Embed Size (px)
Citation preview
Diet, vitamin D and cognition
Dr Tom Hill and Dr Antoneta Granic
& The Newcastle 85+ Research Team
Human Nutrition Research Centre &
Institute of Health & Society
Newcastle University
AgeingGeriatricsEpidemiology

Outline
• General overview of diet and
cognition
o Recent evidence on key dietary
components
o Potential mechanisms
• Highlights of recent work from
the Newcastle 85+ study
o Dietary patterns
o Vitamin D
IHS & NUIA
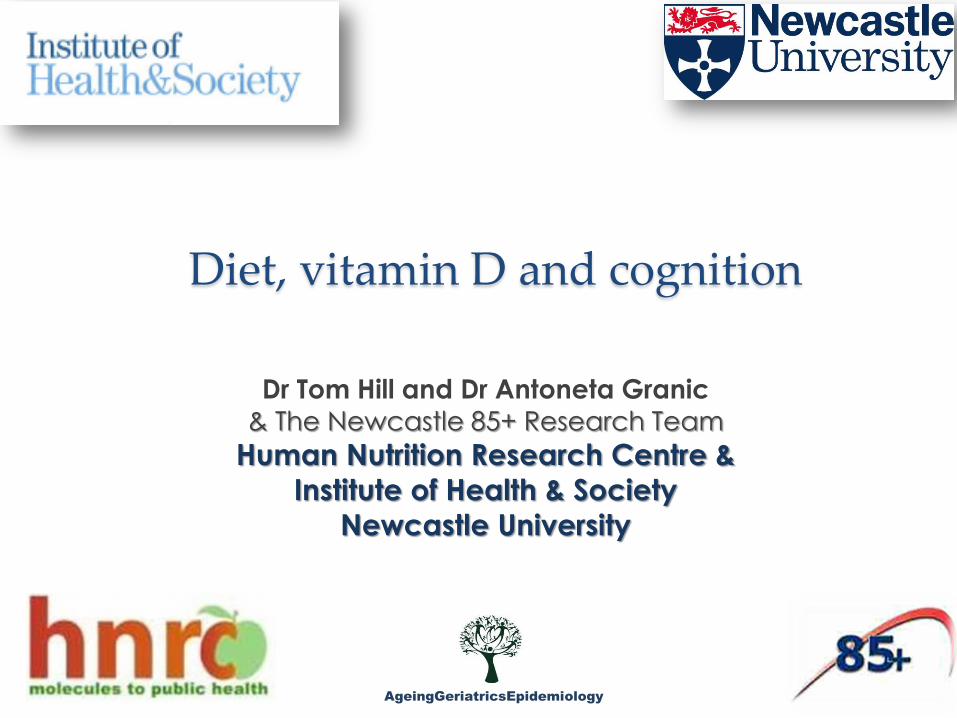
Prevalence & incidence of dementia in UK
Matthews F, Brayne C, MRC CFAS Investigators . PLoS Med 2005;2(8): e193. Matthews FE, Arthur A, Barnes LE, MRC CFA S Collaboration. Lancet 2013; 382: 1405-1412.
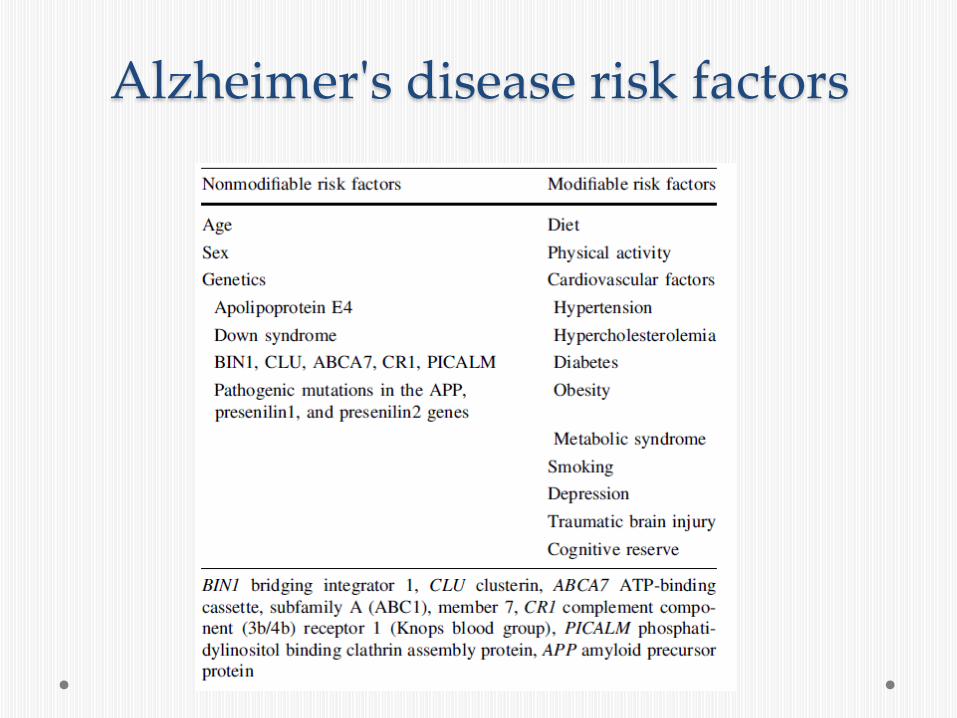
Alzheimer's disease risk factors

