itself, but to be as close toit as possible. It is thought that thenerve in this proximal area is small-er, without surrounding perineuralfibrosis or adjacent thickened tis-sues, making it easier to destroy atthis level with the chemical solu-tion than it would at the actualneuroma or en-trapment site.Furthermore, it isnot necessary norrecommended toperform a localanesthetic nerveblock prior to theinjection of the4% ethyl alcoholsolution, sincethis will causeanesthesia to thearea, making itvery difficult tolocate the involved nerve and couldpotentially dilute the 4% alcoholsolution even further. Also, the useof corticosteroid in the mixture isnot recommended since it has ananti-inflammatory response andwill decrease the neurolysis effect ofthe alcohol solution, thereby de-
creasing its effect onthe nerve tissue.
Results of OriginalStudy
The results of the10-year prospectivestudy showed that, in100 patients, therewere 73 females and 27males ranging from 20to 75 years of age (av-erage 51 years). Therewere 62 left feet and 38right feet involved.Fifty percent of the pa-tients had 6 or 7 injec-tions. The third inter-metatarsal space wasinvolved in 81 cases.Follow-up evaluationwas performed for eachpatient from 6 monthsto 2 years (average of13 months) followingcompletion of treat-ment. As was statedpreviously, the final re-sults showed that 82patients reported 100%improvement of their
tions to the epinephrine.The protocol involves the injec-
tion of 0.5-mL of the 4% ethyl alco-hol solution proximal to the pointof maximum tenderness at the in-volved intermetatarsal space. Un-like cortisone, I typically give theinjection of 4% alcohol about 1/2-inch proximal to the tender area.The injection is given from the dor-sal aspect of the foot with a 1 1/4-inch, 27-gauge needle penetratingdeep into the intermetatarsal spacebelow and proximal to the inter-metatarsal ligament and neuroma(Figure 6). The needle is then gen-tly and slowly moved around in thedeep tissue layers until the patientresponds with a sensation of tin-gling, pins and needles, radiatingpain into the toes, or burning intothe ball of the foot. This would in-dicate a relatively close proximityto the nerve and once the sensationis felt by the patient, then the in-jection is performed. This is donein an attempt to get the 4% dilutedethyl alcohol solution close to thenerve tissue, but proximal to theactual neuroma.
Dilute... symptoms and 7 pa-tients reported from 60-85% improvement, giving anoverall success rate of 89%.Eleven patients had continuedpain or other symptoms at the endof the study and elected to proceedwith surgical neurectomy. It wasinteresting to note the appearance
of the tissuesaround the neu-roma in theeleven patientsthat failed the in-jection treat-ment. In sevenpatients the tis-sues around theneuroma were at-rophic and thinin appearance,even though theneuromas wereenlarged and dis-
tinct. It gave the impression thatadditional injections of the alcoholsolution may have eventually suc-ceeded in destroying the proximalnerve. The other four patients hadwhat appeared to be coagulationand melting of the adjacent adi-pose tissues and the neuromaswere more difficult to remove dis-cretely. The surgeries were all suc-cessful with no major complica-tions or delayed healing noted.
Complications of AlcoholInjections
The complications with this 4%alcohol injection technique appearto be minimal and include failureto relieve the original symptoms,recurrence of symptoms, increasedsymptoms after the first, and possi-bly the second, injection (postinjec-tion neuritis), and, finally, a postin-jection lymphatic reaction has beenreported. The failure to work andrecurrence of symptoms is not trulya complication, but something thathappens with most forms of treat-ment. The increase in symptomsfollowing the first or second injec-tions appears to be relatively com-mon and occurs in the first 48hours after the injection and thenthe intensity decreases rapidly. Bythe subsequent clinical visit all pa-tients reported that the ‘new’ painhad decreased significantly andwere now absent in most patients.
Continued on page 122
Continuing
Medical Education
The solution should be mixed
by the physician’s office to maintain
quality control and consistency.
Figure 6: Placement of the injection proximal to thepoint of maximum tenderness.

