Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Diagnostic laparoscopy in the era of modern imaging—retrospectiveanalysis from a single center
Deepak Amarapurkar & Nirav Bhatt & Nikhil Patel &Pooja Amarapurkar & Anjali Amarapurkar
Received: 8 July 2012 /Accepted: 14 April 2013# Indian Society of Gastroenterology 2013
AbstractIntroduction A retrospective analysis of utility and out-comes of diagnostic laparoscopy at our center in the last5 years was done.Material and Methods In the last 5 years, we subjected 90patients to diagnostic laparoscopy (DL) when final diagno-sis could not be achieved after all necessary imagingmethods and serological, cytological, and microbiologicalinvestigations. DL was performed under sedation and localanesthesia, and patients were discharged within 24 h. Videodocumentation along with guided biopsies/collection of thesamples for culture and other tests was performed.Results The commonest indication was ascites (46/90),followed by diffuse liver disease (15), focal liver disease(9), intraabdominal malignancies (10), and miscellaneous(10). Overall accuracy of DL was 91 %. In 64 % of patients,laparoscopy confirmed the clinical diagnosis, and in 27 % ofpatients, laparoscopy was useful in correcting the diagnosis.DL was performed in 46 patients with low-serum asciticfluid albumin gradient ascites and ascites of mixed etiology.DL confirmed the suspected diagnosis in 48 %, corrected in38 %, and yielded unsuspected diagnosis in 15 % patients.In 6 % of patients, laparoscopy was inconclusive. In threepatients, there were extensive intraperitoneal adhesions, andadequate examination was not possible. No serious compli-cations were encountered. Minor complications of pain atthe port site, ascitic fluid leakage, and port site infectionwere seen in three, two, and one patient, respectively.
Conclusion DL is useful in patients when diagnosis andextent of the disease were unclear especially in ascites ofundetermined etiology.
Keywords Ascites . Diagnostic accuracy . Imagingmodalities . Serum ascitic fluid albumin gradient
Introduction
Diagnostic laparoscopy (DL) is an endoscopic examinationof the peritoneal cavity which facilitates visualization ofmore than two thirds of the liver surface, gallbladder, spleen,falciform ligament, parietal peritoneal surface, serosal as-pects of the gastrointestinal (GI) tract, and the pelvic organs[1]. Though the first DL was performed more than 100 yearsago, its role has significantly reduced in recent years due tothe advent of new imaging techniques like radioisotopescan, ultrasonography, computed tomography, and magneticresonance imaging [2, 3]. Imaging capabilities of the newtechniques do overlap with DL and can accomplish some-thing that DL can never do. These modalities are useful inmaking accurate diagnosis but also produce findings thatmay require visual clarifications. Ultrasound requires highprofessional skill, and findings remain dubious in obesepatient’s gaseous distention of bowel loops. Lesions lessthan 1 cm cannot be identified and the parietal peritoneumcannot be assessed by the imaging techniques. In contrast,DL can identify lesions as small as 1 to 2 mm in size whichcan be biopsied with pinpoint accuracy under direct vision.DL provides the capability to obtain large histological spec-imens as compared to imaging-directed biopsies which aremore of a cytological than histological examination. Theutility of DL has been reduced but not eliminated by newerimaging techniques [2].
Currently, DL is indicated in patients with (a)intraabdominal/retroperitoneal masses, (b) liver disease,
D. Amarapurkar (*) :N. Bhatt :N. Patel : P. AmarapurkarDepartment of Gastroenterology and Hepatology,Bombay Hospital and Medical Research Centre, 12, Marine Lines,Mumbai 400 020, Indiae-mail: [email protected]
A. AmarapurkarSRL, Dr Avinash Phadke Laboratory, Mumbai, India
Indian J GastroenterolDOI 10.1007/s12664-013-0338-x

(c) ascites, (d) abdominal pain or acute abdomen, or (e)abdominal trauma [3–5]. Retrospective analysis of utilityand outcomes of DL at our center in the last 5 yearswas done.
