Embed Size (px)
Citation preview

Diabetes: New drugs & Treatment ApproachDr G R Letchuman

Main message
• Patient as partner (his & her views) – diet, exercise, weight, drugs
• Use patient characteristics to decide the most appropriate therapies needed
• Test one therapy at a time for a reasonable period to gauge its efficacy and side effects
• Do not continue therapies that do not give appropriate efficacy or has unacceptable adverse events.
• Use combinations when needed to improve compliance
• Any improvement is still useful
Contents
• New drugs – crucial points
• Treatment Approach
• Few case studies



Glucose lowering drugs
Increase insulin
1. Sulphonylureas
2. Meglitinides
3. Insulin
Stimulate insulin @ hyperglycemia
1. DPP-IV inhibitors
2. GLP-1 agonist
3. Oral GLP-1 agonist*
Reduce resistence
• Biguanides
• Thiazolidinediones
Glucose lowering drugs
Delaying absorption
1. Alpha glucosidase inhibitors
Increase urinary loss
• SGLT-2 inhibitors

Dipeptidyl peptidase 4 (DPP-IV)inhibitor
• Inhibit degradation of GLP
• Excreted by kidneys (except linagliptin)
• Can be used in renal failure with reduced dose.
• Check kidney function before & then 6 monthly
• Hepatitis with vildagliptin and alogliptin. LFT pre and 3 monthly post in the 1st yr.
• No hypo or weight gain risk except in combination…
• May cause CHF by degradation of BNP. (SAVOR-TIMI 53 & EXAMINE)
• Adverse events: URTI. Do not start in patients with hx of heart failure and pancreatitis

DPP4 inhibitor CVOTs: baseline characteristics
10
Data are provided for the DPP4 inhibitor treatment arm. Mean values show unless otherwise indicated.
– indicates that the data are not reported.
*Median.
1. Scirica et al. N Engl J Med 2013;369:1317–26. 2. White et al. N Engl J Med 2013;369:1327–35. 3. Green et al. N Engl J Med 2015; DOI: 10.1056/NEJMoa1501352. 4. Marx et al. Diabetes Vasc Dis Res 2015;12:164–74. 5. NCT01897532.
SAVOR-TIMI 531 EXAMINE2 TECOS3 CAROLINA®4 CARMELINA®5
Mean age, years 65.1 61.0* 65.4 64.0 –
% with prior MI 38.0 87.5 42.7 13.8 –
% with prior HF 12.8 27.8 17.8 – –
% with prior CVD 78.4 – 73.6 34.5
Diabetes duration, y 10.3* 7.3* 11.6 6.2* –
HbA1c,% 8.0 8.0 7.2 7.2 –
Statin use, % 78.3 90.6 79.8 64.1 –
T2D therapy, %
Naive MetforminSUTZDInsulin
4.169.940.56.241.6
NaiveMetforminSUTZDInsulin
1.165.046.92.529.4
NaiveMonoDualTZDInsulin
–47.751.4–23.5
NaiveMonoDualTZDInsulin
9.266.023.8–Ex.
–

Glucagon-like Peptide-1 (GLP-1) agonist
• ↑ insulin in presence of hyperglycemia
• ↓ glucagon, gastric emptying, ↑satiety
• Nausea, vomiting
• 6 hours / 24 hours / 7 days
• No dose adjustment in renal impairment but no experience in ESRF

Glucagon-like Peptide-1 (GLP-1) agonist
• Weight loss, reduction in CV events as secondary prevention (LEADER, SUSTAIN-6, HARMONY, REWIND)
• CV death & death fr all causes by liraglutide (LEADER)
• Moderate effect on renal outcomes
• Useful for those who are overweight, risk of hypoglycaemia or who have CV event already
• Avoid in those with history of pancreatitis, personal of family hx of medullary carcinoma of thyroid or MEN


Sodium-glucose cotransporter (SGLT2) inhibitor
• Inhibit glucose reabsorption at proximal convoluted tubules
• No risk of hypoglycaemia unless in combination with ….
• Weight ↓. BP ↓ , CV events esp heart failure ↓ in patients with high risk of CV disease.
• ↓ progression of renal disease and delay the need for dialysis.
• Particularly good for those uncontrolled, overweight and has had CVD.
(EMPA – REG, CANVAS & DECLARE-TIMI 58)

