Embed Size (px)
Citation preview

Gut 1993; 34:1075-1080
Failure of colonoscopic surveillance in ulcerativecolitis
D A F Lynch, A J Lobo, GM Sobala, M F Dixon, A T R Axon
AbstractA prospective surveillance programme forpatients with longstanding (>=8 years),extensive (>=splenic flexure) ulcerativecolitis was undertaken between 1978 and 1990.It comprised annual colonoscopy with pan-colonic biopsy. One hundred and sixty patientswere entered into the programme and had 739colonoscopies (4.6 colonoscopies per patient;709 patient years follow up). Eighty eight percent of examinations reached the right colon.There was no procedure related death. OneDukes's A cancer was detected. Forty onepatients (25%) defaulted. Of these 25 remainwell; 13 are unaccounted for, and one diedfrom colonic cancer. One patient had colec-tomy for medical reasons, and another died ofcarcinoma of the pancreas. Retrospectively anadditional 16 eligible patients were identifiedwho had not been recruited. Of these, 14remain well, two are unaccounted for. Nonedeveloped colonic cancer. Four patientsrefused colonoscopy. All remain well. Over thesame period seven other cases of coloniccancer were found in association with ulcera-tive colitis, two in patients who had errone-ously been diagnosed as having only proctitisand were therefore not entered into the pro-gramme, but were found at operation to havetotal colitis, one in a patient with colitis ofseven years duration, and four patients whohad previously attended the clinic but had beenlost to follow up before 1978 and then had re-presented with new symptoms during the sur-veillance period. Thus, of the nine colitisrelated cancers diagnosed in this centre duringthe study period only one was detected by thesurveillance programme. The results of thislarge study, and a review of published works,cast doubts on the effectiveness of colono-scopic surveillance programmes in detectingcolorectal cancer in patients with ulcerativecolitis.(Gut 1993; 34: 1075-1080)
Centre for DigestiveDiseases, The GeneralInfirmary, LeedsD A F LynchA J LoboGM SobalaM F DixonAT R AxonCorrespondence to:Dr D A F Lynch,Gastroenterology Unit,The General Infirmary, LeedsLS1 3EX.
Accepted for publication26 November 1992
Colorectal carcinoma was recognised as a
complication of ulcerative colitis over 65 yearsago.' The risk of developing cancer is increasedin those individuals who have had extensivecolitis for more than 10 years after the firstattack, the cumulative cancer rate being 7% at 20years and 17% at 30 years disease duration.2 Suchwas the perceived risk of a patient developingcancer that prophylactic colectomy has beenrecommended.The strong association between colorectal
dysplasia and cancer in ulcerative colitis wasdescribed in 1967.7 The development of flexibleendoscopy, which allows pancolonic biopsy, has
supported this finding-' and has led to a changein practice such that in many centres at riskpatients are examined at intervals, with colono-scopy and biopsy, to detect premalignant dys-plasia or early cancer.These cancer surveillance programmes are
now widely implemented despite not havingbeen subjected to clinical trial. A number ofreports'-" have supported the use of colono-scopic surveillance in ulcerative colitis, butdoubts have also been expressed about itsefficacy.'8
Surveillance programmes are expensive, timeconsuming, and unpleasant for patients andshould be shown to be effective before imple-mentation. Colonoscopic surveillance in colitisshould reduce cancer related death comparedwith routine clinical care, by detecting earlycurable cancer. It might be deemed unethical,however, to perform a controlled trial. Gastro-enterologists, therefore, have a responsibility toreview their results to show whether or not thisform of surveillance is effective.
In 1978 a prospective surveillance programmewas started9'14 whereby all patients with long-standing extensive ulcerative colitis were invitedto have annual colonoscopy with biopsy. In thispaper the results of this large programme andother reported series are reviewed to discover ifcolonoscopic surveillance works.
Methods
SURVEILLANCE PROGRAMMEFrom 1978 to December 31 1990 all patients withlongstanding (>= 8 years) and extensive (diseaseextending to or beyond the splenic flexure)ulcerative colitis were advised to have annualcolonoscopy with pancolonic biopsy.
