Embed Size (px)
Citation preview

Device therapy for hypertension current status and horizon scanning
Dr Vikas Kapil MA MRCP PhD
Consultant in Clinical Pharmacology
& Cardiovascular Medicine

Disclosures
Research Funding: British Heart Foundation
National Institute for Healthcare Research
Barts Charity
Honoraria: nil
Speaker bureaux: nil
Share holdings: nil

Outline
Renal sympathetectomy (renal denervation)
Carotid baroreflex strategies
Baroreflex Activation Therapy (BAT)
Carotid baroreflex amplification
Central arterio-venous anastomosis
Emerging clinical and pre-clinical stage technologies and strategies
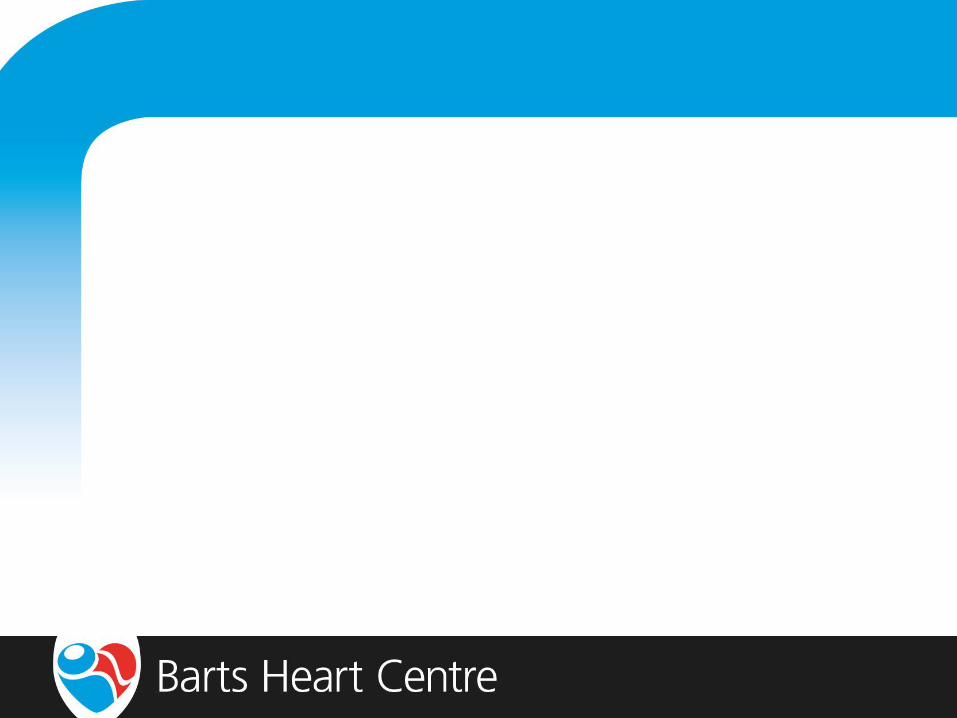
Approaches: targeting the autonomic NS
Schlaich et al., Hypertension 2004; 43: 169-
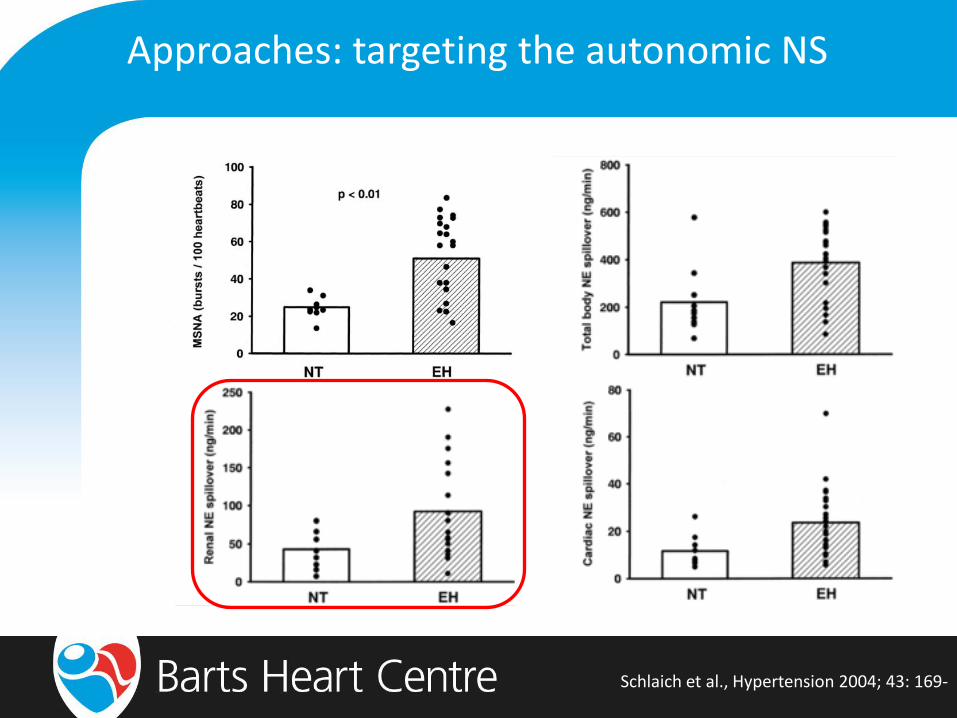
Afferent Renal Sympathetics
The kidney is a source of central sympathetic drive in hypertension, heart failure, chronic kidney disease, and
ESRD
Efferent Sympathetic Activation
Patients cannot develop and/or maintain elevated BP without renal involvement
HR Contractility
RBF/GFR Renin
Na+/Volume
Vasoconstriction
Approaches: renal sympathectomy