SGLT2 inhibitors
Can cause a mild dehydration, thus be cautious:
• NSAIDs, ACE inhibitors/ARBs, diuretics.
• Hypovolemia, heart failure, liver injury.
• Predisposition to UTI
• Low BMD and high risk for fractures
• Avoid if eGFR) <60 mL/min (dapagliflozin, ertugliflozin) or <45 mL/min (canagliflozin, empagliflozin)
●Ketosis-prone type 2 diabetes

SGLT2 inhibitors
• Post exposure – renal function in 3 months initially.
• Use of empaglifozin 12.5mg?

SGLT2 inhibitors – side effects
• Vulvovaginal candidiasis : 9.5 versus 2.6 percent in the control groups
• Urinary tract infections (8.8 versus 6.1 percent)
In addition, the US Food and Drug Administration (FDA) has received reports of potentially fatal:
• Urosepsis and pyelonephritis
• Necrotizing fasciitis of the perineum (Fournier's gangrene)
• Reports of acute kidney injury (some requiring hospitalization and dialysis) in patients taking canagliflozin or dapagliflozin. Approximately one-half occurred within one month

SGLT2 inhibitors – side effects
• Bone fractures with canagliflozin (1.4 and 1.5 bone fractures per 100 patient-years exposure to canagliflozin 100 mg and 300 mg, respectively, compared with 1.1 per 100 patient-years in the comparator [placebo or active] group – not significant
• Greater loss of BMD over time
• "Euglycemic" (usually meaning plasma glucose < 14 mmol/l) diabetic ketoacidosis has been reported in patients with type 2 diabetes taking SGLT2 inhibitors
• Amputations - history of prior amputation, peripheral vascular disease, and neuropathy were at highest risk for amputation.
SGLT2 inhibitors
• More robust and consistent effects in prevention of heart failure and renal outcomes than on atherosclerotic CV events
Many drugs now for diabetes
• Confusing!

Genomic factors: > 40 independent loci demonstrating an association with an increased risk for type 2 diabetes identified. Some of them:• Decreased beta-cell responsiveness, leading to impaired insulin processing and decreased insulin secretion
(TCF7L2)
• Lowered early glucose-stimulated insulin release (MTNR1B, FADS1, DGKB, GCK)
• Altered metabolism of unsaturated fatty acids (FSADS1)
• Dysregulation of fat metabolism (PPARG)
• Inhibition of serum glucose release (KCNJ11) [18]
• Increased adiposity and insulin resistance (FTO and IGF2BP2) [19, 20]
• Control of the development of pancreatic structures, including beta-islet cells (HHEX) [21]
• Transport of zinc into the beta-islet cells, which influences the production and secretion of insulin (SLC30A8) [21]
• Survival and function of beta-islet cells (WFS1) [22]
• Susceptibility to type 2 diabetes may also be affected by genetic variants involving incretin hormones
• The high mobility group A1 (HMGA1) protein is a key regulator of the insulin receptor gene (INSR). [24]
• Functional variants of the HMGA1 gene are associated with an increased risk of diabetes

The Ominous Octet – Pathophysiology of T2DM
Islet b-cell
Islet a-cell
Adapted from: DeFronzo R et al. Diabetes. 2009;58:773–95.
Pathophysiology different but complications similar• Pathophysiology of the disease differs between the types of diabetes
but most of the complications, including microvascular, macrovascular, and neuropathic, are similar regardless of the type of diabetes.

