Embed Size (px)
Citation preview

Diabetes MellitusDisease Management in a Multispecialty Group Practice
Jeremy M. Gleeson, Michael Foris, Marjorie Cypress, Donna J. Rodriguez,Neal Friedman and Martha Kent
Lovelace Health Systems, and Lovelace Healthcare Innovations, Albuquerque, New Mexico, USA
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 611. Diabetes Disease Management Concepts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
1.1 Prevention and Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 621.2 Acute and Inpatient Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 631.3 Outpatient Follow-Up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 631.4 Outcomes Measurement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
2. The Lovelace Health Systems Diabetes Episodes of Care® Programme . . . . . . . . . . . . . . . 642.1 The Diabetes EOC® Team . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 652.2 Programme Development and Implementation . . . . . . . . . . . . . . . . . . . . . . . . . . 652.3 Practice Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 652.4 Patient Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 682.5 Evaluation of the Diabetes EOC® Programme . . . . . . . . . . . . . . . . . . . . . . . . . . . 682.6 Glycaemic Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 682.7 Patient Education Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 692.8 Retinal Eye Examination Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 692.9 Foot Examination Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
3. Achievements of Diabetes Disease Management Programmes . . . . . . . . . . . . . . . . . . . 703.1 Coordination of Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 703.2 Reduction of Complications and Long Term Costs . . . . . . . . . . . . . . . . . . . . . . . . . 703.3 Meeting Accreditation Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
4. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
Abstract Because of the extensive burden that diabetes mellitus imposes on individualsand healthcare systems, this disease state is frequently on the priority lists ofmanaged-care organisations for improving quality of care while controlling costs.This article explains diabetes disease management concepts and interventionsaimed at improving clinical outcomes illustrated with details of the LovelaceHealth Systems Diabetes Episodes of Care® programme.
The effectiveness of diabetes disease management programmes can best beevaluated by the clinical outcome of haemoglobin A1c measures. Process meas-urements include diabetes education access, annual eye examinations and docu-mentation of annual clinical evaluations of feet. Short term cost reductions arefrequently unrealistic expectations of diabetes disease management programmesbecause of the complex, chronic nature of the disease. Coordination of previously
PRACTICAL DISEASE MANAGEMENT Dis Manage Health Outcomes 1999 Feb; 5 (2): 61-721173-8790/99/0002-0061/$06.00/0
© Adis International Limited. All rights reserved.

fragmented services, eventual reduction of long term complications and meetingregulatory standards are potential achievements of these programmes.
Diabetes mellitus is of epidemic proportions inthe US affecting approximately 15 million Ameri-cans with 7.2 million diagnosed and an estimated8 million undiagnosed adults with the disease.[1,2]
In New Mexico, an estimated 9% of the populationor 150 000 people are affected by diabetes,[3] ap-proximately double the national rate. This rate isinfluenced by Hispanics who are 2 to 3 times morelikely, and by Native Americans who may be 10times more likely to develop diabetes than the gen-eral US population.[4]
Diabetes is the leading cause of blindness inpeople aged 20 to 74 years of age,[5] it is the causeof about 35% of new onset end-stage renal dis-ease[6] and conveys an increased risk for cardiovas-cular disease.[1] The US national economic burdenof diabetes in 1992 was estimated at approximately$US100 billion, with direct medical costs repre-senting $US45.2 billion and indirect costs due toproductivity losses accounting for $US46.6 billiondollars.[1,2] Hospitalisation costs contributed thegreatest proportion or 83% of the total direct med-ical costs.[1,2]
The landmark Diabetes Control and Complica-tions Trial (DCCT) demonstrated that improvedglycaemic control in patients with type 1 (insulin-dependent) diabetes can reduce long term compli-cations of the disease, with reductions in albumin-uria by 54%, retinopathy by 50% and neuropathyby 60%.[7] A reduction in these complications canpotentially improve functional status, employeeproductivity and reduce costs. Similar benefits oftight glucose control in patients with type 2 (non–insulin-dependent) diabetes were demonstrated ina Japanese study at Kumamoto University.[8] A na-tional consensus also exists that DCCT results canbe applied to patients with type 2 diabetes.[9] Thisapproach has been very recently confirmed by theUnited Kingdom Prospective Diabetes Study(UKPDS).[10] Presumably, reductions in complica-tions will have a greater overall impact in patients
with type 2 diabetes because of the prevalence ofthis type of diabetes mellitus.
Diabetes disease management is a novel, sys-tematic approach designed to deliver optimal patientcare while controlling costs. This article: (i) ex-plains key diabetes disease management conceptsillustrated with a description of the Lovelace HealthSystems (LHS) Diabetes Episodes of Care® (EOC)programme; and (ii) describes advantages that canbe achieved by implementing these programmesand improving clinical outcomes.