Patients were seen at routine clinic follow upand the reasons for surveillance explained. If thepatient failed to attend for their clinic/colono-scopy then a repeat appointment was made. If asecond reminder was unsuccessful no furtheraction was taken. If patients were known to bemoving away a letter detailing their surveillancehistory was sent to their doctor or next supervis-ing consultant.The duration of disease was taken from the
date of diagnosis except where obvious symp-toms of 'colitis came before the diagnosis by amatter of years. Disease extent was verified bybarium enema or colonoscopy, or both. Patientsolder than 75 years were not entered and thosereaching 75 during surveillance were withdrawn.
Colonoscopy was carried out under lightsedation after standard laxative and bowel enemapreparation. Biopsy specimens were taken withforceps from flat mucosa at about 10 cm intervals
1075

Lynch, Lobo, Sobala, Dixon, Axon
along the colorectum and from any identifiable'mass lesions'. These correspond to the followingdescriptive sites: caecum; proximal ascendingcolon; distal ascending colon; proximal trans-verse colon; distal transverse colon; proximaldescending colon; distal descending colon;sigmoid colon; rectum. Biopsy specimens weremounted on filter paper or placed in cassettesbefore fixation in formalin and after routineprocessing were sectioned at three levels andstained with haematoxylin and eosin.
If dysplasia was present it was classified as lowgrade, high grade, or carcinoma. If high gradedysplasia was found, repeat biopsies wereperformed within six months. Surgery was per-formed in cases of persistent high grade dys-plasia, or carcinoma.
DETERMINING OUTCOME OF SURVEILLANCEPROGRAMMEOur review of the surveillance programme hadthree distinct goals: (a) to obtain full follow up ofall patients who had participated at any time inthe surveillance programme; (b) to identify anyother patients who attended the departmentover this time and who should have beenrecruited into the surveillance programme; and(c) to identify all cases of colonic carcinomaoccurring in association with ulcerative colitispresenting to the department over this period.These goals were achieved as follows: (a) the
outcome of patients entered into the surveillanceprogramme was obtained from departmentalrecords, patient case notes, histopathologyreports, doctor, supervising consultant or
patient by clinic, letter or telephone; (b) eligiblepatients with ulcerative colitis were identifiedfrom index cards used to document all colitisclinic patients, and review of notes of all patientsattending the clinic for a 12 month period. Usingthis information notes were obtained from therecords departments. Information extractedincluded date of birth, relevant medical andsurgical history, date of onset of symptoms, dateof diagnosis (histological/radiological), diseaseextent (barium enema/colonoscopy), surveil-lance colonoscopy date and findings, biopsy siteand histological findings, and present status ifknown; (c) cases of cancer in association with
100 -
co 80 -
60
0
°40 -
' 20._
0 10 20 30 40 50
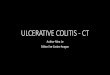
Years from diagnosisA low grade dysplasia free survival curve shows that25% ofpatients with ulcerative colitis had exhibited low gradedysplasia at least once by 17years after diagnosis ofulcerativecolitis, 50% at 25 years, and 75% by 38years.
colitis were identified from histopathologydepartment records that document all colitispatients who developed dysplasia, cancer, or hadcolonic surgery since 1978.
ResultsOne hundred and eighty patients fulfilledthe criteria for entry into the surveillanceprogramme.
RECRUITMENT FAILURESSixteen patients were erroneously not enteredinto the programme by the supervising physicianbecause they were unaware that the patient waseligible for surveillance. Fourteen of thesepatients are well, a mean of 9-4 years (range3-12) after what should have been their pro-gramme entry date. Two are unaccounted forafter a mean of three years.
SURVEILLANCE REFUSALSFour patients refused colonoscopic surveillance,but continue with regular clinical supervision.All are well, a mean of 9 75 years (range 6-12)after programme entry date.
PATIENTS STARTING SURVEILLANCEOne hundred and sixty patients entered thesurveillance programme and had 739 colono-scopies (4-6 colonoscopy/patient; 709 yearsfollow up). The mean length ofduration of colitiswas 14-1 years (range 8-46). Eighty eight percent of examinations reached the right colon.There was no procedure related death. Biopsyspecimens (5695) were taken giving a mean of7-8 per colonoscopy (range 1-9).
SURVEILLANCE DEFAULTERSForty one patients who started surveillancedefaulted. Twenty five remain well, a mean of2 5 years (range 2-10) after default. Thirteenpatients are unaccounted for, mean 6 5 years(range 2-12) later. One patient died of dissemi-nated colonic cancer after three years (see TableI, patient E), the three previous complete annualcolonoscopies had been negative for dysplasia.One patient had colectomy for medical reasonssix years later. No cancer was found. One patientdied of pancreatic cancer seven years later.