Goals of treatment are as follows:
• Metabolic and neurologic risk reduction through control of glycemia
• Microvascular (ie, eye and kidney disease) risk reduction through control of glycemia and blood pressure
• Macrovascular (ie, coronary, cerebrovascular, peripheral vascular) risk reduction through control of lipids and hypertension, smoking cessation
The EASD/ADA position statement on management of T2DM1. Individualized glycemic targets and therapies
2. Diet, exercise, and education as the foundation of the treatment.
3. Use of metformin as the optimal first-line drug unless contraindicated
4. After metformin, the use of 1 or 2 additional oral or injectable agents, to minimize adverse effects.
5. Ultimately, insulin therapy alone or with other agents.
6. Where possible, all treatment decisions should involve the patient, i.e. patient preferences, needs, and values
7. A major focus on comprehensive cardiovascular risk reduction

Treatment Approach – Initial
1. Diet, Exercise, weight – talk about it each time, patients enjoy it as long as you are not judgemental, home glucose monitoring chart, weight chart
2. Go thro previous therapy and its effectiveness / side effects
3. Identify relevant characteristics : weight issues, complications, hypo risk, renal & liver function, past and family history, social background
4. Start drug therapy with metformin. Insulin if very symptomatic
Treatment approach – follow up
1. See after 3 months with HbA1c or
2. See earlier with home monitoring – pre and post prandial with food diary
3. Go thro actual drugs for compliance, weight, renal and liver function when needed, side effects
4. Make definite decisions with timelines. Decide targets together.
5. Stop therapy that does not work

PPG & FPG contribution at different HbA1c quintiles
50% 55% 60%70%
50% 45% 40%30%
30%
70%
< 7.3 7.3–8.4 8.5–9.2 9.3–10.2 > 10.2
PPGFPG
0
20
40
60
80
100
HbA1c quintiles
Co
ntr
ibu
tio
n (
%)
Monnier et al. Diabetes Care 2003;26:881–5

Relationship of HbA1c to plasma glucoseHbA1c Average ( range ) of plasma glucose
5 5.4 (4.2 – 6.7)
6 7.0 (5.5 – 8.5)
7 8.6 (6.8 – 10.3)
8 10.2 (8.1 – 12.1)
9 11.8 (9.4 – 13.9)
10 13.4 (10.7 – 15.7)
11 14.9 (12.0 – 17.5)
12 16.5 (13.3 – 19.3)
In general, the reference range (that found in healthy persons), is about 4%–5.9%.[
Average blood glucose = HbA1c X 1.59 – 2.59HbA1c = BG + 2.59 / 1.59
Home monitoring – a must for those on insulin therapy.

Home monitoring – a must for those on insulin.

Home Monitoring ChartDate Time &
Result of Glucometer
Time of injection/Insulin type
Dose of insulin
Time / type / amount of Food
Time & Result of Glucometer
Remarks


Have a systematic way to reduce diabetic complications:
1. HbA1c every 3-6 months
2. Yearly eye examinations / fundal camera
3. Annual microalbumin checks
4. Foot examinations at each visit
5. BP < 130/80 mm Hg, lower in diabetic nephropathy
6. Statin therapy ↓LDL

Case study
Case
• 63 year old businessman
• C/O urgency, incontinence, strangury, end dribbling, wets pants, penile erosions past few weeks
• T2DM for 12 years. Strong F/Hx
• 113 kg BMI: 44 BP 110/75 96/min
• Decreased sensation to monofilament. Fundoscopy was normal.
• Microalbuminuria, no cells

Present medication:
• Dapaglifozin 10mg daily
• Gliclazide 60mg daily
• Sitagliptin 100mg daily
• Mix insulin analog 25/75 OE
• Rosuvastatin 10mg daily
• Tamsulosin 400mg daily
• HM: 10.7 to 15.0 pre meals
• Intolerant of metformin

• T2DM – poor control
• Peripheral neuropathy & nephropathy
• Balanitis
• Impotence
• BPH
Present medication:
• Dapaglifozin 10mg daily
• Gliclazide 60mg daily
• Sitagliptin 100mg daily
• Mix insulin analog 25/75
• Rosuvastatin 10mg daily
• Tamsulosin 400mg daily
• Stop
• Continue
• Continue
• Glargine 20 units on night
• Continue
• Continue
• HM: 16 to 19.8 pre meals - worse
• But no more penile erosions or urinary symptoms

• Talked about GLP-1 agonist
• No family history of medullary carcinoma of thyroid
• Informed about possible side effects of nausea and GIT upset
• To report back if any abdominal pain – gall bladder issue and pancreatitis
• Started on S/C Liraglutide 0.6 mg daily
• Stop sitagliptin
• Increase Lantus dose gradually

