Embed Size (px)
Citation preview

Diffusion -weighted MRImaging of the Kidneysand the UrinaryTract
Sooah Kim, MDa, Mohit Naik, MDa, Eric Sigmund, PhDb,BachirTaouli, MDc,*KEYWORDS� MR imaging � Diffusion � Kidney � Renal neoplasm� Renal function
Diffusion-weighted imaging (DWI) provides quanti-fication of Brownian motion of water protons bycalculating the apparent diffusion coefficient(ADC), and can be used for in vivo quantificationof the combined effects of capillary perfusionand diffusion.1 Diffusion contrast is based on thethermally driven random motion of molecules intissue. Bulk fluids show a mean-squared displace-ment that grows linearly with time at a rate given bythe ADC. In such free fluids, the diffusion coeffi-cient is determined by molecular architecture,interactions, and temperature. In tissue, however,the protons’ motion is hindered or restricted bydifferent components such as cell membranes,cellular density, or macromolecules. This is mani-fested macroscopically by an ADC that is reducedfrom the bulk value. If the underlying tissue struc-ture is ordered (such as the medullary tubules inthe kidney), the ADC shows a correspondinganisotropy along different directions. If the tissuestructure shows no preferred direction when aver-aged over the MR imaging resolution (such as inthe renal cortex), the ADC will appear isotropic,although reduced from the bulk value. In all ofthese cases, the ADC (and other indices derivedfrom them) serves as markers of the structuraland functional state of the imaged tissue. Someexamples include (1) anisotropic diffusion in whitematter tissue in diffusion tensor imaging (DTI),2
providing both quantitative biomarkers andqualitative fiber tractography information, and
a Department of Radiology, New York University Medicab Department of Radiology, New York University MedicAvenue, New York, NY 10016, USAc Department of Radiology, New York University LangNY 10016, USA* Corresponding author.E-mail address: [email protected] (B. Taouli).
Magn Reson Imaging Clin N Am 16 (2008) 585–596doi:10.1016/j.mric.2008.07.0061064-9689/08/$ – see front matter ª 2008 Elsevier Inc. All
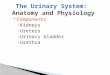
(2) corticomedullary differentiation in the kidneydue to the medulla’s anisotropic tubules.3 In gen-eral, the clinical implications of ADC changedepend on the tissue under investigation; ananomalous rise in ADC can indicate increasededema, cystic changes, and necrosis; whereasan anomalous reduction in ADC might indicateischemia, infection, or tumor. As such, diffusionmeasures should be taken in context with otherimaging contrasts to ensure an accurate diagno-sis. In DWI, the ADC is quantitatively measuredthrough the application of a diffusion gradient,a magnetic field that spatially varies along a partic-ular direction, which induces a variation in Larmorprecession frequency among the spins.4,5 Further-more, the stochastic motion of the spins along thisgradient causes an irreversible loss of phasecoherence that reduces the total magnitude ofthe spin magnetization, ie, the MR signal. Therate of this decay as a function of an experimen-tally determined diffusion-weighting factor bdetermines the ADC. DWI incorporates this mea-surement into a spatially resolved scan. Themost common method employed in clinical MRIscanners is bipolar-gradient diffusion preparationwith single-shot echo-planar imaging (EPI)(Fig. 1).6,7 This approach captures the diffusioncontrast while minimizing both eddy current8 andmotion artifacts, but can be limited by susceptibil-ity artifacts at high magnetic field. Many otherDWI techniques9–12 have been developed to
l Center, 560 First Avenue, New York, NY 10016, USAal Center, Center for Biomedical Imaging, 660 First
one Medical Center, 560 First Avenue, New York,
rights reserved. mri
.thec
lini
cs.c
om

Fig.1. Gradient scheme for the single shot echo planar imaging sequence with diffusion-sensitizing gradients (ingray) located on each side of the 180� pulse.
Kim et al586
circumvent this problem, and may prove vital in thesuccessful migration of DWI to the high- and ultra-high field platforms (3 T and above).
