Embed Size (px)
DESCRIPTION
Differential Diagnosis. Presented by M.A. Kaeser, DC Winter 2010. Introduction. Patients seek physician services for 2 reasons To establish the correct diagnosis To obtain the appropriate intervention, including prevention - PowerPoint PPT Presentation
Citation preview

Differential DiagnosisDifferential Diagnosis
Presented by M.A. Kaeser, DCPresented by M.A. Kaeser, DCWinter 2010Winter 2010

IntroductionIntroduction Patients seek physician services for 2 Patients seek physician services for 2
reasonsreasons• To establish the correct diagnosisTo establish the correct diagnosis• To obtain the appropriate intervention, To obtain the appropriate intervention,
including preventionincluding prevention Treatment provided for an incorrect Treatment provided for an incorrect
diagnosis fails the patient to the diagnosis fails the patient to the same degree as does diagnosis w/o same degree as does diagnosis w/o appropriate treatmentappropriate treatment

Process of Differential DiagnosisProcess of Differential Diagnosis Diagnosis is obtained after considering a Diagnosis is obtained after considering a
number of competitive etiologies and number of competitive etiologies and progressively eliminating themprogressively eliminating them
Rational and intuitive skillsRational and intuitive skills The essence of cost-effective health careThe essence of cost-effective health care An orderly approach is necessaryAn orderly approach is necessary
• Data acquisition, analysis with ranking of Data acquisition, analysis with ranking of positive findings, construction of the diff dx, positive findings, construction of the diff dx, narrowing of diff dx by testing strategynarrowing of diff dx by testing strategy
After diagnosis, therapeutic intervention is After diagnosis, therapeutic intervention is designed and implementeddesigned and implemented

Acquisition of DataAcquisition of Data History and physical exam are the most History and physical exam are the most
essential components of the diff dx essential components of the diff dx processprocess• Achieved by intuition and sensory inputAchieved by intuition and sensory input• Verbal and nonverbal clues help formulate the Verbal and nonverbal clues help formulate the
tentative diagnostic impressionstentative diagnostic impressions Nonverbal example: oversized clothing from weight Nonverbal example: oversized clothing from weight
lossloss All diagnostic decisions are dependent All diagnostic decisions are dependent
upon reliable dataupon reliable data

Acquisition of Data: Chief Acquisition of Data: Chief ComplaintComplaint
Explore thoroughlyExplore thoroughly Patient should review all relevant symptomsPatient should review all relevant symptoms Interview reveals the patient’s level of expression Interview reveals the patient’s level of expression
and personalityand personality Pitfalls in the interview processPitfalls in the interview process
• Cultural influences, attitudes, fears, ignorance and Cultural influences, attitudes, fears, ignorance and memory loss altering the reliability of the historianmemory loss altering the reliability of the historian
Ask branching questionsAsk branching questions• Intention is to amplify and distill various diagnostic Intention is to amplify and distill various diagnostic
hypotheses or “hunches”hypotheses or “hunches” Past medical, family and social history may reveal Past medical, family and social history may reveal
cluesclues ROS provides informationROS provides information

Acquisition of Data: Physical Acquisition of Data: Physical ExaminationExamination
Concentrates on region of the chief complaint and Concentrates on region of the chief complaint and any associated findingsany associated findings
General survey physical examination is importantGeneral survey physical examination is important Vital signs – one of the most cost-effective tests Vital signs – one of the most cost-effective tests
• Elevated temperature with back pain may indicate Elevated temperature with back pain may indicate pyelonephritispyelonephritis
Abnormal findings must be independent of their Abnormal findings must be independent of their specific anatomic location, and separate from the specific anatomic location, and separate from the designation or diagnosisdesignation or diagnosis
Physical examination answers the question, “How Physical examination answers the question, “How sick or abnormal is this patient?”sick or abnormal is this patient?”