• Home monitoring Wt Action taken
• Two weeks later : 13.2 to 18.6 113 kg Liraglutide added
• One month later : 10.0 to 14.5
• Two months later: 8.8 to 15.9 112 kg Empagliflozin 12.5 mg added
• Four months later: 10.0 to 12.0
• Six months later : 7.0 to 8.0 110 kg

• In this patient ....
• DPP IV had little effect
• Both GLP1 agonist and SGLT2 had therapeutic effect.
• Weight loss.
• Multiple drugs needed

Case
• 65 year old lady with previous myocardial infarction was recruited into TECOS study. Dec 2010
• HbA1c – 6 .2 - 7.6% - throughout the 5 years
• HM 5 to 8
• Also on metformin 1 g BD & gliclazide 80mg BD ; statin; aspirin; ARB; beta blocker;
• Weight 62 to 71.3 kg (June 2014)

Case
• After study ended, her HM went to about ‘teens’ within the next few months.
• HbA1c was 12.6% (April 2015) wt 61.8 kg
• Reintroduced DPP-IV inhibitor (April 2015)
• HbA1c 6 months later was 7.7% (Oct 2015) – 66kg
• Serum Creatinine was stable from 73 to 78 umol/l.

• In this lady, though not tried on every drug, restarting DPP IV made a lot of difference
Case - December 2006
• 43 year old Indian man. Works in a car spare parts shop
• Diabetes diagnosed at age of 31
• Strong family history of diabetes – both parents & sister
• Referred for poor control.
• Already on:
• Gliclazide MR 120mg daily
• Metformin 1 g bd
• Simvastatin 20mg ON
• S/C Mixtard 32 OM & 16 ON

Diagnosis
• T2DM – uncontrolled
• Diabetic neuropathy, retinopathy, impotence
• Hypertension
• Overweight

Dec 2006 to May 2016
• Multiple dietician referrals
• Spoke about exercise
• Basal bolus insulin therapy – different types; admission
• Tried acarbose, DPP IV inhibitor, GLP 1 agonist
• Offered pioglitazone, bariatric surgery

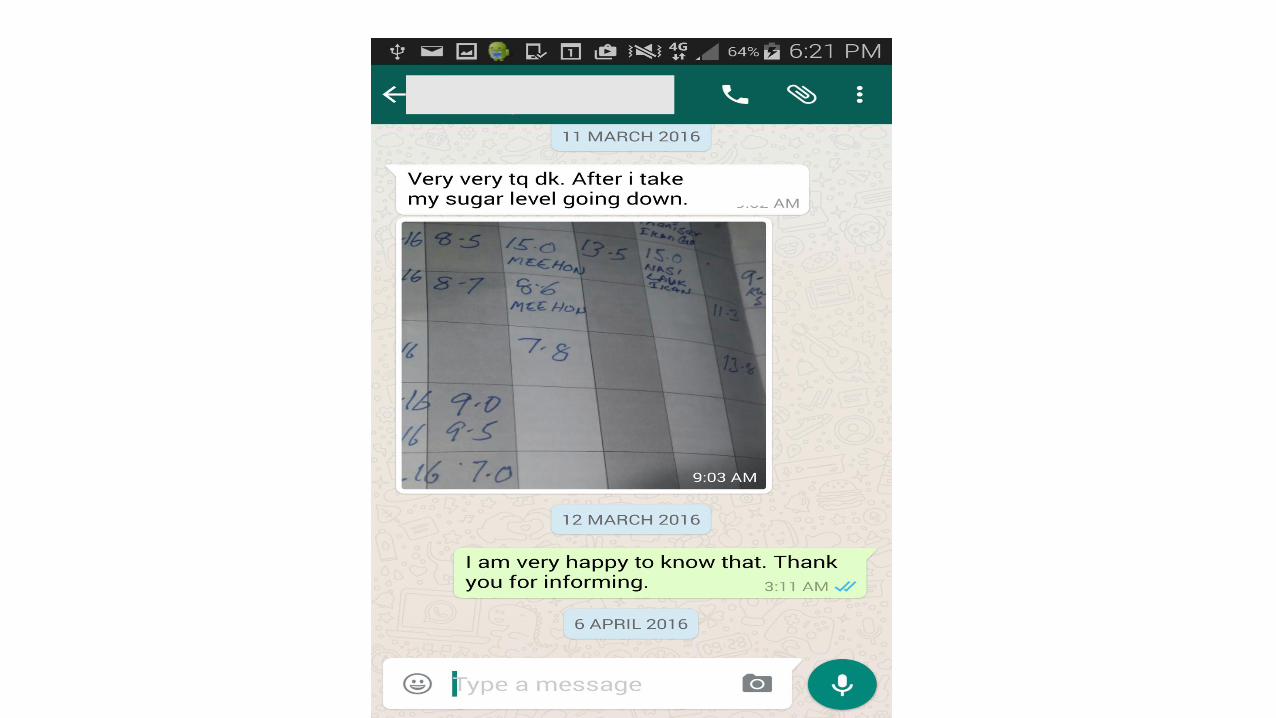
case – March 2016
• Weight 86 to 99kg HbA1c 12.6%
• Started on SGLT-2 inhibitor
• Within a few days – got an sms
case – End May 2016
• Weight 95
• HbA1c 8.7%
• GFR 112
• Urine protein negative
• LDL 2.3
Present medication
• SGLT-2 inhibitor• Metformin • Mix analog – slowly reducing dose. Now 20% less of previous dose• Ace- inhibitor• CCB• Beta blocker• Aspirin • Statin• Gabapentin – for a short while. • On eye and feet private follow-up.

