Embed Size (px)
Citation preview

Diffusion Magnetic Resonance as the Basis of Novel
Biomarkers Using Multidimensional Statistics
in the Brain
PhD thesis
Gyula Gyebnár
János Szentágothai Doctoral School
Semmelweis University
Supervisor: Lajos Rudolf Kozák MD, PhD
Official reviewers: András Jakab, MD, PhD
Pál Kaposi Novák, MD, PhD
Head of the Final Examination Committee:
Kinga Karlinger, MD, PhD
Members of the Final Examination Committee:
Miklós Krepuska, MD, PhD
Regina Deák-Meszlényi, PhD
Budapest
2020

Table of contents
Table of contents 2
List of abbreviations 6
I. Introduction 8
1. Foreword 8
2. Diffusion Magnetic Resonance Imaging 10
2.1 Basics of diffusion MRI 10
2.2 Diffusion MRI approaches in neuroimaging 12
2.2.1 Diffusion weighted imaging 13
2.2.2 Diffusion tensor imaging 14
2.2.3 Outlook on dMRI methods beyond DTI 19
2.2.4 Imaging, correction, and data processing in dMRI 22
3. Statistics in brain MRI studies 24
3.1 Univariate statistics 24
3.2 The problem of multiple comparisons 25
3.3 Multivariate approaches 26
4. The Mahalanobis‒distance 28
4.1 Definition 28
4.2 The Mahalanobis‒distance in neuroimaging 29
4.3 Statistical inference based on critical values 30
5. Research topics – Clinical importance 32
5.1 Mild Cognitive Impairment 32
5.1.1 MRI diagnostics of MCI 32
5.1.2 The role of DTI in MCI diagnostics 33
5.2 Drug resistant epilepsies (DREs) 33
5.2.1 DTI in the diagnosis of epilepsy 34
II. Aims 35
1. DTI and Mild Cognitive Impairment 35
2. Mahalanobis‒distance in MCD lesion detection 35
III. Materials and Methods 36
1. DTI and Mild Cognitive Impairment 36

3
1.1 Study data and Participants 37
1.2 Preprocessing and diffusion tensor fitting 40
1.3 Voxelwise analysis 40
1.3.1 Voxelwise correlation analysis 41
1.3.2 Voxel‒based between group statistical analysis 42
1.3.3 Visualization 43
1.4 ROI‒based statistics 43
1.4.1 ROI‒based correlation analyses and between‒group comparisons 43
1.4.2 ROI‒based logistic regression analysis for a combined cortical thickness
and DTI based differentiation between study groups 43
2. Mahalanobis‒distance in MCD lesion detection 45
2.1 Study data and participants 45
2.2 Data processing 46
2.3 Independent automatic evaluation of MCDs 48
2.4 Mahalanobis‒distance related calculations 48
2.5 Simulations 49
2.5.1 Simulations with Gaussian distributions 49
2.5.2 Simulations with real eigenvalues 52
2.6 Leave‒one‒out examination of controls 53
2.6.1 Cluster description based on tissue probability maps (TPMs) 54
2.7 Representative cases of MCDs 55
IV. Results 56
1. DTI and Mild Cognitive Impairment 56
1.1 Voxelwise analyses 56
1.1.1 Voxelwise correlation analysis 56
1.1.2 Voxelwise ANOVA and between-group differences 60
1.2 ROI‒based analyses 64
1.2.1 ROI‒based correlations with the results of the neuropsychology tests 64
1.2.2 ROI‒based between group differences 66
1.3 ROI‒based logistic regression analysis: combined cortical thickness and DTI‒
based differentiation between study groups 67
1.3.1 Differentiation between aMCI subjects and healthy controls 68
1.3.2 Differentiation between naMCI subjects and healthy controls 72

4
1.3.3 Differentiation between aMCI and naMCI subjects 76
2. Mahalanobis‒distance in MCD lesion detection 80
2.1 SMVND simulations 82
2.1.1 False Positives 82
2.1.2 True positive rates and hit rates 82
2.2 Real Eigenvalue simulations 84
2.2.1 False Positives 84
2.2.2 True positive rates and hit rates 84
2.3 Real data examinations 87
2.3.1 Leave‒one‒out analysis of controls 87
2.3.2 Patient Examination 89
V. Discussion 91
1. DTI and Mild Cognitive Impairment 91
1.1 Functional‒structural correlations 91
1.2 Impairments in aMCI patients compared to naMCI patients and healthy controls
93
1.3 Impairments in naMCI patients compared to control subjects 94
1.4 Differentiation between study groups by logistic regression 94
1.5 On the value of DTI measurements in MCI and AD 95
1.6 Limitations of the study 96
2. Mahalanobis‒distance in MCD lesion detection 97
2.1 Multidimensional approaches 97
2.2 On information sources and dimensionality considerations 98
2.3 Simulation results 99
2.4 Leave‒one‒out examination of controls 101
2.5 Patient examinations 101
2.6 Limitations 105
VI. Conclusions 107
1. DTI and Mild Cognitive Impairment 107
2. Mahalanobis‒distance in MCD lesion detection 107
3. General conclusions 108
VII. Summary 109

5
VIII. Összefoglalás 110
References 111
List of publications 132
1. Articles related to the thesis 132
2. Other articles 132
Acknowledgements 133
Reprints of publications related to the thesis 134
Supplementary material 135

6
List of abbreviations
2D Two Dimensional
3D Three Dimensional
3T Three Tesla
ACE Addenbrooke’s Cognitive
Examination
AD Alzheimer’s Disease
ADC Apparent Diffusion Coefficient
AFROC Alternative Free-Response
Receiver-Operator Characteristics
aMCI Amnestic Subtype of Mild
Cognitive Impairment
ANOVA Analysis of Variance
AUC Area Under the Curve
BOLD Blood Oxygen Level
Dependent (signal)
CHARMED Composite Hindered and
Restricted Model of Diffusion
CNR Contrast‒to‒Noise Ratio
CNS Central Nervous System
CSF Cerebrospinal Fluid
CSD Constrained Spherical
Deconvolution
D2 Squared Mahalanobis‒Distance
DARTEL Diffeomorphic Anatomical
Registration using Exponentiated Lie
Algebra
DDF Diffusion Displacement Function
DKI Diffusional Kurtosis Imaging
dMRI Diffusion Magnetic Resonance
Imaging
DNT Disembryoplastic Neuroepithelial
Tumor
DRE Drug Resistant Epilepsy
DSI Diffusion Spectrum Imaging
DTI Diffusion Tensor Imaging
DWI Diffusion Weighted Imaging
EPI Echo Planar Imaging
FA Fractional Anisotropy
FCD Focal Cortical Dysplasia
FDR False Discovery Rate
FLAIR Fluid Attenuated Inversion
Recovery
fMRI Functional Magnetic Resonance
Imaging
fODF fiber Orientation Distribution
Function
FOV Field Of View
FPR False Positive Rate
FWE Family‒Wise Error Rate
FWHM Full Width at Half Maximum
GLM General Linear Model
GM Grey Matter
HARDI High Angular Resolution
Diffusion Imaging
HTP Heterotopia
HME Hemimegalencephaly
JHU Johns Hopkins University
LEAT Long‒Term Epilepsy‒
Associated Tumor
MD Mean Diffusivity

7
MCI Mild Cognitive Impairment
MCD Malformation of Cortical
Development
MNI Montreal Neurological Institute
MMSE Mini Mental State
Examination
MRI Magnetic Resonance Imaging
naMCI Non‒Amnestic Subtype of
Mild Cognitive Impairment
NODDI Neurite Orientation Dispersion
and Density Imaging
PAL Paired Associates Learning
PET Positron Emission Tomography
PFGSE Pulsed Field Gradient Spin
Echo
PMG Polymicrogyria
QSI q‒Space Imaging
RAVLT Rey Auditory Verbal
Learning Test
RD Radial Diffusivity
RESTORE Robust Estimation of
Tensors by Outlier Rejection
ROC Receiver‒Operator
Characteristics
ROI Region of Interest
SD Standard Deviation
SE Spin Echo
SMVND Standard Multivariate Normal
Distribution
T1 and T2 Characteristic Relaxation
Time for Longitudinal and Transverse
Magnetization
TBI Traumatic Brain Injury
TBSS Tract‒Based Spatial Statistics
TFCE Threshold‒Free Cluster
Enhancement
TE Echo Time
TI Inversion Time
TPM Tissue Probability Map
TPR True Positive Rate
TPRB True Positive Rate Binary
TR Repetition Time
VBA Voxel‒Based Analysis
VBM Voxel‒Based Morphometry
VLOM (Verbal Fluency + Language
Score / Orientation + Memory Score)
Ratio in the ACE
VLPFC Ventrolateral Prefrontal
Cortex
WM White Matter

8
I. Introduction
1. Foreword
The development of magnetic resonance imaging (MRI) in the last two decades have
propelled the investigation of the central nervous system (CNS) at an unprecedented rate.
With the increasing availability of high‒quality equipment and the inventions of novel
imaging and processing techniques, MRI has been pushed to the forefront of brain
research, facilitating several large‒scale initiatives, such as the Human Connectome
Project [1-3], the Human Brain Project [4], or the UK Biobank Project [5], and imaging
was also given due attention in the Hungarian Brain Research Program (NAP).
The ever‒growing amount of multimodal brain imaging data, especially with the
introduction of diffusion and functional MRI, has been driving the development and use
of novel processing and statistical methods. Since different modalities, even distinct MR
contrast mechanisms, provide complementary information on brain structure and
function, methods combining data from various approaches could aim for more accuracy
and sensitivity by leveraging their advantages.
The work behind the present Thesis was aimed at developing methods and new
biomarkers using combinations of state of the art neuroimaging techniques with diffusion
MRI. Although the machine learning‒based methods for image processing and analysis
(some of which are referred to with the alluring term ‘radiomics’), that received an
exponentially growing interest in the past few years are promising optimized, data‒based,
automated feature selection, their general use is still hampered by, among other factors,
the need for vast amounts of well‒annotated training data. The author firmly believes that
knowledge‒driven studies addressing specific research questions, such as the ones
presented in this Thesis, still hold merit, at least by forming basis for and interpreting the
results of such endeavors.
In the first study of the thesis, conventional whole brain two sample parametric
statistics and correlation analyses, followed by subsequent white matter region‒level
analyses were used to identify the brain structures where mild cognitive impairment
inflicts substantial alterations on the diffusion profile, and measurements from these

9
structures were fed into stepwise logistic regression. Our results demonstrated that
combining volumetry measurements from anatomical scans with robust region‒level
diffusion tensor metrics significantly aids distinguishing patients from healthy subjects,
and improves the differentiation between amnestic and non‒amnestic subtypes of mild
cognitive impairment even more.
In the second study a novel approach was proposed and demonstrated for single
subject whole brain voxel‒level analyses, based on the squared Mahalanobis‒distance
with analytically derived critical values. The problem of identifying epilepsy‒related
structural abnormalities was implemented as a data‒driven detection problem, treating
diffusion tensor eigenvalues from lesion voxels as outliers compared to the distribution
derived from healthy controls. The expected detection rate and sensitivity to different
effect strengths and lesion volumes was explored through simulations, and verified in
select cases with malformations of cortical development.

10
2. Diffusion Magnetic Resonance Imaging
2.1 Basics of diffusion MRI
Diffusion magnetic resonance imaging (dMRI) is a general term referring to a group
of methods widely used for the non‒invasive examination of biological samples and
porous materials [6-8]. The term diffusion in dMRI refers to the random thermal motion
of water molecules in the extracellular space, described by Einstein’s theory: the
ensemble average translation is proportional to the elapsed time, and the ratio is called
the diffusion coefficient:
< (𝒓′ − 𝒓)2 >= 6𝐷𝑡 (𝐸𝑞. 1)
By using spatially varying magnetic fields (referred to as diffusion encoding
gradients), the magnetic resonance (MR) signal can be made sensitive to the microscopic
motion of water molecules [9, 10]. An ‘encoding gradient’ means that the magnetic field
component parallel to the polarizing field (B0) changes linearly across the sample space.
This is achieved by generating additional magnetic fields much smaller than B0, using
coils with special geometry. The gradient of the parallel component, denoted as g,
describes the change in magnetic field along the direction of the pulsed magnetic field.
By employing the encoding gradient, the Larmor frequencies (ω) of the nuclear magnetic
spins of water molecules (at coordinates r) also vary linearly along the direction of g:
𝜔(𝒓) = 𝛾𝐵0 + 𝛾𝒈 ∙ 𝒓 (𝐸𝑞. 2)
where γ is the gyromagnetic ratio. The use of the gradient over an evolution time t
results in an accumulated phase shift dependent on the position: 𝛥𝜑 = exp (𝑖𝛾𝒈 ∙ 𝒓𝑡).
In practice, most diffusion‒weighted MR sequences follow the Stejskal‒Tanner
encoding scheme [11] with a spin echo (Fig 1).

11
Fig 1 The Stejskal‒Tanner diffusion encoding scheme
Two identical diffusion encoding gradients (g) are used, with pulse length δ and diffusion time Δ. The 180°
RF pulse inverts the phase shift accumulated during the first gradient, thereby the second gradient
effectively rewinds the phases for stationary spins, but displacement along the direction of the gradient
results in remaining phase error.
Diffusion encoding is achieved by two identical pulsed gradients preceding and
following a 180° spin‒echo (SE) pulse. The SE‒pulse inverts the phase shift resulting
from the first gradient, so the second one completely recovers the phase for stationary
spins. For moving spins, with displacement R along the direction of the gradients, the
remaining phase error is Φ = 𝛾𝐺𝛿𝑅, with gradient pulse strength G = |g|, and pulse length
δ. The signal attenuation in a pulsed field gradient spin echo (PFGSE) sequence with
short, rectangular gradient pulses and echo time TE, as shown in [11], is:
𝐴(𝑇𝐸) = exp [−𝛾2𝐺2𝐷𝛿2 (𝛥 −𝛿
3)] (𝐸𝑞. 3)
Parameters describing the diffusion encoding are generally merged in order to
simplify the equation, defining the so‒called b‒value:
𝑏 = 𝛾2𝐺2𝛿2 (𝛥 −𝛿
3) (𝐸𝑞. 4)

12
As diffusion means the flux of particles through a surface during a given period of
time, its’ dimension is in the form of [area/time]. In order for the exponent –bD to be
dimensionless, b is expressed as [time/area]. In practice, b‒values are given in units of
𝑠/𝑚𝑚2, in the range of 0 – 10000. From the attenuated signal (Sb) corresponding to a
given b‒value, and a reference measurement (S0) without diffusion encoding, the apparent
diffusion coefficient (ADC) along the direction of the gradient can be calculated:
𝐴𝐷𝐶(𝑏) =ln (
𝑆𝑏
𝑆0)
𝑏(𝐸𝑞. 5)
It is important to note, that the mono‒exponential signal attenuation in (Eq.3) is only
accurate for rectangular gradient pulses and free diffusion. In practice, gradient shapes
are trapezoidal and the b‒values given by MR scanners are calculated slightly differently,
accounting for the finite rise times and the auxiliary effects of imaging gradients as well.
Free diffusion means that the displacement of water molecules can be described as a
simple Gaussian process (i.e. the probability distribution of spin displacement can be
described with a three dimensional Gaussian function). Strictly, this is only true for pure,
homogenous liquid samples with infinite size, but the approximation also holds for water
molecules in the extracellular space with most b‒values used in human studies, except for
those specifically chosen to measure the non‒Gaussian behavior of the dMRI signal (see
subsection 2.2.3).
2.2 Diffusion MRI approaches in neuroimaging
Even though diffusion only results in displacements on the microscopic scale, the
degree, at which water molecules can move in the three‒dimensional space of the
extracellular environment may be hindered due to the physical arrangement of obstacles
in one, two, or all three directions, resulting in restricted, and in many cases anisotropic
diffusion [12]. Therefore, the measured signal attenuation in biological samples reflects
properties of tissue microstructure [6-8]. Measurement and data processing approaches
can be described according to the level of information extracted about the diffusion
pattern. By measuring ADC‒values in several directions, one can define the diffusion
profile as a three dimensional surface describing the orientation distribution of the
observed displacement in each voxel (Fig 2).

13
Fig 2 Diffusion profiles of several voxels in the deep parieto‒occipital white matter
Apparent diffusion coefficients in each measured direction can be used to construct 3D surfaces, visualizing
the orientation distribution of the observed mean displacement of extracellular water molecules. The
difference between white matter structures with a single main orientation (e.g. the callosal fibers on the
middle on the left side), with two or three orientations (on the bottom in the middle and the right side), in
gray matter with no clear maxima (lower left corner), and in the cerebrospinal fluid (CSF ‒ upper left
corner) can be measured and visualized.
2.2.1 Diffusion weighted imaging
The simplest approach of dMRI, called diffusion weighted imaging (DWI), quickly
gained interest in the clinical field for its superior sensitivity detecting cerebral ischemia
through the restricted diffusion signal of cytotoxic edema, appearing in minutes after the
occlusion [13]. DWI has also been proven useful in onco‒radiology. In DWI, diffusion‒
encoding gradients are applied separately in three perpendicular directions; restricted
diffusion can be identified as high signal intensity after averaging the corresponding
images. Due to averaging, directional, and therefore anisotropy information is not
extracted; DWI can be viewed as measuring only the volume enclosed by the diffusion
profile (with the three orthogonal directions, the corresponding surface is a cuboid). By

14
acquiring a reference image and calculating the ADC‒values from the averaged images,
other biological and physics‒related phenomena (e.g. differences in T2‒relaxation times)
can be disentangled from the effects of the diffusion process.
2.2.2 Diffusion tensor imaging
The most widely known (and simplest) technique, capable of handling anisotropy
information, used in both clinical neuroradiology and for innumerable research questions
about the CNS, is diffusion tensor imaging (DTI) [14, 15]. Since DTI was the method of
choice in both research projects of the present Thesis, this section contains a detailed
explanation of the approach, with emphasis on its strengths and limitations.
In the DTI representation, the 3D Gaussian model uses a 3‒by‒3 tensor D to describe
diffusion anisotropy, instead of a scalar ADC:
𝑫 = [
𝐷𝑥𝑥 𝐷𝑥𝑦 𝐷𝑥𝑧
𝐷𝑦𝑥 𝐷𝑦𝑦 𝐷𝑦𝑧
𝐷𝑧𝑥 𝐷𝑧𝑦 𝐷𝑧𝑧
]
Using the observed properties of molecular diffusion, the tensor describing the
physical process must be real and symmetric, therefore Dxy = Dyx, Dxz = Dzx, and
Dyz = Dzy. By writing the diffusion encoding b‒vectors in matrix format, and utilizing this
symmetry, (Eq.5) takes the following form for DTI:
ln (𝑆𝒃
𝑆0) = −(𝑏𝑥𝑥𝐷𝑥𝑥 + 2𝑏𝑥𝑦𝐷𝑥𝑦 + 2𝑏𝑥𝑧𝐷𝑥𝑧 + 𝑏𝑦𝑦𝐷𝑦𝑦 + 2𝑏𝑦𝑧𝐷𝑦𝑧 + 𝑏𝑧𝑧𝐷𝑧𝑧) (𝐸𝑞. 6)
The six unknowns in (Eq. 6) means that at least six measurements with diffusion
encoding in non‒collinear directions are required in a dMRI measurement indented for
DTI processing. In typical DTI‒studies 30 – 40 directions are used [16] and tensor fitting
usually forgoes simple least squares methods; iterative approaches with outlier rejection
strategies [17] benefit from the higher number of measurements.
This representation means that the diffusion profile is modeled as an ellipsoid in each
voxel (Fig 3), which is understandable after the eigenvalue decomposition of the tensors:

15
𝑫 = [
─ 𝒗𝟏 ── 𝒗𝟐 ── 𝒗𝟑 ─
] [
𝜆1 0 00 𝜆2 00 0 𝜆3
] [| | |
𝒗𝟏 𝒗𝟐 𝒗𝟑
| | |] (𝐸𝑞. 7)
The lengths of the ellipsoids half‒axes are the eigenvalues (λ1, λ2, λ3) of D and the
corresponding eigenvectors (v1, v2, v3) determine their orientation.
The principal eigenvector (v1) signals the direction in which the measured diffusion
displacement is largest and is used by convention for color coding the voxels: right‒left
direction is red, anterior‒posterior is green, superior‒inferior is blue, and their mixtures
represent in‒between orientations (Fig 3).
Fig 3 Diffusion ellipsoids in the deep parieto‒occipital white matter
The tensor representation in DTI means that the 3D diffusion displacement profile is approximated as an
ellipsoid in each voxel. This approach handles the anisotropy and directionality information, measured in
dMRI, but fails to resolve the geometry of crossing fibers and to capture the signal behavior of non‒
Gaussian diffusion processes.

16
Diffusion tensor data can be utilized with two distinct approaches: the orientation
information facilitates tractography, while the eigenvalues can be used to derive
anisotropy and diffusivity‒related measures that reflect tissue microstructure.
In tractography, neighboring voxels are linked sequentially, following the ellipsoids
angulation, to form fiber tracts (i.e. supposed axonal bundles in the white matter of the
brain and spinal cord), using interpolation with sub‒voxel step size [18]; methods similar
to those describing flow patterns in fluid dynamics.
Tracts are identified through the following logic: so‒called seeds voxels act as starting
points, and tracts are propagated while considering limits on anisotropy and geometric
parameters (e.g. angulation). There are two distinct approaches for propagation:
deterministic [19], when a single tract follows the direction determined by v1 and
probabilistic [20, 21], when a large number of tracts are observed simultaneously,
sampling the diffusion profile for the selection of propagation direction in each step
following a Monte Carlo procedure. Tractography results have been used in innumerable
clinical and research applications, e.g. studying specific white matter regions for
neurosurgical planning [22] and in developmental studies [23, 24]. By defining seed
points throughout the entire brain parenchyma, whole brain tractography (Fig 4) enables
network‒studies with quantitative measures on connectivity between different structural
or functional regions [25, 26].

17
Fig 4 Result of whole brain, deterministic DTI tractography on a healthy volunteer
Conventional color‒coding, defined by the direction of the primary eigenvector: right‒left direction is red,
anterior‒posterior is green, and superior‒inferior is blue
Although after its introduction, DTI‒based tractography gained substantial interest, it
has been shown that its approach of identifying one primary direction per voxel is overly
simplistic, since the vast majority of white matter voxels contain two or more distinct
fiber bundles [27]. A brief overview on the more recent approaches surpassing these
limitations is given in subsection 2.2.3.
DTI data has also been used to probe tissue microstructure through rotationally
invariant scalar metrics, derived from the tensor eigenvalues [28]. The most well‒known
are the diffusivity measures and fractional anisotropy (FA). The first eigenvalue,
representing diffusion strength along the primary direction, is usually referred to as axial
diffusivity. Following the same logic, the arithmetic mean of λ2 and λ3 is radial diffusivity
(RD), measuring diffusion perpendicularly to the main direction; and the average of all

18
three is mean diffusivity (MD), which can be interpreted similarly to the ADC‒value in
DWI, but, with the high number of measurements and subsequent model‒fitting, is less
prone to imaging errors and noise. FA measures diffusion anisotropy in the voxel in the
range [0, 1], with FA = 0 representing isotropic, FA = 1 perfectly anisotropic diffusion.
Defining equations for the above described diffusivity measures and FA are as follows:
𝑅𝐷 =𝜆2+𝜆3
2; 𝑀𝐷 =
𝜆1+𝜆2+𝜆3
3; 𝐹𝐴 = √
3
2
(𝜆1−𝑀𝐷)2+(𝜆2−𝑀𝐷)2+(𝜆3−𝑀𝐷)2
𝜆12+𝜆2
2+𝜆32
A vast number of DTI‒based studies have used these metrics as indicators of
neuropathological progress with popular interpretations for various findings. FA is
generally viewed as a measure of fiber coherence in the white matter (WM), and has been
shown to increase with brain maturation [29], supposedly reflecting axon myelination.
The same process results in concordantly observed decreases in MD and RD. On the other
hand, neurodegenerative diseases has been shown to inflict opposing changes in white
matter: reduced FA and increased RD, possibly indicating demyelination [30]. Decreased
axial diffusivity has also been confirmed in cases with axonal damage [31]. More details
and examples regarding DTI‒related findings and interpretations concerning our research
topics, i.e. mild cognitive impairment and malformations of cortical development, are
given in subsections 5.1.2 and 5.2.1.
The straightforward interpretations and seemingly clear connections between various
pathological processes and the observed changes in these scalar parameters made DTI
popular in the field of neuroimaging, but limitations of the tensor representation also stand
for such microstructural applications, and must be considered when discussing highly
diverse or even controversial findings. These limitations stem from the fact that scalar
metrics are calculated from the volume‒averaged signal attenuation, which reflects the
mixed behavior of the various contents of voxels. A simple example is when a voxel
contains two perpendicular fiber populations, and the demyelination of one results in
increasing FA [32]. Such considerations do not necessarily undermine past or novel
findings using the DTI approach, but instead demonstrate the limits on the complexity of
processes it can interpret.

19
With the various diffusivity and anisotropy measures calculated from the same three
eigenvectors, deciding which of them are of interest in any given study has also been a
highly debated topic, especially considering the problem of multiple comparisons. In [33],
the second article behind this thesis, we proposed a novel and more straightforward
approach for statistical evaluation of DTI data that works with the raw eigenvalues
themselves and utilizes all of the scalar information in the diffusion tensor using
multidimensional statistics.
2.2.3 Outlook on dMRI methods beyond DTI
Several, more complex methods have been proposed to surpass the above described
limitations of DTI [34]; the common prerequisite for all is the need for collecting more
data, i.e. more diffusion encoding directions and strengths [35]. For the complete
description of the three dimensional diffusion displacement function, especially the non‒
monoexponential signal attenuation at high b‒values, the so‒called q‒space imaging
formalism was introduced [36]. The q‒vector describes the encoding strength, similarly
to the previously described b‒vector: 𝒒 = 𝜸𝜹𝒈/2𝜋, and can be used to describe the
Fourier‒relationship between signal attenuation (A(Δ, 𝐪)) and the average displacement
function (�̅�(𝑹, 𝛥)) for given mixing time Δ and net displacement R:
A(Δ, 𝐪) = ∫ �̅�(𝑹, 𝛥) exp(𝑖2𝜋𝒒 ∙ 𝑹) 𝑑𝑹 (𝐸𝑞. 8)
In theory, the displacement function itself can thus be measured by sampling the
whole of q‒space in a Cartesian fashion and subsequently applying the three dimensional
Fourier‒transform ‒ analogously to the sampling and reconstruction of k‒space in MR
image formation. Such a measurement, however, would require short gradient pulses that
cannot be fully achieved with clinical scanners, and total scan times that are not tolerable,
even to highly motivated subjects. Therefore, complete q‒space imaging (also referred to
as diffusion spectrum imaging – DSI [37]) has only been seldom applied in human studies
[38], but several, more or less simplified approximations has been proposed, which may
all be illustrated in the q‒space formalism (Fig 5).

20
Fig 5 The q‒space sampling schemes of different dMRI methods
A: Diffusion spectrum imaging (DSI) aims to sample the whole q‒space to reconstruct the complete
diffusion displacement function (DDF). B and C: with less demanding scan times, q‒space imaging (QSI)
resolves displacement along one and three (or more) directions. D: Diffusion weighted imaging (DWI)
samples only four points in q‒space (one along each main axis plus the origin). E: a typical measurement
for diffusion tensor imaging (DTI) essentially means the sampling of a half‒sphere (shell) in q‒space and
the origin. F: the majority of recent dMRI processing methods use data with one or multiple q‒shells
(multiple b‒values) along many encoding directions; common terms are q‒ball imaging (QBI), or high
angular resolution diffusion imaging (HARDI).
With measurements along one or several axes with different q‒values (Fig 5, panels
B and C), the diffusion displacement function (DDF) for the corresponding direction(s)
can be reconstructed. This model‒free approach, called q‒space imaging (QSI) has been
used in examining certain diseases of the central nervous system, e.g. multiple sclerosis
[39, 40]. From the q‒space sampling patterns, it is evident how little of the available
information is collected in conventional DWI (Fig 5, panel D) and even in typical
measurements for DTI (Fig 5, panel E).

21
With technical and methodological improvements, such as parallel imaging and, more
recently, simultaneous multi‒slice imaging, the acquisition time needed for a single whole
brain image has been substantially reduced, enabling tolerable scan times for high angular
resolution (typically around 60 – 130 directions) and multi‒shell dMRI data [41-43], with
b‒values in the order of 0 – 10000 𝑠/𝑚𝑚2 [44] (Fig 5 panel F). The term ‘high angular
resolution diffusion imaging’ (HARDI) became generally accepted for such
measurements over the last two decades [45], and numerous processing approaches and
models were proposed leveraging the increased quality and quantity of information.
The higher number of encoding directions facilitates higher order fitting methods that
can resolve complex fiber geometry (e.g. crossing fibers) in tractography. Examples of
such methods are Q‒ball imaging [46] (the name referencing the fact that measurements
with a single b‒value along several directions correspond to a sphere or shell in q‒space),
or the more recent and currently most popular constrained spherical deconvolution (CSD)
approach [47, 48], in which the fiber orientation distribution function (fODF) is
reconstructed using symmetrical spherical harmonic functions.
With at least three different b‒values or even more complex encoding schemes, tissue
microstructure can be described more accurately, as well. A relatively simple extension
to DTI is diffusional kurtosis imaging (DKI) that requires at least three different b‒values
(e.g. 0, 1000, and 2000 𝑠/𝑚𝑚2) and is able to separate multiple water compartments by
quantifying the non‒Gaussian behavior of the diffusion signal [49]. Several model‒based
methods has also been proposed, such as the straightforward biexponential model [50],
or geometric models using ensembles of spheres, cylinders, ellipsoids, and planes to
describe the microstructural environment of neural tissue, with or without exchange of
water molecules between various compartments. A few notable examples are
CHARMED [51], NODDI [52], and the diffusion tensor distribution approach by
Szczepankiewicz et al. [53].
Although in both papers providing the basis of this theses the processing of dMRI
data was performed with DTI, the proposed multidimensional statistical approaches are
also applicable when working with more advanced methods, yielding more sophisticated
descriptions of tissue microstructure or connectivity.

