Embed Size (px)
Citation preview

Renal Structure & Functions
Dr. C.H. Lai
PT-RN-Human Biology
07-01-10
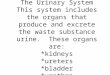
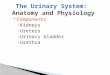
Urinary System Organs
Urinary System Organs: Kidneys
• Filter 200 liters of blood daily, allowing toxins, metabolic wastes, and excess ions to leave the body in urine
• Regulate volume and chemical makeup of the blood• Maintain the proper balance between water and salts,
and acids and bases• Produce renin to help regulate blood pressure and
erythropoietin to stimulate red blood cell production

Life Cycle of Red Blood Cells Other Urinary System Organs
• Urinary bladder – provides a temporary storage reservoir for urine
• Paired ureters – transports urine from the kidneys to the bladder
• Urethra – transports urine from the bladder out of the body
Internal Anatomy
Nephron
Internal Anatomy

The Nephron
• Nephrons are the blood-processing units that form urine, consisting of:• Glomerulus – a tuft of capillaries associated with a
renal tubule• Glomerular (Bowman’s) capsule – blind, cup-shaped
end of a renal tubule that completely surrounds the glomerulus
• Renal corpuscle – the glomerulus and its Bowman’s capsule
The Nephron
(Bowman’s capsule)
The Nephron
• Glomerular endothelium – fenestrated epithelium that allows solute-rich, virtually protein-free filtrate to pass from the blood into the glomerular capsule
Filtration Membrane
• Filter that lies between the blood and the interior of the glomerular capsule

Renal Blood Flow & Glomerular Filtration
Dr. C.H. Lai
PT-RN-Human Biology
07-01-10• Every nephron has two capillary beds
• Glomerulus• Peritubular capillaries
Capillary Beds of the Nephron• Each glomerulus
is: • Fed by an
afferent arteriole
• Drained by an efferent arteriole
• Vasa recta – long, straight efferent arterioles of juxamedullary nephrons
Capillary Beds of the Nephron
• Blood pressure in the glomerulus is high because:• Arterioles are high-resistance vessels• Afferent arterioles have larger diameters than efferent
arterioles• Fluids and solutes are forced out of the blood throughout
the entire length of the glomerulus
Vascular Resistance in Microcirculation
• Afferent and efferent arterioles offer high resistance to blood flow• Blood pressure declines from 95mm Hg in renal arteries to 8 mm Hg in renal
veins

Vascular Resistance in Microcirculation
• Resistance in afferent arterioles:• Protects glomeruli from fluctuations in systemic
blood pressure• Resistance in efferent arterioles:
• Reinforces high glomerular pressure• Reduces hydrostatic pressure in peritubular
capillaries
Juxtaglomerular Apparatus (JGA)
Juxtaglomerular Apparatus (JGA)• Where the distal tubule lies against the afferent /efferent
arteriole• Arteriole walls have juxtaglomerular (JG) cells
• Enlarged, smooth muscle cells • Have secretory granules containing renin• Act as mechanoreceptors
Juxtaglomerular Apparatus (JGA)• Macula densa
• Tall, closely packed distal tubule cells • Lie adjacent to JG cells • Function as chemoreceptors or osmoreceptors
• Mesanglial cells appear to control the glomerularfiltration rate

Mechanism of Urine Formation
• The kidneys filter the body’s entire plasma volume 60 times each day
• The filtrate:• Contains all plasma components except protein• Loses water, nutrients, and essential ions to become
urine• The urine contains metabolic wastes and unneeded
substances
Mechanism of Urine Formation
• Urine formation and adjustment of blood composition involves three major processes • Glomerular
filtration• Tubular
reabsorption• Secretion
Glomerular Filtration
• The glomerulus is more efficient than other capillary beds because:• Its filtration membrane is significantly more permeable• Glomerular blood pressure is higher • It has a higher net filtration pressure
• Plasma proteins are not filtered and are used to maintain oncotic pressure of the blood
NFP = HPg – (OPg + HPc)
HPg
OPg
HPc
Net Filtration Pressure (NFP)