cohol solution was picked up by thedorsal superficial lymphatic systemand the irritation is subsequentlyseen soon after the injection. Deepinjections of the solution do not ap-pear to have this secondary effectand therefore, one can avoid thiscomplication by being certain not toinject the solution until the needle isdeep within the tissues and to refrainfrom performing additional injectionwhile withdrawing the needlethrough the superficial tissues. Thisreaction is probably very similar tothe condition reported by Kravettewith cortisone injections, termedperi-lymphatic atrophy.14
DiscussionThe primary component of the
4% sclerosing solution discussed inthis article isdehydratedalcohol injec-tion, USP,which is alsotermed abso-lute alcohol,pure ethyl al-cohol for in-jection, desic-cated alcohol,and ethanol.Dehydratedalcohol con-sists of notless than 98%by volume ofethyl alcohol(ethanol) andis distributedin sterile 1
ml, glass vials, ready for injection.Ethyl alcohol is a clear, colorless liq-uid that is miscible with local anes-thetic agents. Once the ethanol is di-luted to 4% by the method describedearlier, it produces neuritis and Wal-lerian nerve degeneration or chemi-cal neurolysis when absorbed intonerve tissue. Repeated injections ofthis dilute solution in close proximityto nerve tissue, on a weekly basis,presumably causes selective degener-ation or neurolysis until the nervecompletely ceases nerve function oris directly destroyed. The volumeneeded to produce therapeutic neu-rolysis involves amounts too small toproduce systemic side-effects relatedto ethanol.15,16
The dehydrated alcohol may beordered from the local pharmacistand is also available from a varietyof medical supply companies, in-cluding Moore Medical and Surgi-cal Supply Service. Dehydrated al-cohol is usually purchased in 1-mlglass vials in quantities of 10 vialsper box. My recommendation isthat the materials be ordered andthe solution mixed by the physi-cian’s office to maintain qualitycontrol and consistency.
Other Nerve ConditionsThe treatment of other nerve
conditions is performed in a similarfashion as described for the inter-metatarsal neuroma17. When thereis nerve damage, nerve entrapment,or painful scars, it is necessary tofind the point of maximum tender-
Continued on page 123
122 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2004
Dilute...
Very few patients had similarincreased pain after the third or
subsequent injections due to theincreasing neurolysis effect andsubsequent numbness of the previ-ous injections.
I have never actually seen theperi-lymphatic irritation in the past25 years of doing this injection;however, a few podiatric physicianshave contacted me in the past sever-al years to report having seen it fol-lowing the injection of the 4% alco-hol solution. They report that thesymptoms include increased pain,intense redness with streaking fromthe injection point proximally upthe foot and blistering in a few cases.It is my opinion that the 4% ethyl al-
Contin
uing
Medica
l Edu
catio
n
Figure 9: Injection for medial calcaneal heel nerve pain.Figure 8: Painful scar nerve entrapment may be in-jected with a 4% alcohol solution.
Figure 7: Injection of the painful medial pinch callus digital nerve.

JANUARY 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 123
mas, especially on the toes.19
Several unrelated keratotic-likelesions have similar appearances tocorns and calluses and these condi-tions include arsenical keratosis, ec-crine poroma, keratodermas, plan-tar verrucae, and porokeratosisplantaris discreta.
