Embed Size (px)
Citation preview

Behçet’s disease ?Diagnostic criteria
Intestinal BD ?Colonoscopic findingsDifferential diagnosisSerologic markers
Won Ho Kim, M.D.Yonsei University, Seoul
Diagnostic Challenges in Asia; Intestinal Behçet’s Disease
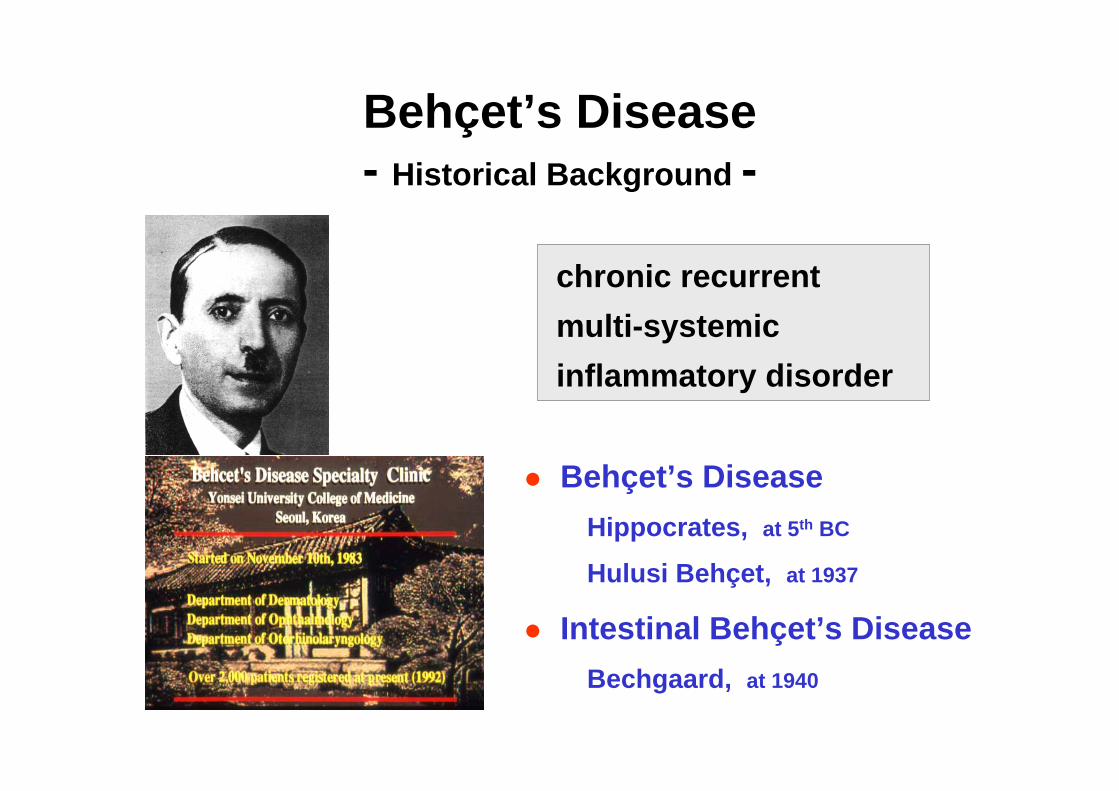
Behçet’s Disease- Historical Background -
Behçet’s DiseaseHippocrates, at 5th BC
Hulusi Behçet, at 1937
Intestinal Behçet’s DiseaseBechgaard, at 1940
chronic recurrent multi-systemicinflammatory disorder