Acquisition of Data: Abnormal Acquisition of Data: Abnormal FindingFinding
Often will trigger additional physical Often will trigger additional physical assessmentsassessments• Ex. T/S scoliosis in a very tall person may Ex. T/S scoliosis in a very tall person may
prompt a cardiac evaluation to exclude prompt a cardiac evaluation to exclude Marfan’sMarfan’s
Patient’s examination should be Patient’s examination should be considered ongoingconsidered ongoing
Subsequent visits should allow for a brief Subsequent visits should allow for a brief review of the positive findings and review of the positive findings and identification of new findings or identification of new findings or complicationscomplications

Analysis and Ranking of Positive Analysis and Ranking of Positive FindingsFindings
Pertinent findings are listed in the order of Pertinent findings are listed in the order of apparent relevanceapparent relevance
This is point where diagnostic accuracy is This is point where diagnostic accuracy is compromisedcompromised• Improper significance results in either too much, or too Improper significance results in either too much, or too
little, consideration for a given findinglittle, consideration for a given finding Time and natural course of a disease may alter Time and natural course of a disease may alter
the frequency and significance of a given findingthe frequency and significance of a given finding Primary or key findings demonstrate high Primary or key findings demonstrate high
sensitivity or specificitysensitivity or specificity• Ex. Weakness in all extremities or quadriparesis Ex. Weakness in all extremities or quadriparesis
suggests a stenosis of the spinal cord. Constipation or suggests a stenosis of the spinal cord. Constipation or vertigo are nonspecificvertigo are nonspecific

Analysis and Ranking of Positive Analysis and Ranking of Positive Findings: Common ErrorsFindings: Common Errors
Arise when insufficient data are available Arise when insufficient data are available as a result of careless interview or as a result of careless interview or examination techniques (or the physician’s examination techniques (or the physician’s knowledge is inadequate or lacks knowledge is inadequate or lacks interpretive experience)interpretive experience)
Last case bias – influences clinical Last case bias – influences clinical reasoning due to recent diagnosis reasoning due to recent diagnosis
Avoid the tendency to force congruence Avoid the tendency to force congruence with a diagnostic classificationwith a diagnostic classification

System AssignmentSystem Assignment Positive findings should be assigned to one or Positive findings should be assigned to one or
more of the physiological systemsmore of the physiological systems Acute or chronic ambulatory pain syndromes Acute or chronic ambulatory pain syndromes
arise in association with MSK and neurological arise in association with MSK and neurological systemssystems• Radiculopathy, myelopathy, weakness, muscle atrophy Radiculopathy, myelopathy, weakness, muscle atrophy
and spinal segmental fixationand spinal segmental fixation GU systemGU system
• M/C extraspinal source of referred pain to the lower T/S M/C extraspinal source of referred pain to the lower T/S and L/Sand L/S
Other systemsOther systems• Endocrine, cardiovascular, respiratory, GI and Endocrine, cardiovascular, respiratory, GI and
dermatologicaldermatological

Differential CategoriesDifferential Categories May be variable and arbitraryMay be variable and arbitrary Categories include:Categories include:
• NeoplasmNeoplasm• InfectionInfection• VascularVascular• TraumaTrauma• ArthritideArthritide• EndocrineEndocrine• CongenitalCongenital

NeoplasmNeoplasm Most life-threatening Most life-threatening Malignant neoplasms of the primary or Malignant neoplasms of the primary or
metastatic variety must be suspected in metastatic variety must be suspected in any adult patient presenting with any adult patient presenting with progressive spinal or pelvic painprogressive spinal or pelvic pain
Average delay in the diagnosis of skeletal Average delay in the diagnosis of skeletal metastasis is 10 monthsmetastasis is 10 months
Suspicious findingsSuspicious findings• Intractable skeletal pain or pain persisting day Intractable skeletal pain or pain persisting day
and night for a duration exceeding 5 daysand night for a duration exceeding 5 days

Neoplasm: Clues with Important Neoplasm: Clues with Important ValueValue
Physical findings of weakness, unexplained fever, Physical findings of weakness, unexplained fever, lymphadenopathy, organomegaly, or any lymphadenopathy, organomegaly, or any progressive sensory or motor deficitprogressive sensory or motor deficit
Lab findingsLab findings• Microcytic or macrocytic anemia, elevated Microcytic or macrocytic anemia, elevated
sedimentation rate (ESR), hypercalcemia, elevated sedimentation rate (ESR), hypercalcemia, elevated alkaline or acid phosphatase, proteinuria, and alkaline or acid phosphatase, proteinuria, and monoclonal gammopathy are associated with skeletal monoclonal gammopathy are associated with skeletal malignancymalignancy
Negative lab tests and radiographs Negative lab tests and radiographs nevernever exclude exclude the possibility of skeletal malignancythe possibility of skeletal malignancy
Poor sensitivity of radiography limits its role in Poor sensitivity of radiography limits its role in the early diagnosis of skeletal malignancythe early diagnosis of skeletal malignancy