Diffuse hyperkeratotic tissue isgenerally found on the weight-bear-ing surface of the sole of the footand is usually asymptomatic. Thisdiffuse type is seen more often inpatients who regularly go barefootand in patients who have a form ofposterior equinus. The more dis-crete types of hyperkeratosis are fre-quently painful and are often foundon the ball of the foot. Close evalu-ation of these lesions may show acentral conical core of keratin at thepoint of greatest pressure.20
Discrete isolated lesions may
also be similar to cutaneous horns,but unlike skin horns, careful de-bridement of hyperkeratotic lesionwill lift the superficial keratin plugoff completely, leaving visible skinlines underneath. Other distinctareas of pressure hyperkeratosis for-mation may be seen under individ-ual metatarsal heads. These lesionsare frequently resistant to regularconservative care of debridementand protective padding. These le-sions may be seen under any or allof the lesser metatarsal heads andare referred to as intractable plantarkeratoses (IPK’s).21
Other lesions that may be visi-bly similar to corns and callusesshould be identified to obtain themost beneficial results from treat-ment. These conditions include:
Arsenical KeratosesThese are discrete hyperkeratot-
ic lesions found on the soles of the
ness by clinical examination. Oncethe area has been identified, thenthe injections of 0.5-ml of the 4%alcohol solution may be injectedproximal to the maximum point oftenderness on a weekly basis untilthe symptoms resolve. It has beenmy experience that a minimum ofthree injections is necessary to as-sess the improvement of the condi-tion. If the condition is not re-sponding after the third injection,the treatment is discontinued. If,however, there has been an im-provement, the injections are con-tinued for the full treatment ofseven injections.18
Painful nerve entrapment at themedial pinch callus of the halluxcan successfully be treated with aseries of the 4% alcohol injections(Figure 7). Painful scars with dermalnerve entrapments may be injectedin a similar fashion (Figure 8).Moreover, many patients that com-plain of heel pain may have symp-toms secondary to entrapment ofthe medial calcaneal nerve branchrather than true medial plantarfasciitis symptoms. If I can repro-duce their heel or arch pain by pal-pating along the medial aspect ofthe heel, rather than at the plantarcalcaneal tubercle, then I will per-form a series of injections proximalto the point of maximum tender-ness on the medial heel (Figure 9).
Painful Keratotic LesionsThere are a number of keratotic
and painful lesions that form onthe weight bearing and pressureareas of the foot. Many of theseconditions are difficult to treat andoften do not respond to simple de-bridement and padding. Abnormal-ities in keratinization may repre-sent thickenings referred to ascorns, calluses, helomas, hyperker-atoses, or tylomas.
In general, hyperkeratosis indi-cates an increased keratinocyte ac-tivity in which the hyperkeratosis isdue to stimulation of the epidermisby intermittent or increased pres-sure. Hyperkeratoses that are dif-fuse and generalized are usually re-ferred to as calluses or tylomas. Ifthe hyperkeratoses are more dis-tinct and isolated, they are com-monly referred to as corns or helo-
Dilute... feet and palms of thehands secondary to arsenicexposure. These lesions maymimic discrete intractable plan-tar keratoses, seed corns (helomamilliare) or plantar verrucae. Thiscondition is usually very difficult totreat but many will respond com-pletely to injections of 4% alcoholsolution.
Eccrine PoromasSlow-growing, painless, superfi-
cial, smooth-surfaced, and partiallyflattened, these lesions may resem-ble pyogenic granulomas, der-matofibromas, or foreign-bodygranulomas. Eccrine poromas mayappear rubbery to firm and canreach 3 cm. in diameter. Eccrineporomas are commonly found inwomen during the fourth decadeand typically are found on the heelor ball of the foot.
KeratodermasThese are localized forms of ker-
atodermas may be similar to dif-fuse, generalized or isolated formsof hyperkeratosis. Most types ofkeratodermas are inherited as auto-somal dominant traits and mayalso be associated with systemicmanifestations. Diffuse hyperker-atosis of the plantar skin may be-come so thick that it tends to formcracks or fissures and may becomevery painful for the patient to walkon. The punctate form of palmo-plantar keratoderma looks very sim-ilar to arsenical keratoses with theexception that a central translucentcenter is commonly present in eachlesion. These keratodermatous con-ditions are all persistent and diffi-cult to treat.
Porokeratosis Plantaris DiscretaThis lesion is represented by
small (1- to 3-mm diameter) punc-tate lesions usually found on theweight-bearing aspect of the ballof the foot. The porokeratosis isprobably developed by direct pres-sure on the plantar surface of theskin but is not usually associatedwith an underlying bony condi-tion. There is still some debate asto whether the underlying ductsof sweat glands are involved.These distinct lesions appear aswhite or yellow-white lesions that
Continued on page 124
Continuing
Medical Education
After several injections the nerve will stop sending
pain signals to the central
nervous system.

ception of pain from theneedle penetrating throughthe skin.