Material and Methods
This was a single-center retrospective study of 90 patientsundergoing DL at our center over a period of 5 years (2006–2010). We reviewed records of all the patients who hadundergone DL. History, clinical examination, investigationfindings, and clinical diagnosis were evaluated by the seniorauthor prior to DL. No definitive conclusion could bereached in spite of biochemical investigations, which in-cluded complete blood count, liver function test (serumbilirubin, serum proteins, transaminases, gamma-glutamyltranspeptidase, and prothrombin time), and serum creati-nine. Tumor markers like carcinoembryonic antigen (CEA),CA125, and CA19-9 were determined whenever suspected.Ultrasonographic examination of the abdomen and pelvis wasdone in all patients. Computerized tomography and/or mag-netic resonance imaging was done as per clinical information.Imaging-guided fine-needle aspiration biopsies of focal le-sions were done whenever possible. Ascitic fluid examinationincluding total proteins, albumin, cell count, lactate dehydro-genase (LDH), adenosine deaminase (ADA), PCR for tuber-culosis, and cytology for malignant cells were done. Otherancillary studies like upper and lower GI endoscopies andendoscopic retrograde cholangio pancreaticography and sero-logical markers for viral, autoimmune, or metabolic diseaseswere performed as deemed necessary. Inclusion criteria—allthe patients with suspected intraabdominal pathology whichwas not diagnosed conclusively with the above-described testswere subjected to DL. Out of 90 patients subjected to DL, thecommonest indication was ascites of undetermined etiology(51 %), followed by diffuse liver disease (17 %), focal liverdisease (10 %), intraabdominal malignancies (11 %), andmiscellaneous (11 %) (Table 1). Prelaparoscopy indicationsin patients with ascites included suspected malignant
peritonitis (13), tubercular peritonitis (22), liver disease (3),miscellaneous (pancreatic ascites, panniculitis—2), and noprovisional clinical diagnosis (6). Post-DL outcomes in thesepatients were malignancy (4), tubercular peritonitis (25), focalliver disease (6), and other diagnoses in the remaining(Table 2). Suspected diffuse liver diseases were nonalcoholicsteatohepatitis, cirrhosis, and multinodular diseases like nod-ular regenerative hyperplasia and sarcoidosis. Peritoneal car-cinomatosis and pancreatobiliary malignancy were thecommon causes of suspected malignancy. All patients withacute abdomen who had undergone DL were investigatedwith routine biochemical workup along with plain X-ray,ultrasonography, and CT scan of the abdomen. In the absenceof a definitive diagnosis, patients were subjected to DL. Awritten informed consent was obtained from each patient. DLwas performed in the operation theater under strict asepticprecautions. All the procedures were carried out under localanesthesia and mild sedation with a standby anesthetist [6].
During the procedure, a thorough visualization of theperitoneal cavity and its content was done along with videorecording. Laparoscopic findings were confirmed by at leasttwo observers. In the case of ascites, biopsies from theperitoneal or omental lesions were taken. If there were liverabnormalities or focal liver lesions on the surface, liverbiopsies were done. In the case of mass lesions, biopsiesfrom the surface of the mass were taken. After the procedure,the incision site was stitched. The patient’s vital signs wereobserved closely for the first 4 h. Stitches were removed on theseventh postoperative day.
Results
A total of 90 patients (44 male, 46 female) underwent DLduring the 5-year period from 2006 to 2010. The age rangeof the patients was 10–72 years with a mean age of43.7 years. DL and biopsy revealed diagnosis of tuberculo-sis in 36 patients, malignancy in 13 patients, and diffuseliver disease and focal liver disease in 7 and 8 patients,respectively. Rare conditions that were diagnosed included
Table 1 Indications and outcomes in patients undergoing diagnostic laparoscopy
Indications of diagnostic laparoscopy (provisional diagnosis) No. Post diagnostic laparoscopy diagnosis No.
Ascites of undetermined etiology 46 Malignancy 13
Diffuse liver disease (cirrhosis, multinodular disease, diffuse hepatomegaly) 12 Tubercular abdomen 36
Focal nodular liver disease 4 Diffuse liver disease 7
Suspected malignancies 10 Focal liver disease 8
Suspected tuberculosis of peritoneum or mesentery 5 Miscellaneous 19
Suspected miscellaneous diagnosis of acute abdominal pain(cholecystitis, subacute intestinal obstruction, or appendicitis)
5 Inconclusive 5
Undiagnosed abdominal pain 8
Indian J Gastroenterol

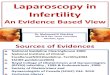
pseudomyxoma peritonei (two), mesenteric panniculitis(one), GI stromal tumor (two), endometriosis (one), Budd–Chiari syndrome (two), and nephrogenous ascites (two).Pseudomyxoma peritonei was diagnosed on findings of apale translucent jelly like material in the abdominal cavity aswell as attached to the peritoneal surface [7] (Fig. 1a). In apatient with mesenteric panniculitis, the peritoneum showedmultiple areas of fat necrosis and the liver was grossly fatty,which were confirmed histologically [8] (Fig. 1d). The GIstromal tumor was a well-circumscribed capsulated tumorpresent on the external surface of the third and fourth partsof the duodenum with metastatic deposits on the liver sur-face (Fig. 1c). Peritoneal endometrial implants were identi-fied as invasive peritoneal fibrotic nodules and adhesions
which were confirmed histologically [9]. The patient withBudd–Chiari syndrome was misinterpreted as having a liver-infiltrating mass on ultrasonography and CT scan; at DL, thecaudate lobe was markedly enlarged with a nodular contour inthe right lobe of the liver. The external surface of the livershowed whitish dilated lymphatics, tortuous dilated veins, andcongested liver. This patient had no ascites and mild spleno-megaly. Liver histology demonstrated hemorrhagic necrosisand dilated sinusoids filled with erythrocytes; diagnosis wasconfirmed with hepatic angiography later. Similar changeshave been reported previously [10]. Nephrogenous ascites isa complex diagnostic problem with poorly understood patho-physiology. Diagnosis of nephrogenous ascites should beconsidered in patients with chronic renal failure on dialysis,
Table 2 Indications and outcomes of patients with ascites undergoing laparoscopy
Indications of diagnostic laparoscopy No. Post diagnostic laparoscopy diagnosis No.