Net Filtration Pressure (NFP)
• The pressure responsible for filtrate formation• NFP equals the glomerular hydrostatic pressure (HPg)
minus the oncotic pressure of glomerular blood (OPg) combined with the capsular hydrostatic pressure (HPc)
NFP = HPg – (OPg + HPc)
Glomerular Filtration Rate (GFR)
• The total amount of filtrate formed per minute by the kidneys
• Factors governing filtration rate at the capillary bed are:• Total surface area available for filtration• Filtration membrane permeability• Net filtration pressure
• Changes in GFR normally result from changes in glomerular blood pressure
Renal Tubular Transport
Dr. C.H. Lai
PT-RN-Human Biology
07-01-10
Tubular Reabsorption
• All organic nutrients are reabsorbed• Water and ion reabsorption is hormonally controlled• Reabsorption may be an active (requires ATP) or
passive process

Renal Transport – Tubular Reabsorption
• Passive diffusion - movement along the chemical and/or electrical gradient. e.g K+, Cl- and urea
Renal Transport – Tubular Reabsorption• Active transport - movement with the expenditure of
energy and always against a concentration gradient
• Na+ to ECF• K+ into cell• ATP-ase• Uses energy
• Na+ ECF→ peritubularcapillaries
• Reabsorption → blood
Primary Active Transport
Renal Transport – Mechansims• Secondary active transport - organic molecules such as glucose
and amino acids together with Na+ combine with a carrier at the luminal surface of the proximal tubule (symport)
Nonreabsorbed Substances
• Substances are not reabsorbed if they: • Lack carriers• Are not lipid soluble• Are too large to pass through membrane pores
• Urea, creatinine, and uric acid are the most important nonreabsorbed substances

Tubular Secretion
• Essentially reabsorption in reverse, where substances move from peritubular capillaries or tubule cells into filtrate
• Tubular secretion is important for:• Disposing of substances not already in the filtrate • Eliminating undesirable substances such as urea and
uric acid• Ridding the body of excess potassium ions• Controlling blood pH
Regulation of Volume & Osmolality of Body Fluids
Dr. C.H. Lai
PT-RN-Human Biology
07-01-10
• Drinking & eating provides water
• Kidney conserves water so output = intake
Body Water Balance
Figure : Water balance in the body
Osmolality
• Osmolality• The number of solute particles dissolved in 1L of
water• Reflects the solution’s ability to cause osmosis
• Body fluids are measured in milliosmols (mOsm)• The kidneys keep the solute load of body fluids
constant at about 300 mOsm• This is accomplished by the countercurrent mechanism

A Counter-Current Heat Exchanger
Countercurrent Mechanism
A V
Countercurrent Mechanism
How does an osmotic counter-current exchanger conserve osmolarity?
300 mOsm
1000 mOsm
H2O
H2O
solutes
solutes
H2O
H2O
solutes
solutes
1000 mOsm
bath
Solutes are quickly washed out of the bath.
1000 mOsm
300 mOsm
320 mOsm
H2O
solutes
H2O
solutes 1000
400 600 800
850640430
solutes
H2O
bathLoss of solutes from the bath is much slower.
Countercurrent Mechanism Loop of Henle

Loop of Henle Loop of Henle: Countercurrent Multiplier
• The descending loop of Henle:• Is relatively impermeable to
solutes• Is permeable to water
• The ascending loop of Henle:• Is impermeable to water • Actively transports sodium
chloride into the surrounding interstitial fluid
Countercurrent Mechanism• Dissipation of the medullary osmotic gradient is prevented
because the blood in the vasa recta equilibrates with the interstitial fluid
Countercurrent Exchanger: vasa recta
• The vasa recta is a countercurrent exchanger that:• Maintains the osmotic gradient• Delivers nutrient blood supply to the cells in the area

