Embed Size (px)
Citation preview
INTRODUCTION
DESPITE MANY RECENT ADVANCES in the man-agement of infectious diseases, intra-ab-
dominal infection remains an important chal-lenge for the surgeon. These infections can stillcause substantial mortality and morbidity, es-pecially for some patient subgroups. Althoughantimicrobial therapy is important for pre-venting or managing abscesses, it cannot standalone. Prompt recognition, early localization,and effective drainage are essential for effectivetreatment of a patient with an intra-abdominal
abscess [1,2]. This article reviews imaging tech-niques that are used to aid in the diagnosis andlocalization of intra-abdominal abscess and dis-cusses appropriate antimicrobial therapy anddrainage techniques aimed at controlling theseinfections.
The abscess environment
The etiology of intra-abdominal abscessesvaries according to the source of the infectionand the status of the patient’s immune system.Many intra-abdominal abscesses are polymi-
SURGICAL INFECTIONSPremier IssueVolume 1, Number 1, 2000Mary Ann Liebert, Inc.
Diagnosis and Treatment of Intra-Abdominal Abscesses
KENNETH R. SIRINEK
ABSTRACT
Despite recent advances in the diagnosis and management of intra-abdominal abscesses, theseinfections still cause substantial morbidity and mortality. Low pH, large bacterial inocula,poor perfusion, the presence of hemoglobin, and large amounts of fibrin (which impedes an-tibiotic penetration) make the abscess a cloistered environment that is penetrated poorly bymany antimicrobial therapies. Therefore, management of these infections requires promptrecognition, early localization, and effective drainage, as well as appropriate antimicrobialuse. Although various imaging techniques, such as ultrasonography, gallium scans, and in-dium-labeled white-blood-cell scans, can be used for the diagnosis and localization of intra-abdominal abscesses, computer-assisted tomography is the most useful study. Once the di-agnosis is made and the abscess is localized, treatment should begin promptly. Percutaneousor open surgical drainage should be used. Broad-spectrum antibiotics should be given untilculture and sensitivity data are obtained. Once these data are obtained, a therapy with ap-propriate coverage that is likely to work in the abscess environment should be chosen. Per-cutaneous drainage is inappropriate for abscesses in the posterior subphrenic space or in theporta hepatis, for those among loops of small bowel, for suspected echinococcal cysts, and forabscesses containing necrotic or neoplastic tissues. Finally, surgeons need to be cognizant ofrisk factors, such as advanced age, obesity, complex abscesses, and high Acute Physiologyand Chronic Health Evaluation (APACHE) II or APACHE III scores, which correlate with pooroutcomes for these patients.
Department of Surgery, University of Texas Health Science Center at San Antonio, San Antonio, TX.
31

32 SIRINEK
crobial, although anaerobic gut organisms suchas Bacteroides often predominate [3–5]. The ab-scess environment often presents special chal-lenges for antimicrobial therapy [6]. Abscesseshave a low oxidation-reduction potential andlow pH as a consequence of limited vascular-ity and poor perfusion, anaerobic conditions,and dying tissue. High bacterial concentrationstend to depress oxygen-dependent phagocyto-sis and killing of bacteria by neutrophils andsuffuse the confined space with high concen-trations of b -lactamase enzymes. Antibioticpenetration into the abscess is limited not onlyby poor perfusion but also by mechanical bar-riers such as fibrin clots and the abscess wall[7–9]. Thus, treatment with antimicrobial ther-apy alone is usually insufficient to clear theseinfections—effective management requires ab-scess drainage.
DIAGNOSIS AND LOCALIZATION
Intra-abdominal infection should be sus-pected immediately in a patient who is at riskand who has the hallmark signs—tachycardia,tachypnea, leukocytosis, and cyclic or constanttemperature elevation characteristic of a sys-temic proinflammatory response [1]. The initialevaluation should include a history, physicalexamination, laboratory tests, plain roentgeno-grams of the chest and abdomen, and appro-priate cultures. The physical examinationshould not be omitted because a palpable massmay be found that indicates the presence of anabscess [10]. On plain films, one might find apleural effusion, atelectasis, elevated hemidi-aphragms, free intraperitoneal air, ileus, or dis-placed viscera. If a mass effect is identified ona plate the diagnostic challenge is to differen-tiate an abscess from a true cyst, biloma, loopsof bowel, lymphocele, or urinoma [11].
