Embed Size (px)
Citation preview

Eur J Vasc Endovasc Surg 19, 197–201 (2000)
doi:10.1053/ejvs.1999.0988, available online at http://www.idealibrary.com on
Dilatation of the Proximal Neck of Infrarenal Aortic Aneurysms afterEndovascular AAA Repair
J. J. Wever1, A. J. de Nie1, J. D. Blankensteijn∗1, I. A. M. J. Broeders1, W. P. Th. M. Mali2 andB. C. Eikelboom1
Departments of 1Vascular Surgery and 2Radiology, University Medical Center, Utrecht, The Netherlands
Objectives: to assess size changes of the proximal aortic neck after endograft placement.Methods: since 1994, 54 consecutive patients have undergone abdominal aortic aneurysm (AAA) repair with theEndovascular Technologies (EVT) endograft. The study group comprised the 33 patients who had completed at least sixmonths of the prospective follow-up protocol. The pre-, postoperative and follow-up helical computed tomography (CT)angiograms (CTAs) were processed on a workstation. The proximal neck dimensions were measured perpendicular to thecentral lumen line of the aortic neck. The cross-sectional area was measured at the proximal attachment system and at1 cm proximal to the renal arteries.Results: while the dimensions of suprarenal aorta did not change, a significant dilatation of the proximal neck was found.The median increase was 10.3% at 6 months and 15.5% at 12 months. No correlation could be found between the amountof dilatation and pre- or postoperative neck-size, graft diameter and amount of graft-oversizing.Conclusion: the infrarenal aortic neck demonstrates continued dilatation during follow-up after endograft placement.
Key Words: Abdominal aortic aneurysm; Endoprosthesis; Endovascular repair; Spiral computed tomography angiogram(CTA).
Introduction This study was performed to assess size changes of
the supra- and infrarenal aorta after endovascular
Long-term success after endovascular treatment of aneurysm exclusion, as measured along the central
lumen line on spiral CTA scans.abdominal aortic aneurysms depends on durable fixa-
tion of the endograft at the proximal and distal necks.
Gradual dilatation of the aorta at the level of at-
tachment systems may cause leakage and stent mi-
gration. Studies in healthy persons have shown that Patients and Methodsthe infrarenal aortic diameter increases 26% in males
and 24% in females between the age of 25 and 70 From January 1994 until November 1998, 54 con-
secutive patients underwent endovascular treatmentyears.1 After conventional abdominal aortic aneurysm
(AAA) repair higher rates of increase have been de- of an infrarenal aortic aneurysm, using the EVT Endo-
graft (Guidant, Menlo Park, CA, U.S.A.). Post-scribed.2–5
Some studies show dilatation of the proximal aortic operatively, all patients were subjected to contrast-
enhanced computed tomography (CTA) scanning atneck following endovascular AAA repair, but these
studies were performed on axial CT slices.6–8 Proximal discharge, 6 months, 12 months and yearly thereafter.
In 21 patients follow-up was less than 6 months dueneck measurements performed on linear reformats
perpendicular to the central lumen line are preferable. to operative mortality in one, non-related mortality in
one, conversion in six and duration in 10, while threeWith this method the position relative to the renal
arteries is not dependent on the slice thickness, and patients were followed in another hospital. The re-
maining 33 patients were included in the study. Intherefore the reproducibility is better.
these patients, 11 tube, 19 bifurcated and three aorto-
iliac endografts were implanted. There were four fe-∗ Please address all correspondence to: J. D. Blankensteijn, De-
male and 29 male patients. The median age was 69partment of Vascular Surgery, G.04.232, University Medical Center,PO Box 85500, 3508 GA Utrecht, The Netherlands. years (IQ range 63–73).
1078–5884/00/020197+05 $35.00/0 2000 Harcourt Publishers Ltd.