Additionally, some plan-tar foot lesions may actuallybe injected from a dorsalapproach if a long needlepassing between themetatarsals can be placed atthe level of the lesion. Inmany cases, the patients re-port that this is somewhatless painful than injectingdirectly into the plantar le-sion from below.
Painful bursae, with orwithout overlying callusformation, and other cysticlesions may be injectedwith 0.25 to 0.5 ml. of 4%alcohol sclerosing solution,depending upon its size(Figure 9). This may be repeated upto seven times at weekly intervals.The sac or bursal cyst tends toshrink in the following weeks, witha dramatic decrease in painfulsymptoms and callus formationwhich may last as long as one yearand in many instances never recur.
Plantar fibromas are injectedwith 0.5 ml. to 1.0 ml.of 4% alcohol scleros-ing solution directlyinto the central portionof the mass. Subsequentinjections may be infil-trated throughout themass and the injectionis followed by a 5-to 10-minute ultrasoundtreatment. This is re-peated weekly for up toseven visits and addi-tional softening andshrinking of the fibro-ma may be expected tobe seen for severalmonths after the finalinjections. In almost allcases, the pain of the le-sion will resolve com-pletely.
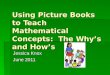
Painful porokerato-sis plantaris discretaand other punctate ordeeply nucleated plan-tar lesions respond ex-tremely well to 4% al-cohol sclerosing injec-tions.22-25 A total of 0.25ml. to 1.0-ml., depend-ing upon the size of the
lesion, of 4% sclerosing solution isinjected at a 45-degree angle tothe lesion with a 5/8 inch, 25-gauge needle, using a 1 ml. tuber-culin syringe (Figure 10). This in-jection procedure is repeated atweekly intervals for up to seveninjections. Larger punctate lesionswill also respond to a similar in-jection process of weekly intervals(Figure 11). Usually there is dra-matic change by the third injec-tion and, if the lesion has re-sponded, no further treatment isperformed. If, however, after threeinjections there has been poor orno response, the program is termi-nated and alternative treatmentsare recommended. The weekly in-tervals seem to be relatively im-portant and longer intervals be-tween injections may delay theend-results.
Once the local anesthesia wearsoff there may be considerable burn-ing or pain at the injection site thatmay last for several hours. This dis-comfort may be reduced by the ap-plication of cool foot soaks or ice tothe area. Analgesics, especially as-pirin, may also help reduce thepain.
The remarkable thing about thistreatment is that not only do thelesions become asymptomatic innature, presumably due to thechemical neurolysis that occurs fol-lowing the alcohol injections, butalso the lesions frequently go away.Over the past 25 years I have seen
Continued on page 125
124 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2004
Dilute...
are most tender with side-to-side pressure.
Injection Therapy for KeratoticLesions
It may be worthwhile to treatcertain keratotic lesions or condi-tions, such as the intractable plan-tar keratosis, porokeratosis, fibro-ma, or keratodermas with intrader-mal or subdermal injections to cre-ate a neurolysis and therefore re-duce the pain associated with theselesions(21). In many cases, the le-sions themselves will resolve fol-lowing a series of three or more 4%alcohol injections. Unlike withneuroma injections, local infiltra-tive nerve block with a local anes-thetic agent may be necessary priorto giving a sublesional injection onthe plantar foot. Because injectionsinto the plantar aspect of the footmay be extremely painful, a poste-rior tibial nerve block may be givenprior to any other injection on thesole area of the foot. The use ofskin coolants, such as ethyl chlo-ride, will greatly decrease the per-
Contin
uing
Medica
l Edu
catio
n
Figure 11: Injection of painful porokeratosis plan-taris discreta. A. Pre-injection. B. After three injec-tions. Note the reduction in size.
Figure 10: Injection of painful bursa with 4% al-cohol solution.

JANUARY 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 125
treatment. And even if this ap-proach is unsuccessful, othertreatments can still be performedat a later date.