22
2.2.4 Imaging, correction, and data processing in dMRI
Image formation for dMRI acquisitions is a complex problem since several conflicting
requirements have to be met simultaneously. The use of the diffusion sensitizing gradients
and the need for adequate mixing time demands longer echo times (in the order of
100 ms), which requires a spin echo (SE) based technique. Conventional SE, or fast SE
sequences would be preferential for their high signal to noise ratio, excellent image
contrast, and since they are mostly free form geometric distortions, but their use is
inadequate for multiple reasons.
First, the diffusion weighting brings a new set of steps into the pulse sequence that
needs to be performed for each k‒space line; this would naturally lead to intolerable
acquisition times. More importantly, the diffusion sensitizing gradients cause random,
spatially varying phase differences over the field of view (FOV), therefore multi‒shot
techniques would be tainted by these phase errors between k‒space lines, resulting in
uncontrollable image ghosting and signal voids. Thus, the need for a single‒shot imaging
approach is evident; historically the most popular of such sequences has been echo planar
imaging (EPI) [54].
In EPI, all the two dimensional (2D) k‒space data is read after a single excitation,
thereby diffusion weighting only needs to be performed once for each slice, facilitating
short acquisition times and ghost‒free images. On the other hand, single‒shot EPI has
several limitations and inherent artefacts that need to be acknowledged and/or corrected.
Since the whole k‒space is to be acquired in one readout, the number of phase encoding
steps, therefore spatial resolution is limited: typical dMRI acquisitions for whole brain
imaging achieve 2 mm isotropic voxel size by the aid of parallel imaging or partial Fourier
techniques.
The consecutive reading of k‒space lines leads to the accumulation of phase errors,
resulting in distortions along the phase encoding direction. These errors are most severe
in brain regions with strong variations in magnetic susceptibility, for example, around the
edges of the frontal and temporal lobes.

23
Furthermore, the strong diffusion sensitizing gradients often induce eddy currents in
the gradient coils and other conductive elements of the MRI scanner. These eddy currents
generate spatially and temporally varying magnetic fields that could taint the EPI readout,
resulting in shifting, shearing, or scaling of the image, visible over the whole FOV.
These image distortions, as well as other types of artefacts, such as insufficient fat
suppression, ghosting from timing errors, patient motion, gradient nonlinearities etc. all
lead to inaccuracies in dMRI processing, hindering all types of inference [55].
Fortunately, most systemic errors can be aided to some degree and typical dMRI
processing pipelines usually include corrections, preferentially also conserving the
directional information of the diffusion measurement while performing various spatial
transformations on the data [56]. By using the non‒diffusion weighted (b = 0) image(s)
as reference, distortions caused by eddy‒currents or patient motion can be mitigated
through linear and non‒linear transformations. If an additional image, preferentially a
high‒resolution, T1‒weighted, anatomical scan is available in the processing pipeline, it
can be used as a target for registration in order to correct susceptibility and EPI‒related
distortions.
With sophisticated interpolation approaches, the description of tissue microstructure
and tractography can even benefit from the higher resolution [57]. Both studies of the
present thesis leveraged this and a further advantage of this approach: the spatial
correspondence between dMRI and anatomical data enables high performance
coregistration between subjects and identification of various brain regions by using
methods that were developed for anatomical scans [58].

24
3. Statistics in brain MRI studies
3.1 Univariate statistics
Since the inception of brain MRI, numerous approaches has been employed to utilize
its superior image quality and various contrast mechanisms for studying brain structure,
morphology, maturation, and the effects of various diseases. The simplest methods
measure the size or volume of specific structures, e.g. the hippocampus and either
compare it between individuals or cohorts of different diseases [59, 60] and healthy
control subjects; or correlate it with specific, often neuropsychology‒related measures
[61]. Information about tissue microstructure, e.g. average DTI scalar metrics can also be
extracted from manually or automatically delineated regions of interest (ROIs), and
compared with conventional parametric or non‒parametric tests [62].
Explorative methods also emerged for identifying systemic effects throughout the
brain. Structural and functional atlases have been proposed as the extension of the ROI‒
based approach, yielding automated labeling of white [63] or gray matter structures [64].
In conjunction with the advances in processing functional MRI data, standard coordinate
systems gained wide acceptance for identifying brain structures: so called template
spaces, of which the most well‒known were the single subject – based Talairach–space
[65, 66] and the Montreal Neurological Institute (MNI) template [67], the latter created
from the average of the structural images from hundreds of subjects. Nowadays, the latter
became almost exclusively used, being the default coordinate system of the two most
popular MRI processing software: FSL [68] and SPM [69].
Templates are used by spatially registering the individual’s data through linear and
non‒linear volumetric transformations [70, 71], and the resulting spatial correspondence
across subjects not only means that the structures can be labeled automatically with the
use of atlases, but also facilitates statistical inference on the voxel level. Such methods
are called voxel‒based analysis (VBA) or, particularly, when working with measures
describing gray matter structure, voxel‒based morphometry (VBM) [72]. Along the VBA
methods that work with scalar values, other approaches have also been proposed to utilize
the information of the spatial deformations called deformation‒based morphometry [73]
and tensor‒based morphometry [74, 75].

25
In cohorts with certain diseases or specific age groups, the widely used templates may
not be accurate, as they were derived from images of healthy adult brains. Such could be
the case e.g. with the atrophied GM of the elderly or patients with Alzheimer’s disease.
In these avenues of research, study‒specific templates yield better spatial coregistration
performance and therefore more homogeneous samples. The DARTEL method [58] for
defining such specific common coordinate systems was used in both studies of the present
thesis.
3.2 The problem of multiple comparisons
With the high number of ROIs in finer atlases and even more so with VBA methods,
the problem of multiple comparisons has severe impact on neuroimaging studies [76, 77].
Performing a large number of statistical tests simultaneously (mass univariate testing)
inherently degrades the reliability of the inference as the likelihood of false positives
increases. Remedies for this problem generally follow one of the following three
approaches: (1) reducing the number of the performed tests by the limiting the number of
examined structures or volume, (2) utilizing the fact that the measured values in the brain
are not independent, or (3) applying conservative thresholds for inference in order to
control the rate of false positives.
An example for the first approach, designed for dMRI‒studies is the tract based spatial
statistics (TBSS) [78] method, which projects DTI‒scalars onto the center of WM
regions, defined as the so‒called FA‒skeleton, and performs statistical inference on this
limited volume. Methods of the second approach, such as the cluster‒level inference
based on random field theory in SPM, are widely accepted in functional MRI (fMRI)
processing, when the assumption holds, that the observed blood oxygen level dependent
(BOLD) signal alteration of neighboring voxels is linked, as it follows from the nature of
hemodynamic response [79].
Historically the oldest, simplest, and most conservative is the third approach,
generally associated with the name of Bonferroni, and is based on simple probability.
With 𝑛 measurements converted to probability values using some null distribution, if all
n samples are from the null distribution, then, with a threshold (level of significance) α,

26
the probability of all tests being less then α is (1 ‒ α)n. The probability of one or more of
the n test values being greater than α is called the family‒wise error rate (FWE):
𝑃𝐹𝑊𝐸 = 1 − (1 − 𝛼)𝑛 (𝐸𝑞. 9)
This can be approximated for a small α as PFWE ≤ nα, from which it follows that in
order to achieve a given desired error rate, the probability threshold has to be adjusted as
α = PFWE / n. This procedure, called the Bonferroni‒correction was used in in both studies
of the present thesis.
Another method with similar logic, which was also employed in our work as a more
liberal point of reference, is controlling the false discovery rate (FDR). In FDR‒
correction, instead of constraining the probability of one false positive result, only the
rate at which type I error occurs is controlled, resulting in less conservative testing and
yielding less false negatives.
Although it has been demonstrated that when spatial correlation is present in the
samples, therefore the performed tests are not independent, FWE and even FDR‒
correction methods tend to be overly strict. Thus, several, more liberal approaches have
been proposed to deal with the problem of multiple comparisons, yet both FWE and FDR
are both still widely used as conservative approaches to retain specificity in statistical
testing. Moreover, results ‘surviving’ Bonferroni‒correction are generally considered to
signal substantial effects.
3.3 Multivariate approaches
Multidimensional studies aim to combine information from independent sources in
order to raise statistical power; a feat sought after in the neuroimaging literature. Several
strategies were employed to implement such combination at different levels of statistical
analysis throughout the past two decades, using (and sometimes combining) voxelwise,
surface‒based, or ROI‒level methods. The performance of this pooling of information
has been evaluated on the level of p‒values [80, 81], T‒score maps [82], and by using
multivariate [83, 84] and, as in the first study, logistic regression [85] analyses.

27
The lowest level at which neuroimaging information can be combined is achieved by
working with raw data, or derived parameter maps. Such was the approach e.g. in [86],
working with voxelwise MD and volumetry data. More recently, the performance of
machine learning based classifiers in the scope of lesion detection was demonstrated with
satisfying performance, e.g. on the voxel level, working on T1‒weighted data using a one‒
class support vector machine‒based classifier and outlier detection approach [87]; or on
the vertex‒level, working with morphologic and intensity‒based metrics, using surface‒
based methodology [88] [89].
Although the aforementioned models and studies demonstrated (further detailed in
subsection 2.1) that multidimensional approaches can increase statistical power by
combining the sensitivity profiles of independent modalities, their usage is often
complicated, computationally expensive, and includes arbitrary choices (for example the
choice of combining functions in [82] or the selection of weighting factors for
multivariate linear regression).
The second study of the Thesis was aimed at developing a more straightforward and
easier to use method, based on the Mahalanobis‒distance for testing neuroimaging
(specifically DTI) data in the context of lesion detection when comparing a single patient
to a group of healthy controls.

28
4. The Mahalanobis‒distance
4.1 Definition
The Mahalanobis‒distance is a measure of dissimilarity, commonly used in
multivariate outlier detection problems [90-92], which we employed in our second study
as the basis for epileptic lesion detection, searching for abnormal voxels as outliers when
comparing a single subject to a group of controls.
Following the original definition by Mahalanobis [93], in a P dimensional statistical
field (constructed from P separate variables) the squared distance between an observed
distribution with mean μ = (μ1, μ2, … μP) and covariance matrix S, and any point X = (X1,
X2, …XP) is expressed in the form:
𝐷𝑀2 = (𝑿 − 𝝁)𝑇𝑺−1(𝑿 − 𝝁) (𝐸𝑞. 10)
Multiplication with the inverse of the covariance matrix maps the inter‒point
distances to a standard L2 – norm (i.e. Euclidean space), cleared of any possible
correlations and differences in standard deviations (σ1, σ2,… σP) between the dimensions
(Fig 6); therefore D2 values reflect how far a given point is from the underlying
multivariate distribution.
Fig 6 The effect of the multiplication with the inverse of the covariance matrix.
The multidimensional distribution is cleared of possible correlations and differences in standard deviation,
therefore the distances are effectually calculated in a Euclidean space.

29
This mapping feature is potentially useful in diffusion weighted image processing and
the detection of pathological tissue microstructure in the DTI framework, as different
tensor eigenvalues are sensitive to different pathologies but they generally exhibit strong
correlations [94-96].
By definition, the Mahalanobis‒distance is related to Hotelling’s T2 (e.g. used in [86])
with the exception that the latter compares a group of subjects to the reference
distribution, by using 𝑿 (the group average of Xi = (X1, X2, …XP) vectors, each
corresponding to an individual subject) instead of a single X. Like Hotelling’s T2 is often
referred to as the multidimensional equivalent of Fischer’s two‒sample T‒test, one may
view the squared Mahalanobis‒distance as a multidimensional one‒sample T‒statistic.
4.2 The Mahalanobis‒distance in neuroimaging
The Mahalanobis‒distance has been employed in neuroimaging in relation to various
disorders and at different levels of information processing: in discrimination between
normal tissue types and brain tumors [97]; in ordering the eigenvectors of discriminatory
principal component analysis, differentiating Schizophrenia patients from controls using
whole brain FA [98]; in combining DTI‒scalar metrics with T1 and T2‒weighted images
in WM‒ROIs, quantifying brain maturation [99]; in discerning subtypes of mild cognitive
impairment based on T1, T2, and proton density‒weighted images [100]; and, more
recently, in quantifying the difference between patients with autism spectrum disorder
and subjects with normal aging, using different sets of DTI scalars from major WM tracts
[101].
In [33], the second study behind the thesis, 3 dimensional distributions were
constructed in each voxel from the eigenvalues of the diffusion tensor, and the voxelwise
squared Mahalanobis‒distance was calculated using empirical μ and S from samples
containing one patient and a group of control subjects (Fig 7).

30
Fig 7 Mahalanobis‒distance in the 3D space of DTI eigenvalues.
Outlying diffusion profile in a given voxel of a single subject under examination (red) is detectable through
the distance (D2) from a group of controls (blue and green) in the three dimensional parameter space of the
diffusion tensor eigenvalues. Common alterations of the diffusion profile, such as a higher first eigenvalue
(as in the case of point A; usually detected through increased fractional anisotropy in univariate tests); an
increase in all three eigenvalues (B; commonly observed as increased mean diffusivity); or an altered
diffusion profile with normal‒appearing diffusion strength (like in the case of C, when MD equals to the
average MD of the controls, but the eigenvalues differ) are all detectable in the multivariate framework
with a single test.
4.3 Statistical inference based on critical values
Critical values for detecting a single multivariate outlier at a desired level of
significance, as shown in [102], can be calculated using Wilks’s criterion [103], with the
following formula:
𝐷𝑐𝑟𝑖𝑡2 =
𝑝(𝑛 − 1)2𝐹𝑝,𝑛−𝑝−1;
𝛼𝑛
𝑛 (𝑛 − 𝑝 − 1 + 𝑝𝐹𝑝,𝑛−𝑝−1;
𝛼𝑛
), (𝐸𝑞. 11)

31
where p is the number of dimensions, n is the number of observations (subjects) and
F is the distribution function of the F statistics, with the appropriate numerator and
denominator degrees of freedom at the desired significance level α. By selecting a
sufficiently conservative α, i.e. one aiming to control the FWE or the FDR, the problem
of multiple comparisons (high number of voxels under examination) may also be
addressed. Although the distributions of the diffusion tensor eigenvalues are usually not
strictly Gaussian, this generally does not affect the calculation of Mahalanobis‒distance
significantly, however, it may result in an overestimation of the critical values somewhat
reducing sensitivity with the unintendedly more conservative inference. With the
analytically derived critical values accounting for sample size, statistical significance is
not likely to be affected by the bias described in [104], however, as with conventional
statistical approaches, using larger control samples is desirable to increase specificity.

32
5. Research topics – Clinical importance
5.1 Mild Cognitive Impairment
Alzheimer’s Disease (AD) is the most common neurodegenerative disorder among
the aging population [105], which is already an enormous but still a growing economic
burden in western societies such as countries of the European Union or the United States.
While we do not have effective treatment for AD at the moment, but future
interventions will likely be effective in an early stage of the disease, many research efforts
are focused on the early detection of symptoms. Converging evidence from many
previous investigations revealed that pathologic process of AD starts decades before the
first symptoms of cognitive decline [106]. Therefore, the intermediate stage between the
mild decrease of cognitive functioning in physiological aging and the severe decline in
dementia known as ‘mild cognitive impairment’ (MCI) has gained a lot of interest in the
last decade. “In MCI mild impairment of cognitive skills can be revealed by
neuropsychological tests, while global cognitive functions and everyday activities are
preserved” [107]. The higher conversion rate to AD in MCI gives the clinical significance
of this pre‒disease condition. The annual conversion rate is 10 ‒ 15% in MCI compared
to the annual rate of 1 ‒ 4% in the average elderly population; hence, most MCI patients
develop clinical AD [108, 109]. Further subtypes of MCI can be differentiated such as
the amnestic (aMCI) and non‒amnestic subtypes (naMCI) with distinct structural features
[110]. The conversion rate from the aMCI subtype to Alzheimer Disease is much higher
[111] compared to the naMCI subtype, which underlines the significance of
differentiation between the two. Patients with the naMCI subtype tend to develop other
dementia variants (e.g. vascular).
5.1.1 MRI diagnostics of MCI
Though atrophy of grey matter (GM) structures in the medial temporal lobe have been
the most studied feature [110, 112-114], degradation of white matter tracts, especially the
fornix may precede it [115, 116] and has become detectable in preclinical states with use
of DTI and other complimentary imaging techniques [117]. Indeed, the cingulum and the
fornix carry the axons projecting from the CA1 and CA3 pyramidal neurons of the

33
hippocampus, and there is further published evidence underlining their predictive
potential [118, 119].
5.1.2 The role of DTI in MCI diagnostics
DTI is a relatively new and promising neuroimaging technique in the early diagnosis
of Alzheimer Disease and in the identification of early at‒risk groups such as patients
with MCI. FA and MD were found to be good indices of fiber density, axonal diameter
and myelination, and proved to be useful as early signals of cognitive decline [120, 121].
FA is greater and MD is decreased in organized white matter tracts, while both measures
go to the opposite direction in CSF and disorganized fibers [122, 123]. Findings of
previous studies suggest a specific pattern in MCI and AD where white matter damage
begins in the core memory network of the temporal lobe and cingulum and spreads
beyond these regions in later stages [124].
5.2 Drug resistant epilepsies (DREs)
Drug resistance affects about 20 ‒ 30% of the epileptic patient population, causing
severely impaired quality of life and a difficult to treat situation [125, 126]. Most of the
drug resistant cases (~60%) are focal epilepsies; nevertheless, there are generalized forms.
Malformations of cortical development (MCDs) and long‒term epilepsy‒associated
tumors (LEATs) are among the most frequent etiological factors causing DRE [127-130].
Subtypes of MCDs include focal cortical dysplasia (FCD), polymicrogyria (PMG),
heterotopia (HTP), hemimegalencephaly (HME), while subtypes of LEATs include
gangliogliomas, and disembryoplastic neuroepithelial tumors (DNTs) [131]. Most of
these entities may exhibit variable features on MR images collected with an epilepsy
protocol.
DRE patients are often candidates for surgical intervention; however, the probability
of postoperative seizure freedom is remarkably lower in cases lacking any identifiable
lesions on conventional MRI [132]. Therefore better visualization of MCDs and LEATs
e.g. as shown in [87, 88, 133-137] can be crucial for improving surgical outcomes.

34
5.2.1 DTI in the diagnosis of epilepsy
DTI has been proven sensitive to the disrupted tissue microstructure, identified in
MCDs. Abnormalities tend to extend beyond the lesions themselves, for example [138]
identified decreased FA and increased MD and RD in regions spanning 5 – 20 mm around
the nodules in children with periventricular nodular heterotopia. Widespread decrease of
FA was also demonstrated in major WM tracts in both hemispheres (e.g. in the cingulum,
forceps minor, anterior thalamic radiation, superior longitudinal fasciculus, uncinate
fasciculus, and the inferior fronto‒occipital fasciculus) in a group of patients with frontal
FCDs, using TBSS [139].
More sophisticated models such as DKI [140] or the NODDI [52] approach may
further improve lesion detection based on diffusion weighted MRI [141-143]. Once again,
since DTI is still the most widely used approach, mainly because of its simplicity and
clinically feasible acquisition and processing time, we chose to demonstrate our proposed
statistical method using DTI data, however, the framework we introduced in the second
study may be applied to all kinds of voxelwise variables derived from any meaningful
model.

35
II. Aims
1. DTI and Mild Cognitive Impairment
The primary aim of the first study was to find the possible differences between the
subgroups of MCI, which may increase prognostic capability at an early stage, and a
further aim was to confirm the recent findings regarding the DTI differences observed
between controls and MCI subjects [118, 119]. Based on previous evidence [118, 119],
the most prominent between group differences and the strongest correlations with
memory functions were expected in the cingulum and the fornix. The secondary aim of
the study was to determine in which brain regions and DTI measurements can expand the
findings of previous volumetric examinations [110], to help the differentiation between
patients with aMCI, naMCI, and healthy subjects.
2. Mahalanobis‒distance in MCD lesion detection
The main aim of the second study was to evaluate the performance of a novel,
Mahalanobis‒distance–based statistical approach using DTI data, ‒for detecting
microstructural abnormalities; by simulations using data from standard multivariate
normal distribution (SMVND ̶ 𝓝P(0,1)) and from healthy controls. Based on the
simulation results we also aimed to demonstrate the utility of the approach in select cases
of patients with MCDs.

36
III. Materials and Methods
1. DTI and Mild Cognitive Impairment
Briefly, in this study different statistical approaches were applied to (a) identify those
white matter structures which are the most sensitive to early impairment in pathological
aging, and (b) to estimate if diffusion metrics can extend the differentiation performance
of volumetry. First, we performed voxelwise correlation analyses between
neuropsychological tests and the above mentioned DTI parameters to assess and
demonstrate whether these tests capture the examined aspects of cognitive performance
and that the DTI metrics under consideration do reflect the state of tissue microstructure
in relation to them. Next, we compared subgroups of healthy individuals, and at‒risk
subgroups of amnestic and non‒amnestic mild cognitive impairment on the voxel‒level
to solidify the results of the correlation analyses and to identify the regions showing
significant between‒group differences. With voxel‒level calculations being extended to
the whole of the brain parenchyma, the earliest signs of alterations in GM cellular
structure may be detected. We then performed both correlation and between group
analyses in predefined regions of interest (the 48 ROIs of the ‘JHU White‒Matter Atlas’
[63, 144-146]). With less independent tests to perform and thereby being able to apply
more liberal thresholds for multiple comparisons correction, the ROI‒level approach may
exhibit higher sensitivity. Even more so, with the method being used on WM ROIs, its
results may prove to be more stable (as DTI is most sensitive to changes in the WM),
rendering this approach better suited for discriminative models.
Finally, In order to prove our hypothesis that DTI measures of these regions can
improve the differentiation performance achievable with GM volumetry, logistic
regression analysis was performed with a K‒fold cross‒validation approach [147],
combining volumetric data from the same patient population [110] with the DTI
measures.

37
1.1 Study data and Participants
MR imaging data of 65 subjects (18 with amnestic MCI, 20 with non‒amnestic MCI,
and 27 healthy controls) acquired at 3T (Philips Achieva scanner, Philips Medical
Systems, Best, The Netherlands) was included in this study; the subjects were the same
as those in [148], except for three additional healthy controls.
Brain dMRI images were collected with a single shot SE‒EPI sequence, with
b = 800 𝑠/𝑚𝑚2 diffusion weighting in 32 directions and one b = 0 image. In‒plane
resolution was 1.67×1.67 mm; whole brain coverage was achieved with 70 consecutive,
2 mm thick axial slices; repetition time TR = 9660 ms repetition time, TE = 75.6 ms echo
time, and 90° flip angle was used; the total acquisition time was 8:32min. High resolution
T1‒weighted images were also acquired for registration purposes with 1 mm isotropic
voxels, using a 3D gradient‒echo sequence.
All subjects enrolled in the study participated in a cognitive training program
announced in a Retirement Home and among general practitioners (The study is
registered at ClinicalTrials.gov, identifier is 'NCT02310620'). Demographics of the three
groups of subjects are summarized in Table 1. A detailed description of the
neuropsychological tests can be found in the Supplementary Material of [85].
Subjects included in the study were categorized as aMCI, naMCI, and healthy controls
according to the Petersen criteria [107]. The Petersen criteria include subjective memory
complaint corroborated by an informant together with preserved everyday activities, a
memory impairment based on a standard neuropsychological test, preserved global
cognitive functions and finally the exclusion of dementia. It does not specify a
neuropsychological test for the assessment of memory impairments; therefore, we applied
the Rey Auditory Verbal Learning Test (RAVLT), which is the most frequently used test
in the literature [149]. For the differentiation between aMCI and healthy controls, we
applied a cutoff score of one standard deviation (SD) under population mean standardized
for age and gender. Participants, who scored under the cutoff value, either in the delayed
recall subscore or in the total score, was assigned to the aMCI group. The applied criteria
are based on the recommendations of the National Institute on Aging – Alzheimer’s
Association workgroups on diagnostic guidelines for Alzheimer's disease [150]. Subjects

38
who were not in the aMCI group, but scored one SD under the population mean
standardized for age and gender/education either in the Trail making Test B or in the
Addenbrooke’s Cognitive Examination (ACE), were assigned to the naMCI group. An
additional criterion for the naMCI group was a lower than 3.2 VLOM (verbal fluency +
language score / orientation + memory score) ratio in the ACE to exclude possible aMCI
subjects from the naMCI group (these subjects were excluded from the study).
Subjects with dementia according to the Mini Mental State Examination (MMSE)
scores standardized for age and education [151] were excluded from the study, similarly
to subjects with history of head trauma, epilepsy or stroke, or with the diagnosis of acute
psychiatric disorder, schizophrenia or mania, or alcohol dependence. One aMCI patient
was left out of the calculations who was found to be an outlier, performing significantly
worse on each test, thereby biasing the calculations. None of the subjects enrolled in the
study had a history of any neurological disorder.

39
Table 1 Demographic data and result of basic neuropsychological tests.
control (n=27) naMCI (n=20) aMCI (n=18) p value
Age 65.2 ( 7.2) 71.1 ( 8.2) 69.8 (11.3) n.s.*
Education a 7%/33%/59% 20%/30%/50% 17%/22%/61% n.s.*
Gender (Female) 70% 65% 61% n.s.*
Rey Auditory Verbal Learning Test 1 -5 sum b 53.4 ( 7.7) 46.6 (10.0) 29.5 ( 7.4) p<0.0001
ACE Total Score c 94.0 ( 3.1) 89.5 ( 4.6) 82.1 ( 7.7) p<0.0001
ACE VL/OM-ratio d 2.6 ( 0.4) 2.5 ( 0.4) 3.1 ( 0.8) p=0.002
Mini Mental State Examination Total Score e 28.5 ( 1.3) 28.4 ( 0.9) 27.4 ( 1.8) p=0.025
Geriatric Depression Scale Score f 3.3 ( 2.9) 4.5 ( 2.7) 4.4 ( 3.3) n.s.*
STAI Score g 37.3 ( 9.8) 36.4 ( 9.3) 36.7 ( 8.3) n.s.*
aMCI: Amnestic mild cognitive impairment, naMCI: non amnestic mild cognitive impairment ACE:
Addenbrooke’s Cognitive Examination, STAI: state-trait anxiety inventory
a: Participants were categorized into three education groups: 1=less than 12 years; 2=high school
graduation (12 years education); 3=more than 12 years education
b: Sum of all words in the first five trials.
The maximum score is 75.
c: The maximum score is 100
d: VL/OM: verbal fluency and language points/orientation and delayed recall ratio can be defined based
on ACE. Result below 2.2 indicate frontotemporal dementia and result over 3,2 indicate Alzheimer’s
disease.
e: The maximum score is 30.
f: The maximum score is 15.
g: State-Trait Anxiety Inventory. The maximum score is 80.
* n.s. (not significant) = p > 0.05

40
1.2 Preprocessing and diffusion tensor fitting
dMRI data was preprocessed using the Matlab‒based (MATLAB 8.3, The
MathWorks Inc., Natick, MA, 2000) ExploreDTI software package [152]. Processing
steps included coordinate system transformation, rigid body transformations for
correcting subject motion, non‒rigid transformations for correcting susceptibility‒related
and EPI‒induced distortions, with the local rotation of the b‒matrix (the diffusion
weighting directions) to avoid angular inaccuracies [56]. The high‒resolution T1‒
weighted images were used as templates for registration to correct the distortions inherent
to the EPI‒acquisition method [153]; thereby dMRI‒images were spatially aligned to the
T1‒weighted images.
After tensor fitting, using the RESTORE (Robust Estimation of Tensors by Outlier
Rejection) [17] algorithm, two voxelwise DTI‒measures FA and MD [14, 154, 155] were
calculated from the tensor eigenvalues, following their well‒established definitions, to be
used in voxel‒level and ROI‒based analyses.
1.3 Voxelwise analysis
Images containing the DTI scalar values were ‘normalized’, i.e. transformed into a
common coordinate system using the DARTEL tools [58] of the SPM12 toolbox [69].
The DARTEL method is a common approach e.g. in VBM studies [156, 157] using T1‒
weighted images. This method creates a template in several iteration steps that is the
closest to each individual subject’s anatomy. This way the common coordinate system is
study‒specific, resulting in more efficient handling of macroscopic anatomical
differences (such as possible GM‒atrophy), compared to other widely used approaches,
for example those utilizing the MNI152 space [158].
Once the template image was calculated and the transformations (‘flow fields’)
linking each subject’s native space to the common space were determined, we used these
transformations on the DTI parameter images (‘warping’).
The ‘warping’ function of DARTEL includes a ‘modulation’ step to account for
macroscopic anatomical differences. As the method was developed to examine cortical

41
thickness and structure, when e.g. the transformation means merging three voxels in two,
the addition of tissue probability values keeps the information of cortical thickness.
However, when working with DTI scalar parameters, this addition (preserving the
‘concentration’) would falsify the original diffusion traits, thereby we omitted the
‘modulation’ option in our processing framework.
The performance of the spatial alignment was assessed by visual inspection and the
‘Check Data Quality’ function of the Computational Anatomy Toolbox (‘CAT12’, an
extension to SPM12) [159]. This tool calculates a three dimensional spatial correlation
coefficient between images; misaligned data is easily identified by the decreased level of
correlation. Three subjects (two controls and one aMCI patient) were removed from the
voxelwise calculations following the corresponding results of the two quality assurance
methods. The resulting normalized data was used unsmoothed for assessing the
correlation between neuropsychology and microstructure, while, for between group
analyses, Gaussian smoothing (with full width at half maximum: FWHM = 8 mm,
isometric) using SPM was applied.
Use of the widely acknowledged TBSS [78] method was also considered for its higher
statistical power, but because of its inherent loss of spatial information (especially from
the cortex) due to constraining analysis to the FA skeleton (the supposed center of white
matter tracts), and its recently discovered poor spatial alignment performance in regions
with complex WM structures [160], this option was omitted.
The whole brain voxelwise analysis, used in both between group and correlation
analyses was extended to grey matter voxels, hypothesizing that small changes in GM
microstructure which may precede macroscopic symptoms manifest in noticeable
differences in DTI scalar values [161-163].
1.3.1 Voxelwise correlation analysis
In order to accurately localize the brain regions related to cognitive dysfunction, we
calculated partial correlation coefficients in each voxel between the (non‒smoothed)
values of DTI parameters and the results of neuropsychological tests across all subjects
using a high performance Matlab‒based algorithm, including subject’s age and sex as

42
covariates. Statistical significance of the correlations was assessed using Student’s T‒
distribution.
Two types of corrections for multiple comparisons were employed: FWE control was
achieved by the Holm‒Bonferroni method [164], while the less conservative FDR control
was achieved by the Benjamini‒Hochberg step‒up algorithm, which is considered to have
more statistical power at the cost of controlling only the proportion of type I. errors [165].
Due to the large number of voxels in the calculations (280315 grey or white matter voxels,
defined using the DARTEL template), achieving a FWE rate or FDR of 0.05 meant
statistical p‒values in the order of 10‒8 – 10‒6.
In order to distinguish between true and false positive results in the cases of small
clusters spanning the volume of only a few voxels, we also checked the underlying trends
using an exploratory threshold of p < 0.001, uncorrected. True positive result would
appear as the most significant voxels (the focal points) of larger regions achieving
significance with the exploratory threshold, while false positives could show as single
voxels spread in random fashion.
Moreover, similar, homogeneous behavior, or emerging patterns of correlation
coefficients in specific anatomical regions (e.g. the same sign and scale of R‒values in a
specific gyrus) could also support the identification of true positives as the most
significant voxels would be identified as the peaks of such regions.
1.3.2 Voxel‒based between group statistical analysis
A large number of studies have confirmed the connection between various types of
dementia and the changes in diffusion tensor parameter values in several brain regions
[123, 166-171], using voxel‒based analysis (VBA) methods typically in group‒level
comparisons. In order to confirm that our patient groups exhibit such significant
differences, and therefore the identified correlations are meaningful, smoothed diffusion
parameter maps (isometric Gaussian smoothing with FWHM = 8 mm) were examined,
using SPM’s ‘Second‒level’ general linear model (GLM) functions.
Four calculations were performed on both diffusion parameters, using each
individual’s age and sex as covariates: one‒way analysis of variance (ANOVA) test on

43
all three groups and two sample T‒tests between pairs of groups. Each test was performed
with FWE correction for the conservative treatment of the problem of multiple
comparisons.
1.3.3 Visualization
Resulting raw images of the VBA and the correlation analyses were in the DARTEL
Template space; however, in order to easily compare our results to those of previous
publications, FWE or FDR corrected T and R‒score maps were transformed to MNI152
space [158] using SPM’s DARTEL tools.
1.4 ROI‒based statistics
ROI‒s were defined by transforming the 48 regions of the JHU White‒Matter Atlas
[63, 144-146] into each patient’s own image‒space, using the ‘Get diffusion metrics from
ROI labels’ tool of ‘ExploreDTI’. This plugin utilizes the ‘Elastix’ [172] software for
label registration and exports the average DTI‒parameter values (MD, FA) for each
region. Spatial alignment of the ROI labels was validated by visual inspection. In the
further analyses, data obtained from 36 cerebral ROIs was imported into SAS (SAS 9.4
software, SAS Institute, Cary, NC); 12 ROIs outside the cerebrum, such as cerebellar
white matter tracts, were excluded.
1.4.1 ROI‒based correlation analyses and between‒group comparisons
Correlations with neuropsychological tests were analyzed by calculating Pearson’s
correlation coefficients (proc. CORR in SAS), and also Spearman partial correlations as
independent confirmation of the monotonous and linear nature of the relationships.
The three study groups were also compared by Analysis of Covariance (ANCOVA)
using FA and/or MD data from these ROIs with age and gender as covariates; followed
by post hoc between group comparisons using general linear models (proc GLM in SAS).
In order to control for multiple comparisons, Bonferroni correction was applied: the level
of significance was adjusted to p = 0.05 / 36 = 0.0013.
1.4.2 ROI‒based logistic regression analysis for a combined cortical thickness and DTI
based differentiation between study groups

44
GM volumetric data (cortical thickness and subcortical brain structure volumes)
obtained using the freely available Freesurfer 5.3 image analysis suite
(http://surfer.nmr.mgh.harvard.edu/) with its default processing pipeline and parcellation
settings were then analyzed jointly with the DTI‒derived metrics in a logistic regression
analysis (‘proc LOGISTIC’ in SAS, stepwise variable selection) to assess if the
combination of GM and WM DTI data leads to better differentiation between aMCI
subjects and healthy controls than using the GM data alone. Three healthy controls and
one subject with naMCI were excluded from the logistic regression analyses due to
missing volumetric measurements. The Freesurfer‒based processing pipeline for the grey
matter data were described in detail in [148].
Combined MD/GM volume and FA/GM volume models were analyzed separately;
further details on the logistic regression analyses and how measurements were selected
to be included in the model are described below. Discrimination between each pair of
subject groups was tested using a ten‒fold cross‒validation approach [147] (K‒fold
testing in SAS):
First, an independent test‒set of four subjects (two from each group, representing 10%
of the sample population) was assigned; the features of the logistic regression model were
selected on the remaining 90% of the subjects. In the second step, the resulting model was
tested on the small test subset, independent from the model creation. This method was
repeated ten times (nine times when discriminating between aMCI and naMCI) as each
subject was assigned once to a test‒subgroup. The resulting ten (nine) independent
models, their selected effects and corresponding discrimination performances were then
summarized.