LOW GRADE DYSPLASIAForty patients were found to have low gradedysplasia in at least one biopsy. The mean age atfirst diagnosis of low grade dysplasia was 45 2years (SD 13-64) and mean duration of colitis todiagnosis of low grade dysplasia 17-7 years (SD7 33).These 40 patients had a further 201 colono-
scopies (223 patient years follow up). Twenty(50%) had no further dysplasia (mean 4 0 colono-scopies per patient over 4-7 years). Nineteencontinued to exhibit low grade dysplasia in atleast one subsequent biopsy (mean 6-3 follow upcolonoscopies per patient over 6 9 years). One of
1076

Failure ofcolonoscopic surveillance in ulcerative colitis
TABLE I Colorectal cancer in ulcerative colitis 1978-1990
Durationof
Year of ulcerative Extent ofcolitis!cancer colitis method of Dukes'sdiagnosis Age Sex (years) deternination Presentation stage Patient group
Patient A1979 60 M 7 Total/ Previous history of colonic polyps. A Did not fulfil eligibility
colonoscopy Colonoscopy performed at 7 years criteriaduration to determine extent pluspolypectomy (Barium enema showedrecurrence of polyps)
Patient B1983 49 F 20 Rectum/ Patient believed to have proctitis. B Did not fulfil eligibility
sigmoidoscopy Diagnosed 1963. Lost to follow up. criteriaPresented with symptoms 1983. Found tohave rectal carcinoma
Patient C1984 45 M 21 Total/ Patient entered surveillance 1979 at 17 years A Surveillance
colonoscopy duration. High grade dysplasia at fifthcolonoscopy. Colectomy performed
PatientD1984 33 M 12 Total/barium Lost to follow up 1972. Re-presented 1984 A Lost to follow up before
with colitic symptoms. Barium enema programmeshowed sigsnoid polyp. Colonoscopyshowed high grade dysplasia. Colectomyperformed
PatientE1985 36 M 18 Total/barium Normal surveillance 1980-82. Moved away >=C Defaulter
enema 1982/83. Died with a disseminated coloncarcinoma 1985
Patient F1987 42 F 19 Total/ Diagnosed 1968. Lost to follow up. C Lost to follow up before
colonoscopy Presented with rectal bleeding 1987. programmeSigmoidoscopy showed polypoid, rectalcarcinoma. Anterior resection performed.Patient entered into surveillance
Patient G1988 47 M 20 Unknown Lost to follow up in 1970. Re-presented in C Lost to follow up before
1987 with rectal bleeding. Colonoscopy programmeshowed carcinoma in situ at 80 cm
PatientH1990 62 M 21 Unknown Believed to have proctitis. Diagnosed 1969. C Did not fulfil eligibility
Lost to follow up 1972. Presented with criteriachanged bowel habit 1990. Ascendingcolon and sigmoid cancer on bariumenema
Patient I1990 44 M 26 Unknown Diagnosed colitis 1964. Lost to follow up in C Lost to follow up before
1976. Presented with dysphagia and programmeanaemia in 1990. Colonoscopy at that timeshowed sigmoid polyp (cancer)
This table shows the year of diagnosis, age at diagnosis, sex, duration of disease, disease extent (method used), presentation, Dukes'sstaging, and patient group for each of the nine cancers found in association with ulcerative colitis between 1978 and 1990.
these developed an adenoma six years later,which was removed at colonoscopy and hasremained free of dysplasia since (6 years). Onepatient (patient C) who had low grade dysplasiain the distal descending and sigmoid colon wasfound to have high grade dysplasia in the sigmoidcolon at the next colonoscopy 14 months later. Atcolectomy two Dukes's A cancers were found;one in the sigmoid and one in the transversecolon. This patient was the only case of cancerdetected by the surveillance programme.Thus, follow up of patients with low grade
dysplasia found one cancer in 223 patient years.The Figure shows that 25% of patients withulcerative colitis exhibited low grade dysplasiaon at least one occasion by 17 years after diag-nosis of ulcerative colitis, 50% by 25 years, and75% by 38 years.