There are numerous painfulkeratotic and punctate skin le-
sions on the feet and many ofthese can be treated with changesin shoe styles, local tissue de-bridement, padding and strap-ping, accommodative shoe insertsand surgical intervention. Insome of the cases, the painful le-
sions continue to be aproblem even after ex-tensive treatment.Some patients may notbe good surgical candi-dates, but still need ad-dit ional therapy fortheir painful lesions. Inthese cases, the addi-tion of injection thera-py with a dilute 4% al-cohol solution maygreatly improve or eventotal ly resolve thesepainful conditions.
Coding IssuesThe proper diagnos-
tic codes for nerve con-ditions should be used,which include, but arenot limited to the fol-lowing: neuroma 355.6;neuritis, peripheral355.8; nerve entrapment355.9; amputation neu-roma 997.61; nerve in-jury, skin/sensory 956.4;nerve injury, unspecified956.9; and, pain, lowerextremity 729.5. The
very few recurrences of lesions oncethey have responded to the injec-tion process.
ConclusionsThe use of a dilute 4% ethyl al-
cohol solution for the chemicalneurolysis of intermetatarsal neu-roma provided 89% improvementof symptoms with 82% of all pa-tients reporting total relief of theirnerve-like symptoms after com-pleting a series of weekly injec-tions. The 4% ethyl alcohol solu-tion injection has less reportedside-effects than cortisone injec-tions. A complete series of seven4% ethyl alcohol solution injec-tions has less reported complica-tions than surgery. Most patientsare extremely pleased with thisconservative treatment programand refer other patients with simi-lar problems for the same treat-ment. This would indicate thatthe treatment of neuromas with aconservative injection of dilute4% alcohol is a good alternative toother conservative treatments,cortisone injections, and surgical
Dilute... correct CPT-2004 code is64640: Chemical neurolysisby chemical methods. This isnot prolotherapy or an experi-mental injection technique andshould not be recoded by the insur-ance company for this treatment.Podiatric physicians are qualified toprovide this service and should notallow insurance companies to dic-tate that this procedure only beperformed by anesthesiologists orpain clinics.
Additional Considerations
Why Inject Proximal to theNeuroma?
As explained previously, thenerve tissue that is proximal to theneuroma should be thinner, small-er and more susceptible to chemicalneurolysis than the thicker, fi-brosed or enlarged neuroma itself.Therefore, it should be destroyedmuch faster in this area.
Why Not Use a Much StrongerPercent of Alcohol Instead ofthe 4% Solution?
The ethanol solution of 4% al-cohol has a strong affinity for nervetissue, but is not toxic to the adja-cent tissue unless injected directlyintravascular. Some nerve special-ists inject a pure solution to destroynerves. At a greater concentration,the alcohol may cause damage toboth blood vessels and tendonsheaths and is much more reactivewith muscle tissue. Why increaseyour risks if you can achieve greaterthan 80% improvement with the4% solution with very few, if any,complications?
What About After the 7th In-jection?
If there are still symptoms afterthe 7th injection, but the patienthas had some improvements, I sug-gest that you reschedule the patientfor 2-3 months for a follow-up visit.In many cases, the symptoms willhave totally resolved by the nextvisit indicating that the neurolysisprogressed after completion of thelast injection. If there are stillsymptoms after the delay time thenI suggest another series of 4% ethylalcohol injections, cortisone injec-tions or surgery. The patient and
Continued on page 126
Continuing
Medical Education
Figure 12: Large punctate plantar keratotic lesionsmay respond favorably to 4% alcohol injections. A.Large punctate lesion before injection. B. Appear-ance after several injections.
If the time between injections isprolonged then thenerve can recover
significantly and this will delay the
chemical neurolysisresponse that is being sought.

What If the Insurance Compa-ny Does Not Allow the Billing ofCPT 64640?
My suggestion is to contact themedical advisor of the insurance com-pany and explain that this is a seriesof injections and how the processworks. If there is not a favorable con-sideration following this technique, Isuggest writing a letter of justificationfor treatment and sending copies ofcurrent references on this treatmentprogram to the principle decisionmaker of the company in question. Itmay be necessary to talk to the insur-ance commissioner of your state toobtain assistance in this manner.