45
2. Mahalanobis‒distance in MCD lesion detection
2.1 Study data and participants
Diffusion and T1‒weighted MR imaging data of 45 healthy control subjects (25.6
years average age, range: 20 – 37 years, 17 males) and 13 patients (21 years average age,
range: 7 – 46 years , with two children under 10, 7 adolescents between 14 and 18, 9
males) with MCDs was acquired at 3T (Philips Achieva scanner, Philips Medical
Systems, Best, The Netherlands). dMRI images were collected with a single shot SE‒EPI
sequence, with diffusion weighting in 32 directions with b = 800 𝑠/𝑚𝑚2 and one b = 0
image. In‒plane resolution was 2×2 mm (reconstructed to 1.67×1.67 mm with zero
filling); whole brain coverage was achieved with 84 (adjusted when necessary), 2 mm
thick axial slices and no gap; TR = 9660 ms repetition time, TE = 75.64 ms echo time,
and 90° flip angle was used; the total acquisition time was 8:32 minutes. High‒resolution
3D T1‒weighted images were also acquired for registration purposes (1 mm isotropic
voxels), using a standard 3D gradient‒echo sequence. 2D fluid attenuated inversion
recovery (FLAIR) sequences (0.43×0.43 mm in plane resolution, 3.3 mm thick coronal
slices, tilted perpendicular to the axes of the hippocampi, TR = 9000 ms, TE = 125 ms,
TI = 2800 ms, flip angle = 90°) were also acquired for aiding the visualization of the
MCDs.
Patients were selected retrospectively, with several different types of MCDs and other
abnormalities: MCD subtypes included polymicrogyria (in two patients) schizencephaly
(two patients), subependymal heterotopia (in three patients), FCD (in six patients),
cortical dysgenesis (in three patients) and other, not clearly identifiable malformations (in
four patients). Several other types of abnormalities were also identified in the patient
group, such as DNT (in one patient, later confirmed by histopathology), ischemic WM
lesions (in two patients), a gliotic cyst (in one patient), focal gliosis (in one patient, also
confirmed by subsequent histopathology), hippocampal sclerosis (in four patients), and
malrotation of the hippocampus (in one patient). Diagnoses of MCD subtypes were based
on neuroradiology report; the supplementary Table S10 contains detailed information on
each lesion and abnormality, along with the results of neuroradiology assessment and
lesion detection calculations.

46
The study was approved by the Scientific and Research Ethics Committee of the
Medical Research Council, Budapest, Hungary (ETT TUKEB - 20680-2/2012/EKU
(368/PI/2012)) for patients and (ETT TUKEB 23609-1/2011-EKU, 23421-1/2015-EKU)
for controls; all participants provided written informed consent. Following publication
requirements, anonymized T1‒weighted images (facial structures removed using the
‘mri_deface‘ function of Freesurfer ‒ https://surfer.nmr.mgh.harvard.edu/fswiki
/mri_deface) and coregistered DTI‒eigenvalue maps of the patients and controls were
made available in the ‘GIN’ public repository under the DOI 10.12751/g-node.80dd9a.
2.2 Data processing
dMRI data was preprocessed using the Matlab‒based ExploreDTI software package
[152]. Processing steps included the transformation into ExploreDTI’s coordinate system,
rigid body transformations for correcting subject motion, and non‒rigid transformations
for susceptibility‒related and EPI‒induced distortion‒correction, while also rotating the
b‒matrix (the directions of diffusion‒weighting) accordingly, in order to avoid angular
inaccuracies [56]. T1‒weighted images were used as templates for registration to correct
the distortions inherent to the EPI‒acquisition method [153]; thereby DW‒images were
spatially aligned to these T1‒weighted images. After robust tensor fitting, using the
RESTORE [17] algorithm, the tensor eigenvalues were calculated and exported for the
voxel‒level analysis.
We used the DARTEL method with default parameters for the group‒level
coregistration of the eigenvalue images, as described in detail in 1.3, with some
variations:
The DARTEL template was created from the T1‒weighted images of only the control
subjects; patient data was subsequently registered to this common space. As a byproduct
of the registration, ‘flow‒fields’ describing the transformation between each individual’s
native space and the template space were obtained and used to coregister the eigenvalue
images. Finally, the DARTEL template was used to generate a brain mask and subsequent
calculations were limited to this volume.

47
This way, the reference distribution of voxelwise DTI eigenvalues in the common
coordinate system (control data) had low observed sample variance, unbiased by patient
anatomy, and provided a solid basis for sensitive lesion detection. On the other hand, this
subsequent transformation of patient data may have amplified registration artefacts,
especially in cases when a patient was highly different from the controls (e.g. when the
patient was significantly younger, or had large anatomical abnormalities).
This processing pipeline contains only two interpolation steps. First, in the motion
and distortion‒correction step, the DWI data is interpolated to the finer resolution of the
T1‒weighted images [173], while the second is performed in the coregistration step of the
DARTEL method, to a coarser, 1.5 mm isotropic resolution. This is the necessary minimal
number of interpolations when each individual’s T1‒weighted images are used for DWI
distortion correction, and statistical inference is made in a common space.
Spatial alignment was once again assessed by visual inspection and the ‘Check Data
Quality’ function of the Computational Anatomy Toolbox (‘CAT12’, an extension to
SPM12) [159].
The resulting coregistered whole brain tensor eigenvalue images of the healthy
subjects were used for three purposes: (a) as data basis for simulations in a ‘bootstrap’
manner, (b) in a leave one out examination to measure the performance of coregistration
and its effect on false positives, and (c) as controls when patient data was examined.

48
2.3 Independent automatic evaluation of MCDs
As part of our epilepsy post‒processing protocol we also used the MAP07 toolbox
that performs single subject vs. control group comparisons on volumetric T1 data derived
3D feature maps regarding the GM–WM junction (junction map), cortical gyration
(extension map), and cortical thickness (thickness map). The resulting Z‒score maps can
be thresholded and/or combined (combined map) in order to pinpoint areas with suspected
pathologies [135-137].
We analyzed all our cases using the default processing parameters of the MAP07
toolbox, the feature map comparisons were performed against a generic normal database
provided with the software, which consists data of 150 healthy controls scanned on five
different MRI systems [136]. The resulting Z‒score maps were thresholded at the default
Z > 4 value and then combined and converted to ROIs.
The resulting ROIs were used to signify locations being suspicious of malformation
of cortical development in the general neuroradiology workup. They have all been re‒
evaluated by the neuroradiology expert, and those without underlying pathology were
discarded. The ROIs deemed relevant were then edited to completely cover the respective
pathologies. Additional ROIs were created manually to cover lesions that were not
identified by the MAP07 toolbox; finally the ROIs served as ground truth signaling the
lesions in further analysis.
2.4 Mahalanobis‒distance related calculations
We have implemented the calculation of the voxelwise Mahalanobis‒distance (D2)
from the DTI eigenvalue maps according to (Eq. 10), the statistical inference based on
critical values determined by (Eq. 11), and cluster size thresholding, in Matlab scripts and
functions (MATLAB 9.2, The MathWorks Inc., Natick, MA United States). Eigenvalue
maps are being read in nifti format, transformed to vector format for efficient parallelized
calculations, inference is performed voxel‒by‒voxel, followed by cluster identification,
and size thresholding (also see the bottom half of Fig 8). The same framework was used
for subsequent calculations, including simulations, leave‒one‒out examination of
controls and patient evaluations.

49
2.5 Simulations
The performance of the method was evaluated using simulations with two distinct sets
of data: (a) Gaussian random images and (b) real diffusion tensor eigenvalue maps.
Following the fashion described in [174], alternative free‒response receiver‒operator
characteristics (AFROC) analyses were carried out on both sets.
As the critical values calculated by (Eq. 11) depend on sample size, and the aim of
the simulation study was to provide grounds for later analyses; the same number of
control observations (45 subjects) were modelled in both simulations.
In order to evaluate the method’s performance as a lesion detection tool, simulations
were carried out with different contrast‒to‒noise ratios (CNR ‒ i.e. effect strengths:
difference between mean values of the ‘lesions’ and the ‘background’, measured in units
of standard deviation with σ lesion = σ background ), and lesion sizes, with a variable cluster
size threshold for controlling the rate of false positives. An overview ‘flow‒chart’,
describing the steps of the simulations is shown in Fig 8.
2.5.1 Simulations with Gaussian distributions
A group of 45 ‘control subjects’ were generated following 3D Gaussian distribution,
with zero mean and unit standard deviation in all three random variables (𝓝3(0,1),
SMVND) in each voxel (upper left part of Fig 8). The spatial dimensions matched those
of the real coregistered DTI data, described in subsection ‘Data processing’.
True positive images were generated, starting from similar random ‘noise’ data and
adding simulated ‘lesions’: 3D patches with predefined sizes, randomly generated shape,
and voxel values from a distribution with the mean shifted from the background values,
according to the predefined CNR. Each true positive image had one ‘lesion’ with a center
randomly selected from 25 different locations; coordinates were defined on the template,
close to the frontal, temporal, and occipital GM‒WM boundary, in view of the second set
of simulations with real eigenvalue data. One thousand such positives and another
thousand negatives (i.e. just SMVND ‘noise’) were generated to calculate true and false
positive rates (upper left part of Fig 8).

50
Fig 8 Flow chart demonstrating steps of the simulations.
Eigenvalue maps of standard multivariate normal distributions (SMVND – upper left) and random
resampling of the real eigenvalue maps of the control subjects (upper right) were used as reference data.
True negative and true positive ‘cases’ (with added artificial ‘lesions’, i.e. patches of voxel values of shifted
distributions, compared to the background) were generated and the squared voxelwise Mahalanobis‒
distance (D2) was calculated in relation to 45 control cases. D2‒images were subjected to thresholding using
FDR‒ or FWE‒corrected critical values (for multiple comparisons) and cluster size thresholding. False
positive rates (FPR) were calculated from hits in true negative ‘cases’ (Ipositive), while true positive rates
(TPR) and hit rates (TPR‒binary, i.e. TPRB) resulted from hits in the positive cases (Itrue positive) .
After the calculation of voxelwise D2‒values, thresholding was performed using
critical values calculated to control the FWE rate (i.e. Bonferroni bounds) or the FDR
(using the Benjamini‒Hochberg step‒up algorithm on P‒values calculated by the inverse
of (Eq. 10)). The surviving supra‒threshold voxels were subjected to cluster‒size
thresholding following third‒neighbor (26 neighbors) cluster definition (Middle panels in
the lower half of Fig 8).
The resulting binary images were used to calculate the true positive rate (TPR) in
positive, and the false positive rate (FPR) in negative cases. Two types of TPR were
defined, the first as the ratio of identified positive voxels (i.e. the identified lesion volume
ratio, averaged over the pool of positive cases), following the definition of alternative

51
fractional receiver operating characteristics (AFROC) TPR as used in [174] (rightmost
panel in the lower half of Fig 8).
As lesion detection is a binary problem (i.e. identifying only a part of the region of
pathological tissue is also considered a positive result) any true positive voxel was
counted as a hit (Itrue positive) in the second definition of true positives (TPR ‒ Binary ‒
TPRB). False positives were defined similarly, as any positive cluster in a true negative
(only noise) image was considered a false hit (Ifalse positive).
𝑇𝑃𝑅 = ∑∑
#𝑝𝑜𝑠𝑖𝑡𝑖𝑣𝑒 𝑣𝑜𝑥𝑒𝑙𝑠#𝑣𝑜𝑥𝑒𝑙𝑠 𝑖𝑛 𝑙𝑒𝑠𝑖𝑜𝑛
1000
1000
1
(𝐸𝑞. 12)
𝑇𝑃𝑅𝐵 = ∑𝐼𝑡𝑟𝑢𝑒 𝑝𝑜𝑠𝑖𝑡𝑖𝑣𝑒
1000
1000
1
(𝐸𝑞. 13)
𝐹𝑃𝑅 = ∑𝐼𝑓𝑎𝑙𝑠𝑒 𝑝𝑜𝑠𝑖𝑡𝑖𝑣𝑒
1000
1000
1
(𝐸𝑞. 14)
The same sets of simulations were performed for each combination of the controlled
parameters with FDR and FWE critical values. TPR, TPRB and FPR values
corresponding to each set of controlled parameters were used for the creation of ROC
curves and the calculation of ‘area under the curve’ (AUC) values, using the 0 – 0.05
FPR‒range, using trapezoids under the curve and the FPR = 0.05 point determined with
linear interpolation. AUC values were scaled up to the [0, 1] range to compensate for the
limited range of interpretation. This constrained FPR‒range means that in our
simulations, the Family‒Wise Error rate was also controlled at the subject level (above
the voxel‒level FWE or FDR), resulting in thorough correction for multiple comparisons.
Values of the three varied parameters are summarized in Table 2.

52
Table 2: CNR lesion size and cluster size threshold values used in the simulations.
CNR [σ] 1 2√2ln (2) a 3 4√2ln (2) - - -
Lesion size [#voxels] 19 35 50 100 200 - -
Cluster size threshold [#voxels] 1 2 3 4 5 6 7
a Note that CNR = 2√2ln (2) contrast to noise ratio equals to 1 FWHM distance between the peaks
of the distributions.
The desired CNR was calculated by setting the difference between means, in units of
standard deviations. In SMVND simulations σ = 1 was used, while unique values were
calculated in each individual ‘lesion’ volume and for each eigenvalue in the second set of
simulations with real DTI data.
In an exploratory analysis, additional simulations were performed with smaller effect
sizes (down to CNR = 0.1); however, since the lesion detection performance did not
exceed chance level, these results were omitted. Larger cluster size thresholds of 19, 27
and 50 voxels were also used, but, as no false positives were identified above the size of
4 voxels (7 voxels in the second set of simulations; see subsection 2.5.2) these results are
not detailed either.
2.5.2 Simulations with real eigenvalues
The second sets of simulations were performed based on the diffusion tensor
eigenvalue maps of the control group using bootstrap approach, i.e. 2000 resamples
considered as individual ‘subjects’ were generated by random resampling of voxel values
from the pool of 45 control subjects (upper right part of Fig 8). Similar to the first set, half
of these resamples were designed to be ‘positive’ with added simulated ‘lesions’, while
the other half of the resamples was ‘negative’. Finally, the same subsequent TPR, TPRB,
and FPR calculations were performed as with the SMVND data, and corresponding AUC
and optimal threshold vales were obtained.
While the first set of simulations used Gaussian random values in the whole brain, the
bootstrapping in the second set was performed on the voxel level, thereby these values
followed the distribution of tensor eigenvalues in the particular ‘lesion’ volume. Thus the
CNR in each artificial ‘lesion’ was determined using a volume‒specific σ (representing

53
the distribution around the GM‒WM boundary), assuming σlesion= σbackground. Although
this may be considered a limitation, as true MCDs are likely to exhibit atypical
distribution of tensor eigenvalues, since the statistical decision is made independently in
each voxel with no cluster‒level inference, this assumption does not affect the detection
performance directly.
2.6 Leave‒one‒out examination of controls
The simulations demonstrated that lesions with sufficiently high effect strengths
(CNR) and volumes are detectable using the proposed Mahalanobis‒distance based
method, with satisfying sensitivity. On the other hand, this high sensitivity makes the
approach susceptible to registration artefacts and strong individual variability, resulting
in false positive clusters. In order to measure the impact this effect has on patient
evaluation, data of the control subjects was also used in a leave‒one‒out examination,
comparing each individual to the remaining 44. Calculation of D2‒values, inference with
critical values (with FWE or FDR correction), and cluster size thresholding (with the size
of 7 voxels) were performed in the same manner as with the simulations. Resulting
thresholded D2‒maps, indicating regions of significantly outlying diffusion profiles were
transformed back to the native space of each patient’s original T1‒weighted image.

54
2.6.1 Cluster description based on tissue probability maps (TPMs)
The results contained several clusters, in many cases obvious false positives, likely
resulting from the aforementioned registration inaccuracies and individual variability in
gyration patterns. In order to distinguish such false positives and increase the specificity
of our method, clusters were subjected to additional post‒processing in the following
manner:
From each individual’s Tissue Probability Maps (resulting from the initial
segmentation step of the DARTEL‒pipeline), we defined a new parameter describing
voxel position, by subtracting the WM TPM from the CSF TPM: δ = P(CSF) – P(WM)
(Fig 9). This way a δ‒value was assigned to each voxel from the [-1, 1] range, with
positive values indicating voxels closer or belonging to CSF, and negative values
indicating voxels closer or belonging to WM.
Fig 9 Definition of ‘tissue probability’ used for cluster filtering.
δ‒ values were calculated in each voxel by subtracting the probability of a voxel belonging to the white
matter (WM) from the probability of it belonging to the cerebrospinal fluid (CSF), using the tissue
probability maps obtained in the initial segmentation of the T1‒weighted images. The resulting δ‒value
indicates the voxels’ position along the centrifugal WM‒GM‒CSF axis.
Registration artefacts around the brain surface would mainly contain voxels with
positive values (δ > 0; meaning that the majority of voxels are from the CSF). On the
other hand, MCDs under consideration typically occur around the GM‒WM boundary,
thereby true clusters would contain negative values close to zero (δ ≲ 0), the distribution

55
of the 𝛿‒values in any given cluster could be used as an indicator of cluster position along
the centrifugal WM‒GM‒CSF axis.
In the second step, clusters with more than half of the voxels with δ > 0.1 were
eliminated from the analysis. This cutoff, signaling clusters with the majority of voxels
from the CSF, was determined based on the results of leave‒one‒out examination of
controls.
2.7 Representative cases of MCDs
As described in subsection 2.2, DTI eigenvalue maps of patients with MCDs were
registered to the DARTEL‒template created from control data. D2‒calculation and
thresholding using FWE‒corrected critical values (see the corresponding subsection 2.3
for the reasoning behind using the more conservative correction), cluster size thresholding
(again with 7 voxels threshold size), and the δ‒value‒based post‒processing of the
clusters were performed in the same manner as described above.
Results were qualitatively evaluated by comparing the anatomical images and D2
‘heatmaps’ along with the Z‒scored junction maps, resulting from independent
calculations by the MAP07 toolbox [135], as described in 2.3. Clusters of outlying
diffusion profile, remaining after the thresholding and artefact removal steps were
considered true positive, when good spatial concurrence with the underlying pathology
(as observed on anatomical scans) and the reviewed and corrected results of the MAP07
toolbox was ascertained.
An additional step included the calculation of the clusters’ centers of mass (using the
D2‒values as weights), and their (physical) distance from the lesion masks; created as
described in 2.3.

56
IV. Results
1. DTI and Mild Cognitive Impairment
1.1 Voxelwise analyses
1.1.1 Voxelwise correlation analysis
Voxelwise correlation of the FA and MD values with the results of the four
neuropsychological tests was found to be significant (p < 8.4×10-7) in several clusters
with FDR and FWE correction. Table 3 contains the list of these clusters, while the
following paragraphs also highlight the peaks of the underlying test distributions (i.e. the
locations that exhibit the strongest correlation), represented by their corresponding
statistical values and [x, y, z] coordinates in MNI space [158].
The most significant correlation between FA values and the paired associates learning
(PAL) test results was identified in the pars triangularis of the right inferior frontal gyrus
([-38, 19, 27], R = ‒0.67, p < 1.36×10-7 ) (Fig 10/ Panel A).
Neither the ACE‒score values nor the RAVLT or the Trail Making test showed any
significant correlation with FA.
Correlation of MD with three of the four tests was found to be significant in several
clusters. The RAVLT score was found to be correlated to MD in the left parahippocampal
gyrus ([-25, 3, -30], R = ‒0.63) (Fig 10 / Panel B).
The ACE score correlated significantly (p < 1.53×10-7) to MD in the left
parahippocampal gyrus ([-23, 2, -30]) and in the pole of the left middle temporal gyrus
([-34, 5, -47], R = ‒0.62) with FWE correction (Fig 10 / Panel C), and in two additional
clusters with FDR correction.
Ten clusters with significant correlation between the Trail Making test and the MD
values were identified with FDR (p < 5.4×10-6) and two with FWE (p < 2.7×10-8)
correction: one in the angular gyrus ([48, -60, 28], R = ‒0.65) (Fig 10/ Panel D) and one
in the right superior temporal gyrus ([61, -46, 14], R = +0.66) showed the most significant
correlation.

57
Table 3 Results of the voxelwise correlation analyses
FA
FDR FWE
Number of
clusters Peak p
Cluster size
[voxels] R-score Region [175] Peak p
Cluster size
[voxels]
PAL Test 1 8.40 × 10−7 3
-0.63 Posterior Corona
Radiata R
[-29,-29,26]
- - -0.64
-0.64
ACE - - - - - - -
Rey
Auditory - - - - - - -
Trail Making
Test A
- - - - - - -
MD
FDR FWE
Number of
clusters Peak p
Cluster size
[voxels] R-score Region [175] Peak p
Cluster
size [voxels]
PAL Test - - - - - - -
ACE 4 6.30 × 10−7 2 -0.61
Para
Hippocampal L 1.53 × 10−7 1
-0.63 [-23,2,-30]
Rey
Auditory 8 5.00 × 10−6
19 -0.64
Para
Hippocampal L
1.70 × 10−7
4
-0.58 [-25,3,-23]
3 -0.55 Hippocampus L
[-31,-20,-16] -
-0.57
2 -0.55
Fusiform L
[-29,-11,-33] -
-0.56
Trail
Making Test A
10 5.40 × 10−6
11 +0.55 +0.58
Temporal Mid R [56,-28,-9]
2.70 × 10−8
1
2 +0.56
+0.57
Fusiform L
[-39,-17,-21] -
7 +0.56
+0.59
Thalamus L
[-16,-28,12] -
3 +0.65
+0.56
Angular R
[48,-60,28] 1
2 +0.56
+0.57
Occipital Mid L
[-31,-81,11]
FA: fractional anisotropy, MD: mean diffusivity, ACE: Addenbrooke’s Cognitive Examination, FDR: false
discovery rate control, FWE: familywise error rate control, Peak p: the highest significant p‒value in a
cluster, R‒score: Pearson’s correlation coefficient, [175]: coordinates in Montreal Neurological Institute
template space.

58
Fig 10 Results of the voxelwise correlation analyses between DTI scalar values and
neuropsychological tests of healthy subjects and patients with Mild Cognitive Impairment
Regions of significantly (FWE = 0.05 in yellow, FDR = 0.05 in red) correlated DTI‒scalar values: in the
pars triangularis of the right inferior frontal gyrus (R = −0.67) between fractional anisotropy (FA) and the
PAL test scores (Panel A); in the left parahippocampal gyrus (R= −0.63) between mean diffusivity (MD)
and the RAVLT score (Panel B) and the ACE score (Panel C); and in the right angular gyrus (R = +0.65)
between MD and the results of the Trail Making test (Panel D). Thresholded 1‒p value maps transformed
to MNI152 space and overlaid on a single subject T1‒weighted image, shown following neurological
convention (left side on left). Small clusters of significant correlations emerged as peaks of larger regions
with trend‒like behavior; see Fig 11 for details.

59
Fig 11 Voxelwise partial correlation between DTI measures and neuropsychological tests
Maps of positive (red‒yellow) and negative (blue‒green) partial correlation coefficients in the DARTEL
Template space overlaid on a single subject T1‒weighted image (shown following neurological convention,
i.e. left side on left) show clear spatial trends of correlation between fractional anisotropy (FA) and PAL
Test values (Panel A), mean diffusivity (MD) and RAVLT values (Panel B), MD and ACE score values
(Panel C) and MD and Trail Making Test scores (Panel D). Smaller clusters of few voxels with correlations
deemed significant with FWE or FDR corrections are all located at the focal points of larger regions
achieving significance at exploratory thresholds ((1– 𝑝) > 0.999).

60
The small clusters of significant correlations (p‒values in the order of 10-7) were
identified as peaks of trend‒like behavior, (as presented on Fig 11), therefore we chose
not to employ cluster size thresholding, but rather eliminate voxels that did not belong to
significant cluster with an exploratory threshold of p < 0.001, uncorrected. For example,
Panels B and C of Fig 11 demonstrate that the whole left parahippocampal gyrus exhibited
negative correlation (in correspondence with the underlying anatomical structure)
between MD and the RAVLT or ACE scores, where the peaks spanning a few voxels
were deemed significant after the strict correction for multiple comparisons.
1.1.2 Voxelwise ANOVA and between-group differences
Between-group comparison of mean diffusivity values yielded several significant
results with FWE correction, while no regions showed significantly different FA. The
one‒way ANOVA confirmed MD differences in seven clusters of voxels, with p‒values
below 2.3×10-6. A list of all the resulting clusters is summarized in Table 4; the largest
and easily interpreted ones are once again presented in the following paragraphs with
MNI‒coordinates and T‒values of their peaks.
Seventeen regions showed increased MD in patients with aMCI compared to controls
(p < 2.3×10-6). A left inferior temporal cluster of 206 voxels ([-47, -9, -35], T = 6.5) and
a right middle temporal cluster of 72 voxels ([59,-33,-3], T = 5.8) were the largest and
most significant (Fig 12/ Panel A and B), while another cluster in the left superior frontal
gyrus had 12 voxels (Fig 12 / Panel C; [-15, 28, 50], T = 5.6).
Higher MD in the naMCI group compared to the controls was confirmed with the
post‒hoc T‒tests, in a precuneal ([-9, -66, 52], T = 7) and a smaller temporal ([-50, -9, -
39], T = 5.4) cluster (124 and 3 voxels, p < 8.5×10-9), (Fig 12 / Panel D), however, no
significant difference was identified between the DTI scalar values of the two groups of
MCI patients on the voxel level.
As expected, all the regions deemed significant with FWE correction emerged as
peaks of the T‒score “landscape” (Fig 13): focal points of regions with trend‒like MD
differences.

61
Table 4 Results of the voxelwise ANOVA and between group differences
FA-smoothed
Number of
clusters Peak p
Cluster size
[voxels] F/T-score Region [175]
ANOVA - - - - -
aMCI > Control - - - - -
naMCI > Control - - - - -
MD-smoothed
Number of
clusters Peak p
Cluster size
[voxels] F/T-score Region [175]
ANOVA 7 2.3 × 10−6
130 28.3 Precuneus L [-10,-68,49]
17 18.7 Frontal Sup L [-14, 28,51]
15 16.9 Temporal Mid R [59,-33,-3]
67 21.6 Temporal Inf L [-48, -7, -39]
25 21.9 Temporal Inf L [-58,-11,-32]
13 18.6 Supra Marginal L [-56, -49, 33]
aMCI > Control 17 2.3 × 10−6
206 6.5 Temporal Inf L [-47,-9,-35]
13 5.5 Fusiform L [-30,-43,-19]
39 5.2 Fusiform L [-25,-34,-14]
72 5.8 Temporal Mid R [59,-33,-3]
3 5.3 Cingulum Post R [3,-48,32]
4 5.4 Angular L [-55,-50,34]
4 5.3 Supra Marginal R[50, -41, 40]
4 5.4 Supra Marginal R[61, -23, 39]
26 6.0 Frontal Mid L [-31, 23,41]
12 5.6 Frontal Sup L [-15, 28,50]
43 6.0 Precuneus L [-9,-68,50]
39 5.5 Precuneus L [-14,-50,62]
4 5.4 Parietal Inf L [-52,-49,38]
naMCI > Control 2 8.5 × 10−9 124 7 Precuneus L [-9,-66,52]
3 5.4 Temporal Inf L [-50,-9,-39]
FA: fractional anisotropy, MD: mean diffusivity, Peak p: the peak p‒value in a cluster in voxelwise
calculations, ANOVA: analysis of variance, MCI: amnestic mild cognitive impairment, naMCI: non
amnestic mild cognitive impairment, [175]: coordinates in Montreal Neurological Institute template space.