NON-CANCER SURGERYFifteen patients had colectomy for failed medicaltreatment after a mean of 15-6 years (range 9-32)disease duration. Nine had subtotal colectomy,six had panproctocolectomy. Four of thepatients who had low grade dysplasia previouslywere negative for dysplasia at colectomy. Twopatients who had been negative for dysplasia
were found to have low grade dysplasia in theircolectomy specimens.
CANCER COMPLICATING ULCERATIVE COLITISOUTSIDE THE SURVEILLANCE PROGRAMMEDuring the 12 year period there have been sevenother cases of colonic cancer in association withulcerative colitis at this centre. Two patients(patient B and patient H) were believed to havehad proctitis but were subsequently found tohave total colitis at colonoscopy with biopsy orhistological examination of the colectomy speci-men (one Dukes's B, one Dukes's C) (Table I).One patient (patient A) had several colonicpolyps removed endoscopically two years earlier.A barium enema performed at seven yearsdisease duration showed recurrent polyps.Colonoscopy was performed to remove thecolonic polyps and determine disease extent.Total colectom.y was performed because ofincomplete removal of a large tubular adenomawith intra-epithelial malignant change. Atcolectomy a Dukes's A cancer was found on abackground of total colitis. There were no otherareas of dysplasia (Table I). Four patients (D, F,G, and I) had been seen in the Leeds colitis clinicbefore the policy of surveillance had been started
1077

Lynch, Lobo, Sobala, Dixon, Axon
TABLE II Breakdown of12(11 published) studies on cancer surveillance in ulcerative colitis
Dukes's Dukes'sNo of Colonoscopies Dukes's AIB AIB
Year Author patients per patient >=C* excludef success4
1980 Fuson'° 75 1.1 4 7 01981 Blackstone22 112 1-5 2 4 01985 Rosenstock12 248 15 3 4 01988 Jones20 313 5 2 21988 Rutegard" 93 3-6 0 1 01989 Lashner2l 99 4-2 5 0 31990 Lennard-Jones22 344 2-4 8 13 11990 Lofberg2 72 440 0 1 11991 Nugent 213 ? 6 3 11991 Leidenius" 66 2-8 0 0 01992 Woolrich17 121 3-7 2 3 2Sub total 1756 35 38 101993 Lynch 160 4-3 5 3 1Total 1916 40 41 11
*Patients found to have cancer, but stage Dukes's C or worse. tPatients found to have Dukes's A/Bcancer, but not as part of the colonoscopic surveillance policy detailed in the discussion.tPatients found to have cancer as part of surveillance programme.
and were lost to follow up. They re-presentedduring the surveillance period with new symp-toms.
CANCER SURGERYThus, altogether, there were nine cases ofcoloniccancer in association with ulcerative colitis at thiscentre over this time period (Table I); mean age46-4 years (range 33-62), mean disease duration18-2 years (range 7-26), six men. Six patientsdeveloped cancer under the age of fifty. Sevenpatients had total colectomy (three Dukes's A,one Dukes's B, three Dukes's C). One patient(patient F) who had been lost to follow up, hadan anterior resection for a rectal carcinoma (oneDukes's C). Because of the high risk of develop-ing a further cancer the patient was entered intothe surveillance programme. Three subsequentcolonoscopies have been negative for dysplasia.
Therefore, of 180 patients eligible for coloniccancer surveillance in ulcerative colitis 160 wereentered into the programme. During the 12 yearperiod 1978-1990 nine colonic cancers werefound in association with ulcerative colitis, butonly one was detected by the surveillance pro-gramme.
DiscussionMany gastroenterologists consider that patientswith ulcerative colitis with longstanding, exten-sive disease should have annual colonoscopy andbiopsy to detect dysplasia or early cancer. Ifhighgrade dysplasia or carcinoma is detected thepatient can be treated at an early stage.
It is important to define what is 'success' andwhat is 'failure' in a surveillance programme toallow critical analysis of the outcome. An early
cancer - that is, Dukes's A or B found as a resultof the programme represents a success. ADukes's C cancer or worse should be regarded a
failure of surveillance because of the uncertainoutlook.
It is also important to consider the method ofcancer detection when reviewing the results of a
surveillance policy. The generally acceptedsurveillance policy in most centres today isregular colonoscopy for patients with long-standing extensive colitis. If this definition isapplied when reviewing surveillance studies theresult is that cancers found earlier than eightyears from onset or found in left sided colitis or acancer found at colonoscopy performed for any
reason other than surveillance (such as rectalbleeding), cannot be regarded as a success.Colorectal cancer presenting as an abdominalmass or perforation,2021 cancers found on
sigmoidoscopy and barium enema,2022 or colono-scopy performed because of an abnormal bariumenema'0 12 22 23 are outside protocols that use
regular colonoscopic examination as the surveil-lance technique.