J. J. Wever et al.198
Table 1. Median cross-sectional area (IQ range) during follow-upin mm2.
Postoperative 6 months 12 months(n=33) (n=33) (n=24)
Proximal neck 346 (292–379) 365 (321–418)∗ 397 (309–439)∗Suprarenal 378 (340–423) 399 (331–440) 390 (342–442)
∗ p<0.01 Wilcoxon rank.
Table 2. Median of the individual changes (IQ range) comparedto the postoperative value.
6 months 12 months(n=33) (n=24)
Proximalneck +10.3% (+4.9%–+15.1%) +15.5% (+11.7–+24.4%)Suprarenal +1.1% (−4.5%–+5.4%) −3.2% (−6.9%–+4.1%)
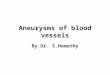
Fig. 1. Drawing of the contour on the linear reformats. The cut-planeis always perpendicular to the vessel axis, providing a reproduciblemeasurement. 6–48). The median cross-sectional area showed a sig-
nificant increase at the level of the proximal attachment
system from 346 (292–379) mm2 to 365 (321–417) mm2
Preoperative, postoperative and follow-up contrast-at 6 months (p<0.01) and to 397 (309–438) mm2 at 12
enhanced CT images were reviewed on an Easy Visionmonths (p<0.01) compared to the postoperative area
workstation (Philips Medical Systems, Best, The Neth-(Table 1). The median increase between 6 and 12
erlands) to determine changes in cross-sectional areamonths was also statistically significant (p<0.05). The
of the abdominal aorta at the levels indicated below.median of the individual changes was +10.3% after
All measurements were taken perpendicular to the6 months and +15.5% after 12 months. These results
central lumen line.9–12 Proximal neck dimensions wereare shown in Table 2. The size changes at the level
measured 1 cm below the most distal renal artery. Onof the proximal attachment system in the individual
the preoperative scans, a contour was drawn outliningpatients are shown in Fig. 2. All but two patients
the aorta. On the postoperative scans this level allowedshowed an increasing cross-sectional area during fol-
measuring the neck in the proximal attachment system,low-up, compared to the first postoperative measure-
and the contour was drawn through the hooks (Fig.ment. In three patients, four years of CTA follow-up
1). The suprarenal aortic dimensions were measuredwas available demonstrating an increased neck-size of
in the same manner at 1 cm above the most proximal11.1%, 21.5% and 24.9% at 24, 36 and 48 months,
renal artery.respectively.
For statistical analysis the Wilcoxon rank test wasThe suprarenal aorta did not show significant
used to assess significance of postoperative and follow-growth (p>0.4) (Fig. 3). The individual neck-sizes on
up size changes. Correlation between the amount ofthe first postoperative scans were all smaller than the
dilatation and pre- and postoperative neck-size, graftnominal (maximal) size of the implanted stent graft,
diameter and amount of graft-oversizing was cal-due to intentional graft-oversizing. The median ratio
culated using Spearman’s test. A value of p<0.05 wasof oversizing was 1.13 (1.07–1.31). The amount of
considered statistically significant. All values are givendilatation did not correlate with preoperative neck-
as median and quartile range or as individual values.size (r=−0.12, p=0.50), postoperative neck-size (r=−0.25, p=0.16), nominal graft diameter (r=0, p=1.00)
or attachment system oversize (r=0.08, p=0.67). No
correlation with the presence of early (r=−0.09, p=Results0.59, n=14) or late endoleak (r=0.06, p=0.74, n=8)
could be demonstrated. Secondary endoleak or mi-The 6-month, 1-, 2-, 3- and 4-year follow-up scans
were available in 33, 24, nine, five and three patients gration was not encountered in the studied patient
group.respectively. Median follow-up was 12 months (range
Eur J Vasc Endovasc Surg Vol 19, Month 2000

Proximal Neck Dilatation after Endovascular AAA Repair 199
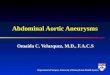
Fig. 2. Cross-sectional area at the proximal aortic neck in the 33 patients. Size in square millimetres is indicated on the vertical axis, andfollow-up interval for each patient is indicated on the horizontal axis.
Discussion Matsumura et al.,13 no significant proximal neck growth
was demonstrated at 12 months. In their study, 34
The postoperative scan data demonstrate significant patients with an EVT endograft were analysed using
axial diameter measurements. One year later, the sameproximal neck dilatation at 6 and 12 months after
endovascular AAA repair. Comparison to the pre- authors reported on a larger group of patients (n=59)
and showed a mean increase of 0.7 and 0.9 mm inoperative scans was not performed because aortic neck
measurements with or without an EVT endograft in proximal neck diameter after 1 and 2 years re-
spectively.7 May et al.8 reported on increasing proximalplace are difficult to compare. The reason for this is
that artefacts caused by the stent material prevent neck diameters when comparing the preoperative val-
ues with the postoperative ones, but no progressivemeasurement of the aortic wall. Therefore, the area
within the stent was measured. For obvious reasons, increase at 6, 12 and 18 months. The diameters were
measured 1 cm below the renal arteries on axial CTthis measurement was not available from the pre-
operative scans. slices. They found no increase in aortic diameter at
the level of the coeliac trunk. The above-mentionedThe use of a workstation allowed measuring cross-
sectional areas. Other groups have studied the changes studies are difficult to compare, as various stent-graft
designs were used.in diameter and circumference but the reproducibility
of these measurements is limited in case of irregular Two possible explanations can be given for continued
growth of the infrarenal neck after endovascular AAAcontours of the proximal neck. Using callipers, Sones-
son et al.6 measured diameters on axial CT planes in repair. It is either a continuation of the aneurysmal dis-
ease process or an effect of the outward force generated31 patients treated with a home-made stent graft. They
found a significant mean increase of 1.7 mm at the last by theendovascular stentonto the infrarenalaortic wall.
Although it is most probably a combination of theseavailable follow-up scan compared to the preoperative
neck-size. In addition an insignificant mean increase two factors, it is interesting to discuss these issues sep-
arately, as the proximal attachment mechanisms varyof the suprarenal aorta was found. In the study of
Eur J Vasc Endovasc Surg Vol 19, Month 2000