62
Fig 12 Significant results of the voxelwise between group analyses
Between‒group, two sample T‒tests identified regions of higher mean diffusivity (MD) in the left inferior
temporal gyrus (A), the right middle temporal gyrus (B), and the left superior frontal gyrus (C) in the
amnestic MCI group, and also in the left precuneus (D) in the non‒amnestic MCI group, compared to
healthy control subjects. Maps showing clusters with significant (FWE corrected on voxel level) differences
transformed to MNI152 space and overlaid on a single subject T1‒weighted image, shown following
neurological convention (left side on left). Small clusters of significant differences all emerge as peaks of
larger regions with trend‒like behavior; see Fig 13 for details.

63
Fig 13 T‒score ‘landscape’ of the voxelwise between group comparisons
Between‒group, two sample T‒tests identified regions of higher mean diffusivity (MD) values in the left
inferior temporal gyrus (A), the right middle temporal gyrus (B), and the left superior frontal gyrus (C) in
the amnestic MCI group, and also in the left precuneus (D) in the non‒amnestic MCI group, compared to
healthy control subjects. Raw T‒score maps in the DARTEL Template space overlaid on a single subject
T1‒weighted image (shown following neurological convention, i.e. left side on left) reveal regions of higher
MD values with clear maxima in locations deemed significant.

64
1.2 ROI‒based analyses
1.2.1 ROI‒based correlations with the results of the neuropsychology tests
Both FA and MD in the left cingulum and in the left stria terminalis / left crus of the
fornix correlated with the RAVLT total scores, with the total adjusted trials in the PAL
test, and with the total and verbal fluency scores of the ACE. The results are summarized
in Fig 14. After correction for age the correlation between RAVLT total score and MD in
the left cingulum (Pearson partial R = ‒0.41 (Spearman partial R = ‒0.39), n = 65,
p = 0.0008), and the correlation between the PAL test result and MD in the left stria
terminalis / left crus of the fornix (Pearson partial R = 0.51 (Spearman partial R = 0.47),
n = 54, p = 0.0001) remained significant. Furthermore, the correlations of the RAVLT
(Pearson partial R = 0.43 (Spearman partial R = 0.43), n = 65, p = 0.0004) and the verbal
fluency subscore of the ACE (Pearson partial R = 0.40 (Spearman partial R = 0.48), n =
65, p = 0.001) with FA in the left cingulum were found significant, while correlation of
the ACE total score with FA in the left cingulum did not reach the level of significance
(Pearson partial R = 0.39 (Spearman partial R = 0.44), n = 65, p = 0.0015).

65
Fig 14 Results of the correlation analyses between DTI measures and neuropsychological tests
Results of the correlation analyses between the average values of mean diffusivity (MD) and fractional
anisotropy (FA) in the ROIs covering the left cingulum and the left crus of the fornix, and the results of the
four neuropsychological tests. (The Rey Verbal test, which measures verbal memory, the PAL – Paired
Associates Learning – test, that measures visual memory, the ACE – Addenbrooke’s Cognitive
Examination –, a comprehensive measure of cognitive functions, and a relevant subscore of the ACE test,
measuring verbal fluency). Different colors represent the three study groups. All correlations are corrected
for multiple comparisons. Correlations remained significant after correction for age are marked with
asterisk. Trend lines in black are fitted for the whole sample.

66
1.2.2 ROI‒based between group differences
Fractional anisotropy of the left cingulum (hippocampal subdivision) was
significantly decreased in the aMCI group relative to the control group (F(1, 44) = 20.4,
p < 0.0001) and to the naMCI group (F(1, 37) = 15.7, p < 0.0004), while FA did not
differ between controls and naMCI subjects (p > 0.05); (lower left panel of Fig 15). Mean
diffusivity of the left cingulum was significantly increased in the aMCI group relative to
controls (F(1, 44) = 19.8, p < 0.0001) and subjects with naMCI (F(1, 37) = 12.5,
p < 0.0012). Again, controls and naMCI subjects did not differ from each other (upper
left panel of Fig 15). Furthermore a tendency level difference in MD was detected
between controls and aMCI patients in the left stria terminalis and the left crus of the
fornix (p = 0.0041; upper right panel of Fig 15), with a similar but non‒significant pattern
of differences regarding FA (lower right panel of Fig 15).

67
Fig 15 Between‒group differences in fractional anisotropy (FA) and mean diffusivity (MD)
Mean values of fractional anisotropy (FA) and mean diffusivity (MD) in the three subject groups in two
regions of interest (ROIs) show between‒group differences from the post‒hoc tests following the Analysis
of Covariance (ANCOVA) calculations, with age and gender as covariates. The ‘Left Cingulum‒
Hippocampus’ ROI showed significant differences after Bonferroni’s correction for multiple comparisons
(marked with asterisks) between the amnestic mild cognitive impairment (aMCI) and control groups; while
the ‘Stria Terminalis/Left Crus of the Fornix’ only contained nominal differences in MD and FA, not
significant after Bonferroni’s correction.
1.3 ROI‒based logistic regression analysis: combined cortical thickness and DTI‒based
differentiation between study groups
In the first set of stepwise logistic regression models, only cortical thickness
measurements and subcortical brain structure volumes were entered as variables.
Structures with the largest discriminatory power (a Cohen’s d of at least one, i.e. more
than one SD difference between study groups) were used as input [110], namely the
volume of the hippocampus, the cortical thickness of the entorhinal cortex, the fusiform
gyrus, the precuneus, and the isthmus of the cingulate gyrus.
These volumetric and thickness measurements of grey matter structures were
amended with the FA and MD measurements of the 36 WM ROIs (i.e. tracts) in the
second and third sets of models, separately. Categorization results of each model, when

68
tested on the independent, albeit small test subsets are summarized in Table 5‒Table 13
and detailed on the subject level in the supplementary Tables S1-S9; the following
subsections contains a brief overview.
1.3.1 Differentiation between aMCI subjects and healthy controls
The volume of the left (in 8 out of the 10 training subsets) or the right (in the remaining
2 subsets) hippocampus stayed in the models after the stepwise logistic regression, based
solely on volumetric measures; the former extended by the cortical thickness of the
precuneus in three subsets. Overall, 78.95% of the subjects was categorized correctly
across the subsets. (Table 5)
The average FA of the aforementioned WM structures did not stay in the models after
stepwise logistic regression, in any but the last subset, where the average FA of the ‘stria
terminalis / left crus of the fornix’ was selected as a potential measure with substantial
difference , however, the overall categorization performance did not change. With the
second test‒subgroup, the volume of the right hippocampus was replaced by the volume
of the left hippocampus, once again, with no resulting effect on categorization. (Table 6)
None of the MD measurements remained in the third set of models, thus the original
GM‒volumetric models were not improved by including DTI this way, however,
categorization of the second test‒subgroup was slightly improved (one more correct
decision) with the average cortical thickness of the precuneus, raising overall correct
categorization to 81.58% across subsets. (Table 7).

69
Table 5 Logistic regression: amnestic MCI vs. Control – only volumetry
Test set no. Effect1 Effect2 Ratio
1 Left
HippocampusV
Meanthickavg
precuneusT 0.75
2 Right
HippocampusV 0.25
3 Left
HippocampusV 1
4 Left
HippocampusV 0.5
5 Left
HippocampusV Meanthickavg
precuneusT 0.75
6 Left
HippocampusV 1
7 Left
HippocampusV 1
8 Right
HippocampusV 1
9 Left
HippocampusV 1
10 Left
HippocampusV
Meanthickavg
precuneusT 0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Effect1
& 2: volumetric, or cortical thickness measurements deemed meaningful in the stepwise logistic regression;
Meanthickavg: average cortical thickness; Ratio: decision performance in each subgroup.
V: volumetry‒based measure T: thickness‒based measure

70
Table 6 Logistic regression: amnestic MCI vs. Control – volumetry with FA
Test set no. Effect1 Effect2 Effect3 Ratio
1 Left
HippocampusV
Meanthickavg
precuneusT
0.75
2 Left
HippocampusV
0.25
3 Left
HippocampusV
1
4 Left
HippocampusV
0.5
5 Left
HippocampusV
Meanthickavg
precuneusT
0.75
6 Left
HippocampusV
1
7 Left
HippocampusV
1
8 Right HippocampusV
1
9 Left
HippocampusV
1
10 Left
HippocampusV
Meanthickavg
precuneusT
Fornix crus
Stria terminalis LDTI 0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data; Effect1,
2 & 3: volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic
regression; Meanthickavg: average cortical thickness; Ratio: decision performance in each subgroup;
V: volumetry‒based measure; T: thickness‒based measure; DTI: DTI‒based measures

71
Table 7 Logistic regression: amnestic MCI vs. Control – volumetry with MD
Test set no. Effect1 Effect2 Ratio
1 Left
HippocampusV
Meanthickavg
precuneusT 0.75
2 Left
HippocampusV
Meanthickavg
precuneusT 0.5
3 Left
HippocampusV
1
4 Left
HippocampusV
0.5
5 Left
HippocampusV
Meanthickavg
precuneusT 0.75
6 Left
HippocampusV
1
7 Left
HippocampusV
1
8 Right
HippocampusV
1
9 Left
HippocampusV
1
10 Left
HippocampusV 0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data.; Effect1
& 2: volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic
regression; Meanthickavg: average cortical thickness; Ratio: decision performance in each subgroup;
V: volumetry based measure; T: thickness based measure

72
1.3.2 Differentiation between naMCI subjects and healthy controls
Volumetry‒ and thickness‒based models with each but one test‒subset included the
average cortical thickness of the precuneus, with the only other meaningful measure being
the volume of the right hippocampus. (Table 8)
Adding the FA measures to the models resulted in having the average values measured
in the fornix (body and column), the posterior thalamic radiation, the right or left external
capsule, or the right superior fronto‒occipital fasciculus staying in the model, separately,
each of them in some of the test subsets, however, the original overall 52.63%
categorization performance was once again only slightly improved (to 55.26%, meaning
only two more correct decisions). (Table 9)
Average MD of the left cingulum (hippocampus), the left external capsule, or the
fornix (body and column) was also found meaningful for few of the models, yet the
overall categorization performance was only slightly improved, with 3 more correct
decisions in total (57.89% of all subjects). (Table 10)

73
Table 8 Logistic regression: non‒amnestic MCI vs. Control – only volumetry
Test set no. Effect1 Effect2 Ratio
1 Meanthickavg
precuneusT 0.5
2 Right
HippocampusV Meanthickavg
precuneusT 0.5
3 Meanthickavg
precuneusT 0.5
4 Meanthickavg
precuneusT 0.5
5 Meanthickavg
precuneusT 0.75
6 Right
HippocampusV
Meanthickavg
precuneusT 0.5
7 Right
HippocampusV 0.5
8 Meanthickavg
precuneusT 0.5
9 Meanthickavg
precuneusT 0.5
10 Meanthickavg
precuneusT
0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data; Effect1
& 2: volumetric or cortical thickness measurements deemed meaningful in the stepwise logistic regression;
Meanthickavg: average cortical thickness; Ratio: decision performance in each subgroup;
V: volumetry based measure; T: thickness based measure

74
Table 9 Logistic regression: non‒amnestic MCI vs. Control – volumetry with FA
Test sett no. Effect1 Effect2 Effect3 Ratio
1 Meanthickavg
precuneusT
Fornix column
& body of fornixDTI 0.75
2 Right
HippocampusV Meanthickavg
precuneusT 0.5
3 Meanthickavg
precuneusT
Posterior thalamic
radiation RDTI
External
capsule RDTI 0.25
4 Meanthickavg
precuneusT
External
capsule_RDTI 0.5
5 Meanthickavg
precuneusT Fornix column
& body of fornixDTI Superior fronto occipital
fasciculus RDTI 1
6 Cingulum
hippocampus LDTI 0.25
7 Right
HippocampusV 0.5
8 Meanthickavg
precuneusT
External
capsule LDTI Tapetum LDTI 0.5
9 Meanthickavg
precuneusT
Fornix column
& body of fornixDTI 0.75
10 Meanthickavg
precuneusT
External
capsule LDTI 0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data.;
Effect1, 2 & 3: volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise
logistic regression; Meanthickavg: average cortical thickness; Ratio: decision performance in each
subgroup; V: volumetry based measure; T: thickness based measure; DTI: DTI‒based measure

75
Table 10 Logistic regression: non‒amnestic MCI vs. Control – volumetry with MD
Test set no. Effect1 Effect2 Ratio
1 Meanthickavg
precuneusT
Cingulum
hippocampus LDTI 0.5
2 Right
HippocampusV
Cingulum
hippocampus LDTI 0.25
3 Meanthickavg
precuneusT 0.5
4 Meanthickavg
precuneusT
Cingulum
hippocampus LDTI 0.75
5 Meanthickavg
precuneusT
Cingulum
hippocampus LDTI 0.75
6 Right
HippocampusV
Meanthickavg
precuneusT 0.5
7 Right
HippocampusV 0.5
8 Meanthickavg
precuneusT
External
capsule LDTI 0.75
9 Meanthickavg
precuneusT
Fornix column
& body of fornixDTI 0.75
10 Meanthickavg
precuneusT
External
capsule LDTI 0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data; Effect1,
2 & 3: volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic
regression; Meanthickavg: average cortical thickness; Ratio: decision performance in each subgroup;
V: volumetry based measure; T: thickness based measure; DTI: DTI‒based measure

76
1.3.3 Differentiation between aMCI and naMCI subjects
The same volume and cortical thickness measures were entered into the first set of
models as in the former comparisons, once again followed by adding the average DTI
scalar values of the same ROIs as before. (Table 11)
The first set of stepwise logistic regression calculations (only volumetric and
thickness measurements) all identified the volume of the left hippocampus as the only
meaningful effect, and achieved an overall 63.89% correct categorization performance
(23 subjects out of the 36) in the nine separate models.
After adding FA measurements of WM ROIs, the average value in the ‘stria terminalis
/ left crus of the fornix’ stayed as a relevant effect in all nine models; interestingly the
volume of the left hippocampus was replaced by the volume of the right hippocampus in
two of the models.
This addition of the average FA of this specific WM region improved correct
categorization with all but one test subsets, resulting in an overall 86.11% (31 correct
decisions out of 36) categorization performance, a solid 22.22% (8 subjects) increase
compared to the solely volumetry‒based models. (Table 12)
Average MD values of the body of the corpus callosum (8 models) or the column and
body of the fornix (one model) also improved the categorization performance in the final
sets of models: together with the volume of the left hippocampus, 75% (27 out of 36) of
subjects were categorized correctly.(Table 13)

77
Table 11 Logistic regression: amnestic vs non‒amnestic MCI – only volumetry
Test set no. Effect1 Ratio
1 Left
HippocampusV 0.5
2 Left
HippocampusV 0.5
3 Left
HippocampusV 1
4 Left
HippocampusV 0.5
5 Left
HippocampusV 0.25
6 Left
HippocampusV 1
7 Left
HippocampusV 0.75
8 Left
HippocampusV 0.75
9 Left
HippocampusV 0.5
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Effect1:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
Ratio: decision performance in each subgroup; V: volumetry based measure

78
Table 12 Logistic regression: amnestic vs non‒amnestic MCI – volumetry with FA
Test set no. Effect1 Effect2 Ratio
1 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 0.75
2 Right
Hippocampus V
Fornix crus
Stria terminalis L DTI 1
3 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 1
4 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 0.25
5 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 1
6 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 1
7 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 1
8 Right
Hippocampus V
Fornix crus
Stria terminalis L DTI 1
9 Left
Hippocampus V
Fornix crus
Stria terminalis L DTI 0.75
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data.
Effect1&2: volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise
logistic regression; Ratio: decision performance in each subgroup; V: volumetry based measure; DTI: DTI‒
based measure

79
Table 13 Logistic regression: amnestic vs non‒amnestic MCI – volumetry with MD
Test set no. Effect1 Effect2 Mean
1 Left
Hippocampus V
Body of corpus
callosum DTI 0.5
2 Left
Hippocampus V
Body of corpus
callosum DTI 1
3 Left
Hippocampus V
Body of corpus
callosum DTI 1
4 Left
Hippocampus V
Body of corpus
callosum DTI 0.25
5 Left
Hippocampus V
Fornix column
& body of fornix DTI 0.5
6 Left
Hippocampus V
Body of corpus
callosum DTI 0.75
7 Left
Hippocampus V
Body of corpus
callosum DTI 1
8 Left
Hippocampus V
Body of corpus
callosum DTI 1
9 Left
Hippocampus V
Body of corpus
callosum DTI 0.75
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data.
Effect1&2: volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise
logistic regression; Ratio: decision performance in each subgroup; V: volumetry based measure; DTI: DTI‒
based measure

80
2. Mahalanobis‒distance in MCD lesion detection
The squared Mahalanobis-distance (D2) and the critical values used for inference were
calculated using in-house algorithms following (Eq. 10) and (Eq. 11). The analytical
derivation uses the number of observations, dimensions, and desired level of significance;
the appropriate critical values were determined for each application.
The FWE‒corrected, D2 critical value, calculated from n = 46, p = 3, and 𝛼𝐹𝑊𝐸 =
0.05
#𝑣𝑜𝑥𝑒𝑙𝑠=
0.05
3.4054×105 = 1.4683 × 10−7 was 27.8324. This value was used in simulations
and subject evaluations.
As FDR correction uses the p‒values of each statistical test and determines the critical
p for a given set (the tests in each voxel, in our case), the FDR corrected D2 critical values
were unique for each patient image, typically in the range between 19 and 21.
Groupwise average values and standard deviation for the whole grey and white matter
of the coregistered eigenvalue maps from the controls are included in Table 14, while
their spatial distributions are presented in Fig 16.
Table 14 Mean values and standard deviations of the tensor eigenvalues
Grey Matter White Matter
Mean SD Mean SD
λ1 1.1295 × 10−3 2.3623 × 10−4 1.2117 × 10−3 2.5012 × 10−4
λ2 9. 3691 × 10−4 2.1694 × 10−4 8.0431 × 10−4 1.6876 × 10−4
λ3 8.1112 × 10−4 2.1290 × 10−4 6.0377 × 10−4 1.7571 × 10−4
Means and standard deviations (SD) of the DTI eigenvalues, averaged over the control sample, in the whole
grey and white matter, presented in units of mm2/s.
During manual revision of the results of independent lesion detection with the MAP07
toolbox, only 11 abnormalities were identified in the example cases, thereby the
remaining lesion masks were entirely hand drawn.

81
Fig 16 Spatial distribution of the sample‒wise mean and standard deviation of the coregistered
eigenvalue maps from the controls.
Mean values (left column) and standard deviations (right column) are presented on the same respective
scales for the three diffusion tensor eigenvalues in units of mm2/s.

82
2.1 SMVND simulations
2.1.1 False Positives
In the simulations with SMVND data, false positives were identified in all cases when
no cluster size thresholding was employed, with both FWE and FDR corrected critical
values. On the contrary, no false positives were identified with thresholds larger than 4
voxels, meaning that for simulated lesions with voxel values from standard Gaussian
distribution, and sizes that are reasonable to assume any true malformation would have,
the method had 100% specificity.
2.1.2 True positive rates and hit rates
AUC values, calculated for each lesion size‒CNR parameter pair, with both FWE and
FDR corrected critical values are summarized in Table 15 for both definitions of true
positives (AFROC curves can be seen in Fig 17). As expected, with increasing CNR and
lesion sizes, both the TPR and the TPRB (hit rate) increased.
Table 15 AUC value results of the simulations with SMVND data
SMVND
FDR
Lesion size [vox] → 19 35 50 100 200
CNR ↓ AUC AUC
Binary AUC
AUC Binary
AUC AUC
Binary AUC
AUC Binary
AUC AUC
Binary
2σ 0.000 0.000 0.000 0.004 0.000 0.003 0.000 0.005 0.001 0.011
1 FWHM 0.296 0.593 0.339 0.840 0.349 0.941 0.368 0.998 0.382 1.000
3σ 0.660 0.953 0.702 0.998 0.713 0.999 0.736 1.000 0.752 1.000
2 FWHM 0.996 1.000 0.998 1.000 0.999 1.000 0.999 1.000 0.999 1.000
FWE
Lesion size [vox] → 19 35 50 100 200
CNR ↓ AUC AUC
Binary AUC
AUC Binary
AUC AUC
Binary AUC
AUC Binary
AUC AUC
Binary
2σ 0.000 0.000 0.000 0.004 0.000 0.003 0.000 0.005 0.000 0.011
1 FWHM 0.158 0.593 0.185 0.840 0.201 0.941 0.216 0.998 0.222 1.000
3σ 0.493 0.953 0.536 0.998 0.555 0.999 0.576 1.000 0.580 1.000
2 FWHM 0.984 1.000 0.991 1.000 0.994 1.000 0.995 1.000 0.996 1.000
Area under the curve (AUC) values resulting from the alternative free‒response receiver‒operator
characteristics curves (AFROC) of simulations with standard multivariate normal distribution (SMVND)
data, FDR and FWE corrected critical values, and following both the fractional and binary definition of true
positive rate (TPR); calculated from the [0; 0.05] false positive rate (FPR) range.

83
Fig 17 Alternative free‒response receiver‒operator characteristic (AFROC) curves of the simulations
with standard multivariate normally distributed (SMVND) data.
Results with both FWE‒ and FDR‒corrected critical values, following both definitions of true positives
(fraction of positive voxels – TPR – and hit rates – TPRB), with all different values for simulated lesion
size and effect strength (contrast to noise ratio) are presented.

84
In the [0; 0.05] FPR interval, all AUC values exceeded 84% in lesion detection, with
lesion sizes above 19 voxels and CNR above 1 FWHM, using either FDR or FWE‒
corrected critical values. More than half of the lesion voxels were identified with CNR >
3σ, with all lesion sizes and critical values (except for the smallest lesions and FWE
correction, were the AUC was 0.493).
2.2 Real Eigenvalue simulations
2.2.1 False Positives
Simulations based on real DTI eigenvalue data resulted in similar behavior of false
positives: every case showed false positive clusters with a minimum size of one or two
voxels, but with cluster size thresholds of 6 (with FWE‒correction) or 7 (with FDR‒
correction) voxels, FPR decreased to 0.1 ‒ 0.3% (i.e. 1 ‒ 3 false positives per sets of 1000
simulations).
2.2.2 True positive rates and hit rates
The resulting AUC values are summarized in Table 16; AFROC curves are presented
in Fig 18.
Lesion identification performance (Binary AUC) was above 70% with CNR =
1FWHM in cases of lesions larger than 50 voxels, or with CNR = 3σ and at least 35 voxels,
using either FDR, or FWE‒corrected critical values. More than half of the lesion voxels
were identified at CNR = 2FWHM, achieving 77.3 ‒ 85.9% AUC with FDR‒corrected,
and 75.1 ‒ 77.8% AUC with FWE corrected critical values.
Based on these simulation results, we expected the proposed method to identify the
abnormal diffusion profile of MCDs in patients. A seven-voxel large cluster size threshold
was used in subsequent analyses, first with FDR‒corrected critical values, but the latter
were replaced by the FWE-corrected ones, as described in 2.3.1.

85
Table 16 AUC value results of the simulations with Real Eigenvalue data
Real Eigenvalues
FDR
Lesion size [vox] → 19 35 50 100 200
CNR ↓ AUC AUC
Binary AUC
AUC
Binary AUC
AUC
Binary AUC
AUC
Binary AUC
AUC
Binary
2σ 0.000 0.000 0.000 0.000 0.000 0.001 0.000 0.002 0.001 0.018
1 FWHM 0.161 0.299 0.228 0.533 0.229 0.596 0.248 0.702 0.272 0.863
3 σ 0.430 0.637 0.450 0.756 0.414 0.740 0.456 0.884 0.463 0.939
2 FWHM 0.773 0.858 0.843 0.940 0.859 0.960 0.822 0.920 0.818 0.920
FWE
Lesion size [vox] → 19 35 50 100 200
CNR ↓ AUC AUC
Binary AUC
AUC
Binary AUC
AUC
Binary AUC
AUC
Binary AUC
AUC
Binary
2σ 0.000 0.000 0.000 0.000 0.000 0.001 0.000 0.001 0.000 0.001
1 FWHM 0.108 0.221 0.141 0.403 0.160 0.544 0.168 0.696 0.166 0.752
3σ 0.337 0.598 0.353 0.712 0.352 0.745 0.356 0.835 0.353 0.946
2 FWHM 0.751 0.947 0.776 0.998 0.778 0.999 0.777 1.000 0.760 0.980
Area under the curve (AUC) values resulting from the alternative fractional receiver operating
characteristics curves (AFROC) of real eigenvalue simulations with FDR and FWE corrected critical values
and following both the fractional and binary definition of true positive rate (TPR); calculated from the [0;
0.05] false positive rate (FPR) range.

86
Fig 18. Alternative fractional receiver operating characteristics (AFROC) curves corresponding to
the simulations based on real diffusion tensor eigenvalue data.
Results with both FWE‒ and FDR‒corrected critical values, following both definitions of true positives
(fraction of positive voxels –TPR– and hit rates –TPRB), with all different values for simulated lesion size
and effect strength (contrast to noise ratio) are presented.

87
2.3 Real data examinations
2.3.1 Leave‒one‒out analysis of controls
The FDR‒corrected critical values resulted in an average of 21.11 (5 ‒ 55)
clusters/subject, while the more conservative FWE‒correction yielded 4.93 (0 ‒ 13)
clusters in average, 1.79 (0 ‒ 5) of those being in the WM. Based on this result, combined
with the observation that the true positive clusters in subsequent patient examinations
were also present with the more conservative approach (Fig 19), we decided to only use
critical values aimed to control the FWE for patient examinations, decreasing the
influence of inherent variability and/or coregistration inaccuracy.
Fig 19 Comparison of the results with FDR and FWE corrected critical values.
Thresholded and clustered D2‒results overlaid on the T1‒weighted image of a 27 y.o. male patient with
polymicrogyria in the basal region of the left inferior frontal gyrus (see panel D of Fig 21, as well.) Coronal
slices presented in neurological orientation, i.e. left side is on the left, slices of the 2D FLAIR image were
angulated perpendicular to the axes of the hippocampi.
After removing clusters based on the δ‒values (those with more than half of the voxels
with δ > 0.1), the number of remaining clusters decreased to an average of 2.79 (0‒7)
with an average size of 16.21 voxels (7‒167), meaning, that most of those resulting from
insufficient coregistration or normal differences in gyrification patterns (mainly located
in the CSF) were filtered out. Examples of the resulting few minimal cluster‒masks
overlaid on each control subject’s T1‒weighted images are shown on Fig 20.

88
Fig 20 Examples of the observed clusters in the leave‒one‒out examinations of healthy control
subjects, using critical values corrected for controlling the FWE rate.
Cluster masks (green with arrows) overlaid on each individual’s T1‒weighted image. Typical clusters that
remained after the filtering steps, emerged deep in the sulci or close to the GM‒CSF boundary (A, B, C,
and D) with small sizes (16.21 voxels in average), and also in the WM in some cases (E, F). Axial and
coronal slices are presented in neurological orientation, i.e. left side is on the left.

89
2.3.2 Patient Examination
After applying the previously detailed processing steps to the 16 D2‒images of the 13
patients, on average 59.4 (35 ‒ 90) clusters per subject were identified with an average
size of 31.4 (7 ‒ 680) voxels (after removing 6 larger clusters emanating from missing
cerebellar slices). The majority of these clusters were obvious artefacts, identifiable by
their shape and location (e.g. in the occipital lobes, close to and following the GM‒CSF
boundary, independent of the underlying gyral and sulcal pattern), see Discussion.
Examples of resulting clustered D2‒images are shown on the rightmost panels of Fig 21,
along with coronal FLAIR images, MAP07 junction maps and the raw D2‒images
overlaid on each subject’s T1‒weighted image. Regions with outlying diffusion
properties, corresponding to 22 (out of the 23) MCDs and other abnormalities were
identified in the patient group, in good spatial concurrence with the neuroradiological
evaluation and the lesion masks. The remaining, 23rd, an FCD‒type malformation only
resulted in two supra‒threshold voxels, subceeding cluster size threshold; it was only
identified when using the less conservative, FDR‒corrected critical values. The (physical)
distances between centers of masses of the resulting D2‒clusters and the lesion masks are
summarized in Table 17.
Table 17 Positive clusters in select cases of MCDs
Code P01 P02 P03 P04 P05 P05 P05
P06 S1 S2 S3
Number of
positive
clusters
1 3 1 1 3 3 7 2
Average
distance (min-max) [mm]
12.2 18.8
6.5 13.6 13.6 10.4 19.0 19.6
(12.9-25.7) (9.44-17.2) (5.1-17.1) (9.5-29.2) (3.7-35.4)
Code P07 P08 P09 P10 P11 P11
P12 P13 S1 S2
Number of positive
clusters
1 1 2 3 1 1 2 4
Average
distance (min-max) [mm]
13.5 11.9 12.1 12.1
7.7 7.7 4.3 17.6
(6.7-17.6) (3.5-9.9) (2.3-6.3) (10.2-24.1)
Number of positive D2‒clusters, presented with the average, minimum, and maximum center-of-mass
distances between the clusters and the lesion masks [mm]

90
Fig 21 Example results in select cases of abnormalities
Coronal 2D FLAIR images, and MAP07 junction maps, raw, and final, clustered D2‒images (red) and lesion
masks (green) overlaid on T1‒weighted images in select cases: presumed right superior temporal FCD or
PMG and hippocampal sclerosis (panel A); cortical dysplasia and presumed PMG in the right medio‒frontal
part of the cingular gyrus (panel B); dysgenesis and partial sclerosis of the left hippocampus (panel C);
presumed PMG or FCD in the basal region of the left inferior frontal gyrus and the posterior pat of the
insula (panel D); and left hippocampal sclerosis (panel E). Coronal slices presented in neurological
orientation, i.e. left side is on the left, coronal slices of the 2D FLAIR images were angulated perpendicular
to the hippocampi.