• In this patient, it took years to get some degree of control.
• Metformin, Sulphonyurea, DPP –IV inb, GLP-1 agonist, high dose insulin all did not solve his hyperglycemic state.
• SGLT-2 inhibitor made a difference in him
• Still needs insulin but less
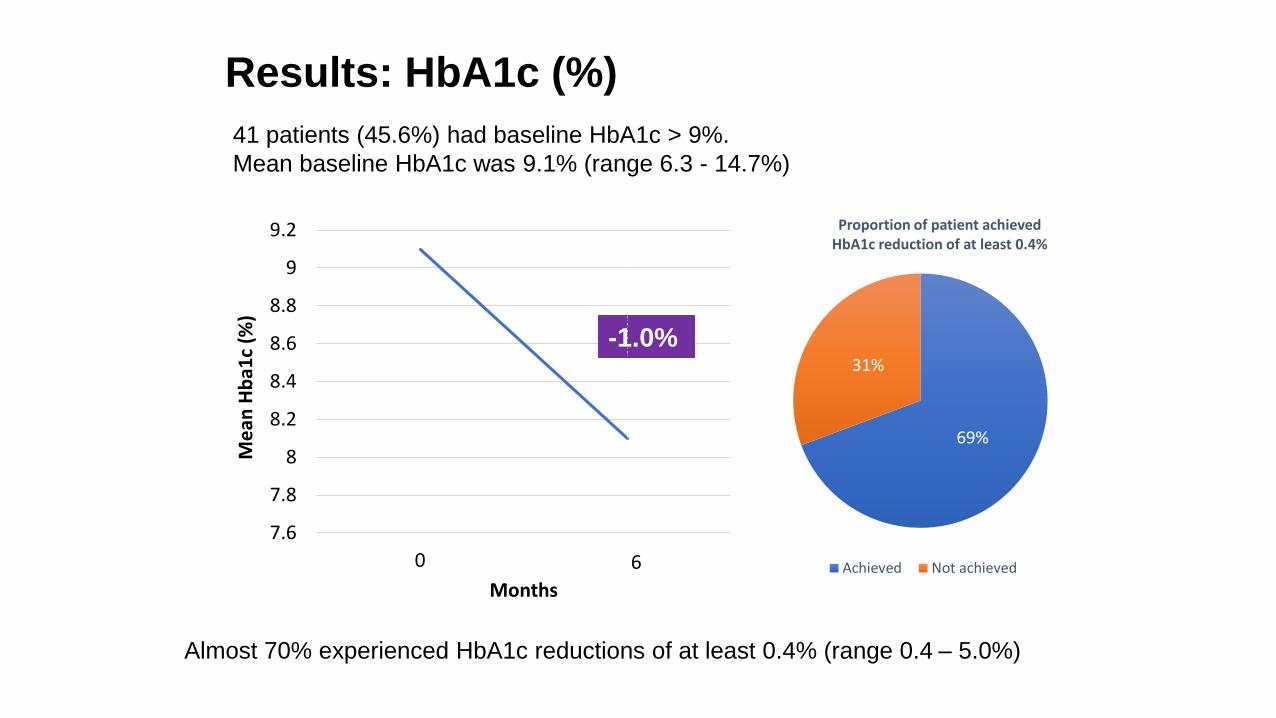
Results: HbA1c (%)
7.6
7.8
8
8.2
8.4
8.6
8.8
9
9.2
0
Me
an H
ba1
c (%
)
Months
6
6.4
-1.0%
69%
31%
Proportion of patient achieved HbA1c reduction of at least 0.4%
Achieved Not achieved
41 patients (45.6%) had baseline HbA1c > 9%.
Mean baseline HbA1c was 9.1% (range 6.3 - 14.7%)
Almost 70% experienced HbA1c reductions of at least 0.4% (range 0.4 – 5.0%)
62
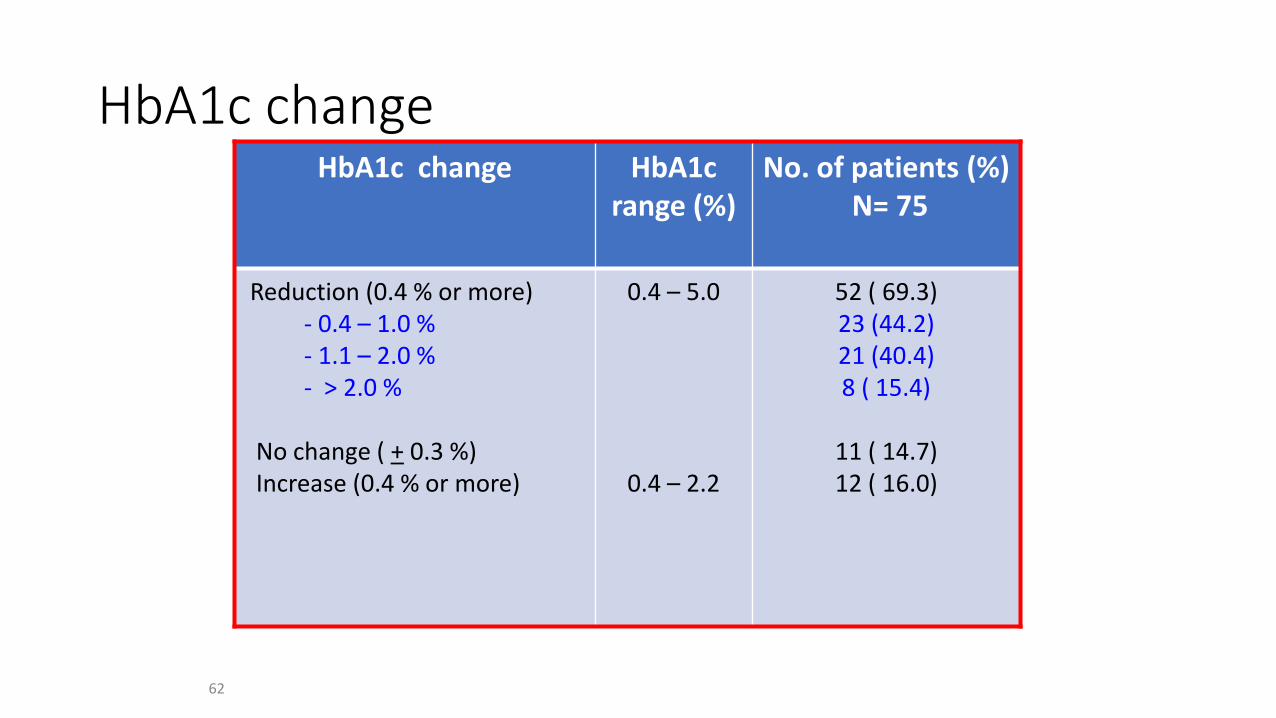
HbA1c changeHbA1c change HbA1c
range (%)No. of patients (%)
N= 75
Reduction (0.4 % or more)- 0.4 – 1.0 %- 1.1 – 2.0 %- > 2.0 %
No change ( + 0.3 %)Increase (0.4 % or more)
0.4 – 5.0
0.4 – 2.2
52 ( 69.3)23 (44.2)21 (40.4)8 ( 15.4)
11 ( 14.7)12 ( 16.0)