Approaches: renal sympathectomy

Approaches: renal sympathectomy
Ott & Schmeider, Curr Hypertes Rep 2015; 17: 65-

Approaches: renal sympathectomy
Ott & Schmeider, Curr Hypertes Rep 2015; 17: 65-

Approaches: renal sympathectomy
Kindermann et al., J Clin Hypertens 2017: 1-

Approaches: renal sympathectomy
Kindermann et al., J Clin Hypertens 2017: 1-

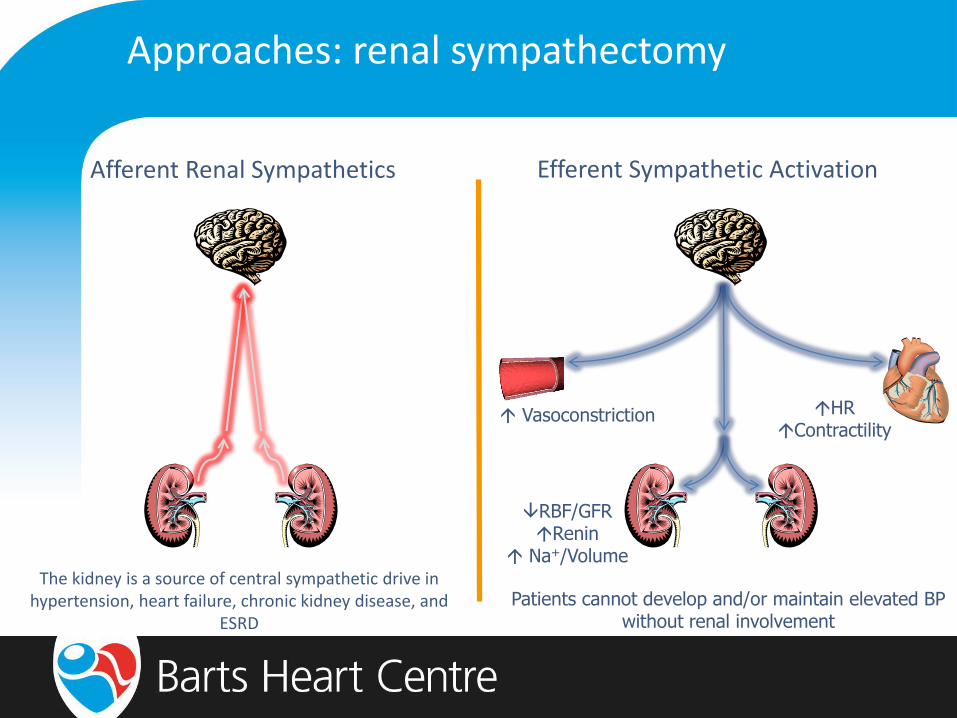
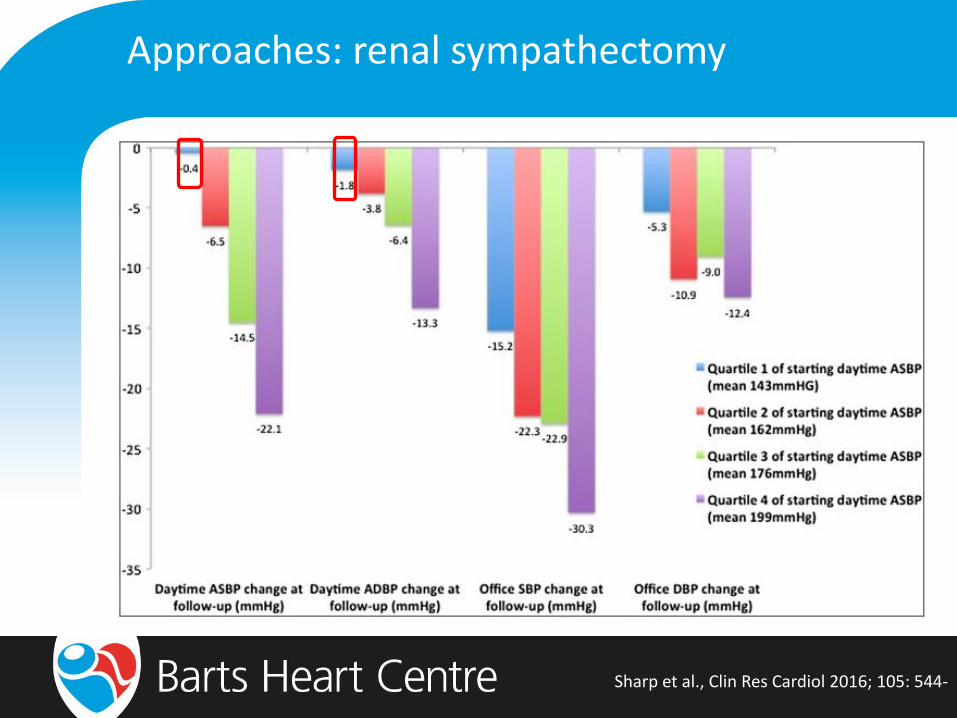
Approaches: renal sympathectomy
Sharp et al., Clin Res Cardiol 2016; 105: 544-
Approaches: renal sympathectomy
Sharp et al., Clin Res Cardiol 2016; 105: 544-
Approaches: renal sympathectomy
Desch et al., Hypertension 2015; 54: 1202-
Randomised, sham controlled, blinded study
RF RSD vs renal angiography
Mild resistant HTN: 24h BP: S 135-149 and/or D 90-94 mmHg
3 medications (inc diuretic)
Screened: 1006
Eligible: 156
Randomised 71
ITT: 67
PP: 63

Approaches: renal sympathectomy
Desch et al., Hypertension 2015; 54: 1202-

Williams et al., Lancet 2015; 386: 2059-

Approaches: renal sympathectomy
Templin et al., Eur Heart J 2013; 34: 2141-
Vasospasm Oedema Dissection Thrombus

Approaches: renal sympathectomy
Baseline 6 months post-RDN
Left renal artery
Right renal artery
Persu et al., J Hypertens 2014; 32: 2102-

Approaches: renal sympathectomy
Bhatt et al., N Engl J Med 2014; 370: 15-

Approaches: renal sympathectomy
Criticisms of and pitfalls in Symplicity HTN-3:
Medicine stability
changes within 2 weeks of study entry allowed
40% of both groups had medication changes within randomisation period
baseline differences in use of spironolactone/vasodilators between groups
Procedural
new technique with inadequate proctoring
inadequate burns [number/location] to achieve renal sympathectomy
Approaches: renal sympathectomy
NHS England. 2016
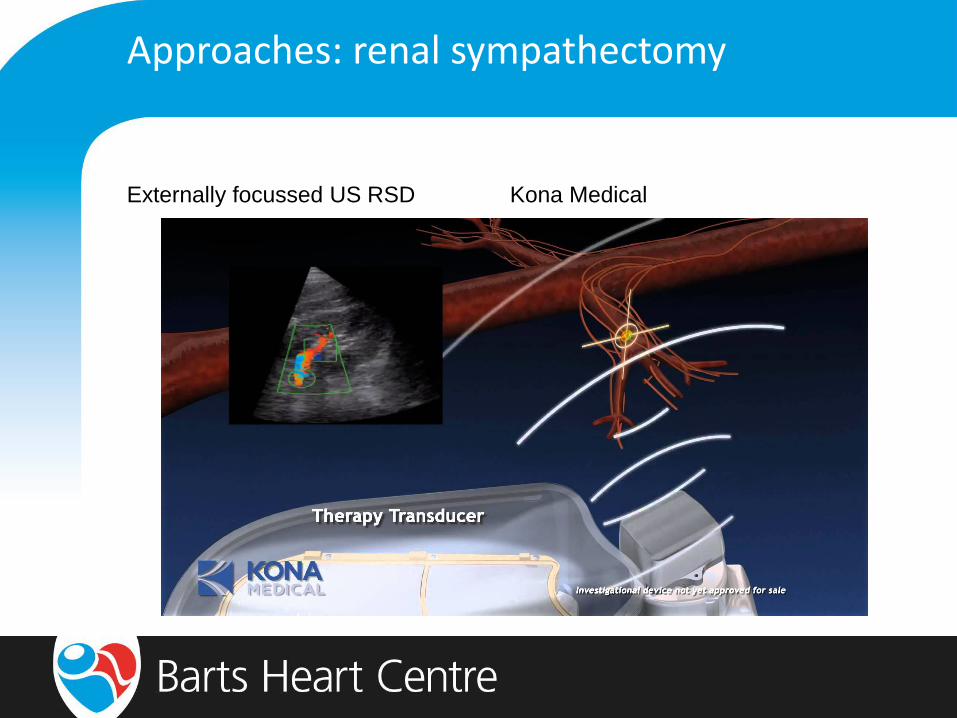
Approaches: renal sympathectomy
Externally focussed US RSD Kona Medical

Approaches: renal sympathectomy
Externally focussed US RSD Kona Medical

Approaches: renal sympathectomy
WAVE IV
Randomised, sham-controlled, blinded trial
Focussed, diagnostic US vs focussed, [therapeutic] high intensity US energy
n=132
Primary efficacy end point: change in OBP at 6m
Secondary efficacy end point: change in 24h ABP at 6m
clinicaltrials.gov/NCT02029885