J. J. Wever et al.200
Fig. 3. Cross-sectional area at the suprarenal aortic neck in the 33 patients. Size in square millimetres is indicated on the vertical axis, andfollow-up interval for each patient is indicated on the horizontal axis.
betweentheavailablestent-graftdesigns. If theoutward Initial dilatation due to the procedure without sub-
sequent dilatation cannot be considered an adequateforce is the predominant cause of postoperative neck
dilatation, the diameter will probably not stretch bey- explanation, as the increase of the proximal neck area
was statistically significant for both the first and secondond the nominal (maximal) stent-size. But as the stent
approaches its maximal size, the friction forces between 6 months’ follow-up interval. No significant increase
of the suprarenal aorta was found in our study. Al-stentandaorticwallmaybecomedangerously low,with
possible stent migration as a result. The preferred graft though this provides some support of the theory that
progression of disease is not the only factor, it mustattachment design from this perspective would consist
of a stent with low outward force to prevent accelerated be realised that the infrarenal aorta has a less dense
fibre structure when compared to the suprarenaldilatation and a fixation mechanism independent of
friction forces between stent and neck (i.e. hooks). If aorta.14 No correlation could be found between the
presence or absence of endoleaks, pre- and post-progressive enlargement is merely a consequence of the
underlying aneurysmal disease, the oversizing of the operative neck-size, graft diameter and amount of
graft oversize, probably due to small numbers.stent graft relative to the neck-size actually allows the
stent to adapt to the neck dilatation. In this scenario, In conclusion, the infrarenal aortic neck dem-
onstrates continued dilatation after endograft place-high outward force would not necessarily be detri-
mental to the neck. Although it may take a longer period ment.
of time, the end-result of continued neck dilatation in
the presence of a stent with a limit to its diameter will
ultimately be the same: potential graft migration if noReferencesother fixation mechanisms are present. In addition, di-
latation beyond the nominal stent size may create a1 Sonesson B, Lanne T, Hansen F, Sandgren T. Infrarenal aortic
secondary attachment site leak, even without stent mi- diameter in the healthy person. Eur J Vasc Surg 1994; 8: 89–95.2 Lipski DA, Ernst CB. Natural history of the residual infrarenalgration.
Eur J Vasc Endovasc Surg Vol 19, Month 2000

Proximal Neck Dilatation after Endovascular AAA Repair 201
aorta after infrarenal abdominal aortic aneurysm repair. J Vasc 9 Balm R, Eikelboom BC, van Leeuwen MS, Noordzij J. SpiralSurg 1998; 27: 805–811. CT-angiography of the aorta. Eur J Vasc Surg 1994; 8: 544–551.
3 Illig KA, Green RM, Ouriel K et al. Fate of the proximal aortic 10 Broeders IA, Blankensteijn JD, Olree M, Mali W, Eikelboomcuff: implications for endovascular aneurysm repair. J Vasc Surg BC. Preoperative sizing of grafts for transfemoral endovascular1997; 26: 492–499. aneurysm management: a prospective comparative study of
4 Curl GR, Faggioli GL, Stella A, D’Addato M, Ricotta JJ. spiral CT angiography, arteriography, and conventional CT im-Aneurysmal change at or above the proximal anastomosis after aging. J Endovasc Surg 1997; 4: 252–261.infrarenal aortic grafting. J Vasc Surg 1992; 16: 855–859. 11 Balm R, van Leeuwen MS, Noordzij J et al. Spiral CT for
5 Sonesson B, Resch T, Lanne T, Ivancev K. The fate of the aortic aneurysms. In: Greenhalgh RM, eds. Vascular Imaging forinfrarenal aortic neck after open aneurysm surgery. J Vasc Surg Surgeons. W. B. Saunders Co Ltd., 1995: 191–202.1998; 28: 889–894. 12 Balm R, Kaatee R, Blankensteijn JD, Mali WP, Eikelboom
6 Sonesson B, Malina M, Ivancev K et al. Dilatation of the BC. CT-angiography of abdominal aortic aneurysms after trans-infrarenal aneurysm neck after endovascular exclusion of ab- femoral endovascular aneurysm management. Eur J Vasc En-dominal aortic aneurysm. J Endovasc Surg 1998; 5: 195–200. dovasc Surg 1996; 12: 182–188.
7 Matsumura JS, Chaikof EL. Continued expansion of aortic 13 Matsumura JS, Pearce WH, McCarthy WJ, Yao JS. Reductionnecks after endovascular repair of abdominal aortic aneurysms. in aortic aneurysm size: early results after endovascular graftEVT Investigators. EndoVascular Technologies, Inc. J Vasc Surg
placement. EVT Investigators. J Vasc Surg 1997; 25: 113–123.1998; 28: 422–430.
14 Wolinsky H. Comparison of medial growth of human thoracic8 May J, White G, Yu W et al. A prospective study of anatomico-
and abdominal aortas. Circ Res 1970; 27: 531–538.pathological changes in abdominal aortic aneurysms followingendoluminal repair: is the aneurysmal process reversed? Eur JVasc Endovasc Surg 1996; 12: 11–17. Accepted 13 August 1999
Eur J Vasc Endovasc Surg Vol 19, Month 2000