Ascites of undetermined etiology 46 Malignancy 4
Diffuse liver disease (low protein, high SAAG) 2 Tubercular abdomen 25
Focal nodular liver disease (high protein, high SAAG) 1 Focal liver disease 6
Suspected malignancies (high protein, low SAAG) 13 Miscellaneous 8
Suspected abdominal tuberculosis of peritoneum or mesentery(high protein, low SAAG)
22 Inconclusive 3
Miscellaneous (low protein, low SAAG, high cell count) 2
Undiagnosed (variable protein, variable SAAG, and variable cell count) 6
SAAG serum ascitic fluid albumin gradient
Fig. 1 Laparoscopicappearances of variousdiseases. a Myxomatousdeposits on peritoneum–pseudomyxoma peritonei. bMultiple tiny tubercles on liver.c Gastrointestinal stromal tumoron the serosal surface of theduodenum. d Fat necrosis onthe peritoneum and mesentery—mesenteric panniculitis. eMultiple secondaries on theperitoneum and mesentery
Indian J Gastroenterol

who develop ascites. Nephrogenous ascites is low-serum as-citic fluid albumin gradient (SAAG) and low-cell-count asci-tes [11]. DL is useful in excluding other causes of ascites. DLwas inconclusive in five patients. Overall outcomes are shownin Table 1. DL confirmed the suspected diagnosis in 64 % ofpatients, corrected the diagnosis in 22 %, and revealedunsuspected diagnosis in 8 % of patients. Utility of DL inpatients with ascites was estimated. It confirmed the diagnosisin 48 % of patients and corrected the diagnosis in 30 % ofpatients while revealing unsuspected diagnosis in 15 % ofpatients.
Discussion
Ascites was the major indication for DL in our patients.Cirrhosis is the cause of ascites in more than 85 % in thewestern world while tuberculosis is seen in 30 % of thepatients with ascites in India [6, 12]. Ascites secondary toperitoneal diseases or chronic liver disease may have re-markably similar clinical presentations. Ascitic fluid is clas-sified on the basis of SAAG. SAAG, cell count, bacterialculture, pH, glucose, LDH, and amylase are useful in thedifferential diagnosis of ascites [12]. Different diseases cancause different types of ascites. Some of the known low-SAAG ascites include tuberculous peritonitis, malignancy-induced ascites (for instance, peritoneal carcinomatosis, gas-tric and ovarian cancer metastases), pancreatic ascites, renalascites, biliary ascites, bacterial peritonitis, and serositis-induced ascites. On the other hand, high-SAAG ascites areuncomplicated cirrhotic ascites, ascites due to heart failure,those induced by extensive liver metastases, and other cir-cumstances such as fulminant hepatic failure [12–14]. Wepreviously reported the value of DL in patients with low-SAAG ascites [6]. Although recent advances in diagnosis oftuberculous ascites like ADA and PCR for mycobacterialtuberculosis have improved efficacy, they still lack specific-ity and are costly. ADA is of no utility in patients ofcirrhosis with tuberculosis. There is no specific biologicalmarker for tuberculosis [15]. Raised levels of CA125 areseen in both tuberculosis and ovarian malignancy. A definitediagnosis of tubercular peritonitis is established only on DLexamination with peritoneal biopsy, and it helps in exclud-ing other causes of ascites [16].