Candidate dietary factors which have been related to cognition throughout life
Nutrients Dietary Fats Antioxidants B vitamins Vitamin D Iodine Foods Oily fish Nuts Olive oil Vegetables Red wine Beverages (teas) Dietary patterns Mediterranean diet DASH Diet MIND diet
General mechanisms ??
Anti-inflammatory agents
Reduce oxidative
stress
Reduce homocysteine
Alter markers of insulin resistance
Others?

The evidence pyramid

Dietary fat and cognition
• Saturated fat o ApoE a gene encoding cholesterol transport is an established risk
factor for AD
o In animal models a high fat hypercholesterolaemic diet: results in various adverse brain events such as significant amyloid ß burden, phosphorylated tau protein and increased immunoreactivity
o Prospective epidemiological studies of dietary fat composition fairly consistently show increased risk of dementia and faster rate of cognitive decline with higher intake of saturated fat
• Omega-3 PUFA o Cardiovascular and cerebrovascular protection
o DHA key component of brain tissue
o Observational studies: majority show beneficial observations
o RCT data: Recent meta analysis (Mazereeuw et al. Neuro biol Ageing 2013) effect on specific cognitive domains in cognitively impaired participants but not in healthy or demented participants.

Micronutrients and cognition
• Antioxidants o The brain is a site of high metabolic activity and is particularly
susceptible to oxidative stress and damage to neural tissue o A prevailing theory is that this oxidative damage and neural
inflammation are underlying mechanisms for neurodegenerative disorders like AD and Parkinson’s disease
o Potential for an array of antioxidant nutrients and non-nutrients alike to influence mental function
• Vitamin E
o Evidence that vitamin E plays a role in the developing brain o The prospective epidemiological studies of dietary vitamin E (i.e.
from food sources) consistently show statistically significant inverse associations with incident dementia and AD and with cognitive decline
o Evidence around the beneficial effects of supplemental vitamin E intakes is conflicting which may be related to wide variation in supplemention regimens and in some cases the problem of choosing ‘fit and well participants’

Micronutrients and cognition
• Other antioxidants o Unfortunately there is weak evidence to support
protection against dementia by dietary intake other antioxidants such as vitamin C, beta-carotene and flavanoids
• B vitamins
o Mainly folate and vitamin B12 have been studied owing to their role as co-factors that are known to affect neurocognitive development and neurodegeneration
o Epidemiological studies and RCTs on the international scene for B vitamins and cognition have shown inconsistent findings that may reflect the complex interrelation between folate and vitamin B12