Diagnostic Criteria for Behçet’s Disease
Major criteria
Arthritis
GI lesions
Vascular lesions
CNS lesions
Epididymitis
Minor criteria
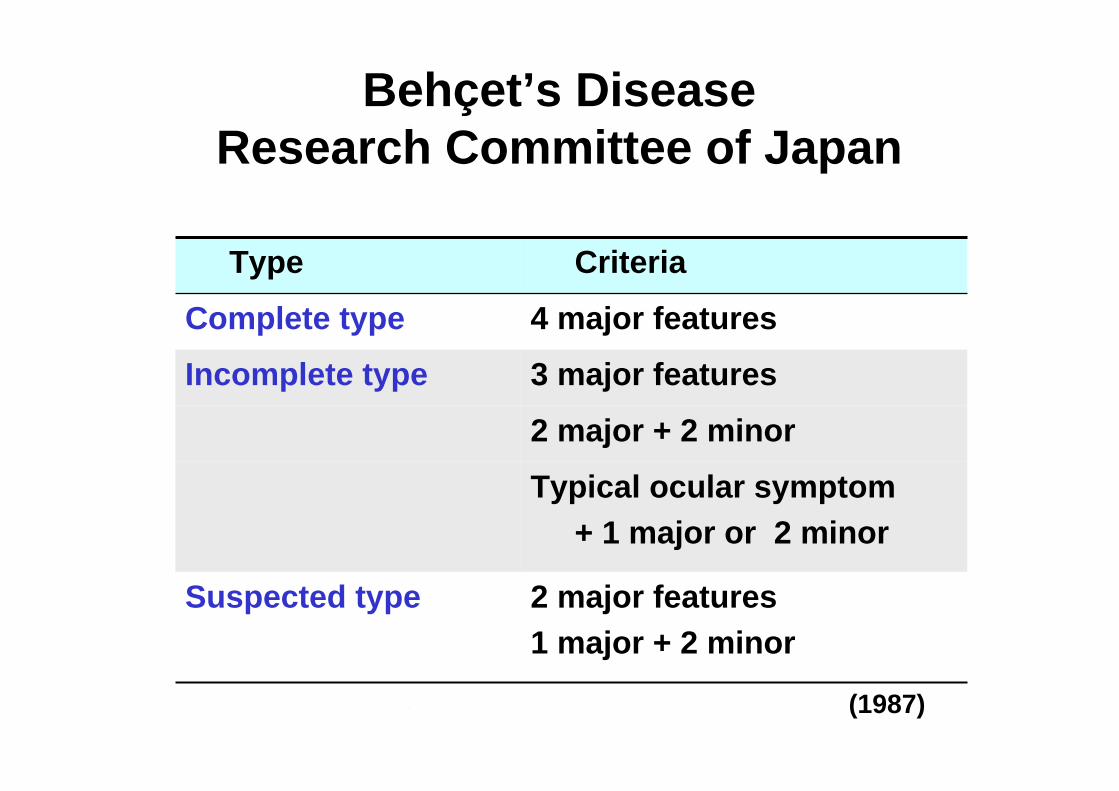
Behçet’s Disease Research Committee of Japan
(1987)
Typical ocular symptom + 1 major or 2 minor
CriteriaType
2 major features1 major + 2 minor
Suspected type
2 major + 2 minor
3 major featuresIncomplete type
4 major featuresComplete type

International Study Groupfor Behçet’s Disease (ISGBD)
Read by physician at 24-48 hPositive Pathergy test
Erythema nodosum, Pseudofolliculitis, or papulopustular lesionsAcneiform nodules in postadolescent patients
Skin lesions
Uveitis, or cells in vitreous on slit lamp Retinal vasculitis
Eye lesionsAphthous ulceration or scarringRecurrent genital ulceration
plus 2 of
Minor, major aphthous, or herpetiformulceration, recurred at least 3 times in one 12 month period
Recurrent oral ulceration
(1990)

GI Involvement in Behçet’s Disease
Perforation
Fistula
Abscess
Bleeding
Complications

General Aspects of Intestinal BD
Frequency3-25% of BDWide geographic differences
East Asia > Mediterranean
Age/Sex ratio3rd decade for BD 4th decade for intestinal BDM > F in intestinal BD
Symptoms: variableAbdominal pain (most common)DiarrheaBleeding

Burdens of Intestinal BD- Compared with UC and CD -
Probability of AZA/6-MP use
Choi CH, et al. presented at the Falk Sym. 2002
Cumulative operation rate
Choi IJ, et al. Kor J Gastroenterol 2000;36:504-14
80
60
40
20
012 24 36 48 60 72 84 96
BD (n=66)
CD (n=140)p=0.20
Months
Ope
ratio
n ra
te (%
)
80
60
40
20
0
Prob
abili
ty (%
)
12 24 36 48 60 72 84 96Months
BD (n=133)
CD (n=72)
UC (n=197)

Diagnosis of Intestinal BD
Diagnosis of BD Diagnostic criteria
Presence of intestinal lesion and differentiation from other disease
Endoscopic and radiologicalHistopathologicLaboratory markersClinical course

Application of Diagnostic Criteria for BD in Intestinal BD
Is the presence of systemic symptoms mandatory for diagnosis of intestinal BD ?Japanese criteria
Too complexMore feasible for diagnosis in cases with step-wise manifestation of symptoms
ISGBD criteriaMore unified, simple diagnosisOral ulcer / Pathergy test ?