1. Diabetes DiseaseManagement Concepts
Diabetes disease management involves the co-ordination of resources across the continuum ofcare provided to patients with diabetes, specificallyprevention, diagnosis, acute treatment, inpatientand outpatient care. It is a process aimed at assuringthat best clinical practices are incorporated withminimal variation across a healthcare system. Type2 diabetes accounts for 90% of all diabetes[9] and,therefore, is the focus of most diabetes manage-ment programmes.
1.1 Prevention and Diagnosis
Screening for type 2 diabetes is especially im-portant for high risk patients (see table I). Diseasemanagement primary prevention targets high riskpopulations through reduction of modifiable riskfactors.[11] The programme emphasises lifestylemodification (e.g. improved nutrition and exercise)and pharmacological intervention is not currentlyrecommended. Whether pharmacological interven-tion can delay or prevent the onset of diabetes inindividuals at risk, but who do not yet have diabe-tes, awaits the completion of the large multicenterDiabetes Prevention Program.
If primary prevention fails, early diagnosis iscrucial so that aggressive secondary prevention ef-forts can begin. The American Diabetes Association
62 Gleeson et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

(ADA) criteria for the diagnosis of diabetes arepresented in table II. Type 2 diabetes is charac-terised by a long asymtomatic period during whichtime complications, such as retinopathy and ne-phropathy, can develop. When impaired glucosetolerance or type 2 diabetes is detected in asymp-tomatic individuals, complications can be aggres-sively delayed or prevented.[9]
Disease management also provides a proactive,organised approach to tertiary prevention withstrategies designed to reduce progression of estab-lished complications. An example of a tertiary pre-vention effort is the establishment of guidelines forthe use of angiotensin converting enzyme (ACE)inhibitors in patients with early manifestations ofnephropathy.
1.2 Acute and Inpatient Treatment
Patients with newly diagnosed type 2 diabetesneed variable levels of care depending on the se-verity of the illness at the time of diagnosis. In wellmanaged healthcare systems, most patients withnewly diagnosed diabetes mellitus can be managedon an outpatient rather than inpatient basis. At LHSin Albuquerque, New Mexico, USA, virtually allnewly diagnosed patients are managed as outpa-tients. In clinical settings where intensive outpa-tient follow-up is not available, newly diagnosedpatients may require costly inpatient care.
When previously diagnosed patients with type2 diabetes require hospitalisation, it is usually forcomorbid illnesses, particularly cardiovasculardisorders, which occur with greater frequency in
patients with diabetes. Reduction in such hospital-isations must be seen as a long term, rather than ashort term, goal of diabetes disease managementprogrammes. However, reductions in emergencyroom visits and avoidable hospital admissions arelegitimate goals of diabetes disease managementprogrammes in order to reduce healthcare expen-ditures.
1.3 Outpatient Follow-Up
After diagnosis and acute treatment, beginningthe lifelong process of diabetes education is thenext step toward achievement of diabetes control.ADA goals for glycaemic control are presented intable III. Effective self-management training re-quires an individualised approach to lifestyle mod-ification (nutrition, exercise and weight control),and if necessary pharmacological therapy, to achieveglycaemic control. Achievement of optimal levelsof blood glucose, haemoglobin A1c (HbA1c) lipids,and blood pressure are essential components of out-patient management. Screening for long term com-plications of diabetes, combined with appropriateinterventions, can prevent or ameliorate these com-plications and thereby enhance quality of life whilereducing costs.
1.4 Outcomes Measurement
A number of objective outcome measures areused to evaluate the effectiveness of diabetes dis-ease management programmes. Using clinical and
Table I. High risk conditions for type 2 diabetes mellitus
Family history of type 2 diabetes
Non-Caucasian ethnic background, especially Native-American,Hispanic-American, African-American, Asian-American or PacificIslander
Obesity (defined as ≥20% over desired bodyweight or bodymass index ≥27 kg/m2)
History of impaired glucose tolerance
History of gestational diabetes mellitus or delivery of babies >9pounds (4kg)
Presence of hypertension or hyperlipidaemia
Age of ≥45y, in addition to the above factors
Table II. Criteria for diagnosis of diabetes mellitus (from the Amer-ican Diabetes Association,[12] with permission)a
Symptoms of diabetes plus casual plasma glucose level ≥200mg/dl (11.1 mmol/L). Casual is defined as any time of daywithout regard to time since the last meal. The classic symptomsof diabetes include polyuria, polydipsia and unexplained weightloss
OR
Fasting plasma glucose ≥126 mg/dl (7.0 mmol/L). Fasting isdefined as no caloric intake for at least 8h
OR
2h postload glucose ≥200 mg/dl during an oral glucose tolerancetest using a glucose load containing the equivalent of 75g ofanhydrous glucose dissolved in water
a These tests must be confirmed on different days.