Diagnostic imaging systems can be helpfulin establishing the correct diagnosis. However,any imaging system has limitations that cangive rise to false-positive and/or false-negativeresults. For patients with an intra-abdominalabscess, such inaccuracies may lead to seriousconsequences—uncontrolled sepsis with its as-sociated high mortality (false negatives) or un-
necessary operations (false positives) in criti-cally ill patients. Therefore, it is important tochoose an imaging method that can identifyand localize an abscess effectively while ex-cluding the possibility that other lesions or col-lections may be present.
Ultrasonography
Ultrasonography is a relatively sensitive anduseful tool for diagnosing an intra-abdominalabscess. Ultrasonography is noninvasive anddoes not require exposing patients to ionizingradiation. Because ultrasonography is portable,it can be brought to very ill patients who arenot easily transported [12]. However, becauseultrasonography is not fully automated, its ac-curacy is user-dependent [13]. It is less accu-rate than computed tomography (CT), less ca-pable of detecting small abscesses, and canmiss an infected focus in the retroperitonealarea [1]. The utility of ultrasonography may beaffected adversely by the size of the patient orthe presence of surgical wounds, dressings,drains, and ostomies that may prevent imag-ing of all areas of the abdomen and pelvis.Large amounts of bowel gas (e.g., ileus) can ob-scure underlying structures. Several studiesthat were undertaken to determine the sensi-tivity and specificity of ultrasonography for di-agnosing intra-abdominal sepsis are summa-rized in Table 1.
Computed tomography
Although ultrasound is somewhat useful,most surgeons rely on CT, which provides highanatomic resolution and has greater specificitythan does ultrasonography [13]. Compared toultrasonography, a CT scan allows better visu-alization of the retroperitoneum, lesser sac, andpelvis. Contrast enhancement may help to dif-ferentiate between a loop of intestine and afluid collection, but administration may be lim-ited by clinical factors (e.g., allergy or renal fail-ure for intravenous contrast, ileus for oral con-trast). Although the presence of debris,loculations, gas, and a contrast-enhanced rimsuggest the presence of an infection, a CT scancannot differentiate between sterile and in-fected fluid collections. A CT scan may not be

INTRA-ABDOMINAL ABSCESSES 33
an option for critically ill patients who are dif-ficult to transport to the area of the hospitalwhere the scanner is located or for those whoare morbidly obese and may not fit on thegantry [12]. However, portable CT scan equip-ment now allows the instrument to be broughtto the bedside. It remains to be determined ifthe image quality in portable CT scan equip-ment will be adequate for imaging the ab-domen. Studies examining the use of CT for in-tra-abdominal abscess are also summarized inTable 1.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) has sev-eral limited advantages over CT scanning inpatients with intra-abdominal infection. MRIcan delineate better the extent of an abscess andthe presence of a capsule [14]. Compared toother imaging techniques, MRI will also clearlyshow the impact of an abscess on adjacentstructures, especially muscle and major blood
vessels. However, image quality is susceptibleto motion artifact, which cannot be avoidedwhen imaging the abdomen with MRI. More-over, it is cumbersome to take even a hemo-dynamically stable intensive care unit patientfor an MRI scan because nonferrous materialsare mandatory for clinical accouterments, suchas mechanical ventilators and infusion pumps.
Scintigraphy
Radioactive gallium (67Ga citrate) concen-trates in infected sites but is not very useful forlocalizing an intra-abdominal abscess becausethis substance accumulates in the intestine,liver, and spleen, causing a high backgroundof radiation [15]. In addition, gallium is con-centrated and excreted in feces, increasing thelikelihood of a false-positive interpretation.Moreover, scintigraphy delays diagnosis, be-cause 48 hours are generally required for studyresults and interpretation [13]. The literature ismixed regarding the sensitivity of this scan.