DIFFUSION ACQUISITION PARAMETERS FORIMAGING THEKIDNEYSANDTHEURINARY TRACT
Breath-hold or respiratory triggered (using anavigator echo) DWI is acquired before contrastinjection using single-shot echoplanar imaging,with the suggested following parameters: axial orcoronal acquisition, fat suppression, tridirectionalgradients using the following b-values: 0 (used asreference), 400 (intermediate), and 800 (high)sec/mm2. The choice of b-values is somehow arbi-trary and depends on the equipment used. Lowerb-values will generate higher ADC values, owing tothe contribution of intravoxel incoherent motioneffects other than diffusion (eg, perfusion or flowphenomena), as opposed to higher b-values,which will enable ‘‘pure’’ diffusion weighting, atthe expense of lower residual signal. To reducethe effects of intravoxel incoherent motion, maxi-mum b-values of 800 sec/mm2 or greater are sug-gested whenever possible. We suggest a baselineb 5 0 sec/mm2 image (used as a reference) andintermediate b-value (for example, 400 sec/mm2),which provides intermediate diffusion weightingwith acceptable image quality, and a higherb-value (for example, b 5 800 sec/mm2), whichprovides higher diffusion weighting, free from per-fusion and flow contamination. In addition, the useof three b-values provides a more precise ADC fit.The other parameters used in our protocol are asfollows: repetition time 1800 to 2300 msec, timeto echo min (65 to 68 msec), field of view 240 to315 � 320 to 420 mm, matrix 180 � 192, slicethickness/gap 7/1.4 mm, number of averages 2(breath-hold) or 4 (respiratory triggered acquisi-tion), parallel imaging (acceleration factor 2), EPIfactor 144 to 192, bandwidth 1302 Hz/pixel, acqui-sition time approximately 2 � 20 seconds to coverthe whole kidneys (for the breath-hold acquisition),and at least 2 minutes for the respiratory triggeredacquisition. We obtain pixel-based ADC maps
(integrating the three b-values) using a commercialworkstation, ADC is calculated with a linear re-gression analysis of the function S 5 S0 � exp(�b � ADC), where S is the SI after applicationof the diffusion gradient, and S0 is the SI atb 5 0 sec/mm2.
DWI APPLICATIONS IN DIFFUSE RENAL DISEASEAND RENALTRANSPLANT
There are several published studies that haveinvestigated the use of DWI in normal kidneys,3,13–19
for the assessment of diffuse renal disease,16,20,21
renal artery stenosis,22 renal infection,23 urinaryobstruction,19 and renal transplants.24
The feasibility of DWI of the kidneys in healthyvolunteers has been reported by several investiga-tors. The reported ADC values of renal cortex andmedulla vary considerably from study to studydepending on the equipment and the sequenceparameters, particularly the b-value,13,15,16,20
with mean ADCs of normal kidney ranging from1.63 to 5.76 � 10�3 mm2/sec. In our experience,using b-values of 0 to 400 to 800 sec/mm2, themean ADC of normal cortex and medulla were2.16 � 0.37 and 1.90 � 0.26 � 10�3 mm2/sec,respectively (in 64 patients), with significantlyhigher ADC in the cortex (P < .05).
Murtz and colleagues17 showed better ADCreproducibility when using a pulse trigger, withsmaller standard deviation of ADC with a triggercompared with the acquisition without a trigger.Muller and colleagues13 investigated the effect ofhydration and anisotropic kidney diffusion usingmultiple b-values on 23 volunteers, and renalADC values of dehydrated subjects were substan-tially increased with rehydration. Ries andcolleagues3 used diffusion tensor imaging toinvestigate the anisotropic diffusion in the normalkidney, and were able to demonstrate the aniso-tropic structure of the renal medulla, which hada higher fractional anisotropy (FA) compared withthe cortex (0.39 � 0.11 versus 0.22 � 0.12,respectively).

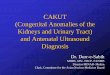
Fig. 2. A 56-year-old woman with renal transplant segmental ischemia caused by high-grade stenosis of the trans-plant renal artery. Axial single-shot echoplanar diffusion-weighted images demonstrate segmental restricteddiffusion involving the anterior aspect of the transplant kidney (arrows) on images at b 5 800 sec/mm2
(A) and ADC map (B) compared with the remainder of the renal parenchyma. Axial contrast-enhanced fatsuppressed T1-weighted images obtained at the corticomedullary (C) and nephrographic (D) phases demonstratedecreased perfusion in the corresponding area consistent with ischemia. Coronal reconstruction of MR angiog-raphy (E) demonstrates severe stenosis of the anterior branch of the transplant renal artery (arrow).