Similarly, if a cancer is found at a screeningcolonoscopy in a patient presenting to a unityears after the programme entry date forexample, colitis of 17 years duration or whenreferred from another centre8 1022 24 it cannot becounted a success becaue these cancers representa selected group detected outside the regularsurveillance protocol. Cancers found at surgery
performed for reasons other than high gradedysplasia or early carcinoma, such as debility or
failed medical treatment,'222 or low grade dys-plasia,81223 (not a generally recognised indicationfor surgery) cannot be counted as successes ofthesurveillance policy either.
Applying these criteria to our results, one ofnine colonic cancers that arose in associationwith ulcerative colitis during the surveillanceperiod was detected by the surveillance pro-
gramme. Analysis of 12 published studies ofcolonoscopic surveillance programmes (TablesII and III) shows that 93 cases of colonic cancer
were found. Twelve (13%) of these representsuccesses for the colonoscopic surveillance pro-grammes - that is, Dukes's A/B cancers detectedby regular colonoscopic surveillance.
It could be argued that these criteria are toorigid. Some surveillance programmes entailroutine clinical follow up, regular sigmoido-scopy, and barium enema examination as wellas regular colonoscopy and biopsy.22 Thesemethods of cancer detection are equally valid ifthey are laid down as part of a surveillanceprotocol. Also, cancers found at the screening(first) colonoscopy may be regarded as a success
TABLE III Ulcerative colitis surveillance papers (amalgamated results of1916 patients). Method ofcancer diagnosis
Mass/ Colonoscopyperforation. Barium Operation for without entry
Dukes's Other signsl Barium enema! enema leading Operation or low grade criteria Screen Surveillancestage symptoms sigmoidoscopy to colonoscopy necropsy dysplasia fulfilled colonoscopy colonoscopy
>=C 13 10 5 1 1 2 8B 6 5 5 2 1 5A 4 2 6 3 7 6
Of the 1916 patients from the 12 studies, 92 cancers were found.This table indicates the Dukes's staging and the method of diagnosis of the colonic cancers.
1078

Failure ofcolonoscopic surveillance in ulcerative colitis
when the examination is performed according tothe protocol. Adopting this approach thenumber of successes in the 12 published studiesis 24 (26%).A workable surveillance programme requires
defined entry criteria and a cheap simple test,which is acceptable to the patient and which hasa sound discriminatory basis.25 Current surveil-lance colonoscopy programmes in ulcerativecolitis fall short in a number of ways.There are no universally accepted entry
criteria for cancer surveillance.26-28 There is ageneral feeling in published studies that colitisextending beyond the splenic flexure can beregarded as extensive in terms of cancer risk.2Assessment of extent, however, may be bybarium enema, colonoscopy or both. Bariumstudies seem to be insensitive to microscopicinvolvement29 and may detect only more severecases. In our study two patients were originallydiagnosed as having proctitis. Ifcolonoscopy hadbeen done the extensive nature of the diseasemight have been recognised and the patientwould have entered the programme. Colitis forat least eight years is considered to be long-standing. In this series, however, one patientdeveloped cancer after seven years diseaseduration so perhaps the criteria for entry shouldbe widened.
Colonscopic surveillance programmes cause aheavy clinical workload as well as a substantialcapital outlay'9 20 - that is, the test is not simple orcheap.
Patient recruitment is a recognised problem;12% were not recruited into our programme.Some were lost to follow up from clinic beforefulfilling the entry criteria for longstandingdisease; others despite being eligible, were notentered. Once recruited, patients had a regular,uncomfortable examination that requires a dayoff work. In our study four patients refusedcolonoscopy, and 41 (27%) patients defaultedfrom the programme - strong evidence thatannual colonoscopy is unacceptable to many.There are problems with the discriminatory
power of colonoscopy and biopsy. Colonicepithelial dysplasia is patchy.303' Multiplebiopsies sample much less than 1% ofthe surfacearea of the colon. The evidence for the associa-tion of dysplasia and cancer is conflicting.Twenty to fifty per cent of cancers are thought toarise de novo.32 I Fozard et al found a weakassociation between colon cancer and distantdysplasia.33 By contrast two other studies con-clude that the association is invariable.234 Thehistological interpretation of biopsy specimensand diagnosis of dysplasia is fraught with theproblems of inter and intraobserver variation35 36- that is, the diagnostic test does not have a sounddiscriminatory basis. The histological recogni-tion of dysplasia is the very cornerstone ofsurveillance yet it would seem that the process oftissue collection to final diagnosis is susceptibleto a number of pitfalls.