91
V. Discussion
1. DTI and Mild Cognitive Impairment
In the first study, two independent statistical approaches were applied consecutively,
in order to establish the findings, starting from the exploratory whole brain analysis on
voxel‒level and then identifying the strongest white matter differences on the more robust
ROI‒level, to be used later in differentiation between study groups by means of logistic
regression. Voxelwise analysis confirmed decreased grey and white matter integrity in
aMCI subjects compared to healthy controls and naMCI subjects; moreover, increased
MD was found in naMCI subjects relative to controls. Decreased WM integrity (as
indexed by MD and FA) was correlated with short‒term memory performance and verbal
fluency in the whole sample, further confirming the sufficiency of the study material in
making inferences about MCI.
Based on previous evidence [118, 119], the most prominent between group
differences and the strongest correlations with memory functions were expected in the
cingulum and the fornix; this hypotheses was also confirmed in our ROI‒based
calculations, and utilized in improving differentiation between study groups in logistic
regression analysis.
Use of the widely acknowledged tract based spatial statistics (TBSS) [78] method was
considered for its higher statistical power, but due to its limited volume of inference and
poor spatial registration performance in complex WM structures — also see section 1.3
— this option was omitted.
1.1 Functional‒structural correlations
Correlations between DTI measures and memory performance in subjects with MCI
and the elderly has been confirmed in previous studies. For example, in [176], a link
between the ADC in the medial temporal lobe and verbal recall was identified, using
rectangular, hand drawn ROIs, and a correlation between ‘composite memory’ and the
FA of large parts of the frontal and occipital WM in a TBSS analysis was found in [177].
Similarly, our calculations confirmed that more severe cognitive impairment (indexed by

92
decreased performance in the neuropsychological tests) is linked to altered diffusion
profile in several GM and WM regions.
Voxelwise analysis revealed negative correlation between the ACE total score (a
comprehensive index of cognitive performance), and increased MD in the left
parahippocampal region and in the pole of the left middle temporal gyrus, regions
demonstrated to show early neuropathological changes in AD, as demonstrated by
histological [178] and volumetry [179] studies. Verbal memory (indexed by the Rey test)
also showed significant correlation with MD in the left parahippocampal region, while
the PAL test, reflecting visual and working memory performance correlated with FA in
the pars triangularis of the left inferior frontal gyrus (Brodmann area 45, a part of the
ventrolateral prefrontal cortex —VLPFC, which has a role in semantic tasks and the
cognitive control of working memory [180]).
Visuospatial attention as indexed by the Trail Making test (part A) correlated with
MD in the angular gyrus, which is associated with orienting attention to salient features
in space [181, 182]. Each of the small clusters with significant differences or correlations
were identified as focal points of larger volumes with relatively high R‒scores, achieving
significance at exploratory thresholds (e.g. T > 3, or |R| > 0.4, p < 0.001) (Fig 10 and Fig
11), supporting the statement that our voxelwise results are pinpointing the key
anatomical structures associated with cognitive impairment.
The voxelwise calculations identified the strongest correlation in voxels around the
GM‒WM boundary, mainly belonging to subcortical WM (in agreement with the
aforementioned histological findings [178]), pointing towards the hypothesis that
pathological changes in the fiber pathways of the temporal WM, assumed to precede the
atrophy of the hippocampus or the entorhinal cortex [179, 183, 184] might be the reason
behind the early evincible cognitive impairment.
The more robust ROI‒level approach strengthened these findings, by identifying
similar correlation between decreased average FA values (decreased WM integrity) in the
left cingulum and decreased verbal memory performance (as indexed by the Rey test),
and decreased verbal fluency (as indexed by the ACE subscore). The left crus of the fornix
/ stria terminalis also showed decreased FA, correlated to visual memory performance as

93
indexed by the PAL test. These results confirmed that the expected microstructural
differences are present and significant in these ROIs therefore they might aid the
automated differentiation between subject groups.
1.2 Impairments in aMCI patients compared to naMCI patients and healthy controls
As described e.g. in [145], the cingulum, the fornix and the stria terminalis are C‒
shaped WM bundles, connecting the hippocampus to other parts of the limbic system,
such as the amygdala, mammillary bodies, septal area, and hypothalamus. The cingulum
also connects the hippocampus to the occipital, parietal, and frontal cortex, while the
fornix and the stria terminalis connects the amygdala to the cortex, and the former also
projects to the medial prefrontal cortex [185].
Similarly to how the structure of the fornix is affected in MCI [186], a disruption in
these WM tracts (increased MD and decreased FA) was detected in our study in patients
with aMCI, compared to healthy controls or patients with naMCI, in the ROI based
analysis. Meanwhile, voxelwise analysis confirmed these findings by showing increased
MD in the left and right temporal regions in aMCI patients relative to controls.
These results are also in line with previous investigations showing that “early
Alzheimer disease is underpinned by the damage of inter‒connected network, which
predominantly involves degeneration of the tracts connecting the circuit of Papez (limbic
system)” as stated in [166]. However, it is yet unclear if these disruptions in WM
connectivity are consequences or causes of disease progression. Changes in metabolism
and atrophy of the precuneus are also shown to be associated in Alzheimer’s disease and
MCI [187]. Similarly, our voxelwise analysis also confirmed its involvement, as
increased MD in left precuneal regions in aMCI patients. Additionally, MD was also
increased in the left frontal cortex of aMCI patients, where axon density was shown to
decrease in AD [188], but no significant differences were identified between the two MCI
groups.
In summary, both methods showed impairments in the temporal regions of patients of
the aMCI group, which is in line with results of numerous previous studies [118, 119,

94
189-191], while the voxelwise approach also found differences in the left frontal and
precuneal regions: differences also revealed by previous investigations [187, 188, 192].
1.3 Impairments in naMCI patients compared to control subjects
Voxelwise analysis showed increased MD in the left precuneus and in the left
temporal region in naMCI subjects, relative to controls. The precuneus is an important
hub of the default mode network, which is linked to several executive functions declined
in dementia [193]. These results are supported by previous DTI, brain metabolism (FDG‒
PET) and fMRI studies [124, 194, 195], however our ROI based analysis did not confirm
this difference, possibly because the ROI‒based analysis was limited to WM tracts (based
on an atlas [63, 145]), while the voxelwise analysis covered the GM as well.
1.4 Differentiation between study groups by logistic regression
Average FA and MD values, measured in the ‘cingulum (hippocampus)’ and the ‘stria
terminalis / left crus of the fornix’ ROIs, were identified to be correlated with cognitive
performance and to differ significantly between the study groups, thereby they were
hypothesized to be potential candidates to improve the volumetry‒based models’
differentiation performance when comparing study groups. A K‒fold cross‒validation
approach was used to test the discriminative models on small test samples, independent
from the data they were constructed on. The features selected by the logistic regression
in the separate models were mostly consistent; chance level discriminative performance
was exceeded in all cases.
Like previous investigations (e.g. in [196]) claiming that combined DTI and
volumetric/cortical thickness measurements can improve categorizations between
subjects with aMCI and controls, three sets of logistic regression models were compared
in our work. Without including DTI scalars, one or two volumetry- or thickness‒based
measures (the volume of the left hippocampus and the cortical thickness of the precuneus)
stayed as relevant effects in the final models. Incorporating ROI‒wise, average MD did
not change the overall outcome; indeed, all MD measures were excluded in the stepwise
regression. On the same token, FA measures were also excluded from all but one final
models. Thereby the introduction of DTI measures in the discriminative models did not

95
improve the approximately 80% categorization performance of volumetry and thickness
based models for discrimination between aMCI patients and healthy controls.
Similarly, three sets of logistic regression models were compared to test
discrimination performance between naMCI and controls. Only the cortical thickness of
the precuneus stayed in all of the models without DTI measures, yielding a low
discriminatory power. No further volumetric or DTI‒based measures could significantly
improve categorization, possibly because of the heterogeneous nature of the non‒
amnestic MCI subtype. A larger sample and the separation of the wide range of
underlying pathologies to meaningful subgroups seem to be necessary for stronger
inference.
Despite the lack of improvement of categorization performance in patient versus
control comparisons, introducing DTI measures had substantial benefit when
discriminating between the two MCI subtypes. Especially the FA of the left crus of the
fornix improved the models, raising correct categorization performance by 22.22%; in the
same token, the MD of the body of the corpus callosum resulted in 11.11% improvement
compared to volumetry‒derived models discriminating based on the volume of the left
hippocampus. Moreover, these two white matter regions were stable in the K‒fold cross
validation, further supporting their importance for future discriminative models, as well.
Note, that our strategy of transforming the predefined ROIs to each subject’s
anatomical space, is less susceptible to registration artefacts compared to similar studies
using coregistration to a common template space (e.g. MNI), therefore it can be
considered more precise, and if implemented properly, the improved categorization
performance may even be achievable for general clinical applications.
1.5 On the value of DTI measurements in MCI and AD
Here, we presented a series of results that represent different levels of description
from the voxel‒level, through ROI‒level to model‒level. Even though the results may
seem fragmented by the analysis methods there is a consistent pattern of WM involvement
that is present through all levels of description. Voxel‒level calculations demonstrated
both strong correlations between the performance in neuropsychology tests and MD

96
values and significant between‒group differences in MD values in GM areas that are
usually affected in Alzheimer’s disease in general, signaled by atrophy [115, 179, 184,
187]. These findings proved that the early involvement of these structures (most
prominently the hippocampus) was present in our sample and was readily detectable
through the altered diffusion profile.
Abnormal tissue microstructure in the hippocampal areas is likely to be accompanied
by measurable changes in the corresponding WM fiber pathways, as well [119, 170].
Although no meaningful clusters were identified in the white matter on the voxel level,
presumably due to the weaker sensitivity resulting from the highly conservative
thresholding (for proper voxel‒level correction for multiple comparisons), the expected
significant correlation with cognitive performance and between‒group differences were
demonstrated on the ROI‒wise average values in the cingulum (hippocampal subdivision)
and the stria terminalis / crus of the fornix ROIs in the left hemisphere.
ROI‒wise average FA and MD values of these two well‒defined, atlas‒based WM
regions were relatively simple to calculate in a straightforward manner. Moreover, as DTI
is most sensitive in the WM, these ROIs also exhibited stable and substantial differences
in between‒group comparisons. Furthermore, the average FA of the stria terminalis / crus
of the fornix also proved to be a relevant effect in the logistic regression analysis when
creating models for discrimination between aMCI and naMCI study groups, with the MD
of the body of the corpus callosum having similar relevance in improving discrimination
performance. Although the FA of the left cingulum was also found significantly decreased
in aMCI patients compared to controls, it was deemed to be irrelevant by logistic
regression, as left hippocampal volumetry proved to contain sufficient information for
correct categorization in itself.
1.6 Limitations of the study
While our results demonstrate the usefulness of DTI measures in improving
categorization between study groups, especially between aMCI and naMCI, the relatively
low sample sizes of the study may limit the generalizability of the findings. Nevertheless,
even the limited size of the study groups allowed the logistic regression analysis to be
performed on separate training and testing datasets using a K‒fold approach that clearly

97
showed stably increased categorization performance with the inclusion of DTI‒metrics,
despite the expected high variability with such low sample sizes. Further studies with
larger sample sizes would be beneficial to corroborate our results.
The cross‒sectional nature of the study can also be considered a major limitation, but
that can also be overcome with further (especially follow‒up) examinations that would
also allow for investigating the negative predictive value of including the DTI measures
in the discriminative models, providing additional means for confirming the presented
results.
2. Mahalanobis‒distance in MCD lesion detection
2.1 Multidimensional approaches
When selecting a multidimensional approach to combine different modalities, the
research question determines the level at which information is pooled, from group‒level,
through individuals, down to voxel‒based methods. Examining more general processes,
like response to stimulation in fMRI calls for ‘cohort level’ statistical methods, like
combining p‒value maps with pooling approaches in [81], or using the conjunction
method, testing a simultaneous null hypothesis [80].
Higher level information pooling has also been proven efficient in examining
systemic disorders of the CNS, e.g. for Alzheimer’s disease in [82], combining T‒score
maps from univariate parametric tests on GM density and perfusion data; or in
amyotrophic lateral sclerosis, with multivariate linear regression on spectroscopy findings
of different metabolites [84]. The superiority of multivariate models compared to
combined univariate models was demonstrated in [83], examining simultaneous changes
in FA, cortical thickness, and perfusion also in AD, and logistic regression was shown to
improve categorization of patients with different subtypes of mild cognitive impairment
in the first study of the present thesis [85] by combining ROI‒level DTI, volumetry, and
cortical thickness data at the subject level.
On the other hand, when searching for unique abnormalities (like injuries or MCDs)
in individuals, inference is made below the subject level: combining data from
independent modalities into multivariate distributions and performing statistical

98
evaluation in this high dimensional space enables the pooling of information on the lowest
level, only preceded by necessary spatial coregistration. An example for the resulting
increased sensitivity was in [86], where the combination of voxelwise MD and volumetry
data (using Hotelling’s T2‒test, a two‒sample equivalent of the Mahalanobis‒distance)
outlined the effects of traumatic brain injury (TBI), even in cases where none of the
individual modalities alone yielded significant results.
Recent studies also demonstrated the utility of machine‒learning based approaches
for epileptic lesion detection. Surface‒based methodology formed the basis of the work
in [88] and [89] using morphologic and intensity‒based features (such as cortical
thickness, sulcal depth, curvature of the surface, and gradient of intensity; all calculated
from T1 or T2‒weighted images on the vertex‒level), with similar performance as our
approach. In [88], higher specificity was achieved in detecting FCD type lesions.
Similarly to the present study, outlier‒detection approach was used in [87],
identifying epilepsy‒related malformations, using a voxel‒based, one‒class support
vector machine classifier. By working on feature maps computed from T1‒weighted data,
comparable sensitivity and less false positives were achieved than with our approach,
partially due to a far more conservative cluster size threshold (82 voxels, compared to 7
in our work).
Such machine‒learning based methods are expected to lead the analysis of
multidimensional neuroimaging data; however, our study drew merit from several
advantages. The straightforward and easy‒to‒use application of the multidimensional
statistics with moderate computation times (only a few seconds per subject on a
commercial PC, after preprocessing and registration) aided the accessibility of the
method, while the use of DTI data opened the scope of research to disruptions in tissue
microstructure.
2.2 On information sources and dimensionality considerations
Theoretically, there is no limitation to the number of examined dimensions in the
multivariate distribution examined with the Mahalanobis‒distance (as long as the number
of subjects exceeds the number of dimensions). Therefore, in order to circumvent the

99
limitations of the diffusion tensor representation, any diffusion processing model (e.g.
diffusion kurtosis imaging [140, 141], spherical deconvolution [197, 198], etc.), or even
raw diffusion weighted data could be evaluated in the same straightforward manner.
On the other hand, since L2‒type distance metrics tend to show decreasing
performance with higher number of dimensions [199], known as the effect of distance
concentration, and, as was demonstrated in [104], the calculation of the Mahalanobis‒
distance may induce a bias, dependent on sample size, that becomes substantial with
higher (P > 10) number of dimensions, simply pooling together every available source of
information would not necessarily increase statistical power. Other types of distance
metrics, particularly an LP‒norm should be a viable choice in such higher dimensional
examinations [200], however, such avenues of research were out of the scope of the
current study.
Another intriguing possibility for MRI‒based lesion detection using the
Mahalanobis‒distance is including voxel‒level data from other modalities, such as T1 or
T2‒weighted images, tissue probability maps, MRI or Positron Emission Tomography
(PET) based perfusion measurements, etc., as long as proper spatial coregistration is
achievable [86]. Since data in any given dimension is rescaled and cleared of correlations,
any meaningful modality could be incorporated to the analysis framework, also including
more complex measures from related processing pipelines, such as cortical parcellation,
volumetry or morphometry results [85, 88, 89], once again, with distance concentration
kept in mind.
Feature selection based on the analysis of meaningful components in such an extended
parameter space may be the aim of future investigations. Quantitative imaging, a feat
currently under intensive research [201], may also benefit from the use of
multidimensional distance‒metrics in statistical evaluation.
2.3 Simulation results
Simulations with standard multivariate Gaussian data were used to demonstrate the
numerical stability and lesion detection performance of the calculations based on the
Mahalanobis‒distance. AUC values calculated from the [0; 0.05] FPR range indicated

100
that above 1 FWHM mean difference, the method is sufficiently sensitive to even the
smallest artificial lesions, using critical values aimed to control either the family‒wise
error rate or the rate of false discoveries. This is the level of sensitivity typically aimed
for in image processing or spectroscopy as the resolution (i.e. the minimal distance
between two peaks required to separate them) is generally defined as 1 FWHM.
The use of eigenvalue maps of the control population yielded similar performance:
for effect strengths and lesion sizes expected in MCDs (i.e. 50 voxels, corresponding to
168.75 mm3 volume, around 5 ‒ 7 mm in diameter, [87]) the proposed method effectively
identifies regions of abnormal diffusion profile. This performance is on pair with that e.g.
[174] achieved in simulations introducing the threshold‒free cluster enhancement
(TFCE) method. Although the distribution of the tensor eigenvalues was not exactly
Gaussian, this only resulted in a small reduction of observed sensitivity, which did not
cause any substantial reduction in lesion detection performance.
False positives were completely eliminated in simulations on Gaussian random data,
with cluster size thresholds of 4 voxels, but a 7 voxel threshold was needed to reduce the
FPR to 0.1 ‒ 0.3% in simulations based on the resampling of real eigenvalue maps, with
both FWE and FDR corrected critical values. Additional exploratory analysis (not
included in the thesis) using larger thresholds ‒ 19, 27, and 50 voxels ‒ confirmed the
complete elimination of false positives, at the cost of reduced sensitivity (reduced true
positive rates) to smaller lesions.
Based on these findings we concluded that a cluster size threshold of 7 voxels (i.e.
one voxel and its nearest neighbors) should be an optimal choice for lesion detection,
when no spatial smoothing is performed on the diffusion tensor eigenvalue images. Only
this value was used in the subsequent examinations of healthy controls and patients with
MCDs.
Outlier values emanating from measurement errors or numerical instability usually
affect single voxels, thereby false positives of such origin could effectively be eliminated
with the cluster size threshold of seven voxels. For applications with statistical inference
performed on images with substantially different resolution from that of the acquisition
(e.g. if the eigenvalue images are resampled to a much smaller voxel size during the

101
processing), an adjusted cluster size threshold (covering roughly the same volume as 7
voxels of the acquisition voxel size) should achieve similar robustness to such effects.
Similar consideration should go for applications where spatial smoothing is performed at
some point during data processing.
2.4 Leave‒one‒out examination of controls
Use of the more conservative FWE‒corrected critical D2‒values and the TPM‒based
cluster‒evaluation method (δ‒values) limited the number of false positives to an
acceptable level. Examination of the control subjects demonstrated that even with the
high performance DARTEL‒coregistration, clusters of voxels with outlying diffusion
profile tend to emerge in (supposedly true negative) control subjects. Most of these
clusters proved to be indeed artefactual, being outside the brain parenchyma, however, in
average 1.79 clusters per subject were identified in the WM as well. At this level there is
no discrimination between clusters emanating from individual anatomical variability and
insufficient registration or noise; this problem is usually addressed (reduced) by spatial
smoothing in most voxel‒level studies [202], which we omitted to retain sensitivity for
smaller lesions.
2.5 Patient examinations
Apart from one case, all of the MCDs and other abnormalities in all patients were
identified on the processed D2‒images, demonstrating the sensitivity of our diffusion‒
tensor based approach for detecting minute structural abnormalities. The remaining one
FCD‒type malformation was identifiable only in results obtained with the more liberal,
FDR‒corrected critical values. This observation demonstrates that the conservative
approach with strict critical values can result in false negatives, thereby decreased
sensitivity, in brain regions where the DTI eigenvalues in the control group showed higher
sample variance.
Raw D2‒‘heat maps’, MAP07 ‘junction maps’, and the final D2‒clusters were
reviewed with an expert neuroradiologist and compared to the ground truth lesion masks.
As the MCDs under consideration are mainly localized around the WM‒GM boundary
(MAP07 also compares voxels from T1 images focused on this compartment) and DTI is

102
expected to be more sensitive in the WM, in most cases, D2‒clusters did only partially
overlap with the lesion masks; hence concurrence was ascertained by spatial adjacency.
The physical distance between the lesion masks and the D2‒clusters’ centers of masses
was also recorded; in clusters deemed positive, the average distance was 12.07 mm, in
agreement with results from literature [138].
Patient data was registered to the study specific DARTEL‒template, created from
only the controls. With this approach, the template was well defined with relatively low
sample variance in diffusion tensor eigenvalue distributions, nevertheless artefactual
clusters were commonly observed, but they were present mainly in the CSF or around the
GM‒CSF boundary. The δ‒value‒based method, evaluating clusters based on tissue
probability maps was efficient in filtering out the more evident ones, however, several
cases showed obvious artefacts identifiable by their shape and location (e.g. in the
occipital lobes, close to and following the GM‒CSF boundary, independent of the
underlying gyral and sulcal pattern) escaping elimination. Additional automatic
classification of artefactual clusters based on spatial distribution properties similar to
those implemented in SOCK [203] and FIX [204] would further aid the evaluation of
results. Since the focus of the present study was on the statistical approach for examining
tissue microstructure and the surviving artefactual clusters were easily discernable among
the results, thus did not severely obstruct patient evaluation, we chose to favor generality
and did not penalize the examined volume any further. Although utilizing any or a
combination of the above mentioned filtering or labeling approaches would possibly have
increase lesion detection specificity, the detailed evaluation of cluster features was
outside the scope the study, but may be investigated in the future.
In most patients, smaller clusters (typically under 50 voxels) further away from the
actual lesions were also identified in the WM. Apart from the ones in the terminal WM,
found in several of the adolescent patients, likely reflecting age‒related differences in
myelination; based on previous studies [138, 139], such extended WM‒abnormalities are
to be expected in epileptic patients [127]: they most likely reflect either the underlying
pathological networks or compensatory effects or elicited by them [205]. Exploratory
analysis of DTI tractography data in select cases demonstrated that most of these

103
additional WM clusters are indeed located in or close to the fiber pathways passing
through the primary lesion volumes (Fig 22).
Fig 22 Comparing the location of distant WM clusters to tractography
Deterministic DTI tractography (performed in ExploreDTI) revealed, that several of the distant WM
clusters are connected to the primary lesions, for example in a 33 y.o. female patient with multiplex right
temporal closed‒loop schizencephaly and subependymal heterotopia (left), and in a 27 y.o. male patient
with presumed polymicrogyria or FCD in the left inferior frontal gyrus and the posterior third of the left
insula (right). Axial and coronal slices presented in neurological orientation, i.e. left side is on the left.
Such clusters suggest that microstructural changes reflected in the DTI data is not
specific to the malformations themselves, but also to the disruptions that the actual MCDs
inflict on the corresponding WM pathways. In qualitative evaluation, they may be of
clinical importance shedding light on the extent and/or organization of the epileptic
networks themselves. Nevertheless, including other sources of information (e.g.
relaxometry, susceptibility, perfusion, or morphometry measurements) in the proposed
multidimensional statistical framework is likely to improve lesion detection specificity.
Following this avenue of research was, once again, outside the scope of the study, but is
the evident direction to go for the future.
As the mean age of our control group was 25.2, the method performed better with
adults. In two younger patients (age < 10) more additional clusters were identified, most

104
likely resulting from differences in myelination and erroneous registration due to more
pronounced anatomical (i.e. head and brain size) differences.
As the method proved to be sensitive to a wide range of malformations and even to
more pronounced physiological variations, more carefully selected control group(s) of
matching age would increase specificity (Fig 21) and thus would yield better
characterization of abnormal tissue microstructure. Nevertheless, since MCDs associated
with the epileptic seizures were identified in all but one cases, even with approximately
17 years of age difference, it was established that detecting disrupted tissue microstructure
using tensor eigenvalues based on the Mahalanobis‒distance is indeed feasible and may
aid in single subject evaluations. Additional case studies, not included in the thesis,
demonstrated that the effects of large anatomical abnormalities, higher level of subject
motion, or differences in scan parameters (even with a robust dMRI processing pipeline
with thorough motion correction and high performance spatial registration) lead to more
severe artefact contamination of the results, therefore age difference, seems to be a less
pronounced limiting factor.
With clusters observed partially outside the brain parenchyma (typically in the sulci)
or evidently following the GM‒CSF boundary, regardless of the underlying tissue
macrostructure, registration performance may also be a major effect; potentially causing
a high number of artefactual clusters, not all of which could be filtered out with the TPM‒
based cluster‒evaluation method. Fortunately, such clusters are easily identifiable as
obvious artefacts, and so are the results of possible missing slices, postoperative resection
sites, large anatomical variations (e.g. agenesis of the corpus callosum), or large‒scale
shifts, rotations, or shears.
Papers in the field of automated lesion detection usually examine single types of
pathologies, for example patients with FCDs [88, 89, 133, 206], benefiting from the more
specific research question. On the other hand, as clinical practice suggests that different
types of MCDs tend to develop together, our patient group of individuals with mixed
pathologies more faithfully represents typical cases of drug resistant epilepsies [127]. The
multidimensional approach proved to be sensitive to the different types of malformations,
which is a satisfying result for a potential lesion detection method, however, if the

105
framework is to be extended with data from other modalities in future studies, feature
selection analysis would benefit from selecting cases with single types of MCDs.
The altered diffusion profile (potentially resulting from several aforementioned
normal, pathological, or compensational processes – that could also be varying across
individuals), can only be detected, not characterized by the distance metric. Therefore,
the generalization of findings would benefit from group‒based measures of the
pathology‒related alterations. For such an endeavor the identified regions of disrupted
microstructure could be subjected to subsequent conventional testing, for example,
exploring whether FA is increased or decreased in the region, or assessing abnormal
connectivity through tractography by using the clusters as seed regions [207]. In future
studies, such subsequent examinations, potentially including group‒based measures
derived from patients with similar pathologies, could help discerning between direct and
compensatory effects, explaining some of the observed distant WM clusters.
The proposed method proved successful in combining separate eigenvalue maps,
benefiting from the advantages of the multidimensional approach, and achieved sufficient
sensitivity in detecting abnormal diffusion profile. The straightforward application of
analytically‒derived critical values [102] allowed making strong inferences, although
specificity was limited due to registration artefacts and normal or pathological variations:
effects inherent to all single subject examinations [208].
2.6 Limitations
The wide range of pathologies and the technical impediments may constrain the
generalization of findings, nevertheless, as the major goal of the present study was to
introduce a new method of statistical evaluation, these predicaments may prove useful in
assessing the flexibility of the method.
Using study specific templates, e.g. the DARTEL approach in the present study may
be considered a limitation, especially when evaluating possible diagnostic tools,
nevertheless, the aim of the current paper was to demonstrate the value of the
Mahalanobis‒distance based approach in single patient vs control group comparisons.
Further analyses using multi‒center multi‒scanner data may further warrant the

106
evaluation of the diagnostic potential of a Mahalanobis‒distance based lesion detection
tool.
During additional patient examinations, not presented in the thesis, we found that a
system upgrade also affected the outcome of the statistical analyses, leading to apparent
alterations in almost the entire WM, this effect may also most probably stem from the
rather homogeneously collected control data. A multi‒center, multi‒scanner
investigation, like mentioned above, may prove to be useful in overcoming such
limitations.

107
VI. Conclusions
1. DTI and Mild Cognitive Impairment
The findings of the first study supported the hypothesis, that impairments of white
matter integrity appear as early signs of pathological cognitive decline in both amnestic
and non‒amnestic clinical manifestations of MCI. DTI measurements in the fornix, the
stria terminalis and the cingulum can add valuable information to analyses based on grey
matter volumetry and thus can help detect Alzheimer Disease in an early, preclinical
stage.
Future medications in AD are expected to be effective in such early stages, therefore
extending volumetric analyses with DTI‒derived metrics may help the early identification
of the disease well within the possible therapeutic window of these proposed medications
to help preventing further decline.
Aside from the prospective advantages of the proposed methods, differentiation
between MCI patient groups was also demonstrated to be improved after extending GM
volumetry‒based models with DTI measurements, yielding an immediate utility of the
addition of DTI‒based metrics in the evaluation of MCI.
Furthermore, the utility of the approach may not be limited to MCI and AD, as based
on our results, it seems that DTI measurements can also help detecting non‒Alzheimer
type dementias in early stage, however, these findings must be confirmed by further
studies with larger sample sizes.
2. Mahalanobis‒distance in MCD lesion detection
Investigating other aspects of the utility of DTI‒based microstructural evaluations,
the Mahalanobis‒distance based method, proposed in the second study, efficiently
combined information from maps of the three diffusion tensor eigenvalues on the voxel‒
level. Altered diffusion profiles corresponding to malformations of cortical development
in single subject vs. control group examinations were detected as outlier values in the
voxelwise multidimensional distributions, based on but not necessarily limited to DTI
data.

108
Searching for pathological brain regions of individuals as outliers, using the
Mahalanobis‒distance in evaluation of diffusion weighted imaging data (even with more
sophisticated models for processing, if necessary) seems to be a viable approach, and as
the calculations could easily cover data from other modalities, this evaluation method
may substantially advance the field of quantitative MRI in general.
3. General conclusions
Multidimensional and multi‒modal approaches in the processing and evaluation of
brain MR images proved to be efficient in detecting the disease‒related alterations of
tissue microstructure based on DTI data, both when characterizing impairments
associated with cognitive decline and when searching for malformations related to drug
resistant epilepsies.
The application of state‒of‒the‒art data processing methods, thorough image
correction and using anatomical scans as targets for registration and “up‒sampling”,
combined with the volume‒based creation of study‒specific templates using the
DARTEL method (originally developed for volumetry) was efficient in treating voxel‒
level dMRI data.
Resulting sample distributions had low observed variance and good spatial
congruency between control subjects, which facilitated strong inferences, even when
considering the high number of simultaneously performed statistical tests. Voxel‒level
correlation analyses and between‒group comparisons pinpointed the key structures
affected through cognitive impairment; these findings subserved the application of multi‒
modal logistic regression on the region‒level and the multidimensional statistics in single
subject evaluation.
The combined information resulted in high sensitivity, yielding improved accuracy in
the detection of abnormal tissue microstructure, originating from MCI‒related changes
or epilepsy‒related malformations, suggesting the clinical utility of such evaluation
methods.

109
VII. Summary
Diffusion magnetic resonance imaging (dMRI) refers to a rapidly developing group
of methods capable of probing tissue microstructure non–invasively, with proven unique
sensitivity to various diseases, thus making them essential in research protocols and
everyday clinical practice. With the increasing amount and complexity of MRI data,
efficient processing methods and the combination of information from different sources
are necessary when searching for biomarkers to detect and characterize abnormalities.
The present thesis describes two separate research projects with state‒of‒the‒art dMRI
processing methods and the use of multidimensional–multimodal statistics to search for
disease–specific alterations of tissue microstructure using diffusion tensor imaging (DTI)
data in the brain.
In the first project, the potential role of DTI in the differential diagnosis of mild
cognitive impairment (MCI) was investigated. A study–specific template using
anatomical information proved to be efficient for registering whole brain voxel–level
data, facilitating strong inference, both when comparing groups of healthy subjects and
patients with amnestic and non-amnestic subtypes of MCI, or when examining correlation
between neuropsychology and tissue microstructure. Robust effects were confirmed with
region–level logistic regression analyses in the white matter, showing substantially
improved discrimination between MCI subtypes, by using a combination of DTI and
volumetry data.
The second part of the thesis describes a novel approach for single subject lesion
localization, employing outlier detection at the voxel level using the multidimensional
squared Mahalanobis-distance on DTI–eigenvalue data. Potential sensitivity and
specificity were evaluated through simulations and clinical utility was demonstrated on
data of epilepsy patients with malformations of cortical development and other
abnormalities. Altogether 15 of the 16 example lesions were detected, whilst false
positives resulting from registration inaccuracies were also marked alongside distant
regions suggesting potential network–level abnormalities.
Advanced dMRI processing combined with multimodal strategies aids the detection
of altered tissue microstructure, yielding potential diagnostic biomarkers in the brain.