Renal DWI 587
Several studies have shown the potential use ofADC as a marker of renal function, most studiesshowing lower ADC in kidney dysfunction. Forexample, Namimoto and colleagues20 demon-strated that the ADC values in both the cortexand medulla in chronic renal failure (CRF) and
acute renal failure (ARF) kidneys were significantlylower than those of normal kidneys. In the cortex,ADC values were above 1.8 � 10�3 mm2/sec in allnormal kidneys (n 5 32), ranging from 1.6 to2.0 � 10�3 mm2/sec in all ARF kidneys (n 5 8),and below 1.5 � 10�3 mm2/sec in 14 of 15 CRF

Fig. 3. A 63-year-old woman with acute pyelonephritis of the right kidney. Axial single shot echoplanar diffusion-weighted images demonstrate multifocal patchy lesions that are hypointense at b 5 0 sec/mm2 (A), isointense atb 5 500 (B), and hyperintense at b 5 1000 sec/mm2 (C) compared with renal parenchyma (arrows). ADC map (D)shows low ADC (1.35 � 0.4 � 10–3 mm2/sec for b = 0 to 500 to 1000 sec/mm2, arrows) compared with the remain-der of the normal parenchyma.
Kim et al588
kidneys (using b-values of 0, 30, and300 sec/mm2). In the medulla, there was consider-able overlap in the ADC values of the normal anddiseased kidneys. There was a linear correlationbetween ADC value and serum creatinine level inthe cortex (r 5 0.75) and a weak linear correlationin the medulla (r 5 0.60). Thoeny and colleagues19
have shown that ADC of cortex was higher thanmedulla in normal kidneys, as in our experience.In addition, the ADC values using all b-valueswere lower in chronic renal disease comparedwith normal kidneys, as well as in patients withpyelonephritis compared with the contralateralside, whereas patients with ureteral obstructionshowed varying degrees of difference in all ADCvalues compared with the contralateral side. How-ever, another study by Muller and colleagues13 onureteral obstruction in an animal model showeddecreased ADC in ureteral obstruction.
Recently,Xuandcolleagues21 reportedapositivecorrelation between ADC (measured with b-valuesof 0 and 500 sec/mm2) and the split glomerular
filtration rate (GFR) in 55 patients (r 5 0.709). TheADCs were significantly lower in impaired kidneysthan in normal kidneys. The mean renal ADCs(� 10�3 mm2/sec) of the four groups (normal renalfunction, GFR > 40 mL/min/1.73 m2; mild renalimpairment, GFR between 20 and 40 mL/min/1.73m2; moderate renal impairment, GFR between 10and 20 mL/min/1.73 m2; and severe renalimpairment, GFR < 10 mL/min/1.73 m2) were2.87 � 0.11, 2.55 � 0.17, 2.29 � 0.10, and 2.20 �0.11, respectively.
Namimoto and colleagues20 also evaluated theADC values in seven kidneys with renal artery ste-nosis (RAS). In RAS, the ADC values in the cortex(1.5 � 10�3 mm2/sec) were significantly lower thanthose of the normal and the contralateral kidneys,but ADC values of medulla were slightly lower thannormal but not significantly different. Recently,Yildririm and colleagues22 compared the ADCvalues of 13 kidneys with RAS and 26 with normalrenal arteries using multiple b-values, and foundsignificant differences in mean ADC of kidneys

Fig. 4. A 83-year-old man with septatedcyst of the left kidney. Axial breath-holdin-phase T1-weighted image (A) andbreath-hold T2-weighted imaging(B) with a half-Fourier acquisition singleshot turbo spin-echo sequence demon-strate a 13 cm partially septated cyst inthe left kidney. Axial single-shotechoplanar diffusion-weighted imagesdemonstrate a left renal mass that ishyperintense on diffusion-weighted MRimage at b 5 0 sec/mm2 (C), with strongsignal drop at b 5 400 (D), and strongerat b 5 800 sec/mm2 (E). ADC map (F)shows high ADC (3.3 � 0.15 10 mm2/secfor b 5 0 to 400 to 800 sec/mm2).
Renal DWI 589
using lower, average, and high b-values betweentwo groups (average ADC 1.7 � 10�3 mm2/secfor RAS versus 1.9 � 10�3 mm2/sec for normalkidneys).