Diabetes Management in a Multispecialty Group Practice 63
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

economic outcomes simultaneously assures thatone is not emphasised to the detriment of the other.In non-academic clinical settings, outcome studiesare more practical for quality improvement pur-poses than are prospective, randomised clinical tri-als. Numerous simultaneous interventions or sys-tem changes, rather than single interventions withrigid controls for confounding variables, are morerealistic in non-academic settings. In ‘real world’clinical settings it is often difficult to determinewhich components of a disease management pro-gramme resulted in an improved outcome measure,and to what degree the individual components ofthe programme contributed to the overall change.
2. The Lovelace Health SystemsDiabetes Episodes of Care® Programme
LHS is the second largest, most fully integratedhealthcare delivery system in New Mexico. The LHSsystem includes:• a 325-physician multispecialty practice group• approximately 1500 contracted network physi-
cians• a 235-bed acute care hospital• 9 primary care centres in Albuquerque, 2 in out-
lying communities• a 208 000 member health maintenance organi-
sation (HMO).
In 1993, LHS identified diabetes as 1 of 9 dis-ease entities that accounted for 25% of the institu-tion’s resource utilisation.[14,15] As a strategic diseasemanagement initiative, LHS launched the DiabetesEOC® programme to further promote a coordi-nated, multidisciplinary approach for this high-volume, high-cost condition.
The Diabetes EOC® programme has primarilyfocused on the outpatient management of type 2diabetes. A secondary focus has been inpatientmanagement of patients with type 2 diabetes whoare typically admitted for comorbid illnesses. In theLHS delivery system, as in most community set-tings, type 2 diabetes is usually managed by gener-alist, not specialist, physicians. LHS primary carephysicians (PCPs) are situated at multiple satellitelocations in 3 New Mexico metropolitan areas. Thechallenge faced by LHS, as well as other healthcaredelivery systems, is to bring current standards ofdiabetes care to patients in this ‘real world’ setting.We sought to improve the care of all patients withdiabetes within LHS rather than concentrating ona particular clinic. We chose not to set up a diabetesspecialty management or ‘carve-out’ system butrather to support and strengthen the ability of PCPsto meet this challenge.
Prior to establishment of the Diabetes EOC®
programme, LHS had a well established diabeteseducation programme based in the endocrinologydepartment. A major strategy of the Diabetes EOC®
programme has been the decentralisation of the di-abetes education programme. This has required thecertified diabetes educators (CDEs) to travel to sat-ellite clinics for specific appointments each week,previously patients received education at the mainLHS facility only. This practice has allowed foreasy patient accessibility to diabetes education andhas increased referrals. At LHS, CDEs have ex-panded roles, frequently comanaging patients withthe PCPs and reviewing management decisionswith the endocrinologists. Almost all PCPs referpatients to the CDEs and there are no disincentivesto physician referrals to CDEs. The endocrinolo-gists do not see patients in the Albuquerque primarycare clinics, but do review management decisions
Table III. Criteria for glycaemic control in patients with diabetesmellitus (from the American Diabetes Association,[13] with permis-sion)a
Biochemicalparameter
Normallevels
Target level Additional actionsuggestedb
Preprandial plasmaglucose (mg/dl)
<110 80-120 <80 or >140
Bedtime plasma(mg/dl)
<120 100-140 <100 or >160
HaemoglobinA1c (%)
<6 <7 >8
a The values shown in this table are by necessity generalised tothe entire population of individuals with diabetes. Patientswith comorbid diseases, the very young and older adults,and others with unusual conditions or circumstances maywarrant different treatment goals. These values are fornonpregnant adults.
b This depends on individual patient circumstances.
64 Gleeson et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

with the CDEs at weekly case conferences. Thisallows for limited specialist resources (endocrinol-ogists) to be made available to a much larger num-ber of patients with diabetes than would be possi-ble on an individual basis. Endocrinologists arereadily available to PCPs by telephone to discusspatient management. Selected patients, includingmost patients with type 1 diabetes, are seen by anendocrinologist. Frequent educational seminarsfor PCPs are held at various locations throughoutthe system.
Patients are not formally enrolled in the Diabe-tes EOC® programme. The function of the EOC®
programme is to support the diabetes managementstructure as outlined above. Thus the programme canbe considered to be a ‘virtual clinic without walls’.The following discussion illustrates how the Dia-betes EOC® programme has incorporated key dia-betes disease management concepts.
2.1 The Diabetes EOC® Team
Patients with diabetes require coordinated carefrom several different healthcare professionals.The Diabetes EOC® team leadership is shared byan endocrinologist and a PCP to foster communi-cation and collaboration between the 2 groups. Inaddition to the physician members, the DiabetesEOC® team consists of a CDE, a quality facilitator,a data consultant and an administrator. Others suchas an ophthalmologist and a podiatrist act as con-sultants to the team. The Diabetes EOC® team pro-motes integration of services by designing and im-plementing the diabetes management guidelinesand overseeing the system-wide deployment of theEOC® programme.