It can be argued that the finding of high gradedysplasia without cancer should be considered tobe a success of surveillance. This argument is notstraightforward. The diagnosis of dysplasia isbeset with problems, as discussed above,furthermore the significance and outcome of
high grade dysplasia is unpredictable. Coloncancer was found in 25% of patients with highgrade dysplasia but another 25% had a negativecolectomy specimen or colonoscopy on followup.22 In another study while 33% of patients withhigh grade dysplasia developed cancer within sixyears 33% were not operated on and were aliveand well five years later so not all authors haveadvised operation even when high grade dys-plasia has been diagnosed.'° 12 15 Low grade dys-plasia was a common finding in ulcerative colitissurveillance in our study and in others2' and haslittle prognostic significance.
All but one of the colorectal cancers in thisseries occurred in patients outside the surveil-lance programme. This experience is notunique.2022 This cannot be construed as acriticism of the surveillance protocol itself. Onlyone of these patients had been recruited and hadthen defaulted. We are not aware of any exten-sive cancer arising in patients who had regularsurveillance colonoscopy. It is apparent, how-ever, that a number of patients who neededsurveillance did not receive it. It is probable thatthese individuals were well and asymptomatic orhad minimal symptoms. This might explain whythey did not attend for clinical review. A reviewof the notes of our cancer patients suggests thatvirtually none of them were taking disease sup-pressant drugs, such as salazopyrin, regularly orat all. It may be that unsuppressed inflammation,while causing few or no symptoms, places thesepatients at increased risk of developing coloniccancer.The main criticism that can be levelled at our
study (and those in published works) is that thefinding of one patient with high grade dysplasia(and carcinoma) does not justify the greatexpense and the effort for staff and patientsinvolved in 739 colonscopies and 709 years offollow up. In 10 of 12 surveillance studies it ispossible to calculate the number ofcolonoscopiesperformed and the number of early cancersdetected by them. Including this study eightearly cancers were found by colonoscopicsurveillance and 3807 colonoscopies were per-formed: one cancer per 476 examinations.
There are 38 deaths per 100 00037 fromcolorectal cancer annually in the UnitedKingdom. As nearly all of these occur in the40-80 age group (and not everyone withcolorectal cancer dies of it) the annual incidencein this group is greater than 38 per 50 000.37 If,therefore, the normal population in this agegroup was screened at five year intervals, andassuming that the polyp/carcinoma sequencetakes longer than five years, 190 cases of canceror premalignant polyp would be found per50000 examinations - that is, 1 in 263: a higherdetection rate in the normal population than thatachieved.by annual colonoscopic surveillance ofextensive longstanding ulcerative colitis. In arecent study colonoscopy was performed on 210asymptomatic subjects aged 50-75 years withnegative faecal occult bloods. Two Dukes's Acancers were detected giving a yield ofone cancerper 105 colonoscopies.38We conclude that in our experience annual
colonoscopic surveillance for cancer has beenunsuccessful; eight of nine colonic cancers
1079

1080 Lynch, Lobo, Sobala, Dixon, Axon
occurred in ulcerative colitis patients not havingsurveillance. Our results and a review of pub-lished works cast doubts on the value of annualcolonoscopic surveillance in this condition whenconsidering its cost effectiveness and the defini-tion of a workable programme.24
Lashner et al39 monitored two groups of 90patients with longstanding, extensive ulcerativecolitis, one with regular colonoscopy, the otherwith regular clinical follow up. There was nodifference in the cancer detection rate. Thoughthe numbers affected are small colonoscopicbiopsy and histological examination for dysplasiaseems to hold no advantage over routine clinicalmanagement.How then should we manage these patients
who are known to be at an increased risk ofdeveloping cancer?The published data show that most cancers are
detected as a result of clinical follow up, wherenew symptoms are investigated at an early stage.Many cancers were found in patients who haddefaulted the clinic before they were eligible forsurveillance returning with new symptoms yearslater. 'Screening' colonoscopy (as opposed to'surveillance' colonoscopy) detected a number ofcancers.