110
VIII. Összefoglalás
A diffúziós mágneses rezonancia képalkotás (dMRI) olyan eljárásokat jelöl,
melyekkel a szöveti mikrostruktúra egyedülálló érzékenységgel vizsgálható, nem invazív
módon; így kutatási projektek és a mindennapi klinikai gyakorlat alapvető részét képezik.
A nagy mennyiségű, komplex MR képanyag értékelését, új biomarkerek azonosítását, és
összetett eltérések jellemzését segítheti hatékony adatfeldolgozó eljárások, illetve a több
forrásból származó információt egységesen kezelni képes megközelítések alkalmazása.
Jelen disszertáció két tudományos munkát mutat be, melyekben betegségspecifikus
eltérések azonosításához a legmodernebb dMRI feldolgozást többdimenziós és
multimodális statisztikai eljárásokkal kombináltuk, agyi diffúziós tenzor (DTI) adatok
értékelésére.
Az első projektben a DTI adatok lehetséges differenciáldiagnosztikai jelentőségét
vizsgáltuk enyhe kognitív zavarban (mild cognitive impairment–MCI). Az egyéni
anatómiai felvételekből vizsgálatspecifikus közös koordinátarendszert képezve javítottuk
a voxel-szintű adatok illesztését. Ennek köszönhetően javult a statisztikai tesztek ereje,
mind az amnesztikus és nem-amnesztikus betegcsoportok illetve egészséges kontroll
alanyok összehasonlításakor, mind a szöveti mikrostruktúra kognitív teljesítménnyel
mutatott korrelációjának vizsgálatában. Fehérállományi területek régió szintű
vizsgálatával erős hatásokat igazoltunk, majd logisztikus regressziós eljárás segítségével
a DTI adatokat volumetriai számítások eredményével kombináltuk, szignifikánsan
javítva az MCI alcsoportok elkülönítését.
A dolgozat második része egyedi páciensek lézióinak voxelszintű detekciójára
alkalmazható új eljárást mutat be, az eltéréseket Mahalanobis-távolság segítségével
kiszóró pontokként azonosítva a DTI-sajátértékek terében. Az elérhető szenzitivitást és
specificitást szimulációkkal vizsgáltuk, majd, kérgi fejlődési rendellenességek példáján,
klinikai adaton is demonstráltuk. Összesen 15 léziót sikerült azonosítani a 16-ból, bár az
értékelést illesztési pontatlanságok nehezítették A primer lézióktól távolabb lézióként
jelölt területek hálózati szintű eltérésekre utalhatnak.
A fejlett dMRI adatfeldolgozás és a multimodális stratégiák kombinációja elősegíti a
mikrostrukturális elváltozások azonosítását és új diagnosztikus biomarkerek fejlesztését.

111
References
1. Behrens TE, Sporns O (2012) Human connectomics. Curr Opin Neurobiol, 22:
144-53.
2. Jbabdi S, Sotiropoulos SN, Haber SN, Van Essen DC, Behrens TE (2015)
Measuring macroscopic brain connections in vivo. Nat Neurosci, 18: 1546-55.
3. Glasser MF, Smith SM, Marcus DS, Andersson JLR, Auerbach EJ, Behrens TEJ,
Coalson TS, Harms MP, Jenkinson M, Moeller S, Robinson EC, Sotiropoulos SN,
Xu J, Yacoub E, Ugurbil K, Van Essen DC (2016) The Human Connectome
Project's neuroimaging approach. Nature neuroscience, 19: 1175-1187.
4. Eickhoff SB, Yeo BTT, Genon S (2018) Imaging-based parcellations of the
human brain. Nature Reviews Neuroscience, 19: 672-686.
5. Miller KL, Alfaro-Almagro F, Bangerter NK, Thomas DL, Yacoub E, Xu J,
Bartsch AJ, Jbabdi S, Sotiropoulos SN, Andersson JLR, Griffanti L, Douaud G,
Okell TW, Weale P, Dragonu I, Garratt S, Hudson S, Collins R, Jenkinson M,
Matthews PM, Smith SM (2016) Multimodal population brain imaging in the UK
Biobank prospective epidemiological study. Nature neuroscience, 19: 1523-1536.
6. Le Bihan D, Breton E (1985) Imagerie de diffusion in-vivo par résonance
magnétique nucléaire. Comptes-Rendus de l'Académie des Sciences, 93: 27-34.
7. Merboldt K-D, Hanicke W, Frahm J (1985) Self-diffusion NMR imaging using
stimulated echoes. Journal of Magnetic Resonance (1969), 64: 479-486.
8. Taylor DG, Bushell MC (1985) The spatial mapping of translational diffusion
coefficients by the NMR imaging technique. Physics in Medicine and Biology,
30: 345-349.
9. Hahn EL (1950) Spin Echoes. Physical Review, 80: 580-594.
10. Carr HY, Purcell EM (1954) Effects of Diffusion on Free Precession in Nuclear
Magnetic Resonance Experiments. Physical Review, 94: 630-638.
11. Stejskal EO, Tanner JE (1965) Spin Diffusion Measurements: Spin Echoes in the
Presence of a Time‐Dependent Field Gradient. The Journal of Chemical Physics,
42: 288-292.
12. Cleveland GG, Chang DC, Hazlewood CF, Rorschach HE (1976) Nuclear
magnetic resonance measurement of skeletal muscle: anisotrophy of the diffusion
coefficient of the intracellular water. Biophysical journal, 16: 1043-1053.

112
13. Moseley ME, Kucharczyk J, Mintorovitch J, Cohen Y, Kurhanewicz J, Derugin
N, Asgari H, Norman D (1990) Diffusion-weighted MR imaging of acute stroke:
correlation with T2-weighted and magnetic susceptibility-enhanced MR imaging
in cats. AJNR Am J Neuroradiol, 11: 423-9.
14. Basser PJ, Pierpaoli C (1996) Microstructural and physiological features of tissues
elucidated by quantitative-diffusion-tensor MRI. J Magn Reson B, 111: 209-19.
15. Pierpaoli C, Jezzard P, Basser PJ, Barnett A, Di Chiro G (1996) Diffusion tensor
MR imaging of the human brain. Radiology, 201: 637-48.
16. Jones DK, Horsfield MA, Simmons A (1999) Optimal strategies for measuring
diffusion in anisotropic systems by magnetic resonance imaging. Magn Reson
Med, 42: 515-25.
17. Chang L-C, Jones DK, Pierpaoli C (2005) RESTORE: Robust estimation of
tensors by outlier rejection. Magnetic Resonance in Medicine, 53: 1088-1095.
18. Basser PJ, Pajevic S, Pierpaoli C, Duda J, Aldroubi A (2000) In vivo fiber
tractography using DT-MRI data. Magnetic Resonance in Medicine, 44: 625-632.
19. Mori S, van Zijl PC (2002) Fiber tracking: principles and strategies - a technical
review. NMR Biomed, 15: 468-80.
20. Behrens TE, Woolrich MW, Jenkinson M, Johansen-Berg H, Nunes RG, Clare S,
Matthews PM, Brady JM, Smith SM (2003) Characterization and propagation of
uncertainty in diffusion-weighted MR imaging. Magn Reson Med, 50: 1077-88.
21. Parker GJ, Haroon HA, Wheeler-Kingshott CA (2003) A framework for a
streamline-based probabilistic index of connectivity (PICo) using a structural
interpretation of MRI diffusion measurements. J Magn Reson Imaging, 18: 242-
54.
22. Clark CA, Byrnes T, Diffusion MRI Theory, Methods, and Applications: DTI and
Tractography in Neurosurgical Planning, Oxford University Press. 2012.
23. Glenn OA, Ludeman NA, Berman JI, Wu YW, Lu Y, Bartha AI, Vigneron DB,
Chung SW, Ferriero DM, Barkovich AJ, Henry RG (2007) Diffusion Tensor MR
Imaging Tractography of the Pyramidal Tracts Correlates with Clinical Motor
Function in Children with Congenital Hemiparesis. American Journal of
Neuroradiology, 28: 1796-1802.

113
24. Goodlett CB, Fletcher PT, Gilmore JH, Gerig G (2009) Group analysis of DTI
fiber tract statistics with application to neurodevelopment. NeuroImage, 45: S133-
S142.
25. Hagmann P, Thiran JP, Jonasson L, Vandergheynst P, Clarke S, Maeder P, Meuli
R (2003) DTI mapping of human brain connectivity: statistical fibre tracking and
virtual dissection. NeuroImage, 19: 545-554.
26. Skudlarski P, Jagannathan K, Calhoun VD, Hampson M, Skudlarska BA,
Pearlson G (2008) Measuring brain connectivity: diffusion tensor imaging
validates resting state temporal correlations. NeuroImage, 43: 554-561.
27. Jeurissen B, Leemans A, Tournier J-D, Jones DK, Sijbers J (2013) Investigating
the prevalence of complex fiber configurations in white matter tissue with
diffusion magnetic resonance imaging. Human Brain Mapping, 34: 2747-2766.
28. Le Bihan D, Mangin JF, Poupon C, Clark CA, Pappata S, Molko N, Chabriat H
(2001) Diffusion tensor imaging: concepts and applications. J Magn Reson
Imaging, 13: 534-46.
29. Lebel C, Walker L, Leemans A, Phillips L, Beaulieu C (2008) Microstructural
maturation of the human brain from childhood to adulthood. Neuroimage, 40:
1044-55.
30. Song SK, Sun SW, Ramsbottom MJ, Chang C, Russell J, Cross AH (2002)
Dysmyelination revealed through MRI as increased radial (but unchanged axial)
diffusion of water. Neuroimage, 17: 1429-36.
31. Budde MD, Xie M, Cross AH, Song S-K (2009) Axial diffusivity is the primary
correlate of axonal injury in the experimental autoimmune encephalomyelitis
spinal cord: a quantitative pixelwise analysis. The Journal of neuroscience : the
official journal of the Society for Neuroscience, 29: 2805-2813.
32. Douaud G, Jbabdi S, Behrens TE, Menke RA, Gass A, Monsch AU, Rao A,
Whitcher B, Kindlmann G, Matthews PM, Smith S (2011) DTI measures in
crossing-fibre areas: increased diffusion anisotropy reveals early white matter
alteration in MCI and mild Alzheimer's disease. Neuroimage, 55: 880-90.
33. Gyebnar G, Klimaj Z, Entz L, Fabo D, Rudas G, Barsi P, Kozak LR (2019)
Personalized microstructural evaluation using a Mahalanobis-distance based

114
outlier detection strategy on epilepsy patients' DTI data - Theory, simulations and
example cases. PLoS One, 14: e0222720.
34. Abhinav K, Yeh F-C, Pathak S, Suski V, Lacomis D, Friedlander RM, Fernandez-
Miranda JC (2014) Advanced diffusion MRI fiber tracking in neurosurgical and
neurodegenerative disorders and neuroanatomical studies: A review. Biochimica
et Biophysica Acta (BBA) - Molecular Basis of Disease, 1842: 2286-2297.
35. Cohen Y, Assaf Y (2002) High b-value q-space analyzed diffusion-weighted
MRS and MRI in neuronal tissues – a technical review. NMR in Biomedicine, 15:
516-542.
36. Callaghan PT, Eccles CD, Xia Y (1988) NMR microscopy of dynamic
displacements: k-space and q-space imaging. Journal of Physics E: Scientific
Instruments, 21: 820-822.
37. Callaghan PT, Xia Y (1991) Velocity and diffusion imaging in dynamic NMR
microscopy. Journal of Magnetic Resonance (1969), 91: 326-352.
38. Wedeen VJ, Hagmann P, Tseng W-YI, Reese TG, Weisskoff RM (2005) Mapping
complex tissue architecture with diffusion spectrum magnetic resonance imaging.
Magnetic Resonance in Medicine, 54: 1377-1386.
39. Assaf Y, Ben-Bashat D, Chapman J, Peled S, Biton IE, Kafri M, Segev Y, Hendler
T, Korczyn AD, Graif M, Cohen Y (2002) High b-value q-space analyzed
diffusion-weighted MRI: application to multiple sclerosis. Magn Reson Med, 47:
115-26.
40. Cohen Y, Assaf Y (2002) High b-value q-space analyzed diffusion-weighted
MRS and MRI in neuronal tissues - a technical review. NMR Biomed, 15: 516-
42.
41. Sotiropoulos SN, Jbabdi S, Xu J, Andersson JL, Moeller S, Auerbach EJ, Glasser
MF, Hernandez M, Sapiro G, Jenkinson M, Feinberg DA, Yacoub E, Lenglet C,
Van Essen DC, Ugurbil K, Behrens TEJ, Consortium WU-MH (2013) Advances
in diffusion MRI acquisition and processing in the Human Connectome Project.
NeuroImage, 80: 125-143.
42. Uğurbil K, Xu J, Auerbach EJ, Moeller S, Vu AT, Duarte-Carvajalino JM, Lenglet
C, Wu X, Schmitter S, Van de Moortele PF, Strupp J, Sapiro G, De Martino F,
Wang D, Harel N, Garwood M, Chen L, Feinberg DA, Smith SM, Miller KL,

115
Sotiropoulos SN, Jbabdi S, Andersson JLR, Behrens TEJ, Glasser MF, Van Essen
DC, Yacoub E, Consortium WU-MH (2013) Pushing spatial and temporal
resolution for functional and diffusion MRI in the Human Connectome Project.
NeuroImage, 80: 80-104.
43. Wu W, Miller KL (2017) Image formation in diffusion MRI: A review of recent
technical developments. Journal of magnetic resonance imaging : JMRI, 46: 646-
662.
44. Tournier J-D, Calamante F, Connelly A (2013) Determination of the appropriate
b value and number of gradient directions for high-angular-resolution diffusion-
weighted imaging. NMR in Biomedicine, 26: 1775-1786.
45. Tuch DS, Reese TG, Wiegell MR, Makris N, Belliveau JW, Wedeen VJ (2002)
High angular resolution diffusion imaging reveals intravoxel white matter fiber
heterogeneity. Magn Reson Med, 48: 577-82.
46. Tuch DS (2004) Q-ball imaging. Magnetic Resonance in Medicine, 52: 1358-
1372.
47. Jeurissen B, Tournier JD, Dhollander T, Connelly A, Sijbers J (2014) Multi-tissue
constrained spherical deconvolution for improved analysis of multi-shell diffusion
MRI data. Neuroimage, 103: 411-426.
48. Tournier JD, Calamante F, Gadian DG, Connelly A (2004) Direct estimation of
the fiber orientation density function from diffusion-weighted MRI data using
spherical deconvolution. NeuroImage, 23: 1176-1185.
49. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczynski K (2005) Diffusional kurtosis
imaging: The quantification of non-gaussian water diffusion by means of
magnetic resonance imaging. Magnetic Resonance in Medicine, 53: 1432-1440.
50. Niendorf T, Dijkhuizen RM, Norris DG, van Lookeren Campagne M, Nicolay K
(1996) Biexponential diffusion attenuation in various states of brain tissue:
implications for diffusion-weighted imaging. Magn Reson Med, 36: 847-57.
51. Assaf Y, Freidlin RZ, Rohde GK, Basser PJ (2004) New modeling and
experimental framework to characterize hindered and restricted water diffusion in
brain white matter. Magn Reson Med, 52: 965-78.

116
52. Zhang H, Schneider T, Wheeler-Kingshott CA, Alexander DC (2012) NODDI:
Practical in vivo neurite orientation dispersion and density imaging of the human
brain. NeuroImage, 61: 1000-1016.
53. Szczepankiewicz F, Lasič S, van Westen D, Sundgren PC, Englund E, Westin C-
F, Ståhlberg F, Lätt J, Topgaard D, Nilsson M (2015) Quantification of
microscopic diffusion anisotropy disentangles effects of orientation dispersion
from microstructure: Applications in healthy volunteers and in brain tumors.
NeuroImage, 104: 241-252.
54. Mansfield P (1977) Multi-planar image formation using NMR spin echoes.
Journal of Physics C: Solid State Physics, 10: L55-L58.
55. Mesri HY, David S, Viergever MA, Leemans A (2020) The adverse effect of
gradient nonlinearities on diffusion MRI: From voxels to group studies.
Neuroimage, 205: 116127.
56. Leemans A, Jones DK (2009) The B-matrix must be rotated when correcting for
subject motion in DTI data. Magn Reson Med, 61: 1336-49.
57. Dyrby TB, Lundell H, Burke MW, Reislev NL, Paulson OB, Ptito M, Siebner HR
(2014) Interpolation of diffusion weighted imaging datasets. NeuroImage, 103:
202-213.
58. Ashburner J (2007) A fast diffeomorphic image registration algorithm.
Neuroimage, 38: 95-113.
59. Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM,
Delaney RC, McCarthy G, Charney DS, Innis RB (1995) MRI-based
measurement of hippocampal volume in patients with combat-related
posttraumatic stress disorder. Am J Psychiatry, 152: 973-81.
60. Lawson JA, Vogrin S, Bleasel AF, Cook MJ, Burns L, McAnally L, Pereira J, Bye
AM (2000) Predictors of hippocampal, cerebral, and cerebellar volume reduction
in childhood epilepsy. Epilepsia, 41: 1540-5.
61. Pohlack ST, Meyer P, Cacciaglia R, Liebscher C, Ridder S, Flor H (2014) Bigger
is better! Hippocampal volume and declarative memory performance in healthy
young men. Brain structure & function, 219: 255-267.

117
62. Catani M, Jones DK, Daly E, Embiricos N, Deeley Q, Pugliese L, Curran S,
Robertson D, Murphy DG (2008) Altered cerebellar feedback projections in
Asperger syndrome. Neuroimage, 41: 1184-91.
63. Mori S, Oishi K, Jiang H, Jiang L, Li X, Akhter K, Hua K, Faria AV, Mahmood
A, Woods R, Toga AW, Pike GB, Neto PR, Evans A, Zhang J, Huang H, Miller
MI, van Zijl P, Mazziotta J (2008) Stereotaxic white matter atlas based on
diffusion tensor imaging in an ICBM template. Neuroimage, 40: 570-582.
64. Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix
N, Mazoyer B, Joliot M (2002) Automated anatomical labeling of activations in
SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject
brain. Neuroimage, 15: 273-289.
65. Collins DL, Neelin P, Peters TM, Evans AC (1994) Automatic 3D intersubject
registration of MR volumetric data in standardized Talairach space. J Comput
Assist Tomogr, 18: 192-205.
66. Talairach J (1988) Co-Planar Stereotaxic Atlas of the Human Brain-3-
Dimensional Proportional System. An Approach to Cerebral Imaging.
67. Evans AC, Collins DL, Mills SR, Brown ED, Kelly RL, Peters TM. 3D statistical
neuroanatomical models from 305 MRI volumes. in 1993 IEEE Conference
Record Nuclear Science Symposium and Medical Imaging Conference. 1993.
68. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-
Berg H, Bannister PR, De Luca M, Drobnjak I, Flitney DE, Niazy RK, Saunders
J, Vickers J, Zhang Y, De Stefano N, Brady JM, Matthews PM (2004) Advances
in functional and structural MR image analysis and implementation as FSL.
Neuroimage, 23 Suppl 1: S208-19.
69. Friston KJ, Holmes, A. P., Worsley, K. J., Poline, J. B., Frith, C. D., and
Frackowiak, R. S. J. (1995) Statistical parametric maps in functional imaging: A
general linear approach. Hum. Brain Mapp., 2: 189–210.
70. Ashburner J, Friston K (1997) Multimodal image coregistration and partitioning-
-a unified framework. Neuroimage, 6: 209-17.
71. Ashburner J, Neelin P, Collins DL, Evans A, Friston K (1997) Incorporating prior
knowledge into image registration. Neuroimage, 6: 344-52.

118
72. Ashburner J, Friston KJ (2000) Voxel-Based Morphometry—The Methods.
NeuroImage, 11: 805-821.
73. Gaser C, Nenadic I, Buchsbaum BR, Hazlett EA, Buchsbaum MS (2001)
Deformation-Based Morphometry and Its Relation to Conventional Volumetry of
Brain Lateral Ventricles in MRI. NeuroImage, 13: 1140-1145.
74. Freeborough PA, Fox NC (1998) Modeling brain deformations in Alzheimer
disease by fluid registration of serial 3D MR images. J Comput Assist Tomogr,
22: 838-43.
75. Thompson PM, Giedd JN, Woods RP, MacDonald D, Evans AC, Toga AW
(2000) Growth patterns in the developing brain detected by using continuum
mechanical tensor maps. Nature, 404: 190-3.
76. Ahlbom A, Bottai M (2016) False-positive findings, multiple comparisons and the
strength of hypotheses. J Intern Med, 279: 399-402.
77. Alberton BAV, Nichols TE, Gamba HR, Winkler AM (2020) Multiple testing
correction overcontrasts for brain imaging. Neuroimage: 116760.
78. Smith SM, Jenkinson M, Johansen-Berg H, Rueckert D, Nichols TE, Mackay CE,
Watkins KE, Ciccarelli O, Cader MZ, Matthews PM, Behrens TE (2006) Tract-
based spatial statistics: voxelwise analysis of multi-subject diffusion data.
Neuroimage, 31: 1487-505.
79. Friston KJ, Holmes A, Poline JB, Price CJ, Frith CD (1996) Detecting Activations
in PET and fMRI: Levels of Inference and Power. NeuroImage, 4: 223-235.
80. Heller R, Golland Y, Malach R, Benjamini Y (2007) Conjunction group analysis:
An alternative to mixed/random effect analysis. NeuroImage, 37: 1178-1185.
81. Lazar NA, Luna B, Sweeney JA, Eddy WF (2002) Combining Brains: A Survey
of Methods for Statistical Pooling of Information. NeuroImage, 16: 538-550.
82. Hayasaka S, Du A-T, Duarte A, Kornak J, Jahng G-H, Weiner MW, Schuff N
(2006) A non-parametric approach for co-analysis of multi-modal brain imaging
data: Application to Alzheimer’s disease. NeuroImage, 30: 768-779.
83. Naylor MG, Cardenas VA, Tosun D, Schuff N, Weiner M, Schwartzman A (2014)
Voxelwise multivariate analysis of multimodality magnetic resonance imaging.
Human brain mapping, 35: 831-846.

119
84. Young K, Govind V, Sharma K, Studholme C, Maudsley AA, Schuff N (2010)
Multivariate Statistical Mapping of Spectroscopic Imaging Data. Magnetic
resonance in medicine : official journal of the Society of Magnetic Resonance in
Medicine / Society of Magnetic Resonance in Medicine, 63: 20-24.
85. Gyebnar G, Szabo A, Siraly E, Fodor Z, Sakovics A, Salacz P, Hidasi Z, Csibri
E, Rudas G, Kozak LR, Csukly G (2018) What can DTI tell about early cognitive
impairment? - Differentiation between MCI subtypes and healthy controls by
diffusion tensor imaging. Psychiatry Res Neuroimaging, 272: 46-57.
86. Avants B, Duda JT, Kim J, Zhang H, Pluta J, Gee JC, Whyte J (2008) Multivariate
Analysis of Structural and Diffusion Imaging in Traumatic Brain Injury.
Academic Radiology, 15: 1360-1375.
87. El Azami M, Hammers A, Jung J, Costes N, Bouet R, Lartizien C (2016)
Detection of Lesions Underlying Intractable Epilepsy on T1-Weighted MRI as an
Outlier Detection Problem. PLOS ONE, 11: e0161498.
88. Hong S-J, Kim H, Schrader D, Bernasconi N, Bernhardt BC, Bernasconi A (2014)
Automated detection of cortical dysplasia type II in MRI-negative epilepsy.
Neurology, 83: 48-55.
89. Ahmed B, Brodley CE, Blackmon KE, Kuzniecky R, Barash G, Carlson C, Quinn
BT, Doyle W, French J, Devinsky O, Thesen T (2015) Cortical feature analysis
and machine learning improves detection of “MRI-negative” focal cortical
dysplasia. Epilepsy & behavior : E&B, 48: 21-28.
90. De Maesschalck R, Jouan-Rimbaud D, Massart DL (2000) The Mahalanobis
distance. Chemometrics and Intelligent Laboratory Systems, 50: 1-18.
91. Gnanadesikan R, Kettenring JR (1972) Robust Estimates, Residuals, and Outlier
Detection with Multiresponse Data. Biometrics, 28: 81-124.
92. Xiang S, Nie F, Zhang C (2008) Learning a Mahalanobis distance metric for data
clustering and classification. Pattern Recognition, 41: 3600-3612.
93. Mahalanobis PC (1936) On the generalised distance in statistics. Proceedings of
the National Institute of Science of India 2: 49-55.
94. Wu Y-C, Field AS, Duncan ID, Samsonov AA, Kondo Y, Tudorascu D,
Alexander AL (2011) High b-value and diffusion tensor imaging in a canine
model of dysmyelination and brain maturation. NeuroImage, 58: 829-837.

120
95. Sun SW, Liang HF, Le TQ, Armstrong RC, Cross AH, Song SK (2006)
Differential sensitivity of in vivo and ex vivo diffusion tensor imaging to evolving
optic nerve injury in mice with retinal ischemia. Neuroimage, 32: 1195-204.
96. Bava S, Thayer R, Jacobus J, Ward M, Jernigan TL, Tapert SF (2010)
Longitudinal characterization of white matter maturation during adolescence.
Brain Res, 1327: 38-46.
97. Taxt T, Lundervold A (1994) Multispectral analysis of the brain using magnetic
resonance imaging. IEEE Transactions on Medical Imaging, 13: 470-481.
98. Caprihan A, Pearlson GD, Calhoun VD (2008) Application of principal
component analysis to distinguish patients with schizophrenia from healthy
controls based on fractional anisotropy measurements. NeuroImage, 42: 675-682.
99. Kulikova S, Hertz-Pannier L, Dehaene-Lambertz G, Buzmakov A, Poupon C,
Dubois J (2015) Multi-parametric evaluation of the white matter maturation.
Brain structure & function, 220: 3657-3672.
100. Lindemer ER, Salat DH, Smith EE, Nguyen K, Fischl B, Greve DN, Alzheimer's
Disease Neuroimaging I (2015) White matter signal abnormality quality
differentiates mild cognitive impairment that converts to Alzheimer's disease from
nonconverters. Neurobiology of aging, 36: 2447-2457.
101. Dean DC, 3rd, Lange N, Travers BG, Prigge MB, Matsunami N, Kellett KA,
Freeman A, Kane KL, Adluru N, Tromp DPM, Destiche DJ, Samsin D, Zielinski
BA, Fletcher PT, Anderson JS, Froehlich AL, Leppert MF, Bigler ED, Lainhart
JE, Alexander AL (2017) Multivariate characterization of white matter
heterogeneity in autism spectrum disorder. NeuroImage. Clinical, 14: 54-66.
102. Penny KI (1996) Appropriate Critical Values When Testing for a Single
Multivariate Outlier by Using the Mahalanobis Distance. Journal of the Royal
Statistical Society. Series C (Applied Statistics), 45: 73-81.
103. Wilks SS (1963) Multivariate Statistical Outliers. Sankhyā: The Indian
Journal of Statistics, Series A (1961-2002), 25: 407-426.
104. Takeshita T, Nozawa S, Kimura F. On the bias of Mahalanobis distance due to
limited sample size effect. in Document Analysis and Recognition, 1993.,
Proceedings of the Second International Conference on. 1993.

121
105. WHO (2017) Global action plan on the public health response to dementia 2017 -
2025. 44.
106. Mattsson N, Zetterberg H, Hansson O, Andreasen N, Parnetti L, Jonsson M,
Herukka SK, van der Flier WM, Blankenstein MA, Ewers M, Rich K, Kaiser E,
Verbeek M, Tsolaki M, Mulugeta E, Rosen E, Aarsland D, Visser PJ, Schroder J,
Marcusson J, de LM, Hampel H, Scheltens P, Pirttila T, Wallin A, Jonhagen ME,
Minthon L, Winblad B, Blennow K (2009) CSF biomarkers and incipient
Alzheimer disease in patients with mild cognitive impairment. JAMA, 302: 385-
393.
107. Petersen RC (2004) Mild cognitive impairment as a diagnostic entity. J. Intern.
Med, 256: 183-194.
108. Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST
(2001) Practice parameter: early detection of dementia: mild cognitive
impairment (an evidence-based review). Report of the Quality Standards
Subcommittee of the American Academy of Neurology. Neurology, 56: 1133-
1142.
109. Bischkopf J, Busse A, Angermeyer MC (2002) Mild cognitive impairment--a
review of prevalence, incidence and outcome according to current approaches.
Acta Psychiatr. Scand, 106: 403-414.
110. Csukly G, Siraly E, Fodor Z, Horvath A, Salacz P, Hidasi Z, Csibri E, Rudas G,
Szabo A (2016) The Differentiation of Amnestic Type MCI from the Non-
Amnestic Types by Structural MRI. Front Aging Neurosci, 8: 52.
111. Grundman M (2004) MIld cognitive impairment can be distinguished from
alzheimer disease and normal aging for clinical trials. Archives of Neurology, 61:
59-66.
112. Chiang GC, Insel PS, Tosun D, Schuff N, Truran-Sacrey D, Raptentsetsang S,
Jack CR, Weiner MW, For the Alzheimer’s Disease Neuroimaging I (2011)
Identifying Cognitively Healthy Elderly Individuals with Subsequent Memory
Decline by Using Automated MR Temporoparietal Volumes. Radiology, 259:
844-851.
113. Desikan RS, Cabral HJ, Hess CP, Dillon WP, Glastonbury CM, Weiner MW,
Schmansky NJ, Greve DN, Salat DH, Buckner RL, Fischl B (2009) Automated

122
MRI measures identify individuals with mild cognitive impairment and
Alzheimer's disease. Brain, 132: 2048-57.
114. Serra L, Giulietti G, Cercignani M, Spano B, Torso M, Castelli D, Perri R, Fadda
L, Marra C, Caltagirone C, Bozzali M (2013) Mild cognitive impairment: same
identity for different entities. J Alzheimers Dis, 33: 1157-65.
115. de la Monte SM (1989) Quantitation of cerebral atrophy in preclinical and end-
stage Alzheimer's disease. Ann Neurol, 25: 450-9.
116. Oishi K, Lyketsos CG (2014) Alzheimer’s disease and the fornix. Frontiers in
Aging Neuroscience, 6: 241.
117. Delano-Wood L, Stricker NH, Sorg SF, Nation DA, Jak AJ, Woods SP, Libon DJ,
Delis DC, Frank LR, Bondi MW (2012) Posterior cingulum white matter
disruption and its associations with verbal memory and stroke risk in mild
cognitive impairment. J Alzheimers Dis, 29: 589-603.
118. Nowrangi MA, Rosenberg PB (2015) The fornix in mild cognitive impairment
and Alzheimer's disease. Front Aging Neurosci, 7: 1.
119. Kantarci K (2014) Fractional anisotropy of the fornix and hippocampal atrophy in
Alzheimer's disease. Front Aging Neurosci, 6: 316.
120. Kantarci K, Senjem ML, Avula R, Zhang B, Samikoglu AR, Weigand SD,
Przybelski SA, Edmonson HA, Vemuri P, Knopman DS, Boeve BF, Ivnik RJ,
Smith GE, Petersen RC, Jack CR, Jr. (2011) Diffusion tensor imaging and
cognitive function in older adults with no dementia. Neurology, 77: 26-34.
121. Zhang B, Xu Y, Zhu B, Kantarci K (2014) The role of diffusion tensor imaging
in detecting microstructural changes in prodromal Alzheimer's disease. CNS
Neurosci Ther, 20: 3-9.
122. Fellgiebel A, Yakushev I (2011) Diffusion tensor imaging of the hippocampus in
MCI and early Alzheimer's disease. J Alzheimers Dis, 26 Suppl 3: 257-62.
123. Stebbins GT, Murphy CM (2009) Diffusion tensor imaging in Alzheimer's disease
and mild cognitive impairment. Behav Neurol, 21: 39-49.
124. O'Dwyer L, Lamberton F, Bokde AL, Ewers M, Faluyi YO, Tanner C, Mazoyer
B, O'Neill D, Bartley M, Collins DR, Coughlan T, Prvulovic D, Hampel H (2011)
Multiple indices of diffusion identifies white matter damage in mild cognitive
impairment and Alzheimer's disease. PLoS One, 6: e21745.