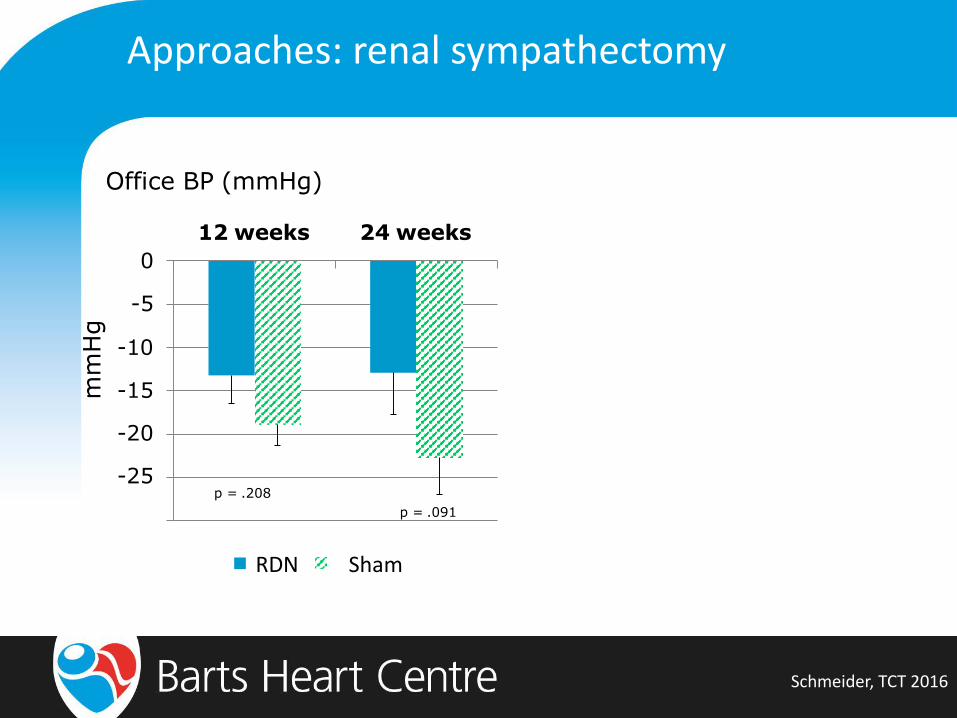
Approaches: renal sympathectomy
Schmeider, TCT 2016
Category Sham Treatment
number 39 42
Male/Female 25/14 30/12
Age, years 62.0 (11.1) 60.3 (11.2)
Ethnicity (W/B/Asian/Other) 30/2/4/3 32/3/3/4
BMI, kg/m² 29.8 (4.2) 29.9 (4.5)
Office SBP, mmHg 184.8 (18.2) 181.1 (19.7)
Office BP, mmHg 100.3 (16.2) 99.5 (16.5)
24h SBP, mmHg 155.5 (11.8) 155.7 (14.3)
24h DBP, mmHg 87.2 (13.1) 86.8 (11.4)
Heart rate, bpm 70.6 (15.8) 68.4 (12.1)
Meds, number 5.0 (1.5) 4.3 (1.4)
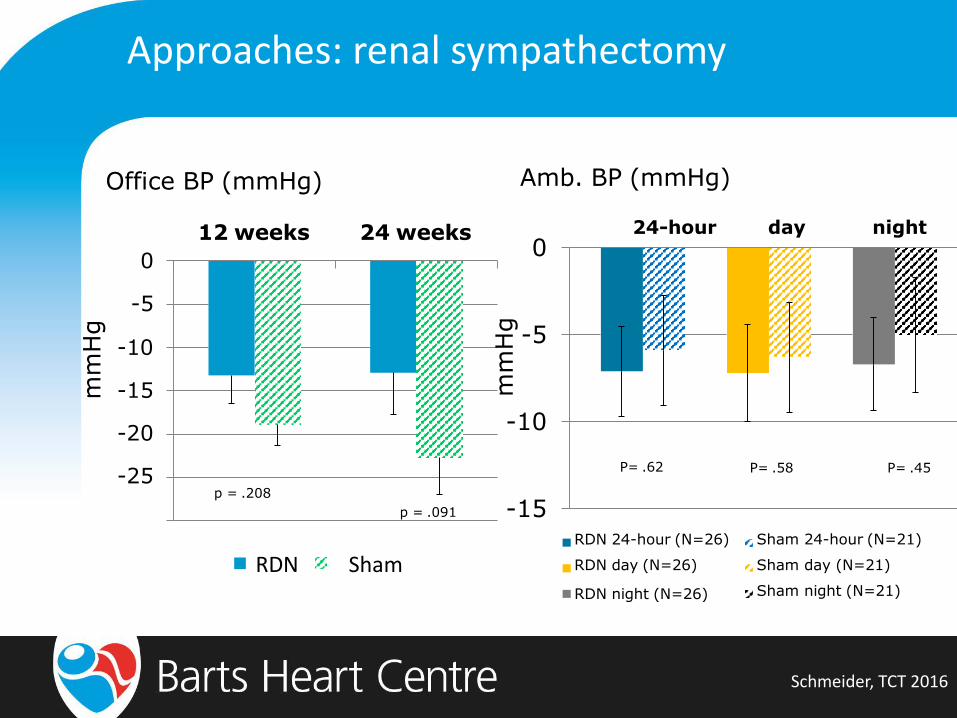
Approaches: renal sympathectomy
Schmeider, TCT 2016
Office BP (mmHg)
N=39 N=29
-10
-15
-20
-25
0
-5
12 weeks 24 weeks
mm
Hg
p = .208
p = .091
RDN Sham
Approaches: renal sympathectomy
Schmeider, TCT 2016
Office BP (mmHg)
N=39 N=29
-10
-15
-20
-25
0
-5
12 weeks 24 weeks
mm
Hg
p = .208
p = .091 -15
-10
-5
0
RDN 24-hour (N=26)
RDN day (N=26)
RDN night (N=26)
Sham 24-hour (N=21)
Sham day (N=21)
Sham night (N=21)
24-hour day night
Amb. BP (mmHg)
mm
Hg
P= .62 P= .58 P= .45
RDN Sham
Approaches: renal sympathectomy
Decision to stop trial in July 2016 on grounds of futility after interim analysis
No safety concerns identified
n=81 completed primary end point analysis
Schmeider, TCT 2016

Approaches: renal sympathectomy
Is this the end of renal sympathectomy?