All patients with ulcerative colitis should bescreened at eight years. This will allow themto be assessed microscopically as 'total','extensive', or 'left sided' providing importantinformation about their cancer risk. All patientswith colitis should be followed up indefinitely. Itis difficult to justify regular colonoscopy there-after.
Clinicians faced with a patient with longstand-ing colitis, at increased risk ofdeveloping coloniccancer, feel compelled to do, or be seen to do,something. There is also an obligation, however,to use effective methods. The argument forcolonoscopic surveillance is not convincing.While it has been deemed unethical to perform acontrolled clinical trial, it could be argued thatthe use of limited resources on surveillanceprogrammes of unproved value is also unethical.The funds released by ending surveillance areconsiderable. They could be channelled into amore cost effective cancer prevention scheme. Itis time to review cancer surveillance in ulcerativecolitis.
We would like to thank Mrs Olive Bell, Miss Julie Mackintosh andMrs Andrea Scales for their help in the preparation and typing ofthis paper.These data were published in abstract form in Gut 1991; 32:
A556 and A561.
1 Crohn BB, Rosenberg H. The sigmoidoscopy picture ofchronic ulcerative colitis (non-specific). Amj Med Sci 1925;170: 220-8.
2 Gyde SN, Prior P, Allan RN, Stevens A, Jewell DP, TrueloveSC, et al. Colorectal cancer in ulcerative colitis: a cohortstudy of primary referrals from three centres. Gut 1988; 29:206-17.
3 de Dombal FT, Watts JMcK, Watkinson G, Goligher JC.Local complications of ulcerative colitis: stricture, pseudo-polyposis, and carcinoma of the colon and rectum. BMJr1966; 1: 1442-7.
4 Devroede GJ, Taylor WF, Sauer WG, Jackman RJ, SticklerGB. Cancer risk and life expectancy of children withulcerative colitis. NEnglJMed 1971; 285: 17-21.
5 Kewenter J, Ahlrnan H, Hulten L. Cancer risk in extensivecolitis. Ann Surg 1987; 188: 824-7.
6 MacDougal 1PM. The cancer risk in ulcerative colitis. Lancet1964; ii: 655-8.
7 Morson BC, Pang LSC. Rectal biopsy as an aid to cancercontrol in ulcerative colitis. Gut 1967; 8: 423-34.
8 Nugent FW, Haggit RC, Gilpin PA. Cancer surveillance inulcerative colitis. Gastroenterology 1991; 100: 1241-8.
9 Dickinson RJ, Dixon MF, Axon ATR. Colonoscopy and thedetection of dysplasia in patients with longstanding ulcera-tive colitis. Lancet 1980; ii: 620-2.
10 Fuson JA, Farmer RG, Hawk WA, Sullivan BH. Endoscopicsurveillance for cancer in chronic ulcerative colitis. Am JGastroenterol 1980; 73: 120-6.
11 Lennard Jones JE, Morson BC, Ritchie JK, Williams C.Cancer surveillance in ulcerative colitis: experience over 15years. Lancet 1983; ii: 149-52.
12 Rosenstock E, Farmer RG, Petras R, Sivak MV, Rankin GB,Sullivan BH. Surveillance for colonic carcinoma in ulcera-tive colitis. Gastroenterology 1985; 89: 1342-6.
13 Brostrom 0, Lofberg R, Ost A, Reichard H. Cancer surveil-lance of patients with longstanding ulcerative colitis: aclinical, endoscopical, and histological study. Gut 1986; 27:1408-13.
14 Manning AP, Bulgim OR, Dixon MF, Axon ATR. Screeningby colonoscopy for colonic epthelial dysplasia in inflamma-tory bowel disease. Gut 1987; 28: 1489-94.
15 Rutegard J, Ahsgren L, Stenling R, Janunger KG. Ulcerativecolitis. Cancer surveillance in an unselected population.ScandJ Gastroenterol 1988; 23: 139-45.
16 Leidenius M, Killokumpu I, Husa A, Riitula M, Sipponen P,Dysplasia and carcinoma in longstanding ulcerative colitis:an endoscopic and histological surveillance programme. Gut1991; 32: 1521-5.