123
125. Kwan P, Schachter SC, Brodie MJ (2011) Drug-resistant epilepsy. N Engl J Med,
365: 919-26.
126. McCagh J, Fisk JE, Baker GA (2009) Epilepsy, psychosocial and cognitive
functioning. Epilepsy Res, 86: 1-14.
127. Sisodiya SM (2004) Malformations of cortical development: burdens and insights
from important causes of human epilepsy. Lancet Neurol, 3: 29-38.
128. Blumcke I, Spreafico R, Haaker G, Coras R, Kobow K, Bien CG, Pfäfflin M,
Elger C, Widman G, Schramm J, Becker A, Braun KP, Leijten F, Baayen JC,
Aronica E, Chassoux F, Hamer H, Stefan H, Rössler K, Thom M, Walker MC,
Sisodiya SM, Duncan JS, McEvoy AW, Pieper T, Holthausen H, Kudernatsch M,
Meencke HJ, Kahane P, Schulze-Bonhage A, Zentner J, Heiland DH, Urbach H,
Steinhoff BJ, Bast T, Tassi L, Lo Russo G, Özkara C, Oz B, Krsek P, Vogelgesang
S, Runge U, Lerche H, Weber Y, Honavar M, Pimentel J, Arzimanoglou A, Ulate-
Campos A, Noachtar S, Hartl E, Schijns O, Guerrini R, Barba C, Jacques TS,
Cross JH, Feucht M, Mühlebner A, Grunwald T, Trinka E, Winkler PA, Gil-Nagel
A, Toledano Delgado R, Mayer T, Lutz M, Zountsas B, Garganis K, Rosenow F,
Hermsen A, von Oertzen TJ, Diepgen TL, Avanzini G (2017) Histopathological
Findings in Brain Tissue Obtained during Epilepsy Surgery. New England Journal
of Medicine, 377: 1648-1656.
129. Colombo N, Bargalló N, Redaelli D, Neuroimaging Evaluation in Neocortical
Epilepsies: The ESNR Textbook. 2018. 1-35.
130. Urbach H, Long-Term Epilepsy Associated Tumors, In Barkhof F, Jager R,
Thurnher M,Rovira Cañellas A, Editors: Clinical Neuroradiology: The ESNR
Textbook, Springer International Publishing, Cham. 2018. 1-13.
131. Barkovich AJ, Guerrini R, Kuzniecky RI, Jackson GD, Dobyns WB (2012) A
developmental and genetic classification for malformations of cortical
development: update 2012. Brain, 135: 1348-1369.
132. Bien CG, Szinay M, Wagner J, Clusmann H, Becker AJ, Urbach H (2009)
Characteristics and surgical outcomes of patients with refractory magnetic
resonance imaging-negative epilepsies. Arch Neurol, 66: 1491-9.

124
133. Hong SJ, Bernhardt BC, Caldairou B, Hall JA, Guiot MC, Schrader D, Bernasconi
N, Bernasconi A (2017) Multimodal MRI profiling of focal cortical dysplasia type
II. Neurology, 88: 734-742.
134. Urbach H, Mast H, Egger K, Mader I (2015) Presurgical MR Imaging in Epilepsy.
Clinical Neuroradiology, 25: 151-155.
135. Huppertz HJ, Grimm C, Fauser S, Kassubek J, Mader I, Hochmuth A, Spreer J,
Schulze-Bonhage A (2005) Enhanced visualization of blurred gray-white matter
junctions in focal cortical dysplasia by voxel-based 3D MRI analysis. Epilepsy
Res, 67: 35-50.
136. Huppertz HJ, Wellmer J, Staack AM, Altenmuller DM, Urbach H, Kroll J (2008)
Voxel-based 3D MRI analysis helps to detect subtle forms of subcortical band
heterotopia. Epilepsia, 49: 772-85.
137. Wagner J, Weber B, Urbach H, Elger CE, Huppertz HJ (2011) Morphometric MRI
analysis improves detection of focal cortical dysplasia type II. Brain, 134: 2844-
54.
138. Filippi CG, Maxwell AW, Watts R (2013) Magnetic resonance diffusion tensor
imaging metrics in perilesional white matter among children with periventricular
nodular gray matter heterotopia. Pediatr Radiol, 43: 1196-203.
139. Fonseca Vde C, Yasuda CL, Tedeschi GG, Betting LE, Cendes F (2012) White
matter abnormalities in patients with focal cortical dysplasia revealed by diffusion
tensor imaging analysis in a voxelwise approach. Front Neurol, 3: 121.
140. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczynski K (2005) Diffusional kurtosis
imaging: the quantification of non-gaussian water diffusion by means of magnetic
resonance imaging. Magn Reson Med, 53: 1432-40.
141. Bonilha L, Lee CY, Jensen JH, Tabesh A, Spampinato MV, Edwards JC,
Breedlove J, Helpern JA (2015) Altered microstructure in temporal lobe epilepsy:
a diffusional kurtosis imaging study. AJNR Am J Neuroradiol, 36: 719-24.
142. Winston GP, Micallef C, Symms MR, Alexander DC, Duncan JS, Zhang H (2014)
Advanced diffusion imaging sequences could aid assessing patients with focal
cortical dysplasia and epilepsy. Epilepsy Research, 108: 336-339.
143. Umesh Rudrapatna S, Wieloch T, Beirup K, Ruscher K, Mol W, Yanev P,
Leemans A, van der Toorn A, Dijkhuizen RM (2014) Can diffusion kurtosis

125
imaging improve the sensitivity and specificity of detecting microstructural
alterations in brain tissue chronically after experimental stroke? Comparisons
with diffusion tensor imaging and histology. Neuroimage, 97: 363-73.
144. Hua K, Zhang J, Wakana S, Jiang H, Li X, Reich DS, Calabresi PA, Pekar JJ, van
Zijl PC, Mori S (2008) Tract probability maps in stereotaxic spaces: analyses of
white matter anatomy and tract-specific quantification. Neuroimage, 39: 336-47.
145. Mori S, Wakana S, van-Zijl PCM, Nagae-Poetscher L, MRI Atlas of Human
White Matter. 1st ed. Elsevier, The Netherlands, Amsterdam, 2005: 276.
146. Wakana S, Caprihan A, Panzenboeck MM, Fallon JH, Perry M, Gollub RL, Hua
K, Zhang J, Jiang H, Dubey P, Blitz A, van Zijl P, Mori S (2007) Reproducibility
of quantitative tractography methods applied to cerebral white matter.
Neuroimage, 36: 630-44.
147. Kohavi R. A study of cross-validation and bootstrap for accuracy estimation and
model selection. in Ijcai. 1995. Stanford, CA.
148. Csukly G, Sirály E, Fodor Z, Horváth A, Salacz P, Hidasi Z, Csibri É, Rudas G,
Szabó Á (2016) The Differentiation of Amnestic Type MCI from the Non-
Amnestic Types by Structural MRI. Front Aging Neurosci, 8: 52.
149. Gomar JJ, Bobes-Bascaran MT, Conejero-Goldberg C, Davies P, Goldberg TE
(2011) Utility of combinations of biomarkers, cognitive markers, and risk factors
to predict conversion from mild cognitive impairment to Alzheimer disease in
patients in the Alzheimer's disease neuroimaging initiative. Arch. Gen.
Psychiatry, 68: 961-969.
150. Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A,
Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps
CH (2011) The diagnosis of mild cognitive impairment due to Alzheimer's
disease: recommendations from the National Institute on Aging-Alzheimer's
Association workgroups on diagnostic guidelines for Alzheimer's disease.
Alzheimers. Dement, 7: 270-279.
151. Strauss E, Sherman E, Spreen O, Mini Mental State Examination (MMSE):
Compendium of Neuropsychological tests, Oxford University Press. 2006. 168-
188.

126
152. Leemans A, Jeurissen B, Sijbers J, Jones D (2009) ExploreDTI: a graphical
toolbox for processing, analyzing, and visualizing diffusion MR data. 17th Annual
Meeting of Intl Soc Mag Reson Med: 3537.
153. Jezzard P, Barnett AS, Pierpaoli C (1998) Characterization of and correction for
eddy current artifacts in echo planar diffusion imaging. Magnetic Resonance in
Medicine, 39: 801-812.
154. Alexander AL, Hurley SA, Samsonov AA, Adluru N, Hosseinbor AP, Mossahebi
P, Tromp do PM, Zakszewski E, Field AS (2011) Characterization of cerebral
white matter properties using quantitative magnetic resonance imaging stains.
Brain Connect, 1: 423-46.
155. Pierpaoli C, Basser PJ (1996) Toward a quantitative assessment of diffusion
anisotropy. Magn Reson Med, 36: 893-906.
156. Simon L, Kozak LR, Simon V, Czobor P, Unoka Z, Szabo A, Csukly G (2013)
Regional grey matter structure differences between transsexuals and healthy
controls--a voxel based morphometry study. PLoS One, 8: e83947.
157. Fushimi Y, Okada T, Takagi Y, Funaki T, Takahashi JC, Miyamoto S, Togashi K
(2016) Voxel Based Analysis of Surgical Revascularization for Moyamoya
Disease: Pre- and Postoperative SPECT Studies. PLoS One, 11: e0148925.
158. Mazziotta J, Toga A, Evans A, Fox P, Lancaster J, Zilles K, Woods R, Paus T,
Simpson G, Pike B, Holmes C, Collins L, Thompson P, MacDonald D, Iacoboni
M, Schormann T, Amunts K, Palomero-Gallagher N, Geyer S, Parsons L, Narr K,
Kabani N, Le Goualher G, Boomsma D, Cannon T, Kawashima R, Mazoyer B
(2001) A probabilistic atlas and reference system for the human brain:
International Consortium for Brain Mapping (ICBM). Philos Trans R Soc Lond
B Biol Sci, 356: 1293-322.
159. Gaser C. Manual Computational Anatomy Toolbox - CAT12. 2016; Available
from: http://dbm.neuro.uni-jena.de/cat12/CAT12-Manual.pdf.
160. Bach M, Laun FB, Leemans A, Tax CM, Biessels GJ, Stieltjes B, Maier-Hein KH
(2014) Methodological considerations on tract-based spatial statistics (TBSS).
Neuroimage, 100: 358-69.
161. Nusbaum AO (2002) Diffusion tensor MR imaging of gray matter in different
multiple sclerosis phenotypes. AJNR Am J Neuroradiol, 23: 899-900.

127
162. Pfefferbaum A, Adalsteinsson E, Rohlfing T, Sullivan EV (2010) Diffusion tensor
imaging of deep gray matter brain structures: effects of age and iron concentration.
Neurobiol Aging, 31: 482-93.
163. Salminen LE, Conturo TE, Laidlaw DH, Cabeen RP, Akbudak E, Lane EM,
Heaps JM, Bolzenius JD, Baker LM, Cooley S, Scott S, Cagle LM, Phillips S,
Paul RH (2016) Regional age differences in gray matter diffusivity among healthy
older adults. Brain Imaging Behav, 10: 203-11.
164. Holm S (1979) A simple sequentially rejective multiple test procedure.
Scandinavian Journal of Statistics, 6: 65-70.
165. Benjamini Y, Hochberg Y (1995) Controlling the False Discovery Rate: A
Practical and Powerful Approach to Multiple Testing. Journal of the Royal
Statistical Society. Series B (Methodological), 57: 289-300.
166. Acosta-Cabronero J, Williams GB, Pengas G, Nestor PJ (2010) Absolute
diffusivities define the landscape of white matter degeneration in Alzheimer's
disease. Brain, 133: 529-39.
167. Cavaliere C, Aiello M, Di Perri C, Fernandez-Espejo D, Owen AM, Soddu A
(2014) Diffusion tensor imaging and white matter abnormalities in patients with
disorders of consciousness. Front Hum Neurosci, 8: 1028.
168. Sajjadi SA, Acosta-Cabronero J, Patterson K, Diaz-de-Grenu LZ, Williams GB,
Nestor PJ (2013) Diffusion tensor magnetic resonance imaging for single subject
diagnosis in neurodegenerative diseases. Brain, 136: 2253-61.
169. Sun Y, Yin Q, Fang R, Yan X, Wang Y, Bezerianos A, Tang H, Miao F, Sun J
(2014) Disrupted functional brain connectivity and its association to structural
connectivity in amnestic mild cognitive impairment and Alzheimer's disease.
PLoS One, 9: e96505.
170. Ukmar M, Makuc E, Onor ML, Garbin G, Trevisiol M, Cova MA (2008)
Evaluation of white matter damage in patients with Alzheimer's disease and in
patients with mild cognitive impairment by using diffusion tensor imaging. Radiol
Med, 113: 915-22.
171. Sexton CE, Kalu UG, Filippini N, Mackay CE, Ebmeier KP (2011) A meta-
analysis of diffusion tensor imaging in mild cognitive impairment and Alzheimer's
disease. Neurobiol Aging, 32: 2322.e5-18.

128
172. Klein S, Staring M, Murphy K, Viergever MA, Pluim JPW (2010) elastix: A
Toolbox for Intensity-Based Medical Image Registration. IEEE Transactions on
Medical Imaging, 29: 196-205.
173. Dyrby TB, Lundell H, Burke MW, Reislev NL, Paulson OB, Ptito M, Siebner HR
(2014) Interpolation of diffusion weighted imaging datasets. Neuroimage, 103:
202-13.
174. Smith SM, Nichols TE (2009) Threshold-free cluster enhancement: addressing
problems of smoothing, threshold dependence and localisation in cluster
inference. Neuroimage, 44: 83-98.
175. Preti MG, Makris N, Papadimitriou G, Lagana MM, Griffanti L, Clerici M, Nemni
R, Westin CF, Baselli G, Baglio F (2014) A novel approach of groupwise fMRI-
guided tractography allowing to characterize the clinical evolution of Alzheimer's
disease. PLoS ONE [Electronic Resource], 9: e92026.
176. Goldstein FC, Mao H, Wang L, Ni C, Lah JJ, Levey AI (2009) White Matter
Integrity and Episodic Memory Performance in Mild Cognitive Impairment: A
Diffusion Tensor Imaging Study. Brain Imaging Behav, 3: 132-141.
177. Bosch B, Arenaza-Urquijo EM, Rami L, Sala-Llonch R, Junque C, Sole-Padulles
C, Pena-Gomez C, Bargallo N, Molinuevo JL, Bartres-Faz D (2012) Multiple DTI
index analysis in normal aging, amnestic MCI and AD. Relationship with
neuropsychological performance. Neurobiol Aging, 33: 61-74.
178. Braak H, Braak E (1990) Neurofibrillary changes confined to the entorhinal
region and an abundance of cortical amyloid in cases of presenile and senile
dementia. Acta Neuropathol, 80: 479-86.
179. Echávarri C, Aalten P, Uylings HBM, Jacobs HIL, Visser PJ, Gronenschild
EHBM, Verhey FRJ, Burgmans S (2011) Atrophy in the parahippocampal gyrus
as an early biomarker of Alzheimer’s disease. Brain Structure & Function, 215:
265-271.
180. Badre D, Wagner AD (2007) Left ventrolateral prefrontal cortex and the cognitive
control of memory. Neuropsychologia, 45: 2883-901.
181. Arsalidou M, Taylor MJ (2011) Is 2+2=4? Meta-analyses of brain areas needed
for numbers and calculations. Neuroimage, 54: 2382-93.

129
182. Seghier ML (2013) The angular gyrus: multiple functions and multiple
subdivisions. Neuroscientist, 19: 43-61.
183. Zhuang L, Sachdev PS, Trollor JN, Reppermund S, Kochan NA, Brodaty H, Wen
W (2013) Microstructural White Matter Changes, Not Hippocampal Atrophy,
Detect Early Amnestic Mild Cognitive Impairment. PLOS ONE, 8: e58887.
184. Villain N, Desgranges B, Viader F, De La Sayette V, Mézenge F, Landeau B,
Baron J-C, Eustache F, Chételat G (2008) Relationships between hippocampal
atrophy, white matter disruption, and gray matter hypometabolism in Alzheimer's
disease. The Journal of Neuroscience, 28: 6174-6181.
185. Poletti CE, Creswell G (1977) Fornix system efferent projections in the squirrel
monkey: an experimental degeneration study. J Comp Neurol, 175: 101-28.
186. Bozoki AC, Korolev IO, Davis NC, Hoisington LA, Berger KL (2012) Disruption
of limbic white matter pathways in mild cognitive impairment and Alzheimer's
disease: a DTI/FDG-PET study. Hum Brain Mapp, 33: 1792-802.
187. Bailly M, Destrieux C, Hommet C, Mondon K, Cottier J-P, Beaufils E, Vierron
E, Vercouillie J, Ibazizene M, Voisin T, Payoux P, Barré L, Camus V, Guilloteau
D, Ribeiro M-J (2015) Precuneus and Cingulate Cortex Atrophy and
Hypometabolism in Patients with Alzheimer's Disease and Mild Cognitive
Impairment: MRI and (18)F-FDG PET Quantitative Analysis Using FreeSurfer.
BioMed Research International, 2015: 583931.
188. Ikonomovic MD, Abrahamson EE, Isanski BA, Wuu J, Mufson EJ, DeKosky ST
(2007) Superior frontal cortex cholinergic axon density in mild cognitive
impairment and early Alzheimer disease. Arch Neurol, 64: 1312-7.
189. Nowrangi MA, Lyketsos CG, Leoutsakos JM, Oishi K, Albert M, Mori S, Mielke
MM (2013) Longitudinal, region-specific course of diffusion tensor imaging
measures in mild cognitive impairment and Alzheimer's disease. Alzheimers
Dement, 9: 519-28.
190. Zhuang L, Wen W, Zhu W, Trollor J, Kochan N, Crawford J, Reppermund S,
Brodaty H, Sachdev P (2010) White matter integrity in mild cognitive
impairment: a tract-based spatial statistics study. Neuroimage, 53: 16-25.
191. Mielke MM, Kozauer NA, Chan KC, George M, Toroney J, Zerrate M, Bandeen-
Roche K, Wang MC, Vanzijl P, Pekar JJ, Mori S, Lyketsos CG, Albert M (2009)
130
Regionally-specific diffusion tensor imaging in mild cognitive impairment and
Alzheimer's disease. Neuroimage, 46: 47-55.
192. Thillainadesan S, Wen W, Zhuang L, Crawford J, Kochan N, Reppermund S,
Slavin M, Trollor J, Brodaty H, Sachdev P (2012) Changes in mild cognitive
impairment and its subtypes as seen on diffusion tensor imaging. Int
Psychogeriatr, 24: 1483-93.
193. Vasconcelos Lde G, Jackowski AP, Oliveira MO, Flor YM, Souza AA, Bueno
OF, Brucki SM (2014) The thickness of posterior cortical areas is related to
executive dysfunction in Alzheimer's disease. Clinics (Sao Paulo), 69: 28-37.
194. Coutinho AM, Porto FH, Duran FL, Prando S, Ono CR, Feitosa EA, Spindola L,
de Oliveira MO, do Vale PH, Gomes HR, Nitrini R, Brucki SM, Buchpiguel CA
(2015) Brain metabolism and cerebrospinal fluid biomarkers profile of non-
amnestic mild cognitive impairment in comparison to amnestic mild cognitive
impairment and normal older subjects. Alzheimers Res Ther, 7: 58.
195. Machulda MM, Senjem ML, Weigand SD, Smith GE, Ivnik RJ, Boeve BF,
Knopman DS, Petersen RC, Jack CR (2009) Functional magnetic resonance
imaging changes in amnestic and nonamnestic mild cognitive impairment during
encoding and recognition tasks. J Int Neuropsychol Soc, 15: 372-82.
196. Wang L, Goldstein FC, Veledar E, Levey AI, Lah JJ, Meltzer CC, Holder CA,
Mao H (2009) Alterations in cortical thickness and white matter integrity in mild
cognitive impairment measured by whole-brain cortical thickness mapping and
diffusion tensor imaging. AJNR Am J Neuroradiol, 30: 893-9.
197. Tournier JD, Calamante F, Gadian DG, Connelly A (2004) Direct estimation of
the fiber orientation density function from diffusion-weighted MRI data using
spherical deconvolution. Neuroimage, 23: 1176-85.
198. Tournier JD, Yeh CH, Calamante F, Cho KH, Connelly A, Lin CP (2008)
Resolving crossing fibres using constrained spherical deconvolution: validation
using diffusion-weighted imaging phantom data. Neuroimage, 42: 617-25.
199. Beyer KS, Goldstein J, Ramakrishnan R, Shaft U, When Is ''Nearest Neighbor''
Meaningful?, in Proceedings of the 7th International Conference on Database
Theory. 1999, Springer-Verlag. p. 217-235.

131
200. Schnitzer D. FA (2014) Choosing the Metric in High-Dimensional Spaces Based
on Hub Analysis. Proceedings of the 22nd European Symposium on Artificial
Neural Networks, Computational Intelligence and Machine Learning, Bruges,
Belgium.
201. Adler S, Lorio S, Jacques TS, Benova B, Gunny R, Cross JH, Baldeweg T,
Carmichael DW (2017) Towards in vivo focal cortical dysplasia phenotyping
using quantitative MRI. Neuroimage Clin, 15: 95-105.
202. Van Hecke W, Leemans A, De Backer S, Jeurissen B, Parizel PM, Sijbers J (2010)
Comparing isotropic and anisotropic smoothing for voxel-based DTI analyses: A
simulation study. Human Brain Mapping, 31: 98-114.
203. Bhaganagarapu K, Jackson G, Abbott D (2013) An Automated Method for
Identifying Artifact in Independent Component Analysis of Resting-State fMRI.
Frontiers in Human Neuroscience, 7.
204. Salimi-Khorshidi G, Douaud G, Beckmann CF, Glasser MF, Griffanti L, Smith
SM (2014) Automatic denoising of functional MRI data: combining independent
component analysis and hierarchical fusion of classifiers. Neuroimage, 90: 449-
68.
205. van Diessen E, Diederen SJ, Braun KP, Jansen FE, Stam CJ (2013) Functional
and structural brain networks in epilepsy: what have we learned? Epilepsia, 54:
1855-65.
206. Jin B, Krishnan B, Adler S, Wagstyl K, Hu W, Jones S, Najm I, Alexopoulos A,
Zhang K, Zhang J, Ding M, Wang S, Wang ZI (2018) Automated detection of
focal cortical dysplasia type II with surface-based magnetic resonance imaging
postprocessing and machine learning. Epilepsia, 59: 982-992.
207. Jeong J-W, Asano E, Juhász C, Chugani HT (2014) Quantification of Primary
Motor Pathways Using Diffusion MRI Tractography and Its Application to
Predict Postoperative Motor Deficits in Children With Focal Epilepsy. Human
brain mapping, 35: 3216-3226.
208. Scarpazza C, Nichols TE, Seramondi D, Maumet C, Sartori G, Mechelli A (2016)
When the Single Matters more than the Group (II): Addressing the Problem of
High False Positive Rates in Single Case Voxel Based Morphometry Using Non-
parametric Statistics. Frontiers in Neuroscience, 10.

132
List of publications
1. Articles related to the thesis
Gyebnar G, Szabo A, Siraly E, Fodor Z, Sakovics A, Salacz P, Hidasi Z, Csibri E, Rudas
G, Kozak LR, Csukly G (2018) What can DTI tell about early cognitive impairment? -
Differentiation between MCI subtypes and healthy controls by diffusion tensor imaging.
Psychiatry Res Neuroimaging, 272: 46-57.
https://doi.org/10.1016/j.pscychresns.2017.10.007
IF: 2.270
Gyebnar G, Klimaj Z, Entz L, Fabo D, Rudas G, Barsi P,Kozak LR (2019) Personalized
microstructural evaluation using a Mahalanobis-distance based outlier detection strategy
on epilepsy patients' DTI data - Theory, simulations and example cases. PLoS One:
14(9):e0222720.
https://doi.org/10.1371/journal.pone.0222720
IF: 2.740
2. Other articles
Lakatos A, Kolossvary M, Szabo M, Jermendy A, Barta H, Gyebnar G, Rudas G, Kozak
LR (2019) Neurodevelopmental effect of intracranial hemorrhage observed in hypoxic
ischemic brain injury in hypothermia-treated asphyxiated neonates - an MRI study. BMC
Pediatr,19(1):430.
https://doi.org/10.1186/s12887-019-1777-z
IF: 1.909
Csukly G, Szabó Á, Polgár P, Farkas K, Gyebnár G, Kozák LR, Stefanics G (2020).
Fronto-thalamic structural and effective connectivity and delusions in schizophrenia: A
combined DTI/DCM study. Psychological Medicine, 1-11.
https://doi.org/10.1017/S0033291720000859
IF: 5.813 (2019)

133
Acknowledgements
First and foremost I would like to thank Dr. Lajos R Kozák for his guidance and
supervision throughout my projects. His valuable insights, critical suggestions, and
thorough proofreading of all of my texts helped me improve as a researcher and made this
dissertation possible through innumerable ways. I would like to thank Dr. Gábor Rudas
for supporting and facilitating my work with the opportunities to focus on my research
and participate in the research community. I would also like to thank Prof. Péter Barsi for
sharing his vast knowledge in Neuroradiology and supporting the evaluation of our results
with critical insights and practical suggestions. I am grateful to Dr. Gábor Csukly for his
advices, suggestions, and effort during our cooperation. I would like to thank all of my
colleagues at the Department of Neuroradiology (the former MR Research Centre –
MRKK), for their support and understanding, and all their help I received in learning the
language of the medical field and fitting into the everyday work in the clinical
environment. Last but not least, I would like to thank my family, especially my loving
wife Emese, for their patience and unquestioning support throughout my PhD education
and candidacy.