Approaches: renal sympathectomy
Issues to be solved
What is the true effect of RSD, taking out medication/adherence effects?
Can we identify patients who will respond?
Can we identify if we have achieved renal denervation?
Do we need to know which technologies are better?
Approaches: renal sympathectomy
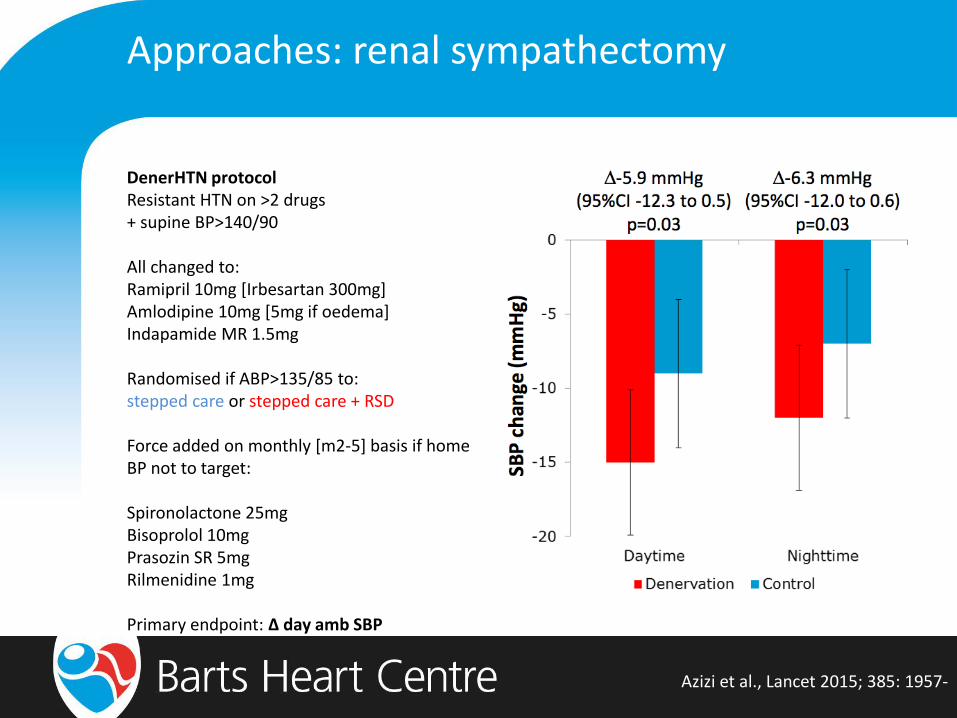
Azizi et al., Lancet 2015; 385: 1957-
DenerHTN protocol Resistant HTN on >2 drugs + supine BP>140/90 All changed to: Ramipril 10mg [Irbesartan 300mg] Amlodipine 10mg [5mg if oedema] Indapamide MR 1.5mg Randomised if ABP>135/85 to: stepped care or stepped care + RSD Force added on monthly [m2-5] basis if home BP not to target: Spironolactone 25mg Bisoprolol 10mg Prasozin SR 5mg Rilmenidine 1mg Primary endpoint: Δ day amb SBP

Approaches: renal sympathectomy
Azizi et al., Circulation 2016; 134: 847-
DenerHTN protocol Resistant HTN on >2 drugs + supine BP>140/90 All changed to: Ramipril 10mg [Irbesartan 300mg] Amlodipine 10mg [5mg if oedema] Indapamide MR 1.5mg Randomised if ABP>135/85 to: stepped care or stepped care + RSD Force added on monthly [m2-5] basis if home BP not to target: Spironolactone 25mg Bisoprolol 10mg Prasozin SR 5mg Rilmenidine 1mg Primary endpoint: Δ day amb SBP
50% of patients non adherent [partial or complete] Not difference in either group No difference in magnitude of effect of RSD in sub groups
Approaches: renal sympathectomy
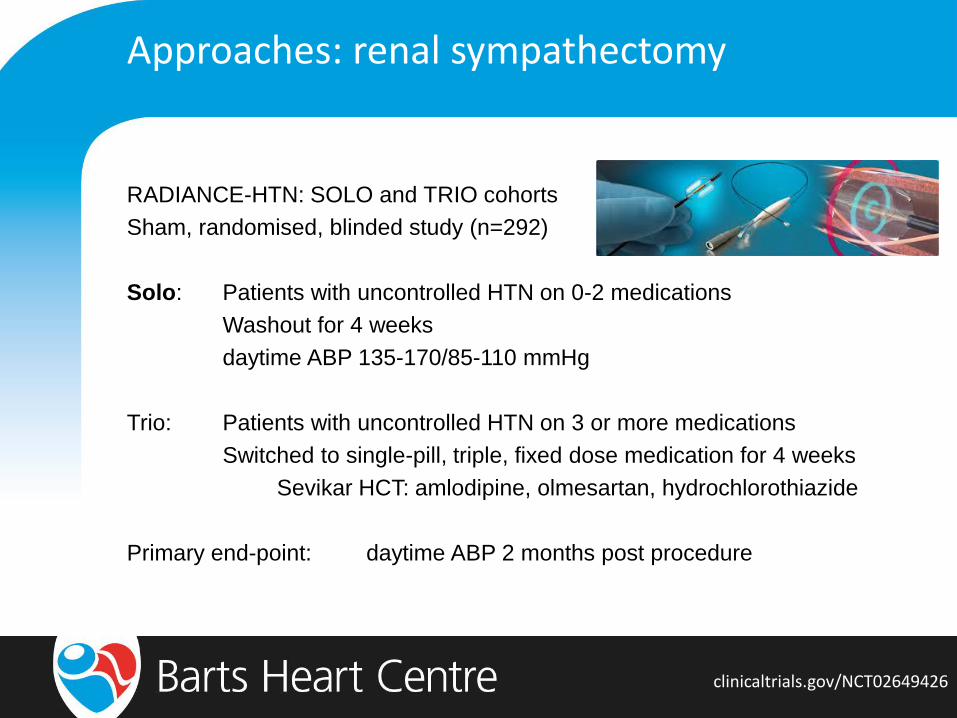
clinicaltrials.gov/NCT02649426
RADIANCE-HTN: SOLO and TRIO cohorts
Sham, randomised, blinded study (n=292)
Solo: Patients with uncontrolled HTN on 0-2 medications
Washout for 4 weeks
daytime ABP 135-170/85-110 mmHg
Trio: Patients with uncontrolled HTN on 3 or more medications
Switched to single-pill, triple, fixed dose medication for 4 weeks
Sevikar HCT: amlodipine, olmesartan, hydrochlorothiazide
Primary end-point: daytime ABP 2 months post procedure
Approaches: renal sympathectomy
Issues to be solved
What is the true effect of RSD, taking out medication/adherence effects?
Can we identify patients who will respond?
Can we identify if we have achieved renal denervation?
Do we need to know which technologies are better?

Approaches: renal sympathectomy
Mahfoud et al., Eur Heart J 2017; 38: 93-

Approaches: renal sympathectomy
de Jong et al., Hypertension 2016; 68: 707-

Approaches: renal sympathectomy
Issues to be solved
What is the true effect of RSD, taking out medication/adherence effects?
Can we identify patients who will respond?
Can we identify if we have achieved renal denervation?
Do we need to know which technologies are better?
Approaches: renal sympathectomy
ATTENUATION OF SPLANCHNIC AUTOTRANSFUSION FOLLOWING NON-
INVASIVE ULTRASOUND RENAL DENERVATION: A NOVEL MARKER OF
PROCEDURAL SUCCESS
Manish Saxena, Tariq Shour, Mussadiq Shah, Christopher Wolff, David J Collier,
Vikas Kapil, Armida Balawon, Jane Pheby, Anne Zak, Peter Julu, Benjamin
O’Brien, Roland E. Schmieder, Melvin D Lobo
ESH 2017 Oral presentation