TABLE 1. STUDIES ASSESSIN G THE UTILITY OF ULTRASONOGRAPHY AND COMPUTED
TOMOGRAPHY FOR DIAGNOSIS OF INTRA-ABDOM INAL INFECTION
Patients Sensitivity Specificity AccuracyAuthor (year) (#) (%) (%) (%)
UltrasonographyTaylor et al. (1978) a 220 93.5 99.5 97Knochel, et al. (1980)b 123 82.5 94.5 90
(136 examinations)Butler, et al. (1987) c 21 — — 72Weldon, et al. (1995)d 50 71.5 87.5 —
Computed tomographyButler, et al. (1987) c 11 — — 82Haaga, et al. (1977) e 17 — — 91Knochel, et al. (1980)b 74 97.5 95.5 96
(80 studies)Wolverson, et al. (1979) f — 95.5 94.5 —
— 5 Not reported.aTaylor KJ, Wasson JF, De Graaf C, et al. Accuracy of grey-scale ultrasound diagnosis of abdominal and pelvic ab-
scesses in 220 patients. Lancet 1978;i:83–84.bRef. 20.cRef. 36.dWeldon MJ, Joseph AEA, French A, et al. Comparison of 99mTechnetium hexamethylpropylene-amine oxime la-
belled leucocyte with 111-Indium tropolonate labelled granulocyte scanning and ultrasound in the diagnosis of intra-ab-dominal abscess. Gut 1995;37:557– 564.
eHaaga JR, Alfidi RJ, Havrilla TR, et al. CT detection and aspiration of abdominal abscesses. Am J Roentgenol1977;128:465– 474.
fWolverson MK, Jagannadharao B, Sundaram M, et al. CT as a primary diagnostic method in evaluating intraabdom-inal abscess. Am J Roentgenol 1979;133:1089– 1095.
34 SIRINEK
Sensitivity has been reported as low as 59%[16], although a large-scale review showed gal-lium to have high sensitivity and specificity[17]. In one study of 50 patients, gallium wasfound to have a 63% sensitivity and 94% speci-ficity [18]. Another study showed a sensitivityand a specificity of more than 90% for galium[19].
Indium (111In)-labeled leukocytes are gener-ally more accurate than gallium in labeling sitesof inflammation. Still, the liver and spleen nor-
mally accumulate these cells in high concen-trations, leading to high background radiationand consequent difficulty in detecting an up-per-abdominal abscess [15]. Labeled leuko-cytes are not as sensitive as a CT scan in iden-tifying an intra-abdominal abscess. A studycomparing labeled leukocytes, CT scan, andultrasonography found a sensitivity of 86% forlabeled leukocytes, 82% for ultrasonography,and 98% for CT [20]. Tumor uptake can alsobe a problem. However, the use of labeled
A
B
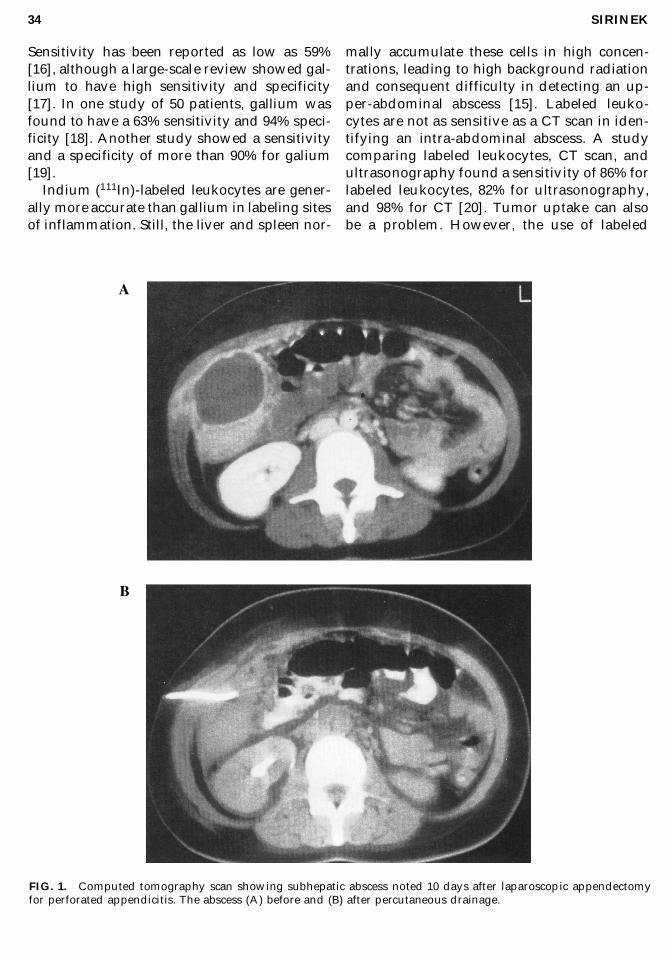
FIG. 1. Computed tomography scan showing subhepatic abscess noted 10 days after laparoscopic appendectomyfor perforated appendicitis. The abscess (A) before and (B) after percutaneous drainage.