Have shifts in glucose-lowering drug prescribing made a difference?• Guidelines leave second-line agent choice (after metformin)
to clinicians and patients.
• Study of 81,532 individuals with T2D initiating first- to fourth-line glucose-lowering drug prescriptions in UK primary care during 2010-2017.
• Funding: Medical Research Council (UK).
• Limitations
• Study limited to UK population.
• Macrovascular/microvascular outcomes not evaluated.
• Source: Diabetes Obes Metab
• Curated by: Miriam Tucker
• March 06, 2019
• In 2010 vs 2017, first-line metformin use was 91% at both time points.
• Second-line sulfonylurea prescribing decreased from 53% to 29%, while prescribing of dipeptidyl peptidase-4 inhibitors rose from 22% to 41%.
• Second-line sodium-glucose cotransporter 2 inhibitor prescribing rose to 19% following 2013 approval.
• No HbA1c improvement after second-line therapy (0.0% change; P=.80).
• Weight loss trend seen at 6 months overall, primarily with second- and third-line therapy (2017 vs 2010: −1.5 and −1.2 kg, respectively; both P<.001).
• Trend in BP reduction at 6 months (2017 vs 2010: range −1.7 to −2.1 mmHg; all P<.001); no change in diastolic BP.
• Hypoglycemia reduction seen with second-line therapy initiation (5.7 vs 8.2/1000 person-years for 2017 vs 2010, respectively).