Approaches: renal sympathectomy
Issues to be solved
What is the true effect of RSD, taking out medication/adherence effects?
Can we identify patients who will respond?
Can we identify if we have achieved renal denervation?
Do we need to know which technologies are better?
Approaches: renal sympathectomy
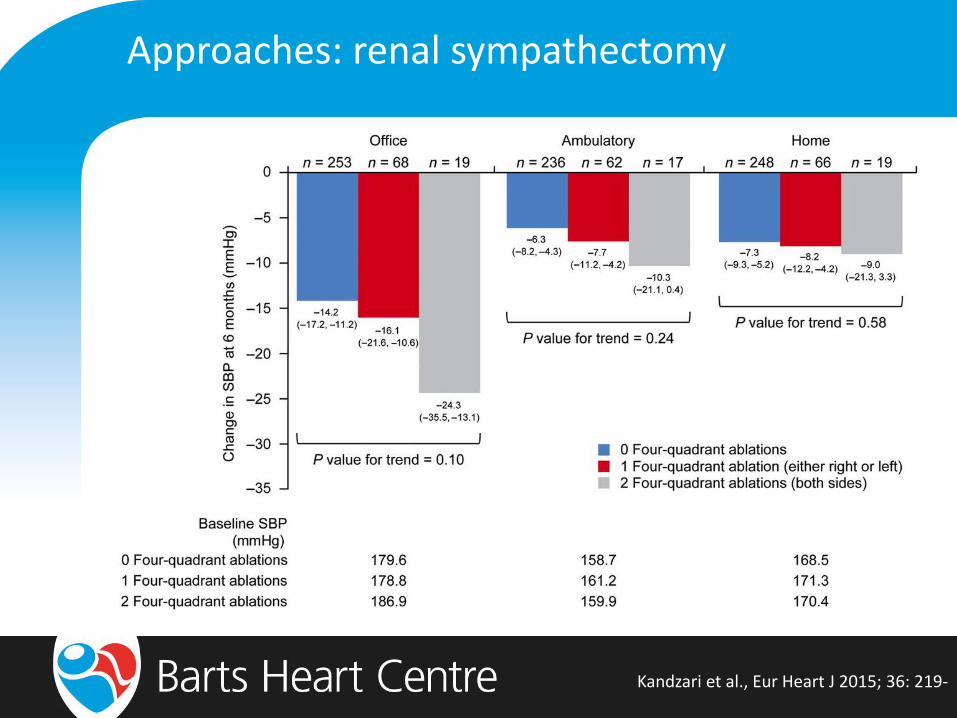
Kandzari et al., Eur Heart J 2015; 36: 219-

Approaches: renal sympathectomy
Mahfoud et al., J Am Coll Cardiol; 2015: 1766-

Approaches: renal sympathectomy
Pekarskiy et al., J Hypertens 2017; 35: 369-
Approaches: renal sympathectomy
clinicaltrials.gov/NCT02920034
RADIOSOUND study
Resistant HTN on stable meds for 4 weeks
OBP >160 mmHg
US main braches
vs
RF main branches
vs
RF main and accessory branches
n=120
Primary end point: daytime ABP at 3m
Approaches: renal sympathectomy
clinicaltrials.gov/NCT02920034
How do we design robust clinical studies that give meaningful results when
interventional sham procedures give such a large reduction in BP?
Approaches: baroreflex modulation
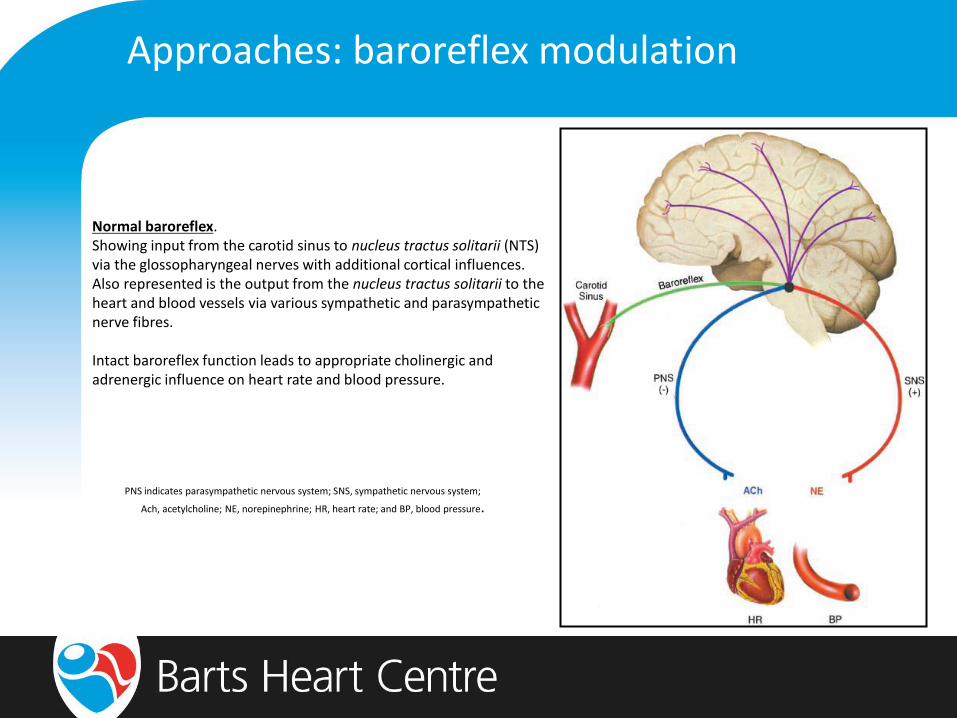
Normal baroreflex. Showing input from the carotid sinus to nucleus tractus solitarii (NTS) via the glossopharyngeal nerves with additional cortical influences. Also represented is the output from the nucleus tractus solitarii to the heart and blood vessels via various sympathetic and parasympathetic nerve fibres. Intact baroreflex function leads to appropriate cholinergic and adrenergic influence on heart rate and blood pressure. PNS indicates parasympathetic nervous system; SNS, sympathetic nervous system;
Ach, acetylcholine; NE, norepinephrine; HR, heart rate; and BP, blood pressure.

Approaches: baroreflex modulation

Approaches: baroreflex amplification
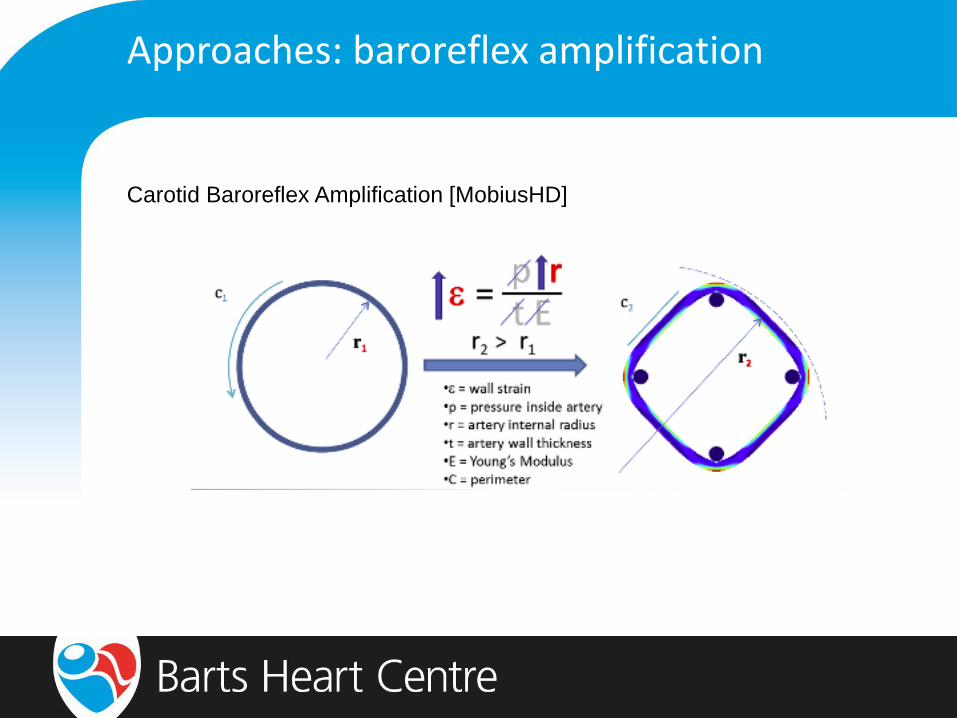
Carotid Baroreflex Amplification [MobiusHD]
Approaches: baroreflex amplification
Carotid Baroreflex Amplification [MobiusHD]

Approaches: baroreflex amplification
CALM FIM Europe & US studies [n=50 total]
Neuro-interventional radiologists experienced in carotid stent placement [>100]
US Duplex and CT or MR angiography to determine suitability
DAPT required pre and post procedure
OBP > 160 mmHg
3 medications (inc diuretic)