How Long Does the SolutionLast Once it is Mixed?
It is my opinion that the mixedalcohol and local anesthetic solutionis viable for a minimum of 6 monthsas long as it is not exposed to directsunlight or air and is kept in themulti-dose vial during usage. I suggestdating the mixture once it is madeand then replacing it after 6 months.
References:1 Wu, K.K. Morton’s interdigital neuroma:
a clinical review of its etiology, treatment, andresults. J. Foot Ankle Surg. 1996; 35: 112-119.
2 Wachter SC, Nilson RZ, Thul JR. The rela-tionship between foot structure and inter-metatarsal neuromas. J Foot Surg.1984; 23:436-439.
3 Mulder JD. The causative mechanism inMorton’s metatarsalgia. J Bone Joint Surg 1951;33(B): 94-95.
4 Steinberg MD. The use of vitamin B-12 inMorton’s neuralgia. J Am Podiatr Assoc.1955;45: 41-42.
5 Bennett GL, Graham CE, Maudlin DM.Morton’s interdigital neuroma: a comprehen-sive treatment protocol. Foot Ankle Int. 1995;16: 760-763.
6 Dockery GL, Nilson RZ. Intralesional in-jections. Clin Podiatr Med Surg.1986; 3: 473-485.
7 Dockery GL. The treatment of inter-metatarsal neuromas with 4% alcohol scleros-ing injections. J Foot Ankle Surg. 1999; 38(6):403-406.
8 Miller SJ. Morton’s neuroma: a syn-drome. In Comprehensive Textbook of FootSurgery. McGlamry ED (editor), 2nd Edition,Chapter 11, Williams & Wilkins, Baltimore.1992; 304-320.
9 Gaynor R, Hake D, Spinner SM, TomczakRI. A comparative analysis of conservative ver-sus surgical treatment of Morton’s neuroma. JAm Podiatr Med Assoc. 1989; 79: 27-30.
10 Barrett SL, Pignetti TT. Endoscopic de-compression for intermetatarsal nerve entrap-ment—the EDIN technique: Preliminary study
with cadaveric specimens; early clinical results. JFoot Ankle Surg. 1994; 33: 503-508.
11 Hodor L, Barkal K, Hatch-Fox LD. Cryo-genic denervation of the intermetatarsal spaceneuroma. J Foot Ankle Surg. 1997; 36: 311-314.
12 Caporusso EF, Fallat LM, Savoy-Moore R.Cryogenic neuroablation for the treatment oflower extremity neuromas.
13 Dockery GL. Podiatric dermatologic ther-apeutics. In Podiatric Dermatology. McCarthyDJ and Montgomery R (editors), Chapter 24,Williams & Wilkins, Baltimore. 1986: 311-335.
14 Kravette M. Perilymphatic atrophy ofskin. An adverse side effect of Intralesionalsteroid injections. Clin Podiatr Med Surg. 1986;3(3): 457-462.
15 Rengachary SS, Watanabe IS, Singer P,Bopp WJ. Effects of glycerol on peripheralnerve: an experimental study. Neurosurgery.1983; 13: 681-688.
16 Package Insert. Dehydrated Alcohol In-jection, USP. American Regent Laboratories,Inc. Subsidiary of Luitpold Pharmaceuticals,Shirley, NY 11967.
17 Dockery GL. Is injection therapy the bestsolution for foot neuromas? Podiatry Today,January 2002, pp 22-25.
18 Dockery GL. Alcohol injection targets in-termetatarsal pain. Biomechanics, April 2002,pp 57-67.
19 Dockery GL, Crawford ME. Color Atlasof Foot & Ankle Dermatology, Philadelphia,Lippincott-Williams and Wilkins, 1999.
20 Dockery GL, Crawford ME: Evaluationand management of keratotic disorders of thefoot. In, Yoho RM, Mandracchia VJ, Mena-jovsky LB (eds): Atlas of Office Procedures: Footand Ankle Disorders, 2000; 3: 1-21.
21 Dockery GL: Mechanical Injuries. In, Cu-taneous Disorders of the Lower Extremity.Philadelphia, WB Saunders Co., 1997, p 236.