Have shifts in glucose-lowering drug prescribing made a difference?• The recent shift toward prescribing newer, more expensive, glucose-
lowering medication for type 2 diabetes (T2D) may be reducing hypoglycemia, weight, and blood pressure, but does not appear to be improving glycemic control.

Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lean MEJ et al Lancet Diabetes Endocrinol. 2019;7(5):344
• open-label, cluster-randomised, controlled trial done at primary care practices in the UK.
• Integrated structured weight-management programme (intervention) or best-practice care in accordance with guidelines
• individuals aged 20-65 years, with less than 6 years' duration of type 2 diabetes, BMI 27-45 kg/m2, and not receiving insulin
• The intervention consisted of withdrawal of antidiabetes and antihypertensive drugs, total diet replacement (825-853 kcal per day formula diet for 12-20 weeks), stepped food reintroduction (2-8 weeks), and then structured support for weight-loss maintenance.

Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lean MEJ et al Lancet Diabetes Endocrinol. 2019;7(5):344
• 11% in intervention grp & 2% control grp had weight loss of at least 15 kg
• 36% intervention grp and 3% control grp had remission of diabetes
• The adjusted mean difference between the control and intervention groups in change in bodyweight was -5·4 kg (95% CI -6·9 to -4·0; p<0·0001) and in HbA1c was -4·8 mmol/mol (-8·3 to -1·4 [-0·44% (-0·76 to -0·13)]; p=0·0063),
• despite only 40% of in the intervention group using anti-diabetes medication compared with 84% in the control group.
• The DiRECT programme sustained remissions at 24 months for more than a third of people with type 2 diabetes. Sustained remission was linked to the extent of sustained weight loss.