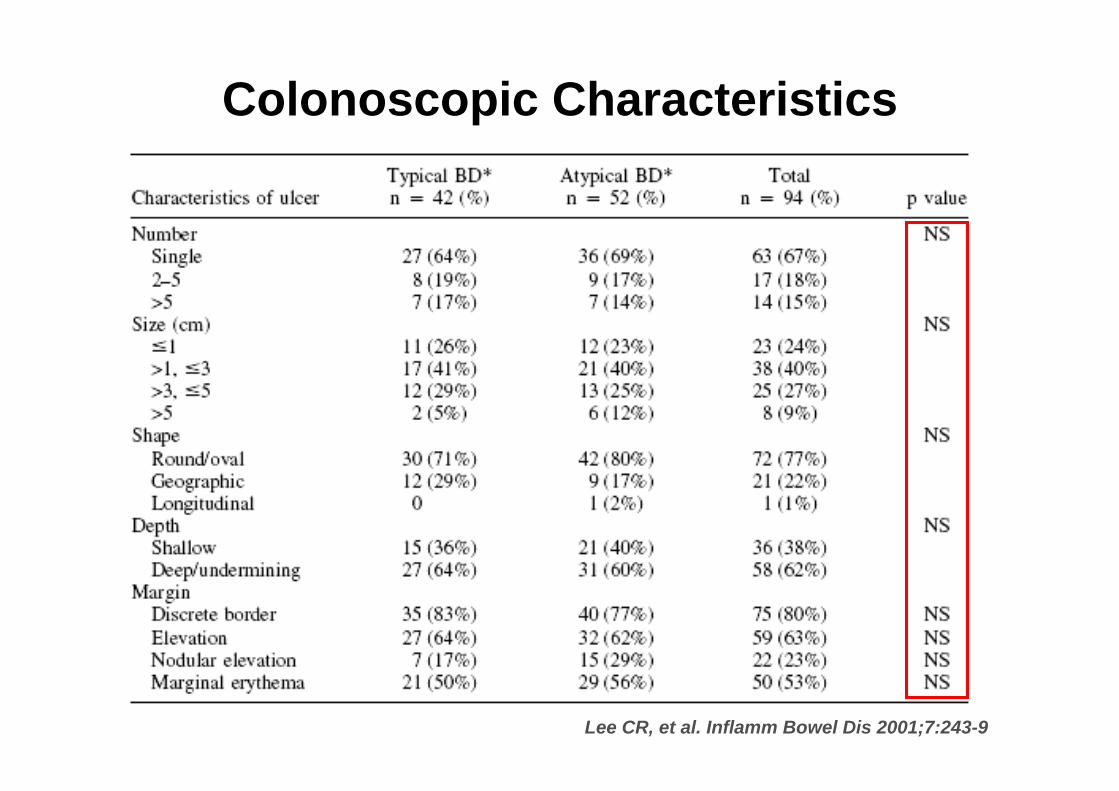
Lee CR, et al. Inflamm Bowel Dis 2001;7:243-9
Symptoms in Intestinal BD - Typical BD vs. Atypical BD -
Lee CR, et al. Inflamm Bowel Dis 2001;7:243-9
Colonoscopic Characteristics

Satisfaction for Diagnostic Criteria
At the end point of follow-up
24 (19.0%)28 (22.2%)suspicious
At diagnosis of intestinal BD
59 (46.8%)67 (53.2%)
17 (13.5%)
62 (49.2%)23 (18.3%)
102 (81.0%)24 (19.0%)
62 (49.2%)
33 (26.2%)3 ( 2.4%)
not-satisfiedsatisfied
ISGBD criterianot-satisfied
incompletecomplete
Japanese criteria
Severance hospital (n = 126 )Mean F/U period after Dx of intestinal BD: 63.9 months

Onset and Prevalence of Systemic Onset and Prevalence of Systemic Manifestation in Intestinal BDManifestation in Intestinal BD
3 (2.4%)0 (0.0%)10.61 ± 5.41CNS Lesions
0 (0.0%)0 (0.0%)-Epididymitis
70 (55.6%)27 (21.4%)0.67 ± 5.29Genital ulcers
8.95 ± 9.00
3.95 ± 7.62
3.32 ± 5.76
0.98 ± 6.80
-5.38 ± 8.40
Onset(yr)
7 (5.6%)
65 (51.6%)
37 (29.4%)
77 (61.1%)
122 (96.8 %)
At the end point of follow-up
1 (0.8%)
24 (19.0%)
14 (11.1%)
38 (30.2%)
97 (77.0 %)
At diagnosis of intestinal BD
Vascular lesions
Arthritis
Eye lesions
Skin lesions
Oral ulcers
Criteria of BD
Pathergy test (n=115):12 (9.6%)