There are extremely limited data on the use ofDWI in renal transplantation. The only availablestudy by Thoeny and colleagues19 was performedin normal-functioning kidney transplants and
normal native kidneys. In their study, the ADCs ofnative kidneys were significantly higher in thecortex than in the medulla, whereas the ADCs ofthe transplant kidneys were almost identical inthe medulla and the cortex, while the perfusionfraction (measured with smaller b-values) showedgreater variation. The perfusion fraction reflectsmicrocirculation of blood and movement in

Fig. 5. A 74-year-old woman with T1 hyperintense cyst of the left kidney. Axial breath-hold unenhanced (A) andcontrast-enhanced subtracted (B) fat-suppressed T1-weighted interpolated spoiled gradient recalled echo imagesshow a 3-cm T-1 hyperintense left renal mass (arrows) without evidence of enhancement on subtraction consis-tent with a benign cyst. Axial single-shot echoplanar imaging diffusion-weighted images demonstrate a rightrenal mass (circles) that is hyperintense on diffusion-weighted MR image at b 5 0 sec/mm2 (C), b 5 50 (D), andat b 5 500 sec/mm2 (E) compared with renal parenchyma. ADC map (F) shows high ADC (3.90 � 0.6 � 10�3
mm2/sec).
Fig. 6. A 35-year-old man with autosomal dominant polycystic kidney disease. Unenhanced axial fat-suppressedT1-weighted gradient echo image (A) shows variable signal intensity of the renal cysts because of intervalhemorrhage or proteinaceous contents. ADC map obtained from axial single-shot echoplanar diffusion-weightedusing b-values of 0 and 400 sec/mm2 (B) shows relatively decreased ADC in some of the cysts with higher signalintensity on precontrast T1-weighted image (long arrows) compared with simple cysts (small arrows).
Kim et al590

Fig. 7. A 43-year-old man with papillary renal cell carcinoma of the right kidney. Large 10 cm centrally cystic andperipherally solid right renal mass demonstrated on coronal single-shot echoplanar diffusion-weighted images atb 5 0 (A), b 5 400 (B), and b 5 800 sec/mm2 (C), ADC map (D), coronal T2-weighted image with a half-Fourieracquisition single-shot turbo spin-echo sequence (E) and subtracted postcontrast coronal reformatted T1-weighted image (F). The ADC was lower in the solid portion compared with the central cystic portion (1.10 vs.1.75 � 10�3 mm2/sec).
Renal DWI 591
predefined structures, such as tubular flow and glo-merular filtration in the kidneys. The corticomedul-lary difference was relatively small and was notsignificantly different in the transplanted kidneys.This suggests that perfusion fraction is influencedpredominantly by factors other than blood perfu-sion, such as tubular flow. There are no reports onthe utility of DWI for the diagnosis of posttransplantcomplications, such as vascular complications (ste-nosis, thrombosis, and infarction), acute tubular ne-crosis, and rejection. Validation of DWI is needed inrenal transplants with histopathologic correlation,given the noninvasive nature of diffusion measure-ment, performed without gadolinium injection.
Based on our experience, DWI could be used todemonstrate acute renal transplant infarction(Fig. 2), and to diagnose acute pyelonephritis(Fig. 3).
DWI FOR THE CHARACTERIZATION OF FOCALRENAL LESIONS
The diagnosis of renal neoplasm is usually basedon the presence of enhancement on CT or MRimaging, and image subtraction has been shownto be superior to signal intensity measurementfor the diagnosis of renal cell carcinoma (RCC).25
DWI provides qualitative and quantitative informa-tion on tissue characterization without the need forgadolinium administration, and there is a strongneed for alternatives to gadolinium-enhancedsequences for renal lesion characterization forthe patients at risk for nephrogenic systemic fibro-sis (NSF).26–28 However, there are limited studieson the application of DWI for the assessment ofrenal masses.29–32 Solid or malignant lesions gen-erally have lower ADC with restricted diffusion

Fig. 8. Papillary urothelial carcinoma of the bladder located at the right ureterovesicular junction. The tumor ishypointense on axial single-shot echoplanar diffusion-weighted image at b 5 0 sec/mm2 (A), and hyperintenseat b 5 500 sec/mm2 compared with urine (B) (arrow). The mass has restricted diffusion with lower ADC comparedwith urine as seen on the ADC map (C) (arrow). The mass demonstrates intense enhancement on contrast-enhanced image (D) (arrow).