INTRA-ABDOMINAL ABSCESSES 35
cells has some advantages. Although ultra-sonography and CT cannot differentiate be-tween infected and noninfected fluid collec-tions, labeled leukocytes only accumulate insites of active infection or inflammation [15].Use of indium-labeled leukocytes has the ad-ditional advantage of allowing identificationof extra-abdominal infections [15], which arenot uncommon in patients with signs andsymptoms suggesting an intra-abdominalprocess. For pyrexia of unknown origin, a se-ries of 166 labeled white-blood-cell studiesfound a sensitivity of 60% and a specificity of70% [21].
TREATMENT
Effective management of intra-abdominalabscesses requires both appropriate antibiotictherapy and surgical drainage.
Choice of antibiotic
Initial therapy should consist of broad-spec-trum antibiotics until culture and antibioticsensitivity results are available. Because thepathogens are frequently similar to those in-volved in secondary peritonitis, it is rational todirect initial therapy against Bacteroides fragilis
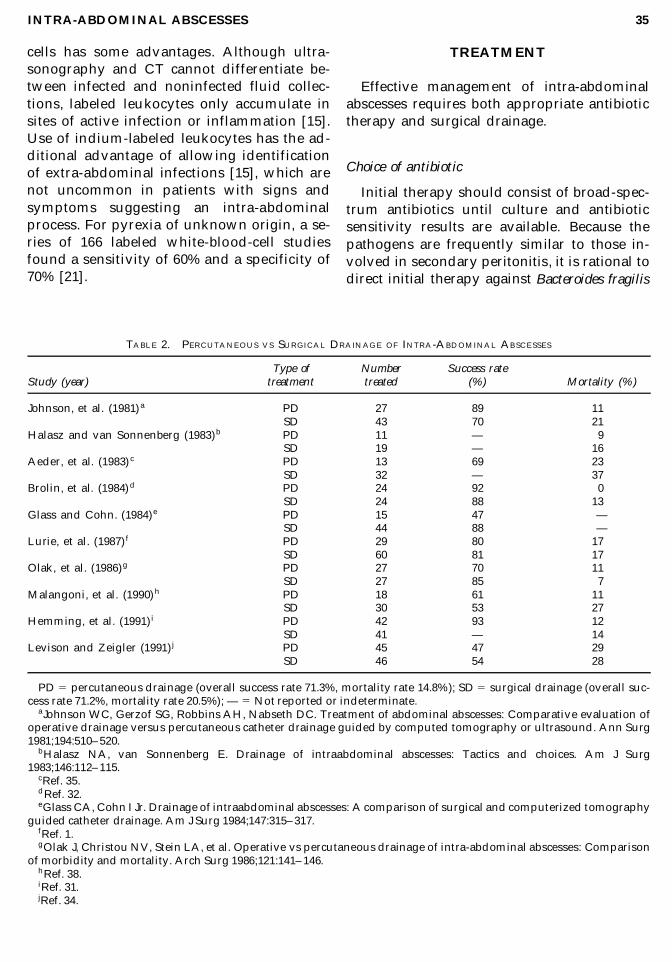
TABLE 2. PERCUTANEOUS VS SURGICAL DRAINAGE OF INTRA-ABDOMINAL ABSCESSES
Type of Number Success rateStudy (year) treatment treated (%) Mortality (%)
Johnson, et al. (1981) a PD 27 89 11.5SD 43 70 21.5
Halasz and van Sonnenberg (1983)b PD 11 — 9.5SD 19 — 16.5
Aeder, et al. (1983) c PD 13 69 23.5SD 32 — 37.5
Brolin, et al. (1984)d PD 24 92 0.5SD 24 88 13.5
Glass and Cohn. (1984)e PD 15 47 —SD 44 88 —
Lurie, et al. (1987) f PD 29 80 17.5SD 60 81 17.5
Olak, et al. (1986)g PD 27 70 11.5SD 27 85 7.5
Malangoni, et al. (1990)h PD 18 61 11.5SD 30 53 27.5
Hemming, et al. (1991) i PD 42 93 12.5SD 41 — 14.5
Levison and Zeigler (1991) j PD 45 47 29.5SD 46 54 28.5
PD 5 percutaneous drainage (overall success rate 71.3%, mortality rate 14.8%); SD 5 surgical drainage (overall suc-cess rate 71.2%, mortality rate 20.5%); — 5 Not reported or indeterminate.