2.2 Programme Developmentand Implementation
To guide development, the Diabetes EOC® pro-gramme began with the following vision and mis-sion statements:• The vision: LHS patients will become skilled
and responsible participants in the manage-ment of their diabetes and will achieve the bestpossible outcomes.
• The mission: To continuously improve a patient-centred system that provides high quality diabe-tes care in the most cost-efficient manner.
2.3 Practice Guidelines
Between 1994 and 1995, significant progress withevidence-based guideline development was madeby the Diabetes EOC® team. Practice guidelineswere based on the ADA Standards of Care[16] thencustomised for the LHS setting. Guidelines wereupdated when new versions of the ADA Standardsof Care were published.[11,17]
According to the unique needs and systems atLHS, individual guidelines or flow charts addressthe following key aspects.
Diagnosis of Type 2 Diabetes MellitusA step-by-step plan for evaluating patients with
symptoms suggestive of diabetes including imme-diate or fasting blood glucose levels, and recom-mendations for annual fasting blood glucose levelsand risk reduction counselling for all patients withrisk factors not meeting the diagnostic criteria fordiabetes (table I).[11]
Acute Intervention and Treatment of HyperglycaemiaManagement recommendations depend on blood
glucose level and presence or absence of signifi-cant ketosis. For patients of normal weight withketosis and blood glucose >200 mg/dl (11.1 mmol/L)rapid initiation of insulin is recommended. For ill-appearing patients with blood glucose >300 mg/dl(16.7 mmol/L) or 2+ ketones, consultation with anendocrinologist is recommended. All patients areseen promptly by CDEs with management beingcoordinated by the primary care physician in mostcases. Acute intervention and treatment is almostalways accomplished on an outpatient rather thanon an inpatient basis.
Outpatient ManagementSetting goals for normal and target glycaemic
control (table III); individualised treatment plans,diabetes education; and re-evaluations of diabetescontrol at 3- to 6-month intervals.
Diabetes Management in a Multispecialty Group Practice 65
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

Pharmacological TreatmentRecommended medication usage, including
dosing guidelines and cost considerations, for sul-fonylureas, metformin, acarbose, troglitazone and/orinsulin.
Complications Screening Recommendations• For retinopathy: annual eye examinations for all
patients with type 2 diabetes, and for any patientwith >5 years duration of type 1 diabetes. Eyeexaminations are performed by optometrists un-der the supervision of ophthalmologists; patientsare referred to retinal specialists as needed whenretinopathy needs treatment.
• For nephropathy: annual urine microalbumin/creatinine ratios with possible use of an ACEinhibitor in patients with persistent micro- ormacroalbuminuria (>30 μg/mg) creatinine.
• For peripheral neuropathy: foot inspectionsevery visit or every 3 months, and a more detailedvascular and neurological examination with re-ferrals to a podiatrist as indicated. Routine elec-trophysiological studies are not recommended.
• For cardiovascular disease: lipid screening and ag-gressive management of hyperlipidaemia in ac-cordance with current ADA recommendations.[11]
• For hypertension, blood pressure monitoring ev-ery visit or every 3 to 6 months. Blood pressuretarget is 130/85mm Hg or less.
These guidelines were intended to provide theframework for diabetes care and reduce inappropri-ate variations in physician practice, but were notdesigned to limit more extensive evaluations ifneeded. These guidelines are not meant to be in-flexible pathways; LHS encourages, not restrictsindividualised patient management. Endocrinolo-gists are readily available by telephone, and for for-mal consultation, to formulate individual manage-ment plans.
Practice guidelines were initially distributed tostaff model physicians with subsequent dissemina-tion to all LHS providers. Adapted guideline ver-sions were also distributed to the telephone triagenurses who address patients’ questions and consultphysicians when urgent care is needed. However,development and dissemination of evidence-based,customised practice guidelines do not assure auto-matic or consistent implementation by practition-ers.[18] Translation of practice guidelines into prac-tical provider tools can influence successfulguideline implementation.
Novel strategies such as a computerised Diabe-tes Profile Screen (fig. 1) and the Provider SupportReport (fig. 2) have been developed by the Diabe-tes EOC® programme to increase practitioners’awareness and utilisation of guidelines. The Diabe-tes Profile Screen is part of a computerised medicalrecord that is used to provide online access to pa-
Diabetes care-treatment summary
REMEMBER FOOT EXAMINATIONIf microalbumin is high consider ACE inhibitor
GlycoHgb
Micro-albumin
Retinalexamination
CDEEd.
T. Chol. HDL LDL TRG
Due
7/13/98 9.6 32 1501/23/98 9.4 1858/24/979/14/96
×
××
× ×
Fig. 1. The Diabetes Profile Computer Screen. This can be displayed on any Lovelace computer terminal. Most examination roomshave terminals. ACE = angiotensin converting enzyme; CDE Ed. = education by a certified diabetes educator; Glyco Hgb = glycatedhaemoglobin; HDL = high density lipoprotein; LDL = low density lipoprotein; T. Chol. = total cholesterol; TRG = tryglyceride.