Approaches: baroreflex amplification
Spiering, TCT 2016

Approaches: baroreflex amplification
Spiering, TCT 2016

Approaches: baroreflex amplification
CALM START
randomised, sham-controlled, end-point blinded study
n=110
ON meds: resistant HTN (3 meds inc diuretic) for 4 weeks
24h daytime ASBP 135-170 mmHg
OFF meds: 24h daytime ASBP 135-170 mmHg after medication washout
Primary outcome: difference in change in 3m ASBP
Approaches: baroreflex activation

Approaches: baroreflex activation
Heusser et al., Hypertension 2010; 55: 619-
Rheos (1st Generation)

Approaches: baroreflex activation
Hoppe et al., J Am Soc Hypertens 2012; 6: 270-
Rheos (1st Generation) Next-generation Barostim neo
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 1 2 3 4 5 6Pe
rce
nt
Fre
e f
rom
Co
mp
lic
ati
on
Months from Implant
1st Generation Rheos
2nd Generation neo

Approaches: baroreflex activation
Hoppe et al., J Am Soc Hypertens 2012; 6: 270-
Next-generation Barostim neo

Approaches: baroreflex activation
Floyd et al., Int J Cardiol 2016; 220: 517-
BAT for extreme BP variability
First in man use
49y old man of work for 2y because
of symptomatic extremes of BP
Systemic sclerosis related autonomic
neuropathy
intact baroreflex on physiological
stimulation
BAT implanted locally in Galway
Approaches: baroreflex activation
BAT in UK
First in UK use for BP variability UK BAT 001
reduced frequency of blackouts and hospital admissions
no longer on oral medications for HTN
on transdermal clonidine
First in UK use for refractory hypertension UK BAT 002
2007-2011; 6 admissions with HTN urgencies/emergencies
total in-patient time: 9 months
On 7 medications orally negative tablet feed study
home BP 240/110
No response RF RSD; no response CB excision; unsuitable conduit AVA
Improved OBP 180/100 on no anti HTN meds

Approaches: baroreflex activation
NICE IPG 533 Cot 2015
“Current evidence on the safety and efficacy of implanting a baroreceptor stimulation device for resistant hypertension is inadequate. Therefore, this procedure should only be used in the context of research.”

Approaches: baroreflex activation
BAT in rest of world
Large studies in resistant hypertension recruiting in:
France French BAT study
Finland Nordic BAT study
Company has pulled out of funding further studies in HTN in Europe
has CE mark
going for heart failure indication
Future for BAT in UK unclear…
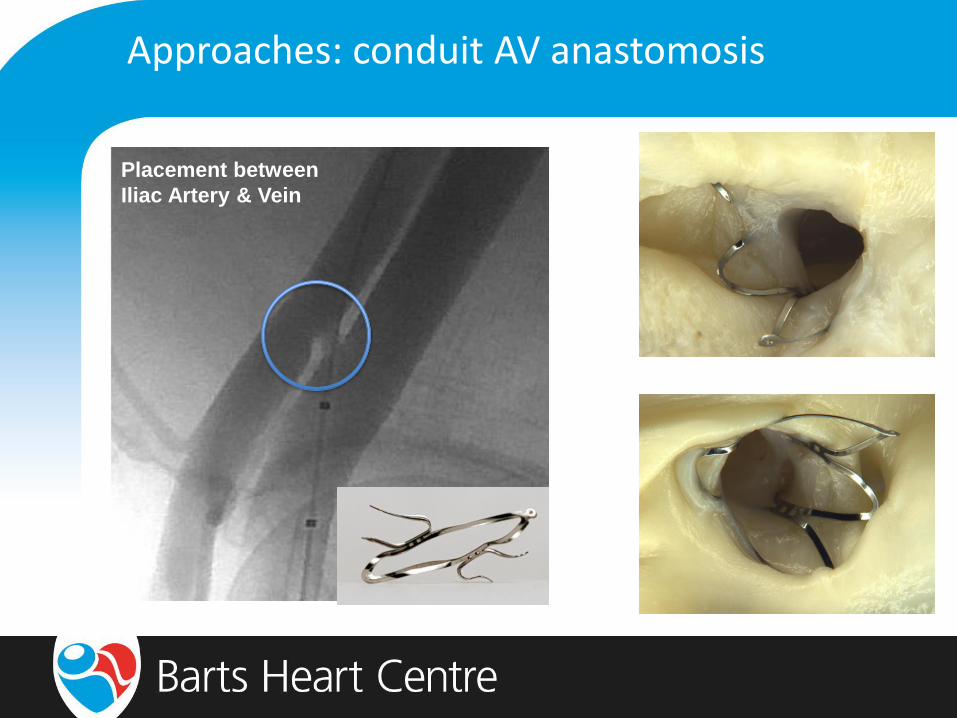
Approaches: conduit AV anastomosis
Placement between
Iliac Artery & Vein

Approaches: conduit AV anastomosis
Approaches: conduit AV anastomosis
Prospective, Randomized, Controlled, Blinded-Endpoint
OBP >140 and daytime ABP S >135 and/or D >85 mmHg
3 meds inc diuretic, maintained for 6m
Primary endpoints:
Change in mean 24-hour ABPM SBP at six months as compared to baseline
Change in mean office SBP at six months as compared to baseline
Secondary endpoints:
Change in mean 24-hour ABPM DBP at six months as compared to baseline
Change in mean office DBP at six months as compared to baseline
Incidence of complications associated with delivery and/or use of the ROX
Coupler

Approaches: conduit AV anastomosis
ROX Coupler (n = 44)
Control (n = 39)
Age (years) 59 ± 9 58 ± 9
Sex (female) 11 (25%) 14 (36%)
Race (white) 40 (91%) 31 (79%)
Body-mass index (kg/m2) 30 ± 4 30 ± 5
eGFR (ml/min) MDRD Calculation 76 ± 20 77 ± 18
Previous renal denervation 10 (23%) 7 (18%)
Coronary artery disease 7 (16%) 10 (26%)
Type 2 diabetes mellitus 9 (20%) 5 (13%)
Prior cerebrovascular events 5 (11%) 8 (21%)
Baseline office systolic BP (mm Hg) 175 ± 18 171 ± 22
Baseline office diastolic BP (mm Hg) 100 ± 13 100 ± 18
Baseline 24-Hr ABPM systolic BP (mm Hg) 157 ± 15 156 ± 14
Baseline 24-Hr ABPM diastolic BP (mm Hg) 93 ± 11 93 ± 13
Lobo et al., Lancet 2015; 385: 9978-