Methodology of Dietary Pattern analysis Basic studies: effects of isolated nutrients on
pathological mechanisms of a disease
Complexity of food intake
Epidemiological studies: association between diet and disease
A priori DP A posteriori DP
Hypothesis driven Data driven and based on diet of given population
Designed to test adherence to established guidelines or a specific diet and diet variety
Accounts for a complex correlation between foods and nutrients in the whole diet
-HEI, HDI, HDS, DQI, RFS, DGI, CHEI, PNNS-GS, HFI, DQI, etc. -MeDi, DASH
Dependent on exploratory statistical analysis: -PCA, clustering methods (k-means; TwoStep), LCA -Hybrid method and RRR
Dietary indices are constantly updated and evaluated in different populations
Limited reproducibility and comparison between studies
Do not capture the complexity of the whole diet Dependent on author’s subjective choices of food groupings, DP labelling and interpretation
Quality of DP depends on quality of data Quality of DP depends on quality of data
Adapted from Alles B et al. Nutr Res Rev 2012;25:207-22

Dietary patterns and cognitive health
Risk of cognitive decline/impairment
/dementia
a priori
a posteriori
MeDi1,2
DASH2
‘MIND’ diet4
Guidelines based on:
HEI, HDI, RFS, DGI, CHEI, PNNS-GS3
: increased risk
: decreased risk
Japanese diet5
‘Western’ DP6
‘Healthy’ diet7
‘Whole food’ diet8
‘Processed food’ diet8
[1] Scarmeas N et al. Arch Neurol 2006;63:1709-17. Feart C et al. JAMA 2009;302:638-48.
Gu Y et al. J Alz Dis 2010;22:483-92
[2] Wengreen H et al. Am J Clin Nutr 2013;98:1263-71.
Smith PJ et al. Hypertension 2010; 55:1331-38. [3] Wengreen H et al. J Nutr 2009;1944-49. Shatenstein B et al. Exp Gerontol
2012;47:353-60.
Kesse-Guyot E et al. Am J Clin Nutr 2011;93:200-10
[4] Morris MC et al 2014. Alzheimer’s Association International Conference; Abstract: O2-
02-04.
‘Prudent’ DP6
[5] Ozawa M et al. Am J Clin Nutr 2013;97:1076-82
[6] Parrott MD et al. J Nutr 2013; 143:1767-73.
Gardener SL et al. Mol Psychiatry 2014; doi:10.1038/mp.2014.79
[7] Samieri C et al. J Am Diet Assoc 2008;108:1461-71. [8] Akbaraly et al. Dement Geriatr Cogn Disord 2009;27:147-54.
Why health and ageing research in the very old?
• 85+ age group are the fastest growing segment of populations worldwide o 351% increase between 2010 and 2050 globally vs. 188% in those 65+1
• The very old have many multiple diseases and disabilities o Men aged 85 have median of 4, and women 5 diseases2 and increased
cost of care
• Difference in the relationship between risk factors and outcomes (including cognition)3 in midlife, the young old and very old o E.g. BMI and mortality; telomere length and mortality
• Knowledge about the role of vitamin D and overall diet (nutrition) as a modifiable lifestyle/risk factor in healthy ageing in 85+is limited4 o Vitamin D and nutritional recommendations based on mostly young-old5
• Research lacking in mediating effect of biomarkers of ageing and the role of dementia-related genes in the cognition-diet relationship
1. WHO Global Health and Aging (NIH Publication no. 11-7737). 2011 2. Collerton J, Davies K, Jagger C, et al. BMJ 2009; 399:b4904. 3. Molander L, Gustafson Y, Lovheim H. Dementia and Geriatric Cognitive Disorders 2010a; 29:243-9. 4. Mak TN, Caldena S. JRC Science and Policy Report : The role of nutrition in active and healthy ageing . 2014; ISSN 1831-9424. 5. EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA Journal 2013;11:3005.

Study objectives • Epidemiology and biomedical sciences support a role of vitamin D
and diet (nutrients) in cognitive functioning and decline in late life
• Research lacks in:
o numbers of the very old (those aged 85 years and over)
o measures of several cognitive domains over time
o whole diet / dietary patterns (DP) approach (‘food synergy’)
o modulating role of genetic risk factors
• Using the Newcastle 85+ Study data we sought to:
o Investigate the role of serum vitamin D in cognitive functioning over 3 years1
o derive and characterize2,3 determine the association between:
• DP and global and attention-specific cognition over 5 years
• and taking into account the APOE ε4 genotype
1. Granic et al Eur J Neurol, 2015; 22(1): 106-e7
2. Granic et al J Nutr: NUTRITION/2015/216952 (under review) 3. Granic et al PLOS ONE: PONE-D-15-12993 (under review)