Kim et al592
compared with benign or cystic lesions, since themotion of water molecules is restricted in tissueswith a high cellular density associated with numer-ous intact cell membranes (eg, tumor tissue),which act as barriers to motion of water molecules.
Cova and colleagues30 applied DWI usingb-values 0 and 500 sec/mm2 for 20 focal renallesions and compared ADC values between le-sions and normal renal parenchyma: mean ADCin simple cysts (n 5 13) was 3.65 � 0.09 � 10�3
mm2/sec, which was significantly higher than nor-mal renal parenchyma (mean 2.19 � 0.17 � 10�3
mm2/sec). Solid benign and malignant tumors(three RCCs, one oncocytoma, and three angio-myolipomas [AMLs]) showed a mean ADC valueof 1.55 � 0.20 � 10�3 mm2/sec, ranging between1.28 � 0.11 and 1.83 � 0.14 x10�3 mm2/sec, sig-nificantly lower than normal renal parenchyma. Inanother study from the same group (using thesame b-values), Squillaci and colleagues29 alsodemonstrated lower ADC values in solid renaltumors (n 5 19, including 12 RCCs) compared
with simple cysts (n 5 20): 1.7 � 0.48 versus3.65 � 0.09 � 10�3 mm2/sec. Yoshikawa and col-leagues31 evaluated a total of 67 renal lesions(including 12 RCCs, ADC 5 2.49 � 0.72, AMLs[n 5 8] 1.81 � 0.41, cysts [n 5 42] 3.82 � 0.39,complicated cysts [n 5 5] 2.78 � 0.71 [b 5 0 to600 sec/mm2]), and found similar results as in thepreviously mentioned studies29,30: ADCs of renalcysts were significantly higher than those ofRCCs (3.82 � 0.39 versus 2.49 � 0.72 � 10�3
mm2/sec). They found, however, no significantdifference between ADCs of RCC versus compli-cated cysts and renal parenchyma. Recently,Zhang and colleagues32 reported the use of DWIin solid and partially cystic renal masses (in 25 pa-tients) using b-values of 0, 500, and 1000 sec/mm2. Their ADC measurement method consistedfirst by putting large regions of interest fitting thewhole lesion, and then by segmenting lesionsinto necrotic/cystic and solid components basedon contrast-enhanced imaging. Their findingsextended those reported previously (high ADC in

Fig. 9. A 39-year-old woman with renal abscess, a false positive of diffusion-weighted imaging. Axial single-shotechoplanar diffusion-weighted images demonstrate a hyperintense lesion with peripheral hypointense rim atb 5 0 sec/mm2 (A), the lesion is hyperintense at b 5 400 sec/mm2 (B) compared with renal parenchyma. ADCmap (C) shows low ADC (1.28 � 0.33 � 10�3 mm2/sec) compared with normal parenchyma. Axial post-contrastfat-suppressed T1-weighted image obtained at the nephrographic phase (D) demonstrates a necrotic lesionwith peripheral rim enhancement consistent with a renal abscess, which was subsequently confirmed by surgicaldrainage.
Renal DWI 593
simple cysts compared with neoplasms), with theaddition of finding lower ADC values incystic/necrotic portions of neoplasms comparedwith simple cysts: 2.21 � 0.63 versus 3.26 � 061(P < .05). However, none of the previouslymentioned studies have evaluated the accuracyof DWI for renal mass characterization.
We have been using DWI systematically since2005, and based on our experience, we believethat renal lesions can be accurately characterizedwith DWI, however with lower sensitivity andspecificity compared with contrast-enhancedsequences. For diagnosing RCC, the AUC (areaunder the curve) sensitivity and specificity were0.856, 85.7% and 80.3%, respectively for DWI(using ADC % 1.92 � 10�3 mm2/sec for b 5 0 to400 to 800 sec/mm2), compared with 0.944,100% and 88.6% for contrast-enhancedsequences (based on 99 lesions in 62 patients).
The distribution of ADC values (mean �SD,� 10�3 mm2/sec) was as follows: simple cysts(category I from the Bosniak classification)33 (high-est ADC 2.78 � 0.45), category II (2.47 � 0.64)
(Figs. 4–6), oncocytomas (1.91 � 0.97), categoryIIF (1.85 � 0.71), category III-IV (1.83 � 0.85), solidRCCs (1.41 � 0.61), and angiomyolipomas (AMLs)(0.74 � 0.45).34
As in prior studies, we found RCCs (Fig. 7) andAMLs to have the lowest ADCs. Cystic RCCsmay have higher ADC values than solid tumorsdue to their cystic components. The decreasedADC in AMLs can be explained by the muscularand fat components restricting diffusion.