Approaches: conduit AV anastomosis
Lobo et al., Lancet 2015; 385: 9978-

Approaches: conduit AV anastomosis
Lobo, ESC 2016

Approaches: conduit AV anastomosis
Lobo, ESC 2016

Approaches: conduit AV anastomosis
Lobo, ESC 2016

Approaches: central AV anastomosis
ROX in the rest of world
Sham controlled US IDE study started March 2017 [n=500]
24h ABP at 6m
ROX registry study ongoing
Other technologies
Approaches: short AV pacing
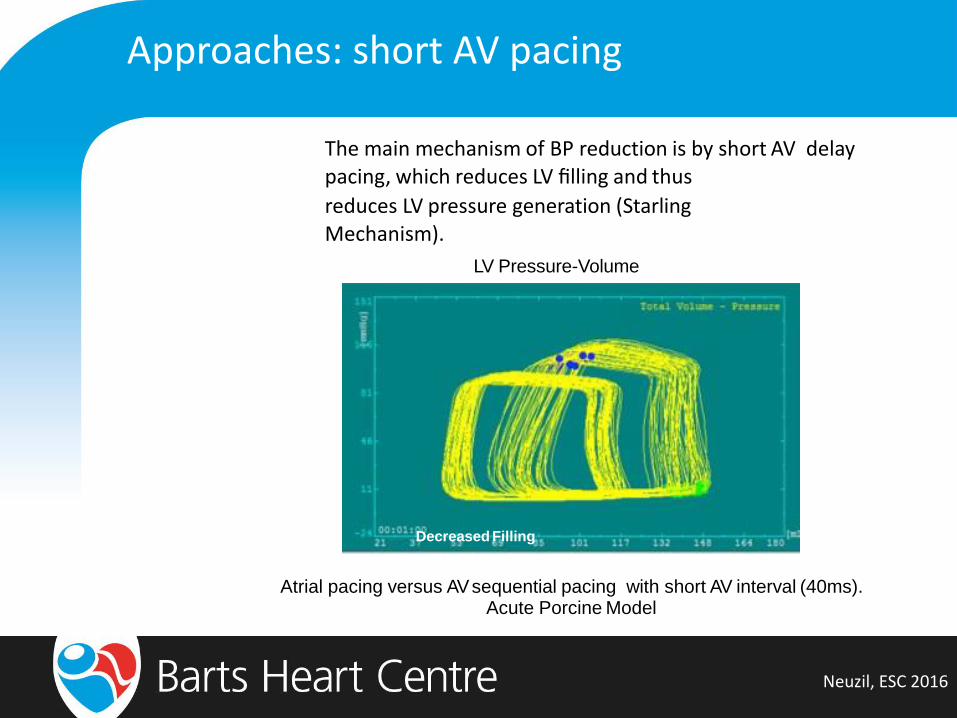
The main mechanism of BP reduction is by short AV delay pacing, which reduces LV filling and thus
reduces LV pressure generation (Starling Mechanism).
LV Pressure-Volume
Decreased Filling
Atrial pacing versus AV sequential pacing with short AV interval (40ms). Acute Porcine Model
Neuzil, ESC 2016

Approaches: short AV pacing
Neuzil, ESC 2016
Approaches: short AV pacing
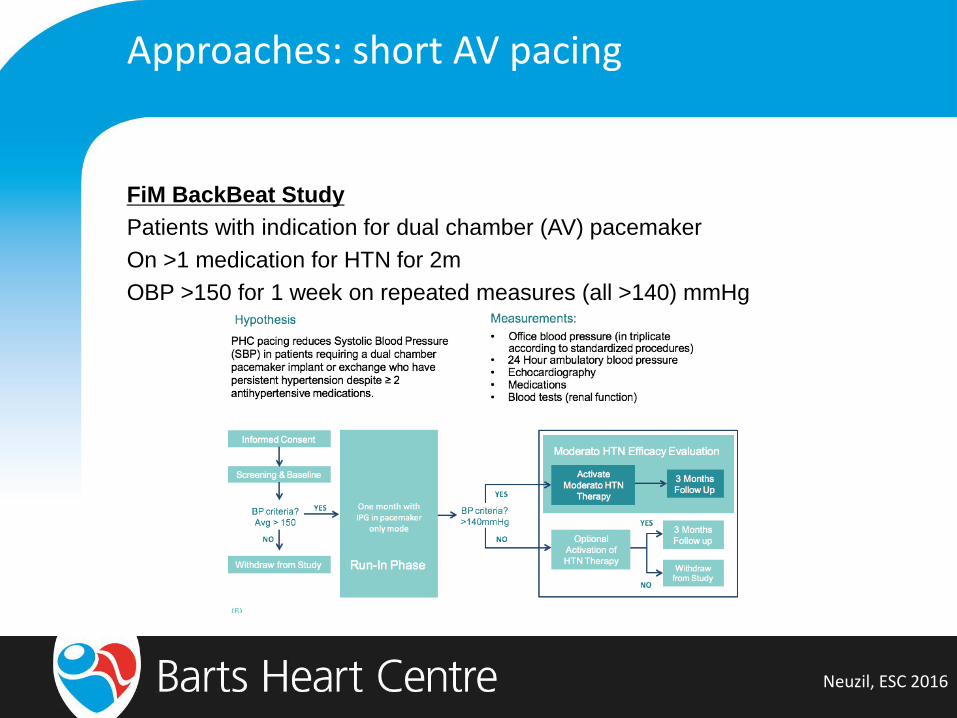
FiM BackBeat Study
Patients with indication for dual chamber (AV) pacemaker
On >1 medication for HTN for 2m
OBP >150 for 1 week on repeated measures (all >140) mmHg
Neuzil, ESC 2016

Approaches: short AV pacing
Neuzil, ESC 2016

Approaches: short AV pacing

Approaches: vagal nerve stimulation
Pre-clinical data only
Hampered by tendency to cause bradycardia, bradypnoea
Novel cuffed electrode may overcome these issues

Approaches: vagal nerve stimulation

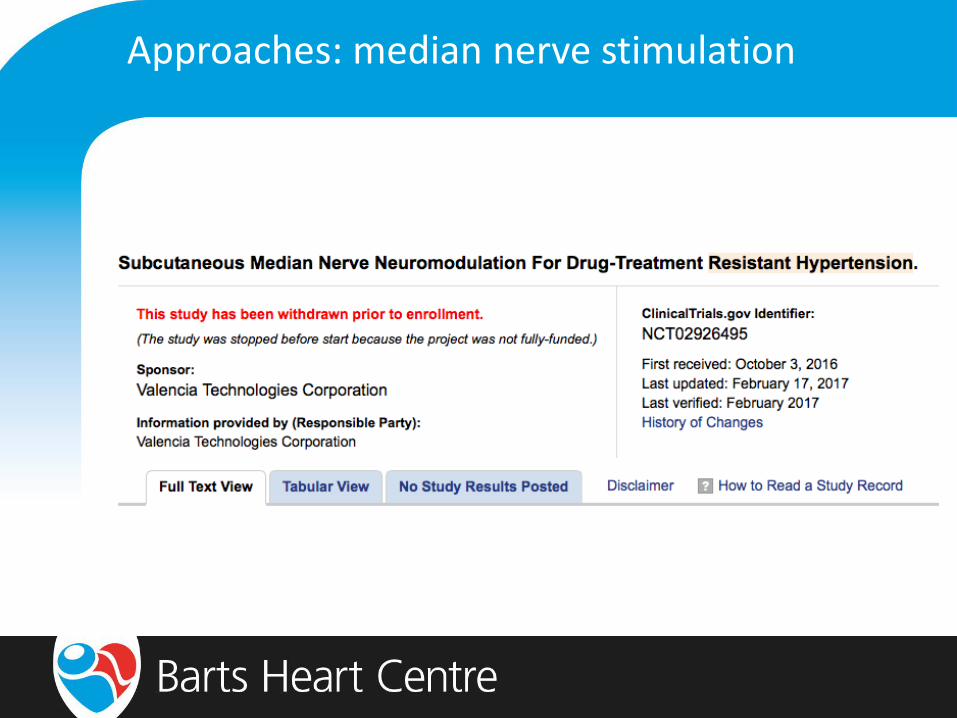
Approaches: median nerve stimulation
Median Nerve Stimulation [Valencia]
positive FiM (n=96) [abstract]
Approaches: median nerve stimulation

Approaches: carotid body modulation
Carotid Body Excision/Ablation

Approaches: carotid body modulation
Narkiewicz et al., JACC Basic Trans Science 2016; 1: 313-