NaCl
NaClNaCl
NaCl
NaCl
NaCl
NaCl
NaCl
NaCl
NaCl
NaCl
active Na+ transport in thick ascending limb
passive NaClleakage from thin ascending limb
NaCl passes from exiting vasa recta blood to entering vasa recta blood (counter-current
exchange).
NaCl picked up from thick
ascending limb is distributed by vasa
recta to deeper medulla .
Countercurrent Mechanism Formation of Dilute Urine
• Filtrate is diluted in the ascending loop of Henle
• Dilute urine is created by allowing this filtrate to continue into the renal pelvis
• This will happen as long as antidiuretic hormone (ADH) is not being secreted
Formation of Dilute Urine
• Collecting ducts remain impermeable to water; no further water reabsorptionoccurs
• Sodium and selected ions can be removed by active and passive mechanisms
• Urine osmolality can be as low as 50 mOsm (one-sixth that of plasma)
Formation of Concentrated Urine
Collecting ducts in the deep medullary regions are permeable to urea

Formation of Concentrated Urine
• Antidiuretic hormone (ADH) inhibits diuresis• This equalizes the osmolality of the filtrate and the
interstitial fluid• In the presence of ADH, 99% of the water in filtrate is
reabsorbed• ADH-dependent water reabsorption is called
facultative water reabsorption• ADH is the signal to produce concentrated urine
Nephron Recycling: Overview
Figure: Osmolarity changes as fluid flows through the nephron
Regulation of Acid-Base Balance
Dr. C.H. Lai
PT-RN-Human Biology
07-01-10
Acid-Base Balance

Chemical Buffer Systems
• One or two molecules that act to resist pH changes when strong acid or base is added
• Three major chemical buffer systems • Bicarbonate buffer system• Phosphate buffer system• Protein buffer system
• Any drifts in pH are resisted by the entire chemical buffering system
Bicarbonate Buffer System
• A mixture of carbonic acid (H2CO3) and its salt, sodium bicarbonate (NaHCO3) (potassium or magnesium bicarbonates work as well)
• If strong acid is added:• Hydrogen ions released combine with the
bicarbonate ions and form carbonic acid (a weak acid) • The pH of the solution decreases only slightly
H2CO3 ↔ H+ + HCO3¯
Bicarbonate Buffer System
• If strong base is added:• It reacts with the carbonic acid to form sodium
bicarbonate (a weak base)• The pH of the solution rises only slightly
H2CO3 ↔ H+ + HCO3¯
Phosphate Buffer System
• Nearly identical to the bicarbonate system • Its components are:
• Sodium salts of dihydrogen phosphate (H2PO4¯), a weak acid
• Monohydrogen phosphate (HPO42¯), a weak base
• This system is an effective buffer in urine and intracellular fluid
H2PO4¯ ↔ HPO42¯ + H+

Protein Buffer System• Plasma and intracellular proteins are the body’s most
plentiful and powerful buffers• Some amino acids of proteins have:
• Free organic acid groups (weak acids) • Groups that act as weak bases (e.g., amino groups)
• Amphoteric molecules are protein molecules that can function as both a weak acid and a weak base
Physiological Buffer Systems
• The respiratory system regulation of acid-base balance is a physiological buffering system
• There is a reversible equilibrium between:• Dissolved carbon dioxide and water• Carbonic acid and the hydrogen and bicarbonate ions
CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3¯
Physiological Buffer Systems• When hypercapnia or rising plasma H+ occurs:
• Deeper and more rapid breathing expels more carbon dioxide
• Hydrogen ion concentration is reduced• Alkalosis causes slower, more shallow breathing, causing
H+ to increase
Renal Mechanisms of Acid-Base Balance
• Chemical buffers can tie up excess acids or bases, but they cannot eliminate them from the body
• The lungs can eliminate carbonic acid by eliminating carbon dioxide
• Only the kidneys can rid the body of metabolic acids (phosphoric, uric, and lactic acids and ketones) and prevent metabolic acidosis
• The ultimate acid-base regulatory organs are the kidneys