Another interesting finding in our series was thepossibility of characterizing solid neoplasms withDWI: oncocytomas having higher ADC than solidRCCs (1.91 � 0.97 versus 1.54 � 0.69, P < .01).Moreover, papillary RCCs demonstrated lowerADC compared with nonpapillary RCCs (mostlyclear cell RCCs): 1.12 � 0.18 versus1.62 � 0.73 � 10�3 mm2/sec (using b-values of0 to 400 to 800 sec/mm2).
We have also shown that T1 hyperintense cysts(which include proteinaceous and hemorrhagiccysts) have slightly lower ADC compared withsimple cysts, probably related to a T2 effect, and

Fig.10. Diffusion tensor imaging (DTI) in a normal kidney at 3 T. Breath-hold single-shot echoplanar DTI sequencewith b 5 0 and 500 s/mm2, using diffusion gradients in six directions. DEC and e1 maps are color coded accordingto standard RGB directional reference (lower right). The b0 map shows normal corticomedullary differentiation.The MD map shows slightly lower ADC in the medulla than in the surrounding cortex. Dramatic contrast betweencortex and medulla appears in the FA map, where the anisotropic microstructure of the medullary tubulesinduces high FA values. Finally, the DEC and eigenvector maps confirm the radial orientation of the diffusiontensor in the medullary compartments, where the tubules point toward the urinary collection system at thecenter of the kidney. b0, T2-weighted reference image; MD, mean diffusivity (ADC map); FA, fractional anisotropymap; DEC, direction encoded color map; e1, principal diffusion eigenvector (length weighted by FA).
Kim et al594
to restricted diffusion in hemorrhage or highprotein component as described in brain hemato-mas.35 However, the ADCs of T1 hyperintensebenign cysts were still higher than those of T1 hy-perintense RCCs: 2.50 � 0.53 versus 1.75 � 0.57,P < .0001.36
DWI FOR DETECTION AND FUNCTIONALEVALUATION OF BLADDER CANCER
Bladder cancer is the most common cancer of theurinary tract, with an estimated 68,810 new casesand 14,100 deaths expected to occur in 2008.37
Urothelial carcinoma is the most common tumorconstituting over 90% of cancers.
Clinically, over 80% of patients with bladdercancer present with hematuria, either macro-scopic or microscopic. All patients with macro-scopic hematuria and those patients withmicroscopic hematuria where a benign causehas been excluded, require urologic workup. Cur-rent guidelines recommend direct evaluation of thebladder with cystoscopy and imaging evaluationof the upper tract.
DWI could be used both for detection and func-tional evaluation of bladder cancer, however thereare extremely limited data on the subject.38,39
Our recent experience with DWI for assessmentof bladder cancer is very promising.40 Bladderneoplasms have restricted diffusion, and aretherefore easily detected in the background urineusing intermediate and high b-values, withincreased conspicuity (Fig. 8). Thus, DWI may beconsidered as an alternative to gadolinium con-trast in patients with chronic renal insufficiencywhere there is increased concern for NSF.
We also demonstrated a significant correlationof ADC and normalized ADC (ADC tumor/ADCurine) with tumor grade and stage (r �0.83,P < .001). Normalized ADC had a sensitivity, spec-ificity, and accuracy of 100% for prediction oftumor stage of III or higher (for a threshold nADC% 0.46).
LIMITATIONS OF DWI
There are several limitations to the technique thatwill delay its widespread use: the ADC values are

Renal DWI 595
highly dependent on the parameters and the scan-ner used, thus the need for standardization ofacquisition parameters and postprocessingmethods between centers. More data are neededfor the correlation between DWI and histopathol-ogy, and for its use as a predictor of treatmentresponse. Another limitation is the lack of sensitiv-ity and specificity of ADC measurement for thediagnosis of neoplasm, as ADC can be decreasedin renal abscesses (Fig. 9), and falsely elevated incystic RCCs. And last but not least, there is a needfor improving image quality, for example usinga combination of 3T, parallel imaging, and a navi-gator echo acquisition.