Approaches: carotid body modulation
Narkiewicz et al., JACC Basic Trans Science 2016; 1: 313-
Responders had higher levels of peripheral chemoreceptor activity prior to
resection
higher hypoxic ventilatory drive
faster ventilatory frequency [short nitrogen breathing protocol]
Possible to identify responders
Possibly amenable to endovascular approach

Approaches: chemical RSD with ethanol
Fischell et al., JACC Cardiovasc Interv 2016; 9: 589-
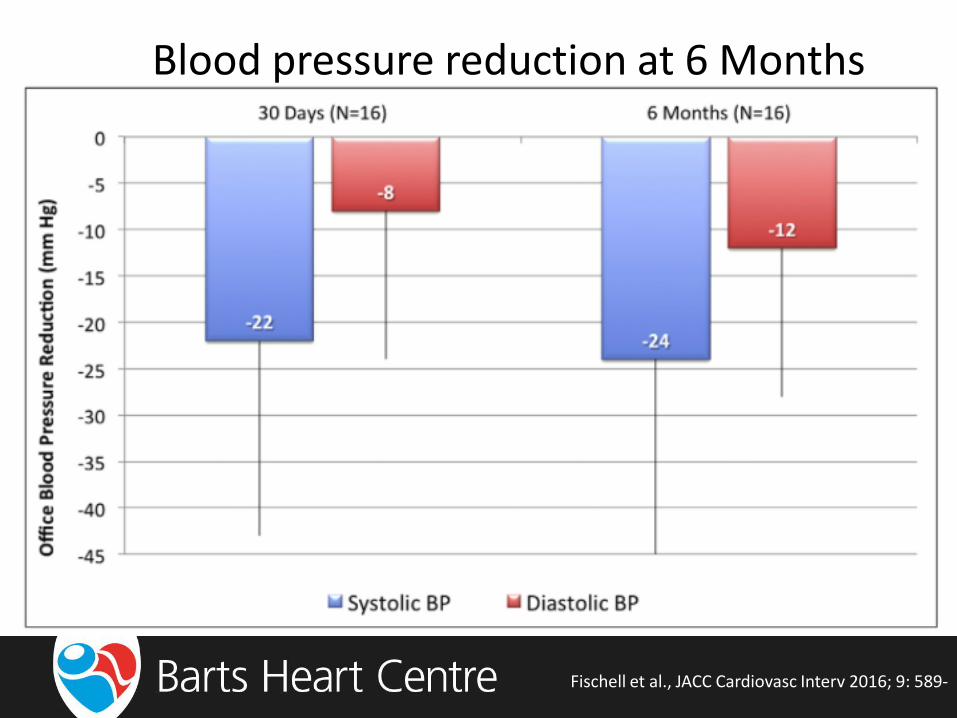
Blood pressure reduction at 6 Months
Fischell et al., JACC Cardiovasc Interv 2016; 9: 589-
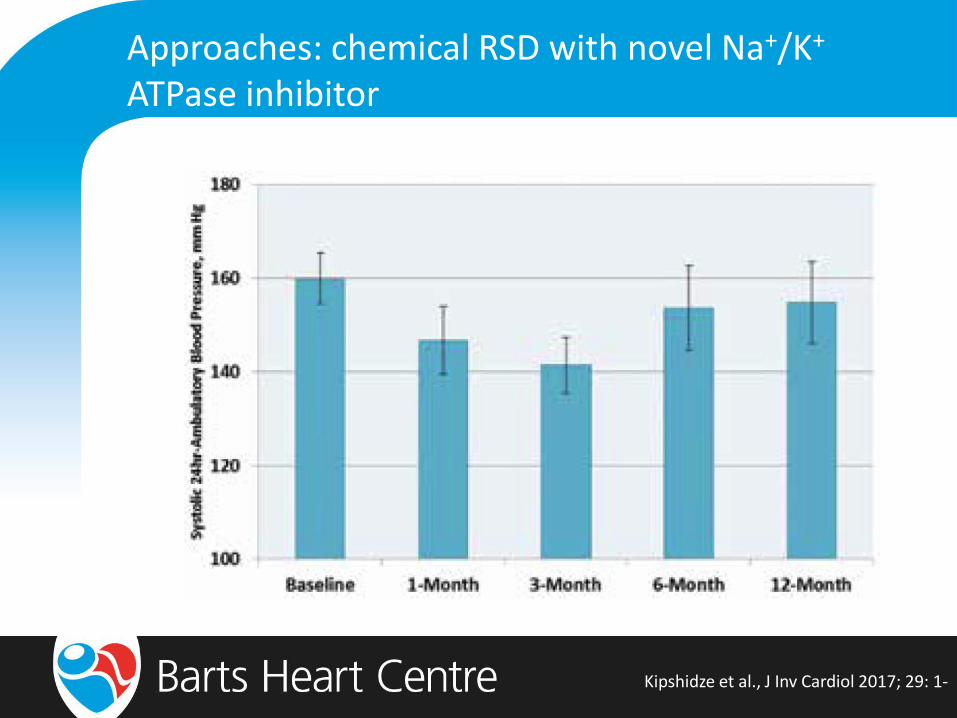
Approaches: chemical RSD with novel Na+/K+ ATPase inhibitor
Kipshidze et al., J Inv Cardiol 2017; 29: 1-

Approaches: pizoelectric gastric stimulation
medautonomic.com
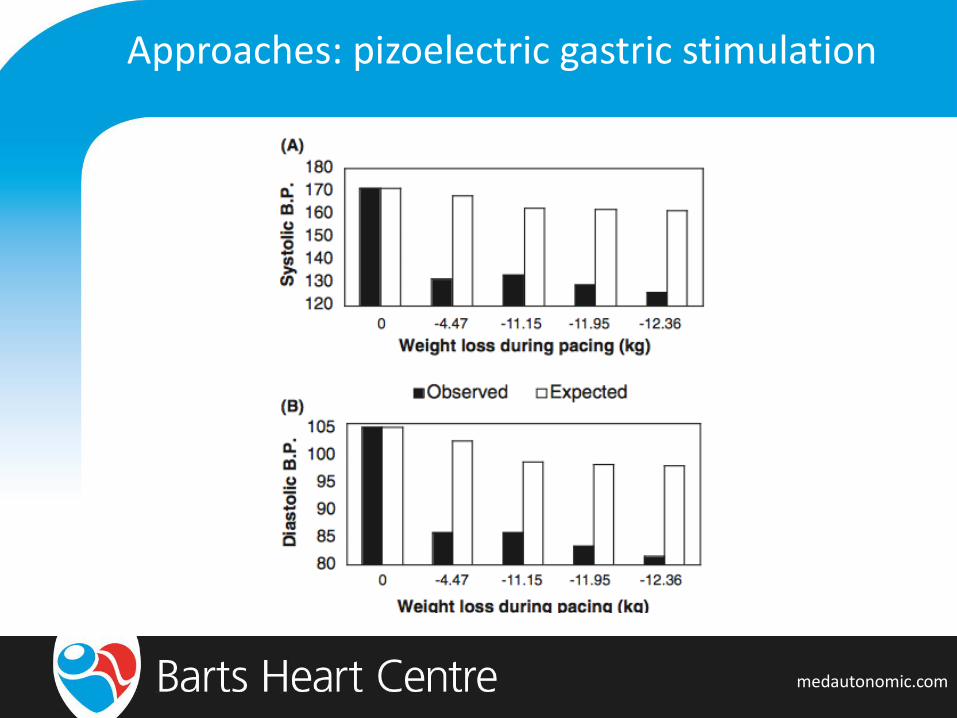
Approaches: pizoelectric gastric stimulation
medautonomic.com