InfectionInfection Can mimic disorders of almost any Can mimic disorders of almost any
etiologyetiology Cardinal clinical manifestationsCardinal clinical manifestations
• Acute onset of fever, chills, adenopathy, Acute onset of fever, chills, adenopathy, malaise and myalgiamalaise and myalgia
Joint infections in the appendicular Joint infections in the appendicular skeletonskeleton• Closed posttraumatic effusion that is warmClosed posttraumatic effusion that is warm
Spinal infections (discitis)Spinal infections (discitis)• Considered when spinal or pelvic surgery is Considered when spinal or pelvic surgery is
antecedent to progressive spinal pain and antecedent to progressive spinal pain and febrile patientfebrile patient

Infection: Constitutional SignsInfection: Constitutional Signs AnorexiaAnorexia Weight loss Weight loss MalaiseMalaise IV drug abusers and IV drug abusers and
immunocompromised patients are immunocompromised patients are prone to bone and joint infectionsprone to bone and joint infections
Lab findingsLab findings• Elevated WBC and ESRElevated WBC and ESR

VascularVascular Often overlooked when acute pain evolves over hours or days Often overlooked when acute pain evolves over hours or days
following an abrupt onsetfollowing an abrupt onset Headaches – esp. occipital, which are sudden and severe in the Headaches – esp. occipital, which are sudden and severe in the
presence of altered consciousness or neurological deficits, herald presence of altered consciousness or neurological deficits, herald a TIA or strokea TIA or stroke
Thromboemboli in the pulmonary or coronary circulation give rise Thromboemboli in the pulmonary or coronary circulation give rise to progressive chest pain, tachypnea, tachycardia or SOBto progressive chest pain, tachypnea, tachycardia or SOB• Often seen in legOften seen in leg
Aneurysms of the abdominal aorta can erode the vertebral body Aneurysms of the abdominal aorta can erode the vertebral body giving rise to paingiving rise to pain
Peripheral occlusive vascular disease Peripheral occlusive vascular disease • Considered when signs of claudication are notedConsidered when signs of claudication are noted
Unilateral edemaUnilateral edema• In either extremity warrants consideration of vascular or lymphatic In either extremity warrants consideration of vascular or lymphatic
compressioncompression Bilateral lower extremity edema is a sign of congestive failureBilateral lower extremity edema is a sign of congestive failure

TraumaTrauma Frequent source of ambulatory pain syndromesFrequent source of ambulatory pain syndromes Often arises from vehicular or work-place accidents or from sports Often arises from vehicular or work-place accidents or from sports
endeavorsendeavors Ligamentous injury in the C/S must be carefully soughtLigamentous injury in the C/S must be carefully sought Atlantoaxial instability can be excluded by flexion –extension x-Atlantoaxial instability can be excluded by flexion –extension x-
raysrays Occult fractures in the neural arches of the mid and lower C/S Occult fractures in the neural arches of the mid and lower C/S
should be considered if severe posttraumatic cervical spine pain should be considered if severe posttraumatic cervical spine pain persists beyond 7 to 10 dayspersists beyond 7 to 10 days
Stress fracturesStress fractures• Skeletal pain provoked by activity and relieved by restSkeletal pain provoked by activity and relieved by rest
Fractures Fractures • Accompanied by history of trauma and pain with the exception of Accompanied by history of trauma and pain with the exception of
neurogenic arthropathy (minimally painful, if at all)neurogenic arthropathy (minimally painful, if at all) Pathological fracturesPathological fractures
• Usually suspected after radiological evaluation reveals features of bone Usually suspected after radiological evaluation reveals features of bone destruction and/or soft-tissue massesdestruction and/or soft-tissue masses

ArthritideArthritide Source of most patient diagnoses Source of most patient diagnoses
presenting with a pain syndromepresenting with a pain syndrome Macrotrauma is often precipitating Macrotrauma is often precipitating
event of degenerative arthrosesevent of degenerative arthroses May be precipitated by aggregate May be precipitated by aggregate
microtrauma from inefficient postural microtrauma from inefficient postural controls or work-place stressescontrols or work-place stresses
Hallmark of a degenerative arthritideHallmark of a degenerative arthritide• Reproducible joint-based painReproducible joint-based pain