Main message
• Patient as partner (his & her views) – diet, exercise, weight, drugs
• Use patient characteristics to decide the most appropriate therapies needed
• Test one therapy at a time for a reasonable period of time to gauge its efficacy and side effects
• Do not continue therapies that do not give reasonable efficacy or has unacceptable adverse events.
• Use combinations when needed to improve compliance
• Any improvement is still useful

Thank you
Biguanides - metformin
• Insulin sensitizer, Inhibition of hepatic glucose production
• ↓ MI by 39% ↓ Coronary deaths by 50% (UKPDS)
• Renal excretion. Stop drug if GFR < 30
• Rare – lactic acidosis. Stop during major illness or prior to contrast
• Vit B12 deficiency
• Very safe drug – first line in all guidelines

Sulphonylureas and Glinides
• Stimulate insulin chronically
• High hypo risk esp in setting of renal failure
• Weight gain
• 2nd generation generally safer
• Glinides – short acting, hepatic excretion, used safely in chronic renal failure
Indications for Insulin pump
• Inadequate glycaemic control with MDI (multiple daily injections) therapy
• Recurrent severe hypoglycaemia
• Hypoglycaemia unawareness
• Dawn phenomenon
• Gastroparesis
• Frequent diabetic ketoacidosis
Continuous glucose monitoring (CGM)
• Especially for patients with T1DM.
• Improve glycaemic control,
• Nocturnal hypoglycaemia
• Hypoglycaemia unawareness.

Once-Weekly Dulaglutide Benefit in REWIND, Longest CVOT to Date
• significantly reduced the risk of major adverse cardiovascular events (MACE) in the REWIND cardiovascular (CV) outcomes trial, primarily by reducing the risk of stroke.
• "The magnitude of benefit on the composite CV outcome (12%) was modest and numerically lower than that seen in the positive GLP-1 agonist studies — namely, LEADER, SUSTAIN-6, and HARMONY — but consistent with the overall effect size from a meta-analysis of all previous GLP-1 receptor agonist trials."
• But they highlight the fact that the population studied in REWIND does differ somewhat.
• "Compared with previous studies of GLP-1 receptor agonists, individuals included in the REWIND trial were at a lower risk of CV events."

Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction 58 -DECLARE–TIMI 58
• The goal of the trial was to assess the cardiovascular (CV) safety of dapagliflozin in patients with type 2 diabetes mellitus (DM2) and either established CV disease (CVD) or multiple risk factors.
Insulin
• Risk of hypoglycaemia
• Weight ↑↑
• HF when combined with TZD
• Lipo atrophy & hypertrophy

Insulin
1. Short acting or rapid acting or prandial - To control post prandialrise
2. Intermediate acting or long acting or basal -To control fasting levels & in between meals
3. Premixed
• Human insulin (recombinant technology) or Analogs (genetically modified human insulin)
• Novo / Elily / Sanofi / Biocon

Insulin Analogs
• Less hypo
• Less weight gain
• More predictable
• Rapid acting – just before the meals. Multiple injections
• Long Acting – once a day
• Much more expensive. Not more efficacious
• New combinations: GLP1 analog + Long acting insulin
• Lessons Learned and Future Direction
• Though initially designed to keep potentially harmful hypoglycemic agents off the market, the CV safety trials have surprisingly provided clinicians with a new set of anti-diabetic drugs with proven CV benefit in patients with diabetes and CV disease, thus expanding the field of CV secondary prevention. New medications like empagliflozin and liraglutide improve not only CV mortality but also all-cause mortality in diabetic patients with CV disease. The FDA has approved specific labels for both empagliflozin and liraglutide to reduce the risk of CV death in adults with diabetes and CV disease. Additionally, SGLT2 inhibitors like empagliflozin and canagliflozin reduce heart failure hospitalizations. If the results of the ongoing trials with empagliflozin in heart failure patients prove utility, these drugs can be considered as an additional choice for the treatment of chronic heart failure patients.
• The choice of hypoglycemic medication may possibly tip in the favor of the orally administered SGLT2 inhibitors rather than injectables like GLP-1 analogs, though this may be less of a concern in patients already on injectable insulin/insulin analogs. Patients with diabetes and CV disease who are at an increased risk of heart failure would probably benefit more from an SGLT2 inhibitor. Future trials should aim at providing a comparative assessment between diabetes medications rather than merely establishing efficacy against placebo.
Thiazolidinediones (TZD) or glitazones
• Insulin sensitizer
• Weight gain
• If patient also has non-alcoholic fatty liver disease – consider it
• Adverse: CCF. MI (Rosi), bladder cancer (Pio), fractures





