aJohnson WC, Gerzof SG, Robbins AH, Nabseth DC. Treatment of abdominal abscesses: Comparative evaluation ofoperative drainage versus percutaneous catheter drainage guided by computed tomography or ultrasound. Ann Surg1981;194:510– 520.
bHalasz NA, van Sonnenberg E. Drainage of intraabdominal abscesses: Tactics and choices. Am J Surg1983;146:112– 115.
cRef. 35.dRef. 32.eGlass CA, Cohn I Jr. Drainage of intraabdominal abscesses: A comparison of surgical and computerized tomography
guided catheter drainage. Am J Surg 1984;147:315– 317.fRef. 1.gOlak J, Christou NV, Stein LA, et al. Operative vs percutaneous drainage of intra-abdominal abscesses: Comparison
of morbidity and mortality. Arch Surg 1986;121:141– 146.hRef. 38.iRef. 31.jRef. 34.

36 SIRINEK
and the Enterobacteriaceae [22]. The antimicro-bial regimen can be selectively revised once thecausative pathogens have been identified inculture [6].
Several antimicrobial regimens have beenused to treat patients with an intra-abdominalabscess. Previously, the most commonly usedtherapy was an aminoglycoside combinedwith either clindamycin or metronidazole [23].More recently, imipenem/cilastatin is amongmany drugs that have proved to be effectivefor this clinical problem [24]. However, basedon in vitro studies, imipenem and aminogly-cosides seem to lose some efficacy against B.fragilis at a reduced pH [25]. Piperacillin/tazobactam, as monotherapy, is also effectivefor treating patients with an intra-abdominalabscess because of the coverage of anaerobesin addition to broad gram-positive and gram-negative coverage [23,26]. Piperacillin/tazo-bactam also penetrates well into abdominal tissues [27] and works well at a low pH [28,29].
Drainage: open surgical vs. percutaneous
Two general approaches can be taken for ab-scess drainage: open surgical and percutaneoustechniques. Percutaneous drainage can beguided by CT or ultrasonography (Fig. 1). CT-assisted drainage has the advantage of high-quality imaging of abscesses and of surround-ing tissues; ultrasound offers dynamic imagingduring the puncture process, which may be im-portant for small abscesses that move duringbreathing [30]. In addition, preoperative per-cutaneous drainage of diverticular abscessesmay allow a patient to undergo just one surgi-cal procedure (subsequent sigmoid resectionwith primary anastomosis) rather than twoduring the same hospitalization [31].
While the relative success rates of percuta-neous and open surgical drainage are quitesimilar (Table 2), not all abscesses should bedrained by the less invasive percutaneousroute [32–34]. CT-assisted percutaneousdrainage has been recommended when thereare no more than two abscess cavities or loca-tions and when the drainage route does not tra-verse the bowel. Also, percutaneous drainage
is recommended for uncontaminated organsand spaces (peritoneal or pleural) and whenthere is an absence of a source of continuouscontamination [30,35]. Open surgical drainagemay appear to have a higher mortality rate(Table 2), but selection bias is always presentin nonrandomized trials of therapy for intra-abdominal infection.
Risk factors for complications
Most published analyses of risk factors havebeen performed retrospectively. Reviewingthese retrospective studies is difficult becausemost were conducted in patients who were notstratified by risk factors. Still, several importantrisk factors can be identified for morbidity andmortality. The number of surgical proceduresappears to influence risk: A 30% mortality ratehas been reported for patients who were un-dergoing multiple exploratory celiotomies forinfections (e.g., tertiary peritonitis) [36]. Deathsin patients with liver abscesses were related todelay in diagnosis, gram-negative sepsis at pre-sentation, and biliary origin of the abscess [37].Fry, et al. found that age greater than 50 years,multiple organ failure, a lesser sac abscess, sub-hepatic abscess, a blood culture that was posi-tive for the presence of infection, and recurrent,persistent, or multiple abscesses were each as-sociated with a fatal outcome [10]. Hemming,et al., in a review of 83 patients, found that highAcute Physiology and Chronic Health Evalua-tion (APACHE) II scores indicated an increasedrisk for the development of complications.APACHE II scores were significantly higher inthe nonsurvivors and in subjects who devel-oped complications in both treatment groups.There was, however, no significant differencein morbidity or mortality for patients treatedby percutaneous vs open surgical drainage[31]. Patients with complex abscesses (e.g.,multiple loculations, inaccessible locations) arealso at increased risk for complications [38]. Fi-nally, obesity is a complicating factor that im-pedes diagnosis as well as increasing morbid-ity [39].