The Newcastle 85+ study
• A longitudinal prospective
study of >1000 individuals
born in 1921 aimed to
o Determine the health
trajectories and bio-psycho-
social factors (including diet)
factors associated with
health maintenance in 85+
• Baseline (2006/07) and
follow-up interview at 1.5
(Phase 2), 3 years (Phase
3)and 5 years (Phase 4)

Cognitive domains of the Newcastle 85+ study
(1) Cognitive measures: global and attention-specific
Multilevel liner modelling for changes in
attention over 3yr

Cognitive functioning in NC85+
• 3% scored 10 or less
• 10% scored 11-21
• 16% scored 22-25
• 70% not impaired (26-30)
• 16% scored 30!
• A longitudinal prospective study of >1000 individuals born in 1921 aimed to
o Determine the health trajectories and bio-psycho-social factors (including diet) factors associated with health maintenance in 85+
• Baseline (2006/07) and follow-up interview at 1.5 (Phase 2), 3 years (Phase 3)and 5 years (Phase 4)

Dietary assessment 24-hr MPR method • Detailed food intake on previous day
o Average intake on two non-consecutive days (g/day)
• Multiple pass through diet data o Food type, amount (portion size), brand, cooking method, recipe,
meal occasion and time
• >2,000 unique food codes in Access data base
• 119 food groups1 (established by the HNRC, Newcastle University) o Further collapsed into 33
• Pilot study to determine whether 24-hr MPR is acceptable dietary assessment in this age group2
[1] Mc Chance & Widdowson’s Composition of Foods (Food Standard Agency, 2002)
[2]Adamson AJ, et al. Eur J Clin Nutr 2009;63:S6-S18.

Clustering analysis
Two Step clustering (SPSS)
• designed to reveal natural subgroupings (clusters) among cases or objects • Step 1: creates small pre-clusters based on log-likelihood
distance criterion
• Step 2: pre-clusters merged into dietary groups using
agglomerative hierarchical clustering method
• Groups subjects into homogenous, non-
overlapping groups
30 food groups
(absence [0] / presence [1])

Food groups by grams/day
Food group DP1 (High Meat) DP2 (Low Meat) DP3 (High Butter)
Fruits 143.95 (SE: 8.74) 199.41 (10.87) 158.03 (9.62)
Eggs 15.5 (1.79) 21.36 (1.93) 18.21 (1.8)
Fish 16.45 (2.17) 29.16 (2.78) 19.19 (2.46)
Coffee 120.42 (13.05) 206.35 (12.67) 128.18 (14.45)
Potato 117.89 (4.46) 63.71 (4.93) 107.38 (4.76)
Butter 1.16 (0.34) 5.80 (0.73) 19.98 (1.02)
Low fat dairy 81.72 (6.52) 88.55 (6.11) 54.62 (5.58)
Gravy 24.14 (2.0) 2.20 (0.75) 16.34 (1.77)
Red meats 91.94 (4.66) 58.47 (5.73) 70.16 (4.67)
Alcohol (ml) 78.90 (16.10) 103.12 (13.33) 88.19 (15.30)

DP2: Low Meat • Lowest Highest

DP differed by sociodemographic factors
Characteristic DP1: High Red Meat (n=276)
DP2: Low Meat (n=260)
DP3: High Butter (n=255)
p
Sociodemographic factors %
Marital status Not married Married
66.9 33.1
76.0 23.9
65.5 34.5
0.02
Type of home Rented Owned/mortgaged Live in institutions
35.9 50.7 13.4
29.5 68.1 1.9
36.9 52.2 11.0
<0.001
Education (yr) low (0-9) middle (10-11) high (≥12)
74.6 19.1 6.3
51.9 25.2 22.9
65.3 26.3 8.4
<0.001
Social class % low (manual) middle (intermediate) high (managerial)
58.1 14.2 27.7
39.4 15.0 45.7
56.1 14.2 29.7
<0.001
Area deprivation index % low (poor) middle high (affluent)
28.6 48.9 22.5
16.5 51.5 31.9
27.5 50.2 22.4
0.003
Χ2
test
; K
rusk
al-W
alli
s