66 Gleeson et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

0%20%
40%
60%
80%
100%
Educ
Eye
exam
Glip
Gly
b Gly
coH
b le
vel Gly
coH
b or
d
Mic
ro o
rd
Test
strp
Pro
vide
rLo
catio
nS
peci
alty
Per
cent
age
of p
atie
nts
with
in s
tand
ard
Nam
eM
RN
Edu
cE
ye e
xam
sG
lipiz
ide
Gly
burid
eG
lyco
haem
oglo
bin
le
vel
or
dere
d
M
icro
albu
min
ord
ered
Te
st
st
rips
John
Doe
Jane
Doe
Juan
Dia
z
Mar
ia D
iaz
Bill
Jon
es
Bet
sy S
mith
N N N
13.2
13.8
10.6
NN
N N N N N N
N N N
Pat
ient
s ou
tsid
e of
sta
ndar
ds
Crit
eria
Sta
ndar
dsTo
tal
pts
w/
diab
etes
Tota
l p
ts
test
ed
No.
with
inst
anda
rd
%W
ithin
stan
dard
Edu
catio
nR
ollin
g 2y
22 22 1 0 22 22 22 22
22 15 1 0 20 20 10 0
22 15 1 0 9 20 10 0
100.
00
68.1
8
100.
00
0.00
45.0
0
90.9
1
45.4
5
0.00
Rol
ling
1y
≤20
mg/
day
≤15
mg/
day
≤10.
5%
With
in 1
y
With
in 1
y
Twic
ew
ithin
1y
Eye
exa
ms
Glip
izid
e
Gly
burid
e
Gly
coH
ble
vel
Gyc
oHb
orde
red
Mic
roal
bum
inor
dere
d
Test
str
ips
EO
C P
rov
ide
r S
um
ma
ryD
iab
ete
s
09/0
1/98
Su
sa
n C
ure
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
××
Fig
. 2. T
he P
rovi
der
Sup
port
Rep
ort.
Indi
vidu
al p
hysi
cian
s ar
e co
mpa
red
to e
ach
clin
ic g
roup
and
to th
e en
tire
prim
ary
care
gro
up. P
atie
nts
who
fall
outs
ide
reco
mm
enda
tions
in
one
or
mor
e m
easu
rem
ents
are
list
ed. E
du
c =
edu
catio
n by
a c
ertif
ied
diab
etes
edu
cato
r; G
lip
= g
lipiz
ide;
Gly
b =
gly
burid
e; G
lyco
Hb
= g
lyco
haem
oglo
bin;
Gly
co
Hb
ord
=
glyc
ohae
mog
lobi
n or
dere
d; M
icro
ord
= m
icro
albu
min
ord
ered
; MR
N =
med
ical
rec
ord
num
ber;
Pts
= p
atie
nts.
Diabetes Management in a Multispecialty Group Practice 67
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

tient records. Computer terminals, available inphysicians’ offices and examination rooms, makeinformation such as demographics, laboratory val-ues, radiology reports and dictated clinic notes,conveniently accessible to physicians during pa-tients’ visits.
The Diabetes Profile Screen (fig. 1) itself pres-ents patient information including levels for HbA1c,
lipid and urine microalbumin, date of eye exami-nations, and date of education visits. Other com-puter screens provide a synopsis of the DiabetesEOC® practice guidelines. The Provider SupportReport (fig. 2) is a simple, 1-page report that illus-trates how physicians are doing in managing theirpatients with diabetes compared with their profes-sional peers. The quarterly report includes lists ofpatients who have not met standard criteria, suchas necessary tests, examinations or services in thespecified time period or who have test results out-side the recommended standards. This pertinent,timely feedback can identify high risk patients andprompt providers to arrange for appointments ortests needed. These reports are utilised for qualityimprovement purposes only, and are not used toevaluate or compensate individual physicians.
Other innovative implementation strategies in-clude guideline information on the LHS Intranetweb pages. Online information enables changesand updates to be rapidly made and disseminatedthroughout the institution. Pocket-sized formularybooklets include reference sections on preferredmedications and reinforce practice guideline infor-mation. Wallet-sized patient care cards list individ-ual educational goals, records of education ses-sions and patient examinations needed.
2.4 Patient Education
A diabetes education programme has been pro-vided at LHS since 1972, consistent with a long-standing belief that patient education is crucial forthe long term success of diabetes management. Re-ferrals to the CDEs occur for all newly diagnosedpatients with diabetes and many previously diag-nosed patients who have inadequate glycaemiccontrol. A variety of educational formats are used
including group classes and individual counsel-ling. The educational process initially takes weeksto months with subsequent periodic reassessments.Patient education and educational materials are in-dividualised, incorporating cultural aspects, liter-acy levels and lifestyle of each patient. In additionto educating patients, CDEs also assume an activerole in diabetes management by adjusting medica-tions in accordance with established protocols, incollaboration with the patients’ PCPs, and underthe supervision of endocrinologists.