Future studies should consider risk factorswhen comparing treatments for intra-abdomi-nal abscesses. In addition, continued refine-

INTRA-ABDOMINAL ABSCESSES 37
ment of imaging technology and greater un-derstanding of the abscess microenvironmentshould help surgeons to manage patients withintra-abdominal abscess appropriately.
REFERENCES
1. Lurie K, Plzak L, Deveney CW. Intra-abdominal ab-scess in the 1980s. Surg Clin North Am 1987;67:621–632.
2. Brismar B, Malmborg AS, Tunevall G, et al.Piperacillin-tazobactam versus imipenem-cilastatinfor treatment of intra-abdominal infections. Antimi-crob Agents Chemother 1992;36:2766– 2773.
3. Walker AP, Condon RE. Peritonitis and intraabdom-inal abscesses. In: Schwartz SI, ed. Principles ofSurgery, 5th ed. New York: McGraw-Hill; 1989,1479–1489.
4. Wilson SR, Arenson AM. Sonographic evaluation ofhepatic abscesses. J Can Assoc Radiol 1984;35:174–177.
5. Lorber B, Swenson RM. The bacteriology of intra-ab-dominal infections. Surg Clin North Am 1975;55:1349–1354.
6. Malangoni MA. Pathogenesis and treatment of intra-abdominal infection. Surg Gynecol Obstet 1990;171(suppl):S31–S34.
7. Hackford AW. Polymicrobial intraabdominal infec-tion: Medical/surgical therapy. Crit Care 1991;33–38.
8. Hau T, Jacobs DE, Hawkins NL. Antibiotics fail to pre-vent abscess formation secondary to bacteria trappedin fibrin clots. Arch Surg 1986;121:163– 168.
9. Tally FP. Factors affecting the choice of antibiotics inmixed infections. J Antimicrob Chemother 1988;22(suppl A):S87–S100.
10. Fry DE, Garrison RN, Heitsch RC, et al. Determinantsof death in patients with intra-abdominal abscess.Surgery 1980;88:517– 523.
11. Doust BD. The use of ultrasound in the diagnosis ofgastroenterological disease. Gastroenterology 1976;70:602–610.
12. McGahan JP, Anderson MW, Walter JP. Portable real-time sonographic and needle guidance systems for as-piration and drainage. Am J Roentgenol 1986;147:1241–1246.
13. Filly RA. Annual oration: Detection of abdominal ab-scesses. A combined approach employing ultra-sonography, computed tomography and gallium-67scanning. J Can Assoc Radiol 1979;30:202– 210.
14. Wall SD, Fisher MR, Ampara EG, et al. Magnetic res-onance imaging in the evaluation of abscesses. Am JRoentgenol 1985;144:1217– 1221.
15. Datz FL. Abdominal abscess detection: gallium, 111In,and 99mTc-labeled leukocytes, and polyclonal andmonoclonal antibodies. Semin Nucl Med 1996;26:51–64.
16. Froelich JW, Swanson D. Imaging of inflammatoryprocesses with labeled cells. Semin Nucl Med1984;14:128– 140.
17. Staab EV, McCartney WH. Role of gallium 67 in in-flammatory disease. Semin Nucl Med 1978;8:219–234.
18. Caffee HH, Watts G, Mena I. Gallium 67 citrate scan-ning in the diagnosis of intra-abdominal abscess. AmJ Surg 1977;133:665– 669.
19. Hopkins GB, Kan M, Mende CW. Gallium-67 scintig-raphy and intraabdominal sepsis: Clinical experiencein 140 patients with suspected intraabdominal ab-scess. West J Med 1976;125:425– 430.
20. Knochel JQ, Koehler PR, Lee TG, Welch DM. Diag-nosis of abdominal abscesses with computed tomog-raphy, ultrasound, and 111In leukocyte scans. Radiol-ogy 1980;137:425– 432.
21. Davies SG, Garvie NW. The role of indium-labelledleukocyte imaging in pyrexia of unknown origin. BrJ Radiol 1990;63:850– 854.
22. Levison ME, Bush LM. Peritonitis and other intra-ab-dominal infections. In: Mandell GL, Douglas RG Jr,Bennett JE, eds. Principles and Practices of InfectiousDiseases, 3rd ed. New York: Churchill Livingstone,1990:636– 670.