In spite of widespread use of percutaneous liver biopsy,there are potential limitations to it. Percutaneous liver biop-sy can have a sampling error of 10 % to 20 % with atendency to underestimate cirrhosis by 30 % [17, 18]. Wepreviously reported usefulness of DL in diagnosis of cirrho-sis and liver tumors [19]. It offers a direct view of the liverand facilitates targeted biopsies for histological confirma-tions. In an elegant study, Poniachik et al. [18] demonstratedthat DL with biopsy is the gold standard for diagnosis of
liver cirrhosis. Recently, DL has been utilized as a diagnos-tic tool in patients with acute appendicitis, chronic abdo-minal pain, patients with peritonitis, and critically illpatients with acute abdomen [5]. DL has been shown to beof great help in the diagnosis of uncertain imaging findingsespecially patients with tumors of the pancreas and biliarytract where pathological confirmation could not be achieved[1–3]. DL has been shown to be highly predictive as asecond look following chemotherapy for ovarian, tubal,and primary peritoneal carcinomatosis [20].
In this retrospective analysis, we demonstrate the role ofDL in the era of modern imaging and show that it continuesto be useful in patients in whom diagnosis and extent ofdisease are unclear.
References
1. Trujillo NP. Peritoneoscopy and guided biopsy in the diagnosis ofintraabdominal diseases. Gastroenterology. 1976;71:1083–6.
2. Lightdale CJ. Diagnostic laparoscopy in the era of minimallyinvasive surgery. Gastrointest Endosc. 1992;38:392–4.
3. Hori Y, SAGES Guidelines Committee. Diagnostic laparoscopyguidelines: this guideline was prepared by the SAGES GuidelinesCommittee and reviewed and approved by the Board ofGovernors of the Society of American Gastrointestinal andEndoscopic Surgeons (SAGES), November 2007. SurgEndosc. 2008;221:353–83.
4. Chang L, Stefanidis D, Richardson WS, Earle DB, Fanelli RD. Therole of staging laparoscopy for intraabdominal cancers an evidencebased review. Surg Endosc. 2009;23:231–41.
5. Stetanidis D, Richardson WS, Chang L, Earle DB, Fanelli RD. Therole of diagnostic laparoscopy for acute abdominal conditions: anevidence based review. Surg Endosc. 2009;23:16–23.
6. Amarapurkar DN, Kalro RH, Desai HG. Peritoneoscopy in diagnosisof ascites. J Assoc Physicians India. 1991;29:933–5.
7. Fernandez RN, Daly JM. Pseudomyxoma peritoni. Arch Surg.1980;115:409–14.
8. Amarapurkar DN, Patel ND, Amarapurkar AD. Panniculitis andliver disease (hepatic Weber Christian disease). J Hepatol.2005;42:149–50.
9. Chamie LP, Blasbalg R, Pereira RM, Warmbrand G, Serafini PC.Findings of pelvic endometriosis at transvaginal US, MR imaging,and laparoscopy. Radiographics. 2011;31:77–100.
10. Nyman R, Kagevi I. Budd–Chiari syndrome misinterpreted as aninfiltrating liver mass. A case report. Acta Radiol. 1995;36:393–5.
11. Bichler T, Dudley DA. Nephrogenous ascites. Am J Gastroenterol.1982;77:73–4.
12. Runyon BA. Management of adult patients with ascites due tocirrhosis. AASLD practice guidelines. Hepatology. 2004;39:1–16.
13. Hou W, Sanyal AJ. Ascites diagnosis and management. Med ClinN Am. 2009;93:801–7.
14. European Association for the Study of the Liver. EASL clinicalpractice guidelines on the management of ascites, spontaneousbacterial peritonitis, and hepatorenal syndrome in cirrhosis. JHepatol. 2010;53:397–417.
15. El Abkari M, Benajah DA, Aqodad N, Bennouna S, Oudghiri B,Ibrahimi A. Peritoneal tuberculosis in the Fes University Hospital(Morocco). Report of 123 cases. Gastroenterol Clin Biol.2006;30:377–81.
Indian J Gastroenterol

16. Littell RD, Hallonquist H, Matulonis U, Seiden MV, BerkowitzRS, Duska LR. Negative laparoscopy is highly predictive ofnegative second look laparotomy following chemotherapy forovarian, tubal, and primary peritoneal carcinoma. GynecoOncol. 2006;10:570–4.
17. van Leeuwen DJ, Wilson L, Crowe DR. Liver biopsy in themid-1990s: questions and answers. Semin Liver Dis.1995;15:340–59.
18. Poniachik J, Bernstein DE, Reddy R, Jeffers LJ, et al. The role oflaparoscopy in the diagnosis of cirrhosis. Gastrointest Endosc.1996;43:568–71.
19. Amarapurkar DN, Parikh SS, Kalro RH, Desai HG. Comparison ofperitoneoscopy and phytate liver scan in diagnosis of liver cirrhosisand hepatic neoplasms. Bombay Hosp J. 1991;33:35–8.
20. Valle M, Garofalo A. Laparoscopic staging of peritoneal surfacemalignancies. Eur J Surg Oncol. 2006;32:25–7.
Indian J Gastroenterol