2.5 Evaluation of the DiabetesEOC® Programme
Disease management programme evaluationscan target different population groups, such as:• the total known population of patients with dia-
betes in the healthcare delivery system• managed-care patients or health plan members
only• subgroups such as the Health Plan Employer
Data and Information Set (HEDIS) subgroup.The HEDIS subgroup consists of health plan
members who are between the ages of 31 and 64years and have been continuously enrolled for theprevious year. HEDIS is a set of standard defini-tions and methodologies used to obtain and com-pare performance measures between health plans.In the US, the HEDIS subgroup must be identifiedfor monitoring of retinal eye examination rates, andprobably other measures in the future.
To assess the impact of disease management in-terventions, selected indicators must measure keyoutcomes. The clinical and process outcomes dis-cussed below are among the measures that havebeen selected by the Diabetes EOC® programme.
2.6 Glycaemic Control
A primary clinical indicator of diabetes manage-ment outcome is HbA1c level. Evaluation of thisoutcome can occur by assessments of the:• annual rate or percentage of the population who
have received HbA1c testing• average annual HbA1c results
68 Gleeson et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)
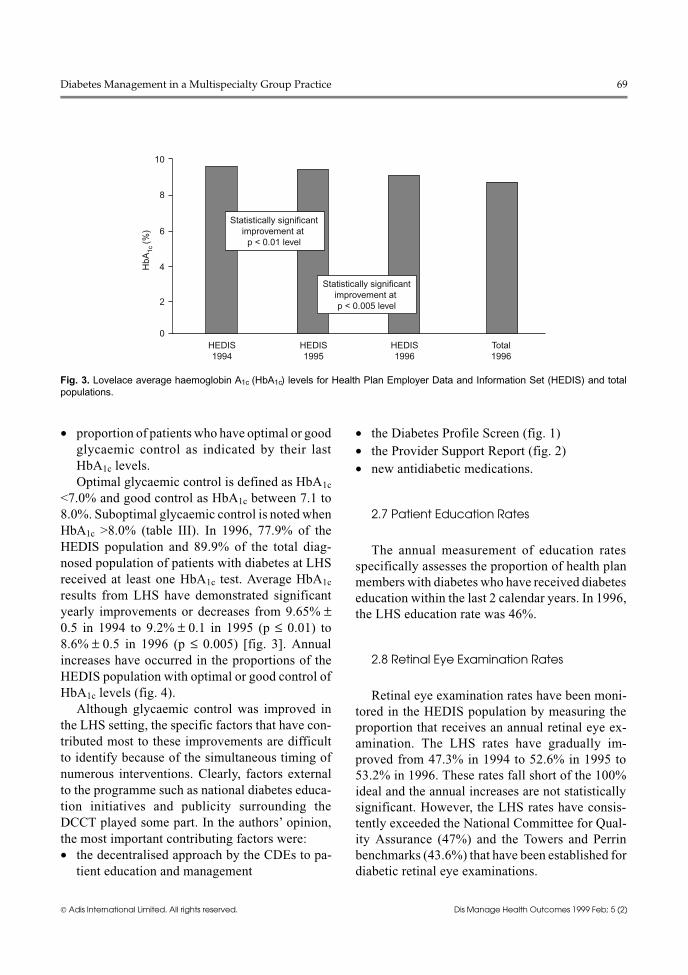
• proportion of patients who have optimal or goodglycaemic control as indicated by their lastHbA1c levels.Optimal glycaemic control is defined as HbA1c
<7.0% and good control as HbA1c between 7.1 to8.0%. Suboptimal glycaemic control is noted whenHbA1c >8.0% (table III). In 1996, 77.9% of theHEDIS population and 89.9% of the total diag-nosed population of patients with diabetes at LHSreceived at least one HbA1c test. Average HbA1c
results from LHS have demonstrated significantyearly improvements or decreases from 9.65% ±0.5 in 1994 to 9.2% ± 0.1 in 1995 (p ≤ 0.01) to8.6% ± 0.5 in 1996 (p ≤ 0.005) [fig. 3]. Annualincreases have occurred in the proportions of theHEDIS population with optimal or good control ofHbA1c levels (fig. 4).
Although glycaemic control was improved inthe LHS setting, the specific factors that have con-tributed most to these improvements are difficultto identify because of the simultaneous timing ofnumerous interventions. Clearly, factors externalto the programme such as national diabetes educa-tion initiatives and publicity surrounding theDCCT played some part. In the authors’ opinion,the most important contributing factors were:• the decentralised approach by the CDEs to pa-
tient education and management
• the Diabetes Profile Screen (fig. 1)• the Provider Support Report (fig. 2)• new antidiabetic medications.