134
Reprints of publications related to the thesis

135
Supplementary material

136
Table S1 Logistic regression: amnestic MCI vs. Control – only volumetry
Test set
no. Subject ID From: group Into: group Effect1 Effect2 Correct Mean
1
15 Control Control
Left HippocampusV
meanthickavg precuneusT
1
0.75 16 Control Control 1
49 a-MCI Control 0
56 a-MCI a-MCI 1
2
24 Control a-MCI
Right
HippocampusV
0
0.25 31 Control a-MCI 0
60 a-MCI Control 0
67 a-MCI a-MCI 1
3
33 Control Control
Left
HippocampusV
1
1 34 Control Control 1
77 a-MCI a-MCI 1
81 a-MCI a-MCI 1
4
37 Control Control
Left HippocampusV
1
0.5 39 Control Control 1
89 a-MCI Control 0
301 a-MCI Control 0
5
40 Control Control
Left HippocampusV
meanthickavg precuneusT
1
0.75 42 Control Control 1
364 a-MCI a-MCI 1
879 a-MCI Control 0
6
48 Control Control
Left
HippocampusV
1
1 75 Control Control 1
30971 a-MCI a-MCI 1
34845 a-MCI a-MCI 1
7
76 Control Control
Left
HippocampusV
1
1 193 Control Control 1
60294 a-MCI a-MCI 1
69355 a-MCI a-MCI 1
8
198 Control Control
Right HippocampusV
1
1 200 Control Control 1
69359 a-MCI a-MCI 1
69367 a-MCI a-MCI 1
9
332 Control Control
Left
HippocampusV
1
1 631 Control Control 1
69371 a-MCI a-MCI 1
69376 a-MCI a-MCI 1
10 23074 Control Control Left
HippocampusV
meanthickavg
precuneusT
1 0.5
60293 Control a-MCI 0
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1 & 2:
volumetric, or cortical thickness measurements deemed meaningful in the stepwise logistic regression; a‒
MCI: amnestic mild cognitive impairment; meanthickavg: average cortical thickness; Correct: indicator
signaling correct test decision; Mean: decision performance in each subgroup. V: volumetry‒based measure
T: thickness‒based measure

137
Table S2 Logistic regression: amnestic MCI vs. Control – volumetry with FA
Test set
no.
Subject
ID From: group Into: group Effect1 Effect2 Effect3 Correct Mean
1
15 Control Control
Left
HippocampusV
meanthickavg
precuneusT
1
0.75 16 Control Control 1
49 a-MCI Control 0
56 a-MCI a-MCI 1
2
24 Control a-MCI
Left
HippocampusV
0
0.25 31 Control a-MCI 0
60 a-MCI Control 0
67 a-MCI a-MCI 1
3
33 Control Control
Left
HippocampusV
1
1 34 Control Control 1
77 a-MCI a-MCI 1
81 a-MCI a-MCI 1
4
37 Control Control
Left
HippocampusV
1
0.5 39 Control Control 1
89 a-MCI Control 0
301 a-MCI Control 0
5
40 Control Control
Left
HippocampusV
meanthickavg
precuneusT
1
0.75 42 Control Control 1
364 a-MCI a-MCI 1
879 a-MCI Control 0
6
48 Control Control
Left
HippocampusV
1
1 75 Control Control 1
30971 a-MCI a-MCI 1
34845 a-MCI a-MCI 1
7
76 Control Control
Left
HippocampusV
1
1 193 Control Control 1
60294 a-MCI a-MCI 1
69355 a-MCI a-MCI 1
8
198 Control Control
Right
HippocampusV
1
1 200 Control Control 1
69359 a-MCI a-MCI 1
69367 a-MCI a-MCI 1
9
332 Control Control
Left
HippocampusV
1
1 631 Control Control 1
69371 a-MCI a-MCI 1
69376 a-MCI a-MCI 1
10 23074 Control Control Left
HippocampusV
meanthickavg
precuneusT
Fornix crus Stria
terminalis LDTI
1 0.5
60293 Control a-MCI 0
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1, 2 & 3:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
a‒MCI: amnestic mild cognitive impairment; meanthickavg: average cortical thickness; Correct: indicator
signaling correct test decision; Mean: decision performance in each subgroup; V: volumetry‒based measure;
T: thickness‒based measure; DTI: DTI‒based measure

138
Table S3 Logistic regression: amnestic MCI vs. Control – volumetry with MD
Test set
no. Subject ID From: group Into: group Effect1 Effect2 Correct Mean
1
15 Control Control
Left
HippocampusV
meanthickavg
precuneusT
1
0.75 16 Control Control 1
49 a-MCI Control 0
56 a-MCI a-MCI 1
2
24 Control a-MCI
Left
HippocampusV
meanthickavg
precuneusT
0
0.5 31 Control Control 1
60 a-MCI Control 0
67 a-MCI a-MCI 1
3
33 Control Control
Left
HippocampusV
1
1 34 Control Control 1
77 a-MCI a-MCI 1
81 a-MCI a-MCI 1
4
37 Control Control
Left
HippocampusV
1
0.5 39 Control Control 1
89 a-MCI Control 0
301 a-MCI Control 0
5
40 Control Control
Left
HippocampusV
meanthickavg
precuneusT
1
0.75 42 Control Control 1
364 a-MCI a-MCI 1
879 a-MCI Control 0
6
48 Control Control
Left
HippocampusV
1
1 75 Control Control 1
30971 a-MCI a-MCI 1
34845 a-MCI a-MCI 1
7
76 Control Control
Left
HippocampusV
1
1 193 Control Control 1
60294 a-MCI a-MCI 1
69355 a-MCI a-MCI 1
8
198 Control Control
Right
HippocampusV
1
1 200 Control Control 1
69359 a-MCI a-MCI 1
69367 a-MCI a-MCI 1
9
332 Control Control
Left
HippocampusV
1
1 631 Control Control 1
69371 a-MCI a-MCI 1
69376 a-MCI a-MCI 1
10 23074 Control Control Left
HippocampusV
1 0.5
60293 Control a-MCI 0
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1 & 2:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
a‒MCI: amnestic mild cognitive impairment; meanthickavg: average cortical thickness; Correct: indicator
signaling correct test decision; Mean: decision performance in each subgroup; V: volumetry based measure;
T: thickness based measure

139
Table S4 Logistic regression: non‒amnestic MCI vs. Control – only volumetry
Test set
no. Subject ID From: group Into: group Effect1 Effect2 Correct Mean
1
15 Control Control
meanthickavg
precuneusT
1
0.5 16 Control na-MCI 0
25 na-MCI na-MCI 1
26 na-MCI Control 0
2
24 Control na-MCI
Right
HippocampusV
meanthickavg
precuneusT
0
0.5 31 Control Control 1
36 na-MCI Control 0
38 na-MCI na-MCI 1
3
33 Control na-MCI
meanthickavg
precuneusT
0
0.5 34 Control Control 1
44 na-MCI Control 0
58 na-MCI na-MCI 1
4
37 Control na-MCI
meanthickavg
precuneusT
0
0.5 39 Control Control 1
59 na-MCI na-MCI 1
63 na-MCI Control 0
5
40 Control Control
meanthickavg
precuneusT
1
0.75 42 Control Control 1
74 na-MCI Control 0
216 na-MCI na-MCI 1
6
48 Control Control
Right
HippocampusV
meanthickavg
precuneusT
1
0.5 75 Control Control 1
69357 na-MCI Control 0
69360 na-MCI Control 0
7
76 Control Control
Right
HippocampusV
1
0.5 193 Control Control 1
69361 na-MCI Control 0
69364 na-MCI Control 0
8
198 Control Control
meanthickavg
precuneusT
1
0.5 200 Control na-MCI 0
69372 na-MCI na-MCI 1
69403 na-MCI Control 0
9
332 Control na-MCI
meanthickavg
precuneusT
0
0.5 631 Control Control 1
69404 na-MCI Control 0
69412 na-MCI na-MCI 1
10 23074 Control Control meanthickavg
precuneusT
1 0.5
60293 Control na-MCI 0
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: identifiers used in the study, Form: group: category, as determined by the Petersen criteria (‘truth’);
Into: group: category determined by the models (‘test decision’); Effect1 & 2: volumetric, cortical
thickness, or DTI measurements deemed meaningful in the stepwise logistic regression; na‒MCI: non‒
amnestic mild cognitive impairment; meanthickavg: average cortical thickness; Correct: indicator signaling
correct test decision; Mean: decision performance in each subgroup; V: volumetry based measure; T:
thickness based measure

140
Table S5 Logistic regression: non‒amnestic MCI vs. Control – volumetry with FA
Test sett
no. Subject ID From: group Into: group Effect1 Effect2 Effect3 Correct Mean
1
15 Control Control
meanthickavg
precuneusT
Fornix column &
body of fornixDTI
1
0.75 16 Control na-MCI 0
25 na-MCI na-MCI 1
26 na-MCI na-MCI 1
2
24 Control na-MCI
Right
HippocampusV
meanthickavg
precuneusT
0
0.5 31 Control Control 1
36 na-MCI Control 0
38 na-MCI na-MCI 1
3
33 Control na-MCI
meanthickavg
precuneusT
Posterior thalamic
radiation RDTI
External
capsule RDTI
0
0.25 34 Control Control 1
44 na-MCI Control 0
58 na-MCI Control 0
4
37 Control na-MCI
meanthickavg
precuneusT
External_
capsule_RDTI
0
0.5 39 Control Control 1
59 na-MCI na-MCI 1
63 na-MCI Control 0
5
40 Control Control
meanthickavg
precuneusT
Fornix column &
body of fornixDTI
Superior
fronto occipital
fasciculus
RDTI
1
1 42 Control Control 1
74 na-MCI na-MCI 1
216 na-MCI na-MCI 1
6
48 Control Control Cingulum
hippocampus
LDTI
1
0.25 75 Control na-MCI 0
69357 na-MCI Control 0
69360 na-MCI Control 0
7
76 Control Control
Right
HippocampusV
1
0.5 193 Control Control 1
69361 na-MCI Control 0
69364 na-MCI Control 0
8
198 Control Control
meanthickavg
precuneusT
External
capsule LDTI Tapetum LDTI
1
0.5 200 Control na-MCI 0
69372 na-MCI na-MCI 1
69403 na-MCI Control 0
9
332 Control Control
meanthickavg
precuneusT
Fornix column &
body of fornixDTI
1
0.75 631 Control Control 1
69404 na-MCI Control 0
69412 na-MCI na-MCI 1
10 23074 Control na-MCI meanthickavg
precuneusT
External
capsule LDTI
0 0.5
60293 Control Control 1
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: identifiers used in the study, Form: group: category, as determined by the Petersen criteria (‘truth’);
Into: group: category determined by the models (‘test decision’); Effect1, 2 & 3: volumetric, cortical
thickness, or DTI measurements deemed meaningful in the stepwise logistic regression; na‒MCI: non‒
amnestic mild cognitive impairment; meanthickavg: average cortical thickness; Correct: indicator signaling
correct test decision; Mean: decision performance in each subgroup; V: volumetry based measure; T:
thickness based measure; DTI: DTI‒based measure

141
Table S6 Logistic regression: non‒amnestic MCI vs. Control – volumetry with MD
Test set
no. Subject ID From: group Into: group Effect1 Effect2 Correct Mean
1
15 Control Control
meanthickavg
precuneusT
Cingulum
hippocampus LDTI
1
0.5 16 Control na-MCI 0
25 na-MCI Control 0
26 na-MCI na-MCI 1
2
24 Control na-MCI
Right
HippocampusV
Cingulum
hippocampus LDTI
0
0.25 31 Control na-MCI 0
36 na-MCI Control 0
38 na-MCI na-MCI 1
3
33 Control na-MCI
meanthickavg
precuneusT
0
0.5 34 Control Control 1
44 na-MCI Control 0
58 na-MCI na-MCI 1
4
37 Control Control
meanthickavg
precuneusT
Cingulum
hippocampus LDTI
1
0.75 39 Control Control 1
59 na-MCI na-MCI 1
63 na-MCI Control 0
5
40 Control Control
meanthickavg
precuneusT
Cingulum
hippocampus LDTI
1
0.75 42 Control Control 1
74 na-MCI Control 0
216 na-MCI na-MCI 1
6
48 Control Control
Right
HippocampusV
meanthickavg
precuneusT
1
0.5 75 Control Control 1
69357 na-MCI Control 0
69360 na-MCI Control 0
7
76 Control Control
Right
HippocampusV
1
0.5 193 Control Control 1
69361 na-MCI Control 0
69364 na-MCI Control 0
8
198 Control Control
meanthickavg
precuneusT
External capsule
LDTI
1
0.75 200 Control Control 1
69372 na-MCI na-MCI 1
69403 na-MCI Control 0
9
332 Control Control
meanthickavg
precuneusT
Fornix column &
body of fornixDTI
1
0.75 631 Control Control 1
69404 na-MCI Control 0
69412 na-MCI na-MCI 1
10 23074 Control na-MCI meanthickavg
precuneusT
External capsule
LDTI
0 0.5
60293 Control Control 1
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1, 2 & 3:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
na‒MCI: non‒amnestic mild cognitive impairment; meanthickavg: average cortical thickness; Correct:
indicator signaling correct test decision; Mean: decision performance in each subgroup; V: volumetry based
measure; T: thickness based measure; DTI: DTI‒based measure

142
Table S7 Logistic regression: amnestic vs non‒amnestic MCI – only volumetry
Test set
no. Subject ID From: group Into: group Effect1 Correct Mean
1
25 na-MCI na-MCI
Left
HippocampusV
1
0.5 26 na-MCI a-MCI 0
49 a-MCI na-MCI 0
56 a-MCI a-MCI 1
2
36 na-MCI na-MCI
Left
HippocampusV
1
0.5 38 na-MCI a-MCI 0
60 a-MCI na-MCI 0
67 a-MCI a-MCI 1
3
44 na-MCI na-MCI
Left
HippocampusV
1
1 58 na-MCI na-MCI 1
77 a-MCI a-MCI 1
81 a-MCI a-MCI 1
4
59 na-MCI na-MCI
Left
HippocampusV
1
0.5 63 na-MCI na-MCI 1
89 a-MCI na-MCI 0
301 a-MCI na-MCI 0
5
74 na-MCI a-MCI
Left
HippocampusV
0
0.25 216 na-MCI a-MCI 0
364 a-MCI a-MCI 1
879 a-MCI na-MCI 0
6
69357 na-MCI na-MCI
Left
HippocampusV
1
1 69360 na-MCI na-MCI 1
30971 a-MCI a-MCI 1
34845 a-MCI a-MCI 1
7
69361 na-MCI na-MCI
Left
HippocampusV
1
0.75 69364 na-MCI a-MCI 0
60294 a-MCI a-MCI 1
69355 a-MCI a-MCI 1
8
69372 na-MCI a-MCI
Left
HippocampusV
0
0.75 69403 na-MCI na-MCI 1
69359 a-MCI a-MCI 1
69367 a-MCI a-MCI 1
9
69404 na-MCI na-MCI
Left
HippocampusV
1
0.5 69412 na-MCI a-MCI 0
69371 a-MCI a-MCI 1
69376 a-MCI na-MCI 0
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
a‒MCI: amnestic mild cognitive impairment; na‒MCI: non‒amnestic mild cognitive impairment;
meanthickavg: average cortical thickness; Correct: indicator signaling correct test decision; Mean: decision
performance in each subgroup; V: volumetry based measure

143
Table S8 Logistic regression: amnestic vs non‒amnestic MCI – volumetry with FA
Test set
no. Subject ID From: group Into: group Effect1 Effect2 Correct Mean
1
25 na-MCI na-MCI
Left
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
0.75 26 na-MCI na-MCI 1
49 a-MCI a-MCI 1
56 a-MCI na-MCI 0
2
36 na-MCI na-MCI
Right
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
1 38 na-MCI na-MCI 1
60 a-MCI a-MCI 1
67 a-MCI a-MCI 1
3
44 na-MCI na-MCI
Left
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
1 58 na-MCI na-MCI 1
77 a-MCI a-MCI 1
81 a-MCI a-MCI 1
4
59 na-MCI na-MCI
Left
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
0.25 63 na-MCI a-MCI 0
89 a-MCI na-MCI 0
301 a-MCI na-MCI 0
5
74 na-MCI na-MCI
Left
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
1 216 na-MCI na-MCI 1
364 a-MCI a-MCI 1
879 a-MCI a-MCI 1
6
69357 na-MCI na-MCI
Left
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
1 69360 na-MCI na-MCI 1
30971 a-MCI a-MCI 1
34845 a-MCI a-MCI 1
7
69361 na-MCI na-MCI
Left
Hippocampus V
Fornix cru Stria
terminalis L DTI
1
1 69364 na-MCI na-MCI 1
60294 a-MCI a-MCI 1
69355 a-MCI a-MCI 1
8
69372 na-MCI na-MCI
Right
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
1 69403 na-MCI na-MCI 1
69359 a-MCI a-MCI 1
69367 a-MCI a-MCI 1
9
69404 na-MCI na-MCI
Left
Hippocampus V
Fornix crus Stria
terminalis L DTI
1
0.75 69412 na-MCI a-MCI 0
69371 a-MCI a-MCI 1
69376 a-MCI a-MCI 1
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
a‒MCI: amnestic mild cognitive impairment; na‒MCI: non‒amnestic mild cognitive impairment;
meanthickavg: average cortical thickness; Correct: indicator signaling correct test decision; Mean: decision
performance in each subgroup; V: volumetry based measure; DTI: DTI‒based measure

144
Table S9 Logistic regression: amnestic vs non‒amnestic MCI – volumetry with MD
Test set
no. Subject ID From: group Into: group Effect1 Effect2 Correct Mean
1
25 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
0.5 26 na-MCI na-MCI 1
49 a-MCI na-MCI 0
56 a-MCI na-MCI 0
2
36 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
1 38 na-MCI na-MCI 1
60 a-MCI a-MCI 1
67 a-MCI a-MCI 1
3
44 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
1 58 na-MCI na-MCI 1
77 a-MCI a-MCI 1
81 a-MCI a-MCI 1
4
59 na-MCI a-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
0
0.25 63 na-MCI na-MCI 1
89 a-MCI na-MCI 0
301 a-MCI na-MCI 0
5
74 na-MCI na-MCI
Left
Hippocampus V
Fornix column &
body of fornix DTI
1
0.5 216 na-MCI a-MCI 0
364 a-MCI a-MCI 1
879 a-MCI na-MCI 0
6
69357 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
0.75 69360 na-MCI a-MCI 0
30971 a-MCI a-MCI 1
34845 a-MCI a-MCI 1
7
69361 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
1 69364 na-MCI na-MCI 1
60294 a-MCI a-MCI 1
69355 a-MCI a-MCI 1
8
69372 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
1 69403 na-MCI na-MCI 1
69359 a-MCI a-MCI 1
69367 a-MCI a-MCI 1
9
69404 na-MCI na-MCI
Left
Hippocampus V
Body of corpus
callosum DTI
1
0.75 69412 na-MCI a-MCI 0
69371 a-MCI a-MCI 1
69376 a-MCI a-MCI 1
Test set no.: number of the test subset. Each test subset consisted of 4 subjects (2 from each group, apart
from the 10th, which contained the last 2 controls), the remaining 35 (37) were used as training data. Subject
ID: subject identifiers used in the study, Form: group: subject category, as determined by the Petersen
criteria (‘truth’); Into: group: subject category determined by the models (‘test decision’); Effect1:
volumetric, cortical thickness, or DTI measurements deemed meaningful in the stepwise logistic regression;
a‒MCI: amnestic mild cognitive impairment; na‒MCI: non‒amnestic mild cognitive impairment;
meanthickavg: average cortical thickness; Correct: indicator signaling correct test decision; Mean: decision
performance in each subgroup; V: volumetry based measure; DTI: DTI‒based measure

145
Table S10: Patient details, description of the separate malformations, and comparative evaluation of the results
Code Sex Age Location Neuroradiology assessment MAP07 Raw D2 images Thresholded and clustered D2
P01 m 14
Right superior temporal
gyrus
Presumed FCD or PMG; subsequent
histology ruled out tumor or dysgenesis
Positive in a small cluster Clear positivity with high distance
values Positive
Right amygdala, uncus, and hippocampus
More voluminous on T1w, with
higher intensity on FLAIR images;
presumable hippocampal sclerosis
The surrounding WM is marked positive
High D2 values in the hippocampus,
reaching significance in the medial
aspect
Positive on the medial aspect
Right insula
Thicker, but iso-intense GM on T1w
and FLAIR images, MCD can not
be ruled out
Small positive cluster in the
vicinity of signal
disturbances
Large area of positivity with several
medium-sized clusters of significant
distance values
Positive
Fronto-basal regions,
occipital and left temporal
lobes, and the cerebellum
No sign of abnormalities
Several, pronounced
positivities distant to the
above-listed lesions
Clusters of probable artefacts; neuroradiologically confirmed MCDs
are distinguishable by a halo of voxels
with higher yet non-significant D2 that surrounds the significant regions
Large fronto-basal, cerebellar, and occipital artefacts, with smaller clusters
in the left temporal lobe contralateral to
the neuroradiologically confirmed pathologies on the right side
P02 f 14
Left and right cella media of
the lateral ventricle and the
border of the right occipital WM
Small lesions on the ventricular wall
consistent with subependymal
heterotopia
Negative
High, albeit not significant D2 values in
the WM surrounding the MCDs in the
ventricular walls
The paraventricular MCDs are positive
with clusters smaller than the lesions
Bilateral frontal WM
Bilateral frontal WM signal
alterations with presumably ischemic origin
Positive Large positivities in the frontal WM and
in the corpus callosum
Large positive clusters consistent with the bilateral frontal ischemic WM-
lesions and a cluster in the corpus
callosum
Terminal WM Possibly due to incomplete
myelination (age difference between
patient and controls)
Positive High D2 values in the terminal WM, significant regions surrounded by non
significant voxels
Several medium-sized positive clusters
in the terminal WM

146
Table S10 (Continued)
Code Sex Age Location Neuroradiology assessment MAP07 Raw D2 images Thresholded and clustered D2
P03 m 16
Right parieto-occipital sulcus
Stable FLAIR signal intensity
alterations on multiple follow-ups in the right parieto-occipital sulcus
consistent with cortical dysgenesis
Negative
Positive voxels clustered around the
neuroradiologically confirmed MCD, a halo of voxels with higher yet non-significant D2 surrounds the
significant regions
The location of the MCD is pointed out by
small clusters of significant D2 in the
adjacent WM
Right occipital and bilateral frontal regions,
right superior temporal
WM
No sign of abnormalities Several positive clusters
Clusters with high D2 values in the right occipital, and bilateral frontal regions representing obvious
registration artefacts; a positive region in the right
superior temporal WM contralateral to the neuroradiologically confirmed lesion; clusters with
higher D2 values in the genu and splenium of the
corpus callosum
There are significant voxels in the regions
observed on the raw D2 map in a distribution consistent with registration artifacts
P04 f 17 Right temporo-occipital
region
Clearly visualized FCD,
(presumably type IIB) on T1w and FLAIR images
Positive
Region of voxels with high, but non-significant D2 values around the MCD, with several voxels above the
FDR-corrected threshold of significance, but only two
voxels surviving FWE correction
Negative with FWE, but positive with FDR-
correction
P05_S1
m
16
Left amygdala, uncus, and hippocampus
Histology confirmed focal gliosis. The increasing involvement of the
contralateral structures in the subsequent examinations (2, and 6
years later) may be resulting from
damaged WM caused by the seizures originating from the left
hemisphere, propagating through
the interconnecting fibers.
Positive
Raw D2 values increased with time demonstrating
expanding involvement of the left and right amygdala,
uncus and hippocampus.
Clear positive results, subsequent examinations showed contralateral regions
of abnormal diffusion; results of the last
examination seemed to be more localized, with smaller clusters than previously
P05_S2 18
Positive, right side
shows higher D2 values
than on previous examinations
P05_S3 22
Positive in the left focal
gliosis, but there are
positive clusters in the
contralateral side

147
Table S10 (Continued)
Code Sex Age Location Neuroradiology assessment MAP07 Raw D2 images Thresholded and clustered D2
P06 f 8 Right medio-frontal part
of the cingulate gyrus
Apparent Cortical dysplasia and
mild WM glial surplus; bilateral frontal-medial cortical disgenesis
with right hemisphere
predominance, presumably polymicrogyria
The neuroradiologically confirmed lesion is
clearly positive
alongside several other clusters including fronto-
basal areas and the genu
of corpus callosum
Most of the neuroradiologically confirmed lesion site
clearly shows high D2 values just below the threshold
of significance (D2≈20), there are several clusters with high D2 including fronto-basal areas and the genu of
corpus callosum
Only the posterior right frontal-cingular part
of the neuroradiologically confirmed lesion
is significant; there are several small clusters in the bilateral frontal WM and the genu of
the corpus callosum
P07 f 15
Left temporo-basal
Confirmed DNT in the left
temporo-basal region. A subsequent lesionectomy was incomplete and
did not affect the hippocampus,
seizure-freedom was not achieved Widespread positive
clusters throughout the
brain, with the left
hippocampus and left Heschl's gyrus also
marked positive
Large clusters of high D2-values in the left temporo-basal region and the left temporal pole, most
pronounced around the neuroradiologically confirmed
lesions
Clear positive result in the left temporo-basal areas, with several positive clusters in
the left temporal lobe
Left hippocampus Apparent hippocampal sclerosis,
dysgenesis cannot be ruled out The left hippocampus is evidently marked
Heschl's gyrus Questionable signal alteration that
proved to be negative on
subsequent examinations
Left superior temporal gyrus and the Heschl's gyrus are
marked by high D^2 values
One significant cluster is observed in the left
Heschl's gyrus
P08 m 46
Left amygdala and hippocampus
Dysgenesis, and partial hippocampal sclerosis
Surrounding tissue around the left
hippocampus is marked positive, along with most
of the temporal and
occipital WM-GM boundary, the right
cingulum, the right
occipital WM, and the
left occipital pole
Both hippocampi (with evident left predominance) are positive
The head of the left hippocampus and a smaller part of the right is positive
Posterior-superior part of
the Sylvian fissure
Most likely pulsation artefact
resulting from anatomical variation of arteries in the vicinity
Small cluster is observed with high D2 values One small cluster of high D2 values above
the threshold of significance
Occipital WM No clear sign of abnormalities Several regions of high D2-values Several small-medium sized clusters in the
occipital WM
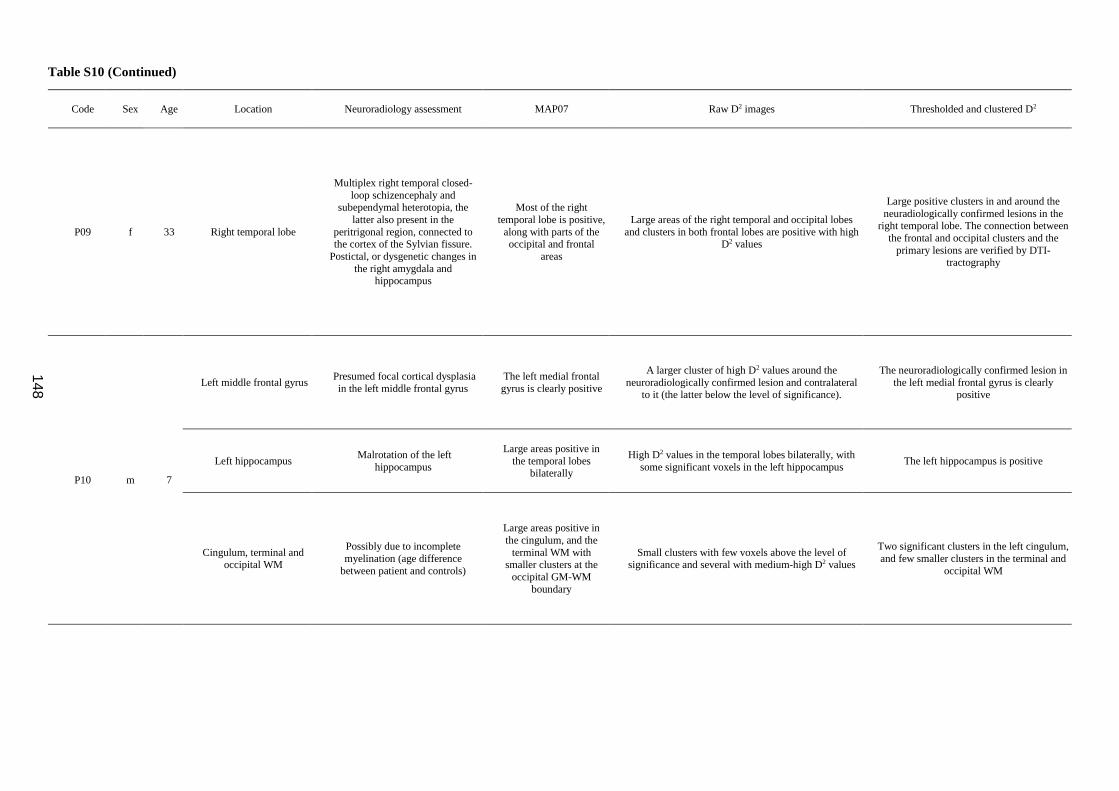
148
Table S10 (Continued)
Code Sex Age Location Neuroradiology assessment MAP07 Raw D2 images Thresholded and clustered D2
P09 f 33 Right temporal lobe
Multiplex right temporal closed-
loop schizencephaly and subependymal heterotopia, the
latter also present in the
peritrigonal region, connected to the cortex of the Sylvian fissure.
Postictal, or dysgenetic changes in
the right amygdala and hippocampus
Most of the right
temporal lobe is positive,
along with parts of the occipital and frontal
areas
Large areas of the right temporal and occipital lobes
and clusters in both frontal lobes are positive with high D2 values
Large positive clusters in and around the
neuradiologically confirmed lesions in the right temporal lobe. The connection between
the frontal and occipital clusters and the
primary lesions are verified by DTI-tractography
P10 m 7
Left middle frontal gyrus Presumed focal cortical dysplasia
in the left middle frontal gyrus
The left medial frontal
gyrus is clearly positive
A larger cluster of high D2 values around the
neuroradiologically confirmed lesion and contralateral to it (the latter below the level of significance).
The neuroradiologically confirmed lesion in
the left medial frontal gyrus is clearly positive
Left hippocampus Malrotation of the left
hippocampus
Large areas positive in
the temporal lobes bilaterally
High D2 values in the temporal lobes bilaterally, with
some significant voxels in the left hippocampus The left hippocampus is positive
Cingulum, terminal and occipital WM
Possibly due to incomplete
myelination (age difference
between patient and controls)
Large areas positive in
the cingulum, and the
terminal WM with smaller clusters at the
occipital GM-WM
boundary
Small clusters with few voxels above the level of significance and several with medium-high D2 values
Two significant clusters in the left cingulum,
and few smaller clusters in the terminal and
occipital WM

149
Table S10 (Continued)
Code Sex Age Location Neuroradiology assessment MAP07 Raw D2 images Thresholded and clustered D2
P11_S1 m 27
Basal region of the left
inferior frontal gyrus and
the posterior third of the left insula
Malformation of cortical development, presumably
polymicrogyria or FCD
Positive Medium-sized area with high D2 values in and around
the neuroradiologically confirmed lesion Positive
Left frontal, bilateral
occipital and temporal WM
No clear sign of abnormalities
Positivities in parts of
the left frontal, and bilateral temporal and
occipital lobes and in
most of the corona
radiata bilaterally
Several high D2 clusters, with some voxels above the
significance threshold
Clusters in the left frontal, the bilateral
occipital, and the left terminal WM, the latter is evidently connected to the primary
lesion, verified by DTI tractography.
Occipital registration artefacts are easy to
identify by their configuration
P11_S2 m 27
Basal region of the left
inferior frontal gyrus and
the posterior third of the
left insula
Malformation of cortical development, presumably
polymicrogyria or FCD
Positive Medium-sized area with high D2 values in and around
the neuroradiologically confirmed lesion Positive
Left frontal, bilateral
occipital and temporal
WM
No clear sign of abnormalities
Positivities in parts of
the left frontal, and
bilateral temporal and occipital lobes and in
most of the corona
radiata bilaterally
Several high D2 clusters, with some voxels above the
significance threshold. The right insula, contralateral to the neuroradiologically confirmed lesion contains
higher D2 values in a larger volume than previously
Most WM clusters further apart from the
neuroradiologically confirmed lesion are
still present. Fewer artefacts than previously

150
Table S10 (Continued)
Code Sex Age Location Neuroradiology assessment MAP07 Raw D2 images Thresholded and clustered D2
P12 m 14
Left hippocampus Left hippocampal sclerosis Negative Significantly high D2 values in the left hippocampus,
with high values in the surrounding WM Positive
Left temporal pole
Malformation of cortical
development (FCD-IIIa) in the left
temporal pole
Most of the left temporal lobe is marked positive
High D2 values in the WM of the left temporal pole, most voxels below the threshold of significance
One small positive cluster in the WM close to the left temporal pole
Right temporal pole Gliotic cyst with approx. 2mm size
in the right temporal pole
Most of the right
temporal lobe is marked
positive
Significantly high D2 values in the volume of the cyst, high D2 values in the surrounding tissue
Positive
WM in the posterior part
of the left and right superior frontal gyri
WM FLAIR signal alterations in
the right superior frontal gyrus
Clusters in the superior corona radiata are
marked positive
bilaterally
High D2 values in the superior frontal WM of both
hemispheres with right predominance
One cluster in either hemispheres in the
posterior parts of the superior frontal gyri
P13 m 35
Right temporal lobe
Right temporal closed-loop
schizencephaly and subependymal
heterotopia
Most of the temporal lobes and the superior
corona radiata are
marked positive bilaterally
The right temporal lobe contains the most voxels with
high D2-values clearly centered around the
neuroradiologically confirmed lesion
Large significant clusters in the right
temporal lobe and the hippocampus clearly
mark the pathology
Right occipital pole
Several WM signal alterations in
the occipital poles bilaterally with
right predominance. May be due to
circulatory disturbance(s) during
the 2nd trimester (the same cause may be behind the schizencephaly,
as well).
Positive, but with
smaller clusters and
weaker effect size
Frontal and occipital lobes contain regions of high D2 values bilaterally with right predominance
Several small clusters in the occipital lobes bilaterally with right predominance
Frontal lobes bilaterally
and the anterior part of
the right internal capsule
No clear sign of abnormalities
The frontal WM is
marked positive
bilaterally
Small clusters of higher D2-values with a few voxels above the level of significance
Few clusters in the frontal lobes and one in the anterior part of the right internal capsule
Results of independent lesion detection (MAP07) and the proposed Mahalanobis-distance based method were evaluated with the expert neuroradiologist (PB); apart from three cases, the
diagnoses of MCD subtypes were based on imaging.





