Colonoscopic Findings in Intestinal BD
Single / Few
Large / Deep
Round / Oval
Discrete / Elevated margin
Lee CR, et al. Inflamm Bowel Dis 2001;7:243-9

Pathologic Findings in Intestinal BD
Non-specific inflammationVasculitis
Lymphocytic infiltration
No granuloma

Differential Diagnosis- Colonoscopic Findings -
Colonic ulceration may be induced by broad spectrums of disease.
Similarity with Crohn’s diseaseGI symptomsExtra-intestinal symptoms
: oral ulcer, skin lesions, arthritis …Clinical course of diseasePresence of intestinal ulceration

0.06514 (20)10 (10)Stricture<0.00123 (33)4 ( 4 )Inflammatory polyp0.00110 (10)1 ( 1 )Perianal lesion
12 (17)7 ( 7 )Aphthous
13 (19)23 (23)Nodular<0.00139 (56)21 21)Aphthous lesion
21 (30)61 (61)Deep / Undermining<0.001Border
34 (49)81 (81)Discrete36 (51)19 (19)Ill-defined
<0.05Erythema of ulcer margin19 (27)43 (43)Normal 51 (73)57 (57)Erythematous
<0.05Ulcer margin44 (63)40 (40)Flat13 (19)37 (37)Smoothly elevated
pCD (%) n=70BD (%) n=100
49 (70)39 (39)Shallow<0.001Depth
21 (30)24 (24)Irregular / Geographic34 (49)1 ( 1 )Longitudinal3 ( 4 )68 (68)Round / Oval
<0.001Shape59 (84)15 (15)>57 (10)17 (17)2~54 ( 6 )68 (68)1
<0.001Number
Intestinal BD vs. CD in Colonoscopic Finding
Kim TI, et al. Journal of Gastroenterol Hepatol 2001;16;30(A)

p < 0.001
CD(n=70)
5 16 35 14
BD(n=100)
68 25 2 5
Focalsingle
Focalmultiple Segmental Diffuse
Distribution of Lesions
Kim TI, et al. Journal of Gastroenterol Hepatol 2001;16;30(A)

Ulcer shape
Round/Oval Longitudinal
Distribution of lesion
Focal singleFocal multiple
SegmentalDiffuse
Intestinal Behçet’s disease Crohn’s disease
Classification And Regression Tree (CART)
Irregular/Geographic
Hit ratio:0.9189

Diagnosis of Intestinal BD- Serologic marker -
Pathogenesis of BDAberrant immune activityTriggering environmentGenetic predisposition
Suggested auto-antibody in BDAntibody to retinal antigensAntibody to heat shock protein (HSP)Antibodies to α-tropomyosinAntibody to endothelial cell antigen (AECA)
Immunologic factor
Genetic factor Environmental factor
Behçet’s Disease

ASCA (Anti-Saccharomyces Cervisiae Antibody)
10-15%UC (reported ranges from other’s study)
40-70%CD (reported ranges from other’s study)
4 (8.8%)Healthy controls (n=45)
1 (3.3%)BD (n=30)
47 (44.3%)
ASCA (+)
Intestinal BD (n=106)
Figure 1. Staining of the cell wall of Saccharomycescerevisiae caused by antibodies to Saccharomycescerevisiae -positive serum (immunofluorescence, x400).
Choi CH, et al. Gatroenterology 2004;126:203(A)

ASCA and Clinical Course in Intestinal BD
(%)100
100806040200
80
60
40
20
ASCA(-)
ASCA(+) p = 0.006
Cumulative probability of the 1st operation
MonthsChoi CH, et al. Gatroenterology 2004;126:203(A)
No differences inClinical findingsTreatment with AZA/6MPProbability of 2nd op. Relapse rates

Anti α-enolase Ab
37.5%BD (n=40)
40 %UC (n=100)
31 %CD (n=100)
0%Healthy controls (n=23)
63%Intestinal BD (n=100)
AAEA (+)
Shin SJ, et al. Journal of Gastroenterol Hepatol 2005;20:143(A)
Glycolytic enzymePlasminogen receptor on the surface of endothelumModulation of fibrinolysis
α-enolase
Association with various autoimmune diseases :RA, SLE, MCTD, IBD, sytemic sclerosis
Anti α-enolase antibody

Summaries and Conclusions
Behçet’s disease is…Intestinal Behçet’s disease is…
Dx of intestinal Behçet’s disease Characteristic colonoscopic findingsApplication of diagnostic criteria Antibody assay
Clinical activity index