2.7 Patient Education Rates
The annual measurement of education ratesspecifically assesses the proportion of health planmembers with diabetes who have received diabeteseducation within the last 2 calendar years. In 1996,the LHS education rate was 46%.
2.8 Retinal Eye Examination Rates
Retinal eye examination rates have been moni-tored in the HEDIS population by measuring theproportion that receives an annual retinal eye ex-amination. The LHS rates have gradually im-proved from 47.3% in 1994 to 52.6% in 1995 to53.2% in 1996. These rates fall short of the 100%ideal and the annual increases are not statisticallysignificant. However, the LHS rates have consis-tently exceeded the National Committee for Qual-ity Assurance (47%) and the Towers and Perrinbenchmarks (43.6%) that have been established fordiabetic retinal eye examinations.
0
2
4
6
8
10
HbA
1c (%
)
HEDIS1994
HEDIS1995
HEDIS1996
Total1996
Statistically significantimprovement at
p < 0.01 level
Statistically significantimprovement at p < 0.005 level
Fig. 3. Lovelace average haemoglobin A1c (HbA1c) levels for Health Plan Employer Data and Information Set (HEDIS) and totalpopulations.
Diabetes Management in a Multispecialty Group Practice 69
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

2.9 Foot Examination Rates
This outcome is more difficult to monitor be-cause of the need for chart audits, since no codingor electronic data exist for determination of theserates. A recent external survey by the New MexicoMedical Review Association found a foot exami-nation rate of 54% at LHS, nearly double the 28%average at 3 other New Mexico HMOs (Prinztz F,personal communication).
3. Achievements of Diabetes DiseaseManagement Programmes
With diabetes disease management programmes,several improvements, including coordination ofservices, reduction in complications, and meetingrecognised accreditation requirements or bench-marks may be achieved.
3.1 Coordination of Services
Fragmentation of care for patients with type 2diabetes can thwart attempts to control costs. Im-plementation of capitation has forced systems, in-volving a wide range of both primary and specialty
care services, to seek more coordinated, effectiveprogrammes. Coordination of the care given byseveral healthcare professionals can eliminate in-efficiencies and professional service duplications,fulfill lacking components of care and facilitateclear communication of care among everyone in-volved.[19]
3.2 Reduction of Complications andLong Term Costs
Several well controlled studies,[7,8,10] have dem-onstrated that improving glycaemic control cangreatly reduce long term diabetes complications. Itcan be expected that some cost increases for sup-plies, education and pharmacy costs will be re-quired to achieve the improved glycaemic controlas demonstrated by the Diabetes EOC® programme.Short term cost control should not therefore be amajor focus of diabetes disease management.
Although costs for intensive treatment of pa-tients with type 2 diabetes may be higher for cur-rent care, they will presumably be lower for thecare of chronic complications. However, it willtake several years to determine the impact of the
0
10
20
30
40
50
60P
atie
nts
test
ed (
%)
HEDIS1994
HEDIS1995
HEDIS1996
Total1996
Optimal control: HEDISGood control: HEDISOptimal control: total 1996Good control: total 1996
Fig. 4. Health Plan Employer Data and Information Set (HEDIS) and total population percentages in optimal (<7%) and good (7.1to 8%) control for haemoglobin A1c (HbA1c) levels.
70 Gleeson et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

Diabetes EOC® programme on the incidence of longterm complications and costs. If improved glycae-mic control can be sustained, long term expensivecomplications such as amputations (surgeries,prosthesis) and end-stage renal disease (dialysis)can potentially be reduced, but the cost-savingswill not be seen immediately.
Disease management programmes address mul-tiple issues simultaneously, including quality im-provement, efficient resource utilisation, patient/employer satisfaction, provider satisfaction, mar-keting, health plan membership retention and ac-creditation. These are possible cost-benefits of dis-ease management that are difficult to quantify andmay not be immediately realised.
3.3 Meeting AccreditationRequirements
Diabetes disease management programmes canhelp healthcare organisations meet accreditationrequirements and potentially achieve an advantagein the competitive US market place. The LHS sys-tem-wide EOC® disease management programmeis a comprehensive programme that fulfills the re-quirements of several agencies. For example, tem-plates were designed to demonstrate linkages be-tween EOC® activities and the Joint Commissionon Accreditation of Healthcare Organizations(JCAHO) functions, specifically illustrated for theDiabetes EOC® programme. Because of the signif-icant contributions of the EOC® teams, in 1996LHS received full accreditation from both theNational Committee for Quality Assurance andJCAHO, as well as being the first JCAHO networkaccreditation site in the country. The recognitionreceived from these credentialling agencies differ-entiates the Lovelace Health Plan from its compet-itors.