FUTURE DIRECTIONS
To be validated as a biomarker of treatmentresponse, studies correlating ADC changes withresponse to treatment are needed (for example,post local ablation of RCC, and post neoadjuvanttherapy in bladder cancer). Histogram analysis ofADC values is also worth investigating in heteroge-neous cystic renal lesions. Another interestingapplication is the use of diffusion tensor imaging,which has the potential to shade light on the micro-structure of the cortex and medulla (Fig. 10).
SUMMARY
In conclusion, DWI has shown promise for theassessment of focal and diffuse renal disease aswell as in bladder cancer, with multiple potentialapplications. Advantages of DWI include the abilityto characterize focal renal lesions, and the predic-tion of stage and grade of bladder cancer. Theability to perform DWI without intravenous gadoli-nium is also a major advantage of DWI. However,more supporting data comparing DWI tocontrast-enhanced imaging and pathology areneeded.
REFERENCES
1. Le Bihan D. Diffusion/perfusion MR imaging of the
brain: from structure to function. Radiology 1990;
177:328–9.
2. Basser PJ. Inferring microstructural features and the
physiological state of tissues from diffusion-
weighted images. NMR Biomed 1995;8:333–44.
3. Ries M, Jones RA, Basseau F, et al. Diffusion tensor
MRI of the human kidney. J Magn Reson Imaging
2001;14:42–9.
4. Callaghan PT. Principles of nuclear magnetic reso-
nance microscopy. Oxford (United Kingdom):
Oxford University Press; 1993. p. 492.
5. Hahn EL. Spin echoes. The Physical Review 1950;
80(4):580–94.
6. Stehling MK, Turner R, Mansfield P. Echo-planar
imaging—magnetic-resonance-imaging in a fraction
of a second. Science 1991;254:43–50.
7. Feinberg DA, Jakab PD. Tissue perfusion in humans
studied by Fourier velocity distribution, line scan,
and echo-planar imaging. Magn Reson Med 1990;
16:280–93.
8. Reese TG, Heid O, Weisskoff RM, et al. Reduction of
eddy-current-induced distortion in diffusion MRI us-
ing a twice-refocused spin echo. Magn Reson Med
2003;49:177–82.
9. Nolte UG, Finsterbusch J, Frahm J. Rapid isotropic
diffusion mapping without susceptibility artifacts:
whole brain studies using diffusion-weighted sin-
gle-shot STEAM MR imaging. Magn Reson Med
2000;44:731–6.
10. Bastin ME, Le Roux P. On the application of a non-
CPMG single-shot fast spin-echo sequence to diffu-
sion tensor MRI of the human brain. Magn Reson
Med 2002;48:6–14.
11. Pipe JG, Farthing VG, Forbes KP. Multishot diffusion-
weighted FSE using PROPELLER MRI. Magn Reson
Med 2002;47:42–52.
12. Miller KL, Pauly JM. Nonlinear phase correction for
navigated diffusion imaging. Magn Reson Med
2003;50:343–53.
13. Muller MF, Prasad PV, Bimmler D, et al. Functional
imaging of the kidney by means of measurement
of the apparent diffusion coefficient. Radiology
1994;193:711–5.
14. Siegel CL, Aisen AM, Ellis JH, et al. Feasibility of MR
diffusion studies in the kidney. J Magn Reson Imag-
ing 1995;5:617–20.
15. Ichikawa T, Haradome H, Hachiya J, et al. Diffusion-
weighted MR imaging with single-shot echo-planar
imaging in the upper abdomen: preliminary clinical
experience in 61 patients. Abdom Imaging 1999;
24:456–61.
16. Fukuda Y, Ohashi I, Hanafusa K, et al. Anisotropic
diffusion in kidney: apparent diffusion coefficient
measurements for clinical use. J Magn Reson Imag-
ing 2000;11:156–60.
17. Murtz P, Flacke S, Traber F, et al. Abdomen: diffu-
sion-weighted MR imaging with pulse-triggered
single-shot sequences. Radiology 2002;224:258–64.
18. Chow LC, Bammer R, Moseley ME, et al. Single
breath-hold diffusion-weighted imaging of the abdo-
men. J Magn Reson Imaging 2003;18:377–82.
19. Thoeny HC, De Keyzer F, Oyen RH, et al. Diffusion-
weighted MR imaging of kidneys in healthy volun-
teers and patients with parenchymal diseases: initial
experience. Radiology 2005;235:911–7.