17 Woolrich AJ, DaSilva MD, Korelitz BI. Surveillance in theroutine management of ulcerative colitis: the predictivevalue of low-grade dysplasia. Gastroenterlogy 1992; 103:431-8.
18 Gyde S. Screening for colorectal cancer in ulcerative colitis:dubious benefits and high costs. Gut 1990; 31: 1089-97.
19 Collins RH, Feldman M, Fordtran JS. Colon cancer, dys-plasia, and surveillance in patients with ulcerative colitis. Acritical review. N EnglJ Med 1987; 316: 1654-8.
20 Jones HW, Grogono J, Hoare AM. Surveillance in ulcerativecolitis: burdens and benefit. Gut 1988; 29: 325-31.
21 Lashner BA, Silverstein MD, Hanaver SB. Hazard rates fordysplasia and cancer in ulcerative colitis. Dig Dis Sci 1989;34:1536-41.
22 Lennard-Jones JE, Melville DM, Morson BC, Ritchie JK,Williams CB. Precancer and cancer in extensive ulcerativecolitis: findings among 401 patients over 22 years. Gut 1990;31: 800-6.
23 Blackstone MO, Riddell RH, Rogers BHG, Levin B.Dysplasia-associated lesion or mass (DALM) detected bycolonoscopy in longstanding ulcerative colitis: an indicationfor colectomy. Gastroenterology 1981; 80: 366-74.
24 Lofberg R, Brostrom 0, Karlen P, Tribukait B, Ost A.Colonoscopic surveillance in longstanding total ulcerativecolitis - a 15 year follow-up study. Gastroenterology 1990; 99:1021-31.
25 Weil J, Langman MJS. Screening for gastrointestinal cancer:an epidemiological review. Gut 1991; 32: 220-4.
26 Lennard Jones JE, Morson BC, Ritchie JK, Shove DC,Williams CB. Cancer in colitis: assessment of the individualrisk by clinical and histological criteria. Gastroenterology1977; 73: 1280-9.
27 Anonymous. Colorectal carcinoma in ulcerative colitis[Editorial]. Lancet 1986; ii: 197-8.
28 Morson BC. Precancer and cancer in inflammatory boweldisease. Pathology 1985; 17: 173-80.
29 Lennard-Jones JE. Compliance, cost, and common sense limitcancer control in colitis. Gut 1986; 27: 1403-7.
30 Ransohoff DF, Riddell RH, Levin B. Ulcerative colitis andcolonic cancer: problems in assessing the diagnostic useful-ness of mucosal dysplasia. Dis Colon Rectum 1985; 26:382-8.
31 Cook MG, Goligher JC. Carcinoma and epithelial dysplasiacomplicating ulcerative colitis. Gastroenterology 1975; 68:1127-36.
32 Riddell RH. The precarcinomatous phase of ulcerative colitis.Curr Top Pathol 1976; 63: 179-219.
33 Fozzard JBJ, Griffiths SB, Dixon MF, Axon ATR, Giles GR.Lectin and mucin histochemistry as an aid to cancersurveiliance in ulcerative colitis. Histopathology 1987; 11:385-94.
34 Cuvelier CA, Morson BC, Roels HJ. The DNA content incancer and dysplasia in chronic ulcerative colitis. Histo-pathology 1987; 11: 927-39.
35 Dixon MF, Brown CTR, Gilmore HM, et al. Observervariation in the assessment of dysplasia in ulcerative colitis.Histopathology 1988; 13: 385-97.
36 Melville DM, Jass JR, Shepherd NA, Northover JMA,Capellano D, Richman PI, et al. Dysplasia and deoxyri-bonucleic acid aneuploidy in the assessment of precancerouschanges in chronic ulcerative colitis. Observer variation andcorrelations. Gastroenterology 1988; 95: 668-75.
37 Fielding LP, -Blesovsky L. Clinical features of colorectalcancer. In: Misiewicz JJ, Pounder RE, Venables CW, eds.Diseases of the gut and pancreas. Oxford: Blackwell ScientificPublications, 1987.
38 Rex DK, Lehman GH, Hawes RH, Ulbright TM, Smith JJ.Screen colonoscopy in asymptomatic average - risk personswith negative occult blood tests. Gastroenterology 1991; 100:64-7.
39 Lashner BA, Kane SV, Hanauer SB. Colon cancer surveillancein chronic ulcerative colitis: historical cohort study.AmJ Gastroenterol 1990; 85: 1083-7.