4. Conclusions
Diabetes mellitus is a chronic disease state thatrequires coordinated, multidisciplinary medicalcare and patient education to prevent acute compli-cations and reduce the risk of long term complica-
tions. Disease management initiatives such as theDiabetes EOC® programme have been designed toprovide high quality care in a cost-efficient mannerto large patient populations. If these programmescan improve glycaemic control and other aspectsof diabetes management, reductions in long termtreatment costs will likely follow and possiblycompensate for short term cost increases. Meetingaccreditation requirements can be a competitiveadvantage achieved by a diabetes disease manage-ment programme.
References1. American Diabetes Association. Direct and indirect costs of
diabetes in the United States in 1992. Alexandria (VA): Amer-ican Diabetes Association, 1993
2. Rubin RJ, Altman WM, Mendelson DN. Health care expendi-tures for people with diabetes mellitus, 1992. J Clin Endo-crinol Metab 1994; 78: 809A-809F
3. Crespin Zigich L. Epidemiology report. New Mexico: Depart-ment of Health, Division of Epidemiology, 1995 Jun
4. Kenny SJ, Aubert RE, Geiss, LS. Prevalence and incidence ofnon-insulin-dependent diabetes. In: Diabetes in America. 2nded. Bethesda (MD): National Institutes of Health, 1995. NIHpublication 95-1468
5. Klein R, Klein BE. Vision disorders in diabetes. In: Diabetes inAmerica. 2nd ed. Bethesda (MD): National Institutes ofHealth, 1995. NIH publication 95-1468
6. Nelson RG, Knowler WC, Pettitt DJ, et al. Kidney diseasesin diabetes. In: Diabetes in America. 2nd ed. Bethesda(MD): National Institutes of Health, 1995. NIH publication95-1468
7. The Diabetes Control and Complication Trial ResearchGroup. The effect of intensive treatment of diabetes on thedevelopment and progression of long-term complicationsin insulin-dependent diabetes mellitus. N Engl J Med 1993;329: 977-86
8. Ohkubo Y, Kishakawa H, Araki E, et al. Intensive insulin ther-apy prevents the progression of diabetic microvascular com-plications in Japanese patients with non-insulin dependentdiabetes mellitus: a randomized, prospective 6-year study.Diabetes Res Clin Pract 1995; 28: 103-17
9. Laine C, Caro JF. Preventing complications in diabetes melli-tus: the role of the primary care physician. Med Clin N Am1996; 80 (2): 457-74
10. UK Prospective Diabetes Study (UKPDS) Group Intensiveblood-glucose control with sulphonylureas or insulin com-pared with conventional treatment and risk of complicationsin patients with type 2 diabetes (UKPDS 33). Lancet 1998;352: 837-53
11. American Diabetes Association. Clinical practice recommen-dations – 1997. Diabetes Care 1997; 20 Suppl. 1: 1-70
12. American Diabetes Association. Report of the expert commit-tee on the diagnosis and classification of diabetes mellitus.Diabetes Care 1997; 20: 1183-97
Diabetes Management in a Multispecialty Group Practice 71
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)

13. American Diabetes Association. Standards of medical care forpatients with diabetes mellitus. Diabetes Care 1998; 21 Suppl.1: 23-31
14. Gunter M, Byrnes J, Shainline M, et al. Improving outcomesthrough disease-specific clinical practice improvementteams: the Lovelace Episodes of Care® disease managementprogram. J Outcomes Manage 1996; 3 (3): 10, 11, 14-7
15. Friedman N. Diabetes and managed care. The Lovelace HealthSystem’s Episodes of Care® Program. Managed Care Q 1996;4 (1): 43-9
16. American Diabetes Association. Clinical practice recommenda-tions – 1995. Diabetes Care 1995; 18 Suppl. 1: 1-96
17. American Diabetes Association: Clinical practice recommenda-tions – 1996. Diabetes Care 1996; 19 Suppl. 1: 1-113
18. Adelson R, Hepburn K, Vanloy W. Performance change in anorganizational setting: a conceptual model. J Cont EducHealth Prof 1997; 17 (2): 69-80
19. Quickel KE. Diabetes in a managed care system. Ann InternMed 1996; 124 (1 Pt 2): 160-3
About the Author: Jeremy Gleeson is Chairman of the Di-vision of Endocrinology at Lovelace Health Systems, andMedical Director of the Lovelace Regional Diabetes Program.He has led the diabetes disease management programme atLovelace since 1994. His research interests are clinical andoutcomes research in diabetes and lipid disorders.Correspondence and reprints: Jeremy M. Gleeson, M.B.,FRACP, FACE, Department of Endocrinology, LovelaceHealth Systems, 5400 Gibson Blvd. SE, Albuquerque, NM87108, USA.E-mail: [email protected]
72 Gleeson et al.
© Adis International Limited. All rights reserved. Dis Manage Health Outcomes 1999 Feb; 5 (2)





