Arthritides: Common Arthritides: Common ComplicationsComplications
Vertebral columnVertebral column• Disc degeneration and herniation, Disc degeneration and herniation,
segmental instability and spinal stenosissegmental instability and spinal stenosis Signs: altered joint mobility, radiculopathy, Signs: altered joint mobility, radiculopathy,
referred pain, reflex sympathetic dystrophy, referred pain, reflex sympathetic dystrophy, atrophy, spasticity, weakness or claudicationatrophy, spasticity, weakness or claudication
Myofascial trigger points are often Myofascial trigger points are often located in neurofacilitated segments located in neurofacilitated segments

Arthritides: InflammatoryArthritides: Inflammatory RARA ASAS Characterized by a history of pain in Characterized by a history of pain in
multiple bilateral joints multiple bilateral joints • Morning stiffnessMorning stiffness• SwellingSwelling

Arthritides: MetabolicArthritides: Metabolic GoutGout Pseudo-goutPseudo-gout Require laboratory diagnosis and Require laboratory diagnosis and
joint aspiration for confirmationjoint aspiration for confirmation

EndocrineEndocrine Also includes metabolic and nutritional Also includes metabolic and nutritional
disordersdisorders One of the most challenging diagnostic One of the most challenging diagnostic
categories to evaluatecategories to evaluate• Endocrine glands and metabolism govern Endocrine glands and metabolism govern
physiological activities throughout the bodyphysiological activities throughout the body Inspection often raises the question of an Inspection often raises the question of an
endocrine-metabolic disorderendocrine-metabolic disorder Usually arise due to excess or deficiency Usually arise due to excess or deficiency
of hormone secretionof hormone secretion Target receptor responsiveness may be Target receptor responsiveness may be
absent or elevated absent or elevated

Endocrine: Common Endocrine: Common EndocrinopathiesEndocrinopathies
ManifestationsManifestations• Weakness, easy fatigability, growth abnormalities, Weakness, easy fatigability, growth abnormalities,
hirsutism, weight loss or obesity and altered hirsutism, weight loss or obesity and altered reproductive function (impotence, irregular menstrual reproductive function (impotence, irregular menstrual cycles)cycles)
DisordersDisorders• Osteoporosis (m/c cause of spinal pain of metabolic Osteoporosis (m/c cause of spinal pain of metabolic
origin)origin)• Diabetes mellitusDiabetes mellitus• Hyper- and hypothyroidismHyper- and hypothyroidism• HypoglycemiaHypoglycemia
Definitive diagnosisDefinitive diagnosis• Lab testsLab tests
Specific hormone levelsSpecific hormone levels• Advanced imagingAdvanced imaging

CongenitalCongenital Also grouped with dysplasias and genetic Also grouped with dysplasias and genetic
disordersdisorders Short stature of dwarfismShort stature of dwarfism Spider-like hands and feet of Marfan’sSpider-like hands and feet of Marfan’s History of recurrent fractures in OIHistory of recurrent fractures in OI Most significant congenital spinal anomaly Most significant congenital spinal anomaly
is an unstable os odontoidiumis an unstable os odontoidium• Diagnosed by flexion/extension radiographsDiagnosed by flexion/extension radiographs

Differential DiagnosisDifferential Diagnosis Constructed in order of declining probabilityConstructed in order of declining probability Influenced byInfluenced by
• Age, gender, race, disease prevalence, clinical featuresAge, gender, race, disease prevalence, clinical features Common sense, logic and intuition will eliminate the Common sense, logic and intuition will eliminate the
diagnostic possibilities and advace the probabilitiesdiagnostic possibilities and advace the probabilities Be specific (ex. Spinal stenosis, myofascitis of gluteus Be specific (ex. Spinal stenosis, myofascitis of gluteus
maximus)maximus) Lack of adequate findings results in a nonspecific diagnosis Lack of adequate findings results in a nonspecific diagnosis
(this is o.k. since testing strategies will help to narrow (this is o.k. since testing strategies will help to narrow diagnosis)diagnosis)
Process involves significant negative or absent findings and Process involves significant negative or absent findings and the presence of positive findingsthe presence of positive findings
Try to include treatable conditionsTry to include treatable conditions