DP differed on cognitive measures Characteristic DP1:
High Red Meat & Low Butter (n=276)
DP2: Low Meat & Potato (n=260)
DP3: High Butter (n=255)
p
Cognitive measures (raw scores; M, SD)
SMMSE points baseline 3-yr follow-up 5-yr follow-up
25.4 (5.7) 25.1 (5.6) 25.0 (6.0)
27.3 (3.3) 26.2 (4.8) 26.2 (5.2)
25.6 (5.4) 25.1 (5.6) 23.3 (7.6)
<0.001 0.05 0.006
SRT (ms) baseline 1.5-yr follow-up 3-yr follow-up
509.8 (516.5) 515.5 (377.8) 499.5 (312.0)
417.9 (149.3) 431.4 (137.7) 458.4 (252.7)
492.8 (665.1) 521.0 (355.9) 473.3 (183.8)
0.01 0.02
PoA (ms) baseline 1.5-yr follow-up 3-yr follow-up
1683.0 (759.2) 1729.6 (682.1) 1713.1 (674.1)
1541.0 (383.1) 1566.7 (285.9) 1666.7 (711.5)
1614.3 (568.7) 1758.3 (717.2) 1690.4 (451.9)
0.03 0.04
Χ2
test
; K
rusk
al-W
alli
s

Change in global cognition* by DP
Effects (β [SE]) Entire cohort p** Men p Women p
Time 0.12 (0.03) <0.001 0.09 (0.04) 0.04 0.13 (0.04) <0.001
Dietary pattern (DP) High Red Meat Low Meat (ref) High Butter
0.07 (0.037) 0 0.03 (0.04)
0.08 0.5
0.13 (0.06) 0 0.01 (0.06)
0.02 0.8
-0.01(0.05) 0 0.02 (0.04)
0.9 0.6
Slope DP x Time Red Meat x Time Low Meat x Time High Butter x Time
-0.02 (0.04) 0 0.01 (0.04)
0.6 0.9
-0.01 (0.06) 0 0.02 (0.07)
0.9 0.8
-0.03 (0.05) 0 -0.01(0.05)
0.5 0.9
*negative skew corrected as NEWX=log10(30.5-X); **Multilevel linear modeling Fully adjusted model included liner (Time) trend of time, random slopes and intercept, sociodemographic, lifestyle and health-related variables, APOE ε4 and interaction terms (DP x Time). Additionally adjusting for sex-specific quartile of total energy and supplement use did not change the outcomes.
Coefficients increased – poorer performance on SMMSE or cognitive decline.
Slopes (rate of change) did not vary by DP between individuals.

Change in attention tasks Outcome Dietary pattern Unadjusted
β (SE) p Adjusted*
β (SE)
p
SRT High Red Meat Low Meat (ref) High Butter
0.05 (0.01) 0 0.03 (0.03)
<0.001 0.003
0.04 (0.01) 0 0.03 (0.01)
0.002 0.02
CRT High Red Meat Low Meat (ref) High Butter
0.03 (0.01) 0 0.03 (0.009)
0.003 0.003
0.01 (0.01) 0 0.03 (0.01)
0.21 0.009
PoA High Red Meat Low Meat (ref) High Butter
0.03 (0.01) 0 0.02 (0.01)
<0.001 <0.001
0.02 (0.01) 0 0.02 (0.01)
0.014 0.03
RTV High Red Meat Low Meat (ref) High Butter
0.03 (0.01) 0 0.02 (0.01)
0.005 0.03
0.01 (0.01) 0 0.02 (0.01)
0.04 0.15
CoA High Red Meat Low Meat (ref) High Butter
0.37 (0.092) 0 0.16 (0.09)
0.05 0.001
0.19 (0.10) 0 0.0004 (0.10)
0.07 0.1
*Includes DP, linear trend of time, DP*time interaction, sociodemographic and lifestyle,
health-related variables, and APOE ε4 genotype.
Coefficients increased – longer time taken to complete the task.
Slopes (rate of change) did not vary by DP between individuals.