22 Dribbon B.S.: The utilization of an alco-hol-local anesthetic solution in the treatmentof the plugged duct cyst. J. Am. Podiatr. Assoc.61: 203-206, 1971.
23 Baruch K: Injection method treatment ofporokeratosis. J. Podiatr. Educ. 3: 1, 1972.
24 Weisfeld, M.: Understanding porokerato-sis plantaris discreta, J Am. Podiatr. Assoc. 63:138-144, 1973.
25 Dockery GL: Evaluation and treatmentof metatarsalgia and keratotic disorders. In, My-erson MS (ed): Foot and Ankle Disorders.Philadelphia, WB Saunders Co., 2000, p 359.
126 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2004
Dilute...
the doctor can now exploreother options that are suitable
for that particular patient.
Why is There Pain After the 1stor 2nd Injections?
The dilute ethanol solution hasa strong affinity for nerve tissue andit is absorbed almost immediately.The alcohol starts to irritate thenerve tissue and the nerve symp-toms may increase at this point dueto the damage that is occurring.Subsequent injections cause addi-tional chemical neurolysis to occurand after several injections thenerve will stop sending pain signalsto the central nervous system.
Why Not Inject a Local Anes-thetic Into the Area Before In-jecting the Alcohol?
The local anesthetic agentwould cause numbness to the areamaking it more difficult to locatethe nerve and therefore make itmore difficult to get into closeproximity to the nerve. The localanesthetic would also potentiallydilute the 4% alcohol solution evenfurther and possibly decrease theneurolysis effects.
Why Not Add Corticosteroid tothe Solution?
The goal of the injections with4% alcohol solution is to cause achemical neurolysis effect on theinvolved nerve. The alcohol solu-tion is irritating to the nerve tissuesand the steroid would, by its na-ture, decrease the desired effect ofthe alcohol and therefore, decreasethe neurolysis. The steroid alsoadds potential side-effects of tissueatrophy, discoloration of the skin,telangiectasia and damage to thesoft tissues not seen with the dilutealcohol solution alone.
Why Is It Important to Injectthe Dilute Alcohol Every 5 to 10Days?
Nerve tissue is relatively dynam-ic and can begin repairing itselfsoon after minor injury occurs. Ifthe time between injections is pro-longed then the nerve can recoversignificantly and this will delay thechemical neurolysis response that isbeing sought.
Contin
uing
Medica
l Edu
catio
n
Dr. Dockery isauthor of Cuta-neous Disor-ders of theLower Extremi-ty, W.B. Saun-ders Co. (1997)and Founderand Director ofScientific Af-fairs of theNorthwest Podiatric Foundation for Ed-ucation & Research, USA, Seattle, WA.

JANUARY 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 127
local anesthetic agentB) 1 ml. alcohol plus 49-mLlocal anesthetic agentC) 4 ml. alcohol plus 46-mLlocal anesthetic agentD) 2 ml. local anestheticagent plus 48-mL alcohol
7) The recommended dosage of4% alcohol per injection is:
A) 2.0 ml.B) 1.0 ml.C) 0.5 ml.D) 0.1 ml.