20. Namimoto T, Yamashita Y, Mitsuzaki K, et al. Mea-
surement of the apparent diffusion coefficient in
diffuse renal disease by diffusion-weighted echo-
planar MR imaging. J Magn Reson Imaging 1999;
9:832–7.

Kim et al596
21. Xu Y, Wang X, Jiang X. Relationship between the
renal apparent diffusion coefficient and glomerular
filtration rate: preliminary experience. J Magn Reson
Imaging 2007;26:678–81.
22. Yildirim E, Kirbas I, Teksam M, et al. Diffusion-
weighted MR imaging of kidneys in renal artery
stenosis. Eur J Radiol 2008;65:148–53.
23. Chan JH, Tsui EY, Luk SH, et al. MR diffusion-weighted
imaging of kidney:differentiationbetween hydroneph-
rosis and pyonephrosis. Clin Imaging 2001;25:110–3.
24. Thoeny HC, Zumstein D, Simon-Zoula S, et al.
Functional evaluation of transplanted kidneys with
diffusion-weighted and BOLD MR imaging: initial
experience. Radiology 2006;241:812–21.
25. Hecht EM, Israel GM, Krinsky GA, et al. Renal
masses: quantitative analysis of enhancement with
signal intensity measurements versus qualitative
analysis of enhancement with image subtraction
for diagnosing malignancy at MR imaging. Radiol-
ogy 2004;232:373–8.
26. Grobner T. Gadolinium—a specific trigger for the
development of nephrogenic fibrosing dermopathy
and nephrogenic systemic fibrosis? Nephrol Dial
Transplant 2006;21:1104–8.
27. Sadowski EA, Bennett LK, Chan MR, et al. Nephro-
genic systemic fibrosis: risk factors and incidence
estimation. Radiology 2007;243:148–57.
28. Boyd AS, Zic JA, Abraham JL. Gadolinium deposi-
tion in nephrogenic fibrosing dermopathy. J Am
Acad Dermatol 2007;56:27–30.
29. Squillaci E, Manenti G, Di Stefano F, et al. Diffusion-
weighted MR imaging in the evaluation of renal
tumours. J Exp Clin Cancer Res 2004;23:39–45.
30. Cova M, Squillaci E, Stacul F, et al. Diffusion-
weighted MRI in the evaluation of renal lesions: pre-
liminary results. Br J Radiol 2004;77:851–7.
31. Yoshikawa T, Kawamitsu H, Mitchell DG, et al. ADC
measurement of abdominal organs and lesions us-
ing parallel imaging technique. AJR Am J Roent-
genol 2006;187:1521–30.
32. Zhang J, Tehrani YM, Wang L, et al. Renal masses:
characterization with diffusion-weighted MR imag-
ing—a preliminary experience. Radiology 2008;
247:458–64.
33. Israel GM, Bosniak MA. MR imaging of cystic renal
masses. Magn Reson Imaging Clin N Am 2004;12:
403–12, v.
34. Taouli B, Thakur R, Mannelli L, et al. Diffusion-
weighted MR imaging for characterization of renal
lesions: comparison with contrast-enhanced MR
imaging. Radiology; in press.
35. Silvera S, Oppenheim C, Touze E, et al. Spontaneous
intracerebral hematoma on diffusion-weighted
images: influence of T2-shine-through and T2-
blackout effects. AJNR Am J Neuroradiol 2005;26:
236–41.
36. Kim S, Jain M, Harris AB, et al. Characterization of
T1 hyperintense renal lesions: performance of diffu-
sion-weighted MR imaging compared to contrast-
enhanced MR imaging. Radiology, in press.
37. Jemal A, Siegel R, Ward E, et al. Cancer statistics,
2008. CA Cancer J Clin 2008;58:71–96.
38. Matsuki M, Inada Y, Tatsugami F, et al. Diffusion-
weighted MR imaging for urinary bladder carci-
noma: initial results. Eur Radiol 2007;17:201–4.
39. Yoshida S, Masuda H, Ishii C, et al. Initial experience
of functional imaging of upper urinary tract neo-
plasm by diffusion-weighted magnetic resonance
imaging. Int J Urol 2008;15:140–3.
40. Naik M, Hardie A, Chandarana H, et al. Diffusion-
weighted imaging for detection and staging of
urothelial neoplasms. ISMRM proceedings, 2008.