Testing StrategyTesting Strategy Proceed with treatment versus employ testing Proceed with treatment versus employ testing
proceduresprocedures Determined by Determined by
• Level of certainty or confidenceLevel of certainty or confidence• Presence of conditions capable of inflicting significant Presence of conditions capable of inflicting significant
morbidity or mortalitymorbidity or mortality• Cost effectiveness of further testingCost effectiveness of further testing
If differential contains morbid or potentially fatal If differential contains morbid or potentially fatal condition, you must rule out or confirm their condition, you must rule out or confirm their presencepresence
Sensitive tests are able to detect a given disorderSensitive tests are able to detect a given disorder Specific tests confirm its presenceSpecific tests confirm its presence

Testing Strategy: Appropriate Test Testing Strategy: Appropriate Test SelectionSelection
Necessary for diagnostic orientation, patient Necessary for diagnostic orientation, patient safety and cost effectivenesssafety and cost effectiveness
Avoid “shot gun”, routine or battery testingAvoid “shot gun”, routine or battery testing All tests flow from the differential diagnosisAll tests flow from the differential diagnosis
• Diff dx arises from the positive findings yielded by H and Diff dx arises from the positive findings yielded by H and P examinationP examination
Many patients will have the results of treatment Many patients will have the results of treatment modify the diff dxmodify the diff dx• Treatment response is of diagnostic valueTreatment response is of diagnostic value
Results of the approriate testing strategy should Results of the approriate testing strategy should be a working diagnosis that is consistent with all be a working diagnosis that is consistent with all clinical informationclinical information

TreatmentTreatment Use of appropriate therapeutic measures Use of appropriate therapeutic measures
directed at one or more diagnosesdirected at one or more diagnoses Natural course of a disorder is known and Natural course of a disorder is known and
should be altered by appropriate should be altered by appropriate treatmenttreatment
Failure to alter the course impliesFailure to alter the course implies• Treatment is inadequateTreatment is inadequate• Other modes of treatment should be employedOther modes of treatment should be employed• The diagnosis needs revision (must be The diagnosis needs revision (must be
performed in a timely manner) – failure to performed in a timely manner) – failure to arrive at a new diagnosis requires specialty arrive at a new diagnosis requires specialty consultationconsultation

Treatment: Clinical HypesthesiaTreatment: Clinical Hypesthesia
Refers to the failure to discriminate Refers to the failure to discriminate b/t a benign etiology of pain and a b/t a benign etiology of pain and a newly superimposed life-threatening newly superimposed life-threatening source of painsource of pain
Physician is lulled into an expectation Physician is lulled into an expectation of incurable chronic painof incurable chronic pain
Periodic exams can prevent this Periodic exams can prevent this mistakemistake

Treatment: Collection and Analysis Treatment: Collection and Analysis of Clinical Informationof Clinical Information
A dynamic processA dynamic process• Begins with the patient’s introduction Begins with the patient’s introduction • Ongoing with constant revisionOngoing with constant revision
Depends on new information from the Depends on new information from the interview, physical examination, test results, interview, physical examination, test results, treatment responsetreatment response

ConclusionsConclusions Effective clinical decisions result from an Effective clinical decisions result from an
orderly and strategic reasoning methodorderly and strategic reasoning method Provides cost effective clinical Provides cost effective clinical
managementmanagement Emergence of one or two diagnoses from a Emergence of one or two diagnoses from a
dozen or more differential considerations dozen or more differential considerations can be as satisfying a feature of patient can be as satisfying a feature of patient care as a favorable response to treatmentcare as a favorable response to treatment

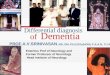
Differential Diagnosis StrategyDifferential Diagnosis Strategy
Data Acquisiton Analysis of Positive Findings Systems Assignment
Differential Category
Differential DiagnosisTesting StrategyDiagnosis
Treatment
Differential Diagnosis Strategy

ReferencesReferences Kettner, N.W. D.C. Tracts, June 1989, Kettner, N.W. D.C. Tracts, June 1989,
Vol. 1, No. 3Vol. 1, No. 3