23. Eklund A-E, Nord CE. A randomized multicenter trialof piperacillin/tazobactam versus imipenem/cilas-tatin in the treatment of severe intra-abdominal in-fections. J Antimicrob Chemother 1993;31(supp l A):S79–S85.
24. Solomkin JS, Dellinger EP, Christou NV, Busuttil RW.Results of a multicenter trial comparing imipenem/cilastatin to tobramycin/clindamycin for intra-ab-dominal infections. Ann Surg 1990;212:581– 591.
25. Falagas ME, McDermott L, Snydman DR. Effect of pHon in vitro antimicrobial susceptibility of the Bac-teroides fragilis group. Antimicrob Agents Chemother1997;41:2047– 2049.
26. Polk HC Jr, Fink MP, Laverdiere M, et al. Prospectiverandomized study of piperacillin/tazobactam ther-apy of surgically treated intra-abdominal infection.Am Surg 1993;59:598– 605.
27. Sörgel F, Kinzing M. The chemistry, pharmacokinet-ics and tissue distribution of piperacillin/tazobactam.J Antimicrob Chemother 1993;31(supp l A):S39–S60.
28. Livermore DM, Corkill JE. Effects of CO2 and pH oninhibition of TEM-1 and other b -lactamases by peni-cillanic acid sulfones. J Antimicrob Chemother 1992;36:1870–1876.
29. Wistanley TG, Wilcox MH, Spencer RC. Effect of pHon antibiotics used to treat anaerobic infection [letter].J Antimicrob Chemother 1992;29:594– 595.
30. Treutner KH, Truong S, Klose K, et al. Intraabdominalabscesses–percutaneous catheter drainage versus oper-ative treatment. Klin Wochenschr 1989;67:486– 490.
31. Hemming A, Davis NL, Robins RE. Surgical versuspercutaneous drainage of intra-abdominal abscesses.Am J Surg 1991;161:593– 595.
32. Brolin RE, Nosher JL, Leiman S, et al. Percutaneouscatheter versus open surgical drainage in the treat-

38 SIRINEK
ment of abdominal abscesses. Am Surg 1984;50:102–108.
33. Bittner R, Block S, Büchler M, Beger HG. Pancreaticabscess and infected pancreatic necrosis: Different lo-cal septic complications in acute pancreatitis. Dig DisSci 1987;32:1082– 1087.
34. Levison MA, Zeigler D. Correlation of APACHE IIscore, drainage technique, and outcome in postoper-ative intra-abdominal abscesses. Surg Gynecol Obstet1991;172:89– 94.
35. Aeder MI, Wellman JL, Haaga JR, Hau T. Role of sur-gical and percutaneous drainage in the treatment ofabdominal abscesses. Arch Surg 1983;118:273– 280.
36. Butler JA, Huang J, Wilson SE. Repeated laparotomyfor postoperative intra-abdominal sepsis: An analysisof outcome predictors. Arch Surg 1987;122:702– 706.
37. Gyorffy EJ, Frey CF, Silva JJ, McGahan J. Pyogenicliver abscess: Diagnostic and therapeutic strategies.Ann Surg 1987;206:699– 705.
38. Malangoni MA, Shumate CR, Thomas HA, Richard-son JD. Factors influencing the treatment of intra-ab-dominal abscesses. Am J Surg 1990;159:167– 171.
39. Sugerman HJ. Surgical infection in the morbidlyobese patient. Infect Surg 1990;9:18– 30.
Address reprint requests to:Kenneth R. Sirinek, MD, PhD
Department of SurgeryUniversity of Texas Health Science Center at
San Antonio7703 Floyd Curl Drive
San Antonio, TX 78284-7842
E-mail: [email protected]







![Case Report Pelvic Primary Staphylococcal Infection ... · as abscesses in extra-abdominal locations [ ], including the ... psoas abscesses require correction of their underlying](https://img.dokumen.tips/doc/110x75/60f8ba0797237226e569ae63/case-report-pelvic-primary-staphylococcal-infection-as-abscesses-in-extra-abdominal.jpg)
![Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis · intra-abdominal and involving the small bowel mesentery [2]. TREATMENT Surgery Margin-negative resection has historically](https://img.dokumen.tips/doc/110x75/5e5a290071d21b380f5b7e74/intra-abdominal-and-abdominal-wall-desmoid-fibromatosis-intra-abdominal-and-involving.jpg)




