8) The recommended interval be-tween injections of 4% alcohol is:
A) 1 monthB) 2 weeksC) 1 weekD) 2 days
9) The injection of 4% alcoholfor intermetatarsal neuroma isplaced:
A) distal to the maximumpoint of tendernessB) directly into the maximumpoint of tendernessC) deep to the maximumpoint of tendernessD) proximal to the maximumpoint of tenderness
10) Which of the following is rec-ommended when injecting 4%alcohol:
A) adding corticosteroid tothe solution to reduce thediscomfortB) mixing the solution withphenol to increase tissue re-actionC) injecting as close to the in-volved nerve as possibleD) pre-injecting the area withlocal anesthetic before using4% alcohol
1) Intermetatarsal neuroma for-mation is most likely caused by:
A) repetitive trauma to thenerveB) wearing incorrect sizedshoesC) athletic activitiesD) poor nutrition
2) Foot neuromas are commonlyfound:
A) between the 1st and 2ndmetatarsalsB) between the 2nd and 3rdmetatarsalsC) between the 3rd and 4thmetatarsalsD) between the 4th and 5thmetatarsals
3) The most accurate assessmentof foot neuromas is made by:
A) x-rays of the footB) clinical examination of thefootC) computed axial tomogra-phy of the footD) posterior tibial nerve block
4) Intermetatarsal neuromas ap-pear to be:
A) more common in menB) more common in womenC) equally common in menand womenD) uncommon in men andwomen
5) The alcohol described for neu-rolysis is:
A) isopropanolB) methanolC) ethylene glycolD) ethanol
6) The mixture recommended toobtain a 4% solution is:
A) 2 ml. alcohol plus 48-mL
11) In the prospective study dis-cussed in the article, what per-cent of patients had 100% im-provement of their symptoms:
A) 82%B) 74%C) 50%D) 26%
12) Complications of the 4% al-cohol injections include all of thefollowing except:
A) failure to relieve originalsymptomsB) ulceration formationC) recurrence of nerve symp-tomsD) perilymphatic irritation
13) Other names for pureethanol include all of the follow-ing except:
A) dehydrated alcoholB) desiccated alcoholC) absolute alcoholD) rubbing alcohol
14) Which of the following le-sions is not injected with 4% al-cohol solution:
A) plantar wartsB) porokeratosis plantarisdiscretaC) eccrine poromasD) arsenical keratoses
15) When injecting painful plan-tar fibromas with 4% alcoholwhat additional treatment is rec-ommended:
A) topical cortisoneB) oral anti-inflammatorydrugsC) ultrasound massageD) ice massage
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 129.
Continued on page 128

128 PODIATRY MANAGEMENT • JANUARY 2004
16) After three consecutive injections of 4%alcohol and there has been no response it isrecommended to:
A) continue with four additional weeklyinjectionsB) discontinue treatment and recommendother optionsC) continue treatment with the addition ofcortisoneD) discontinue treatment and do surgery
17) The increased pain after the first or secondinjection of dilute alcohol is due to:
A) the needle touching the nerve tissueB) the flare from the steroid additiveC) the pressure from fluid injectionD) the inflammatory reaction
18) Delaying the intervals between injections of4% alcohol may:
A) allow the nerve to repair itselfB) cause the patient increased discomfortC) damage the nerve too muchD) decrease the treatment time
19) Mulder’s sign is:A) pain with plantarflexion of the toesB) tingling into the toes with tight shoesC) an audible or palpable click between themetatarsalsD) reproducible in all patients
20) Which of the following statements about4% alcohol injections is true:
A) it is the only conservative treatment thatis successfulB) it is the only treatment that has no side-effectsC) it is recommended for all patientsD) it is a good alternative treatment forcortisone injections or surgery
E X A M I N A T I O N
(cont’d)
See answer sheet on page 129.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2001,your enrollment is valid through August 31, 2002.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. All lessonsare approved for 1.5 hours of CE credit. Please readthe testing, grading and payment instructions to de-cide which method of participation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
PM’s CME program is valid in all statesexcept Kentucky.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania

Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card payment may be used for fax or phone-in grading only.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be charged to your credit card.)
______ I am not enrolled. Enclosed is a $17.50 check payable to Podiatry Management Magazine for each exam submitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $109.00 (thus saving me $66 over the cost of 10 individual exam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcheck to: Podiatry Management, P.O. Box 490, East Islip,NY 11730. Credit cards may be used only if you are faxing orphoning in your test answers.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded and may be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your check to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
E N R O L L M E N T F O R M & A N S W E R S H E E T
✄
129
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $17.50 per exam, or $109 to cover all 10exams (thus saving $66 over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet

✄
130 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2004
E N R O L L M E N T F O R M & A N S W E R S H E E T (cont’d)
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
EXAM #1/04Dilute Alcohol Injections for NerveConditions and Keratotic Lesions of
the Foot (Dockery)
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
Contin
uing
Medica
l Edu
catio
n