Summary • O1: We derived and characterized three distinct DP:
o DP1 (‘High Red Meat’)
o DP2 (‘Low Meat’)
o DP3 (‘High Butter’)
• DP varied by: o sociodemographic, lifestyle, and health variables
o ‘Low Meat ’ more advantaged (all SES measures)
o healthier
o maintained the highest average SMMSE scores over 5 years
• O2: ‘High Red Meat’ and ‘High Butter’ DP associated with: o increased risk of cognitive decline at 5-yr follow-up and worse
overall attention-specific cognition after adjusting for confounders
• Similar rate of change over time across DP for all cognitive measures

Vitamin D is a neurosteroid
Neurons Glial cells
VD
R
1α
-OH
Eyles et al 2005. Journal of Chemical Neuroanatomy, 29:21-30
• Both VDR and 1 α-OH are expressed in human brain • Calcitriol involved in neuroprotection & neurotrophic signalling & regulation of neurotransmitters • Acts as immunomodulating, anti-oxidative, anti- inflammatory agent • Regulates genes and
proteins involved in neuronal development,
survival, migration and growth
Vitamin D deficiency is associated with a range of neurologic disorders: PD, MS, schizophrenia, depression, cognitive decline, and AD.


Vitamin D Deficiency is common in the Newcastle 85+ participants
25 (OH) D (nmol/l) <10 <25 <30 <40 <60 <50 <70
2 25 33 51 63 73 82 % of cohort
<80
88
Institute of Medicine DRI’s Deficiency = 30 nmol/l EAR established at 40 nmol/L RDA established at 50 nmol/L
Hill et al (Osteoporosis International under review)
All seasons
Serum 25(OH)D and cognitive function in older adults
• Inverse relationship (global cognition and/or executive function and <50nmol/l 25(OH)D)
• Four prospective studies with inconsistent results
o InCHIANTI (Llewellyn et al 2010); MrOS (Slinin et al 2010); Study of Osteoporotic Fractures (Slinin et al 2012); Health ABC (Wilson et al 2014)
• Adults aged >65

25(OH)D and cognitive decline
• Both low and high season-specific quartiles of 25(OH)D were associated with:
• - higher odds of prevalent cognitive impairment
• - poorer attention reaction times and greater attention fluctuation compared to those in middle quartiles suggesting a U-shaped relationship.
• No association between 25(OH)D groups and odds of incident cognitive impairment or cognitive decline over 3 years. • Limited evidence for worse cognitive
status at 3-yr follow-up • Similar rate of change over time across
25(OH)D groups for all attention measures.

Implications and ongoing work
• Diet is still important modifiable risk factor for cognitive health at very old age
• Those consuming healthier DP arrived at very old age in better cognitive health compared with others
• Consider synergistic/antagonistic impact of foods/nutrients on cognitive health
o DP enable to explore whole diet – cognition relationship which may be easier to detect
• Maintaining an adequate vitamin D nutritional status may be important for cognitive health
o Preventing deficiency will have musculoskeletal benefits and may very well have benefits to cognitive health also
• B-vitamin status (Red cell folate, plasma vitamain B12) and cognitive decline (Nuno Mendonca, PhD student)
• Tea and cognitive decline with Dr Ed Okello (Director of the Medicinal plants Research Center, AFRD, Newcastle University)

Biomarkers could contribute to provide evidence of impact of nutrients on cognition
• Designing innovative intervention studies should consider:
• Identifying those who will likely benefit from treatment
o NUTRITION: Aim for nutritionally deficient participants ?
o DISEASE STAGE: Disease progression- at what stage should the intervention begin? MCI ?
o GENETICS: Genotyping for key candidate genes to target those most likely at risk
• Identifying biomarkers of disease progression
o Brain/CSF biomarkers of neurodegeneration
• Biomarkers of mechanisms of action
• Use of –omic technologies
o To identify potential metabolic pathways involved in the link between nutrition and brain function

Acknowledgements
Newcastle 85+ Research Team
Research nurses
The Newcastle 85+ Study academic
stakeholders
National Health Service organizations